Embed Size (px)
Citation preview

Chronic myeloid leukemia (CML)
Warunsuda Sripakdee, BCOP,BCP Prince of Songkla University
1

2
Hematologic malignancies
CML
AMLALL

3
CML
CD34+
results from an acquired mutation that affects hematopoietic stem cells
excessive mature neutrophil production
median age at diagnosis is 67 years old more common in males
4
© 2007 Terese Winslow LLC, U.S. Govt. has certain rights
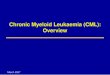
Figure 1. The pathogenesis of CML. Portions of chromosomes 9 and 22 break off and exchange positions. The bcr-abl gene is formed on chromosome 22 where the piece of chromosome 9 attaches. The changed chromosome 22 is called the Philadelphia chromosome.10
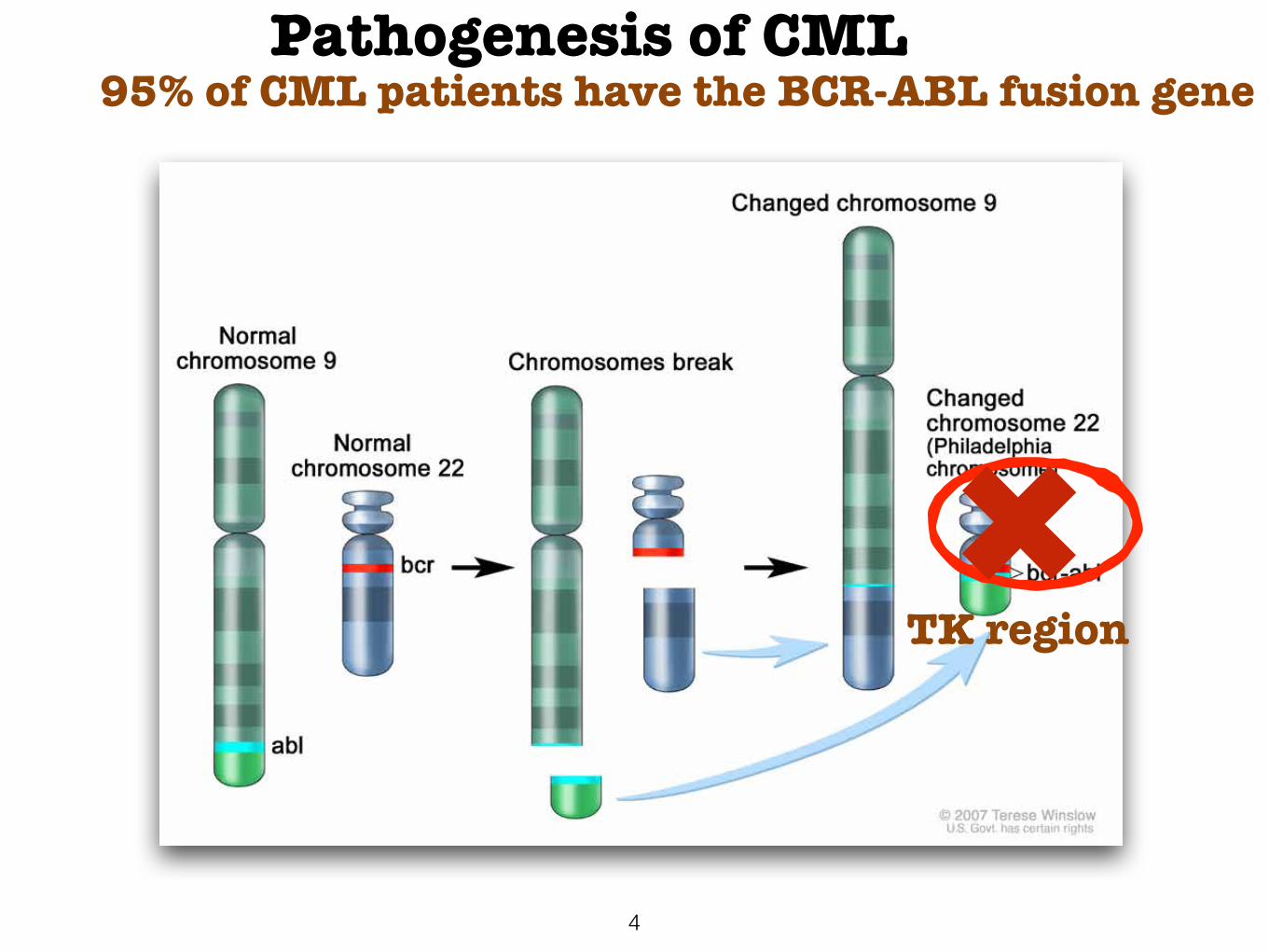
3. The BCR-ABL protein contains the active tyrosine kinase region of ABL, also known as p210BCR-ABL.
a. Typically, the ABL tyrosine kinase carefully regulates downstream targets that are critical to the proliferation and survival of normal cells.
b. Instead, the BCR-ABL fusion protein produces a cytokine-independent, constitutive proliferative signal.
4. The hyperactivity of the BCR-ABL tyrosine kinase signal results in continuous cell cycling and proliferation, altered differentiation, and a loss of apoptosis.
C. Up to 95% of CML patients have the BCR-ABL fusion gene.1, 12, 13
D. Additional cytogenetic abnormalities may develop as a result of BCR-ABL promoting instability of the leukemic clone.12
1. As the leukemic clone expands, the marrow progenitor cells become increasingly likely to undergo proliferation with less capacity for self-renewal.
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
Pathogenesis of CML
TK region
95% of CML patients have the BCR-ABL fusion gene
ₒ
5
Molecular abnormality in CML

6
Molecular abnormality in CML promoting instability of the
leukemic clone marrow progenitor cells -
increasing ly l ikely to undergo proliferation
less capacity for self-renewal
!Additional cytogenetic abnormalities such as trisomy
8, isochromosome 17, trisomy 21 and deletion 7
End-stage disease

7
Risk Factors : ionizing radiation Signs and symptoms
!
CML
Clinical Laboratory Bone marrow
- abdominal pain - early satiety due
to splenomegaly - anorexia - bone pain
purport - unexplained
weight loss ±fatigue
- leukocytosis(usually >25,000 cells/mm
- increased LDH - other CBC:
megakaryocytosis, basophilia, eosinophilia
- hypercellular (75-90%)
- increased erythropoiesis & megakaryocytic
- Blasts <10%

8
Natural history of disease
Chronic phase
Accelerated phase
Blast phase
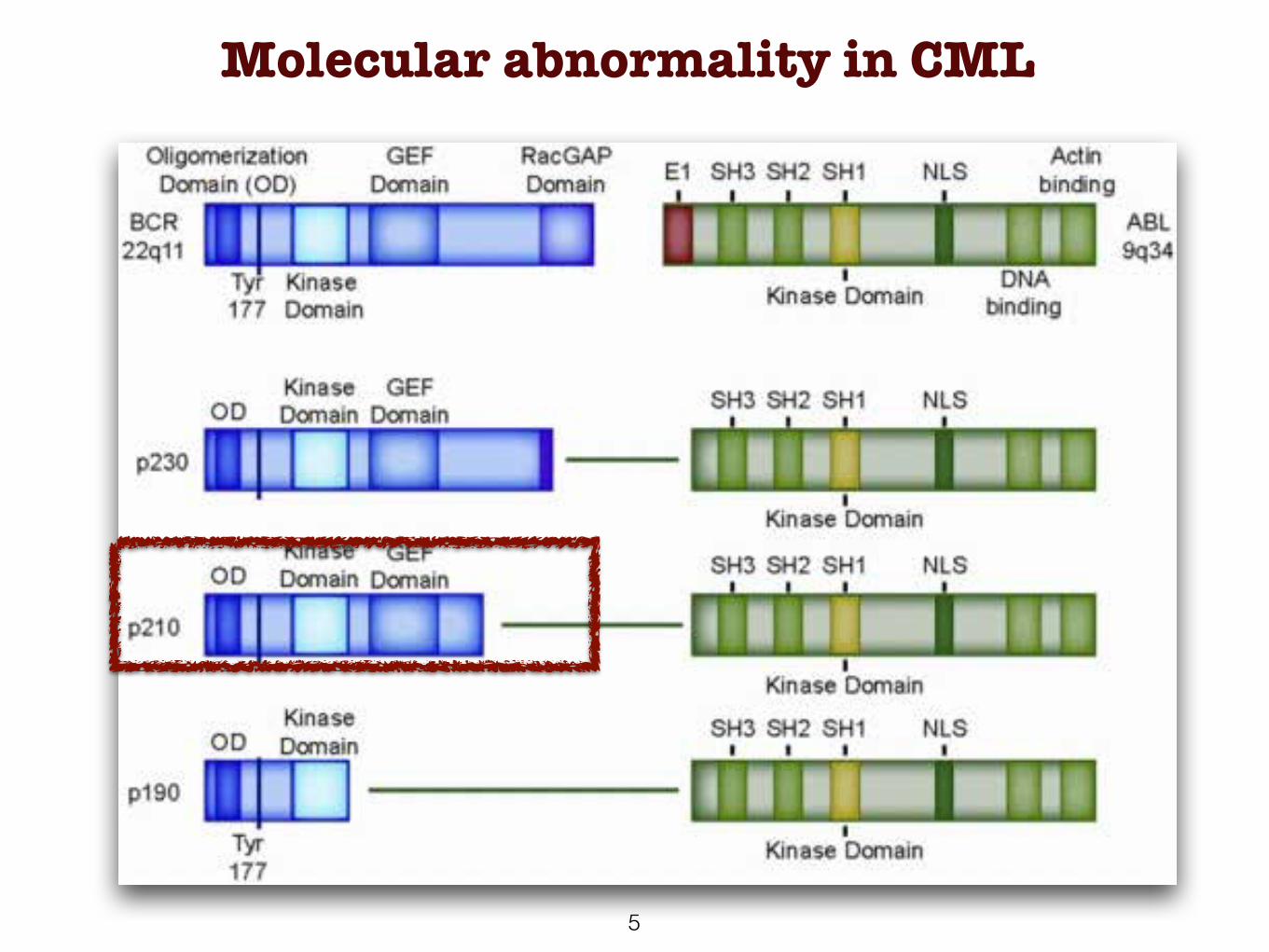
D. Risk stratification scores / prognostic indicators3, 18, 19
1. Sokal score – based on patient age, spleen size, platelet count and percentage of blasts in peripheral blood.
2. Hasford model – uses the same clinical variables as the Sokal score but also includes eosinophils and basophils in the peripheral blood.
3. Both scoring systems stratify patients into three risk groups (low, intermediate and high).
4. Used for risk stratification of patients in clinical trials.
E. Diagnosis of accelerated phase or blast crisis (see Table 1)
Table 1. Criteria for diagnosis of accelerated or blast crisis phase of CML.13
Patient Case #1, continued:
LP is examined by the hematologist and consents to a bone marrow biopsy. The biopsy is notable for marked hypercellularity. Cytogenetic analysis is positive for t(9;22), confirming the diagnosis of chronic phase CML. What is appropriate initial therapy for LP?
VIII. Treatment
A. Until the 1980s, CML was regarded as incurable and inevitably fatal.16
B. Historical treatment of CML9
1. Busulfan and hydroxyurea controlled hematologic symptoms, but did not alter the clinical course of the disease.
2. /ŶƚĞƌĨĞƌŽŶĂůĨĂ;/&EɲͿ improved overall survival compared to busulfan and hydroxyurea in a meta-analysis.
World Health Organization (WHO) Criteria
Accelerated Phase Blast Crisis
Blasts 10-19% of WBCs in peripheral and/or bone marrow
WĞƌŝƉŚĞƌĂůďůŽŽĚďĂƐŽƉŚŝůƐшϮϬй
Persistent thrombocytopenia (< 100,000 cells/mm3) unrelated to therapy
or persistent thrombocytosis (>1,000,000 cells/mm3) unresponsive to therapy
Increasing spleen size and increasing WBC
unresponsive to therapy
Cytogenetic evidence of clonal evolution – additional cytogenetic abnormalities (extra Ph, trisomy 8, trisomy
19 and/or isochromosome 17)
ůĂƐƚƐшϮϬйŽĨƉĞƌŝƉŚĞƌĂůǁŚŝƚĞblood cells or of bone
marrow cells
Extramedullary blast proliferation
Large foci or clusters of blasts in the bone marrow biopsy
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
9
Risk stratifications
NCCN Guidelines Version 4.2018Chronic Myeloid Leukemia
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
Version 4.2018, 01/24/18 © National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.CML-A
1Sokal J, Cox E, Baccarani M, et al. Prognostic discrimination in "good-risk" chronic granulocytic leukemia. Blood 1984;63:789-799. Available at: http://www.ncbi.nlm.nih.gov/pubmed/6584184.
2Hasford J, Pfirrmann M, Hehlmann R, et al. A new prognostic score for survival of patients with chronic myeloid leukemia treated with interferon alfa. Writing Committee for the Collaborative CML Prognostic Factors Project Group. J Natl Cancer Inst 1998;90:850-858. Available at: http://www.ncbi.nlm.nih.gov/pubmed/9625174.
RISK CALCULATION TABLE
Study Calculation 5LVN'H¿QLWLRQE\&DOFXODWLRQ
Sokal et al, 19841 Exp 0.0116 x (age in years - 43.4) + (spleen - 7.51) + 0.188 x >SODWHOHWFRXQW÷ 700)2@[EODVWFHOOV
Hasford et al, 19982 0.666 when age 50 years + (0.042 x spleen) + 1.0956 when platelet count > 1500 x 109/L + (0.0584 x blast cells) + 0.20399 when basophils > 3% + (0.0413 x eosinophils) x 100
Low <0.8Intermediate 0.8 - 1.2High >1.2
Low 780Intermediate 781 - 1480High >1480
Calculation of relative risk found at http://www.icsg.unibo.it/rrcalc.asp. Age is in years. Spleen is in centimeter below the costal margin (maximum distance). Blast cells, eosinophils, and basophils are in percents of peripheral blood differential. All factors must be collected prior to any treatment.
Reprinted with permission. © 2009 American Society of Clinical Oncology. All Rights Reserved. Baccarani M, Cortes J, Pane F, Niederwieser D, et al. European LeukemiaNet. Chronic myeloid leukemia: an update of concepts and management recommendations of European LeukemiaNet. J Clin Oncol 2009;27(35):6041-6051.
Printed by warunsuda sripakdee on 3/4/2018 10:32:24 PM. For personal use only. Not approved for distribution. Copyright © 2018 National Comprehensive Cancer Network, Inc., All Rights Reserved.
clinical trial & initial treatment selection
10
Treatment of CML
tyrosine kinase inhibitors (TKIs): 10 yrs OS 80-90%
dasatinib, nilotinib, bosutinib, and ponatinib
others agent : omacetaxine
goals of treatment
CP-CML: prevent progression to AP or BP
AP-CML : induce second chronic phase
BP-CML : induce second chronic phase
!
!

