-
8/10/2019 Case Report Bursitis
1/19
CASE REPORT
I.I Patient Personal Data
Name : Mr3. . FA
Age : 42 years
Gender : Female
Address : Tegal Gubug
Occupation : House i!e
"eligion : #slam
I.2 Anamnesis
The main complaint :$e!t elbo% lump
History Disease Now :
T&e patient came to t&e emergency room Ar'a%inangun
&ospital complaining %it& $e!t elbo%
lump since 2 mont& ago. (&e told t&at lump at
begingging %as small and by t&e time goes !ly t&e
lump become bigger. (&e !elt pain on t&at lump. (&e
told t&at lump distract daily accti)ities.
T&e lump !ell li*e so!t and slipery. And t&e lump easy
to mo)e.
Past history o !isease :
History o! Heart +isease , -
History o! "enal +isease , -
"amily history o !isease :
History o! &eart disease , -
+isease &istory +M , -
History o! allergy medicines , -
I.# Physical E$amination
General state : /M
0ital (ign :
T+ : 13 5 lying 5 rig&t arm 5 t&e cu!! adult
Nadi : 6menit 5 regular 5 pulse enoug& content 5 t&e
7uality is 7uite
"" : 38.2 6 minute 5 regular
T : 39. degrees using a6illary temperature
-
8/10/2019 Case Report Bursitis
2/19
&ead :
#nspection : anemic con'uncti)a - - 5 sclera 'aundice - - 5
pupil iso*or ; ; 5 lig&t re!le6 ; ;
-
8/10/2019 Case Report Bursitis
3/19
I.% E$amination S&pport
I.' Dia(nosis
Olecranon >ursitis
I.) *o+ernance
O2 3-4 liters minute
#0F+ 29 T
-
8/10/2019 Case Report Bursitis
4/19
CHAPTER II
BURSITIS
+F#N#T#ON
>ursitis is t&e in!lammation or irritation o! t&e
bursa. T&e bursa is a sac !illed %it& lubricating
!luid5 located bet%een tissues suc& as bone5 muscle5
tendons5 and s*in5 t&at decreases rubbing5
!riction5 and irritation.
/A@((
>ursitis is most o!ten caused by repetiti)e5 minor impact on
t&e area5 or !rom a sudden5 more
serious in'ury. Age also plays a role. As tendons age t&ey
are able to tolerate stress less5 are less
elastic5 and are easier to tear.
O)eruse or in'ury to t&e 'oint at %or* or play can also
increase a persons ris* o! bursitis.
6amples o! &ig&-ris* acti)ities include gardening5
ra*ing5 carpentry5 s&o)eling5 painting5
scrubbing5 tennis5 gol!5 s*iing5 t&ro%ing5 and pitc&ing.
#ncorrect posture at %or* or &ome and poor
stretc&ing or conditioning be!ore e6ercise can also lead to
bursitis.
An abnormal or poorly placed bone or 'oint ,suc& as
lengt& di!!erences in your legs or art&ritis
in a 'oint can put added stress on a bursa sac5 causing
bursitis. (tress or in!lammation !rom ot&er
conditions5 suc& as r&eumatoid art&ritis5 gout5
psoriatic art&ritis5 t&yroid disorders5 or unusual
medication reactions may also increase a persons ris*. #n
addition5 an in!ection can occasionally
lead to in!lammation o! a bursa#n!ection t&at causes
bursitis tends to be in bursae t&at are nearer t&e sur!ace
o! t&e s*in5 suc&
as t&ose near t&e elbo%. A cut on t&e s*in is an
opportunity !or t&e bacteria to get in. Most
&ealt&y
people %ould not be a!!ected by opportunistic bacteria trying to
get in t&roug& t&e s*in. Ho%e)er5
people %it& %ea*ened immune systems5 suc& as t&ose
%it& diabetes5 H#0A#+(5 /ancer
,recei)ing c&emot&erapyor radiot&erapy5 as %ell as
people ta*ing steroids5 and &ea)y consumers
o! alco&ol.>ursitis is more common in adults5 especially
in t&ose o)er 4 years o! age.
