Embed Size (px)
Citation preview
1
Tabuk University
Faculty of Applied Medical Sciences
Department Of Medical Lab. Technology
3rd Year – Level 5 – AY 1433-1434
HEMATOLOGY – 2, MLT 307
2
By/Dr. Walid ZAMMITI
CHRONIC MYELOID LEUKEMIA (CML)
3
Objectives Define CML, and know the causes.
Describe clinical signs and symptoms of CML
Classify CML
Explain the prognostic significance of cytogenetic
abnormalities
Cite methods for diagnosing CML
4
Whath is CML? Clonal malignant myeloproliferative disorder characterized
by increased proliferation of the granulocytic cell line without
the loss of their capacity to differentiate.
Results in increases in myeloid cells, erythroid cells and
platelets in peripheral blood and marked myeloid
hyperplasia in the bone marrow
Originate in a single abnormal haemopoietic stem cell
accounts for around 15% of leukaemias and may occur at
any age.
Most frequently between the ages of 40 and 60 years.
Progress slowly (runs a slow course)
Not immediately fatal.

5
Hematopoiesis : process by which blood cell (by bone marrow) lineages are produced
• WBCs (WHITE BLOOD CELLS, or leukocyte) subdivided into
• Myeloid lineages• Lymphoid lineages
6
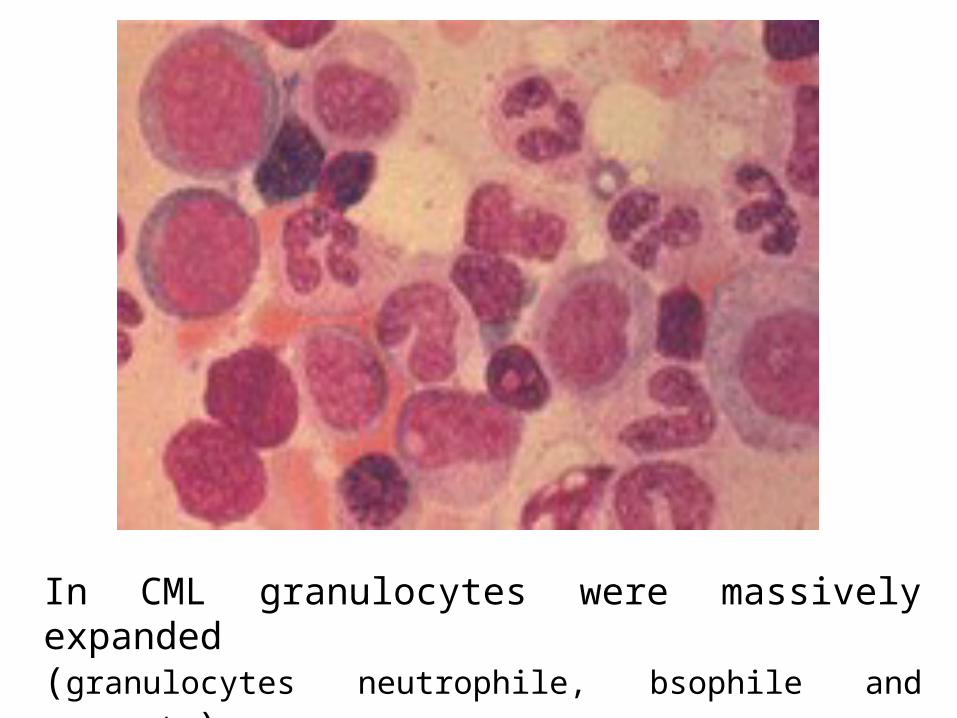
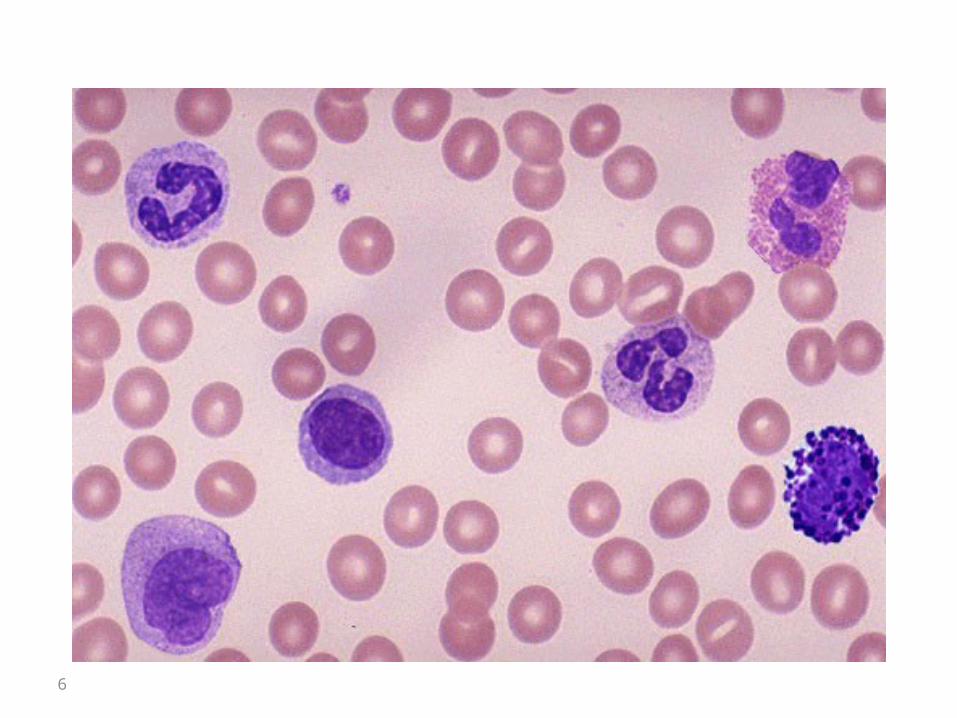
In CML granulocytes were massively expanded(granulocytes neutrophile, bsophile and monocyte)
8
CML Etiology Not clear
Little evidence of genetic factors linked to the
disease
High level radiation/toxin exposure
Increased incidence
Survivors of the atomic disasters at Japan
(Nagasaki & Hiroshima)
Post radiation therapy
9
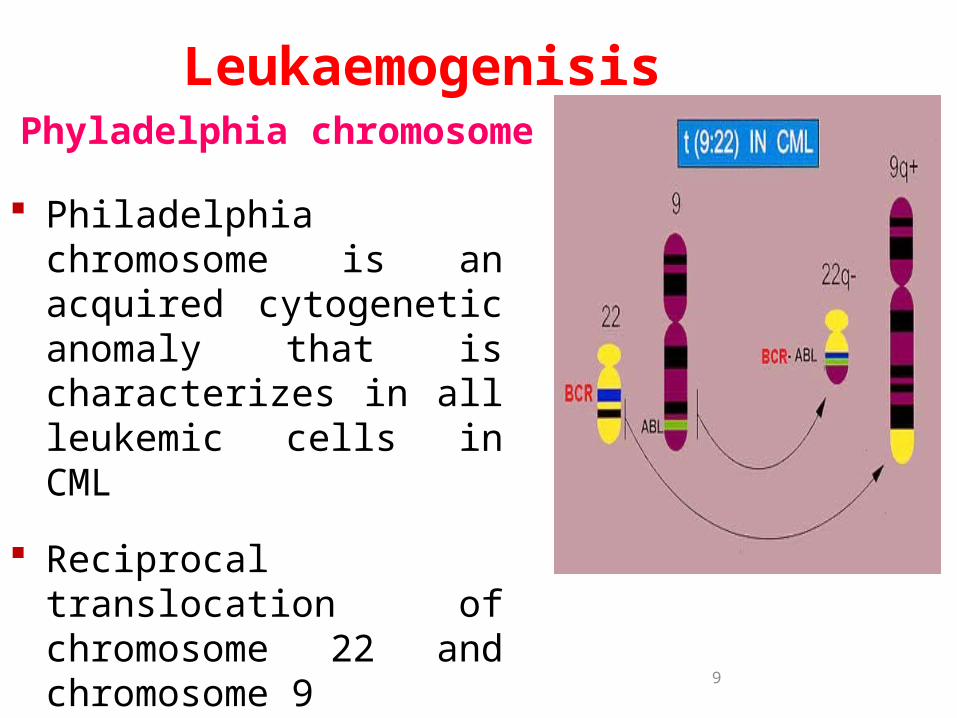
Phyladelphia chromosome
Philadelphia chromosome is an acquired cytogenetic anomaly that is characterizes in all leukemic cells in CML
Reciprocal translocation of chromosome 22 and chromosome 9
90-95% of CML patients have Ph chromosome
Leukaemogenisis
10
• BCR (breakpoint cluster region) gene on chromosome 22 fused to the ABL (Ableson leukemia virus) gene on chromosome 9
