Embed Size (px)
Citation preview

April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 611
PUBLIC HEALTH THEN AND NOW
The first large-scale use of a traditional weapon of mass destruction (chemical, bi-ological, or nuclear) involved the successful deployment of chemical weapons dur-ing World War I (1914–1918). Historians now refer to the Great War as thechemist’s war because of the scientific and engineering mobilization efforts by themajor belligerents. The development, production, and deployment of war gasessuch as chlorine, phosgene, and mustard created a new and complex public healththreat that endangered not only soldiers and civilians on the battlefield but alsochemical workers on the home front involved in the large-scale manufacturingprocesses. The story of chemical weapons research and development during thatwar provides useful insights for current public health practitioners faced with apossible chemical weapons attack against civilian or military populations. (Am JPublic Health. 2008;98:611–625. doi: 10.2105/AJPH.2007.11930)
| Gerard J. Fitzgerald, PhD
Chemical Warfare and Medical Response During World War I
The surprise use of chlorinegas allowed the Germans to rup-ture the French line along a 6-kilometer (3.7-mile) front, caus-ing terror and forcing a panickedand chaotic retreat. Within amatter of minutes, this slow mov-ing wall of gas killed more than1000 French and Algerian sol-diers, while wounding approxi-mately 4000 more.2 A Britishsoldier described the pandemo-nium that flowed from the frontlines to the rear.
[I watched] figures runningwildly in confusion over thefields. Greenish-gray cloudsswept down upon them, turningyellow as they traveled over thecountry blasting everything theytouched and shriveling up thevegetation. . . . Then there stag-gered into our midst French sol-diers, blinded, coughing, chestsheaving, faces an ugly purplecolor, lips speechless with
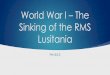
Chlorine gas, released from cylinders, drifts over the Western Front.
Source. Francis Joseph Reynolds and C.W. Taylor, Collier’s New Photographic History ofthe World’s War (New York: P. F. Collier and Son, 1918).
IN THE LATE AFTERNOON OFApril 22, 1915, members of aspecial unit of the German Armyopened the valves on more than6000 steel cylinders arrayed intrenches along their defensiveperimeter at Ypres, Belgium.Within 10 minutes, 160 tons ofchlorine gas drifted over the op-posing French trenches, engulfingall those downwind. Filled withpressurized liquid chlorine, thecylinders had been clandestinelyinstalled by the Germans morethan 3 weeks earlier. The order torelease the gas was entrusted toGerman military meteorologists,who had carefully studied thearea’s prevailing wind patterns.Disregarding intelligence reportsabout the strange cylinders priorto the attack, the French troopswere totally unprepared for thisnew and horrifying weapon.1

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4612 | Public Health Then and Now | Peer Reviewed | Fitzgerald
Although chemical weaponskilled proportionally few soldiersin World War I (1914–1918), thepsychological damage from “gasfright” and the exposure of largenumbers of soldiers, munitionsworkers, and civilians to chemi-cal agents had significant publichealth consequences. Under-standing the origins of chemicalwarfare during World War I andits emergence during that conflictas a physical and psychologicalthreat to both military and civil-ian populations can provide his-torical insight into possible con-temporary medical responses tothis enduring and technologicallypervasive threat.
THE MILITARIZATION OF ACADEMIC ANDINDUSTRIAL CHEMISTRY
World War I had numerouscauses, including colonial competi-tion, economic rivalry, and variousideological and cultural clashesamong the rising nation states ofEurope. A complex and bindingsystem of alliances among theCentral Powers (Germany, Austria-Hungary, and Turkey) and the Al-lied Powers (Britain, France, Rus-sia, and beginning in 1917, theUnited States) placed peace in adelicate balance. The tipping pointcame on June 28, 1914, with theassassination of Archduke FranzFerdinand of Austria-Hungary bya Serbian national. This single actset off a chain of events thatquickly plunged the world into aglobal war that eventually claimedbetween 9 million and 10 millionlives and lasted 4 years.6
The economic and industrialforces that altered the face of Eu-rope during the first decade ofthe 20th century were also in-strumental in creating many ofthe technological innovations
driving the war. In time, tanks,submarines, and aircraft revolu-tionized how World War I waswaged on land, sea, and in theair. Chemical weapons were an-other new marvel of the war,and their successful research, de-velopment, and deployment re-flected the increasing sophistica-tion of scientific and engineeringpractice. At the same time, physi-cians and medical researchers(some of whom worked to createthese weapons) struggled to cre-ate adequate defensive systemsand medical procedures to limitcasualties. By the time of thearmistice on November 11, 1918,the use of chemical weaponssuch as chlorine, phosgene, andmustard gas had resulted in morethan 1.3 million casualties andapproximately 90000 deaths(Table 1).
Although one could argue thatprimitive forms of chemicalweapons were used in earlierconflicts, it was not until the20th century that scientists, engi-neers, and physicians could pre-dictably and consistently producethese weapons to inflict mass ca-sualties.7 At the close of the 19thcentury, the various Europeanpowers became troubled by thepotentiality of chemical weaponsand began holding conferencesand writing various treaties tolimit or curtail the developmentand deployment of this new tech-nology. Suspicion and self-inter-est among both allies and rivalsgenerally limited the usefulnessof these activities, an unfortunatepolitical reality that continues tothe present day. For instance, theHague Declaration of 1899 andthe Hague Convention of 1907forbade the use of “poison or poi-sonous weapons” in warfare, yetmore than 124000 tons of gaswere produced by the end ofWorld War I.8
agony, and behind them in thegas soaked trenches, we learnedthat they had left hundreds ofdead and dying comrades.3
The German High Commandsanctioned the use of gas in thehope that this new weaponwould bring a decisive victory,breaking the enduring stalemateof trench warfare. However, theirfaith in this wonder weapon waslimited. Surprised by the appar-ent success of the attack, andhaving no plan to send a largeoffensive force in after the gas,the Germans were unable to takeadvantage of the situation.Within days, both armies onceagain faced each other from thesame opposing fortifications. Theattack that spring day, nonethe-less, marked a turning point inmilitary history, as it is recog-nized as the first successful useof lethal chemical weapons onthe battlefield.
Here, I offer a window intothe first weapon of mass de-struction (WMD) by chartingthe development and use of gaswarfare during World War I.Defined today as “man-made,supertoxic chemicals that can bedispersed as a gas, vapor, liquid,aerosol (a suspension of micro-scopic droplets), or adsorbedonto a fine talcum-like powderto create ‘dusty’ agents,” chemi-cal weapons remain a viablepublic health threat for civiliansand soldiers across the globe.4
If, in the world since the attacksof September 11, 2001, thethreat of terror weapons seemsa ubiquitous part of the dailynews and the term WMD is nowas familiar to soccer moms as tobeltway defense planners, it isimportant to remember that themedical and public health con-sequences of chemical weaponsuse are as real today as theywere in 1915.5

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 613
The development of these wargases, like many of the other newweapons systems created duringthis period, depended on the workof academic and industrial scientistswho increasingly served the mili-tary needs of the state. Germany,arguably the world’s leader in sci-ence at the time, and withoutquestion the guiding force in aca-demic and industrial chemistry,moved decisively in the researchand production of chemical agentsonce the war began. Fritz Haber,a prominent German chemist andfuture Nobel laureate, led theGerman program.9 Haber, theso-called “father of chemicalweapons,” moved enthusiastically
between the front and the KaiserWilhelm Institute for PhysicalChemistry and Electrochemistryin Berlin. As he organized and ledthe German chemical warfareprogram, solving ongoing prob-lems in chemical agent develop-ment and deployment, his activi-ties anticipated a troubling patternof behavior among future genera-tions of scientists, engineers, andphysicians.
The Germans’ first use of gasmirrored their initial emphasis onthe offensive aspects of chemicalweapons research and their beliefthat a technological fix wouldbring a decisive victory.10 Thoseon the receiving end, France and
Great Britain, moved first on thedefensive aspects of these newweapons. By war’s end, however,the national programs among thewarring nations focused on boththe offensive and defensive as-pect of chemical weapons. Theseprograms were often a result ofthe complete mobilization of theirnations’ academic, industrial, andeconomic resources for war.
The expansion of researchbrought in an array of specialistsfrom chemistry, physics, and en-gineering and, increasingly, frommedicine, biology, and physiol-ogy, further blurring ethical de-marcations in medical research.Throughout the war, the British
Table 1—Chemical Warfare Agents Developed During World War I
Chlorine (Cl2) Phosgene: Carbonyl Chloride Mustard Gas: ββ’-Dichlorethyl Lewisite:β-Chlorovinyldichloroarsine (COCl2) Sulfide (ClCH2CH2)2S (ClCH=CHAsCl2)
US Army chemical warfare service symbol Cl CG HS M-1
Physiological classification Lung injurant Lung injurant Vesicant Vesicant
Tactical classification Casualty agent Casualty agent Casualty agent Casualty agent
Vapor densitycompared with air 2.5 3.5 5.5 7.1
Persistency Summer: 5 min in open, Summer: 10 min in open Summer: 24 h in open, 1 wk in Summer: 24 h in open, 1 wk20 min in woods; winter: 10 min 3 min in woods; winter: 20 min woods; winter: several weeks in in woods; winter: 1 wk in the
in open, 60 min in woods in open, 2 h in woods both the open and woods open and woods
Lethal concentration, mg/L 30-min exposure: 2.53; 30-min exposure: 0.36; 30-min exposure: 0.07; 30-min exposure: 0.48;or oz/1000 cu ft/10 min exposure 10-min exposure: 5.60 10-min exposure: 0.50 10-min exposure: 0.15 10-min exposure: 0.12
Odor Pungent Fresh-cut hay Garlic or horseradish Like geraniums, then biting
Neutralization Alkali solution or solid Steam will hydrolyze; alkalis Bleaching powder 3% solution Alcoholic sodiumand amines react with CG sodium sulfide (Na2S) in water; steam; hydroxide spray
gaseous chlorine; or bury under moist earth
Physiological action Burns upper Burns lower lung Dissolves in skin and then Dissolves in skin then burns respiratory tract surfaces causing edema produces burns and liberates M-1 oxide,
which poisons body
Protection Gas masks, absorbents Gas masks, absorbents Gas masks and protective Gas masks and best ofin canisters only in canisters only clothing protective clothing
First aid Keep patient quiet and Keep patient calm; Wash affected parts with kerosene Wash with oils, hot water,warm and treat for administer heart stimulants; or gasoline, then with strong soap and and soap; dry; first aid must
bronchial pneumonia give oxygen in severe cases, water; rub, dry, rinse with hot clean be applied at oncetreat like pleurisy water; agent must be removed within 3 min
Eye casualty concentration 1 h exposure,.0001 (mg liter).
Source. Compiled from Medical Aspects of Chemical and Biological Warfare, ed. Frederick R. Sidell, Ernest T. Takafuji, and David R. Franz (Washington, DC: Office of the Surgeon General; 1997).

