Embed Size (px)
Citation preview
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Chapter 2: Drug action & Handling
Lisa Mayo, RDH, BSDHPharmacology DH206
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
THANK YOU LAURA!!
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Pharmacodynamics2. Pharmacokinetics 3. Routes of drug administration4. Factors that alter the effect of a drug
LEARNING OBJECTIVES
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Pharmacodynamics1) Definitions2) Dose-Response Relationships
(potency, effi cacy, ceiling effect, toxicity)
3) Drug-Receptor Interactions
OBJECTIVE #1
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Pharmacodynamics: describes the actions of a drug on the body
Involves drug-receptor interaction, mechanism of action, drug response, dose-response relationship
Therapeutic effect: intended effect of the drug in the body
Drug Indication: therapeutic uses of the drug in the body
Contraindication: situation or circumstance when a drug should NOT be given
Undesirable effects: (CH3)1. Side Effects2. Adverse Effects3. Toxic Effects
PHARMACODYNAMICS1.) DEFINITIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Site of Action Location within the body where the drug exerts its
therapeutic effect Ex: aspirin’s site of action is on the hypothalamus
to reduce feverMechanism of Action
Explains how a drug produces its effects Drugs do NOT impact a new function in an organism Drugs either intensify same actions or block actions
in the body Drugs speed up or slow down reactions in the body
PHARMACODYNAMICS1.) DEFINITIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Dose response curveDetermine correct DOSE of drugs to give to patientsDetermines POTENCY & EFFICACY of a drug’s actionResponse of any drug depends on the amount given:
this is called dose-response relationship Dose: amt of drug given to produce a desired effect Response: the effect of that dosage A curve results when DOSE of a drug is plotted against
the INTENSITY of it’s effect ↑ dose = ↑ magnitude of response
Threshold dose: minimum dose of a drug needed to produce a therapeutic/measurable response
PHARMACODYNAMICS2.) DOSE-RESPONSE CURVE
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACODYNAMICS2.) LOG-DOSE CURVE
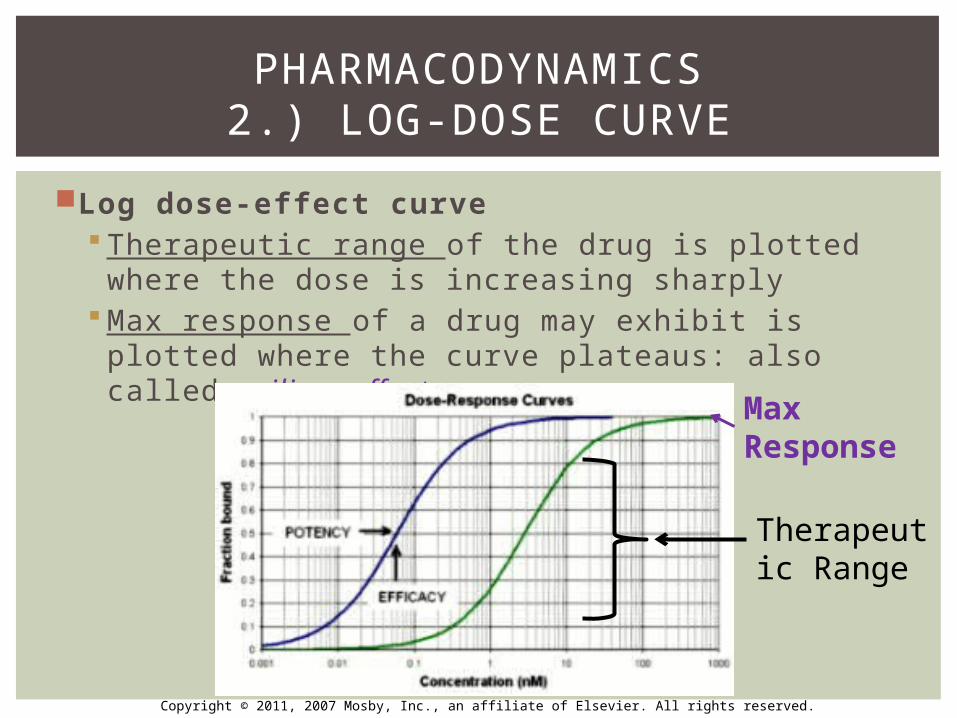
Log dose-eff ect curve Therapeutic range of the drug is plotted where
the dose is increasing sharply Max response of a drug may exhibit is plotted
where the curve plateaus: also called ceiling effect
Max Response
Therapeutic Range
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACODYNAMICS2.) LOG-DOSE CURVE
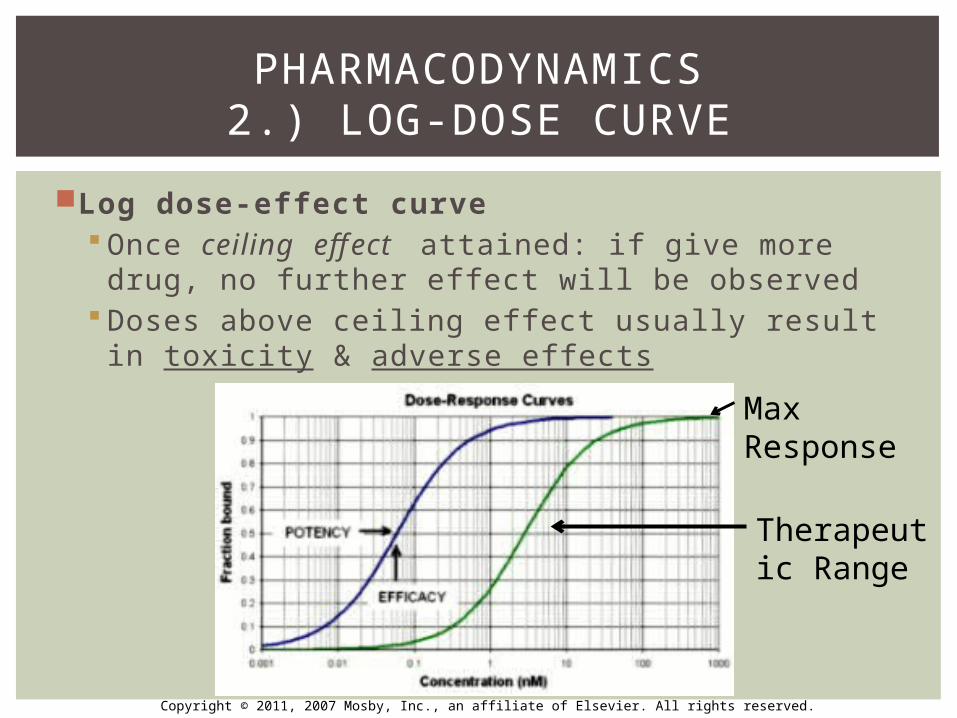
Log dose-eff ect curve Once ceiling effect attained: if give more drug,
no further effect will be observed Doses above ceiling effect usually result in
toxicity & adverse effects
Max Response
Therapeutic Range
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
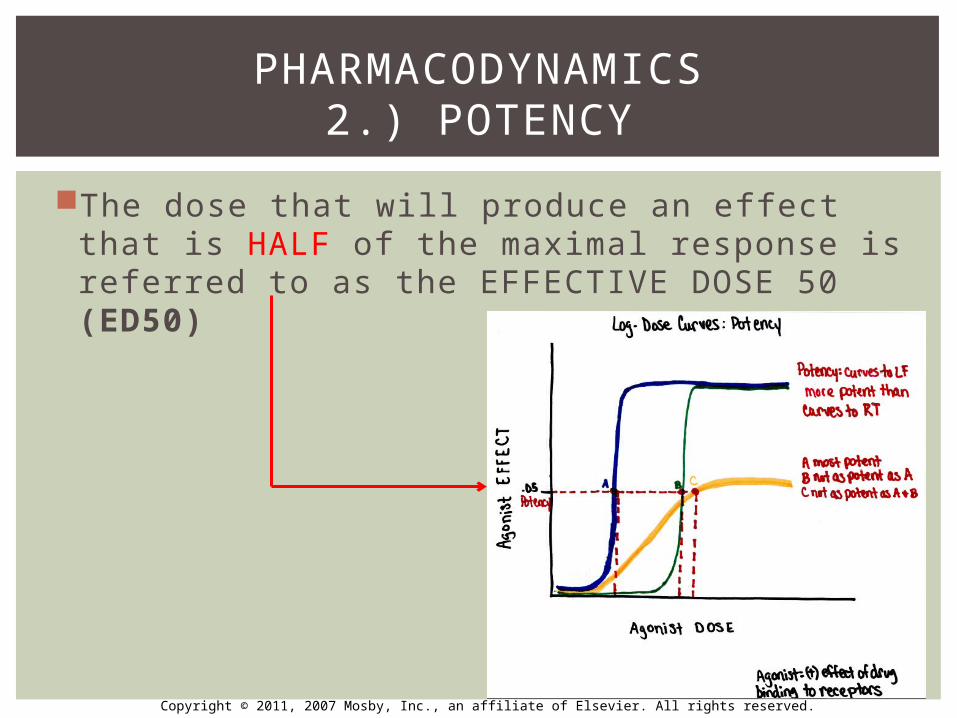
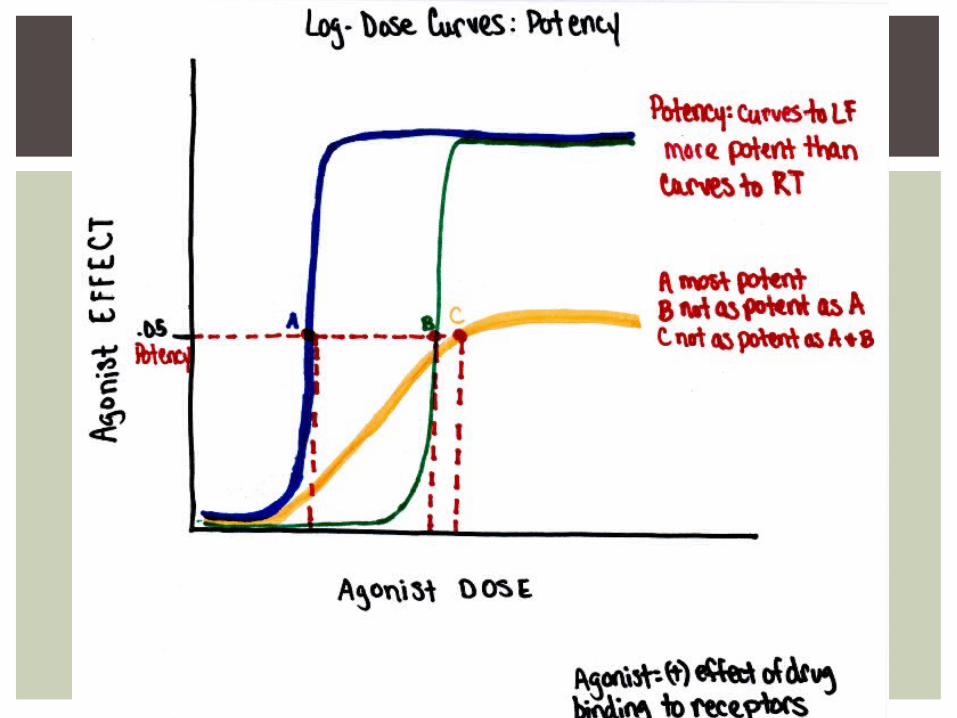
Potency: measure of strength or concentration of a drug Potency is shown by the location of that drug’s curve
along the x-axisLess-potent drugs: need more to produce a
desired effect equivalent to that of a more potent drug
Determined by the affi nity of a drug for its receptors
Potency usually expressed in terms of median effective dose (ED50) – next slide
BEER VS JACK DANIELS
PHARMACODYNAMICS2.) POTENCY (P.13)
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
The dose that will produce an effect that is HALF of the maximal response is referred to as the EFFECTIVE DOSE 50 (ED50)
PHARMACODYNAMICS2.) POTENCY
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
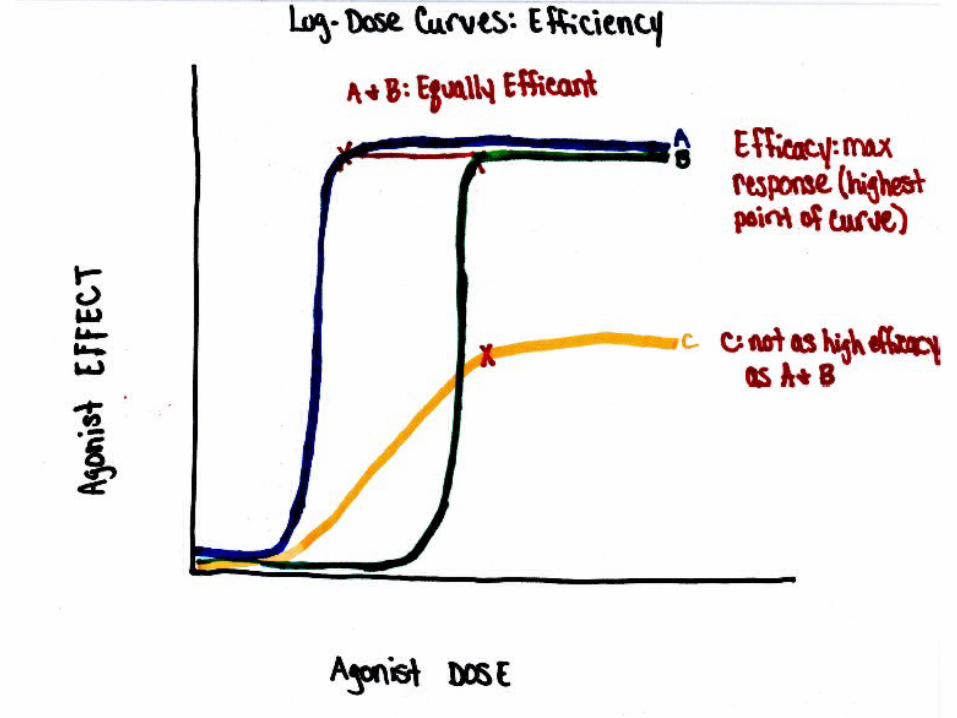
Maximum intensity or effect of a drug that can be reached
Ability to produce a therapeutic effect regardless of the dose
Effi cacy & potency often describe the success of drug therapyDrugs may be equally efficacious, but differ in potency (see next slide)
PHARMACODYNAMICS 2.) EFFICACY (P.13)
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
The strength of a drug with regard to it’s ability to achieve a desired effect is termed
A. efficacyB. potencyC. therapeutic effectD. tolerance
BOARD REVIEW QUESTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Potency of a drug is a function of the amount of the drug required to produce an effect
BOARD REVIEW ANSWER
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
In comparing two drugs, the dose-response curve for the drug that is more effi cacious would
