Embed Size (px)
Citation preview

Accepted Manuscript
Central mechanisms of airway sensation and cough hypersensitivity
Alexandria K. Driessen, Alice E. McGovern, Monica Narula, Seung-Kwon Yang,Jennifer A. Keller, Michael J. Farrell, Stuart B. Mazzone
PII: S1094-5539(17)30016-0
DOI: 10.1016/j.pupt.2017.01.010
Reference: YPUPT 1584
To appear in: Pulmonary Pharmacology & Therapeutics
Received Date: 12 January 2017
Accepted Date: 25 January 2017
Please cite this article as: Driessen AK, McGovern AE, Narula M, Yang S-K, Keller JA, Farrell MJ,Mazzone SB, Central mechanisms of airway sensation and cough hypersensitivity, PulmonaryPharmacology & Therapeutics (2017), doi: 10.1016/j.pupt.2017.01.010.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Central mechanisms of airway sensation and
cough hypersensitivity
Alexandria K. Driessen1, Alice E. McGovern1, Monica Narula2, Seung-Kwon
Yang2, Jennifer A. Keller2, Michael J. Farrell3 and Stuart B. Mazzone1*
1Department of Anatomy and Neuroscience, The University of Melbourne, Australia
2 School of Biomedical Sciences, The University of Queensland, Australia
3Biomedicine Discovery Institute and Department of Medical Imaging and Radiation Sciences, Monash
University, Australia
*Author for correspondence: Department of Anatomy and Neuroscience, The University of Melbourne,
Parkville, Melbourne, VIC 3010, Australia
Email: [email protected]
Phone: +61 3 8344 6457
Funding: NHMRC of Australia #1078943

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Abstract
The airway sensory nervous system is composed of two anatomically distinct
processing pathways that allow for the production of respiratory reflexes and voluntary
evoked respiratory behaviours in response to sensing an airway irritation. Disordered
sensory processing is a hallmark feature of many pulmonary disorders and results in
the development of cough hypersensitivity syndrome, characterised by chronic cough
and a persistent urge-to-cough in affected individuals. However, the mechanism
underpinning how the airway sensory circuits become disordered, especially at the
level of the central nervous system, is not well understood. In this mini-review we
present well-defined mechanisms that lead to the development of chronic pain as a
framework to explore the evidence that cough disorders may manifest due to
neuroplasticity and sensitisation of important components of the airway sensory
circuitry in the brain. We highlight recent discoveries of how airway sensory
processing occurs in the brain in health and disease and additionally suggest areas
where gaps exist in our current knowledge on the topic, with the goal of providing a
better understanding of how airway circuits become dysfunctional in disease. This
may in turn help identify novel therapeutic targets for restoring normal airway sensory
processing and alleviating excessive cough.
Keywords: Central sensitization; Vagal afferents; Brainstem; Descending inhibition;
Neuroinflammation; fMRI

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1.0 Introduction
The airways are innervated by heterogeneous populations of jugular and nodose vagal
ganglia sensory neurons that respond to a wide range of chemical and mechanical
stimuli. Activation of these sensory neurons results in the transmission of information
about the airway environment, firstly to the brainstem and then to higher order brain
regions, allowing for the production of both respiratory and autonomic reflexes, as well
as more complex behavioural respiratory responses. Collectively, these reflexes and
respiratory behaviours serve to protect the airways from endogenous or exogenous
stimuli that are potentially damaging and by doing so they contribute to the maintenance
of adequate physiological respiratory function. The characterisation and physiology of
airway vagal afferent neurons has been reviewed in detail, as has the neuroanatomical
organisation of airway vagal afferent pathways in the brain (Widdicombe, 2001, Carr
and Undem, 2003, Canning et al., 2006, Driessen et al., 2016, Mazzone and Undem,
2016), and as such the present review will only briefly cover these topics. Rather, we
will focus on plasticity in the central neural circuitry involved in airway sensory
processing and the current understanding of how this may provide insight into the
airway sensory dysfunctions that underpin two prominent and related clinical
presentations in pulmonary disease; excessive coughing and the urge-to-cough. In doing
so, we will present some original data and draw from the advanced work that has been
conducted in a comparable area of research (chronic pain), with the aim of highlighting
important gaps in our current understanding of central cough neurophysiology.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2.0 Neuroanatomy of airway sensation
The central representation of jugular and nodose airway afferents has been investigated
using a variety of physiological and neuroanatomical techniques (McGovern et al.,
2012a, McGovern et al., 2012b, Driessen et al., 2015, McGovern et al., 2015a,
McGovern et al., 2015b). Such studies have described in detail a primary termination
site for airway vagal afferents in the brainstem nucleus of the solitary tract (nTS) and
not surprisingly this nucleus has underpinned a substantial body of work on airway
sensory neurotransmission (Katz and Karten, 1983, Kubin et al., 1991, Panneton, 1991,
Ranson et al., 1995, Mazzone and Canning, 2002, Alheid et al., 2011, Zoccal et al.,
2014). However, our own tracing studies from the airways using a novel Herpes
Simplex Virus 1 strain H129 (HSV1 H129) anterograde transynaptic tracer recently
described a second primary termination site for airway vagal afferents in the brainstem
paratrigeminal nucleus (Pa5) (McGovern et al., 2012a, McGovern et al., 2015a,
McGovern et al., 2015b). The Pa5 is a small obscure region of brainstem neurons
located within the tract of the medullary spinal trigeminal nucleus, previously described
as playing a role in somatic nociception, but not recognised for playing a role in airway
sensation (Phelan and Falls, 1989; Lapa and Watanabe, 2005; Koepp et al., 2006).
Using conventional retrograde neuroanatomical tracing from the nTS and Pa5 we have
further shown that the nodose and jugular vagal ganglia have distinct and specific
projections to these two termination sites (Driessen et al., 2015, McGovern et al.,
2015b). Thus, the nodose vagal ganglia display terminations only in the nTS, while the
jugular vagal ganglia predominately project to the Pa5 (Driessen et al., 2015, McGovern
et al., 2015b). This observation is striking and coincides with the reported distinct
embryological origins of nodose and jugular neurons – the former derived from the
epibranchial placodes and the latter from the somatic neural crest. This anatomical