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4614 | Public Health Then and Now | Peer Reviewed | Fitzgerald
armed forces enlisted scientists inmany academic institutions—in-cluding Oxford, Cambridge, Uni-versity College London, theArmy Medical College at Mill-brook, and the Lister Institute—towork on both aspects of gas war-fare. The French governmenttook a more direct approach tochemical weapons research bymilitarizing the chemistry, pathol-ogy, and physiology departmentsof 16 leading medical schoolsand institutes. Additionally, it es-sentially absorbed the Universityof Paris in order to direct, coordi-nate, and research all aspects ofchemical warfare.11
Research conducted by Alliedscientists on the nature of chemi-cal warfare, and the observationsand experience of their combattroops was employed by theUnited States with varying de-grees of success when it joinedthe Allies. The United States hadadopted a policy of formal neu-trality at the beginning of thewar, although ongoing Atlantictrade benefited the Allied cause.American sympathies for Britain,France, and other allies grewduring the course of the war,aided both by the deadlock onthe battlefield and the increasingmenace of unrestricted subma-rine warfare by German U-boats.In 1917, a marked increase in U-boat attacks on commercial ship-ping, in addition to a potentialGerman alliance with Mexico, ledto a formal declaration of war onApril 6, 1917.
The American response tochemical warfare is indicative ofthe growing sophistication of aca-demic, industrial, and military re-search and development capabili-ties in the United States at a timewhen linkages between the fed-eral government and science werebecoming more pronounced.12
As the war intensified, increasing
anxiety about possible entry intothe conflict and the overall lackof military preparation promptedsome in government, industry,and academe to begin planning.The origins of an organized pro-gram for chemical warfare inWashington came first from thecivilian sector. On February 8,1917, Van H. Manning, the direc-tor of the Bureau of Mines, of-fered the technical services of hisagency to the Military Committeeof the National Research Council.The familiarity of the bureau withresearch involving noxious gases,breathing apparatus, explosives,and gas detection technologiesseemed well suited for the task.13
On the same day as the Amer-ican declaration of war, the Na-tional Research Council subcom-mittee on noxious gases wasappointed to “carry on investiga-tions into noxious gases, genera-tion, antidote for same, for warpurposes.”14 Within one year, re-search was under way at a num-ber of prestigious universitiesand medical schools, includingthe Massachusetts Institute ofTechnology, Johns Hopkins, Har-vard, and Yale, in addition tosome of the country’s leading in-dustrial firms.15 The chemicalwarfare program was directedout of offices and laboratories atAmerican University in Washing-ton, DC. During the course of thewar, research programs involving
gas investigations; defense prob-lems; medical science problems;chemical research; gas mask re-search; pyrotechnic research;small-scale manufacturing; me-chanical research; pharmacologi-cal research; [and] administrationwere carried out in Washingtonand across the country.16
Research began as the first UStroops made preparations for com-bat. Fear of gas attacks againstthese members of the American
Expeditionary Force (AEF) em-barking for the European front ini-tially focused research in theUnited States on defensive mea-sures, with priority given to gasmask design and production.
As the American war effort in-tensified, research expanded toinclude offensive weapons, result-ing in numerous discoveries, in-cluding the creation of one of theconflict’s only new chemicalweapons, an arsenic-based agentsimilar to mustard gas calledlewisite (β-chlorovinyldichloroar-sine). Synthesized in his labora-tory by Wilfred Lee Lewis, thisdeadly substance was soon mass-produced by the military underthe direction of chemist and fu-ture Harvard president James. B.Conant.17 By July 1918, researchand development on agents suchas lewisite passed from civilian tomilitary control as the entirechemical weapons programmoved from the Bureau of Minesto the army’s newly organizedChemical Warfare Service.
At that time, chemical warfareresearch in the United States in-volved more than 1900 scientistsand technicians, making it at thattime the largest government re-search program in American his-tory.18 By the time the warended, historians estimate thatmore than 5500 university-trained scientists and techniciansand tens of thousands of indus-trial workers on both sides of thebattle lines worked on chemicalweapons.19 Both the military useand industrial production ofchemical weapons presented anumber of health risks.
GAS MASKS AND THEEVOLUTION OF GASDEFENSE
As the war progressed, theknowledge gained by British,

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 615
French, and German militaryplanners and scientists on the na-ture of gas warfare quicklyevolved into a kind of technologi-cal chess match. New offensivethreats were met by an evolvingarray of defensive countermea-sures. Overall, the deployment ofchemical weapons met withmixed results as the tactics, strat-egy, and military culture of all ofthe armies continually struggledto adjust to this new weapon.Aside from tactical and strategicconsequences, chemical weaponsheralded larger cultural changesfor combatant and observer alike.In perhaps his most celebratedpoem, “Dulce et Decorum Est,”British soldier Wilfred Owen cap-tured in verse the horrors of thisnew form of warfare, a horrorthat he had witnessed first handat the front.
Gas! Gas! Quick, boys!—An ecstasy of fumbling,Fitting the clumsy helmets just in time;But someone still was yellingout and stumbling,And flound’ring like a man on fire or lime . . .Dim, through the misty panesand thick green light, As under a green sea, I saw him drowning . . . 20
The types of gas attacks Owenwitnessed prior to his own deathin 1918 were quite different inkind than those experienced bytroops stationed at the front dur-ing the first years of the war.
Chemical warfare had begunin a tentative way before Ypreswith the French use of tear gasgrenades in 1914 and early1915. Similarly, the Britishbegan developing a range ofnonlethal chemical weaponsmeant to harass enemy troops.The Germans started experi-mental work on chemicalagents in late 1914 at the sug-gestion of University of Berlin
chemist and Nobel laureateWalther Nernst.21 This early re-search quickly produced an ef-fective tear gas artillery shell.Although the Germans fared nobetter than the French with teargas as a debilitating agent, Ger-man chemists, now with a for-mal program led by Fritz Haber,continued to work on the chem-ical weapons problem. By 1915,scientists at the Kaiser WilhelmInstitute had developed an ef-fective chlorine gas weapon. Byplacing chlorine into speciallydesigned cylinders, chlorine gascould be discharged in a densecloud that eventually settledinto enemy trenches. Interest-ingly, the German High Com-mand envisioned gas as an ef-fective tool to draw soldiers outof their trenches so as to kill orwound them with conventionalweapons rather than as a lethalweapon.22
As an offensive response tochlorine, both the French andthe British quickly developed“annoyer” grenades, but thesechemical weapons were notlethal and few even made it ontothe battlefield. By mid-1915,both sides regularly used cylin-ders to deploy chlorine gas, andby mid-1916 both sides mixedchlorine and phosgene in an at-tempt to create larger numbersof casualties.23 By the end of thewar, most belligerents employeda variety of chemical agents incombat, including chlorine, phos-gene, and mustard gas (Table 1).
The Germans’ offensive use ofchlorine led one British soldier toremark that it “was the mostfiendish, wicked thing I haveever seen.”24 In a more graphicdescription, British SergeantElmer W. Cotton vividly remem-bered the suffering of gassed sol-diers. He wrote in his diary thatmen were
propped up against a wall . . . —all gassed—their color wasblack, green & blue, tongueshanging out & eyes staring—oneor two were dead and othersbeyond human aid, some werecoughing up green froth fromtheir lungs.25
This type of suffering movedthe British and the French toquickly develop some type ofprotection from chlorine gas. TheBritish promptly developed aprimitive gas mask that a soldierdescribed as “piece of muslin,which we tied round the noseand mouth and around the backsof our heads,” but these werelargely ineffective.26 Once chlo-rine was identified as the chemi-cal agent, a thiosulfate-laced cot-ton pad effectively neutralizedthe gas.27
By July 1915, the British med-ical corps devised a wool hoodsoaked in thiosulfate, sodium bi-carbonate, and glycerin. This“hypo helmet,” a hood that fullyenclosed a soldier’s head, had amica window so soldiers couldsee.28 Although these early maskswere better than nothing, soldiersfound them difficult to put on,uncomfortable, and easily dam-aged, thus limiting their effi-cacy.29 The development of thesmall box respirator by the Britishin 1916 provided effective protec-tion from most chemical agentsused throughout the war becauseit could be modified to neutralizenew agents, such as mustard gas.
The gas mask drill—the don-ning of all protective gear as rap-idly as possible under the mostdifficult conditions—became an in-tegral part of life in the trenchesand in preparing recruits for bat-tle. As with the rifle drill that an-chors infantry training, the disci-pline and skills needed to quicklyand effectively don protective gearbecame a necessary part of lifefor all at the front. Soldiers were

