Embed Size (px)
Citation preview

Christina Metzler Chief Public Affairs Officer
KOTA Annual Conference September 2015

Identify, promote distinct value
Prepare evidence to improve practice
Promote thinking, implementation of primary care
Engage in transdisciplinary advocacy
Advocate for role in mental health
Create codes that reflect true practice
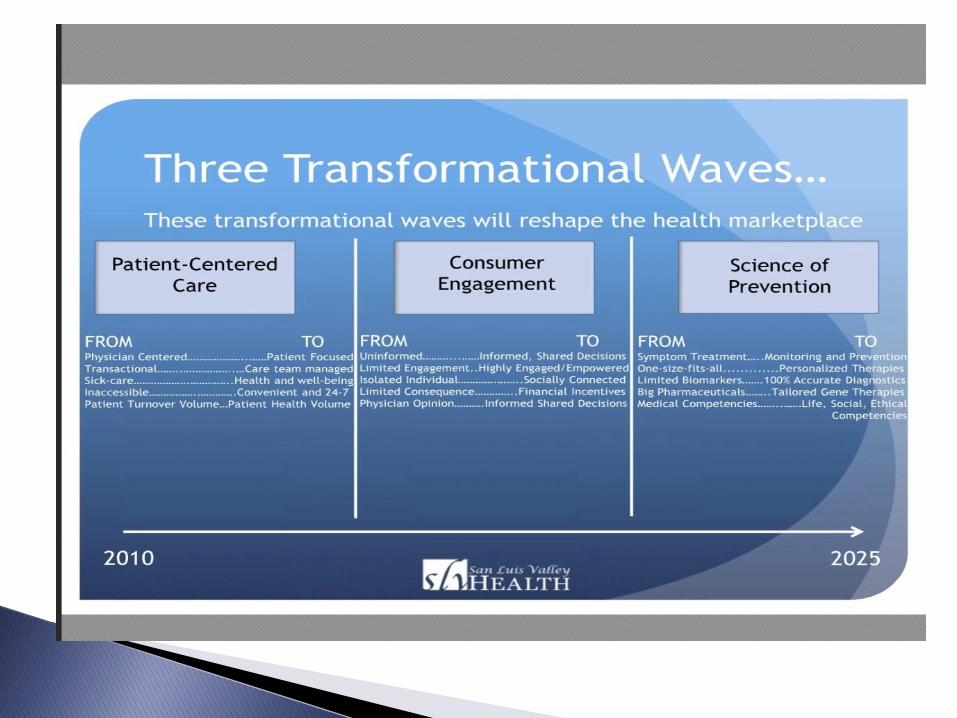
Give you insight into the future

Reducing avoidable hospital readmissions
Assisting patients with adherence to treatment regimens
Helping people maintain independence
Identifying the need for early interventions
Management of chronic conditions
Transitioning patients through care continuum


Occupational therapy's distinct value is to improve health and quality of life through facilitating participation and engagement in occupations, the meaningful, necessary, and familiar activities of everyday life. Occupational therapy is client-centered, achieves positive outcomes, and is cost-effective

“90% of the management of a chronic disease must come from the person who has the disease.”
California Healthcare Foundation, 2008

“Self-management is defined as the tasks that individuals must undertake to live well with one or more chronic conditions. These tasks include having the confidence to deal with medical management, role management, and emotional management of their conditions.” Institute of Medicine, 2003

Readiness/motivation Skills analysis/synthesis Habits Routines Roles Rituals Context & environments
Patient Activation is a fancy word for what OT practitioners have always done.


Alzheimer’s Disease and Related Disorders (Schaber,
2010)
‣ Compensatory and environmental strategies help maintain function.
‣ Compensatory and environmental strategies improve participation in desired activities
‣ Caregiver education increases caregiver self-efficacy
‣ Management of the environment promotes participation in activities, enhancing wellness
‣ Management of nighttime sleep hygiene assists with caregiver burden.


VALUE
◦What matters
◦What can be done
◦What it costs
◦Who cares
VALUE
◦How we calculate
◦How we ask
◦How we ?????

Advancing the Value and Quality of Occupational Therapy in Health Service Delivery
Leland, Crum, Phipps, Roberts, Gage

Prevention and Wellness
◦ Fall Intervention
Systemic Outcomes
◦Discharge Intervention by OT

Health Outcomes:
Policy: ACA/ Healthcare Reform/ Health Systems Reform
Changes in Health Delivery: CMMI; ACO; Medical Homes; Other Innovation Models
PRIMARY HEALTH CARE Interprofessional Collaborative Practice
Chronic
Care
Health &
Wellness Integrated
Health Care
Population
Health
Community
Based Practice
Transition
Planning
Quality Measures/ Outcomes/ Value

Defining Primary Care: Envisioning the
Roles of Occupational Therapy
Metzler, Hartmann, Lowenthal

Integrated, Comprehensive Care
◦Whole person orientation
Range of Life
◦Well-Elderly Study

‣ Body Structure or Body Function
‣ Sensation and Sensory Processing
‣ Mental Functions and Social Skills/Psychosocial
‣ Cognitive Strategies, Actions
‣ Activities of Daily Living (ADLs)
‣ Instrumental activities of daily living (IADLs) ALL WOULD BE PER SESSION; SOME SPECIALTY CODES (WHEELCHAIR ASSESSMENT)
KEPT

• IMPACT Act
Quality Measures
Data Gathering
• 21st Century Cures Act
• AOTA Proposed Core OT Codes

• Collect data in post acute across settings
• Equalize payment?
• Equalize access? Choice?
• Change payment systems?

22
Care Planning/ Decision Support
Payment
Quality Reportin
g
QI Care
Transitions
Data Element and Response Code

IRF-PAI
LTCH CARE
Data Set
OASIS-C
MDS 3.0
Data Elements
HCBS CARE
Uniformity

Data categories:
◦ Functional status
◦ Cognitive function and mental status
◦ Special services, treatments, and interventions
◦Medical conditions and co-morbidities
◦ Impairments
◦Other categories required by the Secretary 24
Use of Standardized Assessment Data: HHAs: no later than January 1, 2019 SNFs, IRFs, and LTCHs: no later than October 1, 2018
Functional Cognition
Appropriate Testing
Role for OT in care to achieve
◦ Better outcomes
◦ Fewer adverse events
◦ Less caregiving
◦Optimum independence


Distinction
Impact Value


Help and Hope for Patients Through Biomedical Innovation
(Passed the House by a vote of 344-77 on July 10, 2015)
Bipartisan!

New incentives to develop new drugs Removing regulatory uncertainty for new medical
options Helping the entire biomedical ecosystem
coordinate more efficiently to find faster cures. Investing in 21st century science and next
generation investigators. Removing barriers to increased research
collaboration Incorporating the patient Measuring success and identifying diseases earlier
through personalized medicine. Modernizing clinical trials.

“We in America do not have government by the majority. We have government by the majority who participate.”
-Thomas Jefferson




