Embed Size (px)
Citation preview

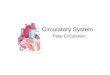
Chapter 34
Christine Limann Dyer, RN, BS CPN

Umbilical vein, umbilical arteries
Foramen ovale Ductus
arteriosus Ductus venosus
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 2

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 3

Poor feeding Tachypnea/tachycardia Failure to thrive/poor weight
gain/activity intolerance Developmental delays Prenatal history Family history of cardiac disease
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 4

Murmurs = heart sounds that reflect flow of blood within the heartMay occur in systole or diastole, or bothCan occur in a normal heart in periods of stress:
anemia, fever, or rapid growthCan reflect abnormalities in heart or vessels
“Innocent murmurs” = normal cardiac anatomy and cardiac functionOccur in up to 50% of all kids at some time
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 5

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 6

Chest x-ray ECG Echocardiograph
y Cardiac
catheterization
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 7

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 8

Transposition of great vessels
Some complex single-ventricle defects
ASD Pulmonary
artery stenosis
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 9

DIAGNOSISDIAGNOSIS INTERVENTIONINTERVENTION
Valvular pulmonic stenosisValvular pulmonic stenosis Balloon dilationBalloon dilation
Recurrent coarctation of aortaRecurrent coarctation of aorta Balloon dilationBalloon dilation
Congenital mitral stenosisCongenital mitral stenosis Balloon dilationBalloon dilation
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc. Slide 10

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 11

CongenitalAnatomic → abnormal function
AcquiredDisease process
Infection Autoimmune response Environmental factors Familial tendencies
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 12

Maternal or environmental = 1% to 2%Maternal drug use
Fetal alcohol syndrome—50% have CHDMaternal illness
Rubella in first 7 weeks of pregnancy → 50% risk of defects including PDA and pulmonary branch stenosis
CMV, toxoplasmosis, other viral illnesses → cardiac defects
IDMs (infant of diabetic mother) = 10% risk of CHD (VSD, cardiomyopathy, TGA most common)
Chromosomal/genetic = 10% to 12% Multifactorial = 85%
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 13

Incidence: 5 to 8 per 1000 live births About 2 or 3 of these are symptomatic in
first year of lifeMajor cause of death in first year of life
(after prematurity)Most common anomaly is VSD28% of kids with CHD have another
recognized anomaly (trisomy 21, 13, 18, + + + )
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 14

AcyanoticMay become
cyanotic Cyanotic
May be pinkMay develop CHF
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 15

Hemodynamic characteristics Increased pulmonary blood flowDecreased pulmonary blood flowObstruction of blood flow out of the heartMixed blood flow
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 16

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 17

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 18

Abnormal connection between two sides of heartEither the septum or the great vessels
Increased blood volume on right side of heart
Increased pulmonary blood flow Decreased systemic blood flow
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 19

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 20

Atrial septal defect Ventricular septal defect Patent ductus arteriosus
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 21

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 22

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 23

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 24

Coarctation of the aorta Aortic stenosis Pulmonic stenosis
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 25

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 26

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 27

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 28

Tetralogy of Fallot(T.O.F.) Tricuspid atresia
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 29

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 30

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 31
Place in thisPosition
During Tet spell

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 32

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 33

Transposition of great vessels Total anomalous pulmonary venous
connection Hypoplastic heart syndrome
RightLeft
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 34

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 35

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 36

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 37

Impaired myocardial functionTachycardia; fatigue; weakness; restless,
pale, cool extremities; decreased BP; decreased urine output
Pulmonary congestion Tachypnea, dyspnea, respiratory
distress, exercise intolerance, cyanosis Systemic venous congestion
Peripheral and periorbital edema, weight gain, ascites, hepatomegaly, neck vein distention
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 38

Help family adjust to the disorder
Educate family Help family cope
with effects of the disorder
Prepare child and family for surgery
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 39

Open heart Closed heart
procedures Staged
procedures Prepare child
and family for procedures
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 40

