Embed Size (px)
DESCRIPTION
Chapter 11: Cardiovascular System. The Cardiovascular System. A closed system of the heart/blood The heart pumps blood It is no more than a transportation pump Blood vessels allow blood to circulate throughout the body MILES of blood vessels – intricate network - PowerPoint PPT Presentation
Citation preview


A closed system of the heart/blood The heart pumps blood
It is no more than a transportation pump
Blood vessels allow blood to circulate throughout the body MILES of blood vessels – intricate network
At all times, blood is contained within the vessels or heart
Function: Deliver oxygen and nutrients and re”move”
carbon dioxide and other waste products

Location Thorax: between the lungs & inferior to the
mediastinum Orientation
Apex (5cm) is pointed toward the left hip Superior surface lies on the diaphragm
Base (9 cm) is towards the right shoulder
Lies anterior to the vertebral column, posterior to the sternum
Size About the size of your fist Weighs less than 1 pound
Shape Hollow & cone shaped



Pericardium Double walled sac containing the heart & the roots
of the greater vessels Two walls: fibrous pericardium & serous
pericardium Functions to protect the heart & lubricate the heart
Fibrous pericardium is loose and superficial Functions:
Protect the heart Anchor the heart to its surrounding structures
(diaphragm & greater vessels) Prevents overfilling of the heart with blood
Serous membrane (pericardium) is deep to the fibrous pericardium and composed of two layers
Visceral pericardium Next to heart; also known as the epicardium
Parietal pericardium Outside layer that lines the inner surface of the fibrous
pericardium Serous fluid fills the space between the layers of
pericardium The fluid is pale yellow, translucent, & benign in
nature (“functionless)

Three layers Epicardium
Outside layer This layer is the visceral pericardium
Produces pericardial fluid Connective tissue layer Lubricates the motion between the inner and outer layers
of the pericardium Often infiltrated with fat, in older people
Myocardium Middle layer Mostly cardiac muscle – arranged in circular/spiral
bundles This arrangement is what links all the structures of the heart
together Collagen & elastin connective tissues form the fibrous
skeleton of the heart Creates additional support where the great vessels issue from
the heart/around the heart valves Over time, these area become “stretched out” from the continual
stress of blood pumping Connective tissue cannot carry electrical impulses - limits the
direct spread of action potential across cardiac tissue

Endocardium Inner layer Endothelium
Thin, white sheet of epithelial tissue Lines the entire surface of the
circulatory system, down to the interior surfaces of the capillaries
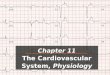
Label it all!

Right and left side act as separate pumps Four chambers & two major separations Atria
Thin walled & small blood just flows down Receiving chambers: blood enters the heart
Right atrium: receives deoxygenated blood from: Superior vena cava
Returns blood from the body that is superior from the diaphragm
Inferior vena cava Returns blood from the body that is inferior from the
diaphragm Coronary sinuses
Collects blood that drains from the myocardium itself Left atrium: receives oxygenated blood from:
Left & right pulmonary veins This makes up most of the heart’s base Transports blood back to the heart, from the lungs

Atria The right and left atria are separated by
the interatrial septum Fossa ovalis: small shallow depression that marks
where the foramen ovale had existed in the fetal heart
Auricles: small “flaps” that increase atrial volume – distinguishing feature of atria
Bundles of muscle in atria are specifically called pectinate muscles – look like they have been “raked with a comb”

Ventricles Makes up most of the mass of the heart Discharging chambers: blood leaves the
heart Right ventricle: pumps deoxygenated blood
to the lungs through the pulmonary arteries Makes up most of the anterior surface of the heart
Left ventricle: pumps (propels) oxygenated blood through the aorta out through the body (systemic circulation) Makes up most of the posteroinferior surface
Trabeculae carneae: irregular ridges in the internal walls of the muscle layer – “crossbars”
Papillary muscles: conelike muscle bundles Play a role in valve function


Interventricular septum Separates the two ventricles
Interatrial septum Separates the two atria

Systemic circulation Blood flows from the left side of the heart through the
body tissues and back to the right side of the heart Left side of the heart – systemic circuit pump
Blood leaves the left side of the heart to smaller arteries attached to body tissues to provide nutrients and gases.
Pulmonary circulation Blood flows from the right side of the heart to the
lungs and back to the left side of the heart Right side of the heart – pulmonary circuit pump
Starts as Oxygen poor/carbon dioxide rich blood in the right atrium/ventricle
OPPOSITE: Pulmonary veins carry OXYGEN RICH blood back to the L.A.