6 JANUARY 19, 2015 • WWW.AOTA.ORG
C A P I T A L B R I E F I N G
he Improving Medicare Post-Acute Care Transformation (IMPACT) Act (Pub. Law 113-185) was passed by both houses of Congress in Septem-ber and signed into law by President Obama on October 6, 2014. AOTA has been proactive with Congress and the Centers for Medicare & Medicaid Services (CMS) regarding the effect of the IMPACT Act on
occupational therapists and occu-pational therapy assistants working in post-acute care (PAC) settings. IMPACT emphasizes several key areas that can provide the opportunity to highlight the distinct value of occupa-tional therapy.
The objective of Congress in passing IMPACT is to capture better, consistent data; carefully and specif-ically document outcomes related to function and cognition; and rethink how services in skilled nursing facil-ities (SNFs), home health agencies, inpatient rehabilitation facilities, and long-term-care hospitals are provided, evaluated, and paid for. Ultimately, the goal is to ensure that appropri-ate, quality care is provided through equitable costs across these settings. But occupational therapy practition-ers will have to be ready to meet the challenges, expand their practice, and meet the targeted patient needs emphasized in IMPACT.
What are the details? Starting on October 1, 2016, and continuing over several years, CMS is directed to have in place systems to capture data sets that will be the same across the four PAC settings. These patient character-istic data must look at certain clinical areas, including critical points of
intervention for occupational therapy, such as:� Function, including mobility, self-
care, and history of falls� Cognitive function and mental
conditions, such as depression and dementia
� Medical conditions and comorbidi-ties, such as diabetes and pressure ulcers
� Impairments, such as incontinence
Occupational therapy practitioners cover all these areas. But cognition and mental health have often been secondary considerations in settings like SNFs and home health. In some cases, this is because reimbursement was thought to be less likely to be approved for treatment that addressed dementia, depression, or executive function. Many therapy providers assume that these areas are not reimbursable and incorrectly advise that these areas be given less or no emphasis in occupational therapy interventions.
The IMPACT Act shows that Con-gress and CMS see things differently. The underlying message of IMPACT is that PAC settings must look more at the whole patient, just as occupational therapy practitioners consider all of their clients’ basic and instrumental activities of daily living needed to function and remain healthy (i.e., not re-hospitalized) when they move from PAC to community outpatient care.
AOTA believes that the profession of occupational therapy is poised to enter this wide-open door presented by IMPACT to prove its distinct value for the whole client, so why wait for
October 2016? The time is now to start thinking about protocols and clinical judgment to be sure that the profes-sion of occupational therapy maxi-mizes its impact on clients’ function, cognition, and mental health.
Will Medicare pay for addressing these areas of intervention? If it does not, we must challenge those denials. We must read and understand the federal Medicare guidance and local coverage determinations for ourselves and be flexible, pushing the boundar-ies of our own clinical thinking as well as the boundaries of our PAC settings. Facilities are also reading the words in the law—function, self-care, cognition, falls, depression, and dementia—and realizing that they must ensure they collect and measure these patient data, as well as provide interventions that demonstrate improvement. Occu-pational therapy practitioners must be ready with the methods of assessment, evidence knowledge, and professional skill to help clients achieve outcomes as well as help facilities be ready for new data collection that reflects a new, focused approach to care.
For more details about the IMPACT Act, see AOTA’s summary and comment letter at http://tinyurl.com/mokjbfn.
Be part of the future. Examine your evaluations and plans of care, think about your assessment choices, and keep your occupational therapy vision wide open. �
Sharmila Sandhu, JD, is AOTA’s director of
Regulatory Affairs.
Chris Metzler is AOTA’s chief public affairs
officer.
TMake an IMPACT on
Post-Acute CareSharmila Sandhu and Chris Metzler

C A P I T A L B R I E F I N G
he Patient Protection and Affordable Care Act (ACA) may seem like ancient history, but its wide-ranging effects are still being felt today on Capitol Hill, with questions about how to fund health care programs intertwined with Medicare spending and many other issues. The debate over the ACA included much discussion about how to “bend the cost curve,” or slow down spending within Medicare. This hoped-for slowdown was partly to correct problems (e.g., inappropriate utiliza-tion, excessive billing) and partly to subsidize new health care programs.
EMPHASIZING VALUEAlthough the debate over the ACA was at times acrimonious, the con-cepts of using alternative payment methodologies (APMs; e.g., account-able care organizations [ACOs], primary care medical homes), coordi-nating care, checking payment levels for errors, and promoting a focus on outcomes has brought Congress and the White House, as well as Repub-licans and Democrats, together: All agree that we must pay for value, not volume, when it comes to health care. The ongoing debate concerns exactly how. The ACA directed the Centers for Medicare & Medicaid Services (CMS) to scale up what had previously been small demonstration projects, and APMs have proliferated in Medi-care, Medicaid, and private insurance. At the same time, the focus on quality reporting in Medicare has increased steadily. For instance, failure to report on quality measures through the Phy-sician Quality Reporting System now results in negative payment adjust-ments for private practitioners in Medicare. The Improving Post-Acute
Care Act, passed last fall, is expected to lead to data collection and quality measures becoming a more critical aspect of payment at skilled nurs-ing facilities, home health, inpatient rehabilitation facilities, and long-term acute hospitals. In January, the U.S. Department Health and Human Ser-vices (HHS) began promoting a long-term initiative to aggressively move payments to quality-based APMs, such as ACOs and the Comprehensive Pri-mary Care Initiative. The HHS goal is for 50% of Medicare reimbursement to be made through APMs by 2018, with all other payment under Medicare to be tied strictly to quality by 2018.
CONGRESSIONAL ACTIONAt press time, Congress was working on a bill to alter how providers are paid under Medicare, also known as the Sustainable Growth Rate, which drives the levels of payment under the Medicare Physician Fee Sched-ule. This overhaul would prevent a 30% cut to therapy and physician payments under Part B, and would provide bonus incentives for certain practitioners participation in APMS beginning in 2017. The overhaul would also, sometime before 2024, launch a Merit-Based Incentive Payment System, the complexity of which makes selecting G-codes seem easy by comparison. These changes are part of a steady move toward reducing the growth of spending in Medicare and toward paying for health care value over volume.
GETTING INVOLVEDCongress and CMS are showing no hesitation about pushing value-based purchasing and APMs in often
untested forms, making advocacy by the occupational therapy profession critical to preserving our clients’ best interests. Thus, you will be at the front lines of defending your profession every time you determine a plan of care and report on an intervention. Occupational therapy practitioners’ ability to speak to quality and value measures, through clear evaluation reports and substantive progress notes, is crucial. Equally important is the profession’s ability to convey its value to the overall health, wellness, and management of the Medicare population.
We must assume that, eventually, all occupational therapy practitioners reimbursed under Medicare will have their payment linked to quality report-ing and participation in an APM. This may create challenges, but providing higher quality, prevention-oriented services is far preferable to the other alternative: caps on and cuts to benefi-ciary services. New and improved sys-tems should mean better outcomes for beneficiaries of occupational therapy services. Occupational therapy practi-tioners possess a unique understand-ing of the interaction between person, task, and environment, and how ones’ habits, role, and routines can affect health outcomes, valuable knowledge in these new, value-oriented systems of care. We must be ready to say so loudly and clearly.
For more on these issues and infor-mation on how to get involved, visit www.aota.org/advocacy. �
Christina Metzler is AOTA’s chief public affairs
officer.
Heather Parsons is AOTA’s director of Legislative
Advocacy.
TValue, Not Volume
Making Occupational Therapy’s Distinct Value ShineChristina Metzler Heather Parsons
7OT PRACTICE • APRIL 13, 2015

HEALTH POLICY PERSPECTIVES
Advancing the Value and Quality of OccupationalTherapy in Health Service Delivery
Natalie E. Leland, Karen Crum, Shawn Phipps, Pamela Roberts,
Barbara Gage
MeSH TERMS
� delivery of health care
� occupational therapy
� patient outcome assessment
� quality of health care
� value-based purchasing
Natalie E. Leland, PhD, OTR/L, BCG, FAOTA, is
Assistant Professor, Mrs. T.H. Chan Division of
Occupational Science and Occupational Therapy and
Davis School of Gerontology, University of Southern
California, Los Angeles; [email protected]
Karen Crum, MA, OTR/L, is Clinical Doctorate
Resident, Rehabilitation Health Services Research Lab,
Mrs. T.H. Chan Division of Occupational Science and
Occupational Therapy, University of Southern California,
Los Angeles.
Shawn Phipps, PhD, MS, OTR/L, FAOTA, is Chief
Quality Officer and Associate Hospital Administrator,
Rancho Los Amigos National Rehabilitation Center, Los
Angeles, and Director, American Occupational Therapy
Association Board of Directors, Bethesda, MD.
Pamela Roberts, PhD, OTR/L, SCFES, FAOTA,
CPHQ, is Program Director, Physical Medicine and
Rehabilitation and Neuropsychology, Cedars–Sinai
Medical Center, Los Angeles, and Vice Chair and
Chair-Elect, Accreditation Council for Occupational
Therapy Education, Bethesda, MD.
Barbara Gage, PhD, MPA, is Senior Vice President,
Scientific Research and Evaluation, PAC Center for
Research, and Fellow, Brookings Institution, Washington,
DC.
Leland, N. E., Crum, K., Phipps, S., Roberts, P., & Gage, B. (2015). Health Policy Perspectives—Advancing the value and
quality of occupational therapy in health service delivery. American Journal of Occupational Therapy, 69,
6901090010. http://dx.doi.org/10.5014/ajot.2015.691001
The Patient Protection and Affordable Care Act of 2010 (ACA; Pub. L. 111–
148) is driving the health care system to shift from a volume-based re-
imbursement system to one based on value and high quality with an emphasis
on evidence-based and patient-centered care. The objective of this new para-
digm is to improve patient outcomes by incentivizing providers to deliver
scientifically grounded best practices by linking payment to performance. The
end goals are to improve population health outcomes, enhance consumer sat-
isfaction, and reduce health care costs—often referred to as the Triple Aim(Berwick, Nolan, & Whittington, 2008). In this health care reform context, it is
imperative to define and delineate the distinct value and unique role of occu-
pational therapy. Failure of the profession to clearly demarcate what constitutes
high-quality occupational therapy and demonstrate its contribution to the
broader patient outcomes that value-based care will measure may marginalize
occupational therapy in the rapidly changing health care environment.
The objective of this article is to provide a foundation on which to build
further dialogue and evidence to highlight the profession’s distinctive contri-
bution, significance, and viability as health care policies shift to focus on quality
and value. To achieve this goal, we present a framework for examining health
care quality and patient outcomes, describe the health care context that is driving
the need for quality measurement in occupational therapy, explain the concept of
value-based care in the context of occupational therapy, and discuss how occu-
pational therapy can define high-quality care processes to enhance outcomes and
ensure a viable future for the profession.
Framework for Examining Health Care Quality
To improve patient outcomes in clinical practice, it is necessary to understand the
theory behind health care quality. Donabedian (1966, 2003) proposed a theo-
retical framework in which health care quality can be evaluated and outcomes
targeted for improvement. In his model, Donabedian postulated that outcomes
The American Journal of Occupational Therapy 6901090010p1
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

