Embed Size (px)
DESCRIPTION
Candice A. Lively, J.D. University of South Carolina Children’s Law Center
Citation preview

PROSECUTING FATAL
CHILD MALTREATMENT
CASES
Candice A. Lively, J.D.
University of South Carolina
Children’s Law Center
1600 Hampton Street, Suite 502
Columbia, SC 29208

OBJECTIVES • 1) Know the law
• 2) Be involved in the investigation
• 3) Understand the medical findings
• 4) Be prepared for defense tactics

S.C. LAW • SECTION §16-3-85. Homicide by child abuse; definitions;
penalty; sentencing.
• (A) A person is guilty of homicide by child abuse (HBCA)
if the person:
• (1) causes the death of a child under the age of eleven
while committing child abuse or neglect, and the death
occurs under circumstances manifesting an extreme
indifference to human life; OR
• (2) knowingly aids and abets another person to commit
child abuse or neglect, and the child abuse or neglect
results in the death of a child under the age of eleven.

WHAT DO OUR COURTS SAY?
LEGAL STANDARD
• State v. Holder, March 18, 2009, Supreme Court
-For purposes of the homicide by child abuse statute… Extreme indifference is defined as “a mental state akin to intent characterized by a deliberate act culminating in death.”
McKnight v. State 378 S.C. 33, 661 S.E.2d 354 (2008); Also quoting State v. Jarrell, 350 S.C. 90, 564 S.E.2d 362 (Ct.App.2002).

What does that mean? • You must establish brutality of the event resulting in the
death of the child in order to prove HBCA beyond a
reasonable doubt.
• That is why you need MEDICAL EXPERTS experienced in
child abuse pediatrics
• That is why a multi-disciplinary team approach is the best
way to ensure a conviction
o Collecting information
o Sharing information

Goals of the State
• To Present :
• 1)thorough medical findings
• 2)child’s complete medical history
• 3)accurate time line of events
• 4)who had access to child
• 5)detailed Law Enforcement CSI evidence
• 6)details of violent injury
• 7)possible inclusion of prior bad acts/abuse

Goals of the defense
• DISCREDIT AUTOPSY FINDINGS
• CONFUSE JURY
• GIVE AN EXCUSE FOR EVERYTHING
I SWEAR IT WASN’T ME!!

Things you always do: CRIME SCENE MUSTS:
• Get suspects to write out 24 hour timeline of child’s activities up until symptomatic o I.E. Did child eat/drink? What did child eat/drink? When did child
sleep and for how long? Where did child sleep? Was child verbal? Was child walking? Was child cranky? Was child having normal bowels? Was child ill (fever, stomach, etc.) Was child acting normal, strange, needy, whiney, describe? Who was with child throughout the day? Who fed child? Who held child? Was child ever left alone? Were you ever alone with the child? If so, for how long? If not, who was with you and did he/she ever leave you alone with the child at anytime? Did you ever see child fall, hit head, etc.? Do you discipline the child? How? When was the last time?
• Take notes and audio record all statements of witnesses – and make sure it’s recording!!!!!!!
• Go to alleged crime scene ASAP
#1. Pictures from scene or where child was allegedly found or injured – doll re-enactment when possible

Things you always do cont….
CRIME SCENE MUSTS:
#2, Retrieve bedding, car seats, bouncy seats, sleeping
paraphenalia, medicines in home (OTC), clothing in wash,
trash (diapers), sippy cups (may have medicine in them)
• Research CPS history of everyone having access to child
• Consider cultural issues and alternative medical trmt
• Obtain all medical AND birth records on child
• Obtain a timeline of child’s last week or more from third party
witnesses
o Also ask if they ever saw abuse
o Do they know who cared for the child on day of event?
o Have them describe child’s behaviors – normal for his age,
lethargic, moody, whiney, etc.

Things you always do, cont….
PROSECUTION/SOLICITOR MUSTS:
• Transcript of all statements
• Timeline of child’s last week and final day
• Meet with ALL medical professionals who saw child
and/or treated the child…ALL of them. (Even a nurse
who may only been a small part of treatment may have
seen demeanor of parent/perpetrator when having
contact with the child)
• Meet with EMS and get detailed records
• Have a trial notebook and a medical records notebook
• Review the 911 tape and have it transcribed
• Do a Powerpoint for your closing to convince jury

State v. Gorman/Palmer
Case Study slide 1

Juror letter to Solicitor Hembree
• “Aside from Lively
presenting what the
Jury felt was a very
thorough case, there
was something she
did with her closing
argument which was
very helpful…visual
recaps assisted the
Jury in coming to a
unanimous decision.”
State v. Julia Gorman and
Robert Palmer
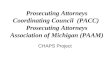
Case Study Slide 2