Monitor vital signs and A/V pressures
Intra-arterial monitoring of BP
Intracardiac monitoring Respiratory needs Rest, comfort, and pain
management Fluid management Progression of activity
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 41

CHF Dysrhythmias Decreased cardiac output syndrome Decreased peripheral perfusion Pulmonary changes Neurologic changes
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 42

Symptoms: fever, WBCs, pericardial friction rub, pericardial and pleural effusion
Occurs in immediate postoperative period Also can occur later (days 7 to 21 postop) Etiology unknown Theories of etiology
Viral infection, autoimmune response, reaction to blood in pericardium
May require pericardiocentesis or pleurocentesis
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 43

Infectious and inflammatory cardiac disorders
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 44

BE, IE, or SBE Streptococci Staphylococci Fungal infections Prophylaxis: 1
hour before procedures (IV) or may use PO in some cases
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 45

RF Inflammatory disease occurs after
group A β-hemolytic streptococcal pharyngitis
Infrequently seen in U.S.; big problem in Third World
Self-limiting Affects joints, skin, brain, serous surfaces,
and heart Carditis Polyarthritis Erythema marginatum Subcutaneous nodules
Rheumatic heart disease Most common complication of RF Damage to valves as result of RFMosby items and derived items © 2007, 2003 by Mosby, Inc., an
affiliate of Elsevier Inc.Slide
46

St. Vitus dance (aka, chorea) reflects CNS involvement
Definition: Chorea refers to sudden, aimless movements of extremities, involuntary facial grimaces, speech disturbances, emotional lability and muscle weaknessWorse with anxiety and
relieved by restMosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 47

Treatment of streptococcal tonsillitis/pharyngitis Penicillin G—IM x 1Penicillin V—oral x 10 daysSulfa—oral x 10 daysErythromycin (if allergic to above)—oral x
10 days Treatment of recurrent RF
Same as above
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 48

IV IgG ASA 80-100
mg/kg/day—fever
Then 3-5 mg/kg/day—antiplatelet
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 49

Primary = no known cause Secondary = identifiable cause Pediatrics: HTN generally secondary to
structural abnormality or underlying pathologyRenal diseaseCV diseaseEndocrine or neurologic disorders
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 50

Identify kids at risk and treat early Treatment = dietary
Restrict intake of cholesterol and fats If no response to diet → Rx
Colestipol (Colestid)Cholestyramine (Questran)
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 51

Contractibility of myocardium is impaired
Secondary cardiomyopathy
Dilated cardiomyopathy
Hypertrophic cardiomyopathy
Restrictive cardiomyopathy
Treatment Correct underlying
cause if possible Often treatment is
aimed at managing CHF and dysrhythmias
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 52

Digoxin Diuretics Beta blockers, calcium channel blockers Dobutamine Nitroprusside Amrinone
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 53

IV IgG Digoxin (Lanoxin) ACE inhibitors ASA, NSAIDs Lasix Spironolactone (Aldactone)
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 54

Diagnostic evaluationECGHolter monitoringElectrophysiologic cardiac catheterTransesophageal recording
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 55

BradydysrhythmiasAV blockMay use pacemaker
TachydysrhythmiasSVT most common tachydysrhythmiaTreatments
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 56

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 57

Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 58

Orthotopic transplant Heterotopic transplant
(piggyback) Organ donation issues Nursing considerations
Mosby items and derived items © 2007, 2003 by Mosby, Inc., an affiliate of Elsevier Inc.
Slide 59

THE CHILD WITH GASTROINTESTINAL DYSFUNCTION
Chapter 33
Christine Limann Dyer, RN, BSE, CPN

DIGESTION
Required to convert nutrients into usable energy
Performs excretory function and detoxification
Mechanical digestion Chemical digestion

ABSORPTION
Principally from small intestine Osmosis Carrier-mediated diffusion Active energy-driven transport (“pump”)
Large intestine Absorption of water Absorption of sodium Role of colonic bacteria

