Embed Size (px)
Citation preview

Charles Darwin University
Reduced in vitro activity of ceftaroline by Etest among clonal complex 239 methicillin-resistant Staphylococcus aureus clinical strains from Australia
Abbott, I. J.; Jenney, A. W. J.; Jeremiah, Cameron; MirÄeta, M.; Kandiah, J P; Holt, Deborah;Tong, Steven; Spelman, DenisPublished in:Antimicrobial Agents and Chemotherapy
DOI:10.1128/AAC.02015-15
Published: 01/12/2015
Document VersionPeer reviewed version
Link to publication
Citation for published version (APA):Abbott, I. J., Jenney, A. W. J., Jeremiah, C., MirÄeta, M., Kandiah, J. P., Holt, D., ... Spelman, D. (2015).Reduced in vitro activity of ceftaroline by Etest among clonal complex 239 methicillin-resistant Staphylococcusaureus clinical strains from Australia. Antimicrobial Agents and Chemotherapy, 59(12), 7837-7841. DOI:10.1128/AAC.02015-15
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright ownersand it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights.
• Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal
Take down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Download date: 08. Nov. 2018
1
TITLE: Reduced In-Vitro Activity of Ceftaroline by Etest among CC239 Methicillin-1
Resistant Staphylococcus aureus (MRSA) Clinical Strains from Australia. 2
3
RUNNING TITLE: Ceftaroline Resistance in MRSA 4
5 I. J. Abbott1#†, A. W. J. Jenney1, C. J. Jeremiah1‡, M. Mirčeta1, J. P. Kandiah2, D. C. Holt2, S. Y. 6 C. Tong2, and D. W. Spelman1 7
8
1 Alfred Hospital, Melbourne, Victoria, Australia 9
2 Menzies School of Health Research, Charles Darwin University, Darwin, NT, Australia 10
11
†Present address: Victorian Infectious Diseases Reference Laboratory, Victoria. 12
‡Present address: The Northern Hospital, Melbourne, Victoria, Australia 13
14
# CORRESPONDING AUTHOR 15 Name: Dr I. J. Abbott 16 Email: [email protected] 17
AAC Accepted Manuscript Posted Online 21 September 2015Antimicrob. Agents Chemother. doi:10.1128/AAC.02015-15Copyright © 2015, American Society for Microbiology. All Rights Reserved.
2
ABSTRACT 18 421 methicillin-resistant Staphylococcus aureus (MRSA) clinical isolates were tested for 19 ceftaroline susceptibility by Etest (bioMérieux). Multidrug resistant phenotype was 20 found in 40.9% and clonal complex 239 (CC239) in 33.5%. Ceftaroline non-21 susceptibility (MIC >1.0 µg/mL) was 16.9% overall. Non-susceptibility was significantly 22 higher in CC239 (41.1%, 58/141) and isolates with a multidrug resistant phenotype 23 (35.5%, 61/172) when compared to comparators (p<0.0001). Non-susceptibility of 24 common multidrug resistant MRSA clones limits the empirical use of ceftaroline for 25 these infections. 26
3
BODY TEXT 27 Ceftaroline, an oxyimino-cephalosporin active against methicillin-resistant 28
Staphylococcus aureus (MRSA) due to enhanced affinity for Penicillin Binding Protein 29 (PBP) 2a, was approved for use in Australia in 2013 for the treatment of complicated 30 skin and soft-tissue infections (SSTI) and community-acquired bacterial pneumonia 31 (CABP), following approvals for the same indications in the U.S. in 2010 and Europe in 32 2012. S. aureus minimum inhibitory concentration (MIC) breakpoints have been set by 33 Clinical Laboratory Standards Institute (CLSI) (1) and European Committee on 34 Antimicrobial Susceptibility Testing (EUCAST) (2). Both report susceptibility MIC ≤1.0 35 μg/ml, although differ in resistance designation (CLSI, resistant MIC >4.0 μg/ml; 36 EUCAST, resistant MIC >1.0 μg/ml). Resistance appears to be associated with decreased 37 PBP2a binding affinity (3-7) and heteroresistance (8). Reports have largely 38 demonstrated minimal resistance, although geographical variation has been noted (4) 39 (Table 1). More recently, in hospital-associated MRSA (HA-MRSA) isolates from China, 40 ceftaroline non-susceptibility was 33.5% (84/251), most (95.2%) belonging to clonal 41 complex (CC) 8, with sequence type (ST) 239-III in the majority (9). Similarly, 42 ceftaroline non-susceptible MRSA isolates from Eastern Australia were all of the ST239-43 III clone (10). A German study also demonstrated increased ceftaroline MIC50/90 values 44 for isolates of clonal lineages ST228 and ST239 (7). 45
46 Non-duplicate, consecutive clinical MRSA isolates were tested from patients treated at 47 the Alfred Hospital, a tertiary-care metropolitan hospital in Melbourne, Australia, over 48 two time periods; July to December 2010 and August to November 2013. Ceftaroline 49 was not in use clinically before 2014. Isolates from 2010 and 2013 were identified using 50 Vitek 2 and Vitek MS (bioMérieux) respectively. Susceptibility testing was performed 51
4
using the Vitek 2 Gram Positive Susceptibility Card (AST-P612) applying EUCAST 52 breakpoints. Multidrug resistant phenotype was defined as resistance to ≥3 non β-53 lactam antibiotics, including each of ciprofloxacin, erythromycin/clindamycin, 54 gentamicin, cotrimoxazole and tetracycline. All isolates were assessed for ceftaroline 55 and vancomycin susceptibility by Etest (bioMérieux). Isolates from 2010 were thawed 56 from frozen and sub-cultured twice before testing. Isolates from 2013 were collected 57 and tested in real time. Ceftaroline Etests were set up on Mueller Hinton Agar (Becton 58 Dickinson BBL, Ref: 211438), incubated and read as per manufacturer’s guidelines. 59 Ceftaroline non-susceptibility was defined as MIC >1.0 μg/ml. Confirmatory broth 60 microdilution (BMD) was not available. Typing was performed by a high-resolution 61 melting-based method, giving inferred CCs (11). 62 63 421 non-duplicate MRSA isolates were identified for testing. 270 isolates were from 64 2010, and 151 isolates from 2013. SSTI accounted for the majority (70.3%) of 65 specimens. Strains with a multidrug resistant phenotype made up 40.9% of the isolates, 66 although this proportion declined over the two time periods, from 47.0% (127/270) in 67 2010 to 29.8% (24/151) in 2013. CC239, the dominant HA-MRSA strain found in 68 Australia and often multidrug resistant (12), was the most commonly identified clonal 69 complex, accounting for 33.5% of all isolates. This proportion also fell between the two 70 time periods, from 41.5% (112/270) in 2010 to 19.2% (29/151) in 2013. CC22 and 71 CC45 were the next most commonly identified clonal complexes, found in 28.5% and 72 11.4% respectively. The proportion of CC22 isolates increased from 26.7% (72/270) in 73 2010 to 31.8% (48/151) in 2013. Among all MRSA isolates, vancomycin MIC50/90 was 74 1.5 μg/ml. Reduced vancomycin susceptibility (i.e. vancomycin MIC > 1.0 μg/ml) was 75 most common in isolates with a multidrug resistant phenotype (84.9%, 146/172) and 76
5
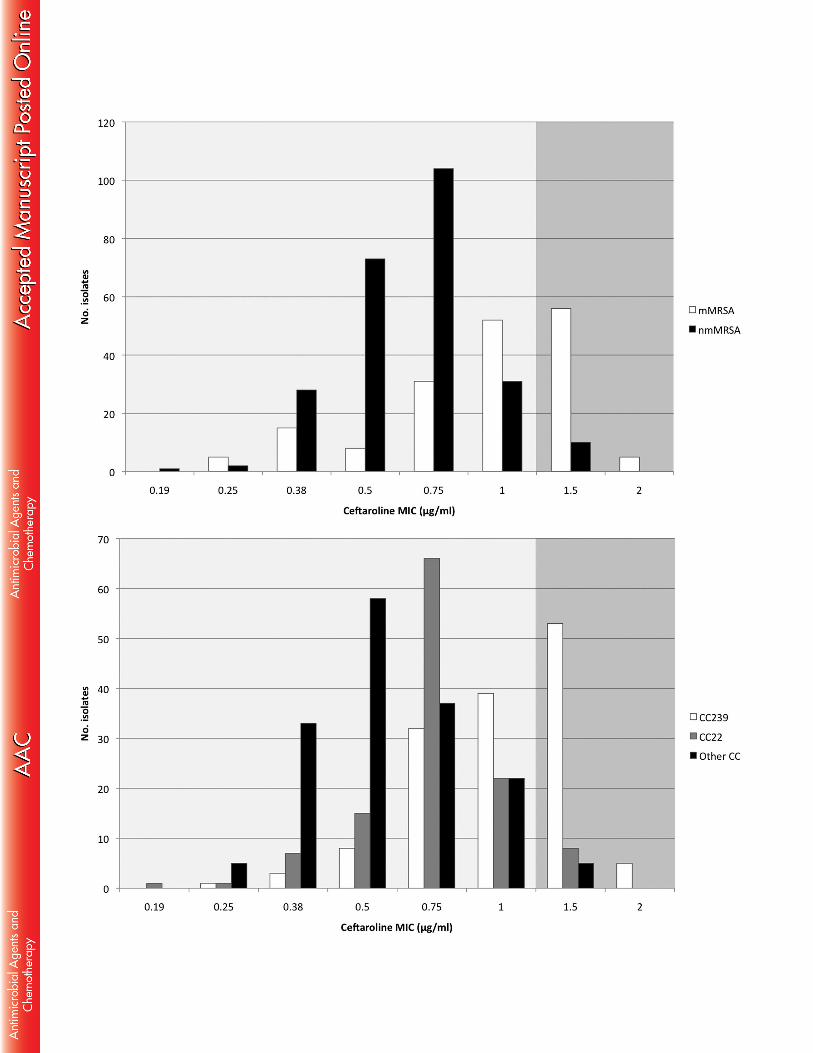