A. Be closer to the Y axisB. Be farther from the Y axisC. Have a greater curve heightD. Have a higher median effective dose
BOARD REVIEW QUESTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
C: The effi cacy of a drug increases as the height of the curve increases
Effi cacy is an expression of maximal activity of a drugThe other choices all refer to indicators of drug potency, not effi cacy
BOARD REVIEW ANSWER
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
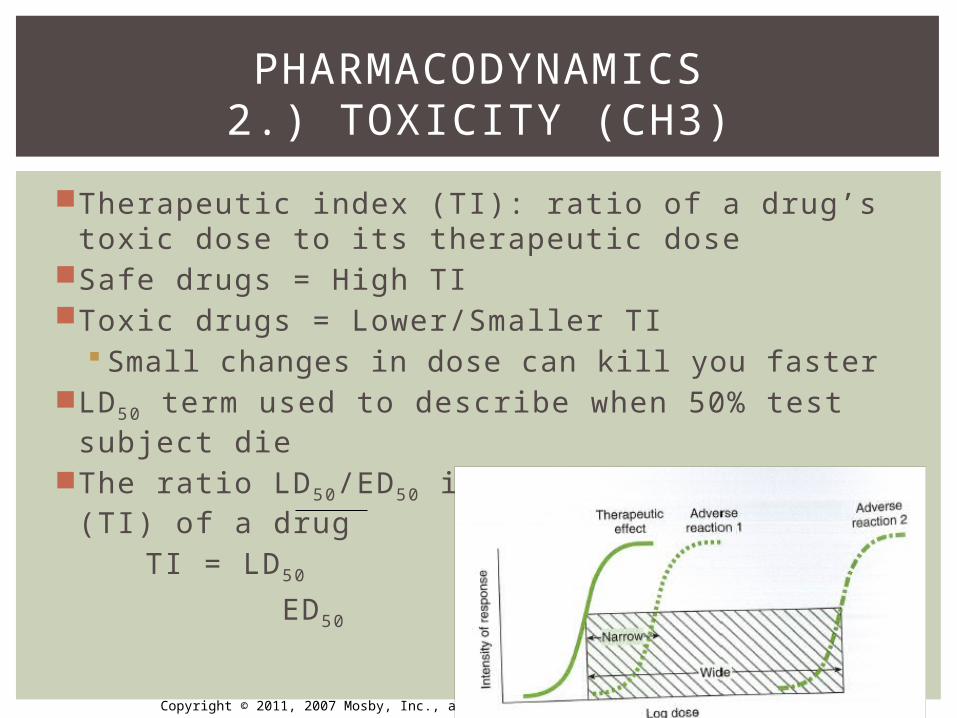
Therapeutic index (TI): ratio of a drug’s toxic dose to its therapeutic dose
Safe drugs = High TIToxic drugs = Lower/Smaller TI
Small changes in dose can kill you fasterLD50 term used to describe when 50% test subject
dieThe ratio LD50/ED50 is the therapeutic index (TI) of
a drugTI = LD50
ED50
PHARMACODYNAMICS2.) TOXICITY (CH3)
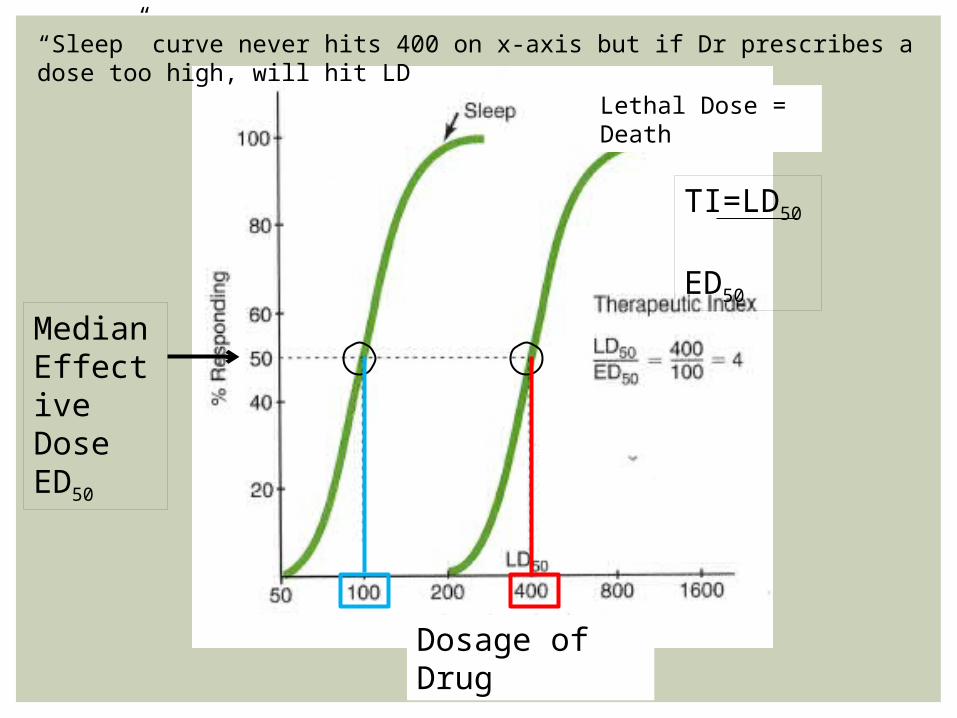
Median Effective DoseED50
Lethal Dose = Death
Dosage of Drug
“Sleep” curve never hits 400 on x-axis but if Dr prescribes a dose too high, will hit LD
TI=LD50
ED50
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
What does ED50 stand for?
What does LD50 stand for?
If a drug has a narrow TI, is the drug safer?
REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drugs have an eff ect in the body by binding to a receptor
Drug receptor: protein located on all cell membranes
Drugs attach to specific receptors & produce an eff ect
Drug attachment done in 2 ways (next slide)1) Direct/Specific drug receptor2) Indirect/Nonspecific drug reaction
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drug attachment done in 2 ways:1) Direct/Specific drug receptor (most common)
Drugs directly binding to cell receptors Cells have 100s of receptors: only certain ones specific
for a drug Drugs bind & form Van der Waal bonds (weak,
reversible bonds)2) Indirect/Nonspecific drug reaction
Drugs do NOT bind to receptors but instead saturate the water or lipid parts of a cell – drug actions occur based on degree of saturation
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Drug+Receptor → Drug-Receptor → Effect Complex
eventually efficacy can be measured (max drug action)
LOCK-AND-KEY FASHION OF DRUGS TO THEIR RECEPTORS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Different drugs often compete for the same receptor sites (morphine & acetaminophen)The drug with stronger affinity for the receptor will bind to more receptors than the drug with weaker affinity
Drugs with stronger affinity for receptor sites are more potent drugs
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Receptor
Morphine Acetaminophen
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
3 classifications of drug-receptor complexes1. Agonist2. Partial Agonist3. Antagonist/Blocking Drugs
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
All 3 have an affinity for a receptor, they differ in what they cause the receptor to do!
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
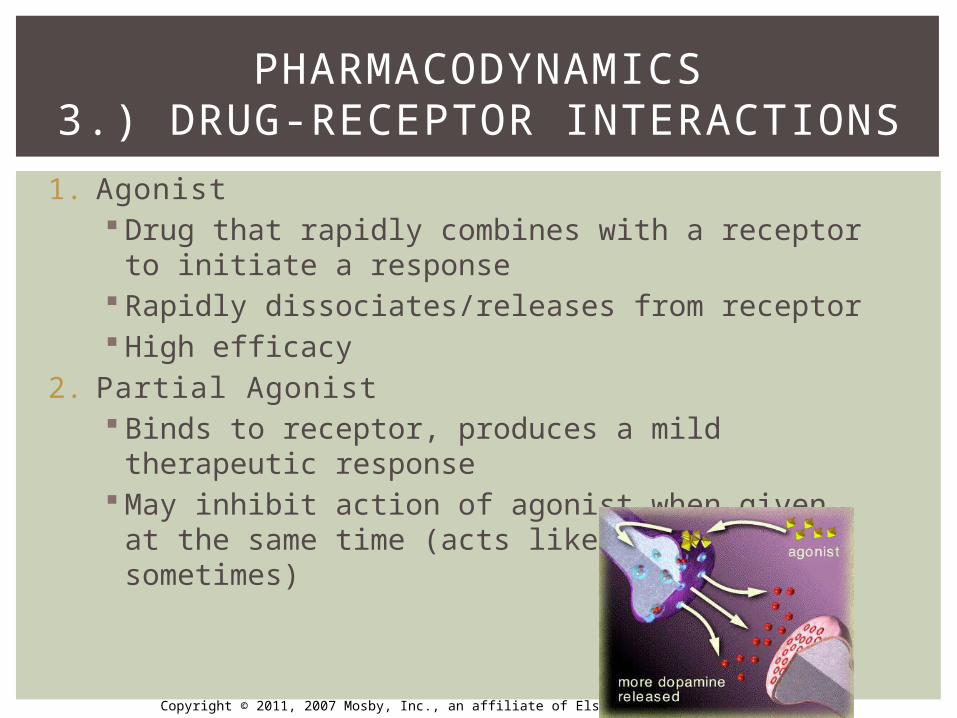
1. Agonist Drug that rapidly combines with a receptor to
initiate a response Rapidly dissociates/releases from receptor High efficacy
2. Partial Agonist Binds to receptor, produces a mild therapeutic
response May inhibit action of agonist when given at the
same time (acts like antagonist sometimes)
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
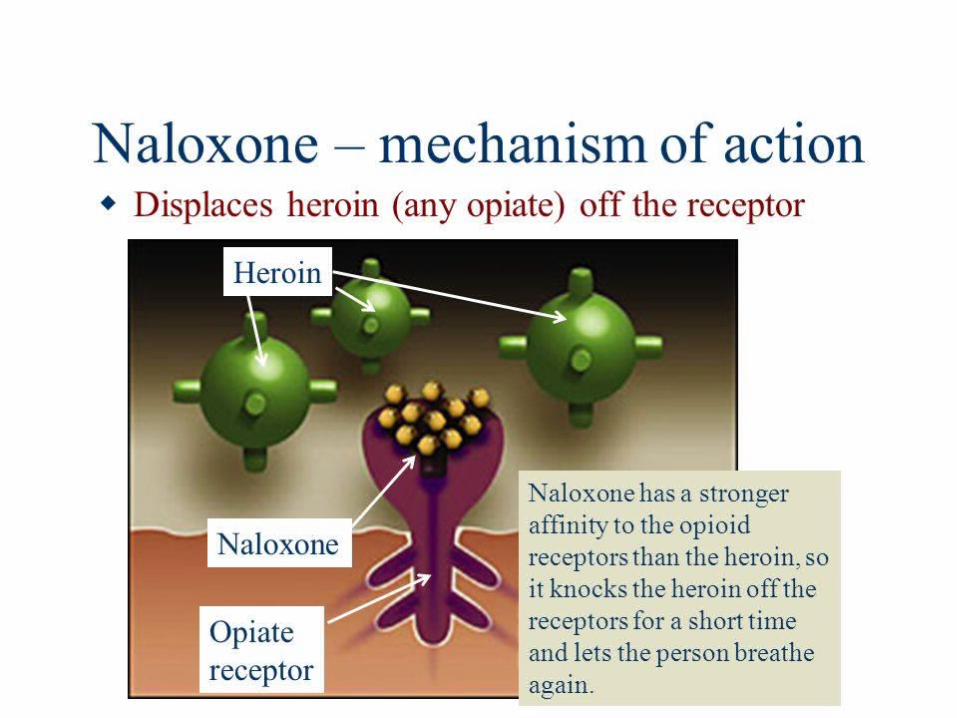
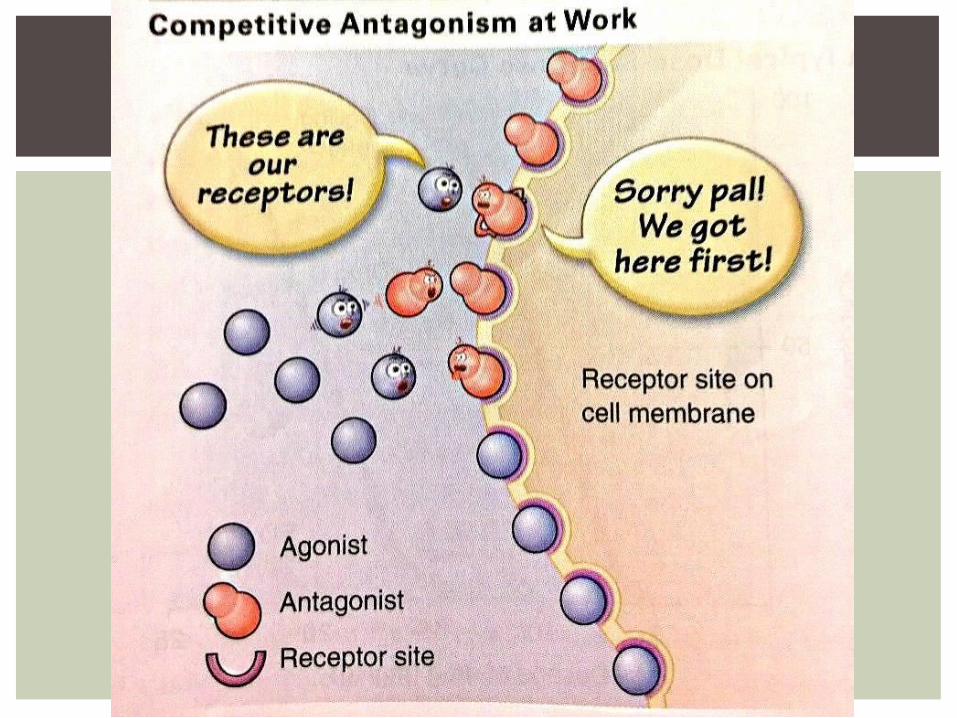
3. Antagonist/Blocking Drugs Binds to receptor but does NOT dissociate Has NO positive response or efficacy Blocks reaction of the agonist Ex: naloxone – morphine antagonist – given if
have morphine OD 3 different types (next slide)
1) Competitive2) Noncompetitive3) Physiologic
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
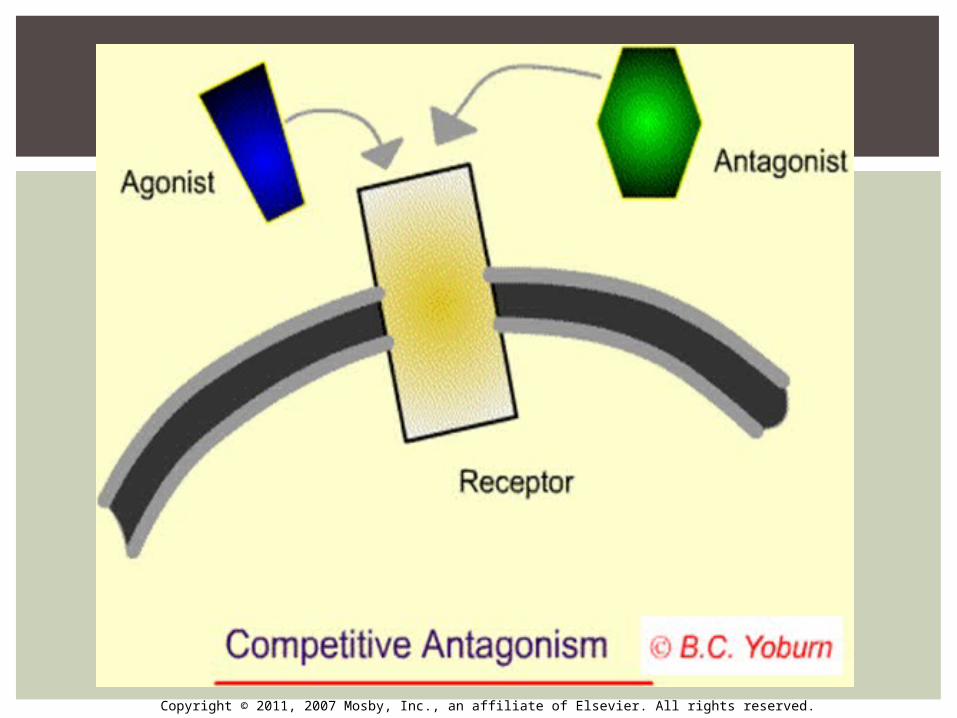
3. Antagonist/Blocking Drugs1) Competitive: drug that occupies a significant
proportion of the receptors and thereby prevents them from reacting maximally with an agonist
2) Noncompetitive: can exert action 2 ways1. React with receptor to prevent an agonist-
receptor response2. Act to inhibit some event that leads to a
response3) Physiologic: Has affinity for a different receptor
site than the agonist but decreases the effect of the agonist by producing an opposite effect via different receptors
PHARMACODYNAMICS3.) DRUG-RECEPTOR INTERACTIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following terms is related to the amount of drug administered?