The resulting fusion gene (BCR-ABL) produce an altered protein believed to play a key role in development of CML
• Ph chromosome is found on myeloid, monocytic, erythroid, megakaryocytic, B-cells and sometimes T-cell proof that CML derived from pluripotent stem cell
BCR-ABL Oncogene
11
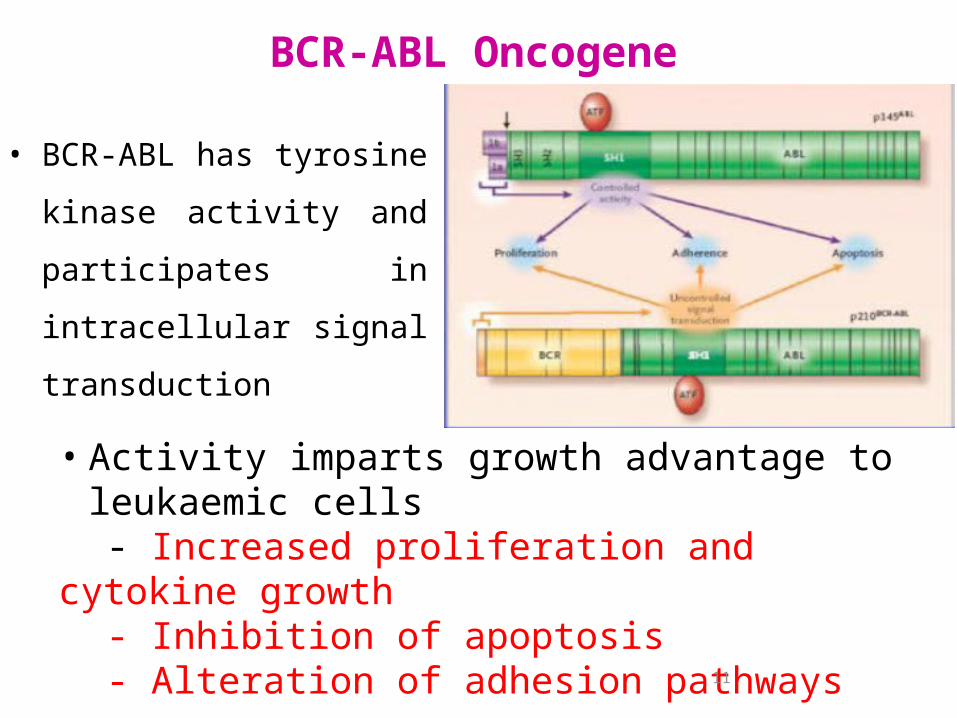
BCR-ABL Oncogene
• Activity imparts growth advantage to leukaemic cells
- Increased proliferation and cytokine growth- Inhibition of apoptosis - Alteration of adhesion pathways
• BCR-ABL has tyrosine
kinase activity and
participates in intracellular
signal transduction
Symptoms related to hypermetabolism (e.g.weight loss, anorexia or night sweats).
Splenomegaly (massive)
Features of anemia may include pallor and tachycardia.
Bruising, epistaxis or haemorrhage from other sites because of abnormal platelet function.
Gout or renal impairment caused by hyperuricemia from excessive purine breakdown may be a problem.
Rare symptoms include visual disturbances.