INGESTION OF FOREIGN SUBSTANCES
Pica Food picas Nonfood picas
Foreign bodies Nursing
considerations

DISORDERS OF MOTILITY

CONSTIPATION
An alteration in the frequency, consistency, or ease of passage of stool
May be secondary to other disorders
Idiopathic (functional) constipation—no known cause
Chronic constipation—may be due to environmental or psychosocial factors

NEWBORN PERIOD
First meconium should be passed within 24 to 36 hours of life; if not assess for: Hirschsprung disease, hypothyroidism Meconium plug, meconium ileus (CF)

INFANCY
Often related to diet Constipation in exclusively breastfed infant
almost unknown Infrequent stool may occur because of minimal
residue from digested breast milk Formula-fed infants may develop
constipation Interventions
- adding cereals, fruits and vegetables may help
(after 4 months)

CONSTIPATION IN CHILDHOOD
Often due to environmental changes or control over body functions
Encopresis: inappropriate passage of feces, often with soiling
May result from stress Management

NURSING CONSIDERATIONS
History of bowel patterns, medications, diet Educate parents and child Dietary modifications (age appropriate)

HIRSCHSPRUNG DISEASE
Also called congenital aganglionic megacolon Mechanical obstruction from inadequate
motility of intestine Incidence: 1 in 5000 live births; more
common in males and in Down syndrome Absence of ganglion cells in colon

HIRSCHSPRUNG DISEASE

CLINICAL MANIFESTATIONS OF HIRSCHPRUNG DISEASE
Aganglionic segment usually includes the rectum and proximal colon
Accumulation of stool with distention Failure of internal anal sphincter to relax Enterocolitis may occur

DIAGNOSTIC EVALUATION
X-ray, barium enema Anorectal manometric exam Confirm diagnosis with rectal biopsy

THERAPEUTIC MANAGEMENT
Surgery Two stages
Temporary ostomy Second stage “pull-through”
procedure
Preoperative carePostoperative care
Discharge care

GASTROESOPHAGEAL REFLUX (GER)
Defined as transfer of gastric contents into the esophagus
Occurs in everyone Frequency and persistency may make it
abnormal May occur without GERD GERD may occur without regurgitation

GER
Diagnostics Therapeutic management Nursing considerations

IRRITABLE BOWEL SYNDROME (IBS)
Identified as cause of recurrent abdominal pain in children (Chapter 18)
Classified as a functional GI disorder Alternating diarrhea and constipation Therapeutic management Nursing considerations

ACUTE APPENDICITIS
Etiology and pathophysiology Diagnostic evaluation Therapeutic management
Ruptured appendix Prognosis
Nursing considerations

MECKEL DIVERTICULUM
Most common congenital malformation of the GI tract
Occurs in 1% to 3% of population Pathophysiology Diagnostic evaluation Therapeutic management Nursing considerations

ULCERATIVE COLITIS (UC)
Pathophysiology –inflamation in colon and rectum
Clinical manifestations – ulceration, bleeding, anorexia, anemia

CROHN’S DISEASE
Pathophysiology-Crohn's disease is an inflammatory bowel disease (IBD)
Clinical manifestations-abdominal pain, severe diarrhea and even malnutrition
Extraintestinal manifestations-arthritis, skin problems, fever, anemia
Therapeutic management Medical- corticosteriods,
Remicade for remission, 6-MP
Surgical Nursing considerations – nutritional support,
education

PEPTIC ULCER DISEASE (PUD)
Etiology and pathophysiology-Loss of tissue of mucosal, submucosal, and even muscular layer
Diagnostic evaluation – upper GI, endoscopy Therapeutic management
Medical – treat increased H.Pylori –PPI, amoxicillin, flagyl
Surgical Nursing considerations -stress

EFFECTS OF UC OR CROHN DISEASE

OBSTRUCTIVE DISORDERS

HYPERTROPHIC PYLORIC STENOSIS
CONSTRICTION OF THE PYLORIC SPHINCTER WITH OBSTRUCTION OF THE GASTRIC OUTLET

INTUSSUSCEPTION Telescoping or invagination of one portion of
intestine into another Occasionally due to intestinal lesions Often cause is unknown Diagnostic evaluation Therapeutic management Prognosis Nursing considerations