a. Doseb. Responsec. Agonistd. Toxicity
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following terms is related to the amount of drug administered?
a. Doseb. Responsec. Agonistd. Toxicity
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
An individual has an overdose on oxycodone, a narcotic, and is administered a narcotic antagonist. Which of the following features describes antagonist drugs?
a. Binds to the same receptor sites as agonist drugsb. Binds to the receptor to reduce the actions of the agonistc. Have a greater affi nity to the receptor than agonistsd. Have a lesser affi nity to the receptor than agonists
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
An individual has an overdose on oxycodone, a narcotic, and is administered a narcotic antagonist. Which of the following features describes antagonist drugs?
a. Binds to the same receptor sites as agonist drugsb. Binds to the receptor to reduce the actions of the agonistc. Have a greater affi nity tot eh receptor than agonistsd. Have a lesser affi nity to the receptor than agonists
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Pharmacokinetics1. Definition2. Absorption3. Distribution4. Metabolism5. Excretion6. Clinical Applications
OBJECTIVE #2
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Describes what a drug does once inside human body
(ADME)AbsorptionDistributionMetabolismExcretion
Drugs usually enter body at a site distant from its intended target – must travel through bloodstream in the body
PHARMACOKINETICSDEFINITION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACOKINETICSABSORPTION
ADME
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Entrance of a drug into the blood streamDrug must first be dissolved in body fluidsRequires the drug to pass through biologic
membranesThe rate of absorption of a drug influenced
by:1) Physicochemical factors (physical &
chemical conditions such as temperature, redux potential…)
2) Site of absorption (determined by route of administration: IV, oral, rectal….)
3) The drug’s solubility
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
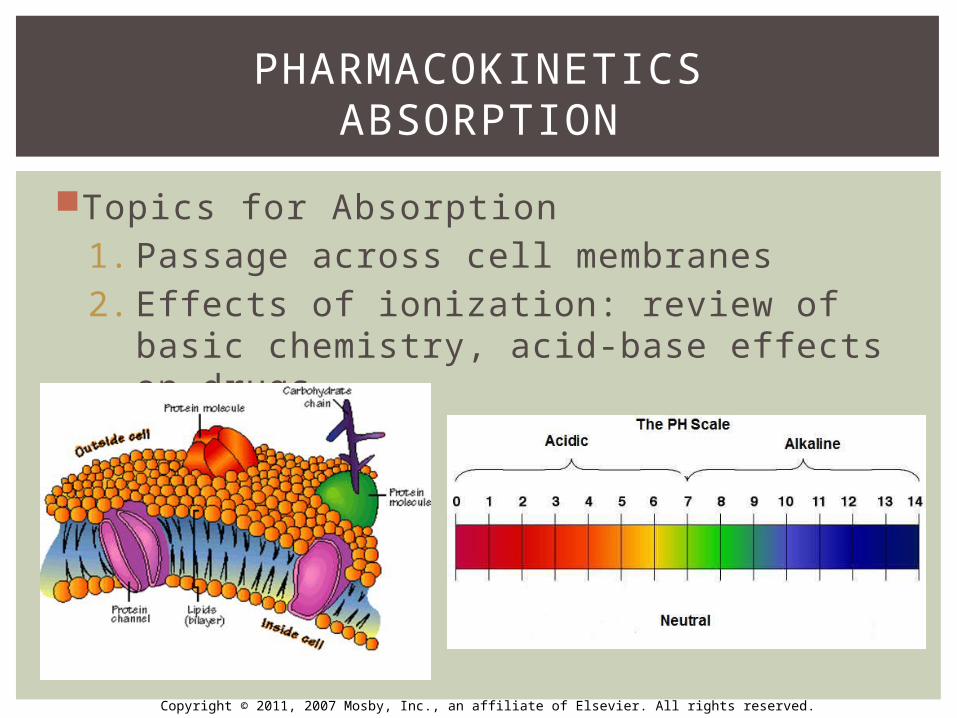
Topics for Absorption1. Passage across cell membranes2. Effects of ionization: review of basic
chemistry, acid-base effects on drugs
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
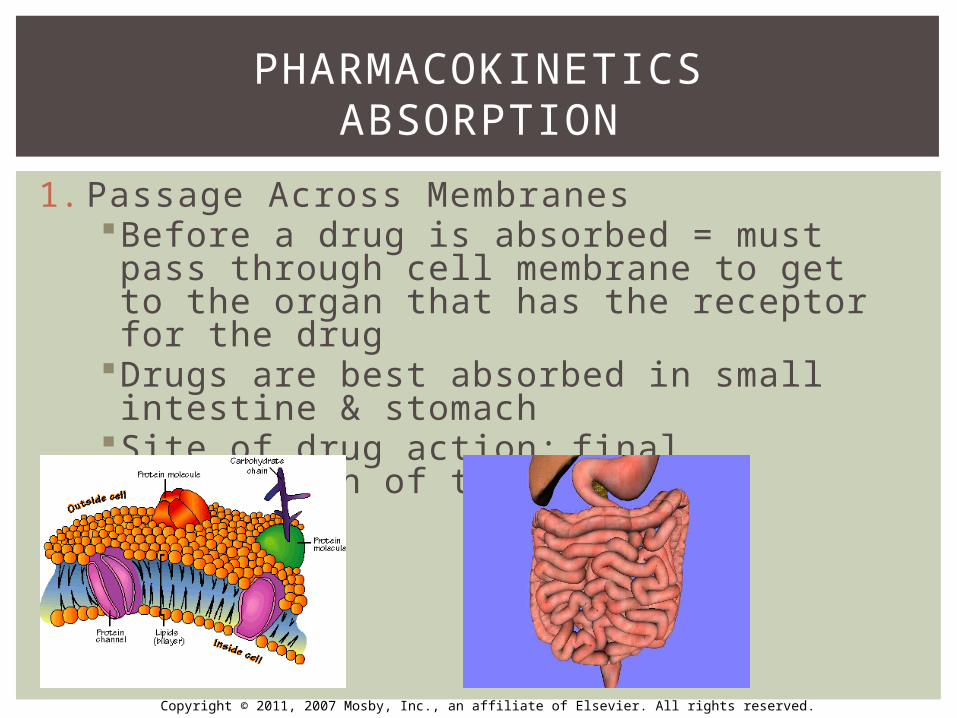
1. Passage Across MembranesBefore a drug is absorbed = must pass through cell membrane to get to the organ that has the receptor for the drug
Drugs are best absorbed in small intestine & stomach
Site of drug action: final destination of the drug
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
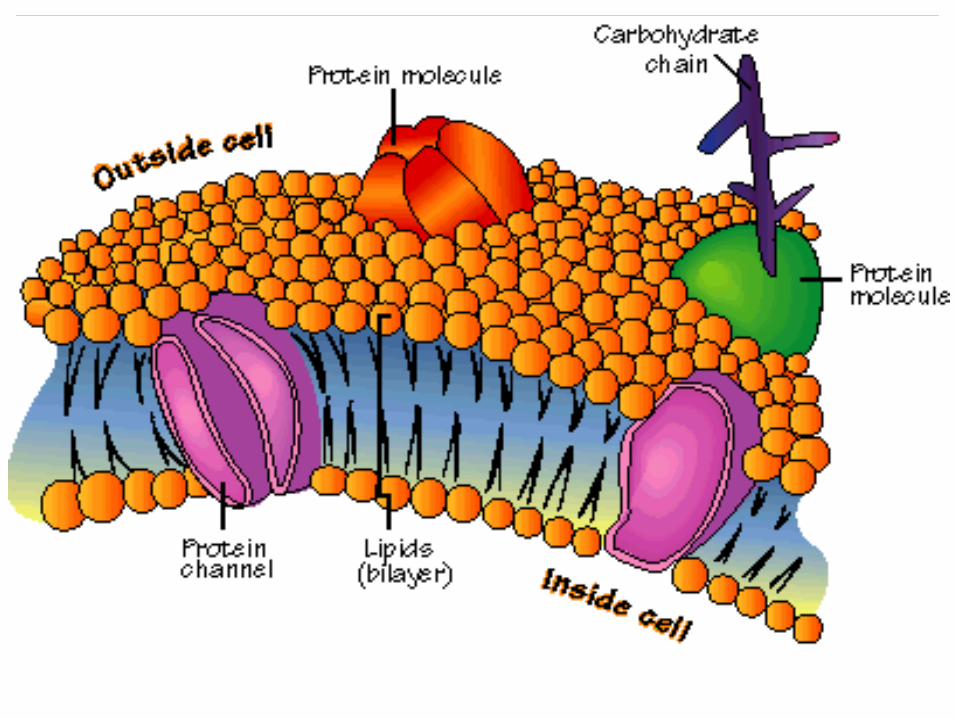
1. Passage Across Membranes Cell membranes: composed of lipids, proteins, &
carbohydrates “Like dissolves like” Lipids: make up biphospholipid layer of cells
Drugs that are water soluble do NOT pass through this layer with ease
Lipid soluble drugs pass with ease (passive diffusion) LIPID SOLUBILITY OF A DRUG IS ONE OF THE MOST
IMPORTANT DETERMINANTS OF THE PHARMACOKINETIC PROPERTY OF THAT DRUG!!