11
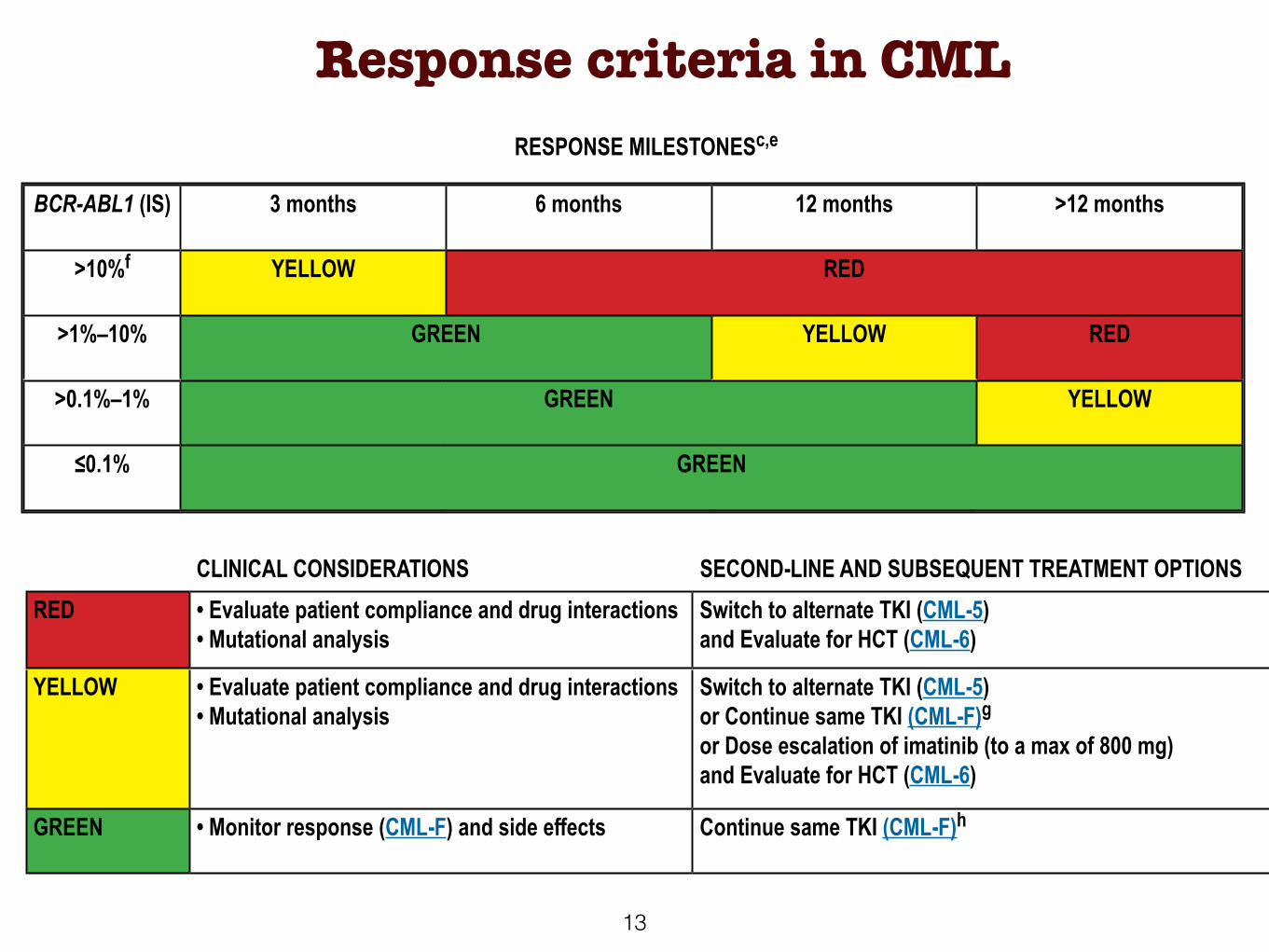
Response criteria in CML
a. Further improvements in survival were seen when IFN was combined with cytarabine.
b. Benefits were tempered by significant adverse effects, including flu-like symptoms, fevers, myalgias, fatigue, depression and immune-mediated complications.
C. The introduction of tyrosine kinase inhibitors (TKIs) revolutionized the management of CML, improving the 10-year overall survival from ~20% to 80-90%. In some patients, expected survival is indistinguishable from that of the general population.7, 9, 20, 21
1. Currently available therapies for CML include the TKIs imatinib, dasatinib, nilotinib, bosutinib, and ponatinib and the agent omacetaxine.
D. Current goals of treatment3, 22
1. Chronic phase
a. Maintain hematologic, cytogenetic and molecular remission
b. Prevent progression to accelerated phase or blast crisis
c. Minimize toxicity
2. Accelerated phase
a. Induce second chronic phase
3. Blast crisis
a. Induce second chronic phase
E. Three types of response: hematologic, cytogenetic and molecular.1, 3, 13, 20, 23-28
Table 2. Response criteria in CML. 1, 24, 25, 28, 29
QPCR (IS) = quantitative real-time polymerase chain reaction using International Scale; Ph+ = Philadelphia chromosome positive.
1. Most patients receiving current therapy will achieve a CHR at 3 months and CCyR at 6, 12 or 18 months. Patients who do not achieve a CHR by 3 months should be considered for a change in therapy.
Type of Response Criteria
Hematologic
Complete (CHR): x Normal peripheral blood count x WBC < 10,000 cells/ mm3 x Platelets < 450,000 cells/mm3 x No immature cells in the peripheral blood x No signs or symptoms of disease
Cytogenetic
Complete (CCyR): 0% Ph+ metaphases Partial (PCyR): 1-35% Ph+ metaphases Major (MCyR): 0 -35% Ph+ metaphases (complete + partial responses) Minor: >35% Ph+ metaphases
Molecular Complete (CMR): no detectable BCR-ABL mRNA by QPCR (IS) Major (MMR): Cytogenetic remission with 3 log or greater reduction in BCR-ABL transcripts by QPCR (IS)
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
“goal standard”- CCyR at 12 month; improved survival
now- MMR is early goal for CML
≥ 4.5 log reduction of BCR-ABL - outcome predictor
!

12
Response criteria in CML
Time Optimal response Warning Failure
Baseline High riskMajor route CCA/Ph+
3 mos. BCR-ABLIS ≤10%*Ph+ ≤35% (PCyR)
BCR-ABLIS >10%*Ph+ 36-95%
No CHR*Ph+ >95%
6 mos. BCR-ABLIS <1%*Ph+ 0% (CCyR)
BCR-ABLIS 1-10%*Ph+ 1-35%
BCR-ABLIS >10%*Ph+ >35%
12 mos. BCR-ABLIS ≤0.1%* (MMR) BCR-ABLIS 0.1-1%* BCR-ABLIS >1%* Ph+ >0%
Then,and at any time
MMR or better CCA/Ph- (-7, or 7q-) Loss of CHRLoss of CCyRLoss of MMR, confirmed**MutationsCCA/Ph+
UPDATE
2013
European LeukemiaNet Recommendations forthe Management of Chronic Myeloid Leukemia (CML)
Response definitions for any TKI first line,and 2nd line in case of intolerance, all patients (CP, AP, and BC)
*and/or **in 2 consecutive tests, of which one ≥1% IS: BCR-ABL on International Scale
Treatment recommendationsLine Event TKI, standard dosage1 Transplantation
Chronic phase
Imat
inib
400
mg/
qd
Nilo
tini
b 30
0 m
g/bi
d
Das
atin
ib 1
00 m
g/qd
Bosu
tini
b 50
0 m
g/qd
Pona
tini
b 45
mg/
qd
Search for alloSCT
Chem
othe
rapy
HLA
type
+ s
ibs
unre
late
d do
nor
cons
ider
reco
mm
ende
d
1st Baseline X X X X2
2nd Intolerance to 1st TKI Any other TKI approved 1st line
Failure 1st line of
imatinib X8 X X X X
nilotinib X X X X X X
dasatinib X8 X X X X X
3rd Intolerance to / failure of two TKI Any remaining TKI X
Any T315I mutation X X X X
Accelerated or blast phase
In newly diagnosed,TKI naïve patients
start with X3 X4 X X
no optimal response, BP X7 X5
TKI pre-treated patients Any other TKI X6 X7 X5
1choice of the TKI consider tolerability and safety, and patient characteristics (age, comorbidities), 2only in case of baseline war-nings (high risk, major route CCA/Ph+), 3400 mg/bid, 470 mg/bid or 140 mg/qd, 5may be required before SCT to control disease and to make patients eligible to alloSCT, 6in case of T315I mutation, 7only patients who are eligible for alloSCT, not in case of uncontrolled, resistant BP, 8400 mg bid in failure setting qd: Once daily bid: Twice dailyReferences: 1. Baccarani M, Deininger M, Rosti G, et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 122:872-884, 2013. 2. Baccarani M, Cortes J, Pane F, et al. Chronic myeloid leukemia. An update of concepts and management Recom-mendations of the European LeukemiaNet. J Clin Oncol. 27:6041-51, 2009. 3. Baccarani M, Sagio G, Goldman J, et al: Evolving concepts in the ma-nagement of chronic myeloid leukemia: recommendations from an expert panel on behalf of the European LeukemiaNet. Blood 108:1809-1820, 2006.
13
Response criteria in CMLNCCN Guidelines Version 4.2018Chronic Myeloid Leukemia
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
Version 4.2018, 01/24/18 © National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.
BCR-ABL1 (IS) 3 months 6 months 12 months >12 months
>10%f YELLOW RED
>1%–10% GREEN YELLOW RED
>0.1%–1% GREEN YELLOW
0.1% GREEN
RED • Evaluate patient compliance and drug interactions• Mutational analysis
Switch to alternate TKI (CML-5) and Evaluate for HCT (CML-6)
YELLOW • Evaluate patient compliance and drug interactions• Mutational analysis
Switch to alternate TKI (CML-5) or Continue same TKI (CML-F)g
or Dose escalation of imatinib (to a max of 800 mg)and Evaluate for HCT (CML-6)
GREEN • Monitor response (CML-FDQGVLGHHႇHFWV Continue same TKI (CML-F)h
cSee Monitoring Response to TKI Therapy and Mutational Analysis (CML-C).eSee Criteria for Hematologic, Cytogenetic, and Molecular Response and Relapse (CML-D).fPatients with BCR-ABL1 only slightly >10% at 3 months and/or with a steep decline from baseline, may achieve <10% at 6 months and have generally favorable
outcomes. Therefore, it is important to interpret the value at 3 months in this context, before making drastic changes to the treatment strategy.gAchievement of response milestones must be interpreted within the clinical context. Patients with more than 50% reduction compared to baseline or minimally above WKHFXWRႇFDQFRQWLQXHWKHVDPHGRVHRIGDVDWLQLEQLORWLQLERUERVXWLQLEIRUDQRWKHUPRQWKV
hDiscontinuation of TKI with careful monitoring is feasible in selected patients. See Discontinuation of TKI Therapy (CML-E).
CML-3
RESPONSE MILESTONESc,e
CLINICAL CONSIDERATIONS SECOND-LINE AND SUBSEQUENT TREATMENT OPTIONS
Printed by warunsuda sripakdee on 3/4/2018 10:31:56 PM. For personal use only. Not approved for distribution. Copyright © 2018 National Comprehensive Cancer Network, Inc., All Rights Reserved.

