Embed Size (px)
Citation preview

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
1
CHIS 2019/2020 Marijuana and Opioid Workgroup Summary
Chair: Ying-Ying Meng, UCLA Center for Health Policy Research Attendees: Patricia Lee, DHCS; Thi Mai, DHCS; Michael Ong, UCLA Medical Center; Samantha Pellon, California Medical Association; Danielle Ramo, UCSF; Minerva Reye, DHCS; Michelle Wong, DHCS; Nicole Lordi, PHI; Royce Park, UCLA; AJ Scheitler, UCLA Note: This document refers to questions on CHIS, described in the attached tables. Recommendations Current marijuana content (Table 1) wording recommendations:
1. AC118 (marijuana and tobacco co-use) -Question should include e-cigarettes; e-cigarettes are tobacco. Add a statement to clarify this.
2. AC123 (Mode of marijuana use). Use the term vape rather than vaporize or add vape in parentheses
3. AC126 (marijuana use recommended by a doctor). Shorten question by deleting healthcare or other provider as only accredited physicians can prescribe.
Proposed additional marijuana content (Table 2)
1. Second-hand marijuana smoke exposure – location: Consider adding outdoor concerts, as a category that is separate from outdoor recreation areas. Some city ordinances are considering whether cannabis will be allowed at city organized events. These response options are not read.
2. Perception of risk or harm of cannabis use: Clarify intent of this question and modify wording. Proposed wording risk harming someone physically vs. NSDUH wording, risk harming themselves.
• Update: The intent is to ask about harm to oneself. CDPH agrees with the workgroup’s recommendation to change wording to “risk harming themselves”
3. Impaired driving: Clarify the intent of this question. If question addresses public safety, add a
question about whether the respondent was a passenger in a car with a marijuana-impaired driver. Make wording consistent with NSDUH question regarding drunk driving.
• Update: CDPH would like to keep the question as proposed. The passenger drunk driving question is not a good model for driving under the influence of marijuana. Given the complexities of marijuana use- various methods of use, the ability to use inconspicuously, non-public use, delayed effects of edibles, etc., it is less likely for a passenger to be able to accurately report riding in a car with a marijuana impaired driver. There aren’t very many good measures of driving under the influence of marijuana but feel strongly that self-report of drivers will yield more accurate responses.
• Prioritizing Marijuana questions (if limited funding, ideally keep all)
1. AC118-Marijuana/Tobacco Co-use is important. Potentially access funding from Prop 56? 2. AC119-AC125: Suggest reducing the number of questions. Consider deleting less common
CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
2
modalities or combining (e.g., combine eating and drinking).
Prioritizing Opioid questions (Table 3) 1. Cut AC130 (prescribing doctor). May not be critical to ask on CHIS, as there are other data
sources. For example, CURES database managed by the DOJ. 2. Cut AC132 (signed contract). This is ideal practice typical for management of chronic pain, but
not commonly followed. 3. Cut AC133 (reasons for prescription). It is hard to relate the conditions back to the type of
medication. Additional Domains to consider for CHIS 2019/20 (contingent on funding)
1. Marijuana and alcohol co-use. UCSF can work with CHIS to identify measures and possibly funding.
2. Cannabis marijuana cross-over use. Group members discussed a growing trend of substituting marijuana for opiate pain medication. This is a new area, though several papers were published in the past two years. Group members suggested assessing substitution among respondents who indicate opiate prescription misuse (AC129=yes). Dr. Tom Strauss, Medical Director, RNPH, UCLA may be a resource in this area. Danielle Ramo shared a recent paper, that is available here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5569620/
• Update: Potential cross-over questions were circulated to the workgroup on 5/25/2018 and are attached here. Further work on this question set is on hold pending final funding priorities.
Next Steps: 1. Royce will clarify the intent of questions regarding perception of risk of cannabis use and
impaired driving with CDPH. 2. Royce will follow-up with Tobacco Control Branch regarding the term ever in the question about
past 30-day second-hand smoke exposure. 3. Identify potential questions about marijuana and alcohol cross-over use.
Discussion summary Current Marijuana Content (Table 1) AC118 (marijuana/tobacco co-use). Danielle Ramo gave some background on the development AC118. The question was adapted from NSDUH but is not identical. The NSDUH question was modified to improve the wording for telephone administration. Danielle Ramo also noted that while the item was important, it was not a funding priority for UCSF. Dr. Michael Ong noted that AC118 is a key question and CHIS may consider accessing funding from AC118. AC123: Dr. Michael Ong commented on the term vaporize rather than the more colloquial vape. He advised changing the wording to “vape” or use “vape” in parentheses. Nicole Lordi asked about the translation of the term; perhaps CHIS could use the English term (vape) in translated questionnaires. AC126: Group discussed including or other healthcare provider. Samantha Pellon noted that only accredited physicians could prescribe marijuana. There was discussion as to whether this would change. Danielle Ramo noted the question was adapted from NSDUH 2015. Other states might allow other providers to prescribe marijuana. Proposed New Content (Table 2)