Proteins: contain small water channels/pores Water soluble drugs can pass through this structure
easily (passive diffusion) Lipid soluble drugs do NOT pass through this structure
with ease
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Passage Across Membranes IV drugs pass directly into bloodstreamOrally administered drug
↓
Pass down esophagus ↓
Small intestine ↓
Blood for distribution to its target organ
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
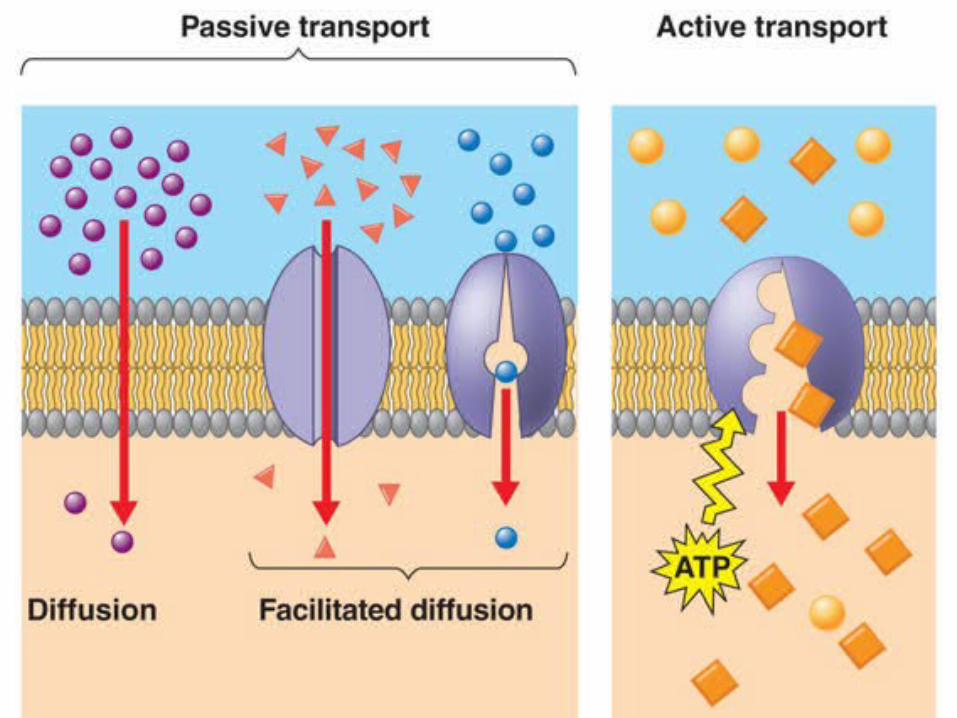
1. Passage Across MembranesMechanism of drug transfer across membranes occurs by one of the following:1) Passive diffusion2) Facilitate diffusion3) Active transport4) Pinocytosis
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Passage Across Membranes1) Passive diffusion
Most drugs absorbed this way (water or lipid soluble) Movement from high to low concentration, along a
concentration gradient Lipid soluble a drugs pass directly through cell
membrane Water soluble drugs pass through water channels or
pores No energy is required for his form of diffusion Ex: General anesthetics pass blood-brain barrier
quickly due to being a lipid soluble drug – fast onset of action
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Passage Across Membranes2) Facilitated diffusion/Passive-mediated
transportCarrier PRO transports drug that is too large to passively diffuse
No energy is needed for transportEx: penicillin, aspirin
3) Active transportCarrier PRO transports a drug against a concentration gradient
Requires use of ATP Not common in pharmacologyEx: vitamin B12, amino acids
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
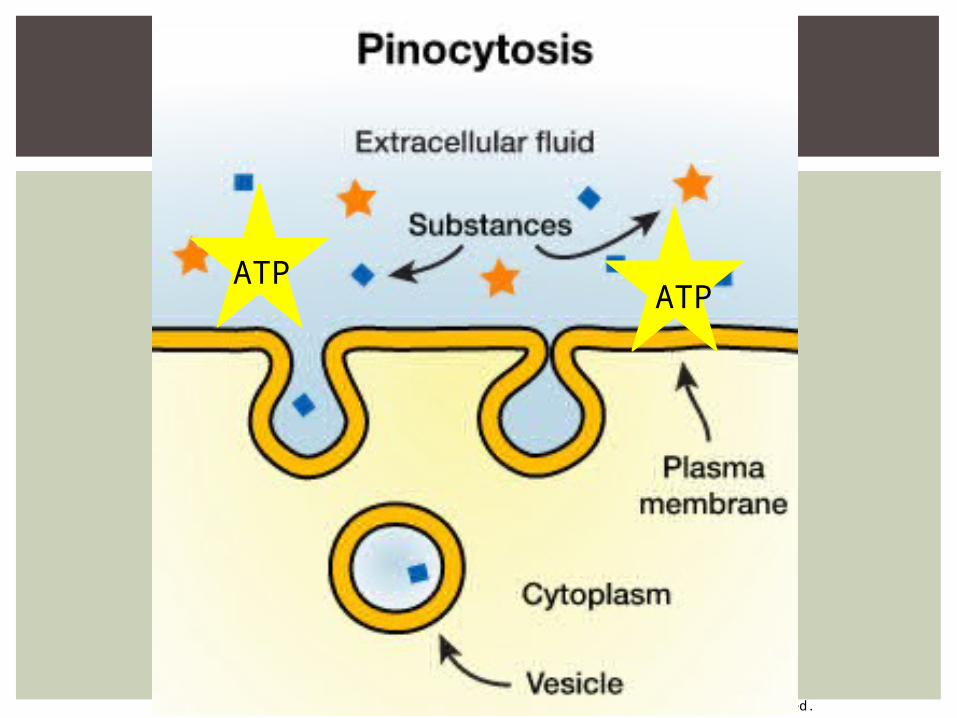
1. Passage Across Membranes4) Pinocytosis
Involves engulfment of fluids or particles by a cell
Minor role in drug movementCell membrane traps the substance
↓Forms a vesicle
↓Detaches and moves to inside the cell
PHARMACOKINETICSABSORPTION
Requires LARGE amount ATP
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
ATPATP
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization
READ PAGE 17: EFFECTS OF IONIZATION
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionizationMost all drugs are weak acids or bases Weak electrolytes dissociate in solution: Non-ionized + Ionized formUn-ionized/non-ionized/uncharged
Lipid soluble Cross lipid cell membranes easily
Ionized/charged Low lipid solubility Cannot easily cross lipid membranes
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization The pH of tissues at the site of administration and
dissociation characteristics (acid dissociation constant, or pKa) of the drug will determine the amount of drug in the ionized vs non-ionized state (ex: aspirin absorption in stomach vs mouth) Portion in each state will determine the ease
with which the drug penetrates tissue Ex: acidic drugs (aspirin) are mostly un-ionized
when they are in an acidic fluid (gastric juices) so drug absorption is favored (same hold true for basic drugs)
Ex: acidic drugs (aspirin) is mostly ionized when in alkaline fluids so absorption occurs at a slower rate & to a lesser extent (same holds true for basic drugs)
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionizationMemorization Tricks
Unionized = mimic lipid = ↑ absorption, ↓ excretion
Ionized = mimic water = ↓ absorption, ↑ excretion
Acidic drugs in basic solution = ↑ excretion
Basic drugs in acidic solution = ↑ excretion
Acidic drugs in acidic solution = ↓excretion
Basic drugs in basic solution = ↓ excretion
PHARMACOKINETICSABSORPTION
↑ Absorption
↓ Absorption
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
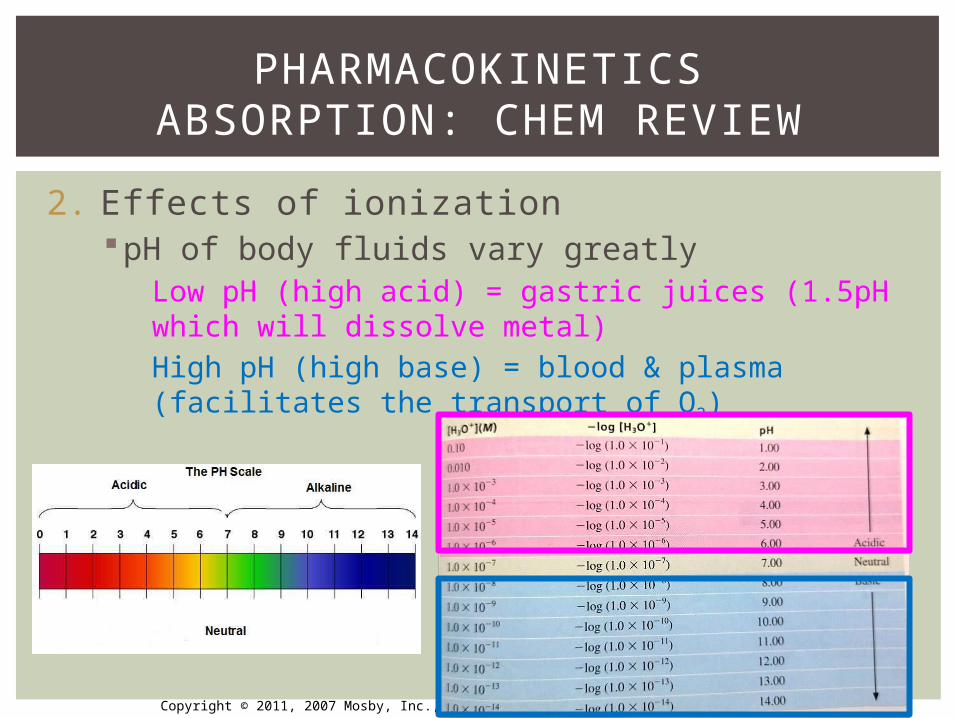
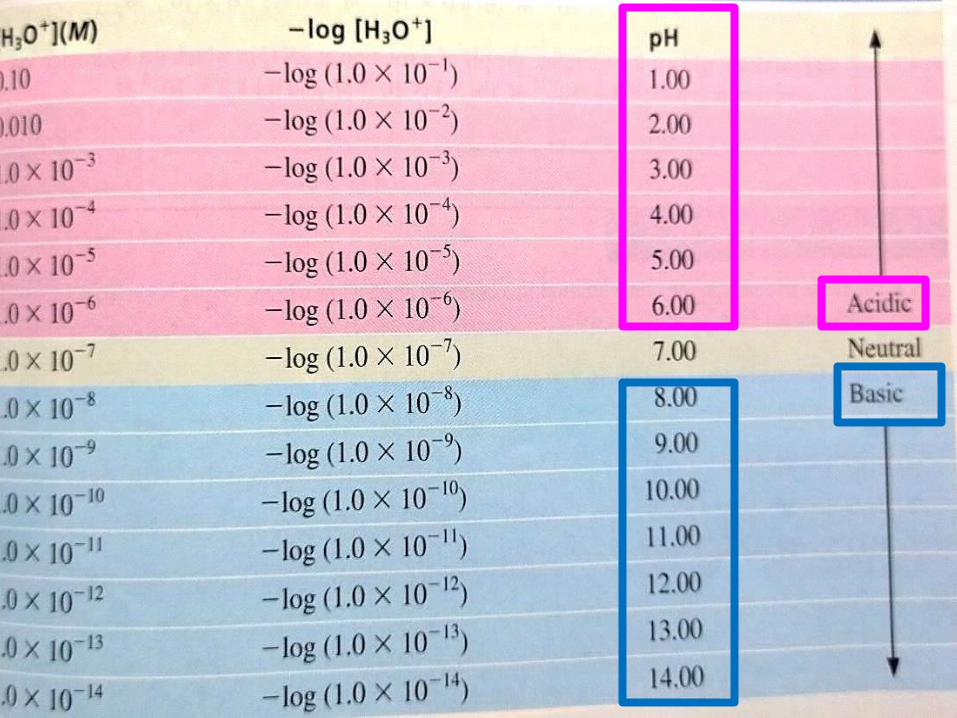
2. Effects of ionizationpH of body fluids vary greatly
Low pH (high acid) = gastric juices (1.5pH which will dissolve metal)High pH (high base) = blood & plasma (facilitates the transport of O2)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization The acid-base nature of drugs is useful in treating
drug toxicity (OD) Drugs are excreted by kidneys in an ionized form To ↑ drug excretion = alter pH of urine Ex: increase renal excretion of an acid drug
(aspirin), the urine is alkalized (pH>7) Alkaline urine - acidic drugs are mostly ionized &
more rapidly excreted
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization (not need to know for test) Example: stomach made of parietal cells
Interior of parietal cells protected from the acidic juices of stomach by their membrane
Membrane allows H2O & neutral molecules to pass in&out but blocks movement of ions like H+
H+ can cross membrane through ACTIVE TRANSPORT
(using ATP)
(cont’d next slide)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization (not need to know for test)Stomach: eating stimulates H+ SECRETION
If acid content excessively high = influx H+ through membrane by active transport & back to plasma
Causes muscle contraction, pain, swelling, bleeding, inflammation
Antacids will neutralize HCl and ↓ H+ concentration
In rxn = all those chemical breakdown into different molecules w/ CO2 and H2O (CO2 makes patient belch)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
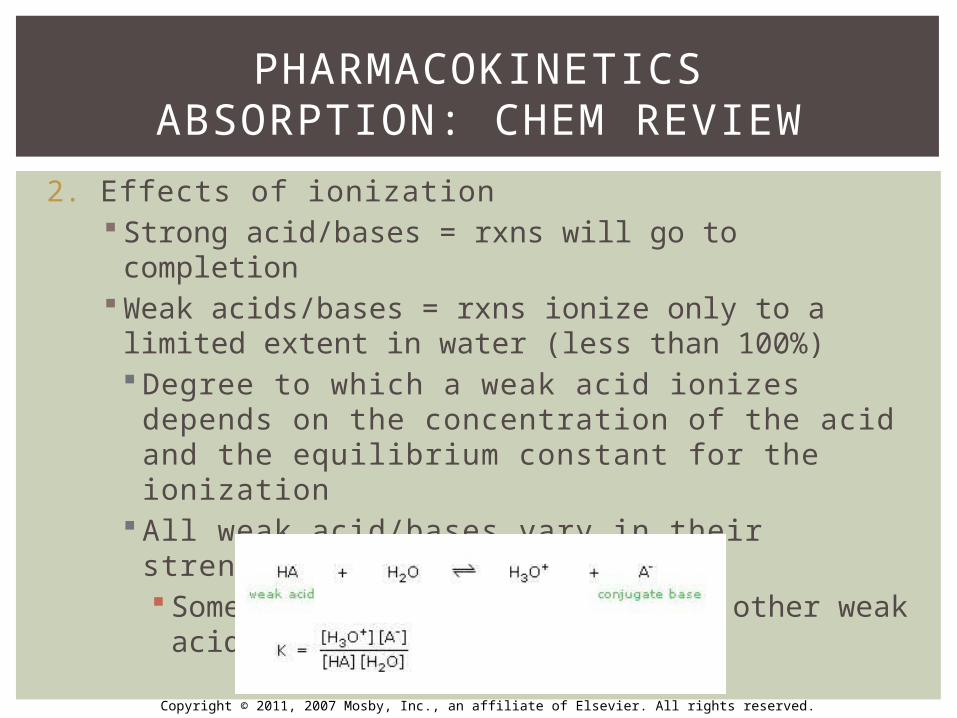
2. Effects of ionization Strong acid/bases = rxns will go to completion Weak acids/bases = rxns ionize only to a limited
extent in water (less than 100%) Degree to which a weak acid ionizes depends on
the concentration of the acid and the equilibrium constant for the ionization
All weak acid/bases vary in their strength of ionization Some weak acids are weaker than other weak
acids
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
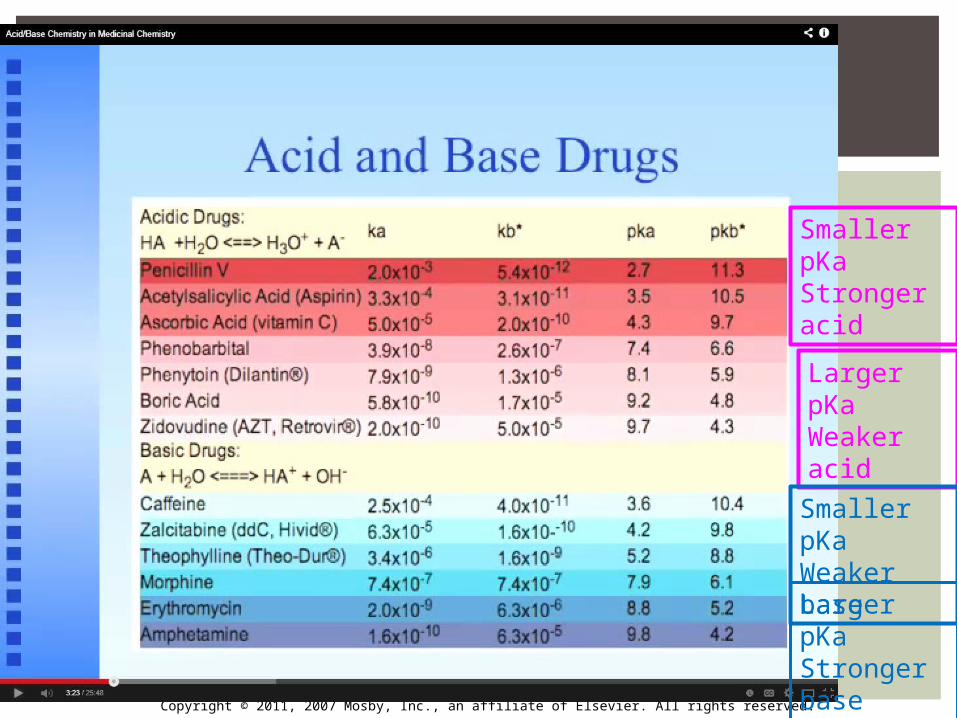
2. Effects of ionization A symbol of Ka is used when discussing acids and
bases and their strength K=symbol used when a molecule breaks apart A=acid Ka is the acid dissociation (molecules breaking apart)
constant In Pharmacology, not use Ka, use pKa which is a
log-rhythm of Ka Ka= 2.0x103 so the pKa=2.0 Larger pKa = weaker the acid (see next slide)
pKa = acid dissociation constant (when 50% of the drug is ionized and 50% is unionized)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Smaller pKa Stronger acid
Larger pKa Weaker acid
Larger pKa Stronger base
Smaller pKa Weaker base
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization Getting drugs into the body can be done 2 ways:
1) Hydrophilically: soluble in aqueous solutions Dissolves well in water molecules Polar molecules
2) Lipophically: fats, alkanes, oil Cell membranes made of lipids Non-polar molecules