14
First line therapy for chronic phase CML

15
First line therapyImatinib:
irreversible TKI,bind to the inactive / closed conformation of ABL enzyme , c-kit, PDGFR
Results of the IRIS trial
2. The “gold standard” is considered the achievement of CCyR within 12 months, as it is associated with improved survival.
3. MMR is now emerging as a possible early therapeutic goal in CML therapy.
4. Emerging data suggests that deep molecular response (reduction of residual BCR->шϰϱůŽŐƐcompared to the standard baseline in two consecutive analyses, or “MR4.5”) may be a predictor of long-term outcome.
IX. First line therapy
A. Imatinib (Gleevec®, Glivec®)3, 7, 9, 24, 28-40
1. First-generation tyrosine kinase inhibitor.
2. Selective inhibitor of BCR-ABL tyrosine kinase.
a. Binds to the adenosine triphosphate (ATP) binding site of the ABL enzyme in the inactive / closed conformation.
b. Also inhibits c-kit and platelet-derived growth factor receptor (PDGFR)
3. Prevents phosphorylation of a critical residue necessary for substrate binding and kinase activity. Ultimately inhibits downstream signaling and results in apoptosis of malignant cells.
4. Initially studied as second-line therapy in CP-CML patients who had failed IFN.
5. Newly diagnosed patients were evaluated in the International Study of Interferon and STI571 (“IRIS”) trial.
a. 1106 patients with CP-CML were randomized to imatinib or IFN + low-dose cytarabine. Crossover was allowed for treatment failure or intolerance.
b. Long-term follow-up data on this trial is now available.
c. Results of the IRIS trial and other similar trials demonstrate that continuous treatment with imatinib induces high, durable responses with a decreasing rate of relapse in a large proportion of patients with CP-CML (see table 3).
1) Due to extremely high rate of crossover to imatinib arm, survival benefit could not be demonstrated in the IRIS trial.
2) Other smaller studies have demonstrated a survival benefit compared to IFN-based regimens.
Table 3. Results of the IRIS trial and subsequent follow-up studies.24, 31, 34
Selected Results of the IRIS Trial and Follow-up Studies Endpoint Imatinib IFN + Cytarabine P value
FFP at 18 months 96.7% 91.5% < 0.001 MCyR at 18 months 87.1% 34.7% < 0.001 CCyR at 18 months 76.2% 14.5% < 0.001 CCyR at 5 years 87% --- NR OS at 5 years 89% --- NR EFS at 8 years 81% --- NR FFP at 8 years 92% --- NR CCyR = complete cytogenetic response; EFS = event-free survival; FFP = freedom from progression to accelerated phase or blast crisis; IFN = interferon; MCyR = major cytogenetic response; NR = not reported; OS = overall survival.
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
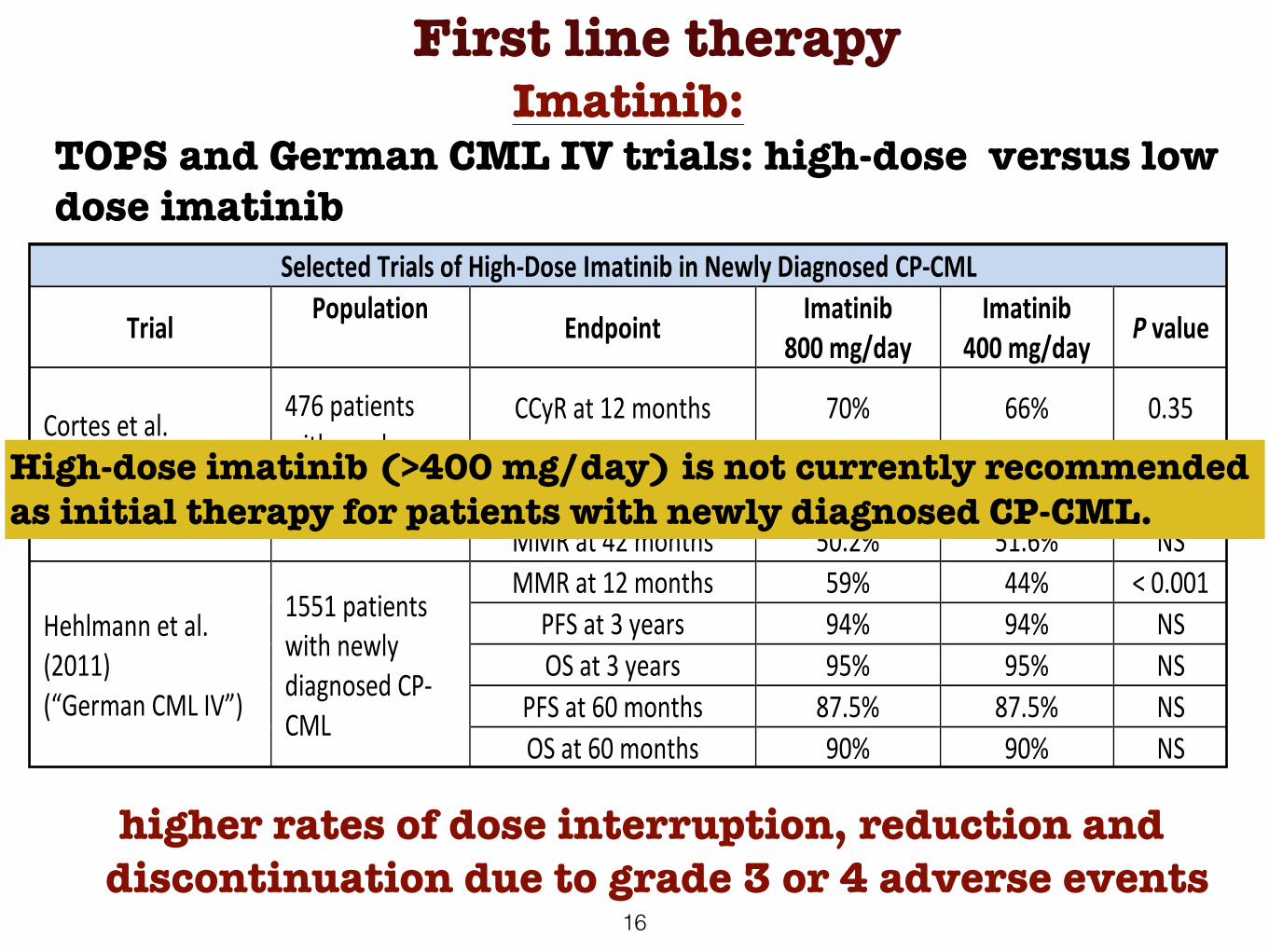
6. High-dose imatinib (>400 mg/day) is not currently recommended as initial therapy for patients with newly diagnosed CP-CML.
a. Although deeper and faster responses are achieved in newly diagnosed patients receiving high-dose imatinib compared to standard imatinib, these responses were not different from standard dose responses at 12 months. Likewise, these early responses do not appear to translate into an overall survival advantage (see Table 4).
1) The Tyrosine Kinase Inhibitor Optimization and Selectivity study (“TOPS”) was a phase III, randomized trial comparing the efficacy of higher-dose imatinib and standard dose imatinib in newly diagnosed CP-CML.
2) The German CML IV study compared imatinib 800 mg/day to imatinib 400 mg/day with or without interferon in newly diagnosed CP-CML patients.
Table 4. Results of selected trials of high-dose imatinib in the first-line setting.27, 35, 41
Selected Trials of High-Dose Imatinib in Newly Diagnosed CP-CML
Trial Population Endpoint Imatinib 800 mg/day
Imatinib 400 mg/day P value
Cortes et al. (2010) (“TOPS”)
476 patients with newly diagnosed CP-CML
CCyR at 12 months 70% 66% 0.35
MMR at 12 months 46% 40% 0.20
MMR at 42 months 50.2% 51.6% NS
Hehlmann et al. (2011) (“German CML IV”)
1551 patients with newly diagnosed CP-CML
MMR at 12 months 59% 44% < 0.001 PFS at 3 years 94% 94% NS OS at 3 years 95% 95% NS
PFS at 60 months 87.5% 87.5% NS OS at 60 months 90% 90% NS
CCyR = complete cytogenetic response; CP-CML = chronic phase chronic myelogenous leukemia; MMR = major molecular response; NS = not significant; OS = overall survival; PFS = progression-free survival.
b. High-dose imatinib is associated with higher rates of dose interruption, reduction and discontinuation due to grade 3 or 4 adverse events in a substantial number of patients.
c. The front-line use of high-dose imatinib may be an option for patients with high-risk disease who do not have access to other TKIs.
7. Therapeutic drug monitoring (TDM) of imatinib plasma trough concentrations may be useful in determining adherence to therapy, but is not routinely recommended at this time.
a. The clinical value of such monitoring has yet to be defined.
b. At present, there is no data to support that change of therapy based on plasma imatinib levels will affect treatment outcomes.
B. Dasatinib (Sprycel®)3, 7, 9, 30, 42-45
1. Second-generation tyrosine kinase inhibitor.
2. Dual inhibitor of ABL and the Src family of kinases. Also inhibits c-kit and PDGFR.
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
16
First line therapy
TOPS and German CML IV trials: high-dose versus low dose imatinib
Imatinib:
High-dose imatinib (>400 mg/day) is not currently recommended as initial therapy for patients with newly diagnosed CP-CML.
higher rates of dose interruption, reduction and discontinuation due to grade 3 or 4 adverse events
17
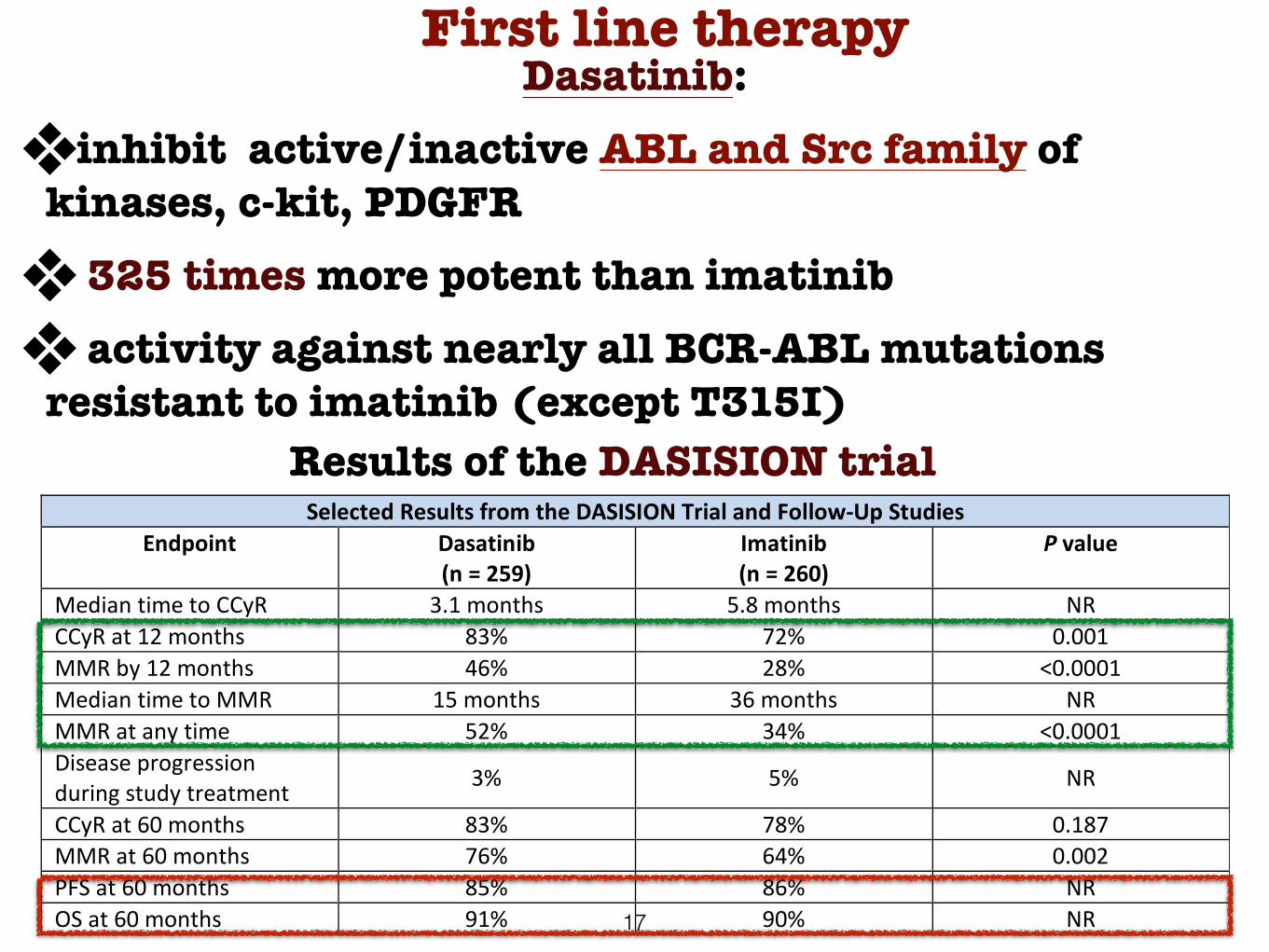
First line therapyDasatinib:
inhibit active/inactive ABL and Src family of kinases, c-kit, PDGFR
325 times more potent than imatinib activity against nearly all BCR-ABL mutations
resistant to imatinib (except T315I) !
Results of the DASISION trial
3. Can bind to both the active / open and inactive / closed conformations of the ABL kinase domain.
a. Approximately 325 times more potent than imatinib in vivo.
b. Results in activity against nearly all BCR-ABL mutations resistant to imatinib (except T315I).
4. Studied as first-line therapy in CP-CML patients in the Dasatinib vs Imatinib in Newly Diagnosed
Chronic Phase CML (“DASISION”) trial.
a. 519 patients with newly diagnosed CP-CML were randomized to imatinib or dasatinib.
b. Long-term follow-up data confirmed that dasatinib induces faster and deeper cytogenetic and
molecular responses, with fewer progressions to AP-CML or BC-CML than imatinib in this patient
population.
c. However, the 3-year overall survival did not differ between groups.
5. Additional trials have supported the findings of the DASISION trial (see Table 5).
Table 5. Results of the DASISION trial and subsequent follow-up studies.7, 42, 43, 45-48
Selected Results from the DASISION Trial and Follow-Up Studies Endpoint Dasatinib
(n = 259) Imatinib (n = 260)
P value
Median time to CCyR 3.1 months 5.8 months NR
CCyR at 12 months 83% 72% 0.001
MMR by 12 months 46% 28% <0.0001
Median time to MMR 15 months 36 months NR
MMR at any time 52% 34% <0.0001
Disease progression
during study treatment 3% 5% NR
CCyR at 60 months 83% 78% 0.187
MMR at 60 months 76% 64% 0.002
PFS at 60 months 85% 86% NR
OS at 60 months 91% 90% NR
CCyR = complete cytogenetic response; MMR = major molecular response; NR = not reported; PFS = progression-
free survival; OS = overall survival; NR = not reported.
C. Nilotinib (Tasigna®)3, 7, 9, 30, 49-51
1. Second-generation tyrosine kinase inhibitor.
2. Highly selective inhibitor of BCR-ABL tyrosine kinase.
a. Also inhibits c-kit and PDGFR.
3. Binds to the inactive / closed conformation of the BCR-ABL tyrosine kinase, but exhibits a higher
affinity to this kinase and a better topographic fit to the ATP binding site than imatinib.
a. Approximately 30 times more potent than imatinib in vivo.
4. Studied as first-line therapy in CP-CML patients in the Evaluating Nilotinib Efficacy and Safety in
Clinical Trials – Newly Diagnosed Patients (“ENESTnd”) trial.
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG

18
First line therapyNilotinib
inhibit inactive/closed ABL, c-kit, PDGFR better topographic fit to the ATP binding site than
imatinib 30 times more potent than imatinib
Results of the ENESTnd trial
a. Randomized 846 CP-CML patients to imatinib or nilotinib.
b. Long-term follow-up data confirmed that nilotinib induces superior molecular responses, with fewer progressions to AP-CML or BC-CML in this patient population.
c. Primary endpoints did not include overall survival. After three years of follow-up, overall survival did not differ significantly between treatment groups.
5. Additional trials have supported the findings of the ENESTnd trial (see Table 6).
Table 6. Results of the ENESTnd trial and subsequent follow-up studies.7, 49-53
Selected Results from the ENESTnd Trial
Endpoint Nilotinib
300 mg BID (n = 282)
Nilotinib 400 mg BID
(n = 281)
Imatinib 400 mg daily
(n = 283)
CCyR by 12 months 80% (p < 0.001)
78% (p < 0.001) 65%
MMR by 12 months 44% (p < 0.001)
43% (p < 0.001) 22%
CCyR by 24 months 87% (p = 0.0018)
85% (p = 0.016) 77%
MMR by 24 months 71% (p < 0.0001)
67% (p < 0.0001) 44%
Disease progression by 24 months
< 0.7% (p = 0.0059)
< 1.9% (p = 0.0196) 4.8%
Treatment failure at 12 months
3% (p = NR)
2% (p = NR) 8%
PFS at 48 months 96.7% (p = NR)
97.8% (p = NR) 93.1%
OS at 48 months 92.7% (p = NR)
96.7% (p = NR) 93.3%
MMR at 60 months 77% (p < 0.001)
77% (p < 0.001) 60%
Still on initial treatment at 60 months
60% (p = NR)
62% (p = NR) 50%
CCyR = complete cytogenetic response; MMR = major molecular response; NR = not reported; PFS = progression-free survival; OS = overall survival.
D. Initial selection of TKI3, 9, 20, 21, 27-29, 38, 46, 54-61
1. Current guidelines support imatinib, dasatinib or nilotinib as reasonable first-line choices for CP-CML.
a. Data from randomized trials demonstrate that dasatinib and nilotinib are associated with superior cytogenetic and molecular response rates at certain time points, as well as lower rates of disease progression when compared to imatinib.
b. Neither dasatinib nor nilotinib has shown improved overall survival or progression-free survival rates compared to imatinib.
1) The lack of significant differences in OS in this setting may be related to the toxicities of each agent.
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
19
Initial selection of TKI
low-risk disease: imatinib, nilotinib, dasainib (category 1)
high-risk disease : nilotinib, dasatinib (categoy 1)
dasatinib and nilotinib -superior CCyR and MMR at lower rates of PD when compared to imatinib
Neither dasatinib nor nilotinib - improved OS or PFS compared to imatinib.
the DASISION and ENESTnd - intermediate- and high- risk patients may preferentially benefit from dasatinib or nilotinib
20
Initial selection of TKI
NCCN Guidelines Version 4.2018Chronic Myeloid Leukemia
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
Version 4.2018, 01/24/18 © National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.CML-2
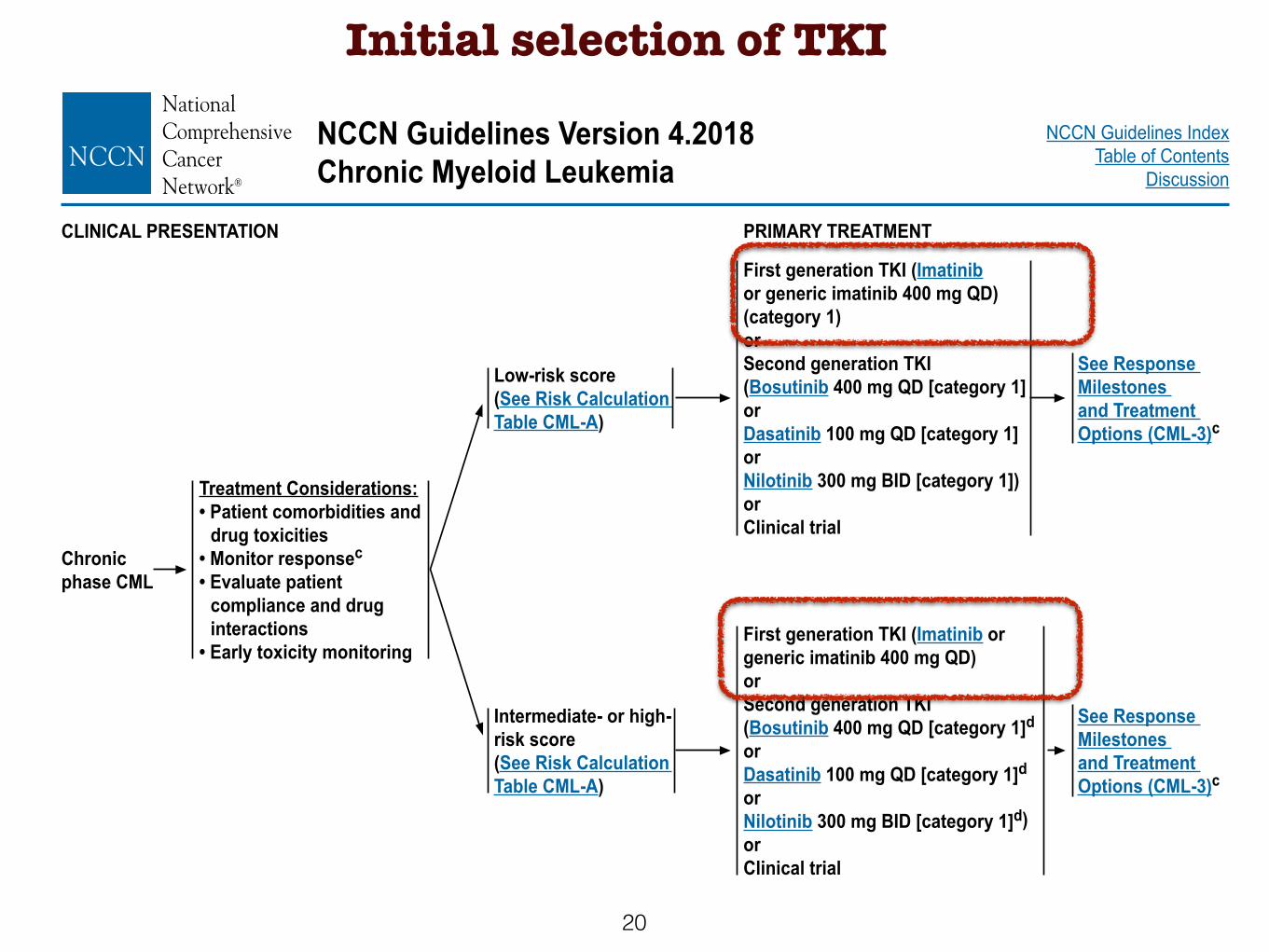
PRIMARY TREATMENT
First generation TKI (Imatinib or generic imatinib 400 mg QD) (category 1)orSecond generation TKI (Bosutinib PJ4'>FDWHJRU\@orDasatinibPJ4'>FDWHJRU\@or NilotinibPJ%,'>FDWHJRU\@orClinical trial
See Response Milestones and Treatment Options (CML-3)c
Chronic phase CML
cSee Monitoring Response to TKI Therapy and Mutational Analysis (CML-C).dLong-term follow-up data from the DASISION and ENESTnd trials and preliminary data from the BFORE trial suggest that patients with an intermediate- or high-risk Sokal or Hasford score may preferentially benefit from second generation TKI (dasatinib, nilotinib, or bosutinib). See Discussion for additional information.
Low-risk score (See Risk Calculation Table CML-A)
Intermediate- or high-risk score (See Risk Calculation Table CML-A)
Treatment Considerations:• Patient comorbidities and
drug toxicities• Monitor responsec
• Evaluate patient compliance and drug interactions
• Early toxicity monitoringFirst generation TKI (Imatinib or generic imatinib 400 mg QD)orSecond generation TKI (Bosutinib PJ4'>FDWHJRU\@d or Dasatinib 100 mg QD >FDWHJRU\@dor Nilotinib 300 mg BID >FDWHJRU\@d)orClinical trial
CLINICAL PRESENTATION
See Response Milestones and Treatment Options (CML-3)c
Printed by warunsuda sripakdee on 3/4/2018 10:32:24 PM. For personal use only. Not approved for distribution. Copyright © 2018 National Comprehensive Cancer Network, Inc., All Rights Reserved.