are the result of the care processes that are provided and the
structure in which care is delivered. Donabedian defined
care processes as actions offered by the health care provider
to the patient, whereas structure includes the character-
istics of the context and environment in which the care is
delivered (e.g., physical space, practice culture, policies
and procedures, staffing). Guided by this model, the most
direct way to improve outcomes is to target the care
processes that are delivered (Donabedian, 1966, 2003).
Care processes have been identified as the most readily
adaptable elements within Donabedian’s model, which
makes them an ideal target for quality improvement.
Medicare’s Physician Quality Reporting System
(PQRS) and the American Medical Association’s (AMA’s)
Physician Consortium for Performance Improvement (PCPI),
among other bodies, are engaged in the development of
both process and outcome measures (Commission on Ac-
creditation of Rehabilitation Facilities, 2014; Joint Com-
mission, 2014; PCPI, 2011). To target outcomes for
improvement, it is necessary to identify what care should
be provided, document the delivery of that care, and
evaluate the outcomes resulting from the delivery of those
care processes, also referred to as care process quality in-dicators. These quality indicators are evidence-based and
patient-centered clinical action items that reflect critical and
prioritized interventions that can be delivered and docu-
mented consistently across organizations and by clinicians in
pursuit of achieving desired patient outcomes (Mainz, 2003).
Defining High-Quality Care: Developing Care ProcessQuality Indicators
Many health care professions have developed care process
quality indicators to improve outcomes, demonstrate their
unique value, and enhance service delivery (Min et al.,
2011; Rubenstein et al., 2004; Wenger et al., 2010).
Although the emphasis has been on the development of
care process measures, outcome measures (e.g., 30-day
readmissions) and composite measures, which combine
information on more than one performance measure, are
also being developed. PCPI, the National Quality Forum
(NQF), and the Agency for Healthcare Research and
Quality (AHRQ) have standardized protocols for de-
veloping both process and outcome quality measures
(Batelle, 2011; NQF, 2011; PCPI, 2011). The protocol
comprises six phases, the first of which is measure de-velopment. During this initial phase, an expert panel is
convened to prioritize a set of measures drawn from the
existing evidence base and stakeholder priorities using the
RAND Appropriateness Model (Battelle, 2011; NQF,
2011). The panel is made up of a broad group of
stakeholders relevant to the measure development topic
area and includes, but is not limited to, providers,
topical experts, researchers, payers, administrators, and
informatics specialists.
The protocol requires that the identified measures
then go through five additional phases: measure specification,evaluation, implementation, maintenance, and enhancement.Measures are currently being developed by a variety of health
care stakeholder groups, including national organizations,
the federal government, consumer advocates, professional
societies, and researchers.
Improving Outcomes: Integrating Quality MeasuresInto Practice
The objective of developing care process quality measures
is to define minimum standards of care. Guided by the
standardized six-phase protocol described in the preceding
section, physicians have been actively engaged in defining
care process quality measures and integrating those
measures into clinical practice in an effort to improve
patient outcomes (Wenger, Shekelle, & ACOVE Investi-
gators, 2001). For example, a group of physician researchers
were acutely aware of the devastating impact accidental falls
had on the health and quality of life of community-
dwelling older adults. In an effort to prevent this undesir-
able outcome and enhance care delivery, they developed
a series of care process quality measures for fall prevention
in primary care (Rubenstein et al., 2004). The objective
was to decrease the likelihood of falling, and the associated
subsequent poor outcomes, for older adult patients.
Using the standardized six-phase protocol, physician
groups have defined fall prevention care processes, oper-
ationalized them as quality measures, and then integrated
these measures into clinical documentation to support
clinical decision making (Min et al., 2011; Rubenstein et al.,
2004). The essential quality measures include improving
screening rates, enhancing fall risk factor identification, and
facilitating necessary referrals to other disciplines targeting
the identified risk factors. A controlled trial found that
primary care facilities that integrated the quality measures
into clinical practice had a higher rate of delivering and
documenting the care process quality measures and im-
proving patient outcomes than facilities that did not use the
measures in their practice (Wenger et al., 2009, 2010).
Although physicians have been at the forefront of
quality measure development through the AMA’s lead-
ership and the establishment of the PCPI, this example
of quality improvement can also be applied and im-
plemented by occupational therapy practitioners. Indeed,
occupational therapy practitioners in private practice who
bill Medicare are able to report these three items as part of
the PQRS (Hitchon, 2014). Furthermore, occupational
6901090010p2 January/February 2015, Volume 69, Number 1
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

therapy practitioners have participated in the fall prevention
measure development process as integral stakeholders,
have attended the AMA’s PCPI biannual meetings, and
have advocated for the linkage of process measures to
occupational therapy.
To align with the priorities of health care reform,
occupational therapy practitioners can use the six-phase
measure development methodology to define and evaluate
the value of occupational therapy services in other areas
of health care delivery. To this end, we must define our
evidence-based and patient-centered care processes to
enhance the delivery of occupational therapy services and
improve patient outcomes, thereby demonstrating the
value that the profession contributes to patient care.
Context of Health Care Reform: Attention toAcute and Postacute Care
The United States spends more than any other developed
country on health care. Unfortunately, despite outspending
other developed countries, patient outcomes in the United
States are worse than those of other countries, indicating
a need to improve the quality and efficiency of our health
care system (Davis, Schoen, & Stremikis, 2010; Honore
et al., 2011). Further, rising health care costs are exacer-
bated by an aging population that is relying on Medicare
in growing numbers, placing further financial strain on the
fee-for-service system in which volume is the key driver
instead of outcomes. For example, Medicare spending
for postacute care has more than doubled over the past
10 years, with expenditures increasing from $26.6
billion to $63.6 billion, yet patient outcomes are sub-
optimal, resulting in Medicare’s growing scrutiny of re-
habilitation quality in postacute care (Medicare Payment
Advisory Commission, 2010, 2012). Cumulatively, esca-
lating health care expenditures, gaps in quality of care, and
the exponential growth of the older adult population served
as drivers of reform in the U.S. health care system, facili-
tating the passage of the ACA.
The transition to value-based reimbursement is an
ACA initiative designed to achieve the Triple Aim. The
traditional fee-for-service model, in which payment is
based on the volume of services provided, has been as-
sociated with a financial incentive to provide more care
without improving outcomes (Schroeder & Frist, 2013).
The ACA’s emphasis on quality is facilitating a paradigm
shift that aims to incentivize the achievement of desired
outcomes by rewarding the provision of high-quality care.
Although most of the ACA’s proposals are linked to
Medicare, some efforts it fosters address multiple types of
payers. Furthermore, because Medicare is the major payer
of health care in the United States, using Medicare to test
innovations will have an impact on the larger U.S. health
care system (Boccuti & Moon, 2003; Finkelstein, 2007).
Initial value-based payment initiatives that have been
rolled out focus on reducing negative outcomes that re-
search has demonstrated are preventable, are associated
with high health care costs, and should not occur (e.g.,
hospital readmissions, hospital-acquired conditions). The
initiatives also have focused on promoting consumer
satisfaction and improving health overall. In any value-
based payment model, facility or provider payments are tied
to performance on outcomes, and the unit of analysis is the
provider (e.g., acute care hospital, individual occupational
therapy practitioner). In such a model, poor performance is
tied to financial penalties. For example, in fiscal year 2013,
2,200 acute care hospitals with excessive 30-day readmission
rates incurred a total of $280 million in penalty payments to
Medicare (Centers for Medicare & Medicaid Services, 2013;
James, 2013). Thus, this reimbursement structure provides
a strong financial incentive for providers to deliver high-
quality care, accompanied by the corresponding preferred
patient outcomes, to avoid such penalties.
Value-Based Care in the Context ofOccupational Therapy
To be responsive to the current health care reform ini-
tiatives, the field of occupational therapy needs measures
that can reliably and validly assess the quality and value of
its services across practice settings. Also, because occu-
pational therapy is now included in lump-sum facility
payments, as value-based purchasing becomes more so-
phisticated it will be important to identify, protect, and
recognize the specific contribution of occupational therapy
to facility or system outcomes (Lamb & Metzler, 2014).
Roberts and Robinson (2014) discussed the important
role occupational therapy practitioners can play in ad-
dressing readmissions and hospital-acquired conditions to
improve provider performance on these outcome measures;
the authors specifically addressed the role occupational
therapy has in improving outcomes in the area of accidental
falls. We must push forward the identity and utility of oc-
cupational therapy in all settings, however, to make sure
a link is understood and validated. One critical aspect of
ensuring the value of occupational therapy’s contribution to
optimizing outcomes is to encourage practitioners to use
evidence to inform clinical interventions. Some estimates
indicate that use of evidence in occupational therapy fall
prevention interventions is limited and that quality im-
provement initiatives are needed (Philibert, Snyder, Judd, &
Windsor, 2003; Thomas, Saroyan, & Lajoie, 2012).
The American Journal of Occupational Therapy 6901090010p3
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