In up to 50% of cases the diagnosis is made incidentally from a routine blood count.
40% asymptomatic
CML: Clinical manifestation
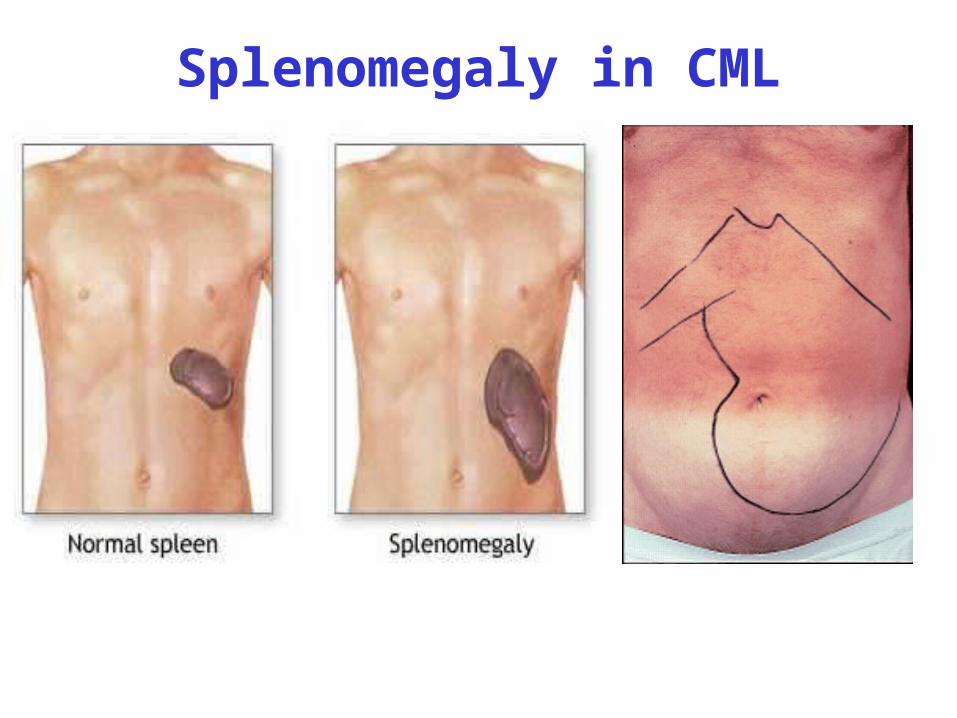
Splenomegaly in CML
14
Stages of Chronic Myeloid Leukemia
• Disease is biphasic, sometimes triphasic.• Chronic phase
• Accelerated phase
• Acute phase (Blast Phase)
15
• Majority (>80%) of cases of CML diagnosed in chronic phase
• Defined by
– Elevated WBC count (≥20 × 109 /L)
– Basophilia & Eosinophilia
– The platelet count is normal or elevated, and may exceed 1,000 × 109/L
Relative lack of blasts (<10% in periferal blood and bone marrow)
The chronic phase
16
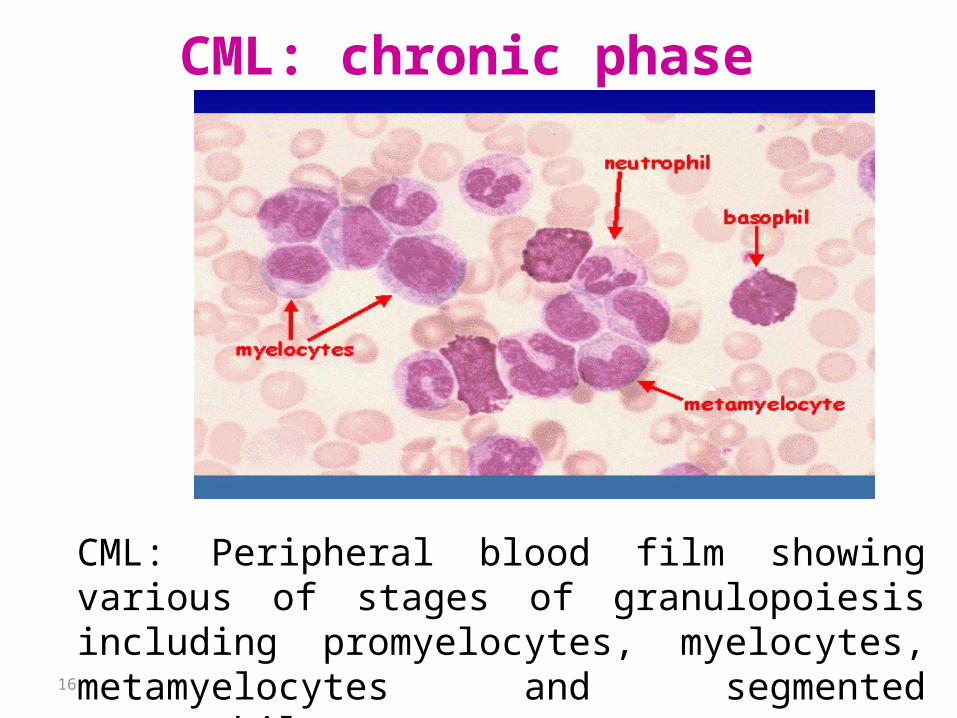
CML: chronic phase
CML: Peripheral blood film showing various of stages of granulopoiesis including promyelocytes, myelocytes, metamyelocytes and segmented neutrophils
17
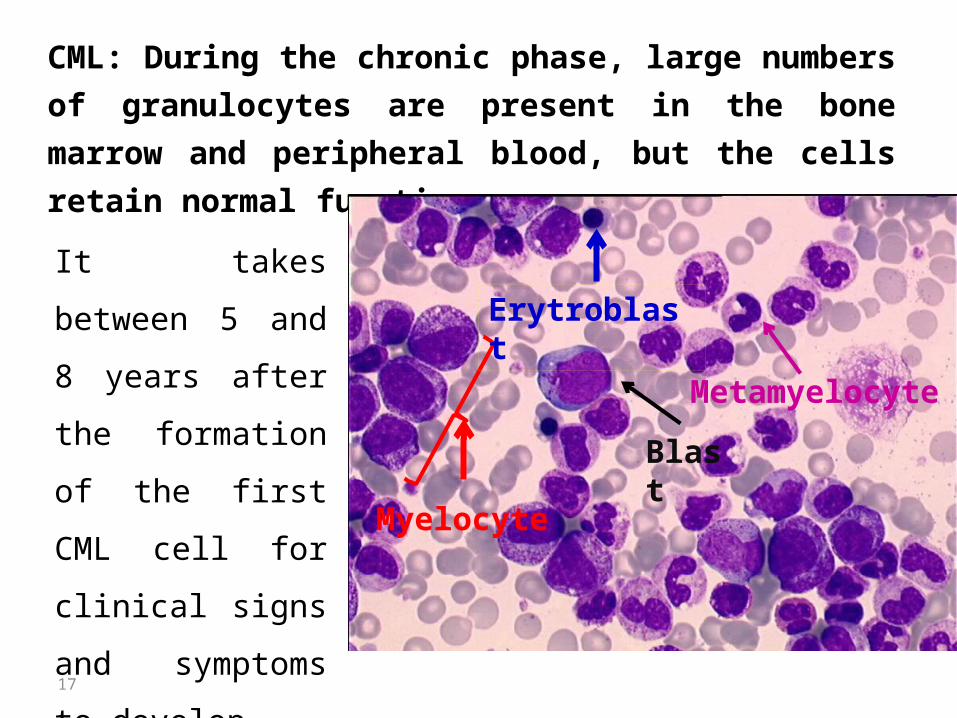
CML: During the chronic phase, large numbers of
granulocytes are present in the bone marrow and
peripheral blood, but the cells retain normal functions.