General Rule for molecule solubility: LIKE-DISSOLVES-LIKE Hydrophilic like hydrophilic (polar dissolves
polar) Lipophilic likes lipophilic (non-polar dissolves
non-polar)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization (not on test) Generic Acid RXN
HA + H2O A- + H3O+
H will be donated eventually Anion Hydronium ion
A=any acid Conjugate base
*Acids will dissociate to form a conjugate base*
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
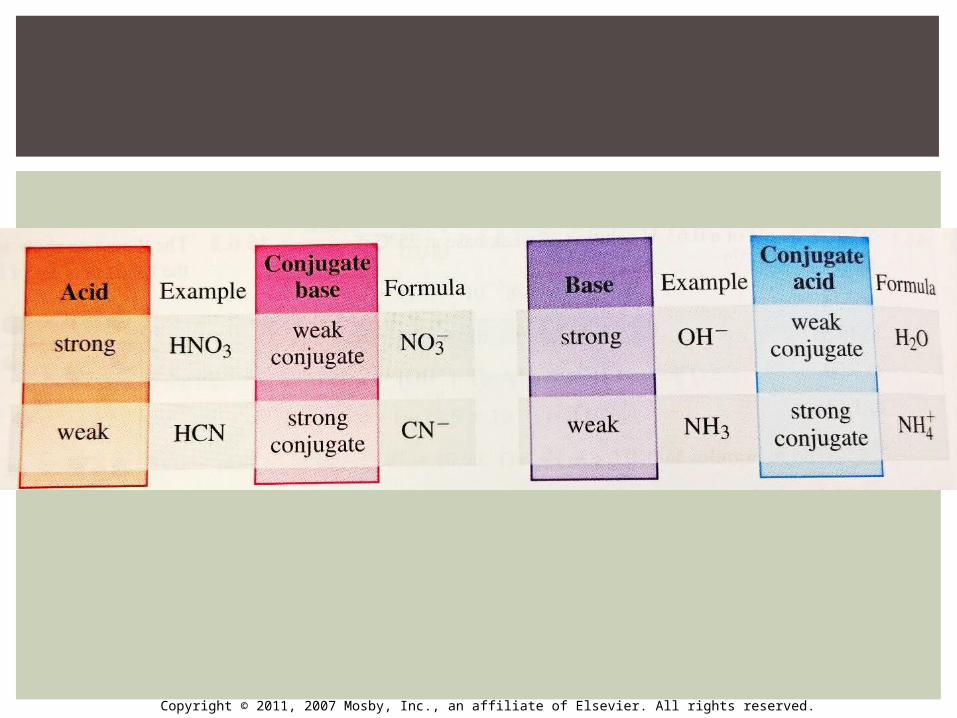
2. Effects of ionization (not on test)Strength of conjugate base in solution
HCl → H+ + Cl-
Strong acid Weak conjugate base
(Will not readily react w/H+ free ion)
HF → H+ + F-
Weak acid ← Strong conjugate base
(will readily react w/H+ free ion)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
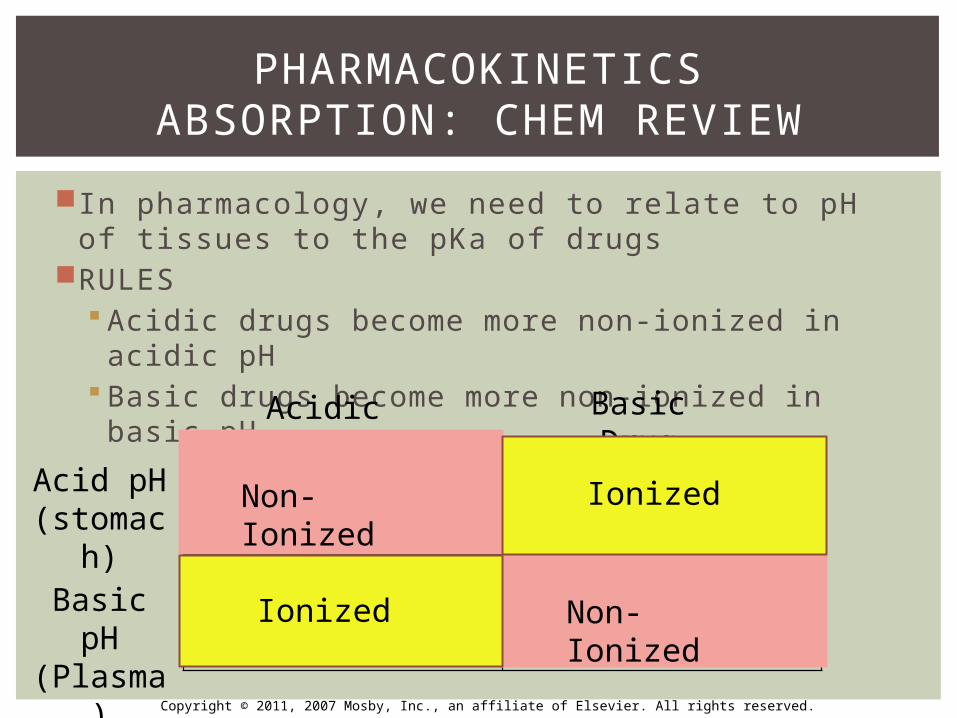
In pharmacology, we need to relate to pH of tissues to the pKa of drugs
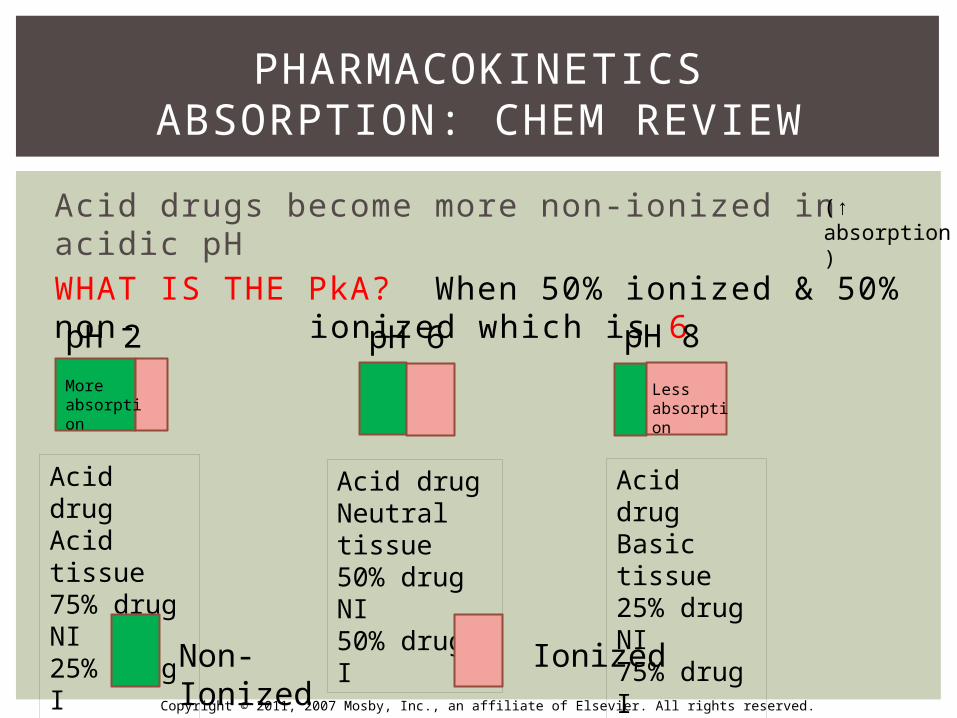
RULES Acidic drugs become more non-ionized in acidic
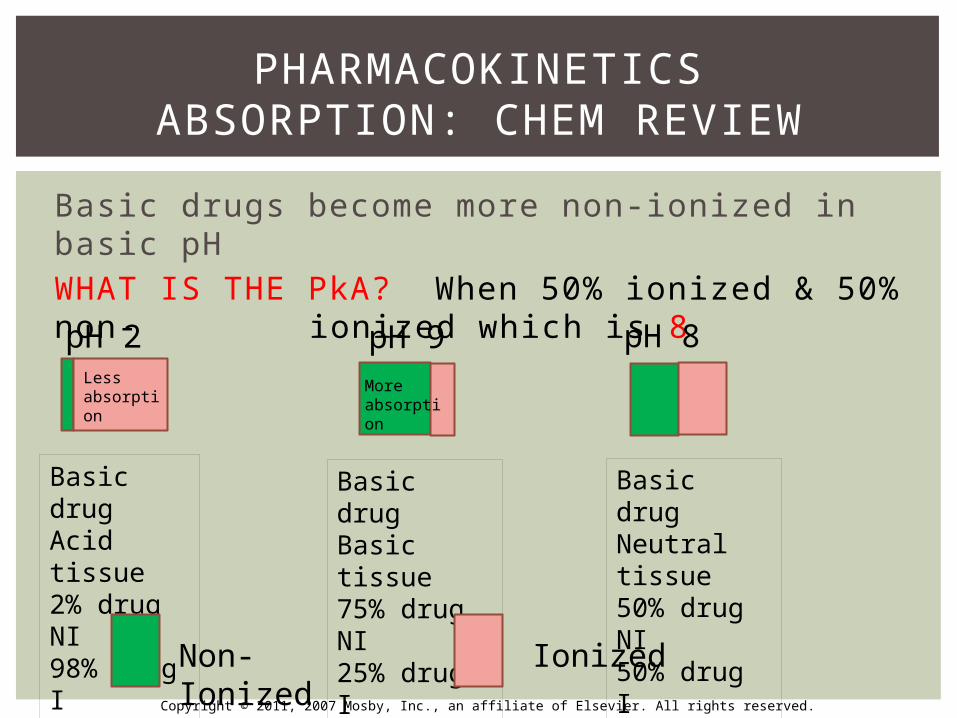
pH Basic drugs become more non-ionized in basic pH
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Acid pH (stomach)
Basic pH (Plasma)
Acidic Drug Basic Drug
Non-Ionized
Non-IonizedIonized
Ionized
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
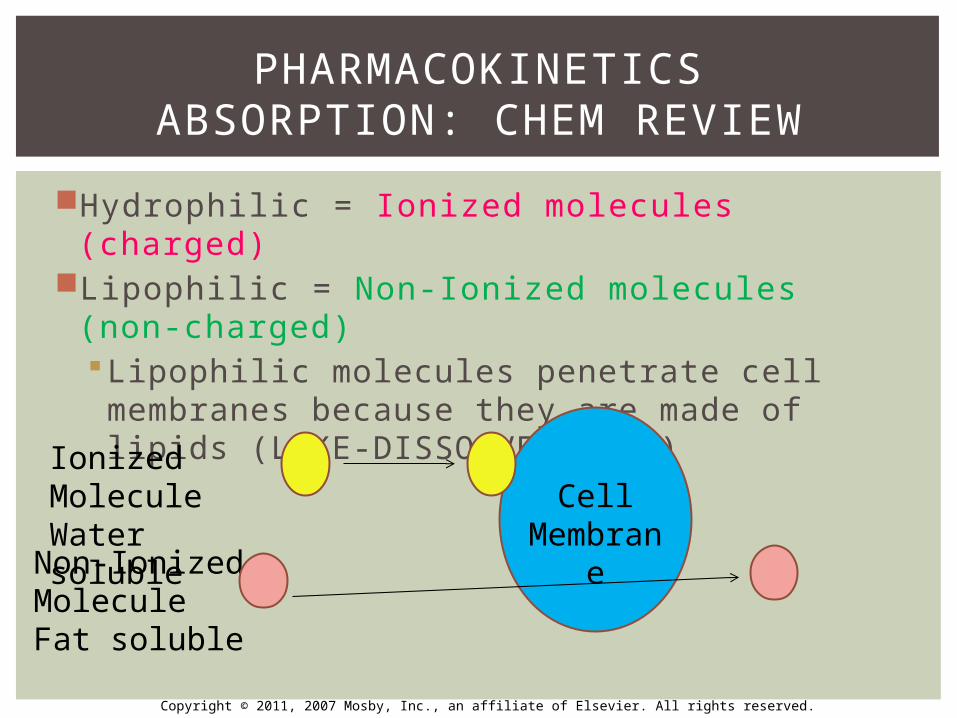
Hydrophilic = Ionized molecules (charged)Lipophilic = Non-Ionized molecules (non-
charged)Lipophilic molecules penetrate cell membranes because they are made of lipids (LIKE-DISSOLVES-LIKE)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Cell Membrane
Ionized MoleculeWater soluble
Non-Ionized MoleculeFat soluble
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Summary: 3 things need to know to find out if a drug is Hydrophilic or Lipophilic1.Whether drug is acid or base (will be
told)2.pKa of the drug (pH at which number
of ionized molecules = number of non-ionized molecules, next slide)
3.pH of tissue into which the drug is going to be placed
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Acid drugs become more non-ionized in acidic pHWHAT IS THE PkA? When 50% ionized & 50% non- ionized which is 6
PHARMACOKINETICSABSORPTION: CHEM REVIEW
pH 2 pH 6 pH 8
Acid drugAcid tissue75% drug NI25% drug I
Acid drugNeutral tissue50% drug NI50% drug I
Acid drugBasic tissue25% drug NI75% drug I
Non-Ionized Ionized
(↑ absorption)
More absorption
Lessabsorption
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Basic drugs become more non-ionized in basic pHWHAT IS THE PkA? When 50% ionized & 50% non- ionized which is 8
PHARMACOKINETICSABSORPTION: CHEM REVIEW
pH 2 pH 9 pH 8
Basic drugAcid tissue2% drug NI98% drug I
Basic drugBasic tissue75% drug NI25% drug I
Basic drugNeutral tissue50% drug NI50% drug I
Non-Ionized Ionized
Lessabsorption
More absorption
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
If know the pKa and pH of the tissues
Can fi gure out if drug mostly ionized or mostly non-ionized
Can then fi gure out if hydrophilic or lipophilic
Can then know if drug will cross the cell membrane or dissolve in water
Ex: drugs given by mouth have to dissolve across a membrane (lipophilic drugs)
Ex: drugs given by IM (intramuscular injection) have to be able to dissolve in water (hydrophilic drugs)
PHARMACOKINETICSABSORPTION: CHEM REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Read p.17 “weak acids”
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization: Weak Acids If pH of the site absorption increases (becomes more basic), H+ concentration falls (pH ↑ = H+↓)
This results in an increase in the ionized form (A–) (hydrophilic), which cannot easily penetrate tissues
If the pH of the site absorption falls (more acidic), H+ concentration will rise (pH↓ = H+↑)
This results in an increase in the un-ionized form(HA) (lipophilic), which can more easily penetrate tissues
PHARMACOKINETICSABSORPTION: (BOOK)
HA + H2O → A- + H3O+
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Read p.17 “weak acids”
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization: Weak Bases If the pH of the site rises (more basic), the H+ concentration will fall
This results in an increase in the un-ionized form (lipophilic), which can more easily penetrate tissues
If the pH of the site falls (more acidic), the H+ concentration will rise
This results in an increase in the ionized form (hydrophilic), which cannot easily penetrate tissues
PHARMACOKINETICSABSORPTION (BOOK)
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization Summary In the presence of infection, the acidity of the tissue ↑ (pH ↓)
Effectiveness of local anesthetics decrease In the presence of infection, the H+ increases because of accumulating waste products in the infected area
Low pH = acidic tissue = lots extra H+ loose & convert anesthetic into SALT form (RNH+) so it will not penetrate fatty tissues because is hydrophillic & will not mix with fatty tissue
Tissues also swollen, lots of fluid = dilutes anes
Big open dilated blood vessels carry anes away faster = wears off faster
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Effects of ionization SummaryRegardless of pH & ionization, absorption usually occur in small intestine where there is more surface area due to presence of microvilli on the surface
Enteric-coated tablets (aspirin, erythromycin) have a layer (wax/cellulose polymer) on the outside to protect the stomach lining from exposure to these acidic drugs
Blood flow to the organ can affect absorption (Ex: nitroglycerin administered sublingual because will have faster absorption due to high vascularity of the organ)
PHARMACOKINETICSABSORPTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
A patient is taking clindamycin for prophylaxis against bacterial endocarditis. In order for the clindamycin to be absorbed into the blood, it must pass through
a. 3 barriers: epithelial cells + blood vessels + brainb. 2 barriers: epithelial cells + blood vesselc. 1 barrier: bloodd. No barrier: drug goes directly into blood
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
A patient is taking clindamycin for prophylaxis against bacterial endocarditis. In order for the clindamycin to be absorbed into the blood, it must pass through
a. 3 barriers: epithelial cells + blood vessels + brainb. 2 barriers: epithelial cells + blood vesselc. 1 barrier: bloodd. No barrier: drug goes directly into blood
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
All of the following statements are TRUE about lipid soluble drugs EXCEPT which one?