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4616 | Public Health Then and Now | Peer Reviewed | Fitzgerald
instructed always to have theirmask handy, no matter where theywere or what they were doing. Re-sponding to the sound of a specificwhistle, clanging alarm bell, orshout, soldiers would move withall due speed to put on their masksor hoods. Far from embracing gasmasks as a life-saving technology,soldiers felt emasculated and claus-trophobic in them. As one Britishofficer explained,
We gaze[d] at one another likegoggle-eyed, imbecile frogs. Themask makes you feel only halfa man. The air you breathe hasbeen filtered of all save a fewchemical substances. A mandoesn’t live on what passesthrough the filter—he merely exists. He gets the mentality of a wide-awake vegetable.30
According to British infantry-man Albert Marshal, “By the sec-ond lot we’d got gas masks whichcame right over your head. Theywere terribly hot and awful, butstill, they stopped the gas.”31
There was also no guaranteethat gas masks would work. Al-though British and German maskswere fairly reliable because of
Gas mask designs used throughoutthe war.
Source. Francis W. Halsey, The LiteraryDigest History of the World War, Vol. V(New York: Funk and Wagnall’s Company,1920).
strict quality control measures, theFrench masks were notoriouslyunreliable. Moreover, treatingwounded soldiers became evenmore difficult when bothstretcher-bearers and injured menneeded to don masks, and insome cases the masks causedmore trauma to victims.32 Thedangers at the front affected allthose that lived and labored there.Besides affecting military popula-tions, gas clouds caused civiliancasualties because the wind oftenblew through villages and townsclose to the front. Unlike soldiers,civilians did not necessarily haveaccess to gas masks or the train-ing to make sure the masks wereused properly. Although the offi-cial number of civilian casualtieswas about 5200, the numberswere undoubtedly much higher.33
The probability of gas attack was so frequent that in time re-searchers on both sides even de-vised masks for horses, dogs, andmessenger pigeons involved inmilitary operations.34
As the Americans watched thewar in Europe, they realized asearly as 1915 that gas masks
were an important defensivemeasure for their troops. TheBoard of Ordnance and Fortifica-tions of the War Departmentstressed the importance of devel-oping masks before the UnitedStates entered the war. In a No-vember 5, 1915, meeting theydecided that “Certain practices inthe present European war haveindicated the necessity for pro-viding some equipment of thiskind. . . . The design and supplyshould not be left unassignedand should be assigned to theMedical Department.”35
Within a month of the USentry into the conflict, the secre-tary of war ordered the surgeongeneral to supply 1000000 gasmasks, 8500 “chemicalsprayer[s] for cleaning trenches,”and 1000 “oxygen apparatus forresuscitating [the] wounded” byJune 30, 1918.36 As the summerof 1917 progressed, it becameevident that unlike the otherpurely laboratory-based researchprograms, the complexity andscale of gas mask manufacture (anew and complex industrial en-deavor) required a separate insti-tutional structure within the newchemical warfare research appa-ratus. On August 31, 1917, theGas Defense Service (laterknown as the Gas Defense Divi-sion) was formally organizedwithin the Army Medical Depart-ment under the auspices of theOffice of the Surgeon General tocarry out gas mask research andmanufacture.37 Even with the na-tion’s elaborate institutional andresearch commitment to gasmasks, masks had their limitsand could not ward off the fearof being gassed.
By late 1915, gas warfare hadbecome a psychological as wellas physical weapon. Much ashellish multiday artillery barragesresulted in mental breakdowns

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 617
associated with “shellshock,” theconstant threat of exposure toeven a single gas shell added tothe already unbearable stress oflife at the front. The fear of beinggassed, along with periodic ha-rassing gas attacks, kept soldierson both fronts on edge and couldlead to anomie, gas fright, and insome cases mental breakdowns.Soldiers on all sides felt that gaswarfare was not a properweapon and went beyond thebounds of humanity.38 H. Allen,who served at the front, de-scribed the psychological effectsof nightly gas threats:
With men trained to believethat a light sniff of gas mightmean death, and with nerveshighly strung by being shelledfor long periods and with thepresence of not a few who re-ally had been gassed, it is nowonder that the gas alarm wentbeyond all bounds. . . . Gashorns would be honked, emptybrass shell-casings beaten, riflesemptied and the mad cry wouldbe taken up. . . . For milesaround, scared soldiers woke upin the midst of frightful pande-monium and put on their masks,only to hear a few minutes laterthe cry of “All safe.” . . . Two orthree alarms a night were com-mon. Gas shock was as frequentas shellshock.39
The psychological conse-quences of gas attacks were notlimited to fear of the air that sol-diers breathed. A 1918 US Army“afteraction report” described anincident in which a platoon of ma-chine gunners became convincedthat their food was contaminatedin a gas attack. When a shell ex-ploded near the men while theyate, a soldier remembered:
[S]omeone yelled “GAS!” andsaid their food had been gassed.All the men were seized withgas fright and a few minuteslater made their way to the AidStation. . . . They came in instooping posture, holding theirabdomens and complaining of
pains in the stomach, while theirfaces bore anxious, frightenedexpressions and some had evenvomited.40
After being given bicarbonateof soda to settle their stomachs, arest, and reassurances that theywere not gassed, the men re-turned to the front. Because bothgas fright and gas attacks becamemore severe in 1917 and 1918,doctors and medics found it diffi-cult to diagnose real as opposedto imagined gas attacks. For themost part, all the medical corpscould do for gas casualties wasprescribe bed rest and wait forsymptoms to emerge. Medicalunits quickly shipped soldierswithout obvious physical symp-toms of gas exposure back to thefront. Moreover, soldiers neverknew if their gas mask wouldleak or if their filter would runout, which caused even moreanxiety as belligerents used morecaustic agents.41 The Allied ef-forts to contain the effects ofchlorine and phosgene brieflystabilized the technological bal-ance through the first half of thewar. The German introduction ofmustard gas would destroy thisbalance and elevate the violenceand terror of chemical warfare toa new level.
MUSTARD, THE “KING OFBATTLE GASES”
By the spring of 1917, the de-fensive measures employed bythe Allied armies to contain theGerman gas threat were increas-ingly successful, as least with re-spect to limiting fatalities. Sur-prisingly, such defensive successcame as the offensive deploymentof gas weapons became increas-ingly sophisticated. Since 1915,the integration of ongoing fieldand laboratory studies involvingagent stability, meteorological
conditions, and weapons designmade the tactical planning in-volved in delivering gas to spe-cific targets much more reli-able.42 There were limits, though,to the destructive range of cer-tain chemical weapons. Bothsides now recognized that al-though a regular gas attack in-volving either chlorine or phos-gene (under optimum conditions)could produce large numbers ofcasualties, such an attack usuallyresulted in relatively few fatalitiesif troops were properly preparedand outfitted.
In a bloody war of attrition,however, the ability to wound in-stead of kill had definite tacticaland strategic value. The contin-ual removal of large numbers ofbattle-ready troops from forwardareas, even for short periods, se-verely compromised the ability ofarmies to conduct successful op-erations. Because of the respira-tory damage both chlorine andphosgene caused, soldiers re-quired a long convalescence be-fore returning to combat. The av-erage number of days an AEFgas victim spent recovering andaway from the front was 60 daysfor chlorine and 45.5 days forphosgene.43 Although such lossescertainly impeded the war effort,by the spring of 1917 the overallmilitary effectiveness of gas at-tacks seemed to be diminishing.This would soon change.
In July 1917, aware of the lossof their technological superiorityand perhaps their ability to winthe war, the Germans deployed anew and more troublesomechemical agent: mustard gas. Al-though mustard was introducedlate in the war, it became knownas the “King of Battle Gases” be-cause it eventually caused morechemical casualties than all theother agents combined, includingchlorine, phosgene, and cyanogen

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4618 | Public Health Then and Now | Peer Reviewed | Fitzgerald
chloride. Harry L. Gilchrist, med-ical director of the Gas Service,US Army Expeditionary Force,described the first mustardcausalities:
At first the troops didn’t noticethe gas and were not uncom-fortable, but in the course of anhour or so, there was markedinflammation of their eyes.They vomited, and there waserythema of the skin. . . . Laterthere was severe blistering ofthe skin, especially where theuniform had been contami-nated, and by the time thegassed cases reached the casu-alty clearing station, the menwere virtually blind and had tobe led about, each man holdingon to the man in front with anorderly in the lead.44
Unlike the lung irritants chlo-rine and phosgene, mustard gaswas a vesicant (similar to lewisite)that produced large blisters onany area of contact. Particularlysevere blisters emerged whenuniforms were soaked in mustardgas. If exposure was high enough,mustard gas could cause perma-nent eye damage, but this was in-frequent.45 The complexity oftreatment required in mustard
injuries involved a new level ofaid and medical care.
Caring for mustard victims dif-fered from caring for chlorine orphosgene casualties. Once evacu-ated, chlorine and phosgene vic-tims received oxygen and bed restuntil they were healthy enoughto return to the front. However,soldiers exposed to mustard gas,especially in high concentrationsor for long periods of time,needed to bathe with hot soapand water to remove the chemi-cal from their skin. If it was notscrubbed off within 30 minutesof exposure, blistering occurred.Portable shower units with spe-cially trained medics helped min-imize its blistering effect. Theseconsisted of a “bath truck [thatwas] provided with [a] hot waterboiler and a number of fold-down shower heads.”46
After the troops showered, thechemical corps issued them newuniforms in exchange for theircontaminated clothing. These dis-carded clothes were then decon-taminated and reissued to otherexposed soldiers. Because mustardgas induced eye injuries, casualties
had their eyes washed as quicklyas possible to minimize the dura-tion of acute conjunctivitis, whichgenerally lasted several weeks.Soldiers’ care became increasinglydifficult in the last year of the warwith the increased frequency ofgas attacks. Also, mustard gasdamaged the lungs more severelythan either chlorine or phosgenedid, and these lesions were muchmore difficult to treat.47 The recu-peration time from mustard gasexposure—46 days—was similar tothat of phosgene.48
Mustard gas was a particularproblem for both sides becauseafter it was released it settled in anarea, contaminating it. The vesi-cant often recontaminated sol-diers and horses in contaminated,unquarantined areas. Cecil With-ers, a British soldier, rememberedbeing exposed to mustard gasduring a mortar attack:
I suffer badly from phlegm andfrom coughs and colds a lot.That all started when the Britishwere shelling hard at the lastBattle of the Somme. One of theshells disturbed the residue ofmustard gas that had been lyingthere for months. They talkabout secondary smoking . . . Igot secondary gas.49
In addition, because mustardgas was heavier than air or water,it settled in ditches or at the bot-tom of trenches and puddles andcreated a persistent environmen-tal hazard for troops, civilians,and animals alike. All a soldierneeded to do was disturb thedirt, mud, or water and he wouldsuffer from gas exposure. Persis-tency was a problem not only onthe battlefield but also for themedical corps. Because of thevolatility of mustard gas, a singlegassed soldier could contaminatemedical personnel, the ambu-lance, and other patients. Themedical corps created a special
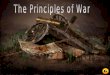
Soldiers from the British 55th (WestLancashire) Division temporarilyblinded by mustard gas nearBethune during the Battle ofEstaires, April 10, 1918.
Source. Photograph by 2nd Lt T. L.Aitken, Imperial War Museum, catalogueno. Q 11586.