21
Initial selection of TKI
Choice of first-line therapy should be individualized.
a.Potential toxicity profiles
b.Patient’s age and ability to tolerate therapy
c.Presence of comorbid conditions
d.Patient’s risk score
e.Physician experience

22
Responding patients should continue therapy indefinitely. STIM & TWISTER trials
STIM TWISTER EURO-SKI 100 patients with CP-
CML who had CMR for > 2 yrs . 61% of patients
relapsed after stop imatinib 95% of relapses
occurring within 7 months of stopping imatinib low-risk Sokol score
and duration of imatinib therapy >54 months -continued response after imatinib cessation
!
40 patients with CP-CML who had been in CMR for 2 or more years TFR at 2 years was
45% High Sokal score and
shorter duration of interferon treatment - increased risk of relapse
!!
200 patients with CP-CML who had been in long term MR 70% TFR
Discontinuation of TKI

23
Discontinuation of TKI ALL of the following criteria are met:
1) Consultation with a CML Specialty Center 2) Age ≥ 18 years 3) no history of accelerated phase or blast crisis 4) On TKI therapy ≥ 3 years 5) Prior evidence of detectable disease via BCR-ABL1 transcript
6) Stable molecular response (MR4) for ≥ 2 years (at least 4 tests performed at least 3 months apart)
7) No history of resistance to any TKI 8) Access to reliable response monitoring 9) Monthly molecular monitoring for the first 6 months following
discontinuation, bimonthly during months 7-24, and quarterly thereafter if still in MMR
10) Prompt resumption of TKI in patients with loss of MMR

24
Second line therapy
25
Second line therapy
the selection of an alternative TKI is based on
prior therapy
concurrent disease states
mutational testing

26
Second line therapy
2nd lind Tx: dasatinib, nilotinib or bosutinib
1st line imatinib
yes
other TKIs
no
other TKIs except imatinib

27
Second line therapy
NCCN Guidelines Version 4.2018Chronic Myeloid Leukemia
NCCN Guidelines IndexTable of Contents
Discussion
Note: All recommendations are category 2A unless otherwise indicated.Clinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
Version 4.2018, 01/24/18 © National Comprehensive Cancer Network, Inc. 2018, All rights reserved. The NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN®.CML-5
TREATMENT OPTIONS BASED ON BCR-ABL1 MUTATION PROFILE
jPatients with disease that is resistant to primary treatment with imatinib should be treated with bosutinib, dasatinib, or nilotinib in the second-line setting. Patients with disease that is resistant to primary treatment with bosutinib, dasatinib, or nilotinib could be treated with an alternate TKI (other than imatinib) in the second-line setting.
kPonatinib is a treatment option for patients with a T315I mutation or for patients for whom no other TKI is indicatedlOmacetaxine is a treatment option for patients with disease that is resistant and/or intolerant to 2 or more TKIs.
Mutation Treatment Recommendationj
Y253H, E255K/V, or F359V/C/I DasatinibF317L/V/I/C, T315A, or V299L NilotinibE255K/V, F317L/V/I/C, F359V/C/I, T315A, or Y253H BosutinibT315I Ponatinib,k Omacetaxine,l allogeneic HCT (CML-6), or clinical trial
Printed by warunsuda sripakdee on 3/4/2018 10:31:56 PM. For personal use only. Not approved for distribution. Copyright © 2018 National Comprehensive Cancer Network, Inc., All Rights Reserved.
TREATMENT OPTIONS BASED ON BCR-ABL1 MUTATION PROFILE

28
Predictive factors for achievement of a cytogenetic response to second-line TKI therapy
1. Low Sokal score at diagnosis
2. Best cytogenetic response on imatinib
3. Neutropenia at any time during imatinib therapy requiring dose
reduction despite growth factor support
4. Time from detection of imatinib failure to start of second-line
TKI

29
Second line therapy
Bosutinib :
inhibit dual ABL/SRC family of kinases
minimal inhibit: c-kit, PDGFR, Src, Lyn and Hck kinases
!
against many BCR-ABL kinase domain mutations that are
resistant to imatinib, dasatinib and nilotinib (except T315I
and V299) !
200 times more potent than imatinib

30
Second line therapy: Bosutinib
which was the key secondary end point of the study. MMR is consid-ered to represent approximately a 1-log deeper response than CCyRwith respect to Bcr-Abl transcript levels and has been shown to predictlonger duration of CCyR.21,22 The times to CCyR and MMR wereshorter with bosutinib, which supports a more rapid debulking oftumor burden with bosutinib compared with standard-dose imatinib.Additionally, patients receiving bosutinib had a lower rate of diseaseprogression/lack of efficacy (3%) compared with patients receivingimatinib (10%), including a trend toward fewer transformations toAP/BP CML (2% v 4%, respectively). Together, these results indicatethat bosutinib may be effective in some patients with newly diagnosedCP CML, even though the primary efficacy end point was not met.Continued follow-up will allow for long-term evaluation of bosutinibefficacy in this population.
There have also been two recent studies with the second-generation TKIs dasatinib and nilotinib versus imatinib in patientswith CP CML in the first-line setting.5,6 Allowing for differences instudy design, patient population, and the inherent difficulties of com-
paring data across multiple studies, rates of CCyR by 12 months weresimilar among all three studies (bosutinib, 79%; dasatinib, 83%; nilo-tinib, 78% to 80%), although the rate achieved with imatinib wasslightly higher in the current study (75%) than in the dasatinib andnilotinib studies (72% and 65%, respectively),5,6 possibly because ofdifferences in ITT population definitions and Sokal and Hasford riskgroups across studies. The MMR rate at 12 months was higher in boththe bosutinib versus imatinib and nilotinib versus imatinib studies(bosutinib, 41%; nilotinib, 43% to 44%; imatinib, 27% and 22%,respectively),6 and the rate of MMR by 12 months was also higher withbosutinib and dasatinib across studies (bosutinib, 47%; dasatinib,46%; imatinib, 32% and 28%, respectively).5 In addition, all threesecond-generation TKIs were associated with faster achievement ofCCyR and MMR compared with imatinib.5,6 Similar rates of transfor-mation to AP/BP CML were observed in all three studies (bosutinib,2%; dasatinib, 2%; nilotinib, 1%; imatinib, 4%, 3%, and 4%).5,6
Overall,bosutinibwasassociatedwithatoxicityprofiledistinct fromthatof imatinib.However,anunexpectedlyhighnumberofpatients(n!48,19%)werediscontinuedfrombosutinibtreatmentasaresultofanAE,including 15 (31%) of 48 patients who discontinued before their firstpostbaseline assessment. These data require confirmation in future stud-ies. Thus, early discontinuations as a result of toxicity may have contrib-uted to the lower rate of CCyR associated with bosutinib in the ITTpopulation, which included these patients as nonresponders.
Although bosutinib therapy was associated with greater rates ofdiarrhea, vomiting, and aminotransferase elevations compared withimatinib, most instances were transient and, in the case of diarrhea,frequently self-limiting after the first 2 to 3 months of therapy. Fluidretention, which has commonly been observed with dasatinib5,17,23-28
and imatinib,5,6,27,29 occurred infrequently with bosutinib. Despitethe occurrence of liver function test abnormalities with bosutinibtreatment, no cases were associated with permanent liver injury. Lowrates of grade 3 or 4 (all causality) anemia (6%), neutropenia (11%),and thrombocytopenia (14%) were reported with bosutinib. Theminimal inhibition of c-KIT by bosutinib may have contributed to thelow incidence of myelosuppressive events, particularly grade 3 or 4
BABosutinibImatinib
Com
plet
e Cy
toge
netic
Resp
onse
(%)
Time Since Treatment Initiation (months)
100
80
60
40
20
03 6 9 12
*
††
63
49
25
49
5954
70 68
BosutinibImatinib
Maj
or M
olec
ular
Resp
onse
(%)
Time Since Treatment Initiation (months)
100
80
60
40
20
03 6 9 12
†
**
35
11
37
27
19
41
27
*
Fig 2. Rates of (A) complete cytogenetic response and (B) major molecular response in the intent-to-treat population. Cytogenetic analysis determined the presence of Philadelphiachromosome in bone marrow aspirate and included fluorescence in situ hybridization imputation; at least 20 metaphases were required. Molecular analysis determined the numberof Bcr-Abl transcripts in peripheral blood. Patients who were not evaluable were counted as nonresponders. (*) Indicates a 2-sided P " .001. (†) Indicates a 2-sided P " .05. P valueswere based on the Cochran-Mantel-Haenszel test and stratified by site-entered Sokal score and geographic region; P values at all time points were considered exploratory, with theexception of month 12.
BosutinibImatinib
3
10
2
4
1
3
Patie
nts
(%)
12
10
8
6
4
2
0Disease
Progression/Lack of Efficacy*
Transformationto AP/BP
Death ResultingFrom CML
Progression
Fig 3. Rates of disease progression while on study treatment in the intent-to-treat population. (*) Includes transformation to accelerated phase (AP)/blastphase (BP) chronic myeloid leukemia (CML).
Cortes et al
3490 © 2012 by American Society of Clinical Oncology JOURNAL OF CLINICAL ONCOLOGY
Downloaded from ascopubs.org by Prince of Songkla University on March 3, 2017 from 202.012.073.133Copyright © 2017 American Society of Clinical Oncology. All rights reserved.
Bosutinib Versus Imatinib in Newly Diagnosed Chronic-Phase Chronic Myeloid Leukemia:
Results From the BELA Trial
The trial did not meet its primary endpoint of improved CCyR at 12 months.

31
not currently recommended in the first-line setting (prep course 2017)
Second line therapy: Bosutinib
The ASCO Post
6/3/61 09:14FDA Grants Accelerated Approval to Bosutinib for Treatment of Newly Diagnosed Philadelphia Chromosome–Positive CML - The ASCO Post
หนา 1 จาก 3http://www.ascopost.com/issues/december-25-2017/fda-grants-accel…eatment-of-newly-diagnosed-philadelphia-chromosome-positive-cml/
FDA Grants Accelerated Approval toBosutinib for Treatment of NewlyDiagnosed Philadelphia Chromosome–Positive CMLBy The ASCO PostDecember 25, 2017Tweet this page
On December 19, 2017, the U.S. Food and Drug Administration (FDA) granted accelerated approval tobosutinib (Bosulif) for treatment of patients with newly diagnosed chronic-phase Philadelphiachromosome–positive chronic myelogenous leukemia (CML).
Approval was based on data from an open-label, randomized, multicenter BFORE trial in 487 patients withPhiladelphia chromosome–positive newly diagnosed chronic phase CML who were randomized to receiveeither bosutinib at 400 mg once daily or imatinib (Gleevec) at 400 mg once daily. The major e!cacyoutcome measure was major molecular response (MMR) at 12 months, defined as ≤ 0.1% BCR-ABL ratio oninternational scale (corresponding to ≥ 3 log reduction from standardized baseline) with a minimum of3,000 ABL transcripts as assessed by the central laboratory.
MMR at 12 months was 47.2% (95% confidence interval [CI] = 40.9–53.4) in thebosutinib arm and 36.9% (95% CI = 30.8–43.0) in the imatinib arm (P = .0200).
The most common adverse reactions in patients with newly diagnosed CML (incidence≥ 20%) are diarrhea, nausea, thrombocytopenia, rash, increased alanineaminotransferase, abdominal pain, and increased aspartate aminotransferase.
Prior Approval
The FDA first approved bosutinib in 2012 for treatment of patients with chronic-,accelerated-, or blast-phase Philadelphia chromosome–positive CML with resistanceor intolerance to prior therapy.
The recommended dose of bosutinib for newly diagnosed chronic-phase Philadelphiachromosome–positive CML is 400 mg orally once daily with food.
For more information, visit FDA.gov.
Reference
1. Cortes JE, Gambacorti-Passerini C, Deininger MW, et al: Bosutinib versus imatinib for newly diagnosedchronic myeloid leukemia: Results from the randomized BFORE trial. J Clin Oncol. November 1, 2017 (earlyrelease online).
1
MAR06
ADVERTISEMENT
ADVERTISEMENT
TODAY IN ONCOLOGY
Dexamethasone-Sparing Antiemetic Regimen inPatients Receiving Highly EmetogenicChemotherapy
Internet-Delivered Cognitive-Behavioral Therapy forInsomnia in Breast Cancer Survivors
Cognitive Decline Prevalent Among Elderly PatientsWith Hematologic Cancers
Study Finds Colorectal Cancer Screenings VaryWidely Throughout the United States
Genomic Analyses Highlight Need for PrecisionTherapies That Target Pediatric Cancers
FDA Grants Fast Track Designation to Pamrevlumabin Locally Advanced Unresectable Pancreatic Cancer
Chemoradiotherapy vs Neoadjuvant Chemotherapyand Radical Surgery in Locally Advanced SquamousCervical Cancer
∠
"
#
$
ADVERTISEMENT
Results from the randomized
BFORE trial. J Clin Oncol.
November 1, 2017

32
Second line therapy: Bosutinib
© 2017 American Society of Health-System Pharmacists, Inc., and American College of Clinical Pharmacy All rights reserved 391
Table 6. Summary of trials of dasatinib in the second-line setting.71, 77-81
Selected Trials of Dasatinib in the Second-Line Setting Citation Population MCyR CCyR PFS
Hochhaus et al. (2007)
186 pts with imatinib-resistant or –intolerant CP-CML 52% 39% 92.4% at 8 mo
Hochhaus et al. (2008) “START-C”
387 pts with imatinib-resistant or –intolerant CP-CML 59% 49% 90% at 15 mo
80% at 24 mo
Kantarjian et al. (2009) “START-R”
150 pts with imatinib-resistant CP-CML 53% 44% 86% at 24 mo
Shah et al. (2010) (“CA180-034”)
670 pts with imatinib-resistant or –intolerant CP-CML 63% 50% 80% at 24 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; NR = not reported; PFS = progression-free survival.
Table 7. Summary of trials of nilotinib in the second-line setting.82-84 Selected Trials of Nilotinib in the Second-Line Setting
Citation Population MCyR CCyR PFS OS Kantarjian et al. (2011)
321 pts with imatinib-resistant or –intolerant CP-CML 59% 44% 64% at 24 mo 87% at 24 mo
Giles et al. 321 pts with imatinib-resistant or –intolerant CP-CML 59% 45% 57% at 48 mo 78% at 48 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; NR = not reported; OS, overall survival; PFS = progression-free survival.
Table 8. Summary of trials of bosutinib in the second-line setting.85
Selected Trials of Bosutinib in the Second-Line Setting Citation Population MCyR CCyR PFS OS
Cortes et al. (2011)
288 pts with imatinib-resistant or –intolerant CP-CML 53% 41% 79% at 24 mo 92% at 24 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; PFS = progression-free survival; OS = overall survival.
VI. Third line therapy and beyond6, 10, 60, 86-92
A. Second-generation TKIs show solid efficacy in patients who have imatinib resistance or intolerance. However, approximately half of the patients receiving these agents in the second-line setting also experience resistance or intolerance.
B. A third TKI (second-generation TKI only) may be considered in this setting. No TKI is specifically indicated for treatment failure of both first- and second-generation TKIs, with current literature restricted to observational studies or studies with small patient populations.
C. Allogeneic stem cell transplantation may be considered (see Hematopoietic Stem Cell Transplantation by Dr. Merten).