CC239 isolates (83.7%, 118/141), compared with those with a non-multidrug resistant 77 phenotype (32.9%, 82/249), or another CC-type (39.3%, 110/280). 78 79 Overall, ceftaroline MIC50 and MIC90 were 0.75 μg/ml and 1.5 μg/ml, with a non-80 susceptibility rate of 16.9% (71/421). The majority of ceftaroline non-susceptible 81 isolates had a multidrug resistant phenotype (85.9%, 61/71), typed as CC239 (81.7%, 82 58/71) and had a vancomycin MIC > 1.0μg/ml (76.1%, 54/71). All ceftaroline non-83 susceptible isolates had MICs that were either 1.5 µg/mL or 2.0 µg/mL, representing the 84 upper tail of a unimodal distribution, resistant by EUCAST criteria and intermediate by 85 CLSI (Figure 1). Two-sample test of proportions demonstrated that ceftaroline non-86 susceptibility was significantly higher in CC239 MRSA isolates than in non-CC239 87 isolates (58/141, 41.1%; compared to 13/280, 4.6%: p<0.0001). Similarly, ceftaroline 88 non-susceptibility in multidrug resistant MRSA isolates was significantly higher than in 89 non-multidrug resistant isolates (61/172, 35.5%; compared to 10/249, 4.0%: 90 p<0.0001). 91 92 MIC gradient strip testing and disc diffusion remain the most common way for clinical 93 laboratories to test ceftaroline susceptibility in the absence of automated methods and 94 the impracticalities of BMD (13). Ceftaroline gradient strip tests have been reported to 95 underestimate (7), overestimate (14) and demonstrate reasonably good MIC correlation 96 with BMD (10). Livermore et al. report discrimination between MICs of 1.0 and 2.0 97 μg/mL by Etest, compared with agar dilution, was poor (15). Despite this, and 98 differences in clinical breakpoints set by CLSI (1) and EUCAST (2), an Etest ceftaroline 99 MIC of 1.0 μg/ml remains an important and conservative breakpoint for the laboratory 100 to report susceptibility. 101
6
102 The pharmacokinetic and pharmacodynamic index that best correlates with ceftaroline 103 efficacy is the percentage of time during the dosing interval that free-drug 104 concentrations remain above the MIC of the infecting organism (f %T>MIC). In a S. aureus 105 neutropenic murine thigh model, the mean f %T>MIC required for bacterial stasis, 1-log10 106 and 2-log10 kill was 26 ±8, 33 ±9 and 45 ±13, respectively. Less killing was observed 107 with more widely spaced dosing intervals (12- and 24-h)(16). Suggestions that 108 susceptibility test interpretive criteria could be MIC ≤2.0 μg/ml (4, 17) are based on 109 achieving a f %T>MIC target of 26%, reflecting bacterial stasis, and would be considered 110 the minimum value required when treating uncomplicated infections in patients with an 111 intact immune system (18). At MIC of 2.0 μg/ml, standard dosing with 600mg twice 112 daily demonstrated lower target attainments aiming for 1- or 2-log10 kill (74.5% and 113 28.8% respectively, in simulated patients with normal renal function, applying f %T>MIC 114 of 36% and 51% for a 1- and 2-log10 kill, respectively) (17). Monte Carlo simulation with 115 ceftaroline administered 600 mg 8-hourly as a 2 hour infusion in patients with normal 116 renal function demonstrated a higher probability of treatment success (from 72% in 117 CABP and 79% in SSTI to ≥99% in both) and may represent a better option than 118 standard dosing, especially when targeting MRSA (19). In practice, off-label dosing has 119 been commonly reported for serious infections (bacteremia, endocarditis, MRSA 120 pneumonia) with good clinical outcomes, although such dosing risks higher toxicity 121 rates (20). 122 123 Ceftaroline resistance among MRSA isolates from Melbourne, Australia, especially 124 isolates with a multidrug resistant phenotype and the CC239 strain, is significant and 125 would preclude its empirical use prior to dedicated susceptibility testing. Empiric usage 126