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 619
evacuation system to minimizethis type of contamination oncelarge quantities of mustard gaswere used in combat.50
Although new to gas warfare,the United States moved quicklyand used mustard gas offensivelyin June 1918, when US mustardgas production was 30 tons perday. Lewisite, which might havereplaced mustard gas had thewar continued into the winter of1919, was a “superior” weaponthat caused instantaneous blister-ing, was lethal in minute quanti-ties, was relatively difficult to de-tect, and perhaps moreimportantly, had a molecularstructure that allowed rapid dissi-pation. This last factor allowedattacking forces to move intoenemy territory without fear ofcontamination and injury.51
The bloody toll of mustard gasby war’s end is indicative of itsusefulness as an offensiveweapon. Although approximately30% of all war casualties werevictims of gas exposure, morethan 80% of the approximately186000 British chemical casual-ties were caused by mustard gasalone, with a death toll of ap-proximately 2.6%. This ex-tremely large number of casual-ties among well-trained andequipped British troops indicatesthe destructiveness mustardcaused on the battlefield. AEFcombat losses included morethan 52800 battlefield fatalities,with approximately 1500 dyingof gas-related injuries.52 Unfortu-nately, death and injury causedby chemical agents were not re-stricted to the battlefield.
INDUSTRIAL WORKERSCOPE WITH CHEMICALAGENTS
The scale of industrial chemi-cal production during the course
of the war was enormous andwithout precedent. Chemicalcompanies, universities, and gov-ernment laboratories from all thewarring nations labored at greatcost to produce chemicals notonly for traditional war materielsuch as munitions and fuel butalso for a new generation ofweapons. The production of cer-tain chemical weapons was com-plex and often involved the syn-thesis of various chemicalprecursors needed for the com-pletion of a specific chemicalagent. Estimates by historiansand military officials place pro-duction in excess of 124200tons of gas, indicating a substan-tial investment on the part of var-ious governments and chemicalmanufacturers to meet expansivewartime production schedules.53
While thoughts of gas warfareusually bring to mind images ofthe battlefield, the risks and sacri-fices workers made in their homecountries to manufacture wargases was no less valuable and inmany ways presented just asmany, if not more, health risks.
Germany, then the world’sleading chemical manufacturer,produced numerous gas warfaremunitions during the course ofthe war, including more than 33million pounds of gas shells. TheGerman firm Badische Aniline &Soda Fabrik produced the largestquantity of phosgene over thecourse of the war. The company’sready access to carbon monoxidefrom its ammonia plant facili-tated the manufacture of approxi-mately 7200 tons of phosgeneper year. Although Germany out-produced the Allies in phosgeneproduction, the French, British,and Americans all made phos-gene using a variety of tech-niques.54 By 1916, the Germansdeployed diphosgene in artilleryshells at Verdun. It superseded
phosgene in German attackslargely because the diphosgeneshells could be assembled in thefield rather than in distant facto-ries.55
Although postwar investiga-tions on the state of the chemicalindustry during the war invari-ably gave Germany high marksoverall for worker safety, a re-port by Lt Col James F. Norris ofthe US Army Chemical WarfareService on the Bayer Company’sdiphosgene (perchloromethylfor-mate) facility at Höchst notedthat German factory men werefrequently poisoned by gas andthat as many as one third wereabsent from the factory at anygiven time because of gas-relatedillnesses. Norris also suspectedthat several men died from gasexposure at the Höchst plant, butthere was no conclusive proof ofthe linkage between working inthe plant and the men’s deaths.56
Superior plant organization anddesign, however, reduced the riskto some German workers, as didtheir choice of productionmethod, most importantly formustard gas.57
The British and French hadmore difficulty manufacturingchemical agents, especially oncethey started producing mustardgas. Because the Allies used themore dangerous Guthrie’s proc-ess, industrial mustard produc-tion necessitated extra care andstate-of-the-art facilities. HistorianLudwig Haber noted that safeproduction required “the tiledconstruction and plumbing con-struction of a municipal wash-house, the ventilation system ofan up-to-date coal mine, and thenursing facilities of a CCS [casu-alty clearing station] in a quietsector of the front.”58 Because ofthe use of smaller and olderplants, British and French facili-ties often employed primitive

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4620 | Public Health Then and Now | Peer Reviewed | Fitzgerald
open vats and substandard pip-ing. Particularly dangerous jobsincluded cleaning the pipes,which inevitably became blockedduring production, as well as re-pairing pumps and chargingdrums to prepare them for trans-porting various toxic and corro-sive liquids. These industrial con-ditions produced the sameinjuries in civilians as they did insoldiers, leading to high rates ofabsenteeism and eventually to arotational schedule that allowedworkers to have a week off forevery 20 days in the plant.
The effects were even moresevere for mustard plant work-ers: “[W]hatever was touched in-flamed and whatever wasbreathed irritated.”59 Factoryworkers suffered from chronicmustard gas poisoning becauseof long-term exposure; symptomsincluded “listlessness, ‘nervousdebility’ . . . headaches, indigestion,
spasms of the eyelids, breathless-ness, and inability to do a fulldays work.”60 Industrial workerssuffered from frequent cases ofbronchitis, asthma, throat andlung infections, chest and heartproblems, and depression orother recurring but vague ail-ments.61 Many gassed soldiersand factory workers found it dif-ficult to work after the war be-cause of frequent illness and dif-ficulty breathing.
The most dangerous job re-gardless of location involved fill-ing artillery gas shells. This pro-duced even more injuries thannormal chemical production, andGerman workers suffered asmuch as British, French, andAmerican workers.62 Thousandsof workers at British loading fa-cilities were adversely affected;at one facility, one worker innine became ill or was injured,and at another the rate reached
100% of the labor force.63 Thesetypes of recurring injuries amongBritish laborers promptedchanges in the approach of gov-ernment and military planners tothe problem of plant design andworker safety. One of the mostsignificant responses was theTrench Warfare Supply Depart-ment’s appointment of F. Shuffel-botham as acting medical super-visor in charge of all British gasfacilities in July 1916.
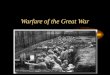
Following the British model,the Americans adopted a morerigorous medical inspection pro-gram to facilitate worker safety.Even before industrial productionbegan, the Bureau of Mines inPittsburgh, Pennsylvania, wascharged with instituting such aprogram. As large-scale productionfacilities came on line, the sur-geon general’s office took over re-sponsibility for workers (Figure 1).They contracted with local physi-cians “whose duty it was to holdsick call, give physical examina-tions at regular intervals, examineapplicants for work in the gasplant, and to be available foremergency calls at all hours.”64
By the end of the war, the pro-duction infrastructure, includingfederal facilities such as the Edge-wood Arsenal in rural Maryland,employed more than 10000 menand women. In addition to Edge-wood, 9 other gas facilities pro-duced over 140 tons of gas perday, “an amount greater than theproduction of Germany, GreatBritain, and France combined.”65
Such mass production quotas,however, were not without risk.An analysis of a single seven-month period at Edgewood re-vealed 925 casualties and threefatalities, with more than 75 in-juries traced directly to mustardgas production.66 For many sol-diers and workers, the long-termhealth consequences of gas
Source. Reprinted from M. W. Ireland, The Medical Department of the United States Army in the World War, Volume XIV: Medical Aspects of GasWarfare (Washington, DC: Government Printing Office, 1926), 34.
FIGURE 1—Diagram illustrating the institutional resources and coordination dedicated to chemicalweapon worker safety.