Coronary circulation Shortest circulation within the body Blood flow within the vessels of the heart itself
Ensures adequate oxygen supply for the heart muscle itself to function The vessels are the coronary arteries & cardiac
veins Coronary arteries are the only source of blood supply for
the actual myocardium Myocardium is too thick to allow for diffusion of nutrients
and gases Delivery of nutrients and gases are specifically
accomplished by the left and right coronary arteries (arising from the base of the aorta)

Coronary circulation The left C.A. runs towards the left side of the
heart, branching into the interventricular artery, supplies blood to the interventricular septum & the anterior walls of both ventricles
Then, that blood travels to the posterior walls of the left ventricle via the circumflex artery.
The right C.A. runs along the right side of the heart, branching in two: Marginal artery serves the myocardium of the
lateral part of the right side of the heart Posterior interventricular artery runs to the heart
apex and supplies the posterior ventricular walls

Coronary circulation Arterial supply of the heart varies considerably
Each person can have different anastomoses (merging points) of arteries These create different networks/routes of blood delivery to the heart This also explains how arterial blockages don’t always stop the heart from
working completely, unless. Complete blockage of a coronary artery leads to tissue death and heart attack
Coronary arteries provide pulsing, intermittent blood flow to the heart Actively deliver blood when the heart is relaxed Ineffective when the ventricles are contracting
Compressed by the contracting heart muscles Entrances to the coronary arteries are partly blocked by the flaps of
the open aortic semilunar valve
Even though the heart only represents 1/200 of body weight, it requires 1/20 of blood supply With the left ventricle using most of that blood supply

Valves allow blood to only flow in one direction (prevent backflow)
Four valves: Between the atria & ventricles: AV valves
Anchored in place by chordae tendinae: “heart strings” Open during heart relaxation and closed during ventricular
contract Bicuspid (mitral): left side of the heart Tricuspid: right side of the heart
Between ventricles & an artery: semilunar valves Closed during heart relaxation & open during ventricular
contract Pulmonary semilunar valve: between the right ventricle &
the pulmonary artery Aortic semilunar valve: between the left ventricle & the
aorta

Arteries: Aorta: leaves the left ventricle
Brings oxygenated blood out to the body Pulmonary artery: leaves the right ventricle
Brings deoxygenated blood to the lungs
Veins Superior & inferior vena cava: enters the right
atrium Brings deoxygenated blood into the heart
Pulmonary veins (there are four): enters the left atrium Brings oxygenated blood into the heart

Superior & Inferior venae cavae bring blood into the right atrium
From the right atrium, blood travels through the tricuspid valve to the right ventricle
Blood leaves the right ventricle, passing through the semilunar valve into the pulmonary trunk
The pulmonary trunk splits into the left/right pulmonary arteries that carry blood into the lungs

Oxygen is picked up and carbon dioxide is dropped off
Oxygen rich blood travels back to the heart through the four pulmonary veins
Blood enters the left atrium, travels through the bicuspid valve into the left ventricle
From the left ventricle, blood leaves the heart via the aortic semilunar valve and ultimately the aorta – allowing the blood to travel through the body.
Simple, no?

Blood in the heart chambers does not nourish the myocardium
The heart has its own nourishing circulatory system consisting of Coronary arteries—branch from the aorta to
supply the heart muscle with oxygenated blood Cardiac veins—drain the myocardium of blood Coronary sinus—a large vein on the posterior of
the heart, receives blood from cardiac veins Blood empties into the right atrium via the
coronary sinus


Intrinsic conduction system (nodal system) Heart muscle cells contract, without nerve
impulses, in a regular, continuous way Special tissue sets the pace
Sinoatrial node = SA node (“pacemaker”) Impulse generating tissue that keeps the regular
contractions of the heart It’s a group of cells called myocytes positioned by the
top of the right atrium It’s a muscle cell that contains some parts of the
contractile unit Atrioventricular node = AV node, is at the junction
of the atria and ventricles Serves as a “backup” for the SA node (pacemaker) Ensures there is a mild delay (0.12 seconds) in the
contraction of ventricles to ensure that there is actually enough blood to pump out of the ventricles