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
3
Exposure to second-hand marijuana smoke: Dr. Ong noted that this topic is relevant to smoke-free housing regulations. Second-hand smoke protections should extend to marijuana. Danielle Ramo suggested dividing the question into 2, to ask about vaping and smoking separately, as the risk is different. Dr. Ong noted that from an enforcement standpoint, smoking and vaping were the same. Thi Mai asked, why the term ever is included in the question, as the question asks about past 30-days. Royce responded that the question is an adaption of a similar question about second-hand tobacco smoke provided by the Tobacco Control Branch. He will check with them about the term ever. Location of exposure to second-hand marijuana smoke: Danielle Ramo suggested adding outdoor concerts to the location list. She noted that some city ordinances were considering banning cannabis from city organized events. Perception of risk of harm of cannabis use: Workgroup members thought the proposed question wording was unclear. Is the intent to ask about harming themselves or harming someone else? The wording used by NSDUH is recommended. Impaired driving. Workgroup members wondered why there was no question about being a passenger in a car with an impaired driver. Danielle Ramo recommended that the question be consistent with NSDUH’s questions on driving while drunk. Question priorities: Workgroup members expressed that all questions are important. AC118 (marijuana co-use with tobacco) is a high priority. The workgroup suggested reducing content by deleting or combining less common modes of marijuana use, such as drinking. Royce reviewed rough frequencies; drinking(AC122) was the least common mode. CHIS could delete AC122 or combine with AC121 (eat). Patricia Lee noted that if resources were scarce, questions do not need to be asked of all adults. Patricia Lee and Royce Park clarified that questions AC118-AC127 of marijuana users aged 18-25 years. Marijuana questions are also asked in the teen questionnaire. Ying-Ying commented that the age pattern for marijuana use might change post-legalization. Opioid (Table 3) Nicole Lordi reviewed the current opioid content, noting there was no identified funder for the questions in 2019/20. The group discussed non-critical questions. Michael Ong noted that the DOJ’s CURES dataset was another source for AC130 and AC131. He also commented that AC 133 was not particularly critical and hard to relate back to the type of medication. Samantha Pellon noted that if we were asking about doctor shopping, might consider asking about multiple pharmacies. It is not clear that use of multiple pharmacies is captured in the CURES database. Both Samantha Pellon and Michael Ong agreed that AC132 was not a high priority. Signing contract is ideal but mostly used in chronic pain management. Workgroup members commented about the absence of a question on frequency of heroin use, which was due to the need to prioritize. The use of fentanyl was raised as a topic of interest, though members agreed that is unclear whether a respondent would know if fentanyl is in their pain medications. Patricia Lee noted that the frequency for AC129 was 358. Additional Domains to consider for CHIS 2019/20 Danielle Ramo suggested adding a question of marijuana and alcohol co-use in addition to marijuana and tobacco. UCSF could support, contingent upon funding.

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
4
Marijuana and opioid cross-over use was discussed, both co-use and a growing trend of substituting marijuana for opioids. Whether this is a true substitution or co-use is unclear. The recommendation was to explore adding a question about marijuana substitution among past year opiate medication mis-users, age 18+. Danielle Ramo forwarded some literature (attached). Dr. Tom Strauss, Medical Director, RNPH, UCLA might be a resource in this domain.

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
5
Table 1. Current marijuana content, CHIS 2017/18
Question # Topic Question TEXT % of
sample Universe Source
INTRO
The next questions are about marijuana also called cannabis or weed, hashish, and other products containing THC. There are many methods for consuming these products, such as smoking, vaporizing, dabbing, eating, or drinking. (THC is the active ingredient in marijuana.)
100.0% Adults 18+ NSDUH
AC115 Marijuana ever use Have you ever, even once, tried marijuana or hashish in any form? 100.0% Adults 18+ NSDUH
AC116 Marijuana last use
How long has it been since you last used marijuana or hashish in any form? 53.3% Adults 18+,
AC115='yes' NSDUH
AC117 Marijuana recent use (<=30 days)
During the past 30 days, on how many days did you use marijuana, hashish, or another THC product? 8.8% Adult 18+,
AC116<=30 days NSDUH
AC118 Marijuana/tobacco co-use
How often have you used tobacco when you have also been using marijuana? Would you say… Usually / Sometimes / Never 4.0%
Adult 18+, AC116<=30 days; AC117>0
NSDUH (adapted)
AC119 Method: smoke
During the past 30 days, how did you use marijuana? Did you… smoke it in a joint, bong, or pipe? 4.0%
Adult 18+, AC116<=30 days; AC117>0
BRFSS

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
6
Table 1 continued
Question # Topic Question Text % of
sample Universe Source
AC120 Method: blunt
During the past 30 days, how did you use marijuana? Did you… smoke part or all of a cigar with marijuana in it, which is sometimes called a blunt?
4.0% Adult 18+, AC116<=30 days; AC117>0
NSDUH
AC121 Method: eat
During the past 30 days, how did you use marijuana? Did you… eat it? For example, in brownies, cakes, cookies or candy.
4.0% Adult 18+, AC116<=30 days; AC117>0
BRFSS
AC122 Method: drink
During the past 30 days, how did you use marijuana? Did you… drink it? For example, in tea, cola, alcohol or other drinks.
4.0% Adult 18+, AC116<=30 days; AC117>0
BRFSS
AC123 Method: vape
During the past 30 days, how did you use marijuana? Did you… vaporize it? For example, in an e-cigarette type vaporizer.
4.0% Adult 18+, AC116<=30 days; AC117>0
BRFSS
AC124 Method: dab
During the past 30 days, how did you use marijuana? Did you… dab it? For example, using butane hash oil, wax or concentrates.
4.0% Adult 18+, AC116<=30 days; AC117>0
BRFSS
AC125 Method: some other way
During the past 30 days, how did you use marijuana? Did you… use it some other way? 4.0%
Adult 18+, AC116<=30 days; AC117>0
BRFSS
AC126 Any recent marijuana use recommended by doctor
Was any of your marijuana use in the past month recommended by a doctor or other healthcare provider? 4.0%
Adult 18+, AC116<=30 days; AC117>0
UCSF
AC 127 All recent marijuana use recommended by doctor
Was all of your marijuana use in the past month recommended by a doctor or other healthcare provider? 1.5%
Adult 18+, AC116<=30 days, AC117>0; AC126='yes'
UCSF