7
in other settings should be determined at an individual institutional level. Ceftaroline 127 non-susceptibility has been identified prior to the clinical use of the drug, and therefore 128 does not represent emergence of resistance. Despite the limitations of this study, which 129 might be biased towards hospital-specific clones, or represent the known laboratory 130 issues with gradient strip susceptibility test with the lack of confirmatory BMD testing, 131 our findings linking ceftaroline resistance to multidrug resistance phenotype and CC239 132 is supported by other recently published studies (4, 9, 10). Our results may also 133 represent changes in resistance over time, highlighting the importance of monitoring 134 MRSA molecular epidemiology in order to understand the underlying genetic 135 background to non-susceptibility and the dynamic relationship that is seen between the 136 pathogen and the drug. In regions where CC239 contributes to a large proportion of 137 MRSA, caution should be exercised in using ceftaroline for suspected or known MRSA 138 infections. Although the association of CC239 and multidrug resistant phenotype are 139 inherently linked, the clinical appreciation, at the time of culture result, that a multidrug 140 resistant MRSA isolate has a higher background rate of ceftaroline non-susceptibility, is 141 an important one. Further studies are required on the clinical efficacy and safety of 142 using more intensive ceftaroline dosing regimens in such settings. 143 144
ACKNOWLEDGMENTS 145 The authors acknowledge the laboratory assistance from the Microbiology Department, 146 Alfred Hospital. Funding received from Alfred Research Trusts Small Projects Grants. 147 SYCT is an Australian National Health and Medical Research Council Career 148 Development Fellow (1065736). 149
150
151
8
REFERENCES 152 1. CLSI. Clinical and Laboratory Standards Institute. Performance standards for 153 antimicrobial susceptibility testing; twenty-fifth informational supplement. CLSI 154 document M100-S25. Wayne, PA: Clinical and Laboratory Standards Institute; 155 2015. 156 2. EUCAST. European Committee On Antimicrobial Susceptibility Testing. 157 Breakpoint tables for interpretation of MICs and zone diameters. Version 5.0. 158 European Committee on Antimicrobial Susceptibility Testing 2015. 159 http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_t160 ables/v_5.0_Breakpoint_Table_01.pdf (Accessed 3 Aug 2015). 161 3. Mendes RE, Tsakris A, Sader HS, Jones RN, Biek D, McGhee P, Appelbaum 162
PC, Kosowska-Shick K. 2012. Characterization of methicillin-resistant 163 Staphylococcus aureus displaying increased MICs of ceftaroline. J Antimicrob 164 Chemother 67:1321-1324. 165 4. Lahiri SD, McLaughlin RE, Whiteaker JD, Ambler JE, Alm RA. 2015. Molecular 166 characterization of MRSA isolates bracketing the current EUCAST ceftaroline-167 susceptible breakpoint for Staphylococcus aureus: the role of PBP2a in the 168 activity of ceftaroline. J Antimicrob Chemother doi:10.1093/jac/dkv131. 169 5. Kelley WL, Jousselin A, Barras C, Lelong E, Renzoni A. 2015. Missense 170 mutations in PBP2A Affecting ceftaroline susceptibility detected in epidemic 171 hospital-acquired methicillin-resistant Staphylococcus aureus clonotypes ST228 172 and ST247 in Western Switzerland archived since 1998. Antimicrob Agents 173 Chemother 59:1922-1930. 174