As an example of quality measure development, fall
prevention is useful. Improvement initiatives addressing
falls must be multidimensional. First, we must clearly
define occupational therapy care processes in the area of
fall prevention, and then these processes must be widely
disseminated to influence practice. For instance, protocols
for patients seen in certain settings (e.g., hospital emer-
gency rooms) must be developed to enable application of
the processes identified in the evidence. Follow-up on
longer-term outcomes, such as monitoring patients who
experience a fall and receive preventive interventions, will
also be necessary to determine effectiveness. Further, docu-
mentation and reporting systems must be transformed to
ensure that clinicians consistently provide and document their
delivery of appropriate, evidence-validated fall prevention
care processes. These systems may then be used to create
a robust data set that can be examined to demonstrate oc-
cupational therapy’s distinct value in preventing falls to in-
form the broader context of health care reform.
Defining High-QualityOccupational Therapy
A growing knowledge base of clinical research trials is
providing evidence of occupational therapy’s efficacy,
but the translation of that evidence into practice must be
amplified. To align with the priorities of the ACA, we
need to ensure that the care occupational therapy prac-
titioners provide and document is grounded in evidence
and is patient centered. Moreover, we need to demon-
strate our efficacy across settings, geographic regions,
and subpopulations to establish care processes for the
specific patient populations we serve (e.g., patients with
stroke, brain injury, spinal cord injury, orthopedics). As
a profession, we need to ask, What are the essential care
processes that every occupational therapy practitioner
should provide for each patient population we serve?
For example, what are the core interventions that
constitute high-quality care to be provided across the
continuum for all patients who have experienced a hip
fracture, regardless of the setting in which they are receiving
care? This is a population at high risk for subsequent falls,
both while in rehabilitation and during the initial transition
back to the community, which can increase the risk of
hospital readmissions and long-term institutionalization
(Mahoney et al., 2000). A recent study found that occu-
pational therapy home safety assessments before commu-
nity discharge decreased 30-day hospital readmissions
(Johnston, Barras, & Grimmer-Somers, 2010). Home
safety assessments are an efficacious care process that
occupational therapy practitioners identify as being within
our scope of practice, particularly in the area of fall pre-
vention (Gillespie et al., 2012; Leland, Elliott, O’Malley,
& Murphy, 2012). An occupational therapy care process
such as “an environmental safety assessment is provided
and documented prior to community discharge” could be
proposed as a process indicator for quality measure de-
velopment using the standardized measure protocol (Min
et al., 2011; Rubenstein et al., 2004; Wenger et al., 2010).
If this process is validated as a quality measure, clinicians
could then provide and document the care process, which
would serve as a means of validating the quality of occu-
pational therapy. Longitudinal data would optimally show
that patients who received the assessment from an occu-
pational therapy practitioner did better (e.g., experienced
fewer injuries from falls), thus improving the facility’s
overall care rating and further validating occupational
therapy’s distinct value in home safety and fall prevention.
Implications for Occupational TherapyPractitioners, Educators, and Researchers
The transition to value-based care will require the partici-
pation of occupational therapy practitioners, educators, and
researchers to develop strategies that will align the practice of
occupational therapy with the Triple Aim of health care
reform. Occupational therapy researchers working together
with clinicians can enhance the translation of evidence into
practice. Furthermore, as a team, researchers and clinicians
can integrate current evidence with the pragmatics of clinical
practice to define high-quality occupational therapy practice
using the standardized quality measure development
methods of the PCPI, AHRQ, and NQF (Min et al., 2011;
Rubenstein et al., 2004; Wenger et al., 2010).
In the context of the ACA’s “meaningful use” man-
date (i.e., the “use of certified electronic health record
[EHR] technology to improve quality, safety, efficiency,
and reduce health disparities” to improve clinical out-
comes; healthIT.gov, 2014) and the emergence of EHRs,
clinicians need documentation platforms that reflect the
clinical reasoning and decision-making processes of oc-
cupational therapy practitioners. Additionally, these sys-
tems must promote documentation of the actual care
provided and the outcomes achieved. For institutions to
develop documentation systems that capture the quality
care occupational therapy practitioners define as value,we must come to consensus as a profession and com-
municate those care processes and critical elements to
the developers of the EHR platforms. Accurate docu-
mentation reflecting high-quality occupational therapy
serves as the foundation for validating the value of our
services.
6901090010p4 January/February 2015, Volume 69, Number 1
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

In the context of value-based care, clinicians need to
ensure that their documentation reflects the care they
provide, that the care is grounded in evidence, and that
they use their own data to assess the quality of their care
processes. Quality improvement in the clinical setting is
a continuous process. Clinicians and administrators need
to work collaboratively, examining practice patterns and
establishing minimum standards of practice. The ongoing
use of clinical data can identify areas in which the facility
exceeds expectations and reveal areas of care delivery that
would benefit from improvement. By taking action and
engaging in self-appraisal, we can enhance our practice,
thereby improving patient outcomes.
The demand is growing for health services research in
occupational therapy. The profession needs researchers to
use new and emerging EHR data sources to examine the
impact of occupational therapy services and build the
evidence that measures the value of our contributions
within the context of the broader health care community.
The use of Medicare administrative data, registries, and
EHRs provides opportunities for the assessment of service
delivery in the clinical setting for populations of patients,
thereby allowing us to move beyond clinical trials to
demonstrate the value of occupational therapy services on
a broader scale. For example, data from fall prevention care
process measures may demonstrate that patients who received
the fall prevention care processes during rehabilitation across
all postacute care settings while recovering from hip fracture
had lower rates of falls and hospital readmissions after dis-
charge back to the community compared with those who did
not receive high-quality care. For the profession to have the
evidence base needed to advocate for high-quality occupa-
tional therapy in the era of value-based reimbursement, we
need not only to produce more research, but also to develop
a critical mass of trained researchers who can evaluate the
quality, access, timing, and utilization of occupational therapy
services.
Each occupational therapy practitioner needs to be
accountable for the type and value of services he or she
provides to ensure optimal outcomes. Measuring and
improving the value of occupational therapy remains
a central priority of the profession (Porter, 2010). Value-
based payment has significant implications for the edu-
cation of occupational therapy practitioners. Health care
is changing so rapidly that educational programs are
challenged to prepare their students for the ever-changing
health care environment. In addition to being prepared to
engage in the evolving practice environment, students
need the skills to appraise evidence, articulate the care
they provide, document evidence-based care processes,
and examine data from clinical practice. Furthermore,
academic programs can team up with health information
technology programs to expose students to the emerging
area of electronic health and health information systems.
It will be critical to have occupational therapy–trained
people on the front lines of health information technol-
ogy, developing EHR systems that capture the quality
and value of occupational therapy.
Conclusion
As the focus in health care shifts toward supporting higher
quality, the occupational therapy profession needs to develop
quality measures that will allow practitioners to provide,
document, and evaluate our valuable contribution to optimal
patient outcomes. This paradigm shift presents an oppor-
tunity for clinicians, researchers, and educators to collabo-
ratively contribute to defining quality care measures, promote
the adoption of these standards of service, and evaluate the
delivery of care that occupational therapy provides. By using
data to reflect our contribution to improved patient outcomes
and recognizing areas for future progress, the profession will
be strengthened. s
Acknowledgments
Natalie Leland was funded during the development of
this manuscript by the National Center for Medical
Rehabilitation Research, National Institute of Child
Health and Development, and the National Institute of
Neurological Disorders and Stroke (K12 HD055929, PI
Ottenbacher).
ReferencesBattelle. (2011). Quality indicator measure development, imple-
mentation, maintenance, and retirement. Rockville, MD:Agency for Healthcare Research and Quality.
Berwick, D. M., Nolan, T. W., & Whittington, J. (2008). TheTriple Aim: Care, health, and cost. Health Affairs, 27,759–769. http://dx.doi.org/10.1377/hlthaff.27.3.759
Boccuti, C., & Moon, M. (2003). Comparing Medicare andprivate insurers: Growth rates in spending over three de-cades. Health Affairs, 22, 230–237. http://dx.doi.org/10.1377/hlthaff.22.2.230
Centers for Medicare and Medicaid Services. (2013, November18). CMS quality strategy: 2013–beyond. Washington, DC:Author. Retrieved from http://www.ahrq.gov/workingforquality/agencyplans/cms-quality-strategy.pdf
Commission on Accreditation of Rehabilitation Facilities.(2014). Standards manual for medical rehabilitation. Tuc-son, AZ: Author.
Davis, K., Schoen, C., & Stremikis, K. (2010, June). Mirror,mirror on the wall: How the performance of the U.S.health care system compares internationally. Common-wealth Fund, pp. 1–34.
The American Journal of Occupational Therapy 6901090010p5
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