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
7
Table 2. Proposed additional marijuana content
Topic Proposed Question Text % of Sample Universe Source
Exposure to second hand marijuana smoke past two weeks
In the past 30 days, have you ever been exposed to secondhand marijuana smoke or vapor in California? 100.0% Adults 18+
Adapted from tobacco smoking exposure questions fielded in CHIS 2017/2018
Type of Location for last secondhand smoke exposure
And, thinking of the most recent time, at what type of location did this occur? Sidewalks/ home – outdoor/ home – indoor/ shopping malls or stores/ workplace – outdoor/ workplace – indoor/ park, beach, playground, outdoor recreation area/ driving/ common area of an apartment complex, condo/ Other (specify)
4.0% Adult 18+ Screener = yes
Adapted from tobacco smoking exposure questions fielded in CHIS 2017/2018
Perception of risk or harm of cannabis use
How much do you think daily or almost daily marijuana use would risk harming someone physically or in other ways? Daily or almost daily marijuana use is use on 20 or more days in the past 30 days. No risk / Slight risk / Moderate risk / Great Risk NSDUH asks: How much do people risk harming themselves physically and in other ways when they smoke marijuana once a month / twice a week
100.0% Adult 18+
Impaired driving
During the past 30 days, how many times have you driven a vehicle while you were under the influence of marijuana? NSDUH asks: During the past 12 months, have you driven a vehicle while you were under the influence of marijuana?
4.0% Adult 18+, AC116<=30 days; AC117>0

CHIS 2019/2020 Marijuana and Opioid Workgroup Summary Notes 5/10/2018 (updated 7/6/2018)
8
Table 3. Current opioid content, CHIS 2017/18
Question # Topic Question Text % of
sample Universe Source
AC128 Ever heroin, past 12 months
Have you used heroin in the past 12 months? 100.0% Adult 18+ NSDUH
AC129 Used pain killer in way not prescribed, past 12 months
In the past 12 months, did you use any prescription painkiller in a way that did not follow your doctor’s directions? Examples include Vicodin, OxyContin, Norco, Hydrocodone, Percocet and Methadone.
100.0% Adult 18+ NSDUH
AC130 # of prescription painkillers How many of these prescription painkillers are you taking? 1.7% Adult 18+
AC129 = Yes New
AC131 # prescribing doctors
Did you get the prescription(s) from one doctor or from more than one doctor? 1.7% Adult 18+
AC129 = Yes New
AC132 Signed contract with doctor
Did you sign a contract with your doctor regarding these medicines? 1.7% Adult 18+ AC129 = Yes New
AC133 Reason for prescription
What condition or conditions are you taking the medicine for? Check all that apply. Dental work/dental pain/ Surgery, not accident related/ Recent injury/ Chronic pain, regardless of cause/ Other (Specify)
1.7% Adult 18+ AC129 = Yes New

CHIS 2019/2020 Marijuana Opioid Workgroup Marijuana Opioid Cross Over Content
Item # Question Text Question Responses Universe
1 Have you ever taken opiate pain medications together with cannabis?
YesNo
Adults who answer yes to AC129 (have used opiate pain medication in way not instructed by doctor, past 12 months)
2
When I use cannabis, I am able to decrease my opiate pain medication use.
Strongly agreeAgreeDisagreeStrongly disagree Adults who have used opiate medication &
marijuana together
3
When I use cannabis by itself it produces the same pain relief as the opiate pain medications I amtaking or have taken previously.
Strongly agreeAgreeDisagreeStrongly disagree Adults who have used opiate medication &
marijuana together
4
I prefer cannabis to the opiate pain medications I am taking or have previously taken.
Strongly agreeAgreeDisagreeStrongly disagree Adults who have used opiate medication &
marijuana together
5 If cannabis were more available (i.e., legalized, accepted, easier to access), I would use it in place of the opiate pain medications I am taking.
Strongly agreeAgreeDisagreeStrongly disagree Adults who have used opiate medication &
marijuana together
ALT2
How has your opioid prescription drug use changed since you started using cannabis?
IncreasedDecreasedThe same
Alternative to Item 2

