Embed Size (px)
Citation preview

CHILD MALTREATMENTCHILD MALTREATMENT
Suspected Child Abuse and Neglect (SCAN) Program
The Hospital for Sick Children

Presentation OutlinePresentation Outline
Types of child maltreatment - photographs Legislation - duty to report Case studies & discussion

THE SCAN TEAMTHE SCAN TEAM
Physicians, nurse practitioner, social workers, psychologist, nurses
medical evaluation of cases of suspected child physical abuse, sexual abuse, neglect
available 24h for consultation at 813-7500, ask for SCAN clinician on call

PHYSICAL ABUSEPHYSICAL ABUSE
Bruising/skin markings Burns Fractures Head injuries
BRUISING:BRUISING:
caused by trauma to the skin leading to leakage of blood into the tissues
areas where skin lies close to underlying bone with little soft tissue underneath bruise more easily i.e. forehead, shins
areas which have more soft tissue to act as a cushion bruise less readily i.e. cheeks, buttocks

Bruising - Bruising - red flagsred flags
age/developmental level: bruising in nonambulatory children (i.e. infants before they are able to crawl) is unusual
location: accidental bruising in ambulatory children is less common in well-cushioned areas i.e. cheeks, buttocks, back of body
pattern: object outlines i.e. loop marks, handprints, usually indicate inflicted injury
BurnsBurns
scald burns - hot liquids
spill/splash
contact
immersion contact burns - hot solids flame burns
resulting injury depends on:
mechanism of burn
temperature
duration of exposure
presence of clothing
Burns - Burns - red flagsred flags
age/developmental stage - contact burns unusual in infants before they are able to crawl
location - buttocks and feet in stocking distribution may indicate forced immersion
pattern - immersion burns have uniform depth, sharply demarcated edges, no splash marks; cigarette burns are round, uniform depth, 8-10mm

FracturesFractures
common manifestation of child abuse may be found incidentally on X-rays done
for another reason majority of nonaccidental fractures occur in
children under 18 months old, few accidental fractures in this age group

Fractures - Fractures - red flagsred flags
age/developmental level - fractures in nonambulatory children are unusual
location - metaphyseal, ribs, scapula, vertebrae, sternum highly suggestive of NAI
pattern - i.e. multiple fractures, complex skull fractures may suggest NAI
age of injury - delay in seeking medical attention, fractures of different ages
Rib fractures in infantsRib fractures in infants
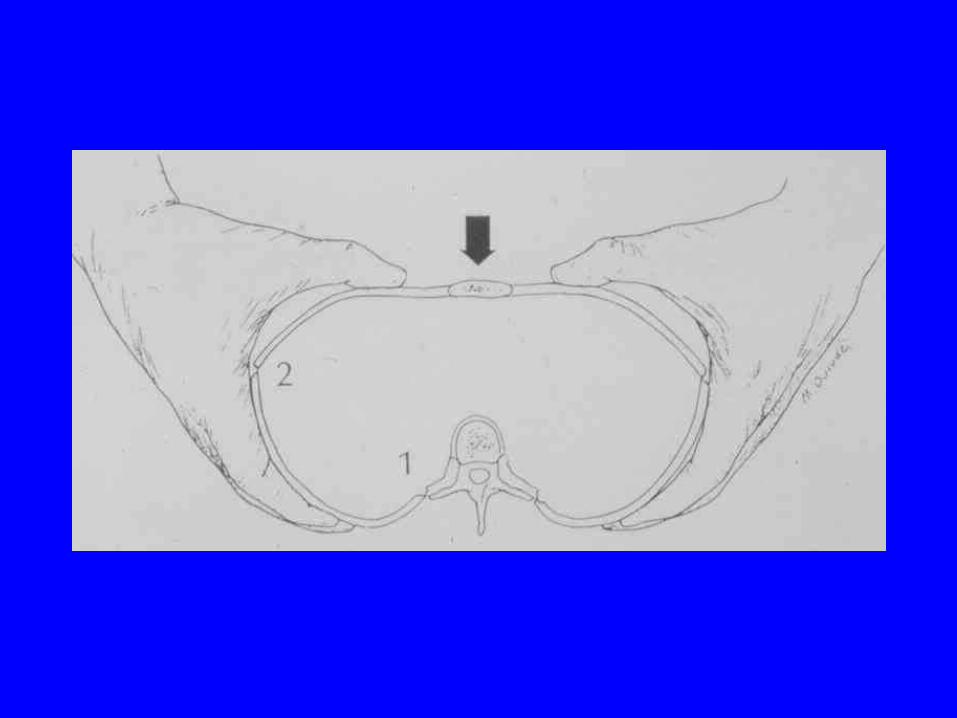
most are likely due to forceful compression of rib cage during forceful squeezing or shaking
rarely seen accidentally without history of significant trauma i.e. MVA, fall from significant height, highly suggestive of NAI
initially painful leading to crying/ screaming, may be few symptoms, rarely bruising
Shaken Baby SyndromeShaken Baby Syndrome
forceful shaking of infant resulting in head whipping back and forth rapidly
may be associated with direct trauma to head
multidirectional forces may lead to brain injury, shearing of blood vessels with resultant intracranial hemorrhage