It takes between 5
and 8 years after
the formation of
the first CML cell
for clinical signs
and symptoms to
develop.
Myelocyte
Blast
Metamyelocyte
Erytroblast
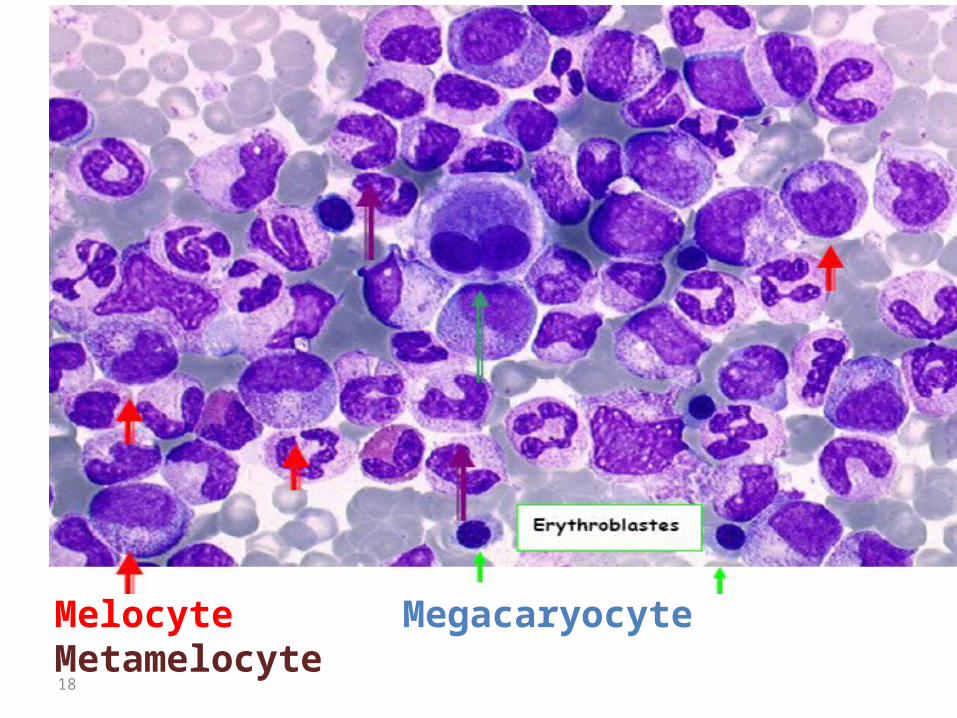
18
Melocyte Megacaryocyte Metamelocyte
19
The accelerated phase• Second and intermediate phase of CML • Defining criterion: ≥ 5% to ≥19% blast in blood and
marrow • Persistent thrombocytopenia (<100 × 109/L) or
thrombocytosis (>1,000 × 109/L) despite treatment. • Characterized by general and progressive anemia
my mark onset – Fever unknown origin– Bone pain– Symptoms related to splenomegaly
• Median duration : 3-18 months

20
Blast phase • Final disease phase characterized by ≥20%
to ≥30% blasts in peripheral blood or marrow they are lymphoid, usually precursor B lymphoblasts.
• Increasing symptomology
– Fatigue related to progressive anemia
– Bleeding
– Infectious complication
– CNS dysfunction
• Phase rapidly fatal, with median survival ranging from 3 to 12 months .