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 621
exposure were lifelong. As vet-eran Albert Marshal noted:
[T]he gas is still with me today.It makes me itch every morningand at six every night. You cansee my skin all dry. Tonight, myarm will itch from the top to theelbow. And so will the back ofmy neck. It feels like a needlepricking you. And that’s fromninety years ago.67
IN THE SHADOW OF THEGREAT WAR
Although memories of theGreat War have now recededinto the past, chemical warfarehas remained surprisingly re-silient over time. Between the1918 armistice and 1933, severalinternational conferences wereheld to try to limit or abolishchemical weapons; these in-cluded the Washington Confer-ence (1921–1922), the GenevaConference (1923–1925), andthe World Disarmament Confer-ence (1933). Although progresswas made toward outlawing theuse of “asphyxiating, poisonousor other gases” per the GenevaProtocol of 1925, programs andresearch continued throughoutthe interwar period and most ofthe rest of the century, despitethe public’s rejection of theseweapons.68
Although condemned, chemi-cal weapons continued to beused during the interwar years,largely against civilians in colo-nial possessions. The most no-table was the Italian govern-ment’s aerial spraying andbombing of Ethiopian soldiersand civilians during the SecondItalo-Abyssinian War. The Span-ish also used chemical weaponsin Morocco, the British in Russiaand Iraq, and the Japanese inChina, respectively. With theJapanese expansion into China
and the rise of National Socialismin Germany in the 1930s, mostcountries, including the UnitedStates, refused to eliminatechemical weapons as a strategicweapon, although all major com-batants dramatically scaled backtheir programs. The difficulties inregulating chemical weapons areperhaps best illustrated by theactions of the United States. Al-though the United States was asignatory of the Geneva Protocolon June 17, 1925, formal ratifica-tion by the US Senate did notcome until April 10, 1975, al-most 50 years later.
This political ambivalence wasreflective of the ongoing debatesabout chemical weapons re-search and production thatwaxed and waned in the UnitedStates over the rest of the cen-tury. During World War II, for in-stance, the US military was vocalabout its avoidance of the de-ployment or use of poison gas. Atthe same time, however, chemi-cal weapons were a mainstay ofthe Army Air Corps strategicbombing campaigns in both theEuropean and Pacific theaters.69
In less than 3 years, more than220000 tons of chemicallybased munitions such as napalmand magnesium were droppedon civilian targets in both Ger-many and Japan, resulting in thedeaths of hundreds of thousandsof civilians. The air campaigns inWorld War II also reflect the dis-turbing shift in the rise of civiliancasualties during war from alltypes of weapons, a trend thathas increased steadily from the1930s until the present day.70
The commitment to a host oflong-term and large-scale militaryresearch programs during theCold War, involving numerousweapons systems, provided an in-stitutional and financial impetusfor work on a variety of chemical
weapons. In an effort to securetheir position as global super-powers throughout the Cold War,the United States, the SovietUnion, and their various NorthAtlantic Treaty Organization(NATO) and Warsaw Pact alliesdeveloped new chemicalweapons programs based in parton German nerve agents likesarin. To expedite their search fornew agents, the United States,Canada, and Britain entered aTripartite Agreement as early as1946 to share research on offen-sive and defensive aspects ofchemical weapons. Many chemi-cal weapons research programs(such as the US program) oftenworked in tandem with nomi-nally smaller but no less sophisti-cated biological weapons pro-grams, which added a wealth ofdata on complex meteorologicaland delivery system problems.Over time, the increasing sophis-tication of mainstream chemicaland biological weapons in theearly postwar period led to thedevelopment of new generationsof nerve agents.71
By the mid-1950s, the UnitedStates was searching for morepowerful nerve agents; these ef-forts culminated in the develop-ment of VX, which was 3 timesas lethal as sarin and had the ad-ditional tactical utility of battle-field persistence. The United Statescontinued to develop traditionalchemical (and nerve) weaponswell into the late 1960s. At thattime, changes in national securitypolicy, coupled with the ongoingmilitary situation in Vietnam, sawa shift toward partial disarmamentof some types of WMDs with asimultaneous expansion of re-search and development programsfor new weapons.
This schizophrenic policy con-tinued into the1980s, culminat-ing in the creation of a new

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4622 | Public Health Then and Now | Peer Reviewed | Fitzgerald
generation of so called “binary”chemical weapons. Binaryweapons, which used relativelyharmless precursors that chemi-cally combined within a warheadat a designated target, producedvarious toxic agents capable oflarge numbers of mass casualties.The promise of binary weaponscame at a time of increasing polit-ical pressures about the dangersof large-scale chemical warfare.
By the late 1980s, in responseto pressure from the SovietUnion and various NATO allies,the United States began thewholesale destruction of much ofits chemical weapons stockpile(at places such as the army arse-nal at Pine Bluff, Arkansas, andthe Johnson Atoll in the SouthPacific) in an effort to disarm, aswell as destroy older weaponsthat had become unstable. Re-search continued in the UnitedStates on various chemicalweapons systems through the1990s and on into the new mil-lennium. At present, the UnitedStates maintains a large and so-phisticated arsenal of chemicaland nerve agents for tactical andstrategic use.72
The future of these weaponsmay best be understood by re-turning to 2 scientists who hadfirsthand knowledge of their de-velopment and use during WorldWar I.73 Their thoughts both atthe time and years later may bestencapsulate the contested natureof chemical warfare during thelast century. Writing in the late1960s, chemist James Conant,who directed US lewisite produc-tion during World War I, ex-pressed moral ambivalence aboutpoison gas, comparing it toweapons systems in general:
To me, the development of newand more gases seemed no moreimmoral that the manufactureof explosives and guns. . . . I did
not see in 1917 . . . why tearing aman’s guts out by high explosiveshell is to be preferred to maim-ing him by attacking his lungsor skin. All war is immoral.74
Otto Hahn, a future Nobel lau-reate in chemistry, was recruitedby his colleague Fritz Haber tothe German chemical weaponsprogram. Hahn went to the east-ern front to see for himself thecapabilities of this new weapon.The experience left him pro-foundly shaken:
I was very ashamed and deeplyagitated. First we attacked theRussian soldiers with our gas,and then, when we saw thepoor chaps lying on the groundand slowing dying, we restoredtheir breathing with our self-res-cue equipment. The total insan-ity of war became obvious to us.First one attempts to eliminatethe unknown enemy in histrench, but when one comesface to face with him, one can-not bear it and sets about help-ing him. Yet often we could nolonger save the poor victims.75
Whether or not the pragmaticviews of Conant were correct, the“insanity of war” remained a con-stant for the rest of the 20th cen-tury, even as the political meansand technological methods tocarry out war continued toevolve. In the years since the endof the Cold War, the continuedevolution of warfare, coupledwith rapid developments in glob-alization, has made the threat ofchemical warfare more immedi-ate. The increased availability ofvarious industrial chemicals, cou-pled with the expansion of asym-metrical warfare and terrorism,presents us with an uncertain fu-ture. During 2007, chemicalweapons were used in Iraqagainst both civilian populationsand American and British occu-pation forces. The detonation ofeither small chemical bombs orlarge chlorine tanker trucks (with
the aid of explosives) in denselypopulated urban areas such asFallujah and Baghdad createsmany of the same medical re-sponse challenges that confrontedmilitary aid workers and physi-cians almost a century ago. Inmany ways, the world still lives inthe shadow of April 1915.
About the AuthorThe author is a postdoctoral researcherwith New York University, New York, NY.
Requests for reprints should be sent toGerard J. Fitzgerald, PhD, Department ofNutrition, Food Studies and Public Health,New York University, 35 W 4th St, 10thFloor, New York, NY 10012 (e-mail:[email protected]).
This article was accepted June 25,2007.
Endnotes1. On the history of the battle atYpres and its relationship to militaryhistory and the history of science andmedicine, see Jeffery K. Smart, “Historyof Chemical and Biological Warfare: AnAmerican Perspective,” in Medical As-pects of Chemical and Biological Warfare,ed. Frederick R. Sidell, Ernest T. Taka-fuji, and David R. Franz (Washington,DC: Office of the Surgeon General,1997), 15; L.F. Haber, The PoisonousCloud: Chemical Warfare in the FirstWorld War (New York: Clarendon Press,1986), 31–32. On the general topic ofchemical weapons history in the UnitedStates, see Leo B. Brophy, Wyndham D.Miles, and Rexmond C. Cohrane, TheChemical Warfare Service: From Labora-tory to Field (Washington, DC: Office ofthe Chief of Military History, Depart-ment of the Army, 1959); Brooks E.Kleber and Dale Birdsell, The ChemicalWarfare Service: Chemicals in Combat(Washington, DC: Center for MilitaryHistory, United States Army, 2003);Leo P. Brophy and George J.B. Fisher,The Chemical Warfare Service: Organiz-ing for War (Washington, DC: Center ofMilitary History, United States Army,2004). On the cultural, political, andscientific history of chemical warfare inthe Unites States, see Edmund P. RussellIII, “ ‘Speaking of Annihilation’: Mobiliz-ing for War Against Human and InsectEnemies, 1914–1945,” Journal of Amer-ican History 82 (March 1996):1505–1529; see also by Russell, Warand Nature: Fighting Humans and InsectsWith Chemicals From World War I toSilent Spring (New York, NY: CambridgeUniversity Press, 2001); Hugh Slotten,“Humane Chemistry or Scientific Bar-barism? American Responses to World
War I Poison Gas, 1915–1930,” Journalof American History 77 (September1990): 476–498; William L. Sibert,“Chemical Warfare,” Journal of Industrialand Engineering Chemistry 11 (Novem-ber 1919): 1060–1062; Newton D.Baker, “Chemistry in Warfare,” Journalof Industrial and Engineering Chemistry11 (September 1919): 921–923.
2. Robert J.T. Joy, “Historical Aspectsof Medical Defense Against ChemicalWarfare,” in Medical Aspects of Chemicaland Biological Warfare, 90.
3. O.S. Watkins, Methodist Report,cited in Amos Fries and C. J. West,Chemical Warfare (New York: McGrawHill, 1921), 13; also cited in Joy, “His-torical Aspects of Medical Defense,” 90.
4. For a very useful and up-to-dateintroduction to chemical weapons andchemical terrorism, see Jonathan B.Tucker, “Introduction,” in Toxic Terror:Assessing Terror Use of Chemical and Bi-ological Weapons, ed. Jonathan B.Tucker (Cambridge, MA: MIT Press,2000), 3. Tucker further explains thevarious classifications of chemicalagents, which include choking agentsthat damage lung tissue (e.g., chlorine,phosgene), blood agents that interferewith cellular respiration (e.g., hydrogencyanide), blister agents that cause se-vere chemical burns to the skin andlungs (e.g., mustard gas, lewisite), andnerve agents that disrupt nerve-impulsetransmission in the central and periph-eral nervous systems, causing convul-sions and death by respiratory paralysis(e.g., sarin, VX).” Tucker, 33.
5. For an introduction to war, medi-cine, and public health, see War andPublic Health, ed. Barry S. Levy andVictor W. Sidel (Washington, DC: Amer-ican Public Health Association, 2000),especially the following articles: WilliamH. Foege, “Arms and Public Health: AGlobal Perspective” (3–11); Richard M.Garfield and Alfred I. Neugut, “TheHuman Consequences of War” (pp.27–38). On the specific topic of chemi-cal weapons, see Allan H. Lockwood,“The Public Health Effects of the Use ofChemical Weapons,” in War and PublicHealth, 84–97; Challenges in MilitaryHealth Care: Perspectives on Health Statusand the Provision of Care, ed. Jay Stanleyand John D. Blair (New Brunswick, NJ:Transaction Publishers, 1993). On cur-rent military–medical approaches to thethreat of chemical warfare and viablemedical responses to that threat, seeErnest R. Takfuji and Allart B. Kok,“The Chemical Warfare Threat and theMilitary Healthcare Provider,” in Med-ical Aspects of Chemical and BiologicalWarfare, 111–128; Ernest T. Takfuji,Anna Johnson-Winegar, and Russ Za-jtchuk, “Medical Challenges in Chemicaland Biological Defense for the 21st

