Embed Size (px)
Citation preview

Causes of Preterm Birth:
“The Preterm Parturition Syndrome”
Roberto Romero,M.D.Chief Perinatology Research
BranchDivision of Intramural
ResearchNICHD/NIH/DHHS

Conflict of Interest Statement
• Official capacity (NICHD/NIH/DHHS)
• Division of Intramural Research
• Trial conducted by the Extramural
Program of NICHD/NIH (17P-CT-002)
• Independent of PRB/NICHD
• No financial conflict of interest
with sponsor

The Lancet Editorial 2006;368:339

Institute of Medicine of the National Academies, 2006
Richard E. Behrman, Adrienne Stith Butler, Editors
Institute of Medicine Report
Preterm Birth: Causes, Consequences, and Prevention

Magnitude of the Problem
•Definition (< 37 weeks)
•2004: more than 500,000 neonates were born preterm
•Frequency: 12.5 %

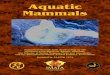
Preterm Births as a Percentage of Live Births in the United States, 1990 to 2004
Institute of Medicine. PRETERM BIRTH: CAUSES, CONSEQUENCES, AND PREVENTION. 2006.
0
2
4
6
8
10
12
1990 1993 1995 1997 1999 2000 2003 2004
10.6 11 1111.4
11.8 11.612.3 12.5

Preterm Births as a Percent of Live Births, by Race and Ethnicity, 1992 to 2003
CDC 2004.
Hispanic
White, non-hispanic
Black
American Indian
Asian orPacific Islander
5
10
15
20
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003

Frequency of Preterm Birth by Ethnic Group
Source: CDC 2004 Births: Preliminary Data for 2003 http://www.cdc.gov/nchs/data/nvsr/nvsr53/nvsr_09.pdf (accessed August 30, 2005)
Non-Hispanic African-American 17.8%
American Indians/Native Alaskans 13.5%
Hispanics 11.9%
Whites 11.5%
Asian and Pacific Islanders 10.5%

Cost of Preterm Birth
• Medical care services:
– 16.9 billion ( $ 33,200 per preterm infant) -
2/3 total cost
• Maternal delivery cost:
– 1.9 billion ( $ 3,800 per preterm infant)
• Special education services:
– 1.1 billion ( $ 2,200 per preterm infant)
• Lost household and labor market productivity:
– 5.7 billion ( $11,200 per preterm infant)
Source: Institute of Medicine of the National Academies 2006, page 47

The Annual Societal Economic Burden
associated with Preterm Birth in the United
States
In excess of $26.2 billion in 2005

© PJS
The Prognosis of Preterm Neonates is a Function of Gestational Age at Birth

Survival by gestational age among live-born resuscitated infants
Mercer BM Obstet Gynecol 2003;101:178 –93.
Results of a community-based evaluation of 8523 deliveries, 1997–1998, Shelby County, Tennessee

Magnitude of the Problem
• The infant mortality rate for very preterm infants (delivered < 32 weeks of gestation) was 186.4, nearly 75 times the rate for infants born at term (2.5) (37–41 weeks of gestation)
• 20% all infants born <32 weeks do not survive the first year of life
Mathews TJ. et al. National Vital Statistics Reports 2004;53:1-32

Acute morbidity by gestational age among surviving infants
Mercer BM Obstet Gynecol 2003;101:178 –93.
Results of a community-based evaluation of 8523 deliveries, 1997–1998, Shelby County, Tennessee

IOM Report – July 2006
• “Babies born before 32 weeks have the greatest
risk for death and poor health outcomes,
however, infants born between 32 and 36 weeks,
which make up the greatest number of preterm
births, are still at higher risk for health
and developmental problems compared to those
infants born full term
IOM Report page 72

Frequency of preterm birth by gestational age
(1995-2000)
• < 28 weeks : 0.82 %
• < 32 weeks: 2.2 %
• 33-36 weeks: 8.9 %
• < 37 weeks: 11.2
IOM Report-July 2006- page 72/2006Alexander GR et al 2006 (under review)

Complications of “Late Preterm or Near Term
Infants”
• Cold Stress
• Hypoglycemia
• RDS
• Jaundice
• Sepsis
IOM Report-July 2006- page 72/2006

Clinical CircumstancesAssociated with Preterm
Birth
• Spontaneous preterm labor with intact membranes
• Preterm PROM
• Indicated preterm delivery– Maternal (e.g. pre-eclampsia)
– Fetal (e.g. SGA/fetal compromise)

Is preterm labor simply “labor before
its time” ?