33
Dasatinib in imatinib-resistant or -intolerant chronic-phase,chronic myeloid leukemia patients: 7-year follow-up of studyCA180-034
Neil P. Shah,1* Philippe Rousselot,2 Charles Schiffer,3 Delphine Rea,4 Jorge E. Cortes,5 Jorge Milone,6 Hesham Mohamed,7
Diane Healey,7 Hagop Kantarjian,5 Andreas Hochhaus,8 and Giuseppe Saglio9
Dasatinib was approved at 100 mg once daily for imatinib-resistant or -intolerant patients with chronicmyeloid leukemia (CML) in chronic phase, based on results of the phase 3 CA180-034 (NCT00123474) study.Here we present the final 7-year analysis of this pivotal study, the longest follow-up to date of any second-generation BCR–ABL1 tyrosine kinase inhibitor (TKI). Patients (n 5 670) with imatinib-resistant or -intolerantCML in chronic phase received dasatinib. Nineteen percent of patients continued on study treatment, with agreater proportion in the 100 mg once daily arm remaining on therapy. Seven-year rates for major molecularresponse (MMR), progression-free survival (PFS), and overall survival (OS) were similar across doses; MMR,PFS, and OS results were 46, 42, and 65% at 100 mg once daily, respectively. Improved PFS and OS rateswere reported in patients who achieved BCR–ABL1 !10% at 3 and 6 months. No new safety signals wereidentified. The incidence of drug-related pleural effusion was 28% at 100 mg once daily and 35% at theother three dose groups. Incidence of drug-related pulmonary hypertension and pulmonary arterialhypertension remained low (!3% across all doses). Arterial ischemic events occurred in !4% of patientsacross all doses. These data support the long-term efficacy and well-established safety profile ofdasatinib for patients with imatinib-resistant or -intolerant CML in chronic phase.Am. J. Hematol. 91:869–874, 2016. VC 2016 The Authors. American Journal of Hematology Published by Wiley Periodicals, Inc.
! IntroductionThe introduction of BCR–ABL1 tyrosine kinase inhibitors (TKIs) for the treatment of chronic myeloid leukemia (CML) resulted in improved
patient prognosis, including greater survival rates, compared with the two previous standards of care [1–3]. Survival in CML patients is now nearlyidentical to that of the general population [4]. CML is currently considered a manageable chronic disease, requiring many patients to remain onTKI therapy indefinitely. Given the long-term nature of treatment for CML, monitoring patients as they continue therapy is valuable for under-standing the durability of responses, and for recognizing the emergence of new or previously unrecognized adverse events (AEs).
Dasatinib, a second-generation TKI active against ABL, PDGFRb, KIT, and SRC family kinases, is approved for the treatment of newly diag-nosed adults with Ph1 CML in chronic phase (CP); adults with Ph1 CML in chronic phase, accelerated phase (AP), or blast phase (BP) withresistance or intolerance to prior therapy including imatinib; and for adults with Ph1 acute lymphoblastic leukemia who have become resistant toor intolerant of other treatment [5]. Previous analysis from the initial report at 6-month follow-up for the phase 3 CA180-034 dose-optimizationstudy in imatinib-resistant or -intolerant CML-CP patients showed similar dasatinib efficacy with all dosing regimens evaluated; however, the100 mg once-daily (QD) dosing schedule showed improved tolerability with a reduced incidence of treatment-related AEs of interest (i.e., pleuraleffusion and cytopenia), leading to a label change as the recommended dasatinib dose regimen in this patient population [5,6]. Longer-term fol-low-up of patients in this trial at 6 years continued to demonstrate durable efficacy and safety with dasatinib at 100 mg QD [1]. Here, we report
Additional Supporting Information may be found in the online version of this article.1UCSF School of Medicine, San Francisco, California; 2Hopital Andr!e Mignot and Universit!e Versailles Saint-Quentin-en-Yvelines, Versailles, France; 3Wayne State Uni-versity School of Medicine, Detroit, Michigan; 4Saint Louis Hospital, Paris, France; 5University of Texas M.D. Anderson Cancer Center, Houston, Texas; 6Hospital Ital-iano De La Plata, La Plata, Argentina; 7Bristol-Myers Squibb, Princeton, New Jersey; 8Universit€atsklinikum Jena, Jena, Germany; 9University of Turin, Turin, Italy
This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs License, which permits use and distribution inany medium, provided the original work is properly cited, the use is non-commercial and no modifications or adaptations are made.Clinical trials identifier: NCT00123474Funding: Bristol-Myers Squibb sponsored this trial.Disclosure: NPS received research funding from Ariad, BMS, and Pfizer. PR acted as a consultant for and received research funding from BMS. CS receivedresearch funding from Ariad, BMS, and Novartis and participates in DSMBs for Teva and Pfizer. DR received honoraria from Ariad, BMS, Novartis, andPfizer. JEC acted as a consultant for and received research funding from Ariad, BMS, Novartis, and Pfizer, and received research funding from Teva. JM holdsmembership on the Boards of Directors or advisory committees and Speakers Bureaus for BMS and Roche. HM and DH are employees of BMS. HK receivedresearch funding from Amgen, Ariad, and Pfizer. AH received research funding from Ariad, BMS, MSD, Novartis, and Pfizer. GS acted as a consultant forand received speaking fees from BMS, and consulted for and received speaking fees from Ariad, Novartis, and Pfizer.*Correspondence to: Neil P. Shah; Division of Hematology-Oncology, UCSF, 505 Parnassus Avenue, Suite M1286, Box 1270, San Francisco, CA 94143. E-mail: [email protected] for publication: 5 May 2016; Revised: 10 May 2016; Accepted: 16 May 2016Am. J. Hematol. 91:869–874, 2016.Published online: 19 May 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24423
VC 2016 The Authors. American Journal of Hematology Published by Wiley Periodicals, Inc.
doi:10.1002/ajh.24423 American Journal of Hematology, Vol. 91, No. 9, September 2016 869
RESEARCH ARTICLE AJHAJHSecond line therapy: Dasatinib
the final 7-year analysis of efficacy and safety outcomes of CA180-034, which represents the longest follow-up to date in the second-lineof any second-generation BCR–ABL1 TKI.
! MethodsDetailed methods have been previously reported and are outlined in Supporting
Information Materials. CA180-034 (NCT00123474), a randomized phase 3 study, com-pared the dose and schedule of dasatinib therapy for optimal benefit/risk ratio amongpatients with imatinib-resistant or -intolerant CML-CP. The primary objective of thisstudy was to compare the major cytogenetic response (MCyR) rates of dasatinib after aminimum follow-up of 6 months when administered QD with dasatinib administeredtwice daily (BID). Secondary end points included other efficacy and safety assessments.
Patient eligibility criteria were previously described [6]. Patients were stratifiedby imatinib resistance or intolerance. The study was conducted in accordance withthe Declaration of Helsinki and was approved by local ethics committees. Writteninformed consent was obtained from each patient before participation.
Eligible patients were randomized 1:1:1:1 to receive dasatinib 100 mg QD,50 mg BID, 140 mg QD, or 70 mg BID. To manage inadequate responses or AEs,dose escalation (up to a total daily dose [TDD] of 180 mg) and dose interruptionor reduction (down to a TDD of 20 mg) were allowed. After 2 years, the protocolwas amended to allow switching from a BID to a QD regimen, at the same TDD, ifthe patient experienced a recurrence of anemia, thrombocytopenia, neutropenia,pleural effusion, or any other fluid retention during study progress following atleast one dose reduction, at the investigator’s discretion [1]. Treatment was admin-istered until protocol-defined disease progression or death, unacceptable toxicity, orpatient/investigator request.
Figure 1. Kaplan–Meier analyses. All subjects included in these analyses were randomized. Rates for PFS and OS at 7 years from randomization were com-parable across treatment arms. Panel A: progression-free survival (PFS), Panel B: overall survival (OS).
Shah et al. RESEARCH ARTICLE
870 American Journal of Hematology, Vol. 91, No. 9, September 2016 doi:10.1002/ajh.24423
the final 7-year analysis of efficacy and safety outcomes of CA180-034, which represents the longest follow-up to date in the second-lineof any second-generation BCR–ABL1 TKI.
! MethodsDetailed methods have been previously reported and are outlined in Supporting
Information Materials. CA180-034 (NCT00123474), a randomized phase 3 study, com-pared the dose and schedule of dasatinib therapy for optimal benefit/risk ratio amongpatients with imatinib-resistant or -intolerant CML-CP. The primary objective of thisstudy was to compare the major cytogenetic response (MCyR) rates of dasatinib after aminimum follow-up of 6 months when administered QD with dasatinib administeredtwice daily (BID). Secondary end points included other efficacy and safety assessments.
Patient eligibility criteria were previously described [6]. Patients were stratifiedby imatinib resistance or intolerance. The study was conducted in accordance withthe Declaration of Helsinki and was approved by local ethics committees. Writteninformed consent was obtained from each patient before participation.
Eligible patients were randomized 1:1:1:1 to receive dasatinib 100 mg QD,50 mg BID, 140 mg QD, or 70 mg BID. To manage inadequate responses or AEs,dose escalation (up to a total daily dose [TDD] of 180 mg) and dose interruptionor reduction (down to a TDD of 20 mg) were allowed. After 2 years, the protocolwas amended to allow switching from a BID to a QD regimen, at the same TDD, ifthe patient experienced a recurrence of anemia, thrombocytopenia, neutropenia,pleural effusion, or any other fluid retention during study progress following atleast one dose reduction, at the investigator’s discretion [1]. Treatment was admin-istered until protocol-defined disease progression or death, unacceptable toxicity, orpatient/investigator request.
Figure 1. Kaplan–Meier analyses. All subjects included in these analyses were randomized. Rates for PFS and OS at 7 years from randomization were com-parable across treatment arms. Panel A: progression-free survival (PFS), Panel B: overall survival (OS).
Shah et al. RESEARCH ARTICLE
870 American Journal of Hematology, Vol. 91, No. 9, September 2016 doi:10.1002/ajh.24423
the final 7-year analysis of efficacy and safety outcomes of CA180-034, which represents the longest follow-up to date in the second-lineof any second-generation BCR–ABL1 TKI.
! MethodsDetailed methods have been previously reported and are outlined in Supporting
Information Materials. CA180-034 (NCT00123474), a randomized phase 3 study, com-pared the dose and schedule of dasatinib therapy for optimal benefit/risk ratio amongpatients with imatinib-resistant or -intolerant CML-CP. The primary objective of thisstudy was to compare the major cytogenetic response (MCyR) rates of dasatinib after aminimum follow-up of 6 months when administered QD with dasatinib administeredtwice daily (BID). Secondary end points included other efficacy and safety assessments.
Patient eligibility criteria were previously described [6]. Patients were stratifiedby imatinib resistance or intolerance. The study was conducted in accordance withthe Declaration of Helsinki and was approved by local ethics committees. Writteninformed consent was obtained from each patient before participation.
Eligible patients were randomized 1:1:1:1 to receive dasatinib 100 mg QD,50 mg BID, 140 mg QD, or 70 mg BID. To manage inadequate responses or AEs,dose escalation (up to a total daily dose [TDD] of 180 mg) and dose interruptionor reduction (down to a TDD of 20 mg) were allowed. After 2 years, the protocolwas amended to allow switching from a BID to a QD regimen, at the same TDD, ifthe patient experienced a recurrence of anemia, thrombocytopenia, neutropenia,pleural effusion, or any other fluid retention during study progress following atleast one dose reduction, at the investigator’s discretion [1]. Treatment was admin-istered until protocol-defined disease progression or death, unacceptable toxicity, orpatient/investigator request.
Figure 1. Kaplan–Meier analyses. All subjects included in these analyses were randomized. Rates for PFS and OS at 7 years from randomization were com-parable across treatment arms. Panel A: progression-free survival (PFS), Panel B: overall survival (OS).
Shah et al. RESEARCH ARTICLE
870 American Journal of Hematology, Vol. 91, No. 9, September 2016 doi:10.1002/ajh.24423
Am. J. Hematol. 91:869–874, 2016. VC 2016

34
Second line therapy: Dasatinib
[grades 3/4], 28% [5%] vs. other treatment arms: any grade [grades 3/4],36% [9%]). No deaths due to pleural effusion events were reported. Inyear 7 of the study, new cases of pleural effusion (regardless of relation-ship to study therapy) occurred in 5% (2/42) of patients at risk treatedin the 100 mg QD arm compared with 8% (7/88) in the other treatmentarms. Half the pleural effusion events (23/46 cases; Table II) occurredwithin the first 2 years of treatment among patients in the 100 mg QDarm. Drug-related pleural effusion was reported at a rate of 28% in the100 mg QD arm vs. 35% in the other dose groups (Table II). Pleuraleffusion cases leading to treatment discontinuation were all considereddrug-related; 7% of patients with pleural effusion in the 100 mg QDarm discontinued therapy (2% grade 3/4) vs. 11% (3% grade 3/4) in theother dose groups.
Pulmonary hypertension (PH), or pulmonary arterial hypertension(PAH), were reported on the basis of diagnostic evaluations includingechocardiogram, chest X-ray, cardiac catheterization, and blood tests.PH of any grade was reported in 16 patients (2.4%) with seven (1.1%)experiencing a grade 3/4 event (100 mg QD: any grade [grades 3/4],three patients (1.8%) [two patients (1.2%)] vs. other treatment arms:any grade [grades 3/4], 3% [1%]). PAH confirmed by right-heart cathe-terization was reported in one patient in the 100 mg QD group (at75 months). Cumulative rates of PH and PAH over time are shown inTable II.
Incidence of arterial ischemic events (all grades) was low overall inthe study. Cardiovascular ischemic events (defined as myocardialinfarction, angina pectoris, or coronary artery disease) were reportedin 4% of patients in the 100 mg QD arm and 4% in the other dosegroups. The specific cardiac ischemic events reported in the 100 mgQD arm and the other dose groups were myocardial infarction (2 vs.1%, respectively), angina pectoris (1 vs. 2%, respectively), and coro-nary artery disease (1 vs. <1%, respectively). The majority of cardiacischemic events were grades 3/4 (2 vs. 2%, respectively); additionally,one patient (<1%) in the other dose groups experienced a fatal grade5 myocardial infarction. Peripheral vascular events (all grades) werereported in 1% of patients in the other dose groups (no events in the100 mg QD arm), with <1% reported as grades 3/4. Cerebrovascularevents (all grades) were reported in 3 and 1% of patients in the100 mg QD and other dose groups, respectively. In the 100 mg QDarm, 1% of cerebrovascular events were grades 3/4; all events in theother dose groups were grades 3/4. There were no reports of stroke.
Over the 7-year course of the study, 66% of all treated patientsexperienced infections (any cause, all grades); 67% of patients in the100 mg QD arm and 65% of patients in the other dose arms experi-enced infections (Supporting Information Table VI). In the 100 mgQD arm, 53% of patients had on-study worst grade 1/2 infections, and13% had worst grade events of 3 or 4; across the other arms, 49% ofpatients had on-study worst grade 1/2 infections and 15% had a worstgrade 3/4 infection. Among the two patients in the 100 mg QD armwho had an on-study worst grade infection of 5, one was a lung infec-tion and one was due to septic shock. In the other arms, three patientshad an on-study worst grade 5 infection, one from pneumonia, and
two from skin infections. The majority of infectious deaths occurredafter dasatinib treatment was discontinued (range, 1 day–16 months).Neutropenia was not associated with infections among patients whoreceived dasatinib. The majority of infections resolved.
! DiscussionAt 7 years of follow-up, this analysis of dasatinib treatment from
the CA180-034 dose optimization trial represents the longest follow-up of a second-generation BCR–ABL1 TKI in the second line. Con-sistent with previous reports, dasatinib treatment at a dose of 100 mgQD demonstrated durable efficacy and a tolerable long-term safetyprofile in imatinib-resistant and -intolerant CML-CP patients.
With the advent of BCR–ABL1 TKIs, CML is currently considered achronic condition, in which most patients are able to achieve long-term survival [1–3]. Initial and continuing monitoring of responses iscritical to ensure optimal management of CML, since early responsesare predictive of long-term outcomes [9–13]. Furthermore, promptidentification of patients who are resistant or intolerant to their first-line therapy is imperative, so that they may be switched early to asecond-line TKI and potentially improve long-term outcomes [12–14].
In this analysis, we report that 19% of extensively pretreated patientscontinued dasatinib on study for at least 7 years, with a greater propor-tion of patients in the 100 mg QD arm remaining on treatment(median duration, 37 months). Dasatinib at 100 mg QD was better tol-erated than other dosing regimens: more patients in this group main-tained their assigned dose (38%) compared with the other treatmentgroups (50 mg BID: 19%, 140 mg QD: 24%, and 70 mg BID: 9%).With a minimum follow-up of 7 years, treatment with dasatinib at100 mg QD continues to provide efficacy similar to the initiallyapproved dose of 70 mg BID, as evidenced by comparable rates ofMMR (46 and 46%, respectively), PFS (42 and 44%, respectively), andOS (65 and 68%, respectively). Deaths were most commonly disease-related.
According to current European LeukemiaNet (ELN) recommenda-tions, achievement of BCR–ABL1 (IS) !10% at 3 months definestreatment response, predictive of long-term benefit and outcomes forfirst-line therapy [9,15]. At 7 years, landmark analyses continue todemonstrate that achieving early responses at 3 and 6 months trans-lates to long-term clinical benefit with superior PFS and OS, consist-ent with our previous study findings [1]. Seven-year OS rates forpatients with BCR–ABL1 (IS) !10% at 3 and 6 months were 72 and74%, respectively, and the 7-year PFS rates for patients with BCR–ABL1 (IS) !10% were 56 and 57% at 3 and 6 months, respectively.
Dasatinib was well tolerated, and no new safety signals weredetected in this analysis. The majority of AEs, both nonhematologicand hematologic, occurred early in the course of treatment. Cumula-tive rates of pleural effusion increased gradually over time in thestudy population, including the 100 mg QD arm; however, with aminimum follow-up of 7 years, incidence of drug-related pleural effu-sion was less common in the 100 mg QD arm relative to other
TABLE II. Drug-Related Adverse Events of Interest Over Time
Treated patients, n/at risk (%)
100 mg QD (n 5 165) Other dose groups (n 5 497)
2-year 5-year 7-year 2-year 5-year 7-year
Pleural effusion 23/121 (14) 40/55 (24) 46/42 (28) 118/309 (24) 158/127 (32) 174/91 (35)Pulmonary hypertension 0 (0) 0 (0) 3 (2) 5 (1) 8 (2) 13 (3)Pulmonary arterial hypertension – 0 (0) 1 (<1) – 0 (0) 0 (0)
Number of patients at risk 5 number of patients treated within a given year not having that adverse event.QD, once daily.
RESEARCH ARTICLE 7 Years of Dasatinib in Chronic Myeloid Leukemia
doi:10.1002/ajh.24423 American Journal of Hematology, Vol. 91, No. 9, September 2016 873
Drug-Related Adverse Events of Interest Over Time