/$A((#F#/AT#ON
>ursitis is generally classi!ied based on t&e site o!
in)ol)ement. 6amples include:
Housemaids *nee #n!lammation o! bursa on !ront o! t&e
*nee
-
8/10/2019 Case Report Bursitis
5/19
/lergymans *nee - #n!lammation o! bursa on !ront and 'ust belo%
t&e *nee
>a*ers cyst - #n!lammation o! bursa 'ust be&ind t&e
*nee
(tudents elbo% - #n!lammation o! bursa 'ust be&ind t&e
elbo%
ump - #n!lammation o! bursa be&ind t&e &eel
(IM
-
8/10/2019 Case Report Bursitis
6/19
coe6istent %it& supraspinatus tendinitis and partial- or
complete-t&ic*ness tears o! t&e supraspinatus
tendon ,1 o! t&e 4 tendons comprising t&e rotator
cu!!.K1L
Subscapular bursitis
(ubscapular bursae become in!lamed as a result o! abnormal bony
structures or so!t-tissue
c&anges t&at a!!ect t&e mo)ement o! t&e scapula
o)er t&e posterior c&est %all.
Olecranon bursitis
T&e more super!icial o! t&e 2 olecranon bursae commonly
in)ol)ed in bursitis is predisposed
to direct trauma or cumulati)e microtrauma !rom acti)ities
re7uiring !re7uent elbo% motion ,eg5
s%imming5 s*iing5 gymnastics5 and %eig&tli!ting. T&is
type o! bursitis is o!ten recurrent.
1ower/e$tremity 0&rsitis
Bursitis of hip
#sc&iogluteal bursitis is associated %it& sedentary
occupations and is caused by direct stress
on t&e bursa ,&ence t&e nic*name %ea)ers bottom.
-
8/10/2019 Case Report Bursitis
7/19
Anserine ,pes anserinus bursitis is not usually associated
%it& o)eruse but may occur in
patients %it& medial compartmental osteoart&ritis.
/linically5 patients complain o! pain and
tenderness o)er t&e anteromedial *nee t&at is %orse
%it& *nee !le6ion. T&is condition may be
con!used %it& medial meniscal pat&ology.K15 18L
-
8/10/2019 Case Report Bursitis
8/19
Alt&oug& septic bursitis is not diagnosed solely on
t&e basis o! clinical signs5 certain signs
tend to !a)or t&e diagnosis o! septic o)er sterile
in!lammatory bursitis. #n particular5 patients %it&
septic bursitis may &a)e !e)er5 bursal %armt&5
tenderness t&at is more se)ere t&an in nonseptic
bursitis5 and associated peribursal cellulitis. =oint motion is
typically preser)ed in septic bursitis5
%&ereas ot&er types o! bursitis are associated %it&
limited range o! motion.
S&0acromial 0&rsitis
(ubacromial bursitis is !re7uently associated %it&
supraspinatus tendinitis because
in!lammation e6tends !rom one structure to t&e ot&er.
"epetiti)e acti)ities %it& an ele)ated arm
most !re7uently cause in!lammation o! t&e bursae. 6amples o!
t&is include !re7uent pitc&ing o! a
baseball or li!ting luggage o)er&ead. $ess commonly5 a
primary process5 suc& as r&eumatoid
art&ritis5 gout5 or tuberculosis5 may lead to bursitis.
ecause o! t&e &ig&er li*eli&ood o! in!ection5
some p&ysicians encourage aspiration and
analysis o! t&e bursa e)en %&en tenderness and
eryt&ema are minimal.
/&ronic stress !rom repetiti)e !or%ard-leaning positions
%it& pressure on t&e elbo%s is seen
in patients on long-term &emodialysis ,so-called dialysis
elbo%5 in patients %it& c&ronic
obstructi)e lung disease5 in students5 and in t&ose
%&ose occupation in)ol)es laying do%n carpet.
T&e term lunger elbo% &as been suggested to describe
t&is a!!liction.
T&e most common nontraumatic cause o! olecranon bursitis is
gout5 !ollo%ed by pseudogout5
r&eumatoid art&ritis5 and uremia.
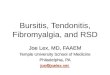
&en in!lamed5 t&e bursa is e)ident as a !luctuant bulge
posterior to t&e olecranon process
,see t&e images belo%.