9
6. Chan LC, Basuino L, Diep B, Hamilton S, Chatterjee SS, Chambers HF. 2015. 175 Ceftobiprole- and ceftaroline-resistant methicillin-resistant Staphylococcus 176 aureus. Antimicrob Agents Chemother 59:2960-2963. 177 7. Strommenger B, Layer F, Klare I, Werner G. 2015. Pre-Use Susceptibility to 178 Ceftaroline in Clinical Staphylococcus aureus Isolates from Germany: Is There a 179 Non-Susceptible Pool to be Selected? PLoS One 10:e0125864. 180 8. Saravolatz SN, Martin H, Pawlak J, Johnson LB, Saravolatz LD. 2014. 181 Ceftaroline-heteroresistant Staphylococcus aureus. Antimicrob Agents 182 Chemother 58:3133-3136. 183 9. Zhang H, Xiao M, Kong F, O'Sullivan MV, Mao LL, Zhao HR, Zhao Y, Wang H, 184
Xu YC. 2015. A multicentre study of meticillin-resistant Staphylococcus aureus in 185 acute bacterial skin and skin-structure infections in China: susceptibility to 186 ceftaroline and molecular epidemiology. Int J Antimicrob Agents 45:347-350. 187 10. Mubarak N, Sandaradura I, Isaia L, O'Sullivan M, Zhou F, Marriott D, Iredell 188
JR, Harkness J, Andresen D. 2015. Non-susceptibility to ceftaroline in 189 healthcare-associated multiresistant MRSA in Eastern Australia. J Antimicrob 190 Chemother 70:2413-2414. 191 11. Lilliebridge RA, Tong SY, Giffard PM, Holt DC. 2011. The utility of high-192 resolution melting analysis of SNP nucleated PCR amplicons--an MLST based 193 Staphylococcus aureus typing scheme. PLoS One 6:e19749. 194 12. Coombs G, Pearson J, Nimmo G, Collignon P, Bell J, McLaws ML, Christiansen 195
K, Turnidge J, Resistance AGfA. 2013. Antimicrobial susceptibility of 196 Staphylococcus aureus and molecular epidemiology of methicillin-resistant S. 197 aureus isolated from Australian hospital inpatients: report from the Australian 198
10
Group on Antimicrobial Resistance 2011 Staphylococcus aureus Surveillance 199 Programme. J Glob Antimicrob Resist 1:149-156. 200 13. Jones RN, Holliday NM, Critchley IA. 2015. Accuracy of the Thermo Fisher 201 Scientific (Sensititre) dry-form broth microdilution MIC product when testing 202 ceftaroline. Diagn Microbiol Infect Dis 81:280-282. 203 14. Espedido BA, Jensen SO, van Hal SJ. 2015. Ceftaroline fosamil salvage therapy: 204 an option for reduced-vancomycin-susceptible MRSA bacteraemia. J Antimicrob 205 Chemother 70:797-801. 206 15. Livermore DM, Mushtaq S, Warner M, James D, Woodford N. 2015. 207 Susceptibility testing challenges with ceftaroline, MRSA and a 1 mg/L 208 breakpoint. J Antimicrob Chemother doi:10.1093/jac/dkv265. 209 16. Andes D, Craig WA. 2006. Pharmacodynamics of a new cephalosporin, PPI-0903 210 (TAK-599), active against methicillin-resistant Staphylococcus aureus in murine 211 thigh and lung infection models: identification of an in vivo pharmacokinetic-212 pharmacodynamic target. Antimicrob Agents Chemother 50:1376-1383. 213 17. Van Wart SA, Ambrose PG, Rubino CM, Khariton T, Riccobene TA, Friedland 214