a. Readily absorbed through blood vessel wallb. Slowly absorbed through cell membranec. Goes through the blood-brain barrierd. Can be given by inhalation
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
All of the following statements are TRUE about lipid soluble drugs EXCEPT which one?
a. Readily absorbed through blood vessel wallb. Slowly absorbed through cell membranec. Goes through the blood-brain barrierd. Can be given by inhalation
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following statements is TRUE regarding absorption of local anesthetics?
a. Lidocaine (pKa 4) is not absorbed easily through lipid membranes
b. Lidocaine (pKa 7.9) has a fast onset because the tissue pH is close to the pKa
c. Lidocaine (pKa 8.3) has a faster onset than lidocaine
d. Lidocaine (pKa 7.7) has a slow onset of action because it is highly ionized
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following statements is TRUE regarding absorption of local anesthetics?
a. Lidocaine (pKa 4) is not absorbed easily through lipid membranes
b. Lidocaine (pKa 7.9) has a fast onset because the tissue pH is close to the pKa
c. Lidocaine (pKa 8.3) has a faster onset than lidocaine
d. Lidocaine (pKa 7.7) has a slow onset of action because it is highly ionized
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
What does pKa stand for?Acid drugs will be in greatest unionized state when
placed into ______ tissue. If a drug has a fast rate of excretion, what does this
mean for absorption? If pKa is small – is the acid strong or weak? If pKa is small – is the base strong or weak? Is H+ concentration high or low in acidic state?
REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACOKINETICSDISTRIBUTION
ADME
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Once a drug in the bloodstream through absorption – then distribution will occur
Distribution phase: time is takes drug to get through lymph, blood, plasma to target organ
The manner in which a drug is distributed in the body will determine:
How rapidly it produces the desired response
Duration of that responseWhether a response will occur at all
PHARMACOKINETICSDISTRIBUTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Factors Aff ecting Drug Distribution1. Presence of specific tissue barriers
Blood-brain barrier & placenta are lipid barriers2. Blood flow
Greater blood flow = greater rate of distribution of the drug to that organ
Drugs distributed faster to the heart, kidney, brain than to skeletal muscle, adipose tissue, skin which have lower blood flow
3. Solubility of the drug Hydrophilic drugs like insulin – do not penetrate lipid cell
membranes, entirely distributed in the extracellular fluid Lipophilic drugs (general anesthetics, alcohol) do cross
lipid layer & are more evenly distributed in all fluids4. Plasma-PRO binding or free drug (next slide)
PHARMACOKINETICSDISTRIBUTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
4. Plasma PRO binding or un-bound/free drug Many drugs are bound to plasma-PRO (esp albumin)
Degree of PRO-binding depends on concentration of drug in the blood & affi nity of that drug for the PRO
PRO-binding ↓ distribution of the drug from the plasma to intended receptor
Some drugs are highly bound to plasma PRO (99%), while other drugs are not bound to any significant degree
Binding is reversible Some drugs compete for PRO-binding sites: remember
drug with higher affi nity for the receptor wins – can cause problems if 2nd drugs knocks 1st drug from the PRO - ↑ levels of 1st drug in system
Only the un-bound/free drug can exert the pharmacologic effect (NBQ)
Only the free drug can pass across cell membranes
PHARMACOKINETICSDISTRIBUTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Blood-Brain BarrierThis barrier is an additional lipid barrier that protects the brain by restricting the passage of electrolytes & other water-soluble substances
Since brain composed of large amts of lipids, lipid-soluble drugs pass readily to the brain
To penetrate the central nervous system, a drug must cross the blood-brain barrier
PHARMACOKINETICSDISTRIBUTION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACOKINETICSMETABOLISM
ADME
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Whenever a drug is taken into the body – the body immediately starts trying to eliminate it Why you can smell alcohol on someone's breath – part of ethyl alcohol excreted via respiratory system
Metabolism is the chemical alteration of drugs & foreign compounds in the body
PHARMACOKINETICSMETABOLISM
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
LIVER is the main organ involved in metabolismGrp of enzymes found in liver are called DMMS (drug microsomal metabolizing system)
DMMS uses cytochrome P-450 enzymes that are important in oxidation & reduction rxns that convert drugs into their metabolites (next slide)
Function of DMMS: convert lipid-soluble drugs into water-soluble so they can be excreted by kidneys & not reabsorbed into circulationRemember: lipid drugs more readily absorbed
Water-soluble form of drugs can be excreted
PHARMACOKINETICSMETABOLISM
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Metabolites will be formed during metabolismMetabolic product Is more ionized/polar/hydrophilic then the original drug Increase excretion of the drug
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
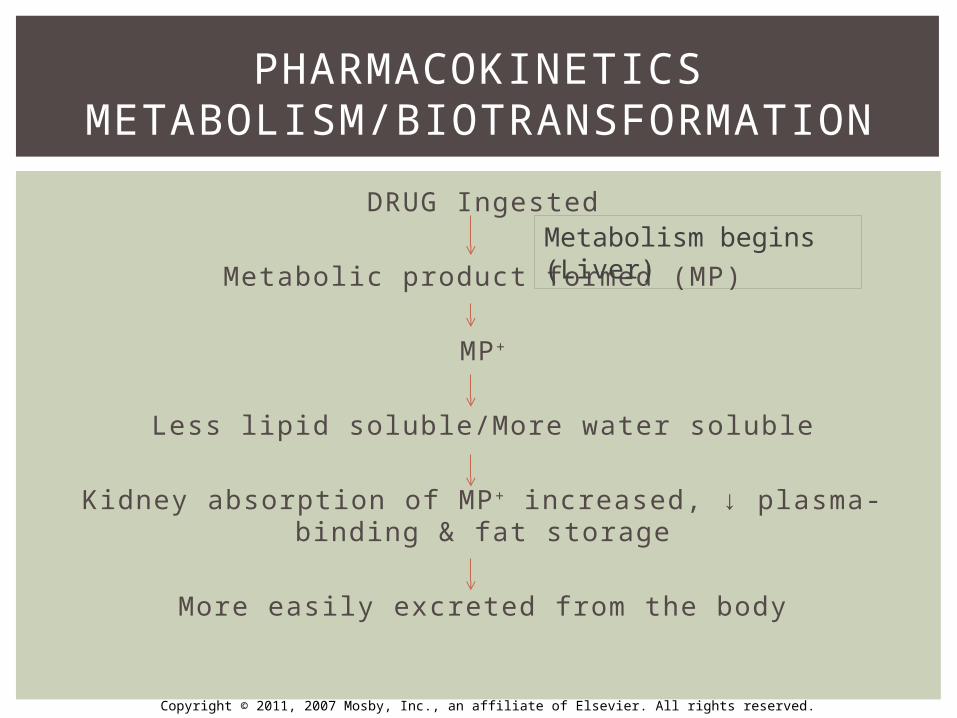
DRUG Ingested
Metabolic product formed (MP)
MP+
Less lipid soluble/More water soluble
Kidney absorption of MP+ increased, ↓ plasma-binding & fat storage
More easily excreted from the body
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Metabolism begins (Liver)
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drug metabolism is an enzyme-dependent process
Drugs can be metabolized 3 ways1. Active to inactive
An inactive metabolite is formed from an active drug
Most common process2. Inactive to active
An inactive drug (also called prodrug) will be transformed to an active compound once ingested
Ex: vyvance used to tx ADHA is inactive – once ingested – changes composition in the GI tract – then active metabolite produced
Helps reduce abuse of ADHD drugs
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drugs can be metabolized 3 ways3. Active to active
An active parent drug may be converted to a second active compound, which is then converted to an inactive product
Ex: Valium is active anti-anxiety drug – metabolized into active metabolite desmethyldiazepam = Valium’s action prolonged because of its active component combining with metabolite active component
This is why Valium’s half-life can be 20 hours
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2 phases of drug biotransformation1. Phase I: occurs in liver
Place drugs into the correct chemical state to be acted upon by Phase II conjugative mechanisms
Prepares chemicals for phase II metabolism and subsequent excretion
Drugs that are lipid soluble go through, if water form – can skip this phase
2. Phase II True “detoxification” step in the metabolism process
Turns drugs into highly water-soluble compounds
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
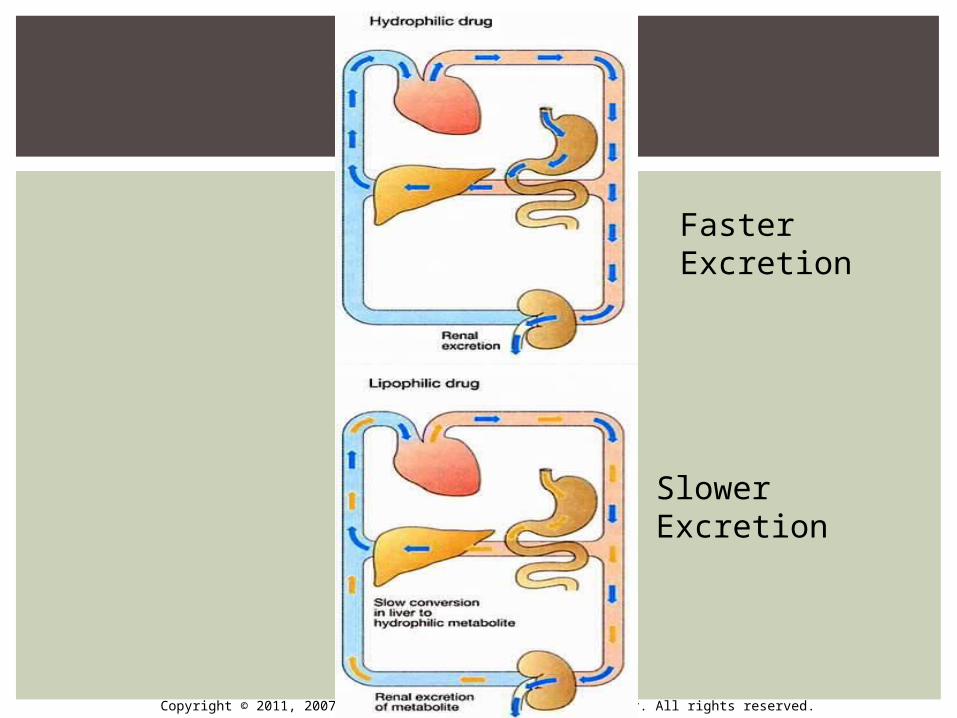
Faster Excretion
Slower Excretion
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Phase I Liver uses enzymes to make lipid-soluble drugs more
water-soluble by adding or unmasking functional groups
(-OH, -SH, -NH2, -COOH, etc.) Cytochrome P450 enzymes located in liver
Concentration affected by drugs like ethanol, narcotics, barbiturates, smoking, etc…
When take these drugs repeatedly, P-450 enzyme concentrations will ↑ in the body = called enzyme induction
↑ P450 = ↑ rate of metabolism = thus a↓ in effects of meds taken
Ex: smoker/alcoholics have higher levels of P-450 = LA will not work as effectively and they will need higher levels of to achieve full anesthesia
TOLERANCE patients develop to drugs/meds explained in part by P-450 actions
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Table 2-1 lists drugs that increase (induce) P-450 enzymes
List to know for boards: Alcohol, tobacco, antidepressants,
anticonvulsants, NSAIDs, antidepressants, antipsychotics, antiarrhythmics, erythromycin, antidepressants, benzos, calcium-channel blockers, opioids
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Different P-450 enzymes1. CYP3A4
Most common enzyme that metabolizes drugs used in dentistry
Ex: lidocaine, erythromycin, clarithromycin2. CYP2D6
Codeine, Prozac, Propranolol3. CYP2C9
Ibuprofen
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Certain drugs can decrease or increase action of these enzymesEx: grapefruit juice inhibits CYP3A4 metabolism of Xanax – results in elevation of drug in system
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Phase I Lipid molecules are metabolized by the 3 processes
1. Oxidation: Causes the loss of part of the drug molecule by incorporating O2 into the drug. MOST COMMON
2. Reduction: occurring in liver with hepatic enzymes3. Hydrolysis: Adding water to molecules
Ex: ester compounds metabolized this way. Enzymes found in plasma = break up ester & add H2O. Ester anes inactivated by plasma cholinesterases
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
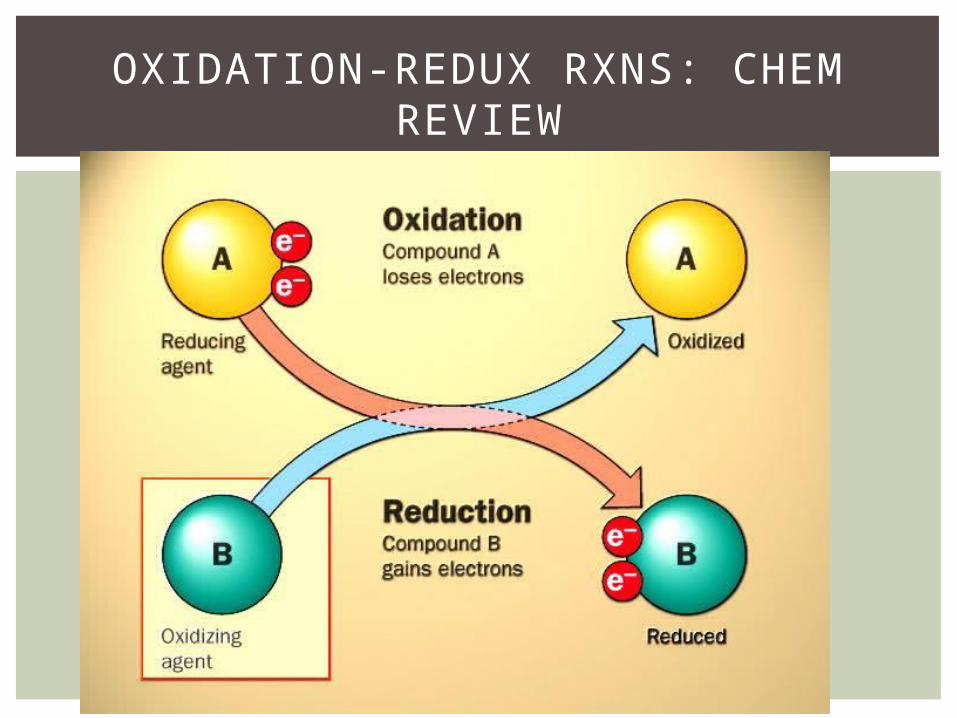
OXIDATION-REDUX RXNS: CHEM REVIEW

Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Phase II Involve conjugation with endogeneous
substrates to further increase water solubility of the drug Glucuronic acid, acetic acid, amino acid, sulfuric
acid The most common conjugation occurs with
glucuronic acid
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Phase I and II - Summary:
Products are generally more water solubleThese reactions products are ready for renal excretionThere are many complementary, sequential and
competing pathwaysPhase I and Phase II metabolism are a coupled
interactive system interfacing with endogenous metabolic pathways
PHARMACOKINETICSMETABOLISM/BIOTRANSFORMATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Displacement of a drug from plasma albumin binding sites would usually be expected to:
a. Decrease the amount of distributionb. Increase blood levels of the drugc. Decrease the metabolism of the drugd. Increase the metabolism of the drug
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Displacement of a drug from plasma albumin binding sites would usually be expected to:
a. Decrease the amount of distributionb. Increase blood levels of the drugc. Decrease the metabolism of the drugd. Increase the metabolism of the drug
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
What is a prodrug?Do hydrophilic drugs have faster excretion?Name something that can induce enzyme induction.
REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
PHARMACOKINETICSEXCRETION
ADME
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drugs may be excreted by any of several routes, but renal excretion is most important Lungs, bile, feces, skin, sweat, saliva, breast milk
Drugs may be excreted unchanged or as metabolites Need conversion into hydrophilic compounds first
& preferably in ionized form Acidic drugs mostly ionized by alkaline urine
Aspirin/barbiturate OD – will want patient to ingest sodium bicarb to alkaline the urine to allow for more rapid excretion of acidic drug
PHARMACOKINETICSEXCRETION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drugs may be excreted by any of several routes, but renal excretion is most important1. Renal Route2. Extrarenal routes3. Biliary routes
Drugs may be excreted unchanged or as metabolites
PHARMACOKINETICSEXCRETION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
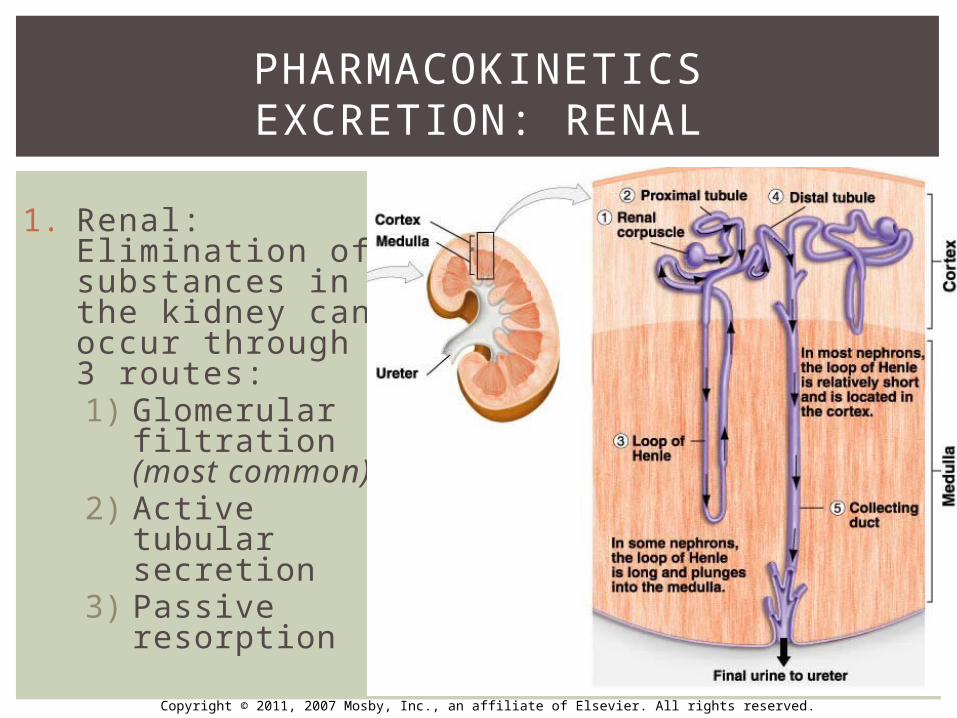
1. Renal: Elimination of substances in the kidney can occur through 3 routes:1) Glomerular
filtration (most common)
2) Active tubular secretion
3) Passive resorption
PHARMACOKINETICSEXCRETION: RENAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
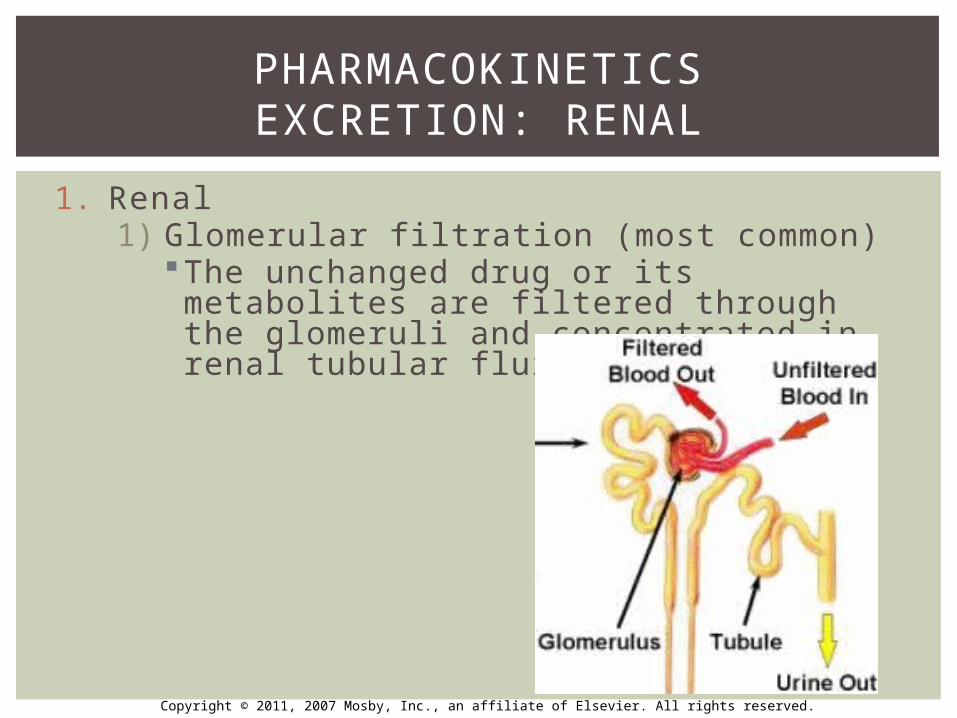
1. Renal1) Glomerular filtration (most common)
The unchanged drug or its metabolites are filtered through the glomeruli and concentrated in renal tubular fluid
PHARMACOKINETICSEXCRETION: RENAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
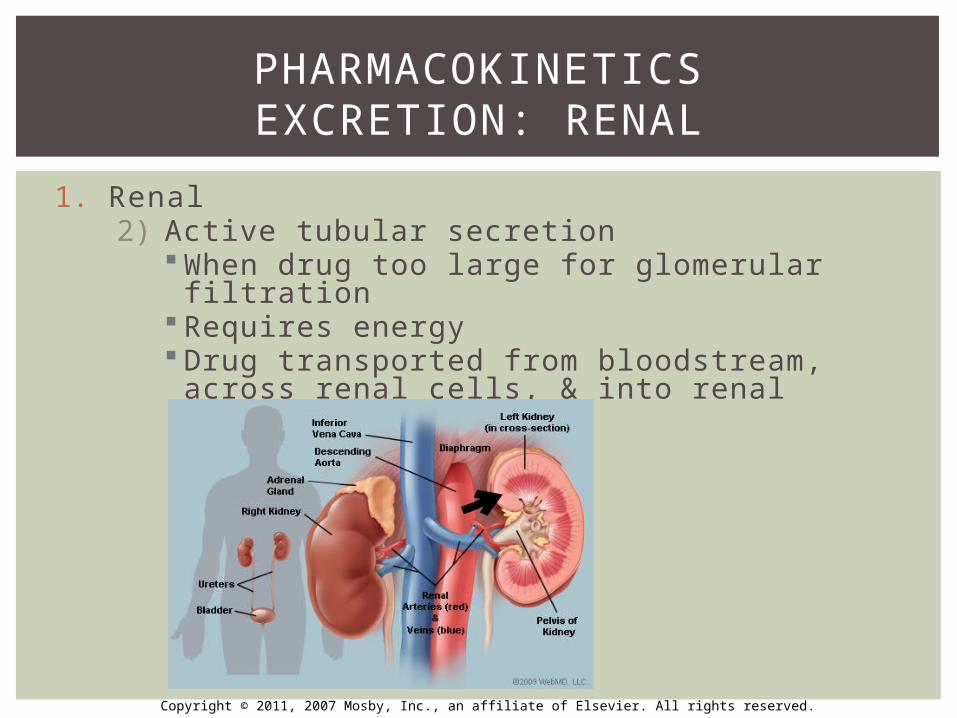
1. Renal2) Active tubular secretion
When drug too large for glomerular filtration Requires energy Drug transported from bloodstream, across
renal cells, & into renal tubular fluid
PHARMACOKINETICSEXCRETION: RENAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Renal3) Passive tubular diffusion
Keeps drugs useful to the body such as water, glucose, salts
Resorbs those drugs and puts them back into blood stream
PHARMACOKINETICSEXCRETION: RENAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
2. Extra-Renal RoutesGases used in general anesthesia are excreted across lung tissue by simple diffusion
Alcohol is partially excreted by the lungs (Breathalyzer)
PHARMACOKINETICSEXCRETION: EXTRARENAL ROUTES
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
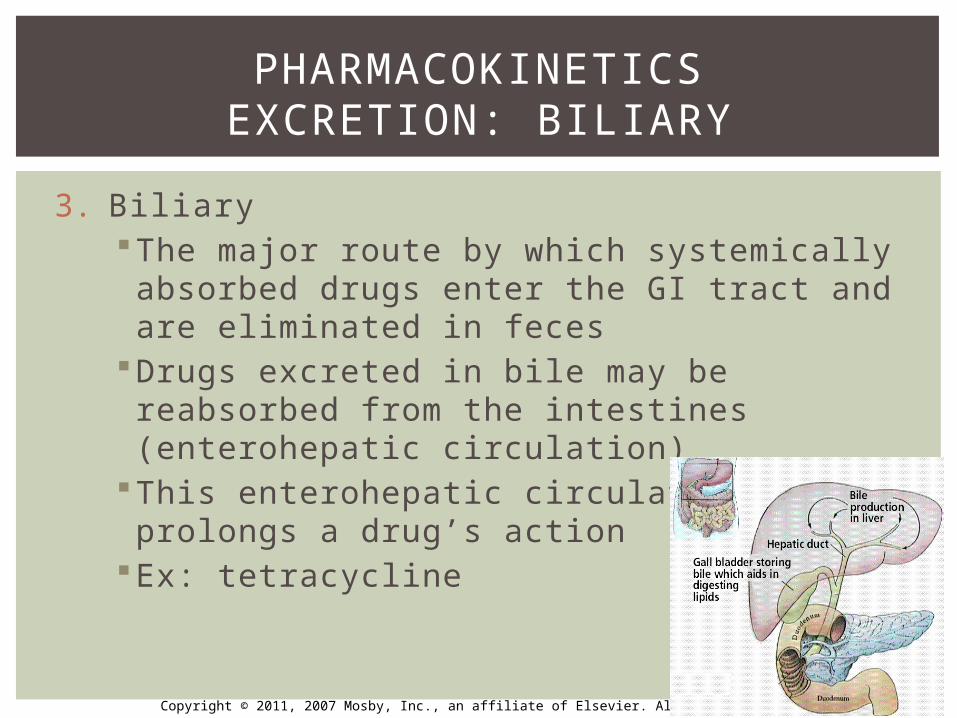
3. BiliaryThe major route by which systemically absorbed drugs enter the GI tract and are eliminated in feces
Drugs excreted in bile may be reabsorbed from the intestines (enterohepatic circulation)
This enterohepatic circulation prolongs a drug’s action
Ex: tetracycline
PHARMACOKINETICSEXCRETION: BILIARY
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Half-Life2. Kinetics3. Drug Dose
PHARMACOKINETICSCLINICAL APPLICATIONS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
READ P.18 “HALF-LIFE”
PHARMACOKINETICS1.) HALF-LIFE
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
The amount of time that passes for the concentration of a drug to fall to 1/2 of its original level
Indicator of how long a drug will produce its effect in the body
Helps define time intervals between dosesWhen the half-life is short = duration of
action is shortWhen the half-life is long = duration of action
is long
PHARMACOKINETICS1.) HALF-LIFE
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Uusally need 4-5 half-lives for drug to be completely eliminatedPen VK given 4x/day but Amox only given 3x/day Due to difference in half-lives of 2 drugs
Half-life of 2% Lidocaine w 1:100,000 is 90-120 minutes
Why many patients need more anesthetic during long procedures?