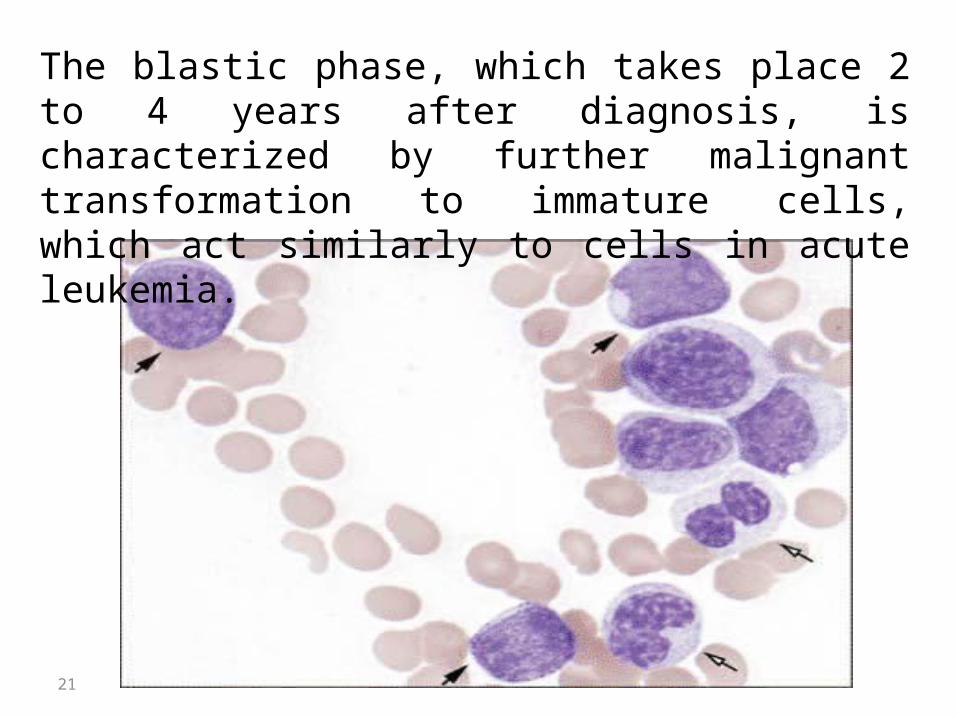
21
The blastic phase, which takes place 2 to 4 years after diagnosis, is characterized by further malignant transformation to immature cells, which act similarly to cells in acute leukemia.
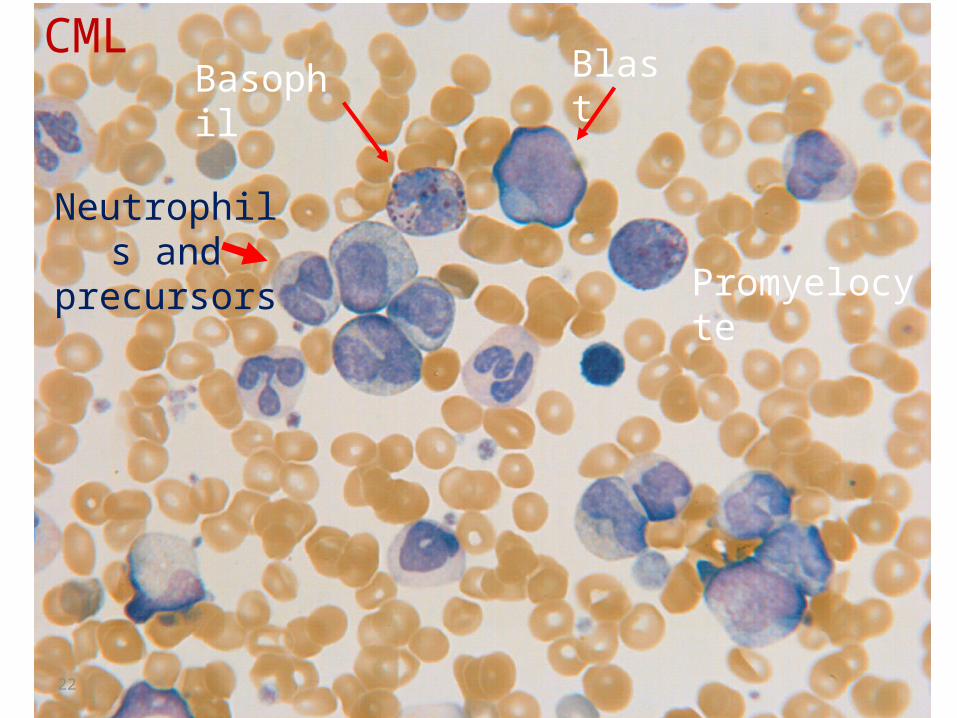
22
Basophil Blast
Neutrophils and
precursors Promyelocyte
CML

23
Clinical presentaion of Ph+ and CML
24
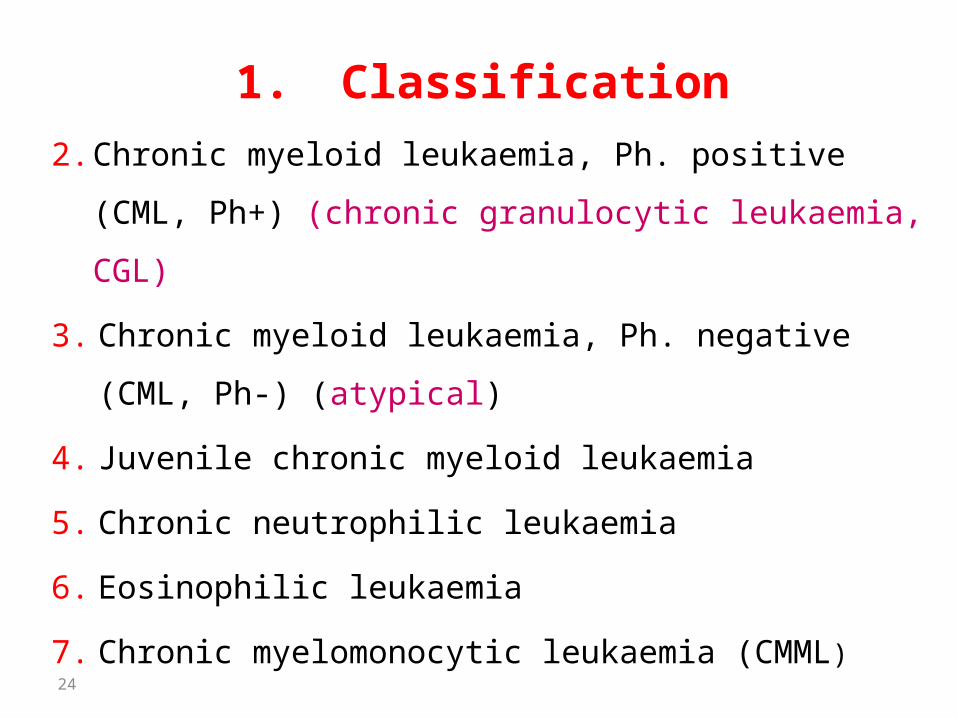
1. Classification
2. Chronic myeloid leukaemia, Ph. positive (CML,