Donabedian, A. (1966). Evaluating the quality of medical care.Milbank Memorial Fund Quarterly, 44, 166–206. http://dx.doi.org/10.2307/3348969
Donabedian, A. (2003). An introduction to quality assurance inhealth care. New York: Oxford University Press.
Finkelstein, A. (2007). The aggregate effects of health insur-ance: Evidence from the introduction of Medicare. Quar-terly Journal of Economics, 122, 1–37. http://dx.doi.org/10.1162/qjec.122.1.1
Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Sherrington,C., Gates, S., Clemson, L. M., & Lamb, S. E. (2012).Interventions for preventing falls in older people living inthe community. Cochrane Database of Systematic Reviews(Online), 9, CD007146. http://dx.doi.org/10.1002/14651858.CD007146.pub3
healthIT.gov. (2014, March 18). EHR incentives and certifica-tion: Meaningful use definition and objectives. RetrievedOctober 1, 2014, from http://www.healthit.gov/providers-professionals/meaningful-use-definition-objectives
Hitchon, J. (2014). AOTA guide to PQRS. Bethesda, MD:American Occupational Therapy Association. Retrievedfrom http://www.aota.org/Advocacy-Policy/Federal-Reg-Affairs/Pay/Medicare/PQRS/AOTAGuidetoPQRS.aspx
Honore, P. A., Wright, D., Berwick, D. M., Clancy, C. M., Lee,P., Nowinski, J., & Koh, H. K. (2011). Creating a frameworkfor getting quality into the public health system.Health Affairs,30, 737–745. http://dx.doi.org/10.1377/hlthaff.2011.0129
James, J. (2013, November 12). Health policy brief: MedicareHospital Readmissions Reduction Program. Health Af-fairs. Retrieved from http://healthaffairs.org/healthpolicy-briefs/brief_pdfs/healthpolicybrief_102.pdf
Johnston, K., Barras, S., & Grimmer-Somers, K. (2010). Re-lationship between pre-discharge occupational therapy homeassessment and prevalence of post-discharge falls. Journal ofEvaluation in Clinical Practice, 16, 1333–1339. http://dx.doi.org/10.1111/j.1365-2753.2009.01339.x
Joint Commission. (2014). Advanced certification: Comprehensivestroke centers. Retrieved from http://www.jointcommission.org/certification/advanced_certification_comprehensive_stroke_centers.aspx
Lamb, A. J., & Metzler, C. A. (2014). Health Policy Perspec-tives—Defining the value of occupational therapy: Ahealth policy lens on research and practice. American Jour-nal of Occupational Therapy, 68, 9–14. http://dx.doi.org/10.5014/ajot.2014.681001
Leland, N. E., Elliott, S. J., O’Malley, L., & Murphy, S. L.(2012). Occupational therapy in fall prevention: Currentevidence and future directions. American Journal ofOccupational Therapy, 66, 149–160. http://dx.doi.org/10.5014/ajot.2012.002733
Mahoney, J. E., Palta, M., Johnson, J., Jalaluddin, M., Gray,S., Park, S., & Sager, M. (2000). Temporal associationbetween hospitalization and rate of falls after discharge.Archives of Internal Medicine, 160, 2788–2795. http://dx.doi.org/10.1001/archinte.160.18.2788
Mainz, J. (2003). Defining and classifying clinical indicatorsfor quality improvement. International Journal for Qualityin Health Care, 15, 523–530. http://dx.doi.org/10.1093/intqhc/mzg081
Medicare Payment Advisory Commission. (2010). MedicarePayment Advisory Commission report to the Congress,March 2010. Journal of Pain and Palliative Care Phar-macotherapy, 24, 302–305. http://dx.doi.org/10.3109/15360288.2010.503732
Medicare Payment Advisory Commission. (2012). Health carespending and the Medicare program. Washington, DC: Au-thor. Retrieved from http://www.medpac.gov/documents/Jun12DataBookEntireReport.pdf
Min, L. C., Reuben, D. B., Adams, J., Shekelle, P. G.,Ganz, D. A., Roth, C. P., & Wenger, N. S. (2011).Does better quality of care for falls and urinary incon-tinence result in better participant-reported out-comes? Journal of the American Geriatrics Society, 59,1435–1443. http://dx.doi.org/10.1111/j.1532-5415.2011.03517.x
National Quality Forum. (2011). Measure evaluation crite-ria. Washington, DC: Author. Retrieved from http://www.qualityforum.org/docs/measure_evaluation_criteria.aspx
Patient Protection and Affordable Care Act, Pub. L. 111–148,x 3502, 124 Stat. 119, 124 (2010). Retrieved from www.healthcare.gov/law/full/index.html
Philibert, D. B., Snyder, P., Judd, D., & Windsor, M. M.(2003). Practitioners’ reading patterns, attitudes, and useof research reported in occupational therapy journals.American Journal of Occupational Therapy, 57, 450–458.http://dx.doi.org/10.5014/ajot.57.4.450
Physician Consortium for Performance Improvement. (2011).Measures Development, Methodology, and Oversight Advi-sory Committee: Recommendations to PCPI Work Groups onoutcome measures. Chicago: American Medical Association.
Porter, M. E. (2010). What is value in health care? New Eng-land Journal of Medicine, 363, 2477–2481. http://dx.doi.org/10.1056/NEJMp1011024
Roberts, P. S., & Robinson, M. R. (2014). Health PolicyPerspectives—Occupational therapy’s role in preventingacute readmissions. American Journal of OccupationalTherapy, 68, 254–259. http://dx.doi.org/10.5014/ajot.2014.683001
Rubenstein, L. Z., Solomon, D. H., Roth, C. P., Young, R. T.,Shekelle, P. G., Chang, J. T., . . . Wenger, N. S. (2004).Detection and management of falls and instability in vul-nerable elders by community physicians. Journal of theAmerican Geriatrics Society, 52, 1527–1531. http://dx.doi.org/10.1111/j.1532-5415.2004.52417.x
Schroeder, S. A., & Frist, W.; National Commission onPhysician Payment Reform. (2013). Phasing out fee-for-service payment. New England Journal of Medi-cine, 368, 2029–2032. http://dx.doi.org/10.1056/NEJMsb1302322
Thomas, A., Saroyan, A., & Lajoie, S. P. (2012). Creation ofan evidence-based practice reference model in falls preven-tion: Findings from occupational therapy. Disability andRehabilitation, 34, 311–328. http://dx.doi.org/10.3109/09638288.2011.607210
Wenger, N. S., Roth, C. P., Hall, W. J., Ganz, D. A., Snow,V., Byrkit, J., . . . Reuben, D. B. (2010). Practice redesignto improve care for falls and urinary incontinence: Primary
6901090010p6 January/February 2015, Volume 69, Number 1
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

care intervention for older patients. Archives of InternalMedicine, 170, 1765–1772. http://dx.doi.org/10.1001/archinternmed.2010.387
Wenger, N. S., Roth, C. P., Shekelle, P. G., Young, R. T.,Solomon, D. H., Kamberg, C. J., . . . Reuben, D. B.(2009). A practice-based intervention to improve primarycare for falls, urinary incontinence, and dementia. Journal
of the American Geriatrics Society, 57, 547–555. http://dx.doi.org/10.1111/j.1532-5415.2008.02128.x
Wenger, N. S., & Shekelle, P. G., & ACOVE Investigators.(2001). Assessing care of vulnerable elders: ACOVEproject overview. Annals of Internal Medicine, 135,642–646. http://dx.doi.org/10.7326/0003-4819-135-8_Part_2-200110161-00002
The American Journal of Occupational Therapy 6901090010p7
Downloaded From: http://ajot.aota.org/ on 01/27/2015 Terms of Use: http://AOTA.org/terms