35
Second line therapy: Nilotinibnilotinib in the second-line setting
© 2017 American Society of Health-System Pharmacists, Inc., and American College of Clinical Pharmacy All rights reserved 391
Table 6. Summary of trials of dasatinib in the second-line setting.71, 77-81
Selected Trials of Dasatinib in the Second-Line Setting Citation Population MCyR CCyR PFS
Hochhaus et al. (2007)
186 pts with imatinib-resistant or –intolerant CP-CML 52% 39% 92.4% at 8 mo
Hochhaus et al. (2008) “START-C”
387 pts with imatinib-resistant or –intolerant CP-CML 59% 49% 90% at 15 mo
80% at 24 mo
Kantarjian et al. (2009) “START-R”
150 pts with imatinib-resistant CP-CML 53% 44% 86% at 24 mo
Shah et al. (2010) (“CA180-034”)
670 pts with imatinib-resistant or –intolerant CP-CML 63% 50% 80% at 24 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; NR = not reported; PFS = progression-free survival.
Table 7. Summary of trials of nilotinib in the second-line setting.82-84 Selected Trials of Nilotinib in the Second-Line Setting
Citation Population MCyR CCyR PFS OS Kantarjian et al. (2011)
321 pts with imatinib-resistant or –intolerant CP-CML 59% 44% 64% at 24 mo 87% at 24 mo
Giles et al. 321 pts with imatinib-resistant or –intolerant CP-CML 59% 45% 57% at 48 mo 78% at 48 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; NR = not reported; OS, overall survival; PFS = progression-free survival.
Table 8. Summary of trials of bosutinib in the second-line setting.85
Selected Trials of Bosutinib in the Second-Line Setting Citation Population MCyR CCyR PFS OS
Cortes et al. (2011)
288 pts with imatinib-resistant or –intolerant CP-CML 53% 41% 79% at 24 mo 92% at 24 mo
CCyR = complete cytogenetic response; MCyR = major cytogenetic response; mo = months; PFS = progression-free survival; OS = overall survival.
VI. Third line therapy and beyond6, 10, 60, 86-92
A. Second-generation TKIs show solid efficacy in patients who have imatinib resistance or intolerance. However, approximately half of the patients receiving these agents in the second-line setting also experience resistance or intolerance.
B. A third TKI (second-generation TKI only) may be considered in this setting. No TKI is specifically indicated for treatment failure of both first- and second-generation TKIs, with current literature restricted to observational studies or studies with small patient populations.
C. Allogeneic stem cell transplantation may be considered (see Hematopoietic Stem Cell Transplantation by Dr. Merten).
36
Second line therapy:
Milestone for second line drug
CO
PYRI
GH
T: N
ETW
ORK
OF
EXC
ELLE
NC
E “E
URO
PEA
N L
EUK
EMIA
NET
“ -
PU
BLIS
HER
: WW
W.L
EUK
EMIA
-NET
.ORG
- D
ESIG
N A
ND
REA
LISA
TIO
N: W
WW
.SC
HA
EFER
-WER
BEA
GEN
TUR.
CO
M -
10.
2013Other definitions
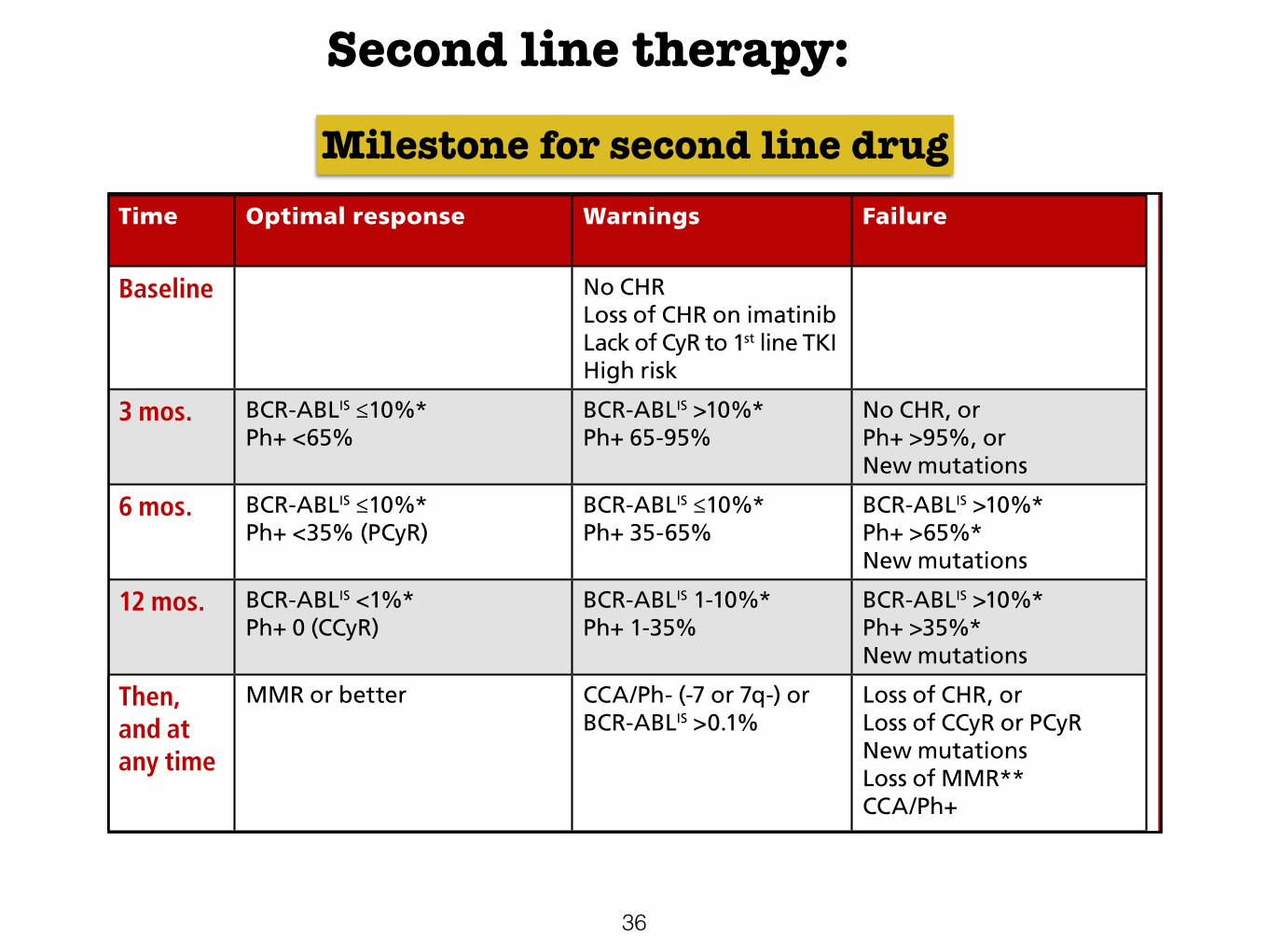
Response definitions to 2nd line therapy in case of failure of imatinib(can be used provisionally, NOT for the response to 3rd line treatment).
Time Optimal response Warnings Failure
Baseline No CHR Loss of CHR on imatinibLack of CyR to 1st line TKIHigh risk
3 mos. BCR-ABLIS ≤10%* Ph+ <65%
BCR-ABLIS >10%*Ph+ 65-95%
No CHR, or Ph+ >95%, orNew mutations
6 mos. BCR-ABLIS ≤10%* Ph+ <35% (PCyR)
BCR-ABLIS ≤10%*Ph+ 35-65%
BCR-ABLIS >10%*Ph+ >65%* New mutations
12 mos. BCR-ABLIS <1%*Ph+ 0 (CCyR)
BCR-ABLIS 1-10%*Ph+ 1-35%
BCR-ABLIS >10%* Ph+ >35%*New mutations
Then, and at any time
MMR or better CCA/Ph- (-7 or 7q-) orBCR-ABLIS >0.1%
Loss of CHR, orLoss of CCyR or PCyRNew mutationsLoss of MMR**CCA/Ph+
*and/or **in 2 consecutive tests, of which one ≥1% IS: BCR-ABL on International Scale
Timing of Cytogenetic and Molecular Monitoring
At diagnosis CBA, FISH in case of Ph- (for cryptic or variant translocations), qualitative PCR (transcript type)
During treatment RQ-PCR every 3 months until MMR has been achieved, then every 3 to 6 months and/orCBA at 3, 6, and 12 months until CCyR has been achieved, then every 12 months. Once CCyR is achieved, FISH on blood cells can be used.
Failure, progression RQ-PCR, mutational analysis, and CBA. Immunophenotyping in blast phase.
Warning Molecular and cytogenetic tests more frequently. CBA in case of myelodysplasia or CCA/Ph-
CBA: Chromosome banding analysis of marrow cell metaphases at least 20 metaphases analysed
Definition of response
Optimal response Best long-term outcome No indication for a change of treatment.
Failure Patient should receive a different treatmentto limit the risk of progression and death
Warning Characteristics of disease and response to treatment requiremore frequent monitoring to permit timely changes in therapy,in case of treatment failure.
CCA Clonal chromosome abnormalties
CCA/Ph+ CCA in Ph+ cells which define failure if newly arisen
CHR Complete hematologic response: Platelet count < 450 x 109 /L; WBC count <10 x 109 /L;Differential: no immature granulocytes, basophils <5%; no palpable spleen
High risk Evaluated by Sokal-Score (>1.2), Euro-Score (>1,480) or EUTOS-Score (>87)
Major route CCA/Ph+
Major route CCA/Ph+ are trisomy 8, 2nd Ph+ [+der(22)t(9;22)(q34;q11)], isochromosome 17[i(17)(q10)], trisomy 19, and ider(22)(q10)t(9;22)(q34;q11)
Mutations BCR-ABL kinase domain point mutations (not to be confused with ABL1 polymorphisms),Mutational analysis by conventional Sanger sequencing is recommended in case of progression, failure and warning.

37
Third line therapy and beyond

38
No TKI is specifically indicated for treatment failure of
both first- and second-generation TKIs.
current literature restricted to observational studies or
studies with small patient populations
Allogeneic stem cell transplantation may be considered
!
Third line therapy and beyond
39
Third line therapy and beyond
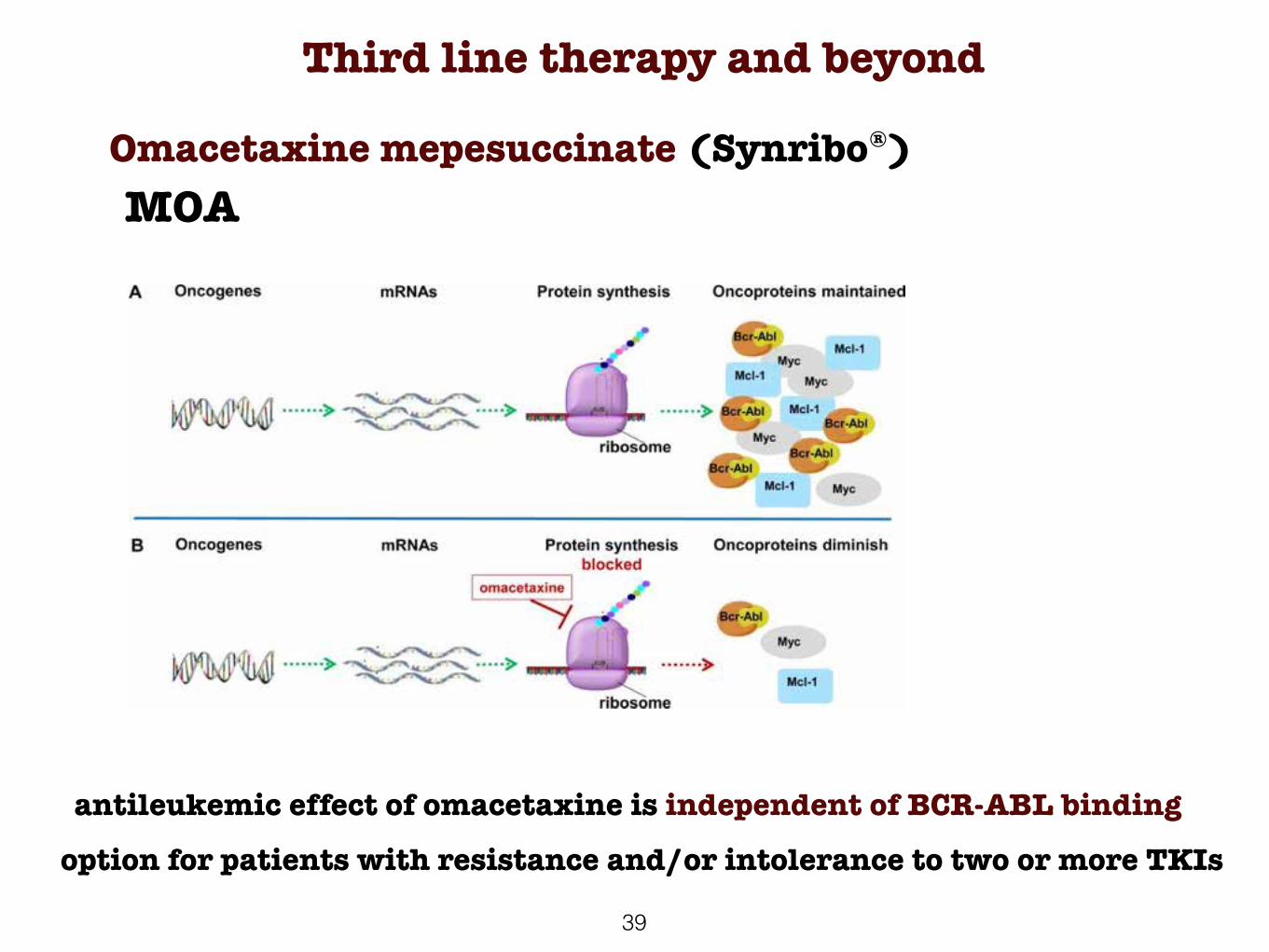
Omacetaxine mepesuccinate (Synribo®) MOA
antileukemic effect of omacetaxine is independent of BCR-ABL binding
option for patients with resistance and/or intolerance to two or more TKIs
!