JULY 2008 SUNDAY MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY
1
* AYDAIN SEEN
BY DR. HUTSON
FOR ANT BITES
& COLD
2
* CESALEE
TRAVELS
BACK TO
ARIZONA
3
4 5
6 7
* AYDAIN
SEEN AT CMC
ER FOR
VOMITING
8
* AYDAIN SEEN
BY DR. HUTSON
FOR VACCINES
9 10 11
*PALMER
GOES OUT IN
P.M.
* GORMAN
ALONE WITH
AYDAIN
12
* AYDAIN
WITH
GORMAN &
PALMER AT
TBONZ
13
* AYDAIN
AT POOL
WITH
GORMAN &
PALMER
14
*AYDAIN IS
INJURED
* 911 IS
CALLED AT
6:06 PM
15
•AYDAIN AT
MUSC
-INFLICTED
HEAD TRAUMA
-HCPD AND DSS
INVOLVED
16
*AYDAIN IS
BAPTIZED
* AYDAIN
PRONOUNCE
D DEAD AT
3:25 PM
17
*GORMAN &
PALMER IN
CONWAY AT
FATZ BAR IN
P.M.
18
*AYDAIN’S
ORGANS
DONATED
*GORMAN &
PALMER
INTERVIEWS
19
*AUTOPSY
C.O.D –
INFLICTED
HEAD
TRAUMA
*M.O.D -
HOMICIDE
20 21 22 23 24 25 26
27 28 29 30 31
Case Study Slide 3

DEFENDANT GORMAN • Page 52: “No I’ve never shook him, never shook him.
Shake a baby no, no I, I no.” o Detective: “you got a little frustrated and you shook him a little
hard”
o Gorman: “I don’t think hard. I don’t believe I.
• Page 58: “We went to Beef O’Brady’s and we went to Fatz, shot some pool.” (Evening of July 17, 2008)
• Page 67: “He cries everyday. He’s cranky everyday, whines everyday.”
• Page 68: Detective: “You were frustrated…it just happened, you shook him. Isn’t that possible?” • Gorman: “Yes that’s possible.”
• Page 69: “I was like damn everytime I walk in the house, I’m going outside. And as soon as I walk outside he stops crying.”
• Page 73: “I’m trying to break all these habits you know and make him a fresh little boy.”
Case Study Slide 4

FIRST RESPONDERS • LT. RAINBOLT – CHILD WAS SEIZING. NO HISTORY OF
FALLS OR SICKNESS.
• ERICA ROSENTHAL – NO HISTORY OF FALLS OR
SICKNESS. STATEMENT BY GORMAN “I’VE RAISED
SEVERAL CHILDREN AND NEVER ONE THIS BAD.” o AYDAIN WAS GIVEN OXYGEN AND VALIUM
o NO CPR, NO INTUBATION AT THAT TIME
Case Study Slide 5

GORMAN AND PALMER
SCENARIO:
LOGAN THE DOG DID IT. Case Study Slide 6

DEFENDANTS’ NEXT SCENARIO
THE STROLLER & THE STAIRS DID IT.
Case Study Slide 7

Child’s Evidence of Injuries • Autopsy Findings: Cause of Death – Inflicted Blunt Head
Trauma. Manner of Death – Homicide.
• Evidence of Injury:
• Comminuted skull fracture
• SDH
• SAH
• Bilateral RH w/multiple layers
Case Study Slide 8

RICHARD AYDAIN GRIMES
THE SILENT WITNESS Case Study Slide 9

Presenting the Medical Evidence • Pick no more than three most compelling medical
experts to hammer the injuries and cause of death. o Avoids overloading jury with medical evidence
o Avoids confusing jury with too many expert opinions on same issues
• Top Three in presenting Child Abuse evidence: 1) Radiologist
2) Board Certified Child Abuse Pediatrician
3) Pathologist
• All other “on hands” medical providers will be more fact
witnesses than experts.