HEALTH POLICY PERSPECTIVES
Defining Primary Care: Envisioning the Roles ofOccupational Therapy
Christina A. Metzler, Kimberly D. Hartmann, Lisa A. Lowenthal
KEY WORDS
� occupational therapy
� patient care management
� Patient Protection and Affordable Care
Act
� primary health care
� professional role
Metzler, C. A., Hartmann, K. D., & Lowenthal, L. A. (2012). Health Policy Perspectives—Defining primary care: Envisioning
the roles of occupational therapy. American Journal of Occupational Therapy, 66, 266–270. http://dx.doi.org/
10.5014/ajot.2010.663001
Christina A. Metzler is Chief Public Affairs Officer,
Public Affairs Division, American Occupational Therapy
Association, and Treasurer, American Occupational
Therapy Political Action Committee, Bethesda, MD;
Kimberly D. Hartmann, PhD, OTR/L, FAOTA, is
Professor and Chair of Occupational Therapy, Quinnipiac
University, Hamden, CT, and Chair, Special Interest
Section Council, American Occupational Therapy
Association; [email protected]
Lisa A. Lowenthal is an Occupational Therapy
Graduate Student, Quinnipiac University, Hamden, CT.
Primary care is a key theme in the Pa-
tient Protection and Affordable Care
Act (ACA; 2010). But what does the term
mean? Is there a difference between pri-mary care and primary health care? Does
primary care encompass occupational ther-
apy? What are the possible roles for occu-
pational therapy in primary care and in
achieving primary health care goals?
This column defines the terms, pro-
vides questions for occupational therapy
professionals to consider in connecting the
domain of practice to primary care and
primary health care, and suggests some
possible connections between the defi-
nitions and practice.
Definition of Primary Care
The ACA addresses primary care in several
ways, but the definition is usually con-
strued as limited, even as the descriptions
of what primary care should be and should
accomplish are expansive. Is this a problem
of expectations—that primary care shouldaddress a “large majority of personal health
needs” (ACA, 2010) or that it should ad-
dress a plurality of care? In defining primarycare practitioners, the ACA identifies
physicians, nurse practitioners, and physi-
cian assistants.
This definition may be a carryover
from the language that defines services
provided by community health centers
(CHCs). Occupational therapy is identi-
fied as a “supplemental service” along with
all other rehabilitative services (42 C.F.R.
x 51c.102(j)(4)); CHCs refer their clients
to other providers of rehabilitative services
because the federal funding provided to
CHCs through the Health Resources and
Services Administration is to be used only
for basic services.
In the ACA, primary care is defined
with similar constraints:
the provision of integrated, accessi-
ble health care services by clinicians
who are accountable for addressing
a large majority of personal health
care needs, developing a sustained
partnership with patients, and
practicing in the context of family
and community. (x 3502)Therefore, the exact definition of
primary care in the ACA is limited by who
can provide it (physicians and physician
extenders), but it is intended to address
most of the needs of patients over a period
of time, including family and community.
Are these contradictory requirements?
There are high expectations for pri-
mary care as expressed in a description of
supports for the primary care workforce:
The Obama Administration believes
that strengthening and growing our
primary care workforce is critical to
reforming the nation’s health care
system. Increasing access to primary
care physicians and nurses can help
prevent disease and illness and ensure
266 May/June 2012, Volume 66, Number 3
Downloaded From: http://ajot.aota.org/ on 11/17/2014 Terms of Use: http://AOTA.org/terms

all Americans—regardless of where
they live—have access to high quality
care. It can also reduce costs by in-
creasing access to preventive care.
(healthreform.gov, n.d., para. 2)
But how can primary care achieve
these lofty goals if it is not viewed more
broadly? Are there conflicting concepts in
these definitions and in the expectations? If
certain care is primary, then what is the rest
of care? Answers to these questions are
critical to ensure quality of health care. But
who will answer these questions, and when?
Can we as a profession mobilize and
promote a broader discussion of the concept
and the actualization of primary care with
occupational therapy as a critical element?
Some have indicated this as a possibility. A
rethinking of what specialist and supple-
mental services are and how they can achieve
the “triple aim” of health care may be one
avenue to promote occupational therapy.
The triple aim of health care as con-
ceived by the Institute for Healthcare Im-
provement, founded by Donald Berwick,
who served as the administrator of the
Centers for Medicare andMedicaid Services
from July 2010 toDecember 2011, provides
a link to be considered:
Improving the U.S. health care
system requires simultaneous pursuit
of three aims: improving the expe-
rience of care, improving the health
of populations, and reducing per
capita costs of health care. Pre-
conditions for this include the en-
rollment of an identified population,
a commitment to universality for its
members, and the existence of an
organization (an “integrator”) that
accepts responsibility for all three
aims for that population. The in-
tegrator’s role includes at least five
components: partnership with in-
dividuals and families, redesign of
primary care, population health man-
agement, financial management, and
macro system integration. (Berwick,
Nolan,&Whittington, 2008, p. 759)
This description of a new and more
effective health care system recognizes
primary care, but Berwick et al. (2008)
also recognized that primary care may
need to be redefined and reconceived:
We believe that any effective in-
tegrator will strengthen primary care
for the population. To accomplish
this, physicians might not be the
sole, or even the principal, providers.
Recently, physicians and other
clinicians have proposed principles
for expanding the role of primary
care under the title of the “medical
home.” This expanded role includes
establishing long-term relations be-
tweenpatients and their primary care
team; developing shared plans of
care; coordinating care, including
subspecialists and hospitals; and
providing innovative access to ser-
vices through improved scheduling,
connection to community resources,
and new means of communication
among individuals, families, and the
primary care team facilitated by a pa-
tient-controlled personalized health
record. (p. 759)
Barbara Starfield is sometimes referred
to as the “pathfinder of primary care” be-
cause of her attempts since the early 1990s to
redefine primary care (Stange, 2011,
p. 292). The four pillars of primary care she
defined continue to be cited: “first contact
care, continuity over time, comprehensive-
nesss, and coordination with other parts of
the health system underlie the practice of the
future” (Starfield, 1998, as cited inMargolius
& Bodenheimer, 2010, p. 779).
This kind of broad thinking goes be-
yond the Minute Clinic concept of readily,
easily available basic care to one that
envisions a coordinated system built on
teams of professionals with many capa-
bilities and varied scopes of practice all
focused on achieving health. This is where
occupational therapy can contribute and
enhance the approach to primary care,
helping to achieve the triple aim of ensuring
care, promoting true health, and using
resources wisely to achieve that health.
Primary Health Care andInternational Models
Although the terms primary care and pri-
mary health care are nearly identical and
influence one another, they differ in the
purpose of their service. As previously de-
scribed, primary care refers to the services
provided by physicians, nurse practi-
tioners, and physician assistants to address
diagnosis, treatment, and management of
illness. Primary health care focuses on idealcomprehensive health care that provides
preventative and curative services that in-
clude the rehabilitation professions (World
Health Organization [WHO], 1978).
Through these services, the goal is to im-
prove health—leading to a decreased occur-
rence of chronic diseases and injuries (which
may lead to hospitalizations)—and support
community development and chronic dis-
ease management (Fong, 2008; Leclair et al.,
2005).
In addition, primary health care val-
ues interprofessional collaborative practice
to improve health and access to services,
more efficiently use resources, and increase
satisfaction for clients and providers
(Fong, 2008; Fong & Siu, 2007; Leclair
et al., 2005; WHO, 2008). The nature of
the core competencies for interprofessional
collaborative practice address the critical
need for health care personnel to work to-
gether as a team to meet the current and
future demands that health care be afford-
able and high quality to meet the needs of
all people (Interprofessional Education
Collaborative Expert Panel, 2011). Thus,
interprofessional collaboration may pro-
vide one method to connect occupational
therapy to primary care to promote healthy
living in a variety of settings, such as the
workplace, the school environment, or the
home (Fong, 2008).
International efforts support the need
for primary health care. Both New Zea-
land and Manitoba, Canada, have de-
veloped charters that advocate for the need
for health promotion for all people (Leclair
et al., 2005; New Zealand Association of
Occupational Therapists, 2009). These
charters are founded on the principles from
WHO (2008), which supports putting the
public’s needs first to provide the most
comprehensive care possible. These tenets
are integral to occupational therapy. A
person is not solely his or her physical or
mental impairment; external factors and
context variables can also hinder or con-
tribute to success and quality of life.
The American Journal of Occupational Therapy 267
Downloaded From: http://ajot.aota.org/ on 11/17/2014 Terms of Use: http://AOTA.org/terms