ILEOCOLIC INTUSSUSCEPTION

MALROTATION AND VOLVULUS Malrotation is due to
abnormal rotation around the superior mesenteric artery during embryonic development
Volvulus occurs when intestine is twisted around itself and compromises blood supply to intestines
May cause intestinal perforation, peritonitis, necrosis, and death

MALABSORPTION SYNDROMES
Characterized by chronic diarrhea and malabsorption of nutrients
May result in failure to thrive Digestive defects Absorptive defects Anatomic defects

CELIAC DISEASE
Also called gluten-induced enteropathy and celiac sprue
Four characteristics Steatorrhea-fatty stool General malnutrition Abdominal distention Secondary vitamin deficiencies

CELIAC DISEASE (CONT.)
Pathophysiology Diagnostic evaluation Therapeutic management Nursing considerations

SHORT BOWEL SYNDROME (SBS) A malabsorptive disorder Results from decreased
mucosal surface area, usually as result of small bowel resection
Etiology and pathophysiology
Result of decreased mucosal surface area, usually due to extensive resection of small intestine
Other causes NEC, volvulus, gastroschisis,
Crohn disease in

THERAPEUTIC MANAGEMENT OF SBS
Nutritional support—first phase: TPN Associated risks and complications
Second phase: enteral feeding Long-term maintenance Medical therapies Surgical therapies Nursing considerations

GI BLEEDING Upper GI bleeding
Esophagus Stomach
“Coffee grounds” emesis Hematemesis
Lower GI bleeding Bright red (rectal bleeding): hematochezia Tarry stools: melena
Diagnostic evaluation Therapeutic management
Assess blood loss Establish hemodynamic stability
Nursing considerations

ACUTE HEPATITIS
Causes Virus Chemical reaction Drug reaction Other disease processes

TYPES OF HEPATITIS
Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Hepatitis G

TYPES OF DIARRHEA
Acute Acute infectious/infectious gastroenteritis Chronic Intractable diarrhea of infancy Chronic nonspecific diarrhea (CNSD)

CIRRHOSIS
End stage of many chronic liver diseases Etiologies
Biliary atresia, chronic hepatitis, hemophilia, CF Pathophysiology
Irreversible Complications

ANORECTAL MALFORMATIONS
Imperforate anus Persistent cloaca Cloacal exstrophy Genitalia may be indefinite Diagnostic evaluation Management

DEHYDRATION
Types of dehydration Diagnostic evaluation Therapeutic management Nursing considerations
1st treatment- Oral hydration Solution-OHS

DAILY MAINTENANCE FLUID REQUIREMENTS
Calculate child’s weight in kg Allow 100 ml/kg for first 10 kg body weight Allow 50 ml/kg for second 10 kg body weight Allow 20 ml/kg for remaining body weight

EXAMPLE 1: DAILY FLUID CALCULATION
Child weighs 32 kg 100 x 10 for first 10 kg of body weight = 1000 50 x 10 for second 10 kg of body weight = 500 20 x 12 for remaining body weight = 240 1000 + 500 + 240 = 1740 ml/24 hr

EXAMPLE 2: DAILY FLUID CALCULATION
Child weighs 8.5 kg 100 x 8.5 for first 10 kg of body weight = 850 No further calculations 850 ml/24 hr

EXAMPLE 3: DAILY FLUID CALCULATION
Child weighs 14 kg 100 x 10 for first 10 kg of body weight = 1000 50 x 4 for second 10 kg of body weight = 200 No further calculations 1000 + 200 = 1200 ml/24 hr

HOMEMADE ELECTROLYTE SOLUTION
2 quarts water 1 teaspoon baking
soda 1 teaspoon salt 7 Tablespoons sugar 1/2 teaspoon salt
substitute