ORIGINAL RESEARCH Open Access
Cannabis as a Substitute for Opioid-Based Pain Medication:Patient Self-ReportAmanda Reiman,1,* Mark Welty,2 and Perry Solomon3
AbstractIntroduction: Prescription drug overdoses are the leading cause of accidental death in the United States. Alter-natives to opioids for the treatment of pain are necessary to address this issue. Cannabis can be an effective treat-ment for pain, greatly reduces the chance of dependence, and eliminates the risk of fatal overdose compared toopioid-based medications. Medical cannabis patients report that cannabis is just as effective, if not more, thanopioid-based medications for pain.Materials and Methods: The current study examined the use of cannabis as a substitute for opioid-based painmedication by collecting survey data from 2897 medical cannabis patients.Discussion: Thirty-four percent of the sample reported using opioid-based pain medication in the past 6months. Respondents overwhelmingly reported that cannabis provided relief on par with their other medica-tions, but without the unwanted side effects. Ninety-seven percent of the sample ‘‘strongly agreed/agreed’’that they are able to decrease the amount of opiates they consume when they also use cannabis, and 81%‘‘strongly agreed/agreed’’ that taking cannabis by itself was more effective at treating their condition than takingcannabis with opioids. Results were similar for those using cannabis with nonopioid-based pain medications.Conclusion: Future research should track clinical outcomes where cannabis is offered as a viable substitute for paintreatment and examine the outcomes of using cannabis as a medication assisted treatment for opioid dependence.
Keywords: opiates; pain; harm reduction; substitution; opioids; cannabis
IntroductionThe Centers for Disease Control (CDC) and Preven-tion report that ‘‘[o]pioids (including prescriptionopioid pain relievers and heroin) killed more than28,000 people in 2014, more than any year on record.’’Unfortunately, this statistic has done little to curb theprescribing and consumption patterns for prescriptionopioids. The CDC estimates that, ‘‘since 1999, the amountof prescription opioids sold in the United States nearlyquadrupled, yet there has not been an overall change inthe amount of pain that Americans report. Deaths fromprescription opioids—drugs like oxycodone, hydroco-done, and methadone—have also quadrupled since
1999.’’1 Interestingly, Bachhuber et al. found that stateswith medical cannabis laws had significantly lower state-level opioid overdose mortality rates.2 Similarly, Bradfordand Bradford evaluated data on all prescriptions filled byMedicare Part D patients from 2010 to 2013 and foundthat the use of prescription drugs for which cannabiscould serve as a clinical alternative fell significantly, oncea state medical cannabis law was implemented. Theyfound that implementing an effective medical cannabislaw led to a reduction of 1826 daily doses for opioidpain relief filled per physician per year.3
Patients who suffer with pain continue to use opioidsfor chronic pain conditions despite their limited long-
1School of Social Welfare, University of California, Berkeley, Berkeley, California.2School of Lifespan Development and Educational Services, Kent State University, Kent, Ohio.3Chief Medical Officer, HelloMD, San Francisco, California.
*Address correspondence to: Amanda Reiman, PhD, MSW, School of Social Welfare, University of California, Berkeley, 120 Haviland Hall, Berkeley, CA 94720, E-mail:[email protected]
ª Amanda Reiman et al. 2017; Published by Mary Ann Liebert, Inc. This is an Open Access article distributed under the terms of the Creative CommonsAttribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cannabis and Cannabinoid ResearchVolume 2.1, 2017DOI: 10.1089/can.2017.0012
Cannabis and
Cannabinoid Research
160

term efficacy. The management of chronic pain impacts11.2% of adults in the United States with about 3% to 4%of these patients receiving long-term opioid therapy.4
This translates to *100 million Americans and incurscosts of up to $635 billion dollars per year.5 Long-termopioid therapy is associated with a number of risks, in-cluding opioid use disorder, overdose, and death. In2012 the National Institute of Drug Abuse estimatedthat there were *2.1 million people in the United Statessuffering from substance use disorders related to pre-scription opioid pain relievers and another half millionaddicted to heroin.6
Used in combination with opioid pain medications,cannabis can lower opioid side effects, cravings, andwithdrawal severity, as well as enhance the analgesiceffects of opioids, thereby allowing for lower dosesand less risk of overdose.7,8 A previous study reportedthat their subjects’ pain ‘‘was significantly decreasedafter the addition of vaporized cannabis’’ and suggestedthat cannabis treatment ‘‘may allow for opioid treat-ment at lower doses with fewer [patient] side effects.’’The authors concluded that their results ‘‘demonstratethat inhaled cannabis safely augments the analgesic ef-fects of opioids.’’9 Research published last year foundthat 80% of medical cannabis users reported substitut-ing cannabis for prescribed medications, particularlyamong patients with pain-related conditions.8
In an 1889 seminal article published in The Lancet,Dr. Edward A. Birch writes about his tremendous suc-cess in using cannabis to help patients who had becomeaddicted to pain medications, including opioids. Hewrote, ‘‘I prescribed the cannabis simply with a view toutilizing a well-known remedy for insomnia, but it didmuch more than procure sleep. I think it will be foundthat there need be no fear of peremptorily withdrawingthe deleterious drug, if hemp be employed.’’ (p. 625).10
Birch’s comments from 127 years ago predicted whatwe know to be true today, despite some controversythat continues to surround the topic of cannabis as med-icine. Numerous scholarly studies have demonstratedthe efficacy of cannabis for multiple conditions, includ-ing the management of pain, while concurrently reduc-ing the reliance on opioid medications and nonopioidmedications.5 In a 2010 pain study conducted in Can-ada, Ware et al. found that ‘‘a single inhalation of25 mg of 9.4% tetrahydrocannabinol herbal cannabisthree times daily for five days reduced the intensity ofpain, improved sleep, and was well tolerated.’’11
While the use of cannabis to treat pain is becomingmore accepted in the United States, the Schedule I status
of cannabis has made it difficult to conduct large-scaleclinical trials on its efficacy. Recent clinical and system-atic reviews have acknowledged the promise that canna-bis might hold as a standardized pain treatment, whilerecognizing the limitations that come from small samplesizes and lack on controlled studies. While these reviewsshow moderate evidence for cannabis as a treatment forpain-related conditions, they also call for additional re-search in the form of standardized clinical trials.12,13
Meanwhile, in parallel, medical cannabis patients arereporting the use of cannabis to treat their pain in lieuof or in conjunction with opioid-based pain medications.
The act of substituting cannabis for opioids has alsobeen documented in several studies of medical cannabispatients. Consistently, these studies saw substitution ratesfor prescription drugs over 50%, with less side effectsfrom cannabis being a top reason for substitution acrossstudies.14–16 Given the efficacy data on how cannabis as-sists patients’ management of pain, while also mitigatingthe risks associated with long-term opioid therapy, thepresent study uses data gathered directly from the im-pressions of patients who have used cannabis. Patientswere provided an opportunity to comment on how can-nabis compared with their use of opioid and nonopioid-based pain medication for the treatment of pain.
Materials and MethodsThis study utilized a cross-sectional survey to gatherdata about the use of cannabis as a substitute for opioidand nonopioid-based pain medication. This study wasapproved by the IRB at the University of California,Berkeley (Protocol No. 2016-08-9044). Drs. Welty andReiman did not receive compensation from HelloMDto complete the study.
InstrumentThe survey instrument (see Supplementary AppendixSA1 for a copy of the instrument) used for this studywas a modified version of the survey used in the TilrayObservational Patient Survey (TOPS). The survey forthis study included questions about demographic charac-teristics, conditions for which cannabis is used, and pre-ferred method of cannabis ingestion. Participants werethen asked about their use of cannabis as a substitutefor opioid and nonopioid-based pain medication to createsubsets of respondents who were engaging in substitution.An affirmative answer led participants to the sections thatasked about their experiences using cannabis as a substi-tute. Questions in this section asked about perceived effi-cacy of cannabis compared to their other medications,
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
161