Occupational therapists are skilled in
evaluating all factors in a client’s life,
leading to a comprehensive understanding
of the link between occupation and health.
The profession’s scope of practice goes
beyond treating illness and can be in-
corporated into promoting healthy living
and preventing disease and disability. De-
spite having the skills and knowledge nec-
essary to get involved in the field of primary
health care, there is a lack of support from
practitioners. Many occupational thera-
pists may actually feel as though they do
not have competency-based training or
knowledge readily available to provide
preventative services (Flannery & Barry,
2003; Seymour, 1999). In addition to these
internal barriers, there is a low rate of re-
ferral from professionals who are unaware
that preventative care falls under occupational
therapy’s scope of practice (Arsenault &
Swan, 2011; Flannery&Barry, 2003; Leclair
et al., 2005; Seymour, 1999).
It is essential for occupational thera-
pists to acknowledge their competency to
work in primary health care and advocate
for the incorporation of these services in
the United States to benefit the general
public. Some literature provides evidence
linking the use of occupational therapy
services in primary health care for a variety
of populations. For example, older adults in
a cost-effective program leading to im-
proved quality of life scores and a greater
prevention of functional decline tend to
have lower future health care costs (Clark
et al., 1997; Jackson, Carlson, Mandel,
Zemke, & Clark, 1998; Matuska, Giles-
Heinz, Flinn, Neighbor, & Bass-Haugen,
2003; Scott, Butin, Tewfik, Burkardt,
Mandel, & Nelson, 2001). Occupational
therapy services can also be used through
ergonomic worksite visits to address envi-
ronmental issues and by restructuring
workplace maladaptive habits to decrease
the prevalence of injuries in the workplace
and their associated costs (Franche et al.,
2004).
Hughes (2009) found that many
general practitioners felt the need for oc-
cupational therapists to be involved in the
care of their patients with chronic fatigue
syndrome or myalgic encephalomyelitis.
Because of the nature of this condition,
those affectedmay experience occupational
disruption that eventually leads to occu-
pational dysfunction. Many physicians felt
that diagnosing the condition and providing
medical management were the only areas
they had time to address. Patients concurred,
feeling that doctors did not provide sufficient
management advice or treatment strategies.
Occupational therapists can address the
psychosocial aspect, providing supportive
advice and meaningful interventions to “fa-
cilitate self-management of fatigue symp-
toms” (Hughes, 2009, p. 8).
Opportunities for OccupationalTherapy in the ACA
Are there opportunities for occupational
therapy in the system the ACA envisions?
There are, but the envelope may need to be
pushed. It is up to the profession and in-
dividual practitioners to create the research,
to advocate for the changes, and to support
what can be done by occupational therapy
within a broadened, more expansive view
of primary care and primary health care
teams.
Several forms of health system design
are supported by the ACA, such as the
medical home concept, accountable care
organizations, and other approaches. The
ACA provided more funding to establish
and support CHCs (healthcare.gov, 2011),
but as noted earlier occupational therapy is
only supplemental, not funded by the basic
grants.Most of these systems are built on the
more limited concept of primary care but
also include the previously noted concepts
of “large majority of personal health needs”
and “plurality” of care.
Section 3502 of the ACA may provide
a glimmer of hope. Grants are allowed for
states to coordinate primary, acute, behav-
ioral, and long-term supports and services for
people eligible for both Medicare and
Medicaid (Center forMedicare andMedicaid
Innovation, 2012).
For the most part, however, the ACA
seems to split care into primary and other.
The ACA continues this bifurcation by
focusing on physicians, nurse practitioners,
and physician assistants. Loan programs and
incentive payments under Medicare and
Medicaid are restricted to these practi-
tioners. Yet, the concept of a long-term
relationship that is responsible for health
care, health, and costs seems to run contrary
to parts of how primary care is defined.
Can occupational therapy overcome
these limitations and challenges? When
comparing the concept of primary care in
the ACA with some of the incentive
programs for systems to provide co-
ordinated care, one can see some overlap
and potential. The role expected of oc-
cupational therapy in this context is not
clear, but what the profession believes
about the best and most important con-
tributions it can make should be what
guides the profession’s advocacy.Wellness,
self-management, rehabilitation, screen-
ing, prevention, and patient education by
occupational therapy practitioners who are
part of the primary care team must be
included.
Implications forOccupational Therapy
There are many implications for occupa-
tional therapy in terms of developing
opportunities in primary care that advo-
cate for the profession and enable signif-
icant contributions to client health. There
are potential challenges to the profession
as well.
The challenges are clear—occupational
therapy is not listed as a primary care
provider. As with other rehabilitation ser-
vices, occupational therapy is considered
supplemental, and its roles in the ability to
procure grants or incentives programs is
unclear. Despite these challenges, the lan-
guage of the ACA does provide opportu-
nities for the profession to align with the
definitions of primary care, international
models of this alignment with primary care
do exist, and the broader definition of
primary health care does include the do-
mains of practice that are consistent with
occupational therapy. What does the pro-
fession need to do?
First, we must collaborate with each
other to become educated in the termi-
nology of primary care and to merge our
collective power to align our knowledge
and skills with that terminology and the
definitions. Second, we must strengthen
alliances with the identified primary care
practitioners (physicians, nurse practi-
tioners, and physician assistants) through
268 May/June 2012, Volume 66, Number 3
Downloaded From: http://ajot.aota.org/ on 11/17/2014 Terms of Use: http://AOTA.org/terms