Term Labor Preterm Labor
© VR RR MM

Common Uterine Features of Term and Preterm Labor
•Increased myometrial
contractility
•Cervical ripening (dilatation
and effacement)
•Decidual/membrane activationRomero R, Mazor M, Munoz H et al: The Preterm Labor Syndrome. Ann NY Acad Sci 1994;734:414

Common Pathway of Parturition
•Anatomic, physiologic,
biochemical, endocrinologic,
immunologic, and clinical events
in the mother and/or fetus in
both term and preterm labor
Romero R, Mazor M, Munoz H et al: The Preterm Labor Syndrome. Ann NY Acad Sci 1994;734:414

The “phenotypes” of spontaneous preterm
parturition

Synchronous and Asynchronous Activation of
Labor
Cervical RipeningCervical Ripening
UterineContractility
UterineContractility
Membrane-Decidual
Activation
Membrane-Decidual
Activation
PretermPROM
PretermPROM
PretermContractions
PretermContractions
CervicalInsufficiency
CervicalInsufficiency
© VR RR MM

Component Test Treatment
Myometrium Uterine Monitor
Tocolysis
Ultrasound Cerclage Cervix
Approaches for the Prevention of Preterm
Birth
Fetal Fibronectin Antibiotics Membrane/Decidua
© VR RR MM

Common Terminal Pathway Common Terminal Pathway
Normal TermLabor
Normal TermLabor
PhysiologicActivation
PhysiologicActivation
PretermLabor
PretermLabor
PathologicActivation PathologicActivation
© VR RR MM

What causes pathologic activation of the
pathway ?

Placental Pathology in Prematurity
Arias et al. Obstet Gynecol 1997;69:285.
Acute Chorioam nionitis
42%
Chronic villitis0.8%
Villous edem a1.7%
Norm al placenta13.3%
M ixed (inflam m ation+ vascular)
20%
VascularLesions20%
© PJS

• Multiple etiologies
• Chronicity
• Fetal diseases
• Clinical manifestations are adaptive
• Symptomatic treatment is ineffective
• Genetic/environmental factors
““Great Obstetrical Great Obstetrical Syndromes”Syndromes”
““Great Obstetrical Great Obstetrical Syndromes”Syndromes”
© VR RR MM Romero R J Prenat Neonat Med 1996;1:8-11

The Preterm Parturition Syndrome
UterineUterineOverdistensioOverdistensio
nn
VascularVascular
InfectioInfectionn
Cervical Cervical DiseaseDisease
HormonalHormonal
ImmunologicalImmunological
© VR RR MM
UnknownUnknown

The Preterm Parturition Syndrome
UterineUterineOverdistensioOverdistensio
nn
VascularVascular
InfectioInfectionn
Cervical Cervical DiseaseDisease
HormonalHormonal
ImmunologicalImmunological
© VR RR MM
UnknownUnknown

• Frequent: 25 % (at
presentation)
• Sub-clinical
• Fetal disease
• FIRS
• Host defense
Intraamniotic Infection
Intraamniotic Infection

• 12% of preterm labor
• 20% of preterm PROM
Sub-clinical Sub-clinical
Clinical Chorioamnionitis

Severe neonatalmorbidity
Severe neonatalmorbidity
Impending pretermdelivery
Impending pretermdelivery
Fetal multisysteminvolvement
Fetal multisysteminvolvement
FIRS FIRS
© VR RR MM

Fetal Inflammatory Response Fetal Inflammatory Response SyndromeSyndrome
Fetal Inflammatory Response Fetal Inflammatory Response SyndromeSyndrome
• Hematologic Abnormalities
• Endocrine System
• Cardiac Dysfunction
• Pulmonary Injury
• Renal Dysfunction
• Brain Injury (PVL)