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 623
Century,” in Medical Aspects of Chemicaland Biological Warfare, 667–686.
6. Historians continue to debate theexact number of casualties incurredduring World War I, because recordkeeping from that period is incompleteand much disputed. Figures vary widelydepending on which sources are usedand how the historian is trying to mea-sure them. In the case of Russia andTurkey, no system for tracking eithermilitary or civilian deaths existed, so itis impossible to determine them withany accuracy. Historian Modris Eksteinsestimates that 9 million died, while his-torian John Keegan places the numberat 10 million and Ian F.W. Becekett at 9million to 10 million. Still others, likeFritz Haber’s son Ludwig Haber, use apercentage of the European populationto estimate the dead. Modris Eksteins,Rites of Spring: The Great War and theBirth of the Modern Age (Boston:Houghton Mifflin, 1989); John Keegan,The First World War (New York: AlfredA. Knopf, 1999); Ian F.W. Beckett, TheGreat War, 1914–1918 (New York:Longman, 2001); Haber, The PoisonousCloud, 31–39.
7. On the use of chemical weapons inthe ancient world, see Adrienne Mayor,Greek Fire, Poison Arrows, and ScorpionBombs: Biological and Chemical Warfarein the Ancient World (New York: Over-look Duckworth, 2003). On uses in the19th century, see Edward M. Spiers,Chemical Warfare (Urbana: University ofIllinois Press, 1986), 13–14. See alsoJoy, “Historical Aspects of Medical De-fense,” 88–90.
8. The full text of the 1899 conven-tion is available at http://www.yale.edu/lawweb/avalon/lawofwar/hague02.htm;the full text of the 1907 convention isavailable at http://www.yale.edu/lawweb/avalon/lawofwar/hague04.htm,both accessed January 15, 2007.
9. Recent interest in the life of Haberincludes 2 new books: Dietrich Stozen-berg, Fritz Haber: Chemist, Nobel Laure-ate, German, Jew (Philadelphia: ChemicalHeritage Press, 2004), and DanielCharles, Master Mind: The Rise and Fallof Fritz Haber, the Nobel Laureate WhoLaunched the Age of Chemical Warfare(New York: Ecco, 2005). For a brief in-tellectual biography of Fritz Haber, seeW.A.E. McBryde, “1918 Nobel LaureateFritz Haber,” in Nobel Laureates inChemistry, 1901–1992, ed. Laylin K.James (Philadelphia: American ChemicalSociety and the Chemical HeritageFoundation, 1993), 114–123.
10. The concept of the “technologicalfix” is embedded in much of the historyof technology. The idea that social, eco-nomic, and cultural problems can besolved quickly by applying technologies
to them is most notably associated withthe development of war technologiessuch as gas weapons, radar, and the gy-roscope. However, as historians ThomasP. Hughes and Wiebe E. Bijker have il-lustrated, technological fixes are also anessential part of electrical systems andmore everyday objects such as bicyclesand light bulbs. On the technologicalfix, see Merritt Roe Smith and LeoMarx, Does Technology Drive History?The Dilemma of Technological Determin-ism (Cambridge, Mass: MIT Press,1996), particularly the introduction. Onthe relationship between Hughes’s con-cepts of the technological fix and tech-nological momentum, see Thomas P.Hughes, Networks of Power: Electrifica-tion in Western Society 1880–1930(Baltimore: Johns Hopkins UniversityPress, 1983), 140–174, 201–226. Fortechnological fixes and large systems,see Hughes, Rescuing Prometheus (NewYork: Pantheon Books, 1998).
11. The mobilization of academic re-sources in Great Britain to solve theproblem of gas warfare reflected theoverall commitment of the country atlarge to prosecuting the war success-fully. Scientists at Birmingham, Cam-bridge, Finsbury Technical College, Im-perial College London, and St. Andrewscarried out specific military researchprograms. Because British soldiers wereinitially unprepared for and unprotectedfrom German gas attacks, defensivemeasures took first priority. The ArmyMedical College at Millbrook took theinitial lead in developing protective de-vices, but soon physiology departmentsat Bedford College, the Lister Institute(including the animal station), OxfordUniversity, the School of Agriculture inCambridge, and University College Lon-don all contributed to the effort. SeeHaber, The Poisonous Cloud, 106–138.
12. For an expansive analysis of indus-trialization in World War I, see Beckett,The Great War. On the relationship be-tween science and technology in WorldWar I in the United States, the bestwork remains Daniel J. Kevles’s ThePhysicists: The History of a ScientificCommunity in Modern America (NewYork: Alfred A. Knopf, 1978); see espe-cially 102–138 and 446–450. See alsoDaniel J. Kevles, “George Ellery Hale,the First World War, and the Advance-ment of Science in America,” Isis 59(1968): 427–437. On the specific topicof research on chemical weapons duringWorld War I, see Daniel P. Jones,“Chemical Warfare Research DuringWorld War I: A Model of CooperativeResearch,” in Chemistry and Modern So-ciety, ed. John Parascondola and JamesC. Whorton (Washington, DC: Ameri-can Chemical Society, 1983). For a gen-eral introduction to the topic of technol-
ogy and war in the United States, seeAlex Roland, “Science and War,” Osiris,1 (1985): 261–261; see also byRoland, “Technology and War: A Biblio-graphic Essay,” in Military Enterpriseand Technological Change: Perspective onthe American Experience, ed. Merritt RoeSmith (Cambridge, MA: MIT Press,1985), 347–379. For a discussion ofmilitary innovation exclusive of chemi-cal warfare in the period immediate fol-lowing World War I, see WilliamsonMurray, “Innovation: Past and Future,”in Military Innovation in the Interwar Pe-riod, ed. Williamson Murray and AllanR. Millet (New York: Cambridge Univer-sity Press, 1996), 300–328. On otheraspects of chemical warfare researchduring the period, see Sarah Jansen,“Chemical-Warfare Techniques for In-sect Control: Insect ‘Pests’ in GermanyBefore and After World War I,” Endeav-our 24 (2000): 28–33.
13. Brophy and Fisher, The ChemicalWarfare Service: Organizing for War, 3.
14. The National Research Council re-port is quoted in Brophy and Fisher,The Chemical Warfare Service, 4.
15. M.W. Ireland, The Medical Depart-ment of the United States Army in theWorld War, Volume XIV: Medical As-pects of Gas Warfare (Washington, DC:Government Printing Office, 1926),35–36. Ireland went on to list the or-ganizations and facilities where war-re-lated research was conducted; these in-cluded “the Bureau of Mines,Pittsburgh, PA; the National Carbon Co.,Cleveland, OH; the Forest Products Lab-oratory, Madison, WI; the University ofChicago; the research laboratory of theAmerican Sheet & Tin Plate Co., Pitts-burgh, PA; the Bureau of Chemistry lab-oratory, Washington, DC; the Yale Med-ical School laboratory, New Haven, CT;the Massachusetts Institute of Technol-ogy, Cambridge, MA; the Mellon Insti-tute, Pittsburgh, PA, and elsewhere. . . .Branch laboratories were organizedfrom time to time at the Catholic Uni-versity of American, Washington, DC;Johns Hopkins University, Baltimore,MD; Princeton University, Princeton,NJ; National Carbon Co., Cleveland,OH; Nela Park, Cleveland, OH; HarvardUniversity, Cambridge, MA; Yale Uni-versity, New Haven, CT; Wesleyan Uni-versity, Middletown, CT; Ohio StateUniversity Columbus, OH; [Bryn MawrCollege,] Bryn Mawr, PA; MassachusettsInstitute of Technology, Cambridge, MA;Cornell University, Ithaca and New YorkCity, NY; University of Michigan, AnnArbor, MI; Clark University, Worcester,MA; Worcester Polytechnic Institute,Worcester, MA; University of Wiscon-sin, Madison, WI; Sprague Institute,Chicago, IL; and Ordnance ProvingGround, Lakehurst, NJ” (35–36). On
the history of American research uni-versities, see Roger L. Geiger, To Ad-vance Knowledge: The Growth of Ameri-can Research Universities in the TwentiethCentury, 1900–1940 (New York: Ox-ford University Press, 1986). For an in-troduction to the history of chemistsand specific scientific research schoolsin the United States, see John Servos,Physical Chemistry From Ostwald to Paul-ing: The Making of a Science in America(Princeton, NJ: Princeton UniversityPress, 1990). See also John Servos, “Re-search Schools and Their Histories,”Osiris 8 (1993): 3–15; Robert E.Kohler, From Medical Chemistry to Bio-chemistry: The Making of a BiomedicalDiscipline (Cambridge, MA: HarvardUniversity Press, 1982).
16. Ireland, Medical Department of theUnited States Army in the World War,35.
17. James Conant became one of thearchitects of the academic–military–in-dustrial complex in the United Statesduring the postwar period. DuringWorld War II, Conant worked closelywith Vannevar Bush in leading the Of-fice of Scientific Research and Develop-ment. Both men were instrumental indirecting much of the country’s militaryresearch during World War II, includingthe Manhattan Project. For a summaryof his research activities during WorldWar I, see James G. Hershberg, James B.Conant: Harvard to Hiroshima and theMaking of the Nuclear Age (New York:Alfred A. Knopf, 1993), 35–48. Seealso James B. Conant, My Several Lives:Memoirs of a Social Inventor (New York:Harper & Row, 1970), especially41–53.
18. Hugh Slotten, “Humane Chemistryor Scientific Barbarism? American Re-sponses to World War I Poison Gas,1915–1930,” Journal of American History77 (September 1990): 485. See also Ire-land, Medical Department of the UnitedStates Army in the World War, 25.
19. Haber, The Poisonous Cloud,107–138.
20. Jon Silkin, The War Poems: WilfredOwen (London: Sinclair-Stevenson,1994), 24. Owen was killed in actionon November 4, 1918 at the Sambre-Oise Canal, a week before the armistice,by bullet, not by gas. For an introduc-tion to the cultural and literary ramifica-tions of Owen's war poetry see: TimKendall, Modern English War Poetry,(New York : Oxford University Press,2006); Daniel W. Hipp, The Poetry ofShell Shock: Wartime Trauma and Heal-ing in Wilfred Owen, Ivor Gurney andSiegfried Sassoon (Jefferson, NC: McFar-land & Co., 2005); and Santanu Das,Touch and intimacy in First World WarLiterature, (New York: Cambridge Uni-versity Press, 2005).