interprofessional care teams and practices
to ensure the inclusion of referrals in the
processes of coordinated and integrated
care (Peranich, Reynolds, O’Brien, Bosch,
& Cranfill, 2010).
The connection of occupational ther-
apy as more than a supplemental service but
instead a key team member in ACA is clear
when we match the components of ACA to
the profession’s domain of practice. “Ad-
dress a large majority of personal health
needs” can be connected to areas of occu-
pation, including activities of daily living,
instrumental activities of daily living, rest
and sleep, education, work, play and leisure,
and social participation (American Occu-
pational Therapy Association [AOTA],
2008). The domain of practice in and of
itself meets the definition of addressing
a large majority of personal health needs.
Within these domains the roles of occupa-
tional therapy in functional mobility, life-
style adaptation, medication management,
and participation for health promotion have
been building evidence to support their ef-
ficacy in health care.
“Coordinated and integrated care”
aligns with practitioners being case manag-
ers and patient enablers in mental health,
long-term care, and acute and rehabilitation
settings. “Developing sustained relation-
ships” can become a trait of occupational
therapy in this component of the definition,
because the profession promotes functional
skills and services across all practice settings
from initial screenings to patient education
to hospital to outpatient to home and to
work or participation in leisure pursuits.
“Practice in the context of family and
community” connects to the profession’s
ability to conduct activity analyses within
the contexts of different environments that
include home and social connections as well
as the community. Programs related to
wellness and lifestyle adjustments, fall pre-
vention, and environment redesign are but
a few areas that align with this terminology.
“Whole person orientation” is em-
bedded in the occupational therapy scope
of practice and skill set. The profession’s
accreditation standards, scope of practice
and other practice and official documents,
and the Occupational Therapy PracticeFramework (AOTA, 2008) all describe our
skill set and practice in the holistic man-
agement of client factors, values, and body
structures and functions to yield a complete
client occupational profile in psychologi-
cal, social, physical, and cognitive function
as it relates to occupations.
“Chronic care coordination” connects
with occupational therapy’s involvement in
engaging the client in goal setting, which
increases participation in activities to pro-
mote well-being. The prevention of reinjury
and increasedmedical involvement is seen in
environmental and ergonomic interventions.
The use of the professional approaches to
create, maintain, modify, and prevent ad-
dresses the needs of those who have chronic
conditions for independent functioning.Not
only the language of the profession but also
its close involvement with clients meets the
definition of primary care and the purposes
of primary health care; occupational therapy
does have roles to “support health and par-
ticipation in life through engagement in oc-
cupation” (AOTA, 2008, p. 652).
Occupational therapy must also ex-
amine its literature and evidence and pro-
mote its role, showing how the triple aim can
be addressed when the profession provides
self-management to address chronic disease,
health promotion to keep older adults in-
dependent, fall prevention in the home,
participation in discharge planning from
acute care, and the integration of mental
health issues into overall care management.
These are but a few of the areas of possible
opportunity for occupational therapy.
Looking to existing models, such
Kaiser Permanente of Northern California
(Murphy, Greathouse, & Matsui, 2005)
and its triage system to refer to physical
therapy before a physician’s visit, may
provide ideas for an occupational therapy
triage focus. The University of Southern
California Health Care System’s Eisner
Family Medical System uses a broad team
concept and integrates occupational ther-
apy throughout family practice from initial
patient contacts through treatment and
management. This unleashes the power of
occupational therapy within the context of
primary care (Prestwich, 2012).
Preparing for the Future
The possibilities for occupational therapy
in primary care are endless, but the op-
portunities must be seized. Research, in-
terprofessional training and collaboration,
education and lifelong learning, and
a mindset that moves beyond the clinic
walls will carry occupational therapy into
primary care and perhaps transform pri-
mary health care into a system that
encompasses the whole person, the family,
and the community. s
References
American Occupational Therapy Association.
(2008). Occupational therapy practice
framework: Domain and process (2nd
ed.). American Journal of Occupational
Therapy, 62, 625–683. http://dx.doi.org/
10.5014/ajot.62.6.625
Arsenault, D., & Swan, H. (2011). Occupa-
tional therapists and primary health care
in New Brunswick. Retrieved from www.
gnb.ca/0053/phc/pdf/2011/sub/TheNew
BrunswickAssociationofOccupational
Therapists.pdf
Berwick,D.M.,Nolan, T.W.,&Whittington, J.
(2008). The triple aim: Care, health,
and cost.HealthAffairs, 27,759–769. http://
dx.doi.org/10.1377/hlthaff.27.3.759
Center for Medicare and Medicaid Innovation.
(2012). State demonstrations to integrate
care for dual eligible individuals. Retrieved
from www.innovations.cms.gov/initiatives/
with-states/
Clark, F., Azen, S. P., Zemke, R., Jackson, J., Carl-
son, M., Mandel, D., et al. (1997). Occupa-
tional therapy for independent-living older
adults: A randomized controlled trial. JAMA,
278, 1321–1326. http://dx.doi.org/10.1001/
jama.1997.03550160041036
Flannery, G., & Barry, M. (2003, Winter). An
exploration of occupational therapists’ per-
ceptions of health promotion. Irish Journal
of Occupational Therapy, pp. 33–41
Fong, K. (2008). Occupational therapy in pri-
mary health care: A new era for involvement
and contributions in the new health system
inHong Kong.Hong Kong Journal of Occu-
pational Therapy, 18, i–ii. http://dx.doi.
org/10.1016/S1569-1861(08)70006-8
Fong, K., & Siu, A. (2007, Winter). OT in
primary health care: A new elective subject
in the undergraduate curriculum. Impact,
pp. 1–2. Retrieved from http://158.132.
119.16/rs/main/pdf/newsletter/Impact%
28Winter08%29.pdf
Franche, R. L., Cullen, K., Clarke, J., MacEachen,
E., Frank, J., Sinclair, S., et al. (2004).Work-
place-based return-to-work interventions: A sys-
tematic reviewof thequantitativeandqualitative
The American Journal of Occupational Therapy 269
Downloaded From: http://ajot.aota.org/ on 11/17/2014 Terms of Use: http://AOTA.org/terms

literature. Toronto, ON: Institute for Work
and Health.
healthcare.gov. (2011). Community health cen-
ters and the Affordable Care Act in 2011:
Increasing access to affordable, cost effective,
high quality health care [Fact sheet]. Re-
trieved February 1, 2012, from www.
healthcare.gov/news/factsheets/2011/08/
communityhealthcenters08092011a.html
healthreform.gov. (n.d.). Creating jobs and in-
creasing the number of primary care pro-
viders [Fact sheet]. Retrieved from www.
healthreform.gov/newsroom/primarycare
workforce.html#
Hughes, J. L. (2009). Chronic fatigue syndrome
and occupational disruption in primary care:
Is there a role for occupational therapy? Brit-
ish Journal ofOccupationalTherapy, 72,2–10.
Interprofessional Education Collaborative Ex-
pert Panel. (2011).Core competencies for in-
terprofessional collaborative practice: Report of
an expert panel. Washington, DC: Author.
Jackson, J., Carlson,M.,Mandel,D., Zemke,R.,
& Clark, F. (1998). Occupation in lifestyle
redesign: The Well Elderly Study Occupa-
tional Therapy Program. American Journal
of Occupational Therapy, 52, 326–336.
http://dx.doi.org/10.5014/ajot.52.5.326
Leclair, L., Restall, G., Edwards, J., Cooper, J.,
Stern, M., Soltys, P., et al. (2005). Occu-
pational therapists in primary health care.
Retrieved from www.msot.mb.ca/occupatio-
nal_therapy_and_primary_health_care.aspx
Margolius, D., & Bodenheimer, T. (2010).
Transforming primary care: From past
practice to the practice of the future.
Health Affairs, 29, 779–784. http://dx.
doi.org/10.1377/hlthaff.2010.0045
Matuska,K.,Giles-Heinz,A.,Flinn,N.,Neighbor,
M., & Bass-Haugen, J. (2003). Outcomes of
a pilot occupational therapy wellness pro-
gram for older adults. American Journal of
Occupational Therapy, 57, 220–224. http://
dx.doi.org/10.5014/ajot.57.2.220
Murphy, B. P., Greathouse, D. G., &Matsui, I.
(2005). Primary care physical therapy prac-
tice models. Journal of Orthopaedic and
Sports PhysicalTherapy, 35,699–707. http://
dx.doi.org/10.2519/jospt.2005.2167
New Zealand Association of Occupational
Therapists. (2009). Occupational therapy
is primary health care in AOTEAROA/New
Zealand: A literature review. Retrieved from
www.nzaot.com/downloads/contribute/
OTinPHCLitReviewFINAL.pdf
Patient Protection and Affordable Care Act,
Pub. L. 111–148, x 3502, 124 Stat. 119,
124 (2010).
Peranich,L.,Reynolds,K.B.,O’Brien,S.,Bosch, J.,
& Cranfill, T. (2010). The roles of occupa-
tional therapy, physical therapy, and speech/
language pathology in primary care. Journal
for Nurse Practitioners, 6, 36–43. http://dx.
doi.org/10.1016/j.nurpra.2009.08.021
Prestwich, B. (2012, January 26). Care delivery/
primary care innovation case study. Presen-
tation at the Care Innovations Summit,
Washington, DC.
Scott, A.H., Butin,D.N.,Tewfik,D., Burkhardt,
A., Mandel, D., & Nelson, L. (2001). Oc-
cupational therapy as a means to wellness
with the elderly. Physical and Occupational
Therapy in Geriatrics, 18, 3–22. http://dx.
doi.org/10.1080/J148v18n04_02
Seymour, S. (1999). Occupational therapy and
health promotion: A focus on elderly peo-
ple. British Journal of Occupational Ther-
apy, 62, 313–317.
Stange, K. C. (2011). Barbara Starfield: Passage
of the pathfinder of primary care. Annals
of Family Medicine, 9, 292–296. http://dx.
doi.org/10.1370/afm.1293
World Health Organization. (1978). Declara-
tion of the Alma–Ata. Retrieved from
www.who.int/hpr/NPH/docs/declaration_
almaata.pdf
World Health Organization. (2008). World
Health Report 2008: Primary health care.
Retrieved from www.who.int/whr/2008/
whr08_en.pdf
270 May/June 2012, Volume 66, Number 3
Downloaded From: http://ajot.aota.org/ on 11/17/2014 Terms of Use: http://AOTA.org/terms
















![[Nuxeo World 2013] BUILDING APPLICATIONS WITH ANGULARJS - DAMIEN METZLER](https://img.pdfslide.us/doc/110x75/554a4919b4c9055a408b553f/nuxeo-world-2013-building-applications-with-angularjs-damien-metzler.jpg)