Embed Size (px)
DESCRIPTION
CHF algorythm
Citation preview

*First Draft 6/2011. Contributing staff: Dr. Charles Moore, Dr. Robert Long, Dr. Richard Summers, Leslie Hood, RN Tammy Thomas, RN, Cori Bitner, RN, Jason Zimmerman, RN.
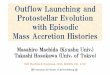
CHF Treatment Algorithm
Patient presents to AED with s/s of CHF
s/s of CHF: Orthopnea DOE/SOB Recent weight gain Ascites Jugular vein distention Peripheral edema Rales on auscultation
Triage per AED policy
Is respiratory failure
imminent?
YES NO
Consider: Bipap/CPAP ETT intubation NTG or other vasodilator for elevated BP Probable ICU admit
Cardiogenic shock or
symptomatic hypotension?
NO
YES
Consider: IV access Inotrope Hemo-dynamic monitoring ABGs Probable ICU admit
Complete H&P CBC,Chem8, Mag,Phos,Ca+, proBNP,Troponin, PT/PTT/INR CXR, EKG Loop Diuretic
Is Decompensated CHF likely?
Critical Severity: ICU CRITERIA Dyspnea with ≥ 1 of the following:
• HR >120, RR >35, SBP <90 • Mental Status changes • IV medication requiring titration • Mechanical ventilation • Afib/flutter >120bpm, SBP <90 • Unresponsive to ED treatment
Moderate Severity: TELEMETRY CRITERIA
• SBP ≥90 or at baseline • RR >26 • Requires continuous cardiac monitoring • Rales/rhonchi (often absent) • Poor response to ED treatment
Low Severity: OBSERVATION CRITERIA
• O2 sat ≥ 90% or PaO2 ≥ 60 on room air • SBP >100 or at baseline • No evidence of ischemia on EKG • At least 1 negative cardiac enzyme resulted • Responsive to ED treatment
NO
Consider other
diagnosis and
treatment.
Yes
DISCHARGE CRITERIA
• Ambulatory for 3-6 minutes with little to no dyspnea
• Reduced body weight
• Resolution of rales • No significant
alterations in electrolytes
• VS stable or at baseline for at least 8 hours.