perceived comparability of unwanted side effects, andhow the stigma around cannabis impacts their decisionto use it as a substitute.
SamplingThe survey was administered through e-mail to a data-base of 67,422 medical cannabis patients in the state ofCalifornia using the HelloMD patient database. HelloMDis a digital cannabis health and wellness platform that alsoprovides Telehealth evaluations for medical cannabis rec-ommendations to patients in California. The members ofthe database received an invitation e-mail describing thestudy and the survey, along with a link to the survey.After clicking the link, respondents were taken to theQualtrics survey site where they could complete the sur-vey confidentially. A reminder e-mail with the link to thesurvey was sent out 2 weeks after the initial invitationwas sent. The survey was closed 4 weeks after the re-minder e-mail was sent. As an incentive for participating,upon completion of the survey, respondents were asked ifthey would like to enter a raffle for one of five Firefly va-porizers. If they wished to enter, they clicked on a linkthat directed them to a form where they could entertheir name and e-mail address. At the completion ofthe sampling, five respondents were selected at randomand awarded the vaporizer.
ResultsDemographicsOf the 2897 participants, 55% were male. Eleven respon-dents identified as trans males and one identified as atrans female. Fifty-three percent of the sample was be-tween the ages of 20 and 39, 29% being over the age of50, and 15% over the age of 60. Sixty-four percent identi-fied as White, 14% Latino(a), and 7% African American.Most patients had some college education or completedcollege (71%) with 14% having completed postgraduatework. There were some significant differences betweenthe general sample and those reporting past 6 monthuse of opioid and nonopioid-based pain medications.Whites were significantly more likely to report past 6month use of both types of pain medication ( p < 0.001).Age was also significantly related to past 6 month useof these medications ( p < 0.001). Other significant deter-minants were being a woman ( p < 0.001) and having apain condition ( p < 0.001) (Table 1).
Condition and cannabis usePain was the most common condition for which respon-dents reported using cannabis with 16% reporting that as
their primary condition. However, when accounting forall pain-related conditions (menstrual cramps, fibro-myalgia, back pain and arthritis, etc.) that rises to 63%.Common mental health conditions for which respon-dents used cannabis included anxiety (13%), insomnia(9%), and depression (5%) (Fig. 1). Smoking was themost common method of ingestion with 50% of the sam-ple reporting using cannabis in that way. Thirty-one per-cent report vaporizing their cannabis, and 10% useedibles. Three percent reported that they do not cur-rently use medical cannabis.
Cannabis and opioidsThirty percent of the sample (N = 841) reported usingan opioid-based pain medication currently or in thepast 6 months. Of those who have used opioids, 61%reported using them with cannabis. Ninety-seven per-cent of the sample ‘‘strongly agreed/agreed’’ that theyare able to decrease the amount of opioids they con-sume when they also use cannabis. In addition, 89%‘‘strongly agreed/agreed’’ that taking opioids producesunwanted side effects such as constipation and nausea.Ninety-two percent of the sample ‘‘strongly agreed/agreed’’ that cannabis has more tolerable side effectsthan the opioid-based medications they have taken.Eighty-one percent ‘‘strongly agreed/agreed’’ that takingcannabis by itself was more effective at treating theircondition than taking cannabis with opioids. Whenasked if cannabis produces the same amount of painrelief as their opioid-based medications, 71% ‘‘stronglyagreed/agreed’’ with that fact. Ninety-two percent ofthe sample ‘‘strongly agreed/agreed’’ that they prefercannabis to opioids for the treatment of their conditionand 93% ‘‘strongly agreed/agreed’’ that they would be
Table 1. Sample Demographics
N (%)
Male 1593 (55)20–29 898 (31)30–39 666 (23)40–49 406 (14)50–59 406 (14)60 + 435 (15)
White (not Hispanic) 1854 (64)Hispanic/Latino(a) 406 (14)African American 203 (7)Asian 145 (5)Pacific Islander 29 (1)American Indian 58 (2)Other ethnicity 203 (7)High school 435 (15)Some college 1130 (39)College graduate 927 (32)Graduate school 406 (14)
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
162

