Embed Size (px)
Citation preview

Community Health and Minorities
Chapter 10

Introduction
• Strength of America lies in diversity of people
• Race remains an issue in U.S.
• U.S. population• Majority – white, non-Hispanic (66%)
• Racial or ethnic minorities (34%)
• Minority health – morbidity and mortality of ethnic minorities

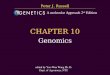
U.S. Population by Race/Ethnicity, 2008

U.S. Population Projection by Race/Ethnicity

Introduction
• Advances in health gains are not equal in U.S.
• Secretary’s Task Force Report on Black and Minority Health
• Initiative to Eliminate Racial and Ethnic Disparities in Health (Race and Health Initiative)

Racial and Ethnic Classifications
• Classifications used to operationalize race and ethnicity
• Challenges with classifications representing diversity of population
• Categories of race are more social than biological
• Self-reported data can be unreliable
• Many nonfederal systems do not collect racial and ethnic data

Health Data Sources and Their Limitations
• Challenges in complete and accurate collection of racial and ethnic data
• Bias analysis
• HHS has long-term strategy for improving collection and use of racial and ethnic data
• Important to understand health beliefs of various groups• Heterogeneity within groups

Americans of Hispanic Origin
• Hispanic origin is an ethnicity, not a race• Persons of Mexican, Puerto Rican, Cuban,
Central American, or South American descent, or some other Spanish origin
• Nearly all Hispanics (96%) in the U.S. are classified by race as white
• Educational attainment
• Income
• Health beliefs

Black Americans
• Black or African Americans• People having origins in any of the black racial
groups from Africa
• More than ½ live in southern regions of U.S.
• Educational attainment
• Income
• Health beliefs and culture

Asian Americans and Pacific Islanders
• Now two separate racial groups
• Generally concentrated in the western states
• Educational attainment
• Income
• Health beliefs• Variations among the many groups• Generational differences

American Indians and Alaska Natives
• Original inhabitants of America
• Economically and socially disadvantaged• Relatively poor health status
• Education
• Income
• Health beliefs• Various tribal groups have distinct customs,
languages, and beliefs• Many share the same cultural values

Native Americans and Health Care
• Many tribes are sovereign nations• Tribes transferred land in U.S. to federal
government in return for provision of certain services
• Indian Health Services (IHS) within HHS• Responsible for federal health services to
Native Americans and Alaska Natives• Goal to raise health status to highest possible
level

Completed High School by Race and Hispanic Origin, U.S.

Real Median Income by Race and Hispanic Origin, U.S.

Poverty Rates by Race and Hispanic Origin, U.S.

Refugees
• Refugees
• Immigrants
• Aliens
• Illegal aliens
• Can be classified into existing racial/ethnic groups; as a single group, present special concerns
• Education, health problems, injuries, employment, etc.

Race and Health Initiative
• Goal to eliminate disparities among racial and ethnic minority populations in six areas of health while maintaining progress of overall health of American people
• Infant mortality
• Cancer screening and management
• Cardiovascular disease
• Diabetes
• HIV/AIDS
• Adult and child immunization

Infant Mortality
• Serious disparity in U.S. among racial and ethnic minorities• Black Americans infant death rate more than
two times that of white Americans• Lack of prenatal care and low-birth-weight
babies

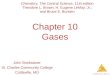
Infant Mortality Rates by Race and Hispanic Origin of Mother, U.S.

Babies of Low Birth Weight by Mother’s Race and Hispanic Origin, U.S.

Cancer Screening and Management
• Incidence and death rates highest among black Americans for various types of cancer• Many disparities attributed to lifestyle factors,
late diagnosis, access to health care
• Less primary and secondary prevention in various minority groups

Cancer Incidence and Death Rates, U.S., by Cancer Site and Race

Cardiovascular Diseases
• Death rates vary widely among racial and ethnic groups• Black Americans have higher rates from CHD
and stroke
• Hypertension prevalence as a risk factor varies according to race/ethnicity• Black American tend to develop hypertension
earlier in life than whites; unknown reason

Diabetes
• Overall prevalence has risen in U.S. in recent years• Prevalence in those 20 and older varies in
minority groups
• Increase in age-adjusted death rates in all racial and ethnic groups• Significantly higher in minority groups

Diabetes Age-Adjusted Prevalence by Race/Ethnicity, U.S.

HIV Infection/AIDS
• Proportional distribution of AIDS cases has increased in black Americans and Hispanics and decreased in white Americans• Attributed to higher prevalence of unsafe or
risky health behaviors, and lack of access to health care to provide early diagnosis and treatment

Percentages of AIDS by Race/Ethnicity and Year of Diagnosis, U.S.

Child and Adult Immunization Rates
• Early childhood immunizations do not vary significantly by race or ethnicity
• Older adult immunization rates are substantially lower in minority groups, even though an overall increase has occurred

Socioeconomic Status and Racial and Ethnic Disparities in Health
• Many factors contribute to health disparities – economic, educational, behavioral, cultural, legal, and political• Socioeconomic status (SES) considered the
most influential single contributor to premature morbidity and mortality• Association between SES and race/ethnicity is
complicated and cannot fully explain all disparity

Relationship Between Race and Health

Equity in Minority Health
• Simple solutions unlikely
• Solutions to problems for one group may not work for another
• Solutions must be culturally sensitive

Cultural Competence
• A set of congruent behaviors, attitudes, and policies that come together in a system, agency, or among professionals, that enables effective work in cross-cultural situations
• Culture is vital in how community health professionals deliver services and how community members respond to programs and interventions

Empowering the Self and the Community
• To enable people to solve their community health problems• Three kinds of power associated with
empowerment• Social – access to “bases”; needed to gain
political power
• Political – power of voice and collective action
• Psychological – individual sense of potency

Discussion Questions
• Why have there been so many changes to racial and ethnic classifications in the United States in recent decades?
• How can community health programs empower minority groups?