PUBLIC HEALTH THEN AND NOW
American Journal of Public Health | April 2008, Vol 98, No. 4624 | Public Health Then and Now | Peer Reviewed | Fitzgerald
21. On the life of Walther Nerst, seeW.A.E. McBryde, “Walther HermanNernst,” in Nobel Laureates in Chemistry,1901–1992, ed. Laylin K. James(Philadelphia: American Chemical Soci-ety and the Chemical Heritage Founda-tion, 1993), 125–133.
22. William Moore, Gas Attack! Chemi-cal Warfare 1915–1918 and Afterwards(New York: Hippocrene Books, 1987), 12.
23. Haber, The Poisonous Cloud, 51,177.
24. Watkins, Methodist Report.
25. Albert Palazzo, Seeking Victory onthe Western Front: The British Army andChemical Warfare in World War I (Lin-coln: University of Nebraska Press,2000), 42.
26. Max Arthur, Last Post (London:Weidenfeld & Nicolson, 2005), 35–36.See also Palazzo, Seeking Victory on theWestern Front, 42–43.
27. On gas attacks, see B.C. Goss, “AnArtillery Gas Attack,” Journal of Indus-trial and Engineering Chemistry 11 (Sep-tember 1919): 829–836; James C.Webster, “The First Gas Regiment,”Journal of Industrial and EngineeringChemistry 11 (July 1919): 621–629;Army War College, Gas Warfare, Part 2:Methods of Defense Against Gas Attacks(Washington, DC: War Department,1918). For interesting views on gas war-fare from earlier periods, see Edward S.Farrow, Gas Warfare (New York: E.P.Dutton & Company, 1920); War Office,Medical Manual of Chemical Warfare(London: His Majesty’s Stationary Of-fice, 1939); Alden H. Waitt, Gas War-fare: The Chemical Weapon, Its Use, andProtection Against It (New York: Duell,Sloan and Pearce, 1942). On the designof gas masks and respirators, see P.W.Carleton, “Anti-Dimming Compositionsfor Use in the Gas Mask,” Journal of In-dustrial and Engineering Chemistry 11(December 1919): 1105–1111; J. Perrot,Max Yablick, and A.C. Fieldner, “NewAbsorbent for Ammonia Respirators,”Journal of Industrial and EngineeringChemistry 11 (November 1919):1013–1019; Army War College, Meth-ods of Defense Against Gas Attacks. Seealso in that series: Army War College,Gas Warfare, Part 1: German Methods ofOffense (Washington, DC: War Depart-ment, 191 8); Army War College, GasWarfare, Part 3: Methods of Training inDefensive Measures (Washington, DC:War Department, 1918); Army War Col-lege, Gas Warfare, Part 4: The Offensivein Gas Warfare, Cloud and Projector At-tacks (Washington, DC: War Department,1918); Palazzo, Seeking Victory on theWestern Front, 42–43.
28. Palazzo, Seeking Victory on theWestern Front, 43. See also Haber, ThePoisonous Cloud, 46–46.
29. Haber, The Poisonous Cloud, 47.
30. Denis Winter, Death’s Men: Soldiersin the Great War (New York: PenguinBooks, 1979), 124; also cited in Joy,“Historical Aspects of Medical Defense,”92.
31. Arthur, Last Post, 35–36.
32. Joy, “Historical Aspects of MedicalDefense,” 97. For information regardingcurrent military procedures for dealingwith chemical warfare causalities andchemical warfare defense, see the fol-lowing in Medical Aspects of Chemicaland Biological Warfare: Frederick R.Sidell, Ronald R. Bresell, Robert H.Mosebar K Mills McNeill, and Ernest T.Takafuji, “Field Management of Chemi-cal Casualties” (325–336); Frederick R.Sidell, “Triage of Chemical Casualties”(337–350); Charles G. Hurst, “Deconta-mination” (351–360); Michael R. O’H-ern, Thomas R. Dashiell, and MaryFrances Tracy, “Chemical DefenseEquipment” (361–397).
33. Haber suggests that the actual fig-ures were significantly higher; see ThePoisonous Cloud, 248.
34. Joy, “Historical Aspects of MedicalDefense,” 91.
35. The report is quoted in Ireland,Medical Department of the United StatesArmy in the World War, 27.
36. Ibid, 28.
37. Ibid, 28, 33–37.
38. Eksteins, Rites of Spring, 162.
39. Winter, Death’s Men, 121.
40. Quoted in Rexmond C. Cochrane,Third Division at Thierry July, 1918(Army Chemical Center, MD: US ArmyChemical Corps Historical Office, 1959),91.
41. Joy, “Historical Aspects of MedicalDefense,” 94.
42. A 1919 article by B.C. Gross of theChemical Warfare Service recom-mended attacking in wind conditions ofless than 3 miles per hour at a relativehumidity of 40% to 50%. The authornoted that having considered “tempera-ture, wind, and humidity conditions, thehours between midnight and daylightare usually the most favorable for a gasattack, and, in addition, surprise is moreeasily possible at this time.” Successfulgas-based artillery barrages were de-signed to hit “small, definitely locatedtargets known to be occupied [with a]concentrated fire of 2 minutes dura-tion.” B.C. Goss, “An Artillery Gas At-tack,” The Journal of Industrial and Engi-neering Chemistry 11 (September 1919):831.
43. Joy, “Historical Aspects of MedicalDefense,” 100.
44. Harry L. Gilchrist and Philip B.
Matz, The Residual Effects of WartimeGases (Washington, DC: GovernmentPrinting Office; 1933), 44; also cited inJoy, “Historical Aspects of Medical De-fense,” 96.
45. German attacks employing mus-tard gas were extremely difficult for allAllied troops, especially newly arrivingAEF. Unaccustomed to gas attacksunder combat conditions with evenchlorine and phosgene, the AEF movedto the front just as gas warfare enteredits most violent and destructive phase.In addition, an earlier decision byAmerican scientific, medical, and mili-tary leaders to focus almost exclusivelyon the gas mask in lieu of a more com-plete approach to gas defense and treat-ment may have been ill conceived. A1926 US Army medical history of gaswarfare noted that the “Medical Depart-ment of the United States Army with re-spect to gas warfare were [sic] con-cerned with furnishing gas masks andother prophylactic apparatus for theArmy, rather than with preparation forthe care and treatment of gas casual-ties.” Ireland, Medical Department of theUnited States Army in the World War,27.
46. August M. Prentiss, Chemicals inWarfare (New York: McGraw-Hill BookCompany, 1937), 579. On the environ-mental consequences of war, see alsoRichard P. Tucker and Edmund RussellNatural Enemy, Natural Ally: Toward anEnvironmental History of War, ed. (Cor-vallis, OR: Oregon State UniversityPress, 2004).
47. Joy, “Historical Aspects of MedicalDefense,” 98. On the medical aspects ofvesicants in general and mustard gas inparticular, see Frederick R Sidell, JohnS. Urbanetti, William J. Smith, andCharles G. Hurst, “Vesicants,” in MedicalAspects of Chemical and Biological War-fare, 197–228; Frederick R. Sidell andCharles G. Hurst, “Long-Term Heal Ef-fects of Nerve Agents and Mustard,” inMedical Aspects of Chemical and Biologi-cal Warfare, 229–246.
48. Joy, “Historical Aspects of MedicalDefense,” 101.
49. Arthur, Last Post, 83.
50. Joy, “Historical Aspects of MedicalDefense,” 98.
51. For a full history of the develop-ment of lewisite, see Joel A. Vilensky,Dew of Death: The Story of Lewisite,America’s World War I Weapon of MassDestruction (Bloomington: Indiana Uni-versity Press, 2005).
52. These figures are based on HarryL. Gilchrist, A Comparative Study ofWorld War Casualties From Gas andOther Weapons (Edgewood Arsenal,MD: Chemical Warfare School, 1928),p. 21, Table 7.
53. Spiers, Chemical Warfare, 13. Onthe general history of chemical manu-facturing and chemical engineering inthe United States, see John Kenly Smith,Jr, “The Evolution of the Chemical In-dustry: A Technological Perspective,” inChemical Sciences in the Modern World,ed. Seymour H. Mauskopf (Philadelphia:University of Pennsylvania Press, 1993).For a view of chemical engineering ac-tivity during World War I, see CharlesO. Brown, “US Chemical Plant for Man-ufacturing Sodium Cyanide, Saltville,Virginia,” Journal of Industrial and Engi-neering Chemistry 11 (November 1919):1010–1013; James F. Norris, “The Man-ufacture of War Gases in Germany,”Journal of Industrial and EngineeringChemistry 11 (September 1919):817–829; Edward H. Hempel, The Eco-nomics of Chemical Industries (New York:John Wiley & Sons, 1939), 28–31.
54. T. Anthony Ryan, Christien Ryan,Elaine A. Seddon, and Kenneth R. Sed-don, Phosgene and Related CarbonylHalides (New York: Elsever, 1996),12–13.
55. Ibid, 15–16.
56. Norris, “Manufacture of War Gasesin Germany,” 823–824. Norris was oneof a group of Allied officers who touredthe occupied zones along the Rhineafter the war to gather intelligence(both military and industrial) on thestate of the German chemical industry.His report on the Bayer Company plantat Höchst, which manufactured per-chloromethylformate (or superpalite), isintriguing, as it offers a window intoone of the best designed and “safest”chemical production facilities in Ger-many. Norris writes that “In the earlydays they had several small explosionswhich were not serious. They had alarge number of cases of poisoningamong the workmen, which were alsonot serious. All the workers were sup-plied with gas masks and put them onin case of emergency only. The workerssuffered from chest and heart affections.Two or three died during the time [sic]though our informant would not admitthis was necessarily the cause of death.They sometimes had as many as one-third of the workers absent owing tosickness. The workers were not changedas they wished to retain those whocould stand it. Only men were em-ployed in the plant.” Norris, 824.
57. Ibid, 824. See also Haber, The Poi-sonous Cloud, 257–258. The Germanmilitary relied on the methods of VictorMeyer involving the preparation of thio-glycol by the Badische Company, whichwas later converted to mustard gas atthe Bayer Company plant at Höchst.Norris, 821–822.
58. Haber, The Poisonous Cloud, 251.
59. Ibid.