FIG
.1.
Prim
ary
cond
ition
s.
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
163

more likely to choose cannabis to treat their condition ifit were more readily available (Fig. 2).
Cannabis and nonopioid-based medicationsSixty-four percent of the sample (N = 1751) reported tak-ing a nonopioid-based pain medication (e.g., Tylenol) fortheir condition currently or in the past 6 months. Seventy-six percent of the sample reported taking a nonopioid-based pain medication along with cannabis currentlyor in the past 6 months. Ninety-six percent ‘‘stronglyagreed/agreed’’ that they do not need to take as muchof their nonopioid-based pain medication when theyuse cannabis and 92% ‘‘strongly agreed/agreed’’ that can-nabis works better for their condition than a nonopioid-based pain medication.
As for preferring cannabis over nonopioid painmedication, 95% ‘‘strongly agreed/agreed’’ with thisstatement.
Similarly to the opioid pain medication group, 93%reported that they would be more likely to use cannabisas a substitute if it were more readily available and eas-ier to access (Fig. 3).
DiscussionSupporting the results of previous research, this studycan conclude that medical cannabis patients reportsuccessfully using cannabis along with or as a substi-
tute for opioid-based pain medication. Echoing theresults of Ware et al. and Abrams et al., patients inthis study who are using cannabis and opioids reportthat they are able to use less opioids and that cannabispresents less unwanted side effects than their opioid-based medication.9,11 In addition, 80% of patientsreported that cannabis by itself was more effectivethan their opioids. It is possible that the variabilityof individual endocannabinoid and endo-opioid sys-tems results in varying levels of efficacy between thetwo treatments. For example, a recent review releasedby the National Academy of Sciences reports conclu-sive evidence cannabis’ efficacy in treating chronicpain, but localized versus neuropathic pain might de-mand different approaches.17 Cannabis has beenfound to be very useful in treating neuropathic painspecifically.11
This study found a similar pattern of results whenlooking at substituting cannabis for nonopioid-basedpain medication like Tylenol and Advil. Researchsuggests that long-term use of these remedies mightlead to organ damage.18 With cannabis not only be-coming more accepted in the mainstream but alsocoming in a variety of preparations, some of whichare nonintoxicating, more people are looking at can-nabis as a viable treatment for everyday ailmentssuch as muscle soreness and inflammation. The
FIG. 2. Use of cannabis as a substitute/in conjunction with opioid-based pain medication (n = 828).
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
164

results of this study support that not only is this prac-tice common but also medical cannabis patients whochoose to use cannabis as a substitute for these med-icines report better outcomes with fewer unwantedside effects with cannabis compared to their othermedications.
Participants in this study overwhelmingly supportedthe notion that they would be more likely to use cannabisas a substitute for pain medication if it were less stigma-tized and more available, suggesting that there are pop-ulations of people who could benefit from this practicebut are shying away due to the stigma and legal restric-tions related to cannabis use. If cannabis laws continue tochange across the country, it will be important to assesshow changes in these laws might impact other publichealth behaviors and outcomes, such as opioid overdose,dependence, risky behaviors, and spending on prescrip-tion medications.
LimitationsThis is a study of patient self-report through online survey.The data for analyses are based on patient perception andnot on objective measure of cannabis and opioid use. Fur-thermore, there is no comparison group of pain patientswho only have access to opioid-based medications or in-dividuals solely using over-the-counter medications forpain. Finally, the solicitation e-mail sent to potential par-ticipants included the title of the study which relates to
cannabis use for pain. This may have biased the respon-dents toward those using for pain versus other conditions.
Response rateThe survey yielded responses from 2897 participants,which is a response rate of 4.3%. Since the surveywas sent to the HelloMD total patient database, includ-ing those not using cannabis for pain, this could reflectin the response rate. Other reasons for nonresponse,besides lack of interest, include people who are no lon-ger patients and those who chose not to participate forother reasons such as privacy concerns.
Amount of cannabis consumedOne of the major limitations of cannabis research is thedifficulty in determining how much cannabis partici-pants are using. Variations in strength of product,size of vessel, and social use patterns all impact the re-liability and validity of consumption measures. Thissurvey did not ask participants to estimate their amountof consumption and therefore cannot comment onreported effective doses.
Prescription status of opioidsThis study did not ask participants if the opioids they con-sumed were from a prescription or by self-medication.The study also did not inquire as to the specific typesof opioids being consumed.
FIG. 3. Use of cannabis as a substitute/in conjunction with nonopioid based medication (n = 1684).
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
165