-
8/10/2019 Case Report Bursitis
9/19
slo%ly o)er %ee*s or mont&s it may be t&e only symptom
present. Tenderness may occur anteriorly
belo% t&e middle o! t&e inguinal ligament and lateral to
t&e !emoral artery. Occasionally5 a palpable
mass or )isible edema may be !ound lateral to t&e !emoral
)essels.
-
8/10/2019 Case Report Bursitis
10/19
T&e super!icial location o! t&e prepatellar bursa allo%s
easy introduction o! microorganisms
and predisposes to septic art&ritis. T&ere!ore5
aspiration o! !luid to rule out in!ection is &ig&ly
recommended i! any clinical suspicion is present.
Inrapatellar 0&rsitis
(uper!icial in!rapatellar bursitis ,clergyman *nee is located
more distally t&an prepatellarbursitis and is o!ten caused by
!re7uent *neeling in an uprig&t position. #t can also be seen
in gout or
syp&ilis. T&e di!!erential diagnosis includes
Osgood-(c&latter disease. T&e deep in!rapatellar bursa
is less !re7uently in!lamed.
/linically5 t&e patient e6&ibits pain %it& !le6ion
and e6tension at t&e e6tremes o! t&e range o!
motion. dema is located on bot& sides o! t&e patellar
tendon and is associated %it& tenderness.
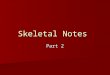
Anserine pes anserin&s3 0&rsitis
T&e anserine bursa separates t&e insertions o! t&e
sartorius5 gracilis5 and semitendinosus
tendons !rom t&e tibial plateau. #t is so named because
t&e edematous bursa5 restrained by t&ese 3tendons5 gi)es
t&e appearance o! a gooses !oot ,pes anserinus. (ee t&e
image belo%
$ocation o! anserine ,pes anserinus bursa on medial *nee.
M/$Qmedial collateral ligament
An abnormal pull on any o! t&e 3 tendons or an abnormal gait
predisposes to repetiti)e
!riction and to bursitis.
-
8/10/2019 Case Report Bursitis
11/19
T&e calcaneal bursa can become in!lamed in patients %it&
&eel spurs or in patients %it& poor-
!itting s&oes ,eg5 &ig& &eels. #n!lammation can
occur secondarily !rom Ac&illes tendinitis5
especially in young at&letes.
lood studies: "outine laboratory blood %or* is generally not
&elp!ul in t&e diagnosis o!
nonin!ectious bursitis. #n cases o! septic bursitis5
&o%e)er5 t&e leu*ocyte count and
eryt&rocyte sedimentation rate ,(" may be mildly to
moderately ele)ated. >lood cultures
may be dra%n i! in!ection o! deep bursae is a concern. ("5
antinuclear antibody ,ANA5
r&eumatoid !actor ,"F5 and anti citric citrullinated peptide
,anti-//ursal !luid s&ould be
dra%n !or monosodium urate crystal determination5 cell count
%it& di!!erential5 Gram stain5
and culture. / count o! -25S$ or &ig&er may be
considered indicati)e o!
in!ection.
Gram stain and culture are per!ormed to identi!y any
pat&ogens. T&e accuracy o! Gram
staining )aries considerably5 %it& sensiti)ities bet%een 1C
and 1C. T&ere!ore5 !luid t&at &as a
&ig& >/ count but is negati)e on Gram staining is
still considered suspicious !or in!ection.
le)ated protein le)el and reduced glucose le)el are associated
%it& in!ection but are not
su!!iciently sensiti)e or speci!ic to be used in isolation.
>ursal !luid culture is t&e conclusi)e test !or
diagnosis. /ulture in li7uid medium &as been s&o%n to be
superior to culture on solid medium.
it& c&ronic or recurrent bursitis5 samples s&ould be
sent !or acid-!ast staining and cultured on
special media !or mycobacteria5Brucella5 and algae.
Fluid s&ould also be e6amined !or crystals. Monosodium urate
crystals are seen in gout
calcium pyrop&osp&ate crystals are seen in pseudogout
c&olesterol crystals are seen in r&eumatoid
c&ylous bursitis and in a )ariety o! c&ronic
e!!usions.