Shaken Baby SyndromeShaken Baby Syndrome
often no external signs of trauma other medical findings may include:
skull fractures
retinal hemorrhages
rib fractures
metaphyseal fractures
Shaken Baby SyndromeShaken Baby Syndrome
variable clinical presentation, depending on severity of force applied, may include:
irritability, lethargy, crying
vomiting, poor feeding
breathing problems, respiratory arrest
seizures, unconsciousness, death

Sexual Abuse/AssaultSexual Abuse/Assault
medical findings classified as:
normal
nonspecific - many possible causes
suspicious - unusual for typical exams
suggestive - representative of injury
definitive - gonorrhea, syphilis,
pregnancy, semen
Child & Family Services ActChild & Family Services Act
The paramount purpose of the Act is to promote the best interests, protection and well-being of children
pendulum has swung from preserving family to well-being of child

CFSA Amendment ActCFSA Amendment Act
Came into effect in March 2000 to provide a “legislative framework
allowing earlier and more decisive intervention into the lives of children where there are reasonable grounds to suspect that a child has suffered or there is a risk that a child is likely to suffer, abuse or neglect”
Child in need of protectionChild in need of protection
Section 32(2)(a)-”the child suffered physical harm, inflicted by the person having charge of the child or caused by or resulting from that person’s i) failure to adequately care for, provide for, supervise or protect the child or, ii) pattern of neglect in caring for, providing for, supervising or protecting the child”

Child in need of protectionChild in need of protection
Section 37(2)(b)’ “there is a risk that the child is likely to suffer physical harm…”
threshold has lowered

CFSA-Sexual AbuseCFSA-Sexual Abuse
Section 37(2)(c & d)-”the child has been (or there is a risk that the child is likely) to be sexually molested or sexually exploited by the person having charge of the child or by another person where the person having charge of the child knows or should know the possibility of sexual molestation or sexual exploitation & fails to protect the child”

CFSA-emotional harmCFSA-emotional harm
Section 37(2)(f)-”the child has suffered emotional harm, demonstrated by serious, – i) anxiety– ii) depression– iii) withdrawal– iv) self-destructive or aggressive behaviour– v) delayed development

CFSA-emotional harmCFSA-emotional harm
Section 37(2)(f) cont.-and there are reasonable grounds to believe that the emotional harm suffered(or that the child is likely to suffer) by the child results from the action, failure to act or pattern of neglect on the part of the child’s parent or the person having charge of the child

CFSA - domestic violenceCFSA - domestic violence
Violence in the family has a severe emotional impact on children and is a form of emotional maltreatment (Tower, 1996)
the estimated overlap between domestic violence and child physical or sexual abuse ranges from 30-50% (Jaffe et al, 1990; Strause & Gelles, 1990)

CFSACFSA
Section 37(2)(e) -”the child requires medical treatment to cure, prevent or alleviate physical harm or suffering and the child’s parent or the person having charge of the child does not provide, or refuses or is unavailable or unable to consent to, the treatment”
CFSACFSA
Section 37(2)-the child suffers from a mental, emotional or developmental condition that, if not remedied, could seriously impair the child’s development and the child’s parent or the person having charge of the child does not provide or refuses or is unavailable or unable to consent to, treatment to remedy or alleviate the condition
CFSA-Duty to Report CFSA-Duty to Report
Section 72(1)-”despite the provisions of any other Act, if a person, including a person who performs professional or official duties with respect to children, has reasonable grounds to suspect (a child in need of protection) the person shall forthwith report the suspicion & the information on which it is based to a society”
CFSA - Duty to ReportCFSA - Duty to Report
Section 72(2)-” a person who has additional reasonable grounds to suspect one of the matters set out in subsection (1) shall make a further report under subsection (1) even if he or she has made previous reports with respect to the same child”
CFSA Duty to ReportCFSA Duty to Report
Section 72(3)-”a person who has a duty to report a matter undersubsection (1) or (2) shall make the report directly to the society and shall not rely on any other person to report on his or her behalf
Steps to take in reportingSteps to take in reporting
Notify CAS immediately provide demographic data & suspicions do not delegate serve as liaison between hospital, family &
CAS provide support to family assist in follow-up intervention document clearly & precisely
What does this mean to you?What does this mean to you?
You are legally obligated to report all suspected cases of abuse including those in which you feel there is a risk of harm
failure to report-reprimanded by the CNO and a fine
never a case of wrong reporting