ConclusionsThe results of this study provide implications from botha micro and macro level. First, from the macro level,there have been three previously published indicatorsof public health changes in states that permit medicalcannabis: decreases in opioid related mortality, de-creases in spending on opioids, and a decrease in trafficfatalities.2,3,19 While none of these studies shows a causeand effect relationship, they do suggest public health re-lated population based changes in localities where can-nabis can be accessed to treat pain. Given that theparticipants in this study reported a greater likelihoodof using cannabis as a substitute in a less stigmatizedand easily accessible environment, it makes sense whywe would see these changes in locations where medicalcannabis is sanctioned versus places where it is illegal.
At the micro level, there is a great deal of individualrisk associated with prolonged use of opioids and per-haps even nonopioid-based pain medications. The pre-scribing of opioids has not been curbed in the UnitedStates, despite the growing number of fatal overdosesand reported dependence. Providing the patient withthe option of cannabis as a method of pain treatmentalongside the option of opioids might assist with painrelief in a safer environment with less risk. A societywith less opioid dependent people will result in fewerpublic health harms.
Author Disclosure StatementNo competing financial interests exist.
References1. Centers for Disease Control. Injury prevention and control: opioid over-
dose. www.cdc.gov/drugoverdose/epidemic (Accessed February 1, 2017).2. Bachhuber MA, Saloner B, Cunningham CO, et al. Medical cannabis
laws and opioid analgesic overdose mortality in the United States,1999–2010. JAMA. 2014;174:1668–1673.
3. Bradford AC, Bradford WD. Medical cannabis laws reduce prescriptionmedication use in Medicare Part D. Health Aff. 2016;35:1230–1236.
4. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioidsfor chronic pain—United States, 2016. JAMA. 2016;315:1624–1645.
5. Boehnke KF, Litinas E, Clauw DJ. Medical cannabis associated with de-creased opiate medication use in retrospective cross-sectional survey ofchronic pain patients. J Pain. 2016; DOI: 10.1016/j.jpain.2016.03.002.
6. Volkow ND. America’s addiction to opioids: heroin and prescription drugabuse. 2014. www.drugabuse.gov/about-nida/legislative-activities/
testimony-to-congress/2016/americas-addiction-to-opioids-heroin-prescription-drug-abuse (last accessed March 27, 2017).
7. Degenhardt L, Lintzeris N, Campbell G, et al. Experience of adjunctivemarijuana use for chronic non-cancer pain: findings from the Pain andOpioids IN Treatment (POINT) study. Drug Alcohol Depend. 2015;147:44–150.
8. Haroutounian S, Ratz Y, Ginosar Y, et al. The effect of medicinal marijuanaon pain and quality of life outcomes in chronic pain: a prospectiveopen-label study. Clin J Pain. 2016;32:1036–1043.
9. Abrams D, et al. Cannabinoid-opioid interaction in chronic pain. ClinPharmacol Ther. 2011;90:844–851.
10. Birch EA. The use of Indian hemp in the treatment of chronic chloral andchronic opium poisoning. Lancet. 1889;625.
11. Ware MA, Wang T, Shapiro S, et al. Smoked cannabis for chronic neuro-pathic pain: a randomized controlled trial. CMAJ. 2010;182:E694–E701.
12. Hill K. Medical marijuana for the treatment of chronic pain and othermedical and psychiatric problems: a clinical review. JAMA.2015;313:2474–2483.
13. Whiting P, Wolff R, Deshpande S, et al. Cannabinoids for medical use: asystematic review and meta-analysis. JAMA. 2015;313:2456–2473.
14. Reiman A. Cannabis as a substitute for alcohol and other drugs. HarmReduct J. 2009;6:35.
15. Lucas P. Cannabis as an adjunct to or substitute for opioids in the treat-ment of chronic pain. J Psychoactive Drugs. 2012;44:125–133.
16. Lucas P, Reiman A, Earleywine M. Cannabis as a substitute for alcohol andother drugs: a dispensary-based survey of substitution effect in Canadianmedical cannabis patients. Addict Res Theory. 2013; DOI: 10.3109/16066359.2012.7334.
17. Institute of Medicine. The health effects of cannabis and cannabinoids:the current state of evidence and recommendations for research.National Academies Press, 2017. www.nap.edu/24625 (last accessedMarch 27, 2017).
18. Food and Drug Administration. Acetaminophen and liver damage: Q andA for consumers. 2017. www.fda.gov/ForConsumers/ConsumerUpdates/ucm168830.htm (last accessed March 27, 2017).
19. Santaella Tenorio J, Mauro C, Wall M, et al. US traffic fatalities, 1985–2014,and their relationship to medical marijuana laws. Am J Public Health.2016;107:336–342.
Cite this article as: Reiman A, Welty M, Solomon P (2017) Cannabis asa substitute for opioid-based pain medication: patient self-report,Cannabis and Cannabinoid Research 2:1, 160–166, DOI: 10.1089/can.2017.0012.
Abbreviations UsedCDC¼Centers for Disease Control
TOPS¼ Tilray Observational Patient Survey
Publish in Cannabis and Cannabinoid Research
- Immediate, unrestricted online access- Rigorous peer review- Compliance with open access mandates- Authors retain copyright- Highly indexed- Targeted email marketing
liebertpub.com/can
Reiman, et al.; Cannabis and Cannabinoid Research 2017, 2.1http://online.liebertpub.com/doi/10.1089/can.2017.0012
166