HD, Critchley IA, Bhavnani SM. 2014. Pharmacokinetic-pharmacodynamic 215 target attainment analyses to evaluate in vitro susceptibility test interpretive 216 criteria for ceftaroline against Staphylococcus aureus and Streptococcus 217 pneumoniae. Antimicrob Agents Chemother 58:885-891. 218 18. Mouton JW, Brown DF, Apfalter P, Canton R, Giske CG, Ivanova M, 219
MacGowan AP, Rodloff A, Soussy CJ, Steinbakk M, Kahlmeter G. 2012. The 220 role of pharmacokinetics/pharmacodynamics in setting clinical MIC breakpoints: 221 the EUCAST approach. Clin Microbiol Infect 18:E37-45. 222

11
19. Canut A, Isla A, Rodriguez-Gascon A. 2015. 223 Pharmacokinetic/pharmacodynamic analysis to evaluate ceftaroline fosamil 224 dosing regimens for the treatment of community-acquired bacterial pneumonia 225 and complicated skin and skin-structure infections in patients with normal and 226 impaired renal function. Int J Antimicrob Agents 45:399-405. 227 20. Stryjewski ME, Jones RN, Corey GR. 2015. Ceftaroline: clinical and 228 microbiology experience with focus on methicillin-resistant Staphylococcus 229 aureus after regulatory approval in the USA. Diagn Microbiol Infect Dis 81:183-230 188. 231 21. Jones RN, Mendes RE, Sader HS. 2010. Ceftaroline activity against pathogens 232 associated with complicated skin and skin structure infections: results from an 233 international surveillance study. J Antimicrob Chemother 65 Suppl 4:iv17-31. 234 22. Jones RN, Farrell DJ, Mendes RE, Sader HS. 2011. Comparative ceftaroline 235 activity tested against pathogens associated with community-acquired 236 pneumonia: results from an international surveillance study. J Antimicrob 237 Chemother 66 Suppl 3:iii69-80. 238 23. Farrell DJ, Castanheira M, Mendes RE, Sader HS, Jones RN. 2012. In vitro 239 activity of ceftaroline against multidrug-resistant Staphylococcus aureus and 240 Streptococcus pneumoniae: a review of published studies and the AWARE 241 Surveillance Program (2008-2010). Clin Infect Dis 55 Suppl 3:S206-214. 242 24. Sader HS, Flamm RK, Jones RN. 2013. Antimicrobial activity of ceftaroline 243 tested against staphylococci with reduced susceptibility to linezolid, daptomycin, 244 or vancomycin from U.S. hospitals, 2008 to 2011. Antimicrob Agents Chemother 245
57:3178-3181. 246

12
25. Richter SS, Heilmann KP, Dohrn CL, Riahi F, Costello AJ, Kroeger JS, Biek D, 247
Critchley IA, Diekema DJ, Doern GV. 2011. Activity of ceftaroline and 248 epidemiologic trends in Staphylococcus aureus isolates collected from 43 249 medical centers in the United States in 2009. Antimicrob Agents Chemother 250
55:4154-4160. 251 26. Karlowsky JA, Adam HJ, Decorby MR, Lagace-Wiens PR, Hoban DJ, Zhanel 252
GG. 2011. In vitro activity of ceftaroline against gram-positive and gram-negative 253 pathogens isolated from patients in Canadian hospitals in 2009. Antimicrob 254 Agents Chemother 55:2837-2846. 255 27. Flamm RK, Sader HS, Jones RN. 2014. Ceftaroline activity against organisms 256 isolated from respiratory tract infections in USA hospitals: results from the 257 AWARE Program, 2009-2011. Diagn Microbiol Infect Dis 78:437-442. 258 28. Pfaller MA, Flamm RK, Sader HS, Jones RN. 2014. Ceftaroline activity against 259 bacterial organisms isolated from acute bacterial skin and skin structure 260 infections in United States medical centers (2009-2011). Diagn Microbiol Infect 261 Dis 78:422-428. 262 29. Sader HS, Flamm RK, Streit JM, Farrell DJ, Jones RN. 2015. Ceftaroline activity 263 against bacterial pathogens frequently isolated in U.S. medical centers: results 264 from five years of the AWARE surveillance program. Antimicrob Agents 265 Chemother 59:2458-2461. 266 30. Sader HS, Farrell DJ, Flamm RK, Jones RN. 2015. Activity of ceftaroline and 267 comparator agents tested against Staphylococcus aureus from patients with 268 bloodstream infections in US medical centres (2009-13). J Antimicrob 269 Chemother 70:2053-2056. 270