Special tissue sets the pace (continued) Atrioventricular bundle = AV bundle (bundle of His), is in
the interventricular septum Transmits impulses from the AV node to the apex of the
heart Purkinje fibers extend out of the AV bundle This bundle of cells is important because it’s regular rate of
impulse messaging is 40-60 beats per minute Bundle branches are in the interventricular septum Purkinje fibers spread within the ventricle wall muscles
Distribute the impulses to the walls of ventricles actually allowing cardiac muscle contraction to happen
Atrial fibrillation: the muscles of the atria “quiver” instead of regularly contract Physiological cause: overwhelming, disorganized
impulses from the SA node or AV node miscommunication
Increases stroke risk up to 7x because blood may pool in atria or clot

Contraction is initiated by the sinoatrial node Sequential stimulation occurs Force cardiac muscle depolarization in one
direction—from atria to ventricles Once SA node starts the heartbeat
Impulse spreads to the AV node Then the atria contract
At the AV node, the impulse passes through the AV bundle, bundle branches, and Purkinje fibers
Blood is ejected from the ventricles to the aorta and pulmonary trunk as the ventricles contract

Tachycardia—rapid heart rate over 100 beats per minute
Bradycardia—slow heart rate less than 60 beats per minutes

Atria contract simultaneously Atria relax, then ventricles contract Systole = contraction
Usually describes left ventricle contraction: cardiomyocytes
Diastole = relaxation Happens after systole; allows the heart to
refill with blood Cardiac cycle—events of one complete heart beat
Mid-to-late diastole—blood flows from atria into ventricles Ventricular systole—blood pressure builds before ventricle
contracts, pushing out blood Early diastole—atria finish refilling, ventricular pressure is
low

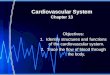
Atrialcontraction
Mid-to-late diastole(ventricular filling)
Ventricular systole(atria in diastole)
Early diastole
Isovolumetriccontraction phase
Ventricularejection phase
Isovolumetricrelaxation
Ventricularfilling
Left atrium
Right atrium
Left ventricle
Right ventricle
http://www.sumanasinc.com/webcontent/animations/content/bloodpressure.swf

Cardiac output (CO) Amount of blood pumped by each side (ventricle) of
the heart in one minute Stroke volume (SV)
Volume of blood pumped by each ventricle in one contraction (each heartbeat)
Usually remains relatively constant About 70 mL of blood is pumped out of the left
ventricle with each heartbeat Heart rate (HR)
Averages: 75 beats per minute CO = HR SV CO = HR (75 beats/min) SV (70 mL/beat) CO = 5250 mL/min Starling’s law of the heart—the more the cardiac muscle is
stretched, the stronger the contraction Changing heart rate is the most common way to change
cardiac output

Increased heart rate Sympathetic nervous system is stimulated
Crisis Low blood pressure
Hormones Epinephrine – released in stressful situations
(adrenaline) Thyroxine – used to increase metabolism
Exercise Decreased blood volume
Decreased heart rate Parasympathetic nervous system is activated in
reaction to a sympathetic stimulation High blood pressure or blood volume Decreased venous return

Transport blood to the tissues and back Carry blood away from
the heart Arteries Arterioles
Exchanges between tissues and blood Capillary beds
Return blood toward the heart Venules Veins

Three layers (tunics) Tunica intima
Endothelium – one layer of cells Have direct contact with
blood
Tunica media Smooth muscle
In larger arteries, there may be elastic tissue
Controlled by sympathetic nervous system
Tunica externa Mostly fibrous connective
tissue (collagen) Anchors blood vessels to
body organs

Walls of arteries are the thickest Lumens of veins are larger Larger veins have valves to prevent
backflow Skeletal muscle “milks” blood in veins
toward the heart Walls of capillaries are only one cell
layer thick to allow for exchanges between blood and tissue
Most arterial blood is pumped by the heart

Capillary beds consist of two types of vessels Vascular shunt—vessel directly connecting an
arteriole to a venule True capillaries—exchange vessels
Oxygen and nutrients cross to cells Carbon dioxide and metabolic waste products cross
into blood

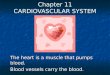
Aorta Largest artery in the body Leaves from the left ventricle of
the heart Regions of the Aorta
Ascending aorta—leaves the left ventricle Left & right coronary arteries
leave here to supply blood to the heart
Aortic arch—arches to the left Thoracic aorta—travels
downward through the thorax Abdominal aorta—passes
through the diaphragm into the Abdominopelvic cavity