Do I need to tell the family?Do I need to tell the family?
not obligated to inform the family about referral to CAS
depends on relationship SCAN can provide this services to allow
therapeutic relationship to be protected ie. chronic patients
What happens after reporting?What happens after reporting?
CAS will take the report and use the “eligibility spectrum” to make a decision
the “eligibility spectrum” is a tool designed to assist CAS staff in making consistent and accurate decisions about eligibility for CAS service at the time of referral
What happens after reporting?What happens after reporting?
Case is discussed with supervisor, therefore you will not receive a decision right away
Following this decision interviews with staff, case conference or direct meeting with family &/or child may take place
CAS are not obligated to inform you of the outcome of the case

Tips for reportingTips for reporting
CAS workers are not medically trained-need to be as clear & concise as possible re:medical information
do not call on the day of discharge SCAN can be a liaison with CAS document objectively!!

DocumentationDocumentation
Be objective not--”parents inappropriate with patient” disclosures/concerning issues presented--
document verbatim injuries--be descriptive, use injury map, use
photographs
Reasons professionals do not Reasons professionals do not report..report..
lack of confidence in the investigatory system lack of confidence in diagnosis difficulty believing abuse present in family discomfort with confrontation reporting is violation of confidentiality legal reprisals & time demands system does not have adequate resources
Effects of AmendmentsEffects of Amendments
Resources have not necessarily been allotted to accommodate changes
CAS will be overwhelmed unsure of legal interpretation--how will this
guide practice review CFSA at least every 5 years

Effects of AmendmentsEffects of Amendments
Reports to CAS have increased since legislative changes
CAST-1998-1999=1700 referrals
1999-2000=3800 referrals Ministry of Attorney General’s office faxes
all domestic violence cases to CAS--approx. 5-10 cases/day
DilemmasDilemmas
Family-centered care & protecting the child Difficult to work through-not black & white many variables will impact decisions may not receive action right away do not lose faith in the system

Case Study #1Case Study #1
Kayla is an 8 year old girl with asthma. She has come to the ER for an acute asthma attack. During your chest assessment with the physician, you notice several large bruises in different locations on her back. Kayla is quite shy. You question her mother about the marks, and she says she does not know. Kayla does not say where they come from either. The physician is concerned and asks you to call CAS.

Case Study #2Case Study #2 You are currently working with youth in a clinic. You are one of
the younger members of staff and the adolescents seem to identify with you. Today, 16yr old Denise approaches you with a problem. She appears quiet and withdrawn, and is requesting information from you about moving out of her home. Upon further probing, Denise tells you that her parents constantly argue, and that her father has been verbally and physically abusive toward her mother when he has been drinking. She recalls that one week ago her father came home drunk and her parents began to fight. Her 8 year old brother began crying and attempted to prevent their father from hurting their mother. Denise took her brother upstairs when the situation became quite violent.
Case Study #3Case Study #3
Two brothers, Ryan (6yr) and Derek (8yr) attend the ambulatory clinic. Both children often come to the clinic with inappropriate clothing and their mother is consistently late picking them up despite discussions about these concerns with staff. They are both quite thin and pale and often have dark circles under their eyes. When working with Derek he often complains of being hungry. Today you have called home to arrange a meeting with their mother and Ryan answers the phone, and when you ask to speak with his mother, he says she isn’t home. When you ask who is home with him he tells you he is home by himself. He tells you his mother is at work and Derek is still at school.

In Summary...In Summary...
“While there are legal repercussions for failure to report, the harm that can result from ongoing maltreatment in a child is severe and must be recognized”
“Approach reporting decisions from the child’s perspective”
Further resourcesFurther resources
“Reporting Child Abuse & Neglect” pamphlet
CAS Website-www.casmt.on.ca O.H.A. Manual “ Identifying & Managing
Child Abuse & Neglect”