13
31. Flamm RK, Sader HS, Farrell DJ, Jones RN. 2012. Summary of ceftaroline 271 activity against pathogens in the United States, 2010: report from the Assessing 272 Worldwide Antimicrobial Resistance Evaluation (AWARE) surveillance program. 273 Antimicrob Agents Chemother 56:2933-2940. 274 32. Farrell DJ, Flamm RK, Sader HS, Jones RN. 2013. Spectrum and potency of 275 ceftaroline tested against leading pathogens causing skin and soft-tissue 276 infections in Europe (2010). Int J Antimicrob Agents 41:337-342. 277 33. Sader HS, Flamm RK, Jones RN. 2013. Antimicrobial activity of ceftaroline and 278 comparator agents tested against bacterial isolates causing skin and soft tissue 279 infections and community-acquired respiratory tract infections isolated from the 280 Asia-Pacific region and South Africa (2010). Diagn Microbiol Infect Dis 76:61-68. 281 34. Sader HS, Flamm RK, Jones RN. 2013. Antimicrobial activity of ceftaroline-282 avibactam tested against clinical isolates collected from U.S. Medical Centers in 283 2010-2011. Antimicrob Agents Chemother 57:1982-1988. 284 35. Flamm RK, Farrell DJ, Sader HS, Jones RN. 2014. Antimicrobial activity of 285 ceftaroline combined with avibactam tested against bacterial organisms isolated 286 from acute bacterial skin and skin structure infections in United States medical 287 centers (2010-2012). Diagn Microbiol Infect Dis 78:449-456. 288 36. Flamm RK, Sader HS, Jones RN. 2014. Ceftaroline activity tested against 289 contemporary Latin American bacterial pathogens (2011). Braz J Infect Dis 290
18:187-195. 291 37. Richter SS, Diekema DJ, Heilmann KP, Dohrn CL, Crispell EK, Riahi F, 292
McDanel JS, Satola SW, Doern GV. 2014. Activities of vancomycin, ceftaroline, 293 and mupirocin against Staphylococcus aureus isolates collected in a 2011 294
14
national surveillance study in the United States. Antimicrob Agents Chemother 295
58:740-745. 296 38. Livermore DM, Mushtaq S, Warner M, James D, Kearns A, Woodford N. 2015. 297 Pathogens of skin and skin-structure infections in the UK and their susceptibility 298 to antibiotics, including ceftaroline. J Antimicrob Chemother 299 doi:10.1093/jac/dkv179. 300 39. Leprince C, Desroches M, Emirian A, Coutureau C, Anais L, Fihman V, Soussy 301
CJ, Decousser JW, group Ps. 2015. Distribution and antimicrobial susceptibility 302 of bacteria from adults with community-acquired pneumonia or complicated 303 skin and soft tissue infections in France: the nationwide French PREMIUM study. 304 Diagn Microbiol Infect Dis doi:10.1016/j.diagmicrobio.2015.06.007. 305 40. Sader HS, Farrell DJ, Mendes RE, Flamm RK, Castanheira M, Jones RN. 2015. 306 Antimicrobial activity of ceftaroline tested against bacterial isolates causing 307 respiratory tract and skin and skin structure infections in US medical centers in 308 2013. Diagn Microbiol Infect Dis 82:78-84. 309 41. Basireddy S, Singh M, Ali S, Kabra V. 2015. In vitro activity of ceftaroline 310 against methicillin-resistant Staphylococcus aureus isolates. Indian J Med 311 Microbiol 33:464-465. 312