40
Third line therapy and beyondOmacetaxine mepesuccinate (Synribo®)
2 phase II studies have been conducted in CP-CML:
patients with a T315I mutation or who had failed treatment
with one or more TKIs
patients that had failed treatment with two or more TKIs
allowed enrollment of patients who were in AP-CML
CCyR of 4-16% ;
median PFS - 7-7.7 months
major adverse effects - myelosuppression
subcutaneous, twice-daily dosing schedule - limit
compliance

41
Resistance to TKIs
A. Primary hematologic resistance
failure to achieve a hematologic remission 3-6 months after initiation of therapy
B. Primary cytogenetic resistance
failure to achieve any cytogenetic response at 6 months, MCyR at 12 months, or CCyR at 18 months
!!
Primary Resistance

42
Resistance to TKIs
Dose escalation of imatinib : 800 mg/day
Pt with cytogenetic relapse who achieved a
complete cytogenetic response with standard-
dose imatinib
suboptimal cytogenetic response to standard
dose imatinib
!
Primary Resistance

43
Resistance to TKIsSecondary Resistance
T315I mutation
“gatekeeper”
resistance to all currently available TKIs except ponatinib
44
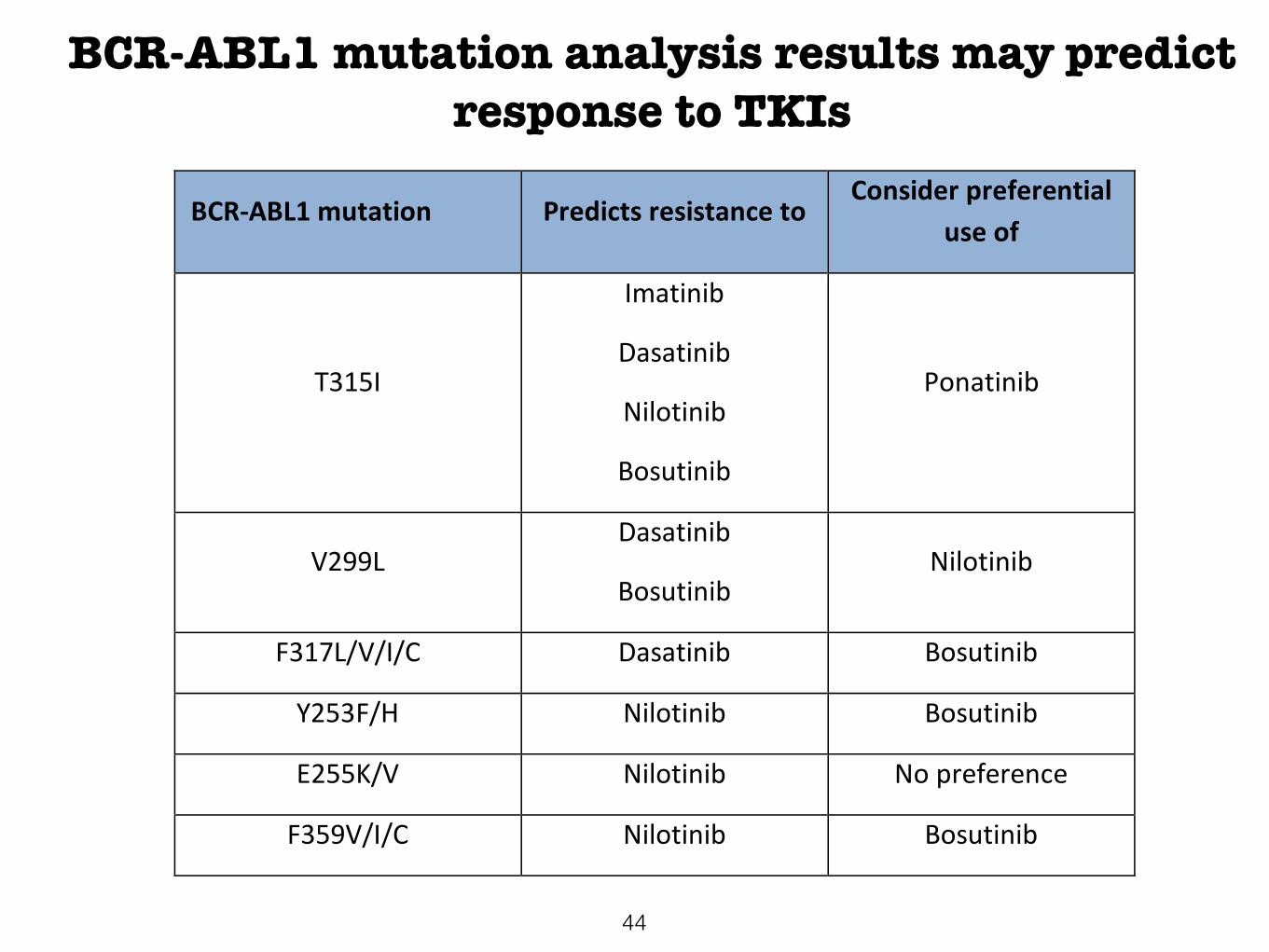
BCR-ABL1 mutation analysis results may predict response to TKIs
1) T315I mutation is also associated with disease progression and poorer survival.
c. Other mutations are emerging as clinically relevant, and may predict response to TKIs (see Table 10).
Table 10. BCR-ABL1 mutation analysis results may predict response to TKIs.3, 64, 82, 86
3. Identification of mutation(s) can support the diagnosis of TKI resistance, and may be helpful in the selection of alternative TKI therapy.54
a. Mutational analysis may also identify which CML patients may be candidates for allogeneic stem cell transplantation.
b. Consider performing BCR-ABL kinase domain mutational analysis in the following scenarios:3, 59, 84
1) For CP-CML patients with an inadequate initial response (defined as failure to achieve PCyR at 3 months or CCyR at 12 and 18 months).
2) For CP-CML patients with any loss of response (defined as hematologic or cytogenetic relapse, or 1-log increase in BCR-ABL transcript levels and loss of MMR).
3) For patients who experience disease progression to AP-CML or BC-CML.
C. Treatment of T315I mutated CML3, 29, 30, 77, 87-93
1. Ponatinib (Iclusig®)
a. Third-generation tyrosine kinase inhibitor.
b. Multi-targeted agent that is active against many BCR-ABL kinase domain mutations, including T315I.
c. The Ponatinib Ph+ ALL and CML Evaluation (”PACE”) trial studied ponatinib in 449 patients with resistance or intolerance to prior TKI therapy or with the T315I mutation.
BCR-ABL1 mutation Predicts resistance to Consider preferential
use of
T315I
Imatinib
Dasatinib
Nilotinib
Bosutinib
Ponatinib
V299L Dasatinib
Bosutinib Nilotinib
F317L/V/I/C Dasatinib Bosutinib
Y253F/H Nilotinib Bosutinib
E255K/V Nilotinib No preference
F359V/I/C Nilotinib Bosutinib
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG

45
Treatment of T315I mutated CML Ponatinib or Omacetaxine
Ponatinib : 3rd generation TKIs
Ponatinib in Ph-Positive Leukemias
n engl j med 369;19 nejm.org november 7, 2013 1789
Patie
nts
(%)
100
80
60
40
20
0
Complet
e
Hemato
logic
Respon
seM
ajor
Cytoge
netic
Respon
se
Complet
e
Cytoge
netic
Respon
seM
ajor
Mole
cular
Respon
se
Prob
abili
ty o
f Sus
atai
ned
Maj
or C
ytog
enet
ic R
espo
nse
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24
Months after First MajorCytogenetic Response
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24Pr
obab
ility
of O
vera
ll Su
rviv
al
30
Months
B Accelerated-Phase CML
A Chronic-Phase CMLTotal(N=267)
Resistance or side effects(N=203)
T315I(N=64)
Total(N=149)
Resistance or side effects(N=104)
T315I(N=45)
Total(N=267)
Resistance or side effects(N=203)
T315I(N=64)
Patie
nts
(%)
100
80
60
40
20
0
Majo
r
Hemato
logic
Respon
seM
ajor
Cytoge
netic
Respon
se
Complet
e
Cytoge
netic
Respon
seM
ajor
Mole
cular
Respon
se Prob
abili
ty o
f Sus
tain
ed M
ajor
H
emat
olog
ic R
espo
nse 1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24
Months after First MajorHematologic Response
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24Pr
obab
ility
of O
vera
ll Su
rviv
al
30
Months
C Blast-Phase CML
Total(N=83)
Resistance or side effects(N=65)
T315I(N=18)
Total(N=46)
Resistance or side effects(N=37)
T315I(N=9)
Total(N=83)
Resistance or side effects(N=65)
T315I(N=18)
Patie
nts
(%)
100
80
60
40
20
0
Majo
r
Hemato
logic
Respon
seM
ajor
Cytoge
netic
Respon
se
Complet
e
Cytoge
netic
Respon
se Prob
abili
ty o
f Sus
tain
ed M
ajor
H
emat
olog
ic R
espo
nse 1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24
Months after First MajorHematologic Response
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24Pr
obab
ility
of O
vera
ll Su
rviv
al
30
Months
D Ph-Positive ALL
Total(N=62)
Resistance or side effects(N=38)
T315I(N=24)
Total(N=19)
Resistance or side effects(N=12)
T315I(N=7)
Total(N=62)
Resistance or side effects(N=38)
T315I(N=24)
Patie
nts
(%)
100
80
60
40
20
0
Majo
r
Hemato
logic
Respon
seM
ajor
Cytoge
netic
Respon
se
Complet
e
Cytoge
netic
Respon
se Prob
abili
ty o
f Sus
tain
ed M
ajor
H
emat
olog
ic R
espo
nse 1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24
Months after First MajorHematologic Response
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24Pr
obab
ility
of O
vera
ll Su
rviv
al
30
Months
Total(N=32)
Resistance or side effects(N=10)
T315I(N=22)
Total(N=13)
Resistance or side effects(N=5)
T315I(N=8)
Total(N=32)
Resistance or side effects(N=10)
T315I(N=22)
9495 91
5651
70
4640
66
3427
56
555750
31 32 29 23 1829
18 16 21
4150
3647
60
41 3850
32
3934
56
242233
161422
The New England Journal of Medicine Downloaded from nejm.org at PRINCE OF SONGKLA UNIVERSITY on March 3, 2017. For personal use only. No other uses without permission.
Copyright © 2013 Massachusetts Medical Society. All rights reserved.
PACE study : patients with resistance or intolerance to prior TKI therapy or with the T315I mutation
4-year MMR rate - 61%, 4-year PFS- 56%, 4- year OS -77%.

46
Treatment of T315I mutated CMLPonatinib : Epic trial was terminated after the
observation of arterial thrombotic events.
pan-VEGF inhibition
!
Black Box Warning
Current guidelines recommend consideration of
ponatinib only for patients with a T315I mutation and
for patients who have failed 2 or more prior TKIs
47
TKI Toxicities

48
strong negative association between comorbidities at
diagnosis and OS in patients with CP-CML
no negative effect of comorbidities on remission rates or
progression to advanced stages of disease
TKI Toxicities