PUBLIC HEALTH THEN AND NOW
April 2008, Vol 98, No. 4 | American Journal of Public Health Fitzgerald | Peer Reviewed | Public Health Then and Now | 625
60. Ibid, 252.
61. Norris, “Manufacture of War Gasesin Germany,” 824. See also Haber, ThePoisonous Cloud, 257–258.
62. Haber, The Poisonous Cloud,250–251.
63. “At first one man reported sick forevery nine shells filled! . . . [B]etween21 June and 7 December 1918, 1,213casualties were recorded, the weeklyrate occasionally reaching 100 per centof the labour force. . . . Avonmouth andChittening between them (there are nofigures for Banbury) reported altogether2,600 gas cases.” Haber, The PoisonousCloud, 251. See also Industrial FatigueResearch Board, The Output of WomenWorkers in Relation to Hours of Work inShell-Making, Report No. 2 (London:His Majesty’s Stationary Office, 1919).
64. Ireland, Medical Department of theUnited States Army in the World War,32–33. The surgeon general’s responsi-bilities involved far more than localplant supervision. They included a re-search service responsible for work onthe “chronic effects of low-concentrationwar gases, protective devices and ther-apy”; a field service responsible forwork on the “selection, appointment,and training of contract surgeons andmedical officers, installation of emer-gency ward[s], dispensary and first-aidequipment, and inspection”; and an ed-ucation service that “collect[ed] reports,case histories, and information,prepar[ed] bulletins of information formedical officers and contracts surgeons,assign[ed] problems for solutions in lab-oratories, and develop[ed] specialcourse[s] of instruction at AmericanUniversity for medical officers, to beused later in factory instruction andassigned to the large plants for duty.”Ibid, 33.
65. Ibid, 25.
66. Haber, The Poisonous Cloud, 252.
67. Arthur, Last Post, 35–36.
68. The text of the Geneva Protocol isavailable from the US Department ofState at http://www.state.gov/t/ac/trt/4784.htm#treaty, accessed January17, 2007. For a detailed examination ofthese international conferences, seeSpiers, Chemical Warfare, 41–47; VictorA Utgoff, The Challenge of ChemicalWeapons: An American Perspective (NewYork: Macmillan, 1990), 14–21.
69. For an introduction to the USstrategic bombing campaigns duringWorld War II and the public healthramifications of large-scale urban de-struction, see Micheal S. Sherry, TheRise of American Air Power: The Creationof Armageddon (New Haven, CT: YaleUniversity Press, 1987); Tami DavisBiddle, “British and American Ap-proaches to Strategic Bombing: Their
Origins and Implementation in theWorld War II Combined Bomber Offen-sive,” in Airpower: Theory and Practice,ed. John Gooch (London, England:Frank Cass & Co, 1995), 91–144; Seealso by Biddle, Rhetoric and Reality inAir Warfare (Princeton, NJ: PrincetonUniversity Press, 2002); HermannKnell, To Destroy a City: Strategic Bomb-ing and Its Human Consequences inWorld War II (Cambridge, MA: DaCapo Press, 2003); Alvin D. Coox,“Strategic Bombing in the Pacific,1942–1945,” in Case Studies in Strate-gic Bombardment, ed. R. Cargill Hall(Washington, DC: Air Force History andMuseums Program, 1998), 253–382;Kenneth Hewitt, “Place Annihilation:Area Bombing and the Fate of UrbanPlaces,” Annals of the Association ofAmerican Geographers 73 (1983):257–284. Finally, it is important tokeep in mind that the US military’s in-vasion plans for Japan (OperationDownfall), originally scheduled to com-mence in November 1945, includedprovisions for the tactical and strategicuse of atomic, biological, and chemicalweapons against various military andcivilian targets.
70. Throughout the 20th century, thenumber of civilian deaths increased at astartling rate. Only 14% of deaths dur-ing World War I were civilians; by con-trast, the rate in World War II was67%; by the 1980s the rate was 75%,and in the 1990s it reached 90%.Garfield and Neugut, “The Human Con-sequences of War,” Table 3–3, 31.
71. On the nature of biologicalweapons programs during World WarII, see Gerard J. Fitzgerald, “Babies, Bar-riers, and Bacteriological Engineers: Bi-ological Warfare Research at LOBUND,1930–1952,” Technology and Culture, inpress; Edward M. Eitzen, “HistoricalOverview of Biological Warfare,” inMedical Aspects of Chemical and Biologi-cal Warfare, 415–423. For an introduc-tion to biological and chemical warfareresearch activities after World War II,see Gradon Carter and Brian Balmer,“Chemical and Biological Warfare andDefence, 1945–1990,” in Cold War,Hot Science: Applied Research in Britain’sDefence Laboratories, 1945–1990, ed.Robert Bud and Philip Gummett (Am-sterdam, The Netherlands: HarwoodAcademic Publishers, 1999), 295–338.See also G.B. Carter and G.S. Pearson,“North Atlantic Chemical and BiologicalResearch Collaboration: 1916–1995,”Journal of Strategic Studies 19 (March1996): 74–103; Mark Wheelis, LajosRózsa, and Malcolm Dando, Deadly Cul-tures: Biological Weapons Since 1945(Cambridge, MA: Harvard UniversityPress, 2006).
72. For a general overview of chemical
weapons development in the UnitedStates, see Smart, “History of Chemicaland Biological Warfare: An AmericanPerspective,” in Medical Aspects ofChemical and Biological Warfare. On thepostwar development of nerve agents,see Frederick R. Sidell, “Nerve Agents,”in Medical Aspects of Chemical and Bio-logical Warfare, 129–179; Michael A.Dunn, Brennie E. Hackley Jr, and Fred-erick R. Sidell, “Pretreatment for NerveAgent Exposure,” in Medical Aspects ofChemical and Biological Warfare,181–196; Jonathan B. Tucker, War ofNerves: Chemical Warfare From WorldWar I to Al-Qaeda (New York: Pan-theon, 2006), 158. For an analysis ofnerve agent development during thecold war, see Bradley S. Davis, “Transi-tional Perspectives on Conventional,Chemical and Biological Weapons Pro-duction,” in United States Post–Cold WarDefense Interests: A Review of the FirstDecade, ed. Karl P. Magyar (New York:Palgrave Macmillan, 2004), 136. For anexamination of contemporary debatesover chemical weapons destruction inrelation to public health, see MichaelGreenberg, “Public Health, Law, andLocal Control: Destruction of the USChemical Weapons Stockpile,” AmericanJournal of Public Health 93 (2003):1222–1226 and Smart, “History ofChemical and Biological Warfare: AnAmerican Perspective.”
73. For fascinating views on the futureof gas warfare as seen by contemporaryobservers during the interwar period,see Edward S. Farrow, Gas Warfare(New York: E.P. Dutton & Company,1920), 166; War College, “Aspects inWhich the Use of Gas Is Likely to Dif-fer in a Future War,” in Medical Manualof Chemical Warfare (London: HisMajesty’s Stationary Office, 1939).
74. James B. Conant, My Several Lives:Memoirs of a Social Inventor (New York:Harper & Row, 1970), 49.
75. Armin Hermann, The New Physics:The Route Into the Atomic Age (Munich:Heinz Moos Verlag, 1979), 47, 73.