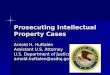
Radiologist • Will be able to provide you with a
timeline of injury to symptomology
better than anyone else
• Have him/her provide powerpoint
slides with 3D images of skull injuries
and brain scans of injuries
• Have him/her compare injured
skull/brain to a normal skull/brain

Head CT 7/15/2008
Dr. Donna Roberts, MUSC
Fractures

Head CT 7/14/2008 normal for comparison
Blood Around Brain (Subdural Hematoma)

The Pathologist • Law enforcement case and medical history
• Scene information and photography
• Any suspicions after initial investigation
• Presence of Investigator is advised
• Cause of death (w/in RDMC); Manner of death
• Keep ME testimony objective
• Detailed Evidence of Injury – tell the story o Dispute the defense claims of cause of injuries to child
o Try to date the timing of injuries – but don’t get cornered by defense
o Describe every listed injury in detail
o Provide detailed analysis of force needed to inflict injuries
o Prosecutor and Pathologist need to know the injuries and “KISS”
o Can testify as to child’s development based on age
• Dispute defense claims of mechanisms for injury

The Child Abuse Pediatric Expert
• Breaks it down so jury can understand the science
• Provides a comprehensive forensically defensible
conclusion o Child Development
o Child’s medical history
o Child’s birth records – apgar score? Type of delivery? Birth trauma?
o Analysis of Caretaker history provided – what does or doesn’t add up
o Can provide an opinion w/in RDMC as to abuse
o Can provide an opinion w/in RDMC as to inflicted head trauma
o Can provide an opinion w/in RDMC as to force and brutality of the act
o Can cite peer reviewed articles to support opinions
o Can discuss triggers for inflicted injuries, especially shaking and head trauma

What will the defense do? • CONFUSE THE JURY – DIVIDE AND CONQUER
• FOR EVERY EXPERT CALLED BY THE STATE, CALL ONE ON BEHALF OF
DEFENSE TO COUNTER
o IF MEDICAL EXPERTS CAN’T AGREE, ISN’T THAT REASONABLE
DOUBT?
• Example – Issue of shaking as mechanism that results in death
• TALK OVER JURY’S HEAD TO MAKE THEM THINK DEFENSE IS RIGHT
• DISPUTE THE STATE’S EXPERTS BUT DON’T PROVIDE CONCLUSIONS
• HUMANIZE THE DEFENDANT(S)

If Defense calls an Expert • Do your homework on the expert
• Tell your State experts who the defense expert is
• Prepare them to address known arguments of that expert
• Call the NDAA – they have extensive information and
transcripts of experts throughout the country
• Call other prosecutors in the State and find out if they
have experience with this expert
• Know the alternative diagnosis the Expert will likely claim

Medical issues in SBS/AHT • IF YOUR CASE INVOLVES SBS/AHT – BE AWARE OF PERCEIVED MEDIA
CONTROVERSY
• MAKE SURE YOUR CHILD ABUSE PEDIATRICIAN AND PATHOLOGIST CAN
ADDRESS IT
• MEDICAL ISSUES WITH IDENTIFYING MECHANISM OF INJURY:
SHAKEN BABY SYNDROME AS A MEDICAL DIAGNOSIS
o AMERICAN ACADEMY OF PEDIATRICS, MAY 2009, CHANGED IT FROM
SBS TO AHT. WHY??
• USE OF ABUSIVE HEAD TRAUMA ADOPTED AS APPROPRIATE
DESCRIPTION FOR INFLICTED HEAD INJURIES IN CHILDREN.
o ACCURATELY INCLUDES IMPACT TRAUMA, SHAKING AND THE
TWO MECHANISMS COMBINED.
o ALLOWS PEDIATRICIAN TO MOVE AWAY FROM LIMITATIONS
ASSOCIATED WITH THE TERM OF SBS WHICH ONLY REFERS TO
“SHAKING” AS A MECHANISM.

ABUSIVE HEAD TRAUMA • Triad of Injuries: 3 injuries which, when seen together,
may be pathognomonic for Abusive Head Trauma.
• 1) Subdural Hematoma: Bleeding into the space
between the dura (the brain cover) and the brain itself.
• 2) Cerebral Edema: Accumulation of excessive fluid in
the substance of the brain; i.e. brain swelling.
• 3) Retinal Hemorrhage: Bleeding in the retina of the eye.
Especially when multi-layered.