49
TKI toxicities
3. Enrollment in a clinical trial is encouraged.
Patient Case #1, continued:
LP’s therapy is changed from imatinib to dasatinib. What toxicities is LP likely to experience from both her first and second-line therapies? What counseling points would be important to stress to LP during your discussions with her?
XIII. TKI toxicities
A. Similar patterns of toxicity are noted across the TKIs.3, 54, 90, 94-97
B. Risk factors of each toxicity include dose of TKI and the patient’s underlying co-morbid conditions.98, 99
C. Hematologic adverse effects are more prominent in second-line therapy compared to front-line therapy.99
Table 11. Suggestions for management of common TKI toxicities.3, 54, 90, 94-97
Toxicity Management Strategy
Neutropenia Hold until recovery, potential dose reduction Myeloid growth factors may be considered
Anemia ESAs not supported in patients with myeloid malignancies. Thrombocytopenia Hold until recovery, potential dose reduction
Rash Topical or systemic steroids Dose reduction, interruption or discontinuation
D. Unique toxicities of each agent are likely related to the agent’s off-target kinase profile (see Table 12).30
E. The risk of each agent’s unique toxicity may be higher in patients who have received TKIs in a sequential manner.98
BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PHULFDQ6RFLHW\RI+HDOWK6\VWHP3KDUPDFLVWV,QFDQG$PHULFDQ&ROOHJHRI&OLQLFDO3KDUPDF\$OOULJKWVUHVHUYHG
Suggestions for management of common TKI toxicities
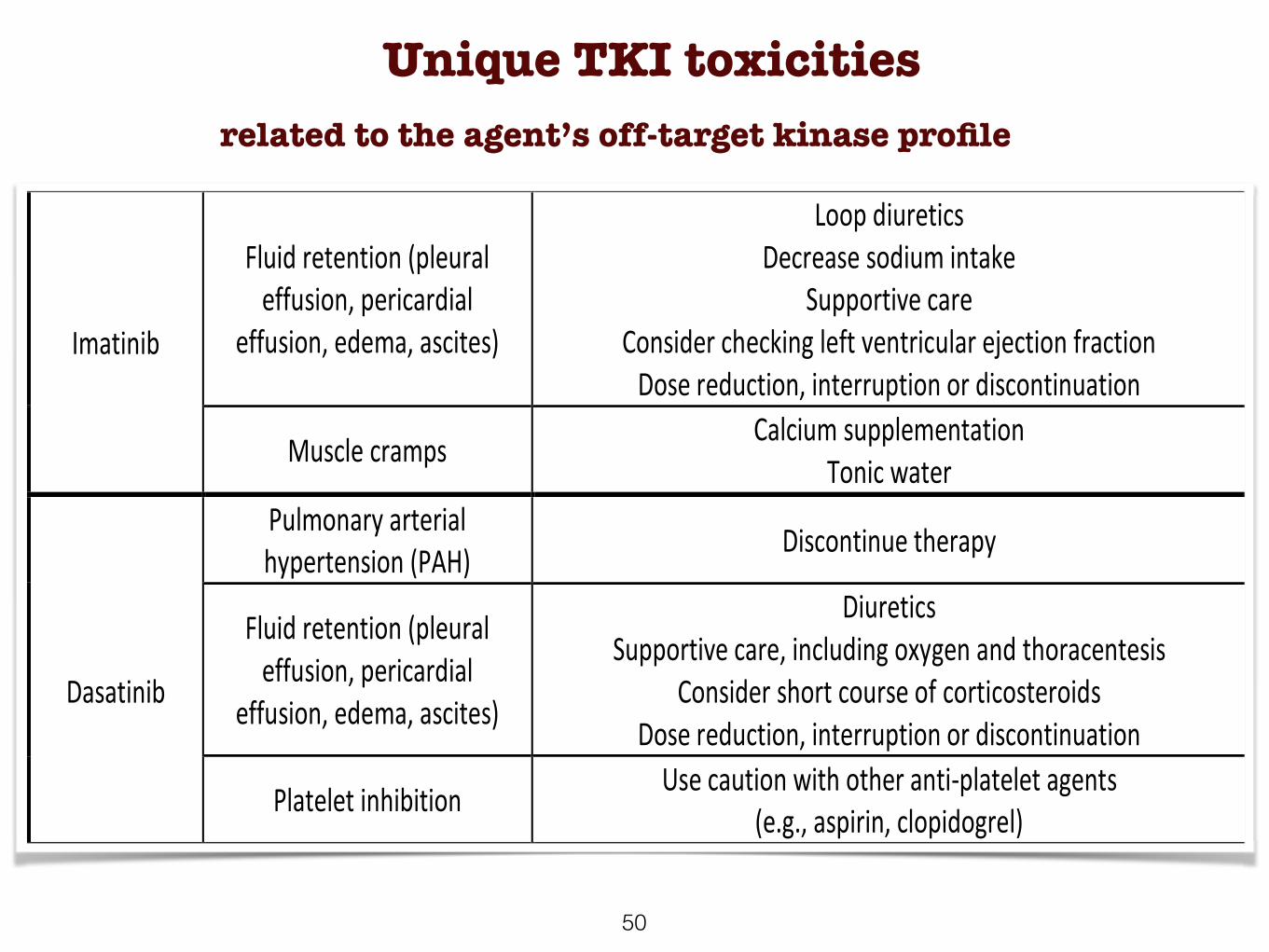
50
Unique TKI toxicities related to the agent’s off-target kinase profile
© 2017 American Society of Health-System Pharmacists, Inc., and American College of Clinical Pharmacy All rights reserved 397
Table 11. Unique TKI toxicities and suggestions for management.6, 10, 17, 18, 59, 73, 75, 101, 107-112, 114-117 Management of Unique TKI Toxicities
TKI Toxicity Management Strategy
Imatinib
Fluid retention (pleural effusion, pericardial
effusion, edema, ascites)
Loop diuretics Decrease sodium intake
Supportive care Consider checking left ventricular ejection fraction
Dose reduction, interruption or discontinuation
Muscle cramps Calcium supplementation Tonic water
Dasatinib
Pulmonary arterial hypertension (PAH) Discontinue therapy
Fluid retention (pleural effusion, pericardial
effusion, edema, ascites)
Diuretics Supportive care, including oxygen and thoracentesis
Consider short course of corticosteroids Dose reduction, interruption or discontinuation
Platelet inhibition Use caution with other anti-platelet agents (e.g., aspirin, clopidogrel)
Nilotinib
QT prolongation
ECG to measure QTc at baseline, 7 days after initiation and periodically thereafter
Correct hypokalemia and hypomagnesemia Consider dose reduction or discontinuation
Elevated serum lipase or amylase
Hold until recovery, then dose reduction
Hepatic toxicity Hold until recovery, then dose reduction or discontinuation
Peripheral arterial occlusive disease (PAOD)
Eliminate all risk factors (smoking, obesity, hypertension, etc) Consider prophylactic aspirin therapy
Discontinue therapy “Metabolic syndrome”
(hyperglycemia, hypercholesterolemia, hypertriglyceridemia)
Maximize glycemic, cholesterol and triglyceride control
Bosutinib Hepatic toxicity Hold until recovery, then dose reduction or discontinuation
Diarrhea Antidiarrheal medication and fluid replacement
Hold until recovery
Ponatinib
Hepatic toxicity Hold until recovery, then dose reduction or discontinuation Ischemic reactions,
hypertension, vascular occlusion,
heart failure
Control risk factors for hypertension and atherosclerosis Referral to cardiologist
Discontinue therapy
Elevated serum lipase or amylase
Symptomatic pancreatitis Hold until recovery, then dose reduction
F. Specific toxicities – for more detailed information, please refer to the prescribing information of the individual agents.10, 52, 55, 101, 109-112, 117, 119
1. Hypophosphatemia and associated changes in bone and mineral metabolism have been reported in small groups of imatinib patients.
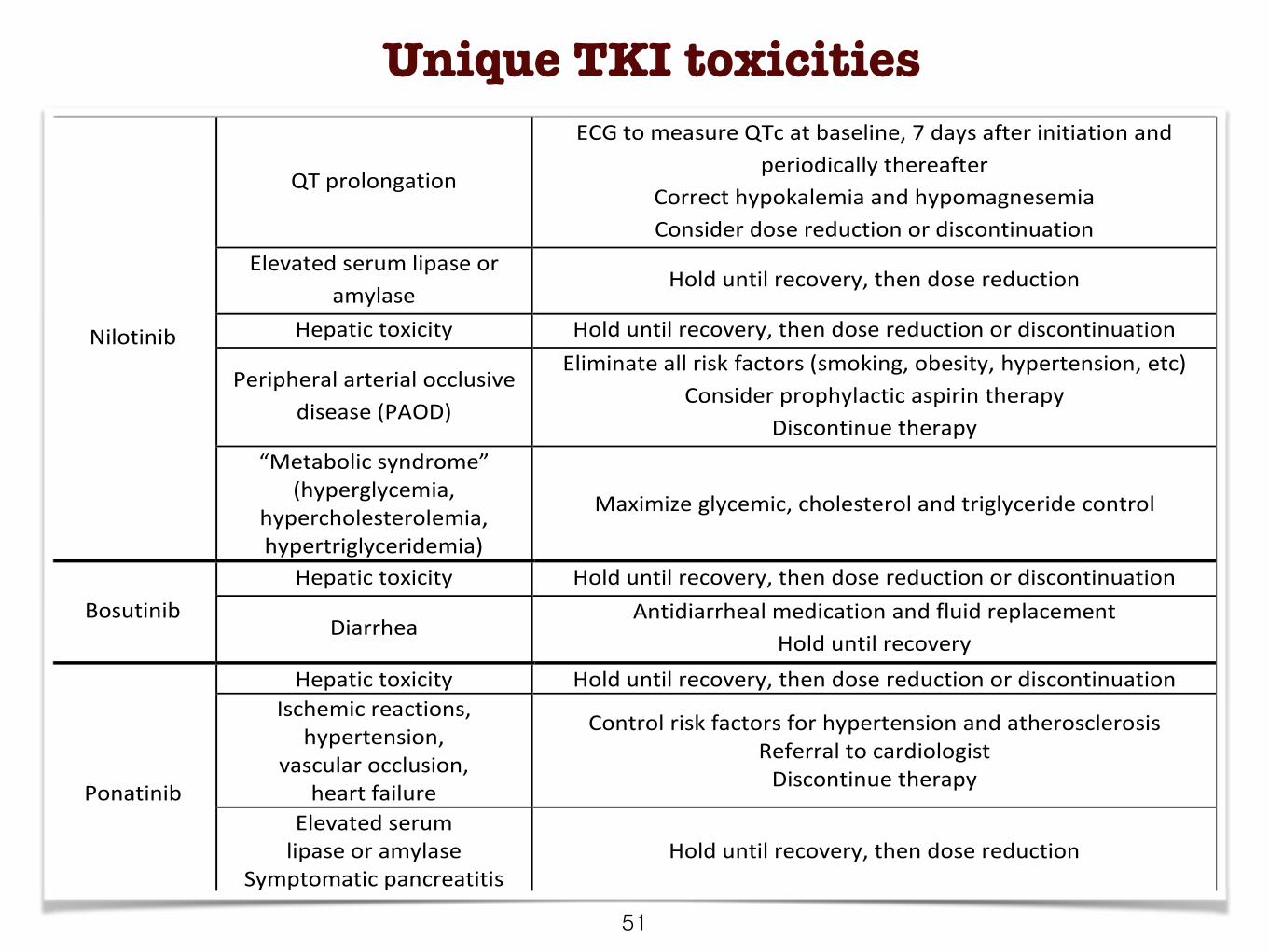
51
Unique TKI toxicities
© 2017 American Society of Health-System Pharmacists, Inc., and American College of Clinical Pharmacy All rights reserved 397
Table 11. Unique TKI toxicities and suggestions for management.6, 10, 17, 18, 59, 73, 75, 101, 107-112, 114-117 Management of Unique TKI Toxicities
TKI Toxicity Management Strategy
Imatinib
Fluid retention (pleural effusion, pericardial
effusion, edema, ascites)
Loop diuretics Decrease sodium intake
Supportive care Consider checking left ventricular ejection fraction
Dose reduction, interruption or discontinuation
Muscle cramps Calcium supplementation Tonic water
Dasatinib
Pulmonary arterial hypertension (PAH) Discontinue therapy
Fluid retention (pleural effusion, pericardial
effusion, edema, ascites)
Diuretics Supportive care, including oxygen and thoracentesis
Consider short course of corticosteroids Dose reduction, interruption or discontinuation
Platelet inhibition Use caution with other anti-platelet agents (e.g., aspirin, clopidogrel)
Nilotinib
QT prolongation
ECG to measure QTc at baseline, 7 days after initiation and periodically thereafter
Correct hypokalemia and hypomagnesemia Consider dose reduction or discontinuation
Elevated serum lipase or amylase
Hold until recovery, then dose reduction
Hepatic toxicity Hold until recovery, then dose reduction or discontinuation
Peripheral arterial occlusive disease (PAOD)
Eliminate all risk factors (smoking, obesity, hypertension, etc) Consider prophylactic aspirin therapy
Discontinue therapy “Metabolic syndrome”
(hyperglycemia, hypercholesterolemia, hypertriglyceridemia)
Maximize glycemic, cholesterol and triglyceride control
Bosutinib Hepatic toxicity Hold until recovery, then dose reduction or discontinuation
Diarrhea Antidiarrheal medication and fluid replacement
Hold until recovery
Ponatinib
Hepatic toxicity Hold until recovery, then dose reduction or discontinuation Ischemic reactions,
hypertension, vascular occlusion,
heart failure
Control risk factors for hypertension and atherosclerosis Referral to cardiologist
Discontinue therapy
Elevated serum lipase or amylase
Symptomatic pancreatitis Hold until recovery, then dose reduction
F. Specific toxicities – for more detailed information, please refer to the prescribing information of the individual agents.10, 52, 55, 101, 109-112, 117, 119
1. Hypophosphatemia and associated changes in bone and mineral metabolism have been reported in small groups of imatinib patients.
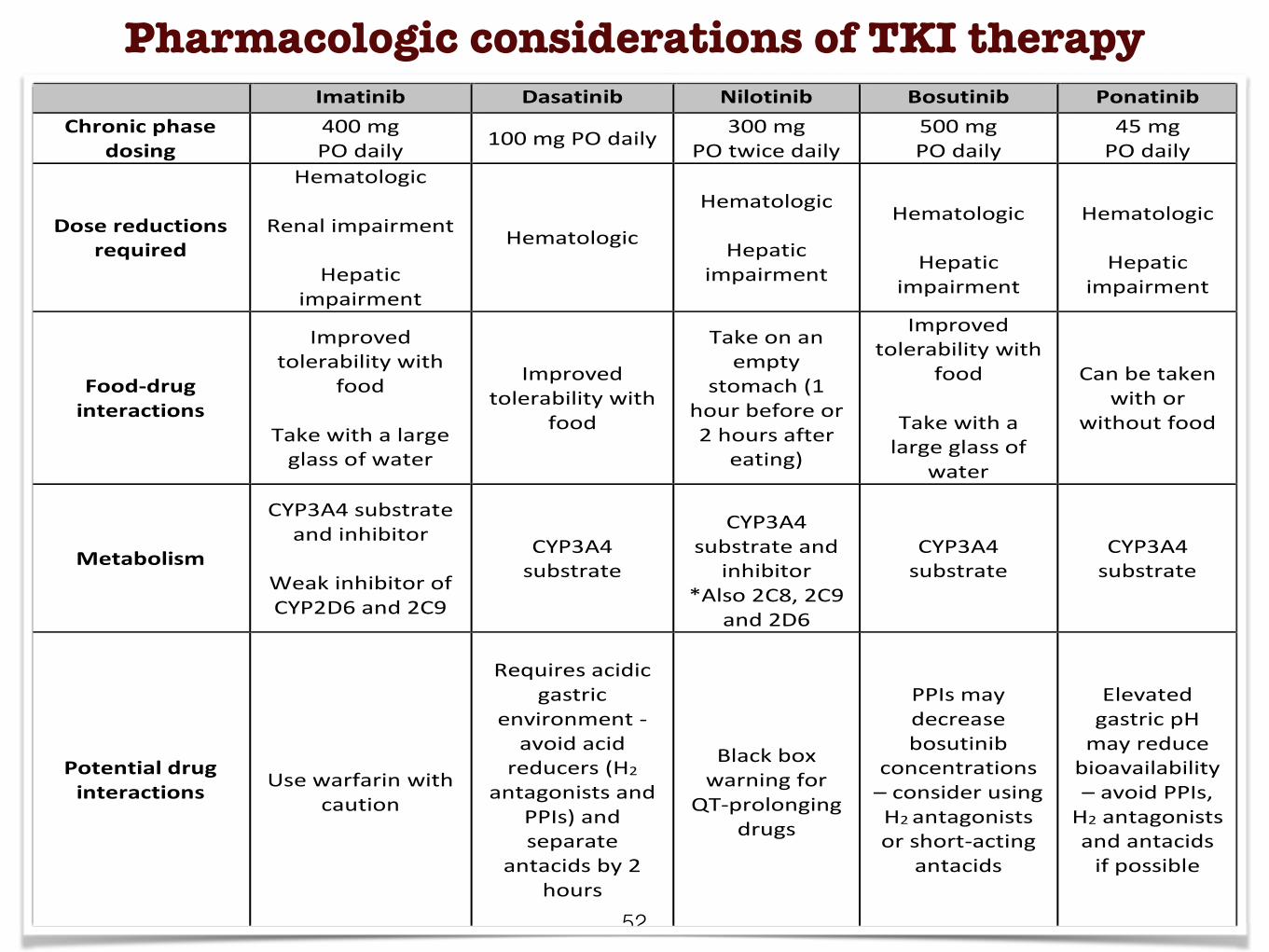
52
© 2017 American Society of Health-System Pharmacists, Inc., and American College of Clinical Pharmacy All rights reserved 399
Table 12. Pharmacologic considerations of TKI therapy.4, 10, 55, 59, 101, 109-112, 120 Imatinib Dasatinib Nilotinib Bosutinib Ponatinib
Chronic phase dosing
400 mg
PO daily 100 mg PO daily
300 mg
PO twice daily
500 mg
PO daily
45 mg
PO daily
Dose reductions required
Hematologic
Renal impairment
Hepatic
impairment
Hematologic
Hematologic
Hepatic
impairment
Hematologic
Hepatic
impairment
Hematologic
Hepatic
impairment
Food-drug interactions
Improved
tolerability with
food
Take with a large
glass of water
Improved
tolerability with
food
Take on an
empty
stomach (1
hour before or
2 hours after
eating)
Improved
tolerability with
food
Take with a
large glass of
water
Can be taken
with or
without food
Metabolism
CYP3A4 substrate
and inhibitor
Weak inhibitor of
CYP2D6 and 2C9
CYP3A4
substrate
CYP3A4
substrate and
inhibitor
*Also 2C8, 2C9
and 2D6
CYP3A4
substrate
CYP3A4
substrate
Potential drug interactions
Use warfarin with
caution
Requires acidic
gastric
environment -
avoid acid
reducers (H2
antagonists and
PPIs) and
separate
antacids by 2
hours
Black box
warning for
QT-prolonging
drugs
PPIs may
decrease
bosutinib
concentrations
– consider using
H2 antagonists
or short-acting
antacids
Elevated
gastric pH
may reduce
bioavailability
– avoid PPIs,
H2 antagonists
and antacids
if possible
Assistance program Yes Yes Yes Yes Yes
CYP = cytochrome P450; H2 = histamine type 2; PPI = proton pump inhibitor.
IX. Monitoring response to TKI therapy
A. Monitoring disease response to TKI therapy is one of the key management strategies of CML.6, 10, 63, 121-123
B. Consensus recommendations support ongoing, regular monitoring of CP-CML patients who receive
treatment with TKIs.10, 21-23, 38, 46, 54, 55, 71, 124
1. Achievement of cytogenetic response is an important prognostic indicator of long-term survival of
patients who receive imatinib.
2. Early cytogenetic responses to initial therapy with second-generation TKIs is also predictive of both
PFS and OS in newly diagnosed CP-CML.
Pharmacologic considerations of TKI therapy
53
Goal - return patient to chronic phase
Bone marrow cytogenetics and mutational analysis prior to the initiation of treatment
use TKIs to reduce the disease burden prior to allo HSCT
Achieving MCyR or CCyR to TKI therapy prior to allo HSCT - better transplant outcome !
Accelerated phase / blast crisis

54
Treatment :
accelerated phase
- imatinib 600 mg OD, dasatinib 140 mg OD,
nilotinib 400 mg bid or bosutinib 500 mg OD
- Omacetaxine - not an option for patients who
present with AP-CML.
Accelerated phase
55
blast crisis
- TKI+chemotherapy - RR 25-60% (AML or
ALL) + HCST
- TKI + steroids
!
Blast crisis

56
TKIs for the treatment of relapse after allo HSCT
1.TKI ± DLI- imatinib, dasatinib, nilotinib, bosutinib !
2. Omacetaxine
!

57



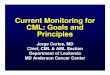








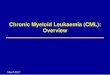






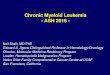




![203341Orig1s000 - Food and Drug Administrationtreatment of adults with chronic myeloid leukemia [CP-CML, AP-CML, and BP-CML] with resistance or intolerance to prior therapy including](https://img.pdfslide.us/doc/110x75/60bcb776f8906f48904ac5cb/203341orig1s000-food-and-drug-administration-treatment-of-adults-with-chronic.jpg)