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
segregation of nodose and jugular afferent processing at the level of the brainstem is
conserved in the ascending higher brain pathways, inasmuch as a comparison of airway
specific projections arising from the nTS and Pa5 showed that nodose-nTS afferents
project largely to regions previously identified in autonomic and limbic/paralimbic
pathways, perhaps representing a central viscerosensory processing circuit in the brain,
while the jugular-Pa5 pathway projects largely to regions involved in somatic
nociceptive (somatosensory) processing (McGovern et al., 2015b). This notion of
multiple cortical circuits involved in airway sensations has been supported by studies in
humans using functional brain imaging (Farrell et al., 2012; Ando et al., 2014; Farrell et
al., 2014), however whether this relates to the anatomical segregation of airway afferent
processing observed in animal models remains unclear.
These data clearly argue for two anatomically distinct airway sensory processing
pathways that may form an anatomical framework for functional distinctions between
respiratory reflex production and the conscious perception of airway irritations. For
example, reflexive cough is a brainstem-mediated process that requires sensory input
into the nTS and subsequent alterations to the activity of respiratory cells located in
nuclei of the ventral and pontine respiratory groups (Baekey et al., 2003, Poliacek et al.,
2009, Mazzone et al., 2011, Smith et al., 2013, Dutschmann et al., 2014, Koshiya et al.,
2014, Zoccal et al., 2014, Ferreira et al., 2015, Wang et al., 2015). On the other hand,
the central mechanisms that underpin the conscious perception of airway sensations
leading to voluntary respiratory behaviours are less well understood and could
conceivably be linked to the understudied somatic representation of airway sensation in
the brain that is seemingly carried by the jugular-Pa5 circuitry. Although this
speculation awaits empirical evidence, it provides intriguing possibilities for

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
interventional regulation of airway sensations without disturbing fundamental protective
reflexes. It also provides unexplored possibilities by which airway sensory processes
may become disordered in disease.
3.0 Can airway afferent circuits in the brain be altered in disease?
Neuronal sensitization. Disordered airway sensory neural circuit activity, precipitated
(for example) by the inflammatory processes induced by acute viral or allergen
exposure or that associated with chronic illness in asthma or other respiratory diseases,
contribute to excessive coughing and the increased perception of airway irritation
common to many pulmonary disorders (Chung et al., 2013, Ando et al., 2014, Hilton et
al., 2015, Ando et al., 2016, Zaccone et al., 2016). As such, it has become increasingly
important to understand how airway sensory circuits are altered in these disease states, a
topic that has been investigated in some detail with respect to the primary afferent
neurons themselves (peripheral sensitisation) but largely unexplored in terms of the
central neural circuits in receipt of airway sensory inputs (central sensitisation).
Surprisingly, the notion of central sensitisation as a mechanism of airway sensory
hypersensitivity has been widely presented in the literature without substantive evidence
for central circuit plasticity or even a well-presented framework for what could be
expected if airway sensory circuits in the brain undergo disease-induced changes. Such
a framework can be laid down by looking at other nociceptive systems where the
mechanisms of central neural plasticity have been extensively investigated. Perhaps the
best example of this is in the chronic pain field where the inflammatory and neuropathic
mechanisms leading to changes in central circuit connectivity, neuronal excitability and
gene expression are well described (Latremoliere and Woolf, 2009, Undem et al., 2015,
Bettini and Moore, 2016).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
The similarities between, somatic and airway afferent neurophysiology supports the
notion that common mechanisms may underlie the development of pain and cough
hypersensitivities (Mazzone et al., 2009, Ji, 2015, Undem et al., 2015, Ando et al.,
2016). Indeed, chronic pain and cough are characterised by common phenotypes that
relate to underlying inflammatory and/or neuropathic processes (Latremoliere and
Woolf, 2009, Chung et al., 2013, Ji, 2015). These include hyperalgesia/hypertussia
(increased pain/cough sensitivity to noxious stimuli), allodynia/allotussia (increased
pain/cough responsivity to innocuous stimuli) and paraesthesia (abnormal sensations
such as numbness or tingling in the affected tissue) (Latremoliere and Woolf, 2009,
Chung et al., 2013, Ji, 2015). In chronic pain, these phenotypes occur due to peripheral
and/or central sensitisation processes (Latremoliere and Woolf, 2009). Peripheral
sensitisation occurs following tissue damage, whereby the release of inflammatory
mediators alters sensory neuron excitability and gene expression within the sensory
neuron cell bodies and at their peripheral terminals (Latremoliere and Woolf, 2009,
Bettini and Moore, 2016). This sensitisation is restricted to a localised area of damage
and drives hypersensitivities at the injury site (Latremoliere and Woolf, 2009, Bettini
and Moore, 2016). The evidence for peripheral sensitisation in chronic cough has been
reviewed elsewhere and won’t be repeated here (Undem et al., 2015; Zaccone and
Undem, 2016; Mazzone and Undem, 2016).
Second order neuron plasticity. Persistent sensory nerve input to the central nervous
system can induce alterations in central neural circuits by changing second order
sensory neuron excitability and their projection profiles, although in the case of nerve
injury central sensitisation can be induced without prior peripheral sensitisation

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
(Latremoliere and Woolf, 2009, Liang et al., 2016). This allows for an uncoupling of
responses to any direct noxious stimulation and thus these processes are important for
the development of secondary hyperalgesia (hypersensitivity outside of the injury zone)
and allodynia (Latremoliere and Woolf, 2009). The induction and maintenance of
centrally sensitised pain states depends on both acute and chronic processes, initially at
the level of the primary afferent synapse in the spinal dorsal horn (Bettini and Moore,
2016). Alterations that occur in the acute phase are remarkably similar to those seen in
peripheral sensitisation, except that they affect second order sensory neurons and their
projections throughout the central nervous system (Latremoliere and Woolf, 2009,
Cornelison et al., 2016, Liang et al., 2016). That is the release of inflammatory
cytokines, neurotrophins and neuropeptides drives hyperexcitability in second order
sensory neurons (Tao et al., 2014, Bettini and Moore, 2016). Collectively these
processes increase the excitability of the post-synaptic neurons in the spinal dorsal horn
and therefore lead to increased activation of neurons elsewhere in key pain processing
regions such as the raphe nuclei in the brainstem and the anterior cingulate and
somatosensory cortices in the higher brain (Li et al., 2014, Tao et al., 2014, Liang et al.,
2016, Potter et al., 2016). This enhanced excitability is largely driven by increased
synaptic delivery of ion channels, transporters, neuropeptides and vesicle release
machinery that are necessary to facilitate and strengthen glutamatergic transmission
(Latremoliere and Woolf, 2009, Tao et al., 2014, Radwani et al., 2016).
With respect to cough, studies have shown that airway afferent second order neurons in
the brainstem can similarly become hyperexcitable (Mutoh et al., 2000, Mazzone and
Canning, 2002, Mazzone et al., 2005, Kline et al., 2007, Sekizawa et al., 2008, Undem
et al., 2015). More specifically, exposure of the airways to environmental pollutants,

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
such as cigarette smoke, is known to increase excitability of nTS neurons with the
neuropeptide substance P playing an essential role in driving increased synaptic
neurotransmission (Mutoh et al., 2000, Sekizawa et al., 2008). Consistent with this, the
activation of pulmonary C-fibre afferents (many of which express neuropeptides)
acutely enhances mechanoreceptor (glutamatergic) reflexes via a brainstem
neuropeptide-dependent mechanism (Mazzone and Canning, 2002, Mazzone et al.,
2005). While glutamatergic and ionic changes may also be directly altered, it is apparent
that dysregulation of neuropeptide expression and transmission is a key component in
the development of central sensitisation of airway sensory circuits at the level of the
sensory integration nuclei in the brainstem. Whether jugular afferent pathways similarly
drive neuropeptide-dependent sensitisation of second order Pa5 neurons has not yet
been studied. However, pulmonary infections induced by pneumovirus exposure in mice
results in elevated neuronal activity within the Pa5 (Mazzone et al., unpublished data),
suggesting that there is persistent sensory input to this region as a consequence of
airway inflammation.
Glia and neuroinflammation. The transition from acute to chronic central sensitisation
includes activation of glia that induce a state of spinal neuroinflammation, which may
reflect the persistent or altered primary sensory neuron input to the central nervous
system that promotes the development of central neuroinflammation (Gwak et al., 2012,
Ikeda et al., 2012, Trang et al., 2012, Chen et al., 2014, Gu et al., 2016, Lei et al., 2016,
Liu et al., 2016). Therefore, both peripheral nerve injury and inflammation can
upregulate the expression of glia, as marked by increased expression of CD11b (OX-42)
or ionized calcium binding adaptor molecule 1 (Iba1) for microglia activation and Glial
Fibrillary Acidic Protein (GFAP) for astrocyte activation, in both sensory ganglia

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
themselves and in the central nervous system (Ikeda et al., 2012, Romero et al., 2013,
M’Dahoma et al., 2015, Liu et al., 2016, Lei et al., 2016). More importantly,
pharmacological inhibition of glia has been shown to largely abolish enhanced neuronal
excitation in models of chronic pain, suggesting that glial cells are the primary drivers
of the neuronal hyperexcitability underpinning painful phenotypes (Ikeda et al., 2012).
Interestingly, in a model of nerve injury, spinal dorsal horn neurons become
hyperexcitable and this coincides with an increase in connexion-43 expression in
astrocytes (Chen et al., 2014). Connexin-43 is a gap junction protein that facilitates glia-
neuron cross talk, and when inhibited leads to suppression of neuronal excitation,
suggesting that more complex interactions between activated glia and neurons after
injury may further enhance the neuroinflammatory state (Chen et al., 2014). Since glia
are not electrically active they interact with neurons via neurotransmitter release, such
as cytokines or other mediators, and in line with this there is a growing body of
evidence that suggests adenosine tri-phosphate (ATP), chemokine CXCL12, interleukin
1 beta (IL-1β), tumor necrosis factor alpha (TNFα) and/or Brain Derived Neurotrophic
Factor (BDNF) may be the primary mediators released to maintain a state of central
sensitisation after peripheral injury and inflammation (Henn, 1976, Guthrie et al., 1999,
Fields and Burnstock, 2006, Ulmann et al., 2008, Trang et al., 2011, Trang et al., 2014,
M’Dahoma et al., 2015, Bai et al., 2016, Gu et al., 2016, Lalo et al., 2016). Furthermore,
the neuroinflammatory state in chronic pain is known to persist due to epigenetic
changes to second order sensory neurons, including histone modifications on important
genes including BDNF (Crow et al., 2013, Tao et al., 2014).
There is a paucity of data to indicate whether vagal ganglia or the brainstem processing
sites of airway afferents display glial activation in models of airway inflammation.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
However, recent studies may support this notion (Chounlamountry et al., 2015,
Spaziano et al., 2015). Allergen sensitisation as well as ozone exposure cause gliosis
within the nTS, and it has been speculated that this upregulation plays a role in airway
hyper-responsiveness (Chounlamountry et al., 2015, Spaziano et al., 2015). Gliosis at
glutamatergic synapses may indicate that the activation of glia could strengthen
glutamatergic transmission and in turn drive neuronal hyper-excitability in second order
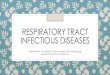
neurons (Chounlamountry et al., 2015). In our own studies, neonatal mice infected with
murine pneumovirus demonstrate a modest increase in Iba1 expression (microglial
cells) and a robust increase in GFAP expression (astrocytes), along with increased
cytokine expression, in the region of the nTS (Figure 1). This gliosis may reflect both
migration and proliferation of glia cells given that we also noted an increase in the cell
proliferation marker PCNA at this site (Figure 1). Correspondingly, influenza infection
alters nTS neuron resting membrane potential and baseline action potential firing,
consistent with a centrally sensitised state (Figure 1). Nevertheless, more extensive
studies still need to be conducted to better understand the role of activated glia in
altering airway sensory neurons but data to date suggests that it is likely an avenue
worth investigating to better understand the role of central neural plasticity in
respiratory disease.
FIGURE 1 HERE

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 1. Brainstem neuroinflammation following respiratory tract viral infection in mice. Central sensitisation in chronic pain is typically underpinned by glial cell activation and central inflammation, which contributes to synaptic plasticity and neuronal hyperresponsiveness. (A) 7 day old neonatal mice infected with an intranasal inoculation of 5 plaque forming units of pneumovirus show increased immunostaining density for the glial markers GFAP (astrocytes) and IBA1 (microglia) 3-10 days post-inoculation (DPI) in the nucleus of the solitary tract. Virus induced increase in the number of cell nuclei expressing the proliferation marker PCNA is consistent with glial cell expansion at this site (data represent the mean ± SEM of 5-7 animals per group). (B) Consistent with this, pneumovirus infected mice have elevated transcripts for the inflammatory mediators Tumor Necrosis Factor alpha (TNFα) and Interleukin 1β in brainstem homogenates (quantitative PCR, mean ± SEM fold change expression over β-actin, n=3 per group). (C) Representative patch clamp electrophysiological recording of two neurons in nucleus of the solitary tract in brainstem slices of two mice, one inoculated intranasally 7 days earlier with vehicle (VEH, lower trace) and the other inoculated with 103 plaque forming units of influenza Pr8 strain (FLU, upper trace). Of note is the more depolarised resting membrane potential and induction of spontaneous action potential discharge after viral infection. Mean data show an average 40mV shift in the resting membrane potential of nucleus of the solitary tract neurons after infection (mean ± SEM resting membrane potential of 10 neurons per group recorded from 3-4 separate preparations per treatment). *, P<0.05 significantly different to vehicle inoculated (VEH) controls.
Higher level plasticity. Plasticity and sensitisation following peripheral injuries and
inflammation are not confined to second order neurons in primary afferent processing
sites, but rather can occur at all levels of the central sensory processing circuit. In this

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
regard, it is interesting to note that unlike the data described above, which is almost
exclusively obtained from animal studies, higher brain plasticity in sensory
hypersensitivities has been studied in both animals and humans. Indeed, functional
magnetic resonance imaging (fMRI) has uniquely allowed higher brain physiological
sensory circuits to be studied in humans in both healthy and disease states (Farrell et al.,
2005, Mazzone et al., 2009, Wager et al., 2013, Farrell and Mazzone, 2014, Hodkinson
et al., 2015, Ando et al., 2016, Flodin et al., 2016). The available evidence would
suggest that sensory hypersensitivity can result from both an enhanced activity of the
brain regions encoding sensation as well as dysfunctional responses in the brain circuits
that ordinarily provide descending control over primary afferent processing (the
descending analgesia system).
In patients with chronic pain, fMRI studies have reported that there is an increased
functional connectivity at most levels of the higher order pain circuit (Zambreanu et al.,
2005, Hodkinson et al., 2015, Flodin et al., 2016). A region of particular importance in
this circuit is the somatosensory cortex where the conscious perception of sensory
stimulation for each body part is mapped onto a restricted cortical region (Endo et al.,
2007). fMRI studies in rodents have shown that in models of chronic pain the integrity
of the primary somatosensory cortex organisation is lost and instead activity extends
beyond the boundaries of the affected region resulting in an increased receptive field
and hyperalgesia (Endo et al., 2007, Potter et al., 2016). Although these changes may
result due to increased afferent input, local mechanisms within the primary
somatosensory cortex have also been identified in rodent models of chronic pain. These
include upregulation of excitatory synapses by significantly increased vesicular
glutamate transporter 1 (VGlut1) synaptic density as well as activation of local

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
astrocytes (Kim et al., 2016, Potter et al., 2016). These profound alterations drive an
excitatory-inhibitory imbalance allowing for dysfunctional pain processing to persist.
Similarly, imaging studies in humans with painful trigeminal neuropathy show signs of
decreased grey matter volume and blood flow to the primary somatosensory cortex as
well as the thalamus (Henderson et al., 2013). These changes represent functional
cortical plasticty as they are correlated with reported increased ongoing pain (Henderson
et al., 2013). In line with human imaging studies, the thalamus and subthalamus have
also been implicated in rodent models of chronic pain whereby changes in the gating
and processing of nociceptive information have been observed (Whitt et al., 2013, Masri
et al., 2009). For example, thalamic sensory regulation is in part dependent on tonic
inhbitory signals from the zona incerta (a subthalamic nucleus) and after spinal cord
injury, neurons of the zona incerta have a decreased firing rate leading to increased
thalmic neuron discharge in response to noxious stimulation (Whitt et al., 2013, Masri et
al., 2009). Thus, the balance between excitatory and inhibitory control within the pain
circuitry is lost and pain signals are processed without appropriate gating allowing for
both hyperalgesia and allodynia to result.
A well described descending circuit provides top down control over ascending
nociceptive processing, and recent studies suggest that this circuit may also undergo
changes in patients with chronic pain. The most extensively studied of these descending
circuits is that involved in pain inhibition, also known as the descending analgesia
system, largely controlled by a neuronal circuit that originates in the frontal cortex and
descends upon the spinal dorsal horn via connections in the midbrain periaqueductal
gray (PAG) and rostral ventromedial medulla (RVM) (Boadas-Vaello et al., 2016). The
RVM contains both ON and OFF cells, which enhance or inhibit pain respectively

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
(Boadas-Vaello et al., 2016). ON cells receive inhibitory control from the PAG in order
to allow for the firing of OFF cells and it is this balance that ultimately provides
endogenous anti-nociceptive benefits (Boadas-Vaello et al., 2016). However, in chronic
pain conditions alterations in the PAG change the balance of excitatory to inhibitory
control, leading to the development of primary and secondary hyperalgesia (Liu et al.,
2010, Hahm et al., 2011, Schwedt et al., 2014, Ho et al., 2015, Boadas-Vaello et al.,
2016). For example, spinal nerve ligations in the rat resulted in both altered
glutamatergic and GABAergic transmission in the PAG and both the PAG and RVM
display signs of neuroinflammation following peripheral injuries, which is presumably
involved in the maintenance of a centrally sensitised state (Ho et al., 2015, Zhuang et
al., 2016). In particular, models of Parkinson’s disease, where pain is a commonly
reported symptom, the dorsal lateral PAG has increased activation of pro-inflammatory
cytokines, while microglia have been shown to be activated in the RVM under
conditions of peripheral inflammatory pain (Roberts et al., 2009, Zhuang et al., 2016).
In human functional brain imaging studies, experimentally induced hyperalgesia
following subcutaneous injections of capsaicin results in a rapid induction of PAG
neuronal activity, suggestive that alterations in the descending analgesia pathway plays
an essential role in the development of hyperalgesia (Zambreanu et al., 2005).
Consistent with this, it has also been shown that these descending pain circuits have
altered connectivity in chronic pain conditions that present with allodynia (Schwedt et
al., 2014).
Patients with chronic cough may similarly display alterations in their higher brain
processing of airway irritant stimuli (Ando et al., 2016). We recently reported that
patients with chronic cough demonstrated enhanced urge-to-cough sensitivity during

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
inhaled capsaicin challenges and that this was associated with elevated activity in
midbrain regions known to be involved in descending nociceptive control. Thus, in
fMRI studies the PAG and neighbouring cuneiform nucleus showed elevated activity in
response to inhaled capsaicin, regardless of whether capsaicin concentrations were the
same for healthy and cough participants or if they were tailored to produce equivalent
behavioural outcomes in the two groups (i.e. to match the urge-to-cough intensities)
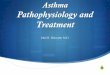
(Ando et al., 2016). Remarkably, the midbrain areas activated in our study overlap with
the areas active during experimental induction of pain hypersensitivity (Figure 2),
strongly suggesting that common central mechanisms are indeed involved in the
development or maintenance of cough and pain hypersensitivity. The midbrain,
however, was not the only higher brain region demonstrating changes in activity. Cough
hypersensitivity patients showed diminished activity compared to healthy controls in
parts of a brain network previously implicated in the voluntary suppression of coughing
(Mazzone et al., 2011, Farrell et al., 2012; Farrell et al., 2014, Ando et al., 2016).
Collectively these findings suggest that altered descending control and/or altered
voluntary cough suppression may contribute to excessive coughing and the urge-to-
cough in airways disease. However, more research is needed in this area as we don’t
know if cough hypersensitivity coincides with any changes in sensory representations in
the brain, nor do we understand the mechanisms that precipitate these changes seen with
fMRI. Furthermore, as our study described above was conducted by investigating brain
responses during inhaled irritant challenges, it will be important to know whether there
are any changes in brain activity, connectivity and/or brain morphometry in cough
patients at baseline in the absence of exogenous stimuli. In addition, whether current or
future antitussive therapies can correct altered brain activity is also unknown.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
FIGURE 2 HERE
Figure 2. A common mechanism of central sensitisation in pain and cough: functional
brain imaging studies in humans. Left panel, Subjects were treated unilaterally on the
right lower eg with a combination of heat and capsaicin to induce hyperalgesia.
Subsequent mechanical stimulation of the area evoked increased pain sensations
which were associated with unilateral increased neural activity in the midbrain nucleus
cuneiformis (reproduced with permission from Zambreanu et al., 2005). Right Panel,
Comparable activations in the midbrain nucleus cuneiformis extending into the
periaqueductal grey (PAG) in subjects with chronic cough hypersensitivity exposed to
inhaled capsaicin challenges (data adapted from Ando et al., 2016). Not shown is an
absence of midbrain activity in control subjects, consistent with the midbrain playing a
specific role in the development or maintenance of hypersensitivity.
3.0 Concluding remarks
Cough and the urge-to-cough contribute significantly to morbidity in pulmonary
diseases and as such understanding the neuronal processes that underpin the
development and maintenance of cough hypersensitivity is essential. We now have a
reasonably advanced knowledge of the central processing circuits involved in airway
sensation that will allow for hypothesis driven investigations of how the brain may
contribute to chronic coughing in disease. Although this area of research is still in its
infancy, the information that we have presented in this review highlights the likely
importance of central plasticity in the development of cough in respiratory disease.
Indeed, there is evidence that sensory circuits are subject to disease induced acute

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
changes in neuronal excitability through alterations in neurotransmission and ion
channel activity in the brainstem, and that this enhanced excitability may be maintained
and transformed to a chronic neuroinflammatory state by glial cell activation. The net
outcome is altered activity of cough regulatory circuits in the brains of patients with
chronic cough. However, there are clearly still many gaps in our understanding of the
processes and it will be important to define the mechanisms underpinning central
sensitisation and plasticity in the airway sensory circuitry as this may help to identify
novel therapeutic targets to better treat patients with sensory hypersensitivities
associated with respiratory diseases.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
References
Alheid GF, Jiao W, McCrimmon DR (2011) Caudal nuclei of the rat nucleus of the solitary
tract differentially innervate respiratory compartments within the ventrolateral
medulla. Neuroscience 190:207-227.
Ando A, Farrell MJ, Mazzone SB (2014) Cough-related neural processing in the brain: A
roadmap for cough dysfunction? Neuroscience & Biobehavioral Reviews 47:457-
468.
Ando A, Smallwood D, McMahon M, Irving L, Mazzone SB, Farrell MJ (2016) Neural
correlates of cough hypersensitivity in humans: evidence for central sensitisation
and dysfunctional inhibitory control. Thorax 71:323-329.
Baekey DM, Morris KF, Nuding SC, Segers LS, Lindsey BG, Shannon R (2003) Medullary
raphe neuron activity is altered during fictive cough in the decerebrate cat.
Journal of Applied Physiology 94:93-100.
Bai L, Wang X, Li Z, Kong C, Zhao Y, Qian JL, Kan Q, Zhang W, Xu JT (2016) Upregulation
of Chemokine CXCL12 in the Dorsal Root Ganglia and Spinal Cord Contributes to
the Development and Maintenance of Neuropathic Pain Following Spared Nerve
Injury in Rats. Neuroscience bulletin 32(1):27-40.
Bettini L, Moore K (2016) Central Sensitization in Functional Chronic Pain Syndromes:
Overview and Clinical Application. Pain management nursing : official journal of
the American Society of Pain Management Nurses 17:333-338.
Boadas-Vaello P, Castany S, Homs J, Alvarez-Perez B, Deulofeu M, Verdu E (2016)
Neuroplasticity of ascending and descending pathways after somatosensory
system injury: reviewing knowledge to identify neuropathic pain therapeutic
targets. Spinal cord 54:330-340.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Canning BJ, Mori N, Mazzone SB (2006) Vagal afferent nerves regulating the cough
reflex. Respirartory physiology and neurobiology 152(3):223-242.
Carr MJ, Undem BJ (2003) Pharmacology of vagal afferent nerve activity in guinea pig
airways. Pulmonary pharmacolology and therapeutics 16(1):45-52.
Chen G, Park CK, Xie RG, Berta T, Nedergaard M, Ji RR (2014) Connexin-43 induces
chemokine release from spinal cord astrocytes to maintain late-phase
neuropathic pain in mice. Brain : a journal of neurology 137:2193-2209.
Chounlamountry K, Boyer B, Penalba V, Francois-Bellan AM, Bosler O, Kessler JP, Strube
C (2015) Remodeling of glial coverage of glutamatergic synapses in the rat
nucleus tractus solitarii after ozone inhalation. Journal of neurochemistry
134:857-864.
Chung KF, McGarvey L, Mazzone SB (2013) Chronic cough as a neuropathic disorder.
The Lancet Respiratory medicine 1:414-422.
Crow M, Denk F, McMahon SB (2013) Genes and epigenetic processes as prospective
pain targets. Genome Medicine 5(2):12.
Driessen AK, Farrell MJ, Mazzone SB, McGovern AE (2015) The Role of the
Paratrigeminal Nucleus in Vagal Afferent Evoked Respiratory Reflexes: A
Neuroanatomical and Functional Study in Guinea Pigs. Frontiers in physiology
6:378.
Driessen AK, Farrell MJ, Mazzone SB, McGovern AE (2016) Multiple neural circuits
mediating airway sensations: recent advances in the neurobiology of the urge-to-
cough. Respiratory physiolology and neurobiology 226: 115-120.
Dutschmann M, Bautista TG, Morschel M, Dick TE (2014) Learning to breathe:
habituation of Hering-Breuer inflation reflex emerges with postnatal brainstem
maturation. Respiratory physiology & neurobiology 195:44-49.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Endo T, Spenger C, Tominaga T, Brené S, Olson L (2007) Cortical sensory map
rearrangement after spinal cord injury: fMRI responses linked to nogo signalling.
Brain 130(Pt 11):2951-2961.
Farrell MJ, Cole LJ, Chiapoco D, Egan GF, Mazzone SB (2012) Neural Correlates Coding
Stimulus Level and Perception of Capsaicin-Evoked Urge-To-Cough in Humans.
Neuroimage 61 (4): 1324-1335.
Farrell MJ, Koch S, Ando A, Cole LJ, Egan GF, Mazzone SB (2014) Functionally Connected
Brain Regions in the Network Activated During Capsaicin Inhalation. Hum Brain
Mapp 35(11):5341-5355.
Farrell MJ, Laird AR, Egan GF (2005) Brain activity associated with painfully hot stimuli
applied to the upper limb: a meta-analysis. Human brain mapping 25:129-139.
Farrell MJ, Mazzone SB (2014) Sensations and regional brain responses evoked by
tussive stimulation of the airways. Respiratory physiology & neurobiology
204:58-63.
Ferreira CB, Schoorlemmer GH, Rossi MV, Takakura AC, Barna BF, Moreira TS, Cravo SL
(2015) Brainstem areas activated by intermittent apnea in awake unrestrained
rats. Neuroscience 297:262-271.
Fields RD, Burnstock G (2006) Purinergic signalling in neuron-glia interactions. Nature
reviews Neuroscience 7:423-436.
Flodin P, Martinsen S, Altawil R, Waldheim E, Lampa J, Kosek E, Fransson P (2016)
Intrinsic Brain Connectivity in Chronic Pain: A Resting-State fMRI Study in
Patients with Rheumatoid Arthritis. Frontiers in human neuroscience 10:107.
Gu N, Eyo UB, Murugan M, Peng J, Matta S, Dong H, Wu LJ (2016) Microglial P2Y12
receptors regulate microglial activation and surveillance during neuropathic
pain. Brain, behavior, and immunity 55:82-92.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Guthrie PB, Knappenberger J, Segal M, Bennett MV, Charles AC, Kater SB (1999) ATP
released from astrocytes mediates glial calcium waves. The Journal of
neuroscience : the official journal of the Society for Neuroscience 19:520-528.
Gwak YS, Kang J, Unabia GC, Hulsebosch CE (2012) Spatial and temporal activation of
spinal glial cells: role of gliopathy in central neuropathic pain following spinal
cord injury in rats. Experimental neurology 234:362-372.
Hahm ET, Kim Y, Lee JJ, Cho YW (2011) GABAergic synaptic response and its opioidergic
modulation in periaqueductal gray neurons of rats with neuropathic pain. BMC
neuroscience 12:41.
Henderson LA, Peck CC, Petersen ET, Rae CD, Youssef AM, Reeves JM, Wilcox SL, Akhter
R, Murray GM, Gustin SM (2013) Chronic pain: lost inhibition? Journal of
neuroscience 33(17):7574-7582.
Henn FA (1976) Neurotransmission and glial cells: a functional relationship? Journal of
neuroscience research 2:271-282.
Hilton E, Marsden P, Thurston A, Kennedy S, Decalmer S, Smith JA (2015) Clinical
features of the urge-to-cough in patients with chronic cough. Respiratory
Medicine 109:701-707.
Ho YC, Cheng JK, Chiou LC (2015) Impairment of adenylyl cyclase-mediated
glutamatergic synaptic plasticity in the periaqueductal grey in a rat model of
neuropathic pain. The Journal of physiology 593:2955-2973.
Hodkinson DJ, Veggeberg R, Wilcox SL, Scrivani S, Burstein R, Becerra L, Borsook D
(2015) Primary Somatosensory Cortices Contain Altered Patterns of Regional
Cerebral Blood Flow in the Interictal Phase of Migraine. PloS one 10:e0137971.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Ikeda H, Kiritoshi T, Murase K (2012) Contribution of microglia and astrocytes to the
central sensitization, inflammatory and neuropathic pain in the juvenile rat.
Molecular pain 8:43.
Ji RR (2015) Neuroimmune interactions in itch: Do chronic itch, chronic pain, and
chronic cough share similar mechanisms? Pulmonary pharmacology &
therapeutics 35:81-86.
Katz DM, Karten HJ (1983) Visceral representation within the nucleus of the tractus
solitarius in the pigeon, Columba livia. The Journal of comparative neurology
218:42-73.
Kim SK, Hayashi H, Ishikawa T, Shibata K, Shigetomi E, Shinozaki Y, Inada H, Roh SE,
Kim SJ, Lee G, Bae H, Moorhouse AJ, Mikoshiba K, Fukazawa Y, Koizumi S,
Nabekura J (2016) Cortical astrocytes rewire somatosensory cortical circuits for
peripheral neuropathic pain. The Journal of clinical investigation 126:1983-
1997.
Kline DD, Ramirez-Navarro A, Kunze DL (2007) Adaptive Depression in Synaptic
Transmission in the Nucleus of the Solitary Tract After In Vivo Chronic
Intermittent Hypoxia: Evidence for Homeostatic Plasticity. J Neurosci 27(17):
4664-4673.
Koepp J, Lindsey CJ, Motta EM, Rae GA (2006) Role of the Paratrigeminal Nucleus in
Nocifensive Responses of Rats to Chemical, Thermal and Mechanical Stimuli
Applied to the Hind Paw. Pain 122(3):235-244.
Koshiya N, Oku Y, Yokota S, Oyamada Y, Yasui Y, Okada Y (2014) Anatomical and
functional pathways of rhythmogenic inspiratory premotor information flow
originating in the pre-Botzinger complex in the rat medulla. Neuroscience
268:194-211.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Kubin L, Kimura H, Davies RO (1991) The medullary projections of afferent
bronchopulmonary C fibres in the cat as shown by antidromic mapping. The
Journal of physiology 435:207-228.
Lalo U, Palygin O, Verkhratsky A, Grant SG, Pankratov Y (2016) ATP from synaptic
terminals and astrocytes regulates NMDA receptors and synaptic plasticity
through PSD-95 multi-protein complex. Scientific reports 6:33609.
Lapa RC, Watanabe I (2005) Synaptic contacts established by inferior alveolar nerve
fibres in the paratrigeminal nucleus: an electron microscopic study in the rat.
Archives of oral biology 50(1): 73-79.
Latremoliere A, Woolf CJ (2009) Central sensitization: a generator of pain
hypersensitivity by central neural plasticity. The journal of pain : official journal
of the American Pain Society 10:895-926.
Lei Y, Sun Y, Lu C, Ma Z, Gu X (2016) Activated Glia Increased the Level of
Proinflammatory Cytokines in a Resiniferatoxin-Induced Neuropathic Pain Rat
Model. Regional anesthesia and pain medicine 41:744-749.
Li W, Wang P, Li H (2014) Upregulation of glutamatergic transmission in anterior
cingulate cortex in the diabetic rats with neuropathic pain. Neuroscience letters
568:29-34.
Liang M, Lee MC, O'Neill J, Dickenson AH, Iannetti GD (2016) Brain potentials evoked by
intraepidermal electrical stimuli reflect the central sensitization of nociceptive
pathways. Journal of neurophysiology 116:286-295.
Liu XJ, Liu T, Chen G, Wang B, Yu XL, Yin C, Ji RR (2016) TLR signaling adaptor protein
MyD88 in primary sensory neurons contributes to persistent inflammatory and
neuropathic pain and neuroinflammation. Scientific reports 6:28188.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
M’Dahoma S, Barthélemy S, Tromilin C, Jeanson T, Viguier F, Michot B, Pezet S, Hamno
M, Bourgoin S (2015) Respective pharmacological features of neuropathic-like
pain evoked by intrathecal BDNF versus sciatic nerve ligation in rats. European
neuropsychopharmacology 25(11):2118-2130.
Masri R, Quiton RL, Lucas JM, Murray PD, Thompson SM, Keller A (2009) Zona incerta: a
role in central pain. Journal of neurophysiology 102(1):181-191.
Mazzone SB, Canning BJ (2002) Synergistic interactions between airway afferent nerve
subtypes mediating reflex bronchospasm in guinea pigs.
Mazzone SB, Cole LJ, Ando A, Egan GF, Farrell MJ (2011) Investigation of the Neural
Control of Cough and Cough Suppression in Humans Using Functional Brain
Imaging. The Journal of neuroscience 31:2948-2958.
Mazzone SB, McGovern AE, Koo K, Farrell MJ (2009) Mapping supramedullary pathways
involved in cough using functional brain imaging: Comparison with pain.
Pulmonary pharmacology & therapeutics 22:90-96.
Mazzone SB, Mori N, Canning BJ (2005) Synergistic interactions between airway
afferent nerve subtypes regulating the cough reflex in guinea-pigs. Journal of
physiology 569(Pt 2):559-573.
Mazzone SB, Undem BJ (2016) Vagal Afferent Innervation of the Airways in Health and
Disease. Physiological reviews 96(3):975-1024.
McGovern AE, Davis-Poynter N, Farrell MJ, Mazzone SB (2012a) Transneuronal tracing
of airways-related sensory circuitry using herpes simplex virus 1, strain H129.
Neuroscience 207:148-166.
McGovern AE, Davis-Poynter N, Rakoczy J, Phipps S, Simmons DG, Mazzone SB (2012b)
Anterograde neuronal circuit tracing using a genetically modified herpes simplex
virus expressing EGFP. Journal of neuroscience methods 209:158-167.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
McGovern AE, Davis-Poynter N, Yang SK, Simmons DG, Farrell MJ, Mazzone SB (2015a)
Evidence for multiple sensory circuits in the brain arising from the respiratory
system: an anterograde viral tract tracing study in rodents. Brain structure &
function 220:3683-3699.
McGovern AE, Driessen AK, Simmons DG, Powell J, Davis-Poynter N, Farrell MJ, Mazzone
SB (2015b) Distinct Brainstem and Forebrain Circuits Receiving Tracheal
Sensory Neuron Inputs Revealed Using a Novel Conditional Anterograde
Transsynaptic Viral Tracing System. The Journal of Neuroscience 35:7041-7055.
Mutoh T, Bonham AC, Joad JP (2000) Substance P in the nucleus of the solitary tract
augments bronchopulmonary C fiber reflex output.
Panneton WM (1991) Primary afferent projections from the upper respiratory tract in
the muskrat. The Journal of comparative neurology 308:51-65.
Phelan KD, Falls WM (1989) The interstial system of the spinal trigeminal tract in the
rat: anatomical evidence for morphological and functional heterogeneity.
Somatosensensory motor research 6(4): 367-399.
Poliacek I, Tomori Z, Simera M, Barani H, Visnovcova N, Halasova E, Donic V, Jakus J
(2009) Provocation of aspiration reflexes and their effects on the pattern of
cough and reflex apnea in cats. Journal of physiology and pharmacology : an
official journal of the Polish Physiological Society 60 Suppl 5:99-104.
Potter LE, Paylor JW, Suh JS, Tenorio G, Caliaperumal J, Colbourne F, Baker G, Winship I,
Kerr BJ (2016) Altered excitatory-inhibitory balance within somatosensory
cortex is associated with enhanced plasticity and pain sensitivity in a mouse
model of multiple sclerosis. Journal of neuroinflammation 13:142.
Radwani H, Lopez-Gonzalez MJ, Cattaert D, Roca-Lapirot O, Dobremez E, Bouali-
Benazzouz R, Eiriksdottir E, Langel U, Favereaux A, Errami M, Landry M, Fossat P

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
(2016) Cav1.2 and Cav1.3 L-type calcium channels independently control short-
and long-term sensitization to pain. The Journal of physiology 594:6607-6626.
Ranson RN, Butler PJ, Taylor EW (1995) Studies on nerves of the upper respiratory tract
in the ferret and the mink. Journal of the autonomic nervous system 52:1-16.
Roberts J, Ossipov MH, Porreca F (2009) Glial activation in the rostroventromedial
medulla promotes descending facilitation to mediate inflammatory
hypersensitivity. The European journal of neuroscience 30:229-241.
Romero A, Romero-Alejo E, Vasconcelos N, Puig MM (2013) Glial cell activation in the
spinal cord and dorsal root ganglia induced by surgery in mice. European journal
of pharmacology 702(1-3):126-134.
Schwedt TJ, Larson-Prior L, Coalson RS, Nolan T, Mar S, Ances BM, Benzinger T,
Schlaggar BL (2014) Allodynia and descending pain modulation in migraine: a
resting state functional connectivity analysis. Pain medicine 15:154-165.
Sekizawa S, Chen CY, Bechtold AG, Tabor JM, Bric JM, Pinkerton KE, Joad JP, Bonham AC
(2008) Extended secondhand tobacco smoke exposure induces plasticity in
nucleus tractus solitarius second-order lung afferent neurons in young guinea
pigs. The European journal of neuroscience 28:771-781.
Smith JC, Abdala AP, Borgmann A, Rybak IA, Paton JF (2013) Brainstem respiratory
networks: building blocks and microcircuits. Trends in neurosciences 36:152-
162.
Spaziano G, Luongo L, Guida F, Petrosino S, Matteis M, Palazzo E, Sullo N, de Novellis V,
Di Marzo V, Rossi F, Maione S, D'Agostino B (2015) Exposure to Allergen Causes
Changes in NTS Neural Activities after Intratracheal Capsaicin Application, in
Endocannabinoid Levels and in the Glia Morphology of NTS. BioMed research
international 2015:980983.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Tao W, Chen Q, Zhou W, Wang Y, Wang L, Zhang Z (2014) Persistent inflammation-
induced up-regulation of brain-derived neurotrophic factor (BDNF) promotes
synaptic delivery of alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid
receptor GluA1 subunits in descending pain modulatory circuits. The Journal of
biological chemistry 289:22196-22204.
Trang T, Begg S, Salter MW (2011) Brain-derived neurotrophic factor from microglia: a
molecular substrate for neuropathic pain. Neuron glial biology 7(1):99-108.
Trang T, Beggs S, Salter MW (2012) ATP receptors gate microglia signaling in
neuropathic pain. Experimental neurology 234:354-361.
Ulmann L, Hatcher JP, Hughes JP, Chaumont S, Green PJ, Conquet F, Buell GN, Reeve AJ,
Chessell IP, Rassendren F (2008) Up-regulation of P2X4 receptors in spinal
microglia after peripheral nerve injury mediates BDNF release and neuropathic
pain. Journal of neuroscience 28(44):11263-11268.
Undem BJ, Zaccone E, McGarvey L, Mazzone SB (2015) Neural dysfunction following
respiratory viral infection as a cause of chronic cough hypersensitivity.
Pulmonary pharmacology & therapeutics 33:52-56.
Wager TD, Atlas LY, Lindquist MA, Roy M, Woo CW, Kross E (2013) An fMRI-based
neurologic signature of physical pain. The New England journal of medicine
368:1388-1397.
Wang X, Guo R, Zhao W (2015) Distribution of Fos-Like Immunoreactivity,
Catecholaminergic and Serotoninergic Neurons Activated by the Laryngeal
Chemoreflex in the Medulla Oblongata of Rats. PloS one 10:e0130822.
Whitt JL, Masri R, Pulimood NS, Keller A (2013) Pathological Activity in Mediodorsal
Thalamus of Rats with Spinal Cord Injury Pain. J Neurosci 33(9):3915-3926.
Widdicombe J (2001) Airway receptors. Respiratory physiology 125(1-2):3-15.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Zaccone EJ, Lieu T, Muroi Y, Potenzieri C, Undem BE, Gao P, Han L, Canning BJ, Undem BJ
(2016) Parainfluenza 3-Induced Cough Hypersensitivity in the Guinea Pig
Airways. PloS one 11:e0155526.
Zambreanu L, Wise RG, Brooks JC, Iannetti GD, Tracey I (2005) A role for the brainstem
in central sensitisation in humans. Evidence from functional magnetic resonance
imaging. Pain 114:397-407.
Zhuang X, Chen Y, Zhuang X, Chen T, Xing T, Wang W, Yang X (2016) Contribution of
Pro-inflammatory Cytokine Signaling within Midbrain Periaqueductal Gray to
Pain Sensitivity in Parkinson's Disease via GABAergic Pathway. Frontiers in
neurology 7:104.
Zoccal DB, Furuya WI, Bassi M, Colombari DSA, Colombari E (2014) The Nucleus of the
Solitary Tract and the coordination of respiratory and sympathetic activities.
Frontiers in physiology 5.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure Legends
Figure 1. Brainstem neuroinflammation following respiratory tract viral infection in mice.
Central sensitisation in chronic pain is typically underpinned by glial cell activation and
central inflammation, which contributes to synaptic plasticity and neuronal
hyperresponsiveness. (A) 7 day old neonatal mice infected with an intranasal inoculation
of 5 plaque forming units of pneumovirus show increased immunostaining density for the
glial markers GFAP (astrocytes) and IBA1 (microglia) 3-10 days post-inoculation (DPI) in the
nucleus of the solitary tract. Virus induced increase in the number of cell nuclei expressing
the proliferation marker PCNA is consistent with glial cell expansion at this site (data
represent the mean ± SEM of 5-7 animals per group). (B) Consistent with this, pneumovirus
infected mice have elevated transcripts for the inflammatory mediators Tumor Necrosis
Factor alpha (TNFα) and Interleukin 1β in brainstem homogenates (quantitative PCR, mean
± SEM fold change expression over β-actin, n=3 per group). (C) Representative patch clamp
electrophysiological recording of two neurons in nucleus of the solitary tract in brainstem
slices of two mice, one inoculated intranasally 7 days earlier with vehicle (VEH, lower trace)
and the other inoculated with 103 plaque forming units of influenza Pr8 strain (FLU, upper
trace). Of note is the more depolarised resting membrane potential and induction of
spontaneous action potential discharge after viral infection. Mean data show an average
40mV shift in the resting membrane potential of nucleus of the solitary tract neurons after
infection (mean ± SEM resting membrane potential of 10 neurons per group recorded from
3-4 separate preparations per treatment). *, P<0.05 significantly different to vehicle
inoculated (VEH) controls.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2. A common mechanism of central sensitisation in pain and cough: functional brain
imaging studies in humans. Left panel, Subjects were treated unilaterally on the right lower
eg with a combination of heat and capsaicin to induce hyperalgesia. Subsequent
mechanical stimulation of the area evoked increased pain sensations which were associated
with unilateral increased neural activity in the midbrain nucleus cuneiformis (reproduced
with permission from Zambreanu et al., 2005). Right Panel, Comparable activations in the
midbrain nucleus cuneiformis extending into the periaqueductal grey (PAG) in subjects with
chronic cough hypersensitivity exposed to inhaled capsaicin challenges (data adapted from
Ando et al., 2016). Not shown is an absence of midbrain activity in control subjects,
consistent with the midbrain playing a specific role in the development or maintenance of
hypersensitivity.