Art&rocentesis s&ould be per!ormed i! 'oint in)ol)ement
is suspected
-
8/10/2019 Case Report Bursitis
12/19
in!lammation. T&ey may also s&o% 'oint e!!usions. #n
c&ronic bursitis5 t&e bursal %alls or
nearby tendons may be calci!ied and radiopa7ue.
>one scanning is not a sensiti)e test !or bursitis5 but it
may be done in cases in %&ic& t&e
diagnosis is unclear to rule out ot&er causes o! pain.
>ecause o! t&e c&aracteristic clinical presentation
o! bursitis5 magnetic resonance imaging,M"# and computed
tomograp&y ,/T are usually unnecessary. M"# can be use!ul
!or
delineating t&e anatomy o! t&e entire 'oint ,including
ad'acent so!t tissues and depicting
bursal or prebursal !luid and associated abscessesK23L i!
needed5 it is a )ery sensiti)e test !or
identi!ication o! bursitis. M"# is also &elp!ul in ruling
out suspected solid tumors and
de!ining pat&ology !or possible surgical e6cision.
@ltrasonograp&y: @ltrasonograp&y is use!ul !or
!urt&er imaging o! t&e bursa %&en t&e
diagnosis is uncertain. For diagnostic aspiration or treatment
in'ections5 ultrasonograp&y
may be per!ormed to elucidate t&e structures and to guide
procedures. T&e accuracy o!ultrasound-guided in'ections &as
increased &o%e)er5 studies o! t&e e!!icacy o!
ultrasound-
guided )ersus blinded in'ections pro)ide contro)ersial
results.K24L #n addition5 ultrasound
studies distinguis& solid !rom cystic masses and are
&elp!ul in detecting >a*er cysts
,popliteal bursitis %&en t&ere are e6tensi)e 'oint
de!ormities. K115 2L >a*er cysts are o!ten
disco)ered incidentally %&en lo%er-e6tremity +oppler studies
are done to rule out deep )ein
t&rombosis.
+#FF"NT#A$ +#AGNO(T#/
/ellulitis Gout and ursitis can be treated in a number o! %ays5
including:
A)oiding acti)ities t&at aggra)ate t&e problem
"esting t&e in'ured area
#cing t&e area t&e day o! t&e in'ury
Ta*ing o)er-t&e-counter anti-in!lammatory medicines
Most patients %it& bursitis are treated conser)ati)ely to
reduce in!lammation. /onser)ati)e
treatment includes rest5 cold and &eat treatments5
ele)ation5 administration o! nonsteroidal anti-
in!lammatory drugs ,N(A#+s5 bursal aspiration5 and intrabursal
steroid in'ections ,%it& or %it&out
local anest&etic agents.K19L
-
8/10/2019 Case Report Bursitis
13/19
ecause o! t&e ris* o! ad&esi)e capsulitis5
s&oulders s&ould not be immobili?ed !or more t&an a
!e% days. A!ter immobili?ation5 patients
s&ould begin graduated range-o!-motion e6ercises.
-
8/10/2019 Case Report Bursitis
14/19
triamcinolone5 betamet&asone5 and de6amet&asone &a)e
been used in t&is setting5 but no single
agent &as been !ound to be demonstrably superior. (teroids
can be mi6ed in t&e same syringe %it&
lidocaine or bupi)acaine.
/orticosteroid in'ections can be per!ormed eit&er in t&e
emergency department ,+ or in an
outpatient setting.K2D5 2LA 1.- to 4-inc& 2-gauge spinal
needle may be used as a probe to determine
t&e points o! ma6imal tenderness in t&e a!!ected bursa.
Typically5 a mi6 o! corticosteroid and local
anest&etic is in'ected into eac& tender site. An
in'ection o! 2 mg or less o! corticosteroid s&ould be
used per lesion5 and no more t&an a total o! 4 mg o!
corticosteroid s&ould be used. K15 145 28L
T&e potential complications o! intrabursal in'ections
include t&e !ollo%ing:
#n!ection
>leeding
Allergy to in'ected agents
$ocal subcutaneous atrop&y ,Met&ylprednisolone is
associated %it& t&e least !re7uent
de)elopment o! local subcutaneous atrop&y.