PHARMACOKINETICS1.) HALF-LIFE
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
The mathematical representation of the way in which drugs are removed from the body
First & Zero Oder Kinetics/Eliminationhttp://www.youtube.com/watch?v=iwVqXeSIOEc
PHARMACOKINETICS2.) KINETICS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
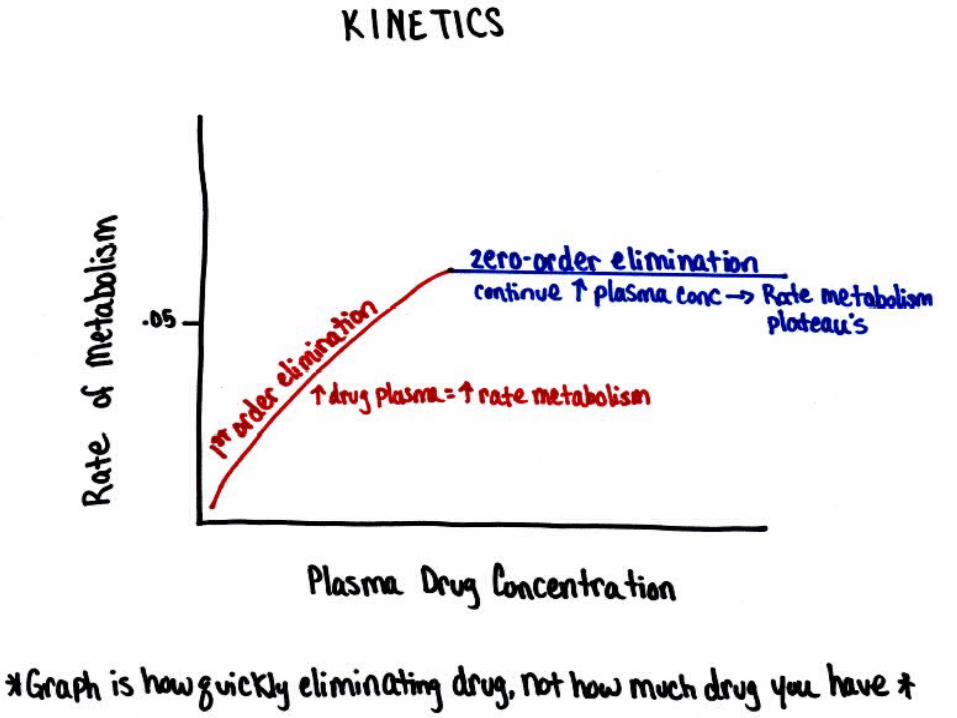
1. Kinetics: First-order kinetics Most drug elimination follows 1st-order Rate of drug metabolism is proportional to drug
concentration Constant % of drug eliminated from body per unit of
time In = Out Effect: half life of drug is constant and predictable
Half life is the amount of time it takes to eliminate 50% of the drug
Clinician knows exactly what will happen and when Decrease chances of toxicity ↑ drug concentration = ↑ rate of metabolism
PHARMACOKINETICS2.) KINETICS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
1. Kinetics: Zero-Oder Kinetics Clinicians do not want to be at zero order
kinetics/elimination because the drug plasma is increasing but the body is not eliminating it
In = Out Effect: drug will build-up and can lead to toxicity Clinician cannot predict when body will eliminate
the drug Drug elimination is at a constant rate in spite of
the amt of drug present Ex: aspirin, alcohol, phenytoin(anti-seizure)
Too many beers = can lead to high blood plasma concentrations as enter into zero-order kinetics = toxicity = death
PHARMACOKINETICS2.) KINETICS
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Drug dose: quantity of a drug administeredDrug w/high rate of absorption = smaller doses neededDrug w/high rate of elimination = larger doses neededLoading dose: large initial dose to rapidly establish a
therapeutic plasma drug concentration May need to establish a rapid response in life-
threatening situationsMaintenance dose: subsequent doses that are smaller
than loading dose Maintained for a desired stead-state plasma drug
concentration
PHARMACOKINETICS3.) DRUG DOSING
Ex: Pen VK for dental infections1,000mg immediately (loading dose)500mg 4x/day doses (maintenance dose)
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
What is half-life?What is a loading dose?What is a maintenance dose?
REVIEW
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
OBJECTIVE #3ROUTE OF DRUG ADMINISTRATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Routes of AdministrationEnteral: Drugs absorbed from GI system
Oral, sublingual, buccal, rectalSlower onset of action than parenterally administered agents
Parental: Bypass GI system IV, IM, Subcutaneous, Intradermal, Intrathecal
Topical
OBJECTIVE #3ROUTE OF DRUG ADMINISTRATION
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Oral PO: written Rx directions, means oral route Most common, convenient route
Sublingual & Buccal (between cheek & tongue) Absorption through mucosa
Rectal Suppository used when a drug is too irritating to
stomach, patient nauseous, cannot swallow, pt unconscious
Common route for infants, children, older adults
ROUTE OF DRUG ADMINISTRATIONENTERAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
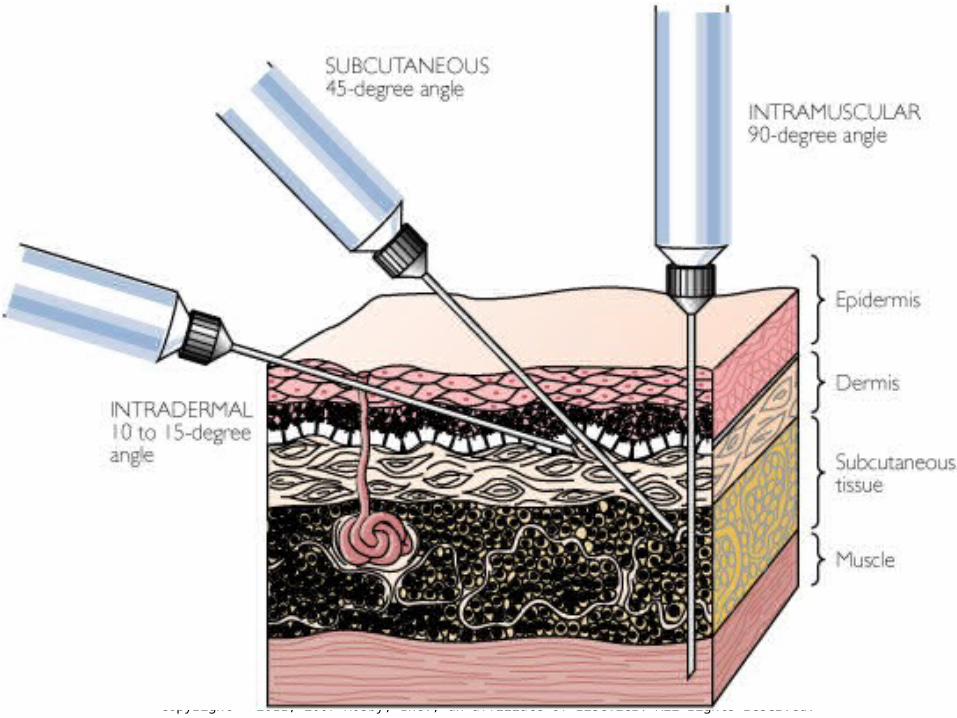
Deliver drugs under skin, subcutaneous tissue. Muscle, cerebral spinal fluid, veins
Needle at different degree depth and anglesFast absorption, rapid onsetUseful for emergencies, unconsciousness,
lack of cooperation, or nauseaSome drugs must be administered by
injection to remain active (insulin)Need good asepsis
ROUTE OF DRUG ADMINISTRATIONPARENTAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
IVAdministered via veinUsed for emergencyProduces the most rapid drug
responseThe absorption phase is bypassed
More predictable drug response because easy to control drug dose
ROUTE OF DRUG ADMINISTRATIONPARENTAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
INTRAMUSCULARAbsorption of drugs injected into the muscle
occurs as a result of high blood flow through skeletal muscle
Useful for irritating drugsRapid absorption: many blood vessels in
musclesSite: deltoid, gluteus muscleHep B vaccine
ROUTE OF DRUG ADMINISTRATIONPARENTAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
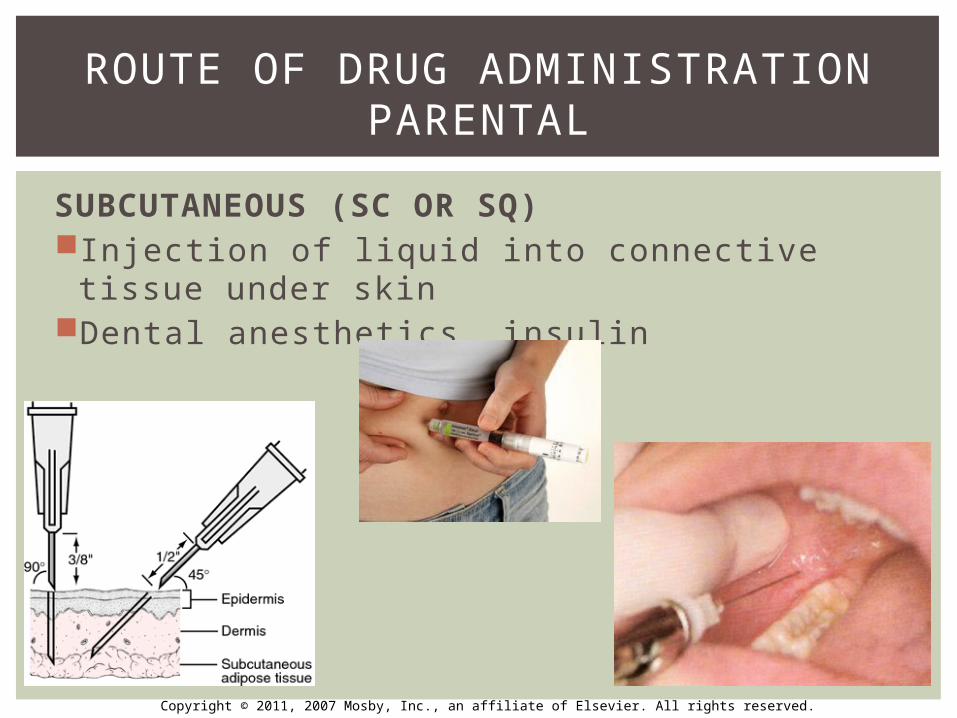
SUBCUTANEOUS (SC OR SQ)Injection of liquid into connective tissue
under skinDental anesthetics, insulin
ROUTE OF DRUG ADMINISTRATIONPARENTAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
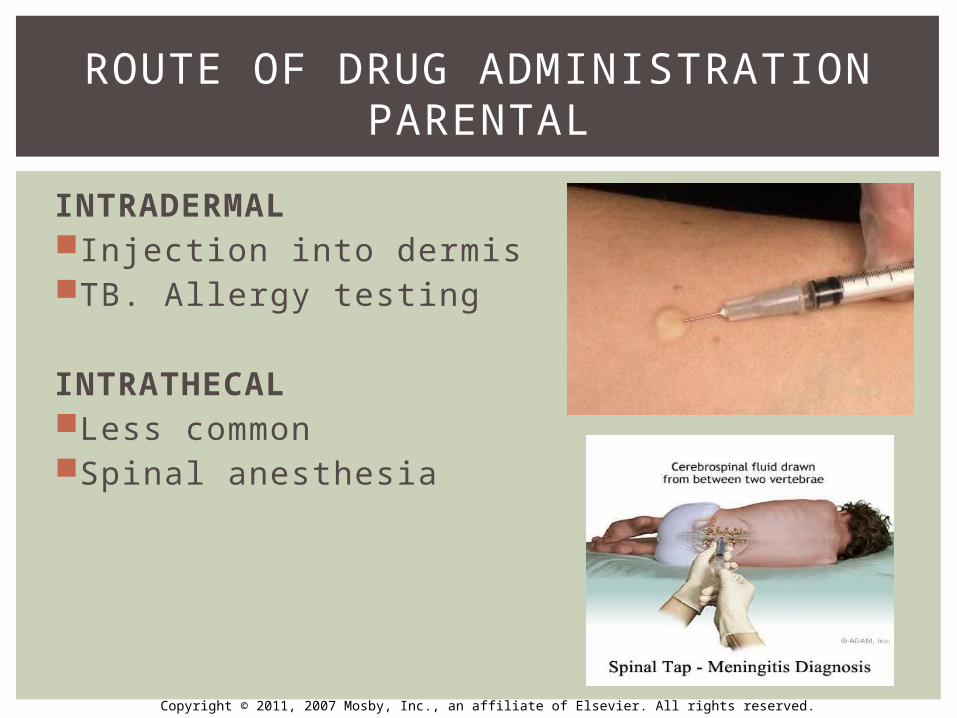
INTRADERMALInjection into dermisTB. Allergy testing
INTRATHECALLess commonSpinal anesthesia
ROUTE OF DRUG ADMINISTRATIONPARENTAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Application to body surfacesMajor barrier is stratum corneum
(outermost layer of skin)Some absorption systemicallyCan be done through
1) Sublingual administration: Oraquix, dental antibiotics (Arestin, Atridox, PerioChip) admin through GCF
2) Nasal passages or trachea: rapid absorption due to presence many capillaries in resp tract, dosing difficult
3) Transdermal: nitroglycerine, smoking cessation
ROUTE OF DRUG ADMINISTRATIONTOPICAL
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following routes will a drug follow after intravenous administration?
a. Vein, general circulation, liver, kidneyb. Esophagus, stomach, small intestine, liver, kidneyc. Liver, small intestine, kidneyd. Vein, liver, general circulation, kidney
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following routes will a drug follow after intravenous administration?
a. Vein, general circulation, liver, kidneyb. Esophagus, stomach, small intestine, liver, kidneyc. Liver, small intestine, kidneyd. Vein, liver, general circulation, kidney
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following reasons explains why an IV drug achieves very high initial blood concentration levels?
a. Drugs made of small moleculesb. Drugs have a higher pHc. No barrier to absorptiond. Expensive to give
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following reasons explains why an IV drug achieves very high initial blood concentration levels?
a. Drugs made of small moleculesb. Drugs have a higher pHc. No barrier to absorptiond. Expensive to give
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following routes of drug administration bypasses the GI tract?
a. Intravenousb. Oralc. Buccald. Sublingual
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
Which of the following routes of drug administration bypasses the GI tract?
a. Intravenousb. Oralc. Buccald. Sublingual
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
A patient had an injection of lidocaine with epi. Which of the following types of injections was given?
a. Subcutaneousb. Intravenousc. Intramusculard. Sublingual
NBQ
Copyright © 2011, 2007 Mosby, Inc., an affiliate of Elsevier. All rights reserved.
A patient had an injection of lidocaine with epi. Which of the following types of injections was given?
a. Subcutaneousb. Intravenousc. Intramusculard. Sublingual
NBQ