Cannabis and Pain Medication Substitution Questionnaire
A. Demographic Information A1. Gender: (circle one) Cis male Cis female Trans male Trans female A2. Age: A3. Race: (circle all that apply) White, not Hispanic Hispanic or Latino African American, not Hispanic Asian, not Hispanic Pacific Islander, not Hispanic Filipino, not Hispanic American Indian or Alaska Native, not Hispanic If other please specify ______________________ A4. What is the highest level of education you have completed? (Circle one) Graduated from High School/GED Some level of college Graduated college Completed graduate school
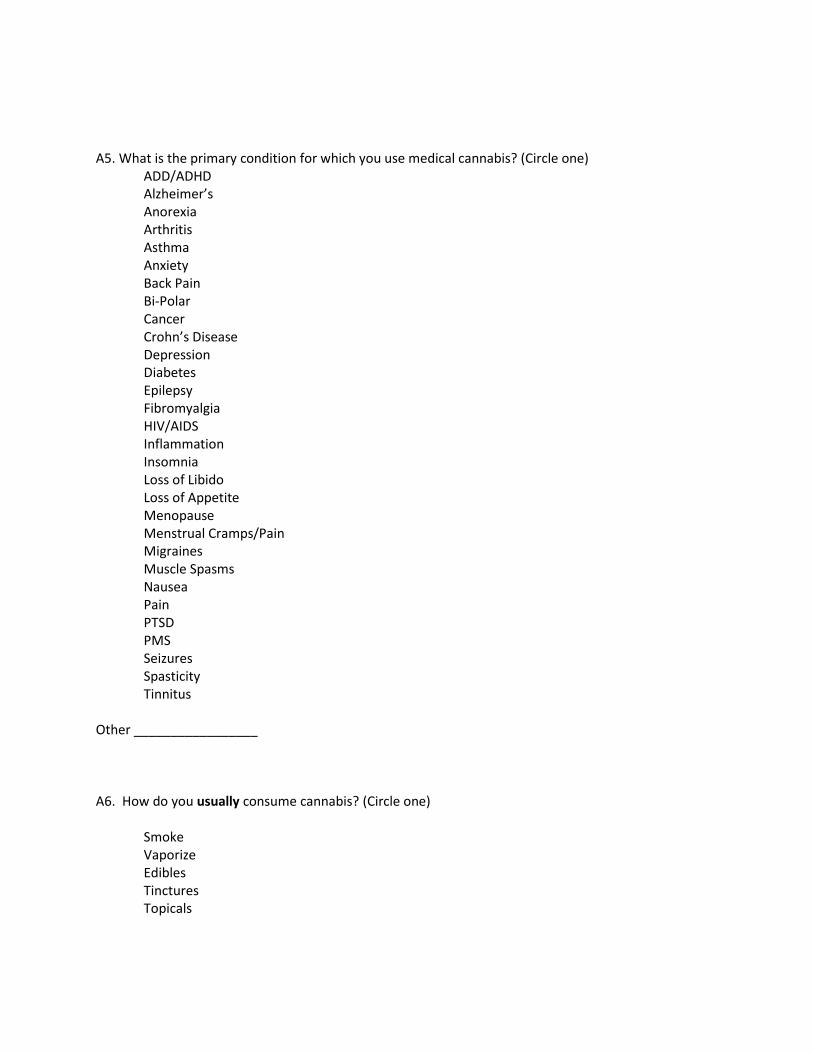
A5. What is the primary condition for which you use medical cannabis? (Circle one) ADD/ADHD Alzheimer’s Anorexia Arthritis Asthma Anxiety Back Pain Bi-Polar Cancer Crohn’s Disease Depression Diabetes Epilepsy Fibromyalgia HIV/AIDS Inflammation Insomnia Loss of Libido Loss of Appetite Menopause Menstrual Cramps/Pain Migraines Muscle Spasms Nausea Pain PTSD PMS Seizures Spasticity Tinnitus Other _________________ A6. How do you usually consume cannabis? (Circle one) Smoke Vaporize Edibles Tinctures Topicals

B. Use of other medications besides cannabis for your medical condition
B1. Are you currently, or within the past 6 months, taken Opiate pain medication (i.e., codeine, vicodin,
oxycontin, etc.) for your medical condition?
Y/N (if no skips section C)
B2. Are you currently, or within the past 6 months, taken a non-opiate pain medication (i.e. Tylenol,
Advil, Ibuprofen, etc.) for your medical condition?
Y/N (if no skips section D)
C. Opiate Pain Medication Questions
C1. Have you ever taken opiate pain medications together with cannabis?
Y/N (if no, skip to C3)
C2. When I use cannabis, I am able to decrease my opiate pain medication use.
Strongly agree
Agree
Disagree
Strongly disagree
C3. I have experienced side effects when taking my opiate medication by itself, such as sedation, dizziness, nausea, vomiting, or constipation.
Strongly Agree
Agree
Disagree
Strongly disagree

C4. Cannabis has more tolerable side effects, such as sedation or dizziness, than the opiate pain
medication I am taking or have taken.
Strongly Agree
Agree
Disagree
Strongly disagree
C5. When I use cannabis by itself it is more effective for relieving pain than the opiate pain medications I
am taking or have taken previously.
Strongly Agree
Agree
Disagree
Strongly disagree
C6. When I use cannabis by itself it produces the same pain relief as the opiate pain medications I am
taking or have taken previously.
Strongly Agree
Agree
Disagree
Strongly disagree
C7. I prefer cannabis to the opiate pain medications I am taking or have previously taken.
Strongly Agree
Agree
Disagree
Strongly disagree

C8. If cannabis were more available (i.e., legalized, accepted, easier to access), I would use it in place of
the opiate pain medications I am taking.
Strongly Agree
Agree
Disagree
Strongly Disagree
D. Non-Opiate Pain Medication Questions
D1. Have you ever taken non-opiate pain medications together with cannabis?
Y/N (If no, skip to D3)
D2. Cannabis works well with the non-opiate pain medications I am taking.
Strongly agree
Agree
Disagree
Strongly Disagree
D3. When I use cannabis, I don’t need to use as much of my non-opiate pain medication (s).
Strongly agree
Agree
Disagree
Strongly Disagree

D4. Cannabis is more effective for relieving pain than the non-opiate pain medications I take or have
previously taken.
Strongly Agree
Agree
Disagree
Strongly Disagree
D5. I prefer cannabis to the non-opiate pain medications I am taking or have previously taken.
Strongly Agree
Agree
Disagree
Strongly Disagree
D6. If cannabis were more available (i.e., legalized, accepted, easier to access), I would use it in place of
the non-opiate pain medications I am taking.
Strongly Agree
Agree
Disagree
Strongly Disagree





