Ph+) (chronic granulocytic leukaemia, CGL)
3. Chronic myeloid leukaemia, Ph. negative (CML,
Ph-) (atypical)
4. Juvenile chronic myeloid leukaemia
5. Chronic neutrophilic leukaemia
6. Eosinophilic leukaemia
7. Chronic myelomonocytic leukaemia (CMML)
25
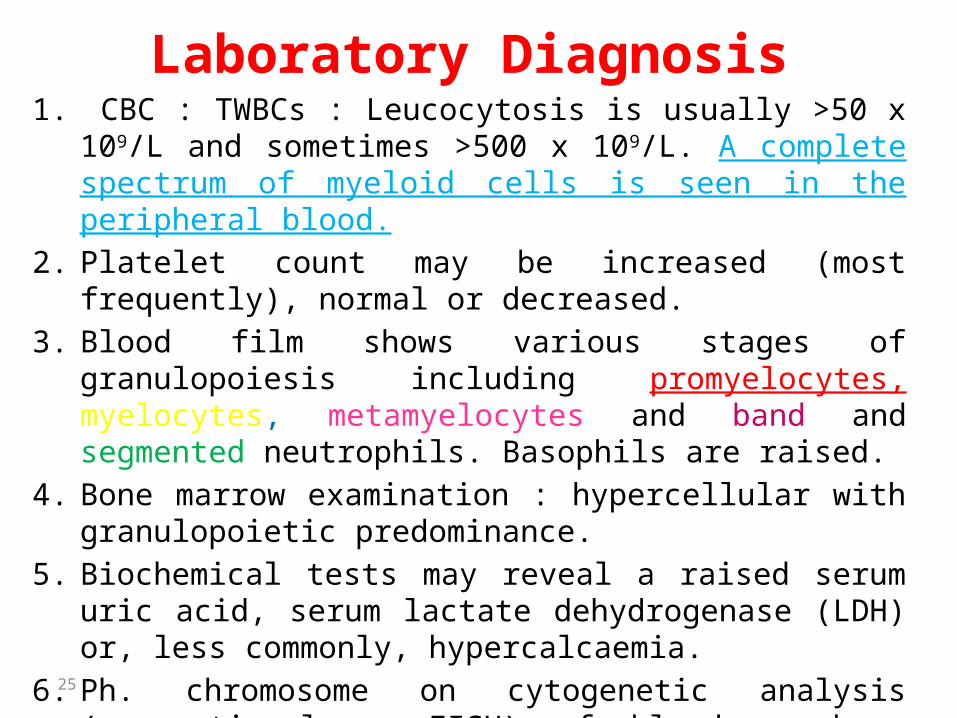
Laboratory Diagnosis1. CBC : TWBCs : Leucocytosis is usually >50 x 109/L and
sometimes >500 x 109/L. A complete spectrum of myeloid cells is seen in the peripheral blood.