Arterial branches of the aortic arch (BCS) Brachiocephalic trunk splits into the
Right common carotid artery Right subclavian artery
Left common carotid artery splits into the Left internal and external carotid arteries
Left subclavian artery branches into the Vertebral artery In the axilla, the subclavian artery becomes
the axillary artery brachial artery radial and ulnar arteries
http://zircon.mcli.dist.maricopa.edu/arle/LabelingExercisesII/activityApplet7.html

Arterial branches of the thoracic aorta Intercostal arteries supply the muscles
of the thorax wall Other branches of the thoracic aorta
supply the Lungs (bronchial arteries) Esophagus (esophageal arteries) Diaphragm (phrenic arteries)

Arterial branches of the abdominal aorta Celiac trunk is the first branch of the abdominal
aorta. Three branches are Left gastric artery (stomach) Splenic artery (spleen) Common hepatic artery (liver)
Superior mesenteric artery supplies most of the small intestine and first half of the large intestine
Left and right renal arteries (kidney) Left and right gonadal arteries
Ovarian arteries in females serve the ovaries Testicular arteries in males serve the testes
Lumbar arteries serve muscles of the abdomen and trunk

Arterial branches of the abdominal aorta Inferior mesenteric artery serves the second half
of the large intestine Left and right common iliac arteries are the final
branches of the aorta Internal iliac arteries serve the pelvic organs External iliac arteries enter the thigh femoral
artery popliteal artery anterior and posterior tibial arteries


Superior and inferior vena cava enter the right atrium of the heart Superior vena cava drains the head and arms Inferior vena cava drains the lower body
Veins draining into the superior vena cava Radial and ulnar veins brachial vein axillary
vein These veins drain the arms Cephalic vein drains the lateral aspect of the arm
and empties into the axillary vein Basilic vein drains the medial aspect of the arm
and empties into the brachial vein Basilic and cephalic veins are jointed at the
median cubital vein (elbow area)

Veins draining into the superior vena cava Subclavian vein receives
Venous blood from the arm via the axillary vein Venous blood from skin and muscles via external jugular
vein Vertebral vein drains the posterior part of the head Internal jugular vein drains the dural sinuses of the
brain Left and right brachiocephalic veins receive venous
blood from the Subclavian veins Vertebral veins Internal jugular veins
Brachiocephalic veins join to form the superior vena cava right atrium of heart
Azygous vein drains the thorax

Veins draining into the inferior vena cava Anterior and posterior tibial veins and fibial veins drain the
legs Posterior tibial vein popliteal vein femoral vein
external iliac vein Great saphenous veins (longest veins of the body) receive
superficial drainage of the legs Each common iliac vein (left and right) is formed by the
union of the internal and external iliac vein on its own side Right gonadal vein drains the right ovary in females and
right testicle in males Left gonadal vein empties into the left renal vein Left and right renal veins drain the kidneys Hepatic portal vein drains the digestive organs and travels
through the liver before it enters systemic circulation Left and right hepatic veins drain the liver


Internal carotid arteries divide into Anterior and middle cerebral arteries These arteries supply most of the cerebrum
Vertebral arteries join once within the skull to form the basilar artery Basilar artery serves the brain stem and cerebellum
Posterior cerebral arteries form from the division of the basilar artery These arteries supply the posterior cerebrum
Circle of Willis Anterior and posterior blood supplies are united by
small communicating arterial branches Result—complete circle of connecting blood vessels
called cerebral arterial circle or circle of Willis


Pulse Pressure wave of
blood Monitored at
“pressure points” in arteries where pulse is easily palpated
Pulse averages 70–76 beats per minute at rest

Normal human range is variable Normal
140–110 mm Hg systolic 80–75 mm Hg diastolic
Hypotension Low systolic (below 110 mm HG) Often associated with illness
Hypertension High systolic (above 140 mm HG) Can be dangerous if it is chronic

BP is blood pressure BP is affected by age, weight, time of day,
exercise, body position, emotional state CO is the amount of blood pumped out of
the left ventricle per minute PR is peripheral resistance, or the amount of
friction blood encounters as it flows through vessels Narrowing of blood vessels and increased blood
volume increases PR BP = CO PR

Neural factors Autonomic nervous system adjustments (sympathetic
division) Renal factors
Regulation by altering blood volume Renin—hormonal control
Temperature Heat has a vasodilating effect Cold has a vasoconstricting effect
Chemicals Various substances can cause increases or decreases
Diet