How common is sub-
clinical intra-
amniotic infection in
asymptomatic
midtrimester pregnancy

• 2461 midtrimester amniocenteses
• 9 patients with U. urealyticum
(0.4%)
• 8 continuing pregnancies• 6 spont. abortions within 4
weeks
• 2 preterm labor
• 8 histologic chorioamnionitis
Infection in mid-trimester
Infection in mid-trimester
Gray DJ. Prenat Diagn 1992;12:111

Prevention of Preterm Labor/Delivery
• Important and desirable goal
• Only proven beneficial strategy is eradication of asymptomatic bacteriuria
• Limited attributable risk
• Patients with previous preterm birth are at increased risk for recurrence
• Potential beneficial effect of progesterone administration– 17OHP-C and vaginal progesterone

The Preterm Parturition Syndrome
UterineUterineOverdistensioOverdistensio
nn
VascularVascular
InfectioInfectionn
Cervical Cervical DiseaseDisease
HormonalHormonal
ImmunologicalImmunological
© VR RR MM
UnknownUnknown

“Progesterone deficient
state” has been
proposed to be a
Mechanism of Disease
in Preterm Labor

http://www.siumed.edu/~dking2/erg/enguidehttp://medstat.med.utah.edu/
Corpus Luteum

AJOG 1973;115:759-65
Prostaglandins 1973;4:421-9
AJOG 1973;115:759-65

What is the Effect of Luteectomy
on Human Pregnancy?
• 64 pregnant women (< 5 weeks)
• Desired tubal ligation
• IRB approval
• Allocated to:– Tubal ligation (control group)– Tubal ligation + luteectomy– Tubal ligation + luteectomy +
progesterone
American Journal of Obstetrics and Gynecology: 1972Prostaglandins: 1973
Ciba Symposium 47: 1977

Csapo AI The Fetus and Birth. Ciba Foundation Symposium 47; 1977.
Pregnancy outcome after lutectomy
Only tuballigation24+2
No AbDC)
5
10
15
0
Days after Lutectomy8
20
25
120 4 16
Incipient Ab(curettage)
)
22+1
19+1
)
Ab
LuteectomyAmenorrheaDays32+2
No AbDC
Progesterone
Plasma Progesterone (ng/ml)

Arpard Csapo
• Progesterone is “indispensable” for normal pregnancy
• Progesterone withdrawal is a prerequisite of normal pregnancy termination

Progesterone in Pregnancy
Maintenance
• Myometrial quiescence
• Down-regulate gap
junction formation
• Inhibit cervical ripening

A progesterone
withdrawal “prepares”
the uterus
for the action of
uterotonic agents

Administration of anti-progestins
(RU-486 or onapristone) can induce
abortion and cervical ripening
Evidence that suspension of progesterone action is
important in human parturition
Kovacs L et al. Contraception 1984; 29: 399Crowley WF. N EJM 1986; 18: 1607
Chwalisz K. 1994 Human Reproduction 1994;9:131Bygdeman et al. Human Reproduction 1994;9:120

40
30
20
10
0No labor(n = 20)
Labor(n = 20)
Progesterone/estradiol ratio
15
10
5
0No labor(n = 20)
Labor(n = 20)
Progesterone/estriol ratio
Romero R et al AJOG 1988;150:650-60

• Key hormone for pregnancy maintenance
• “Progesterone withdrawal”:
– Concentration
– Receptor (A and B)Mesiano S, Chan E, Fitter JT, Kwek K, Yeo G,
and Smith R. J Clin Endocrinol Metab 2002; 87:2924
– Functional (NF-kB)
Allport VC, Pieber D, Slater DM, Newton
R, White JO and Bennett PR. Mol Human Reprod 2001; 7:581-6
Progesterone

The clinical trials and meta-
analysis of progesterone will be analyzed by
FDA staff and the sponsor

Interventions for the prevention
of preterm birth
•Efficacy
•Safety

Criteria for Efficacy