2. Platelet count may be increased (most frequently), normal or decreased.
3. Blood film shows various stages of granulopoiesis including promyelocytes, myelocytes, metamyelocytes and band and segmented neutrophils. Basophils are raised.
4. Bone marrow examination : hypercellular with granulopoietic predominance.
5. Biochemical tests may reveal a raised serum uric acid, serum lactate dehydrogenase (LDH) or, less commonly, hypercalcaemia.
6. Ph. chromosome on cytogenetic analysis (conventional or FISH) of blood or bone marrow.
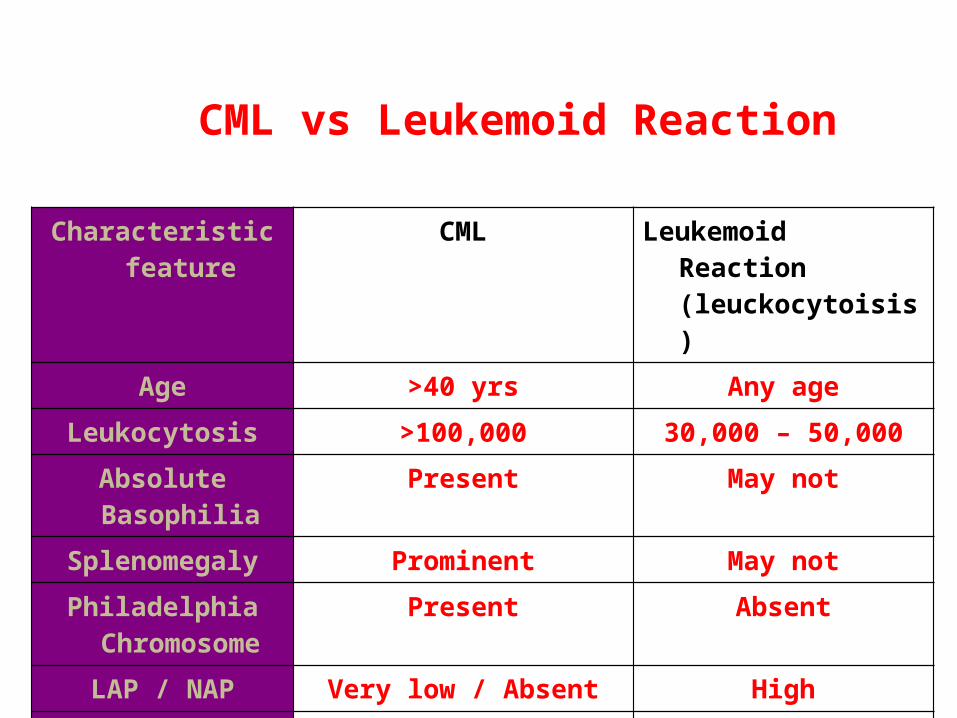
Characteristic feature
CML Leukemoid Reaction (leuckocytoisis)
Age >40 yrs Any age
Leukocytosis >100,000 30,000 – 50,000
Absolute Basophilia Present May not
Splenomegaly Prominent May not
Philadelphia Chromosome
Present Absent
LAP / NAP Very low / Absent High
Transformation to Acute leukemia
Yes No
CML vs Leukemoid Reaction
27
Home work• Describe the main differences between CML and AML
• A 50-year-old man presents with a two-month history of fatigue and early satiety. His complete blood count shows the following:WBC:75,000/µL, Hgb:14 g/dL, Platelets:550,000/µL, Differential: Segmented neutrophils (granulocytes): 33,000/µL (normal range: 1,800-7,000/µL) ,Bands:1,500/µL (normal range: 0-700/µL) Metamyelocytes:11,000/µL (normal: 0),Myelocytes:7500/µL (normal: 0),Basophils: 3,750/µL (normal range: 0-200/µL),Lymphocytes:3,000/µL (normal range 1,000-4,800/µL),Monocytes:750/µL (normal range 0-800/µL).
What are the hematologic abnormalities present here?

28
Thank you