15
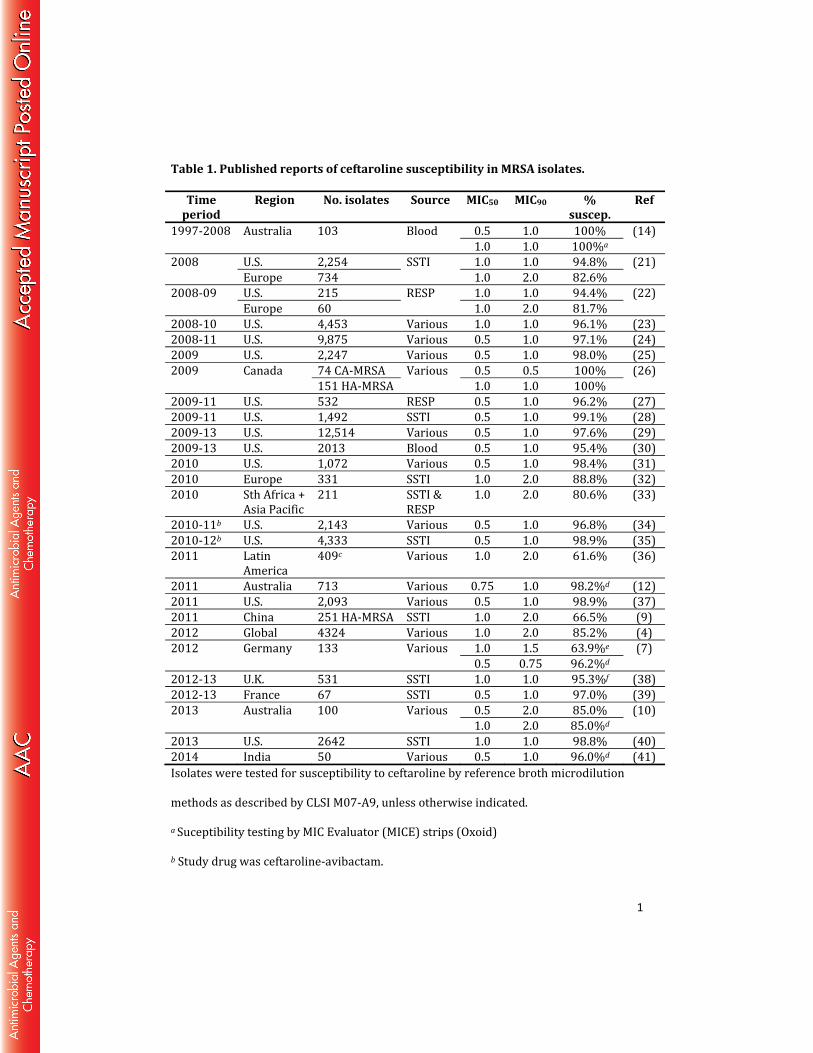
Table 1. Published reports of ceftaroline susceptibility in MRSA isolates. 313 314 Isolates were tested for susceptibility to ceftaroline by reference broth microdilution 315 methods as described by CLSI M07-A9, unless otherwise indicated. 316
a Suceptibility testing by MIC Evaluator (MICE) strips (Oxoid) 317
b Study drug was ceftaroline-avibactam. 318
c Includes isolates from Chile of which 83.9% had an ceftaroline MIC of 2.0µg/ml. 319
d Suceptibility testing by Etest (bioMérieux) 320
e Broth microdilution methods as described by EUCAST 321
f Broth microdilution methods as described by BSAC 322 CA-MRSA, community-associated MRSA. 323 HA-MRSA, healthcare-associated MRSA. 324 SSTI, skin and soft tissue infection. 325 RESP, respiratory. 326

16
Figure 1. Ceftaroline MIC distributions in relation to antibiotic susceptibility 327
phenotype and clonal complex (CC). 328
329 Dark shaded area represents ceftaroline non-susceptible MIC range. 330 nmMRSA, non-multidrug resistant MRSA phenotype. 331 mMRSA, multidrug resistant MRSA phenotype. 332 CC239, clonal complex 239 strain. 333 CC22, clonal complex 22 strain. 334
1
Table 1. Published reports of ceftaroline susceptibility in MRSA isolates. Time
period Region No. isolates Source MIC50 MIC90 % suscep. Ref1997-2008 Australia 103 Blood 0.5 1.0 100% (14)1.0 1.0 100%a 2008 U.S. 2,254 SSTI 1.0 1.0 94.8% (21)Europe 734 1.0 2.0 82.6% 2008-09 U.S. 215 RESP 1.0 1.0 94.4% (22)Europe 60 1.0 2.0 81.7% 2008-10 U.S. 4,453 Various 1.0 1.0 96.1% (23)2008-11 U.S. 9,875 Various 0.5 1.0 97.1% (24)2009 U.S. 2,247 Various 0.5 1.0 98.0% (25)2009 Canada 74 CA-MRSA Various 0.5 0.5 100% (26)151 HA-MRSA 1.0 1.0 100% 2009-11 U.S. 532 RESP 0.5 1.0 96.2% (27)2009-11 U.S. 1,492 SSTI 0.5 1.0 99.1% (28)2009-13 U.S. 12,514 Various 0.5 1.0 97.6% (29)2009-13 U.S. 2013 Blood 0.5 1.0 95.4% (30)2010 U.S. 1,072 Various 0.5 1.0 98.4% (31)2010 Europe 331 SSTI 1.0 2.0 88.8% (32)2010 Sth Africa + Asia Pacific 211 SSTI & RESP 1.0 2.0 80.6% (33)2010-11b U.S. 2,143 Various 0.5 1.0 96.8% (34)2010-12b U.S. 4,333 SSTI 0.5 1.0 98.9% (35)2011 Latin America 409c Various 1.0 2.0 61.6% (36)2011 Australia 713 Various 0.75 1.0 98.2%d (12)2011 U.S. 2,093 Various 0.5 1.0 98.9% (37)2011 China 251 HA-MRSA SSTI 1.0 2.0 66.5% (9)2012 Global 4324 Various 1.0 2.0 85.2% (4)2012 Germany 133 Various 1.0 1.5 63.9%e (7)0.5 0.75 96.2%d 2012-13 U.K. 531 SSTI 1.0 1.0 95.3%f (38)2012-13 France 67 SSTI 0.5 1.0 97.0% (39)2013 Australia 100 Various 0.5 2.0 85.0% (10)1.0 2.0 85.0%d 2013 U.S. 2642 SSTI 1.0 1.0 98.8% (40)2014 India 50 Various 0.5 1.0 96.0%d (41)Isolates were tested for susceptibility to ceftaroline by reference broth microdilution methods as described by CLSI M07-A9, unless otherwise indicated.
a Suceptibility testing by MIC Evaluator (MICE) strips (Oxoid) b Study drug was ceftaroline-avibactam.

2
c Includes isolates from Chile of which 83.9% had an ceftaroline MIC of 2.0µg/ml. d Suceptibility testing by Etest (bioMérieux) e Broth microdilution methods as described by EUCAST f Broth microdilution methods as described by BSAC CA-MRSA, community-associated MRSA. HA-MRSA, healthcare-associated MRSA. SSTI, skin and soft tissue infection. RESP, respiratory.