Case history #2 • 6 WEEK OLD FEMALE MEDICAL HISTORY
o HISTORY OF MYOCLONIC MOVEMENTS – SHORT DURATION
o QUESTIONABLE HISTORY OF REFLUX
o VAGINAL DELIVERY WITHOUT COMPLICATIONS
• FATHER ALONE WITH BABY IN HOTEL ROOM 11:30 A.M.
o FATHER GOES TO CHANGE HER DIAPER
o BABY TURNS RED AND STOPS BREATHING
o HE BELIEVES SHE IS CHOKING
o FATHER ADMITS “SHAKING BABY TO REVIVE”
• 911 CALLED AND BABY TRANSPORTED TO LOCAL HOSPITAL
o BABY LABORED BREATHING
o NO OUTSIDE TRAUMA NOTED
o CHEST SCAN PERFORMED AND NOTHING REMARKABLE
o TRANSFER TO MUSC FOR CARE

VICTIM’S SYMPTOMS AT MUSC
• FINDINGS AT MUSC
o CT SCAN REVEALED
• WIDESPREAD SUBARACHNOID HEMORRAGE
• LEFT-SIDED SUBDURAL HEMORRAGE
• INTRAVENTRICULAR HEMORRAGE
• RETINAL HEMORRHAGING
• SKELETAL SURVEY REVEALED
o BILATERAL FEMORAL METAPHYSEAL FRACTURES
o LEFT TIBIAL METAPHYSEAL FRACTURE

COMPLICATIONS
• BABY DIED 3 DAYS LATER
o COMPLICATIONS INCLUDED:
• BRAIN SWELLING
• REFRACTORY INTRACRANIAL HYPERTENSION
• ANOXIC BRAIN INJURY

Autopsy evidence of injury • CLOSED HEAD INJURY
o SUBDURAL HEMORRHAGE
o DIFFUSE SUBARACHNOID HEMORRAGE
o RETINAL HEMORRHAGES OF RIGHT EYE
o BILATERAL OPTIC NERVE SHEATH HEMORRHAGES
o CONTUSIONS OF MUSCLES OF UPPER BACK
• INCLUDES LACERATION OF POSTERIOR ATLANTOAXIAL MEMBRANE
• INCLUDES CONTUSION OF CERVICAL SPINAL CORD
• SKELETAL INJURIES
o TRANSMETAPHYSEAL FRACTURES OF DISTAL RIGHT AND LEFT FEMORA
o METAPHYSEAL FRACTURES OF DISTAL FEMORAL AND PROXIMAL LEFT TIBIAL CORNER
FRACTURES
• OTHER EVIDENCE OF INJURY
o PARENCHYMAL LACERATION OF LIVER

subarachnoid hemorrhage

cervical spinal cord

transmetaphyseal fracture

fracture line

liver

What did the Defense do? • Humanized defendant and flooded media
• Attacked all medical conclusions with expert witnesses
• Attacked autopsy
• Know what test(s) were not performed and draw
conclusions from it
o MENINGOENCEPHYLITIS
o CLAIM THE BRAIN TISSUE SHOWED PUSS IN SLIDES
o SPINAL FLUID NEVER TESTED FOR INFECTION
• Prepare your witnesses to win over the jury

“He is a good man”

Newspaper pictures

Example of Defense Expert
• Dr. Ronald Uscinski
“The Re-Bleed Expert”
Will testify that shaking alone cannot
cause injury severe enough to kill a
baby.
Will testify that SDH can be a result of a
chronic rebleed in the brain.

Slide A19B – Brain with meningoencephalitis
40x magnification showing menigoencephalitis – Dr. Janice Ophoven

Give an excuse for everything • SAY THE STATE’S EXPERTS ARE WRONG BUT DON’T GIVE AN ANSWER, JUST AN EXCUSE
o EXAMPLES FROM CURRENT CASE:
• CERVICAL SPINE LACERATION WAS ARTIFACT OF AUTOPSY
• BRAIN SWELLING WAS FROM INFECTION NOT INFLICTED TRAUMA
o NO INDEPENDENT TESTS DONE TO PROVE THIS BY DEFENSE
• METAPHYSEAL FRACTURES WERE CAUSED BY EITHER:
o INTRAOSSEUS LINE PLACED IN BABY’S LEGS; OR
o INCIDENT TO CPR AND STRAPPING BABY IN AMBULANCE
o BRITTLE BONE DISEASE – EVEN THOUGH TEST WAS NEGATIVE
• LACERATED LIVER CAUSED BY CPR
o INTERESTING FACT IS THAT NO ONE PERFORMED CPR ON BABY
• RETINAL HEMORRHAGE OF RIGHT EYE COULD BE CAUSED BY INTRACRANIAL PRESSURE
• SUBDURAL HEMATOMA/HEMORRHAGE WAS A CHRONIC RE-BLEED OF A HEMATOMA
BABY HAD AT BIRTH
• ALTE – APPARENT LIFE THREATENING EVENT

Conclusion • Be prepared
• Know the science and medical findings
• Put in the time to do it right
• The case isn’t over until the verdict

What questions do you have?