-
8/10/2019 Case Report Bursitis
15/19
no signi!icant di!!erences bet%een &ig&er ,4 mg and
lo%er ,2 mg doses o! triamcinolone
acetonide. T&ere!ore5 in general5 lo%er doses o! steroids
s&ould be used initially.
6periences %it& platelet-ric& t&erapy ,
-
8/10/2019 Case Report Bursitis
16/19
occasionally may be success!ully treated %it& conser)ati)e
drainage and appropriate
antibiotics.Brucellabursitis is treated %it& e6cision o!
bursae and administration o! tetracycline
%it& or %it&out ri!ampin
(urgical +rainage and 6cision
#n general5 bursitis is not treated surgically. Ho%e)er5
t&ere are some cases in %&ic& surgicalinter)entions
suc& as t&e !ollo%ing are appropriate:
#ncision and drainage
6cision o! c&ronically in!lamed bursae
"emo)al o! underlying bony prominences
As a rule5 surgical inter)ention is reser)ed !or t&e
!ollo%ing situations K3L:
Failure o! needle aspiration to drain t&e bursa
ade7uately
>ursa site inaccessible to repeated needle aspirations
Abscess5 necrosis5 or sinus !ormation
Need !or e6ploration to assess t&e e6tent o! in!ection o!
ad'acent structures
"ecurrent or re!ractory disease a!ter conser)ati)e treatment
(urgical release may be indicated %&en ad&esi)e bursitis
de)elops t&at se)erely limits 'oint
motion. +uring surgery5 t&e ad&ered bursa is remo)ed5
and t&e contiguous tissues are released. K385 45
25 41L
#n t&e upper e6tremity5 subscapular bursitis can be caused
by bony e6ostoses5 and surgery may
be needed to reduce t&ese structures. #n addition5 t&e
association o! subacromial bursitis %it& rotator
cu!! impingement and tears is &ig&5 and surgical repair
o! t&e tear may be indicated.
#n t&e lo%er e6tremity5 >a*ers cysts ,popliteal bursitis
are o!ten remo)ed surgically. >e!ore
open e6cision5 art&roscopy s&ould be per!ormed to
e)aluate !or intra-articular conditions. Most
cysts are approac&ed posteromedially t&roug& a
&oc*ey-stic* incision.
-
8/10/2019 Case Report Bursitis
17/19
An in!lamed s%ollen bursa may get in!ected secondarily. T&is
is particularly common a!ter
attempts at aspiration o! t&e bursa %it& a syringe under
unclean conditions. /&ances o! in!ection are
also &ig&er in diabetic patients.
-
8/10/2019 Case Report Bursitis
18/19
-
8/10/2019 Case Report Bursitis
19/19
SOURCES
http://www.nlm.nih.gov/medlineplus/ency/article/00041.htm
http://www.!etterhealth.vic.gov.au/!hcv"/!hcarticles.ns#/pages/$ursitis
http://emedicine.medscape.com/article/"14%%&&'medication
http://www.we!md.com/pain'management/arthritis'!ursitis
http://www.medicalnewstoday.com/articles/1%"1"0.php
http://www.we!md.com/pain'management/arthritis'!ursitis
&ttp:%%%.do*terbeda&&erryyud&a.com
http://www.nlm.nih.gov/medlineplus/ency/article/000419.htmhttp://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Bursitishttp://emedicine.medscape.com/article/2145588-medicationhttp://www.webmd.com/pain-management/arthritis-bursitishttp://www.medicalnewstoday.com/articles/152120.phphttp://www.webmd.com/pain-management/arthritis-bursitishttp://www.dokterbedahherryyudha.com/2012/02/nephrolithiasis.htmlhttp://www.nlm.nih.gov/medlineplus/ency/article/000419.htmhttp://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Bursitishttp://emedicine.medscape.com/article/2145588-medicationhttp://www.webmd.com/pain-management/arthritis-bursitishttp://www.medicalnewstoday.com/articles/152120.phphttp://www.webmd.com/pain-management/arthritis-bursitishttp://www.dokterbedahherryyudha.com/2012/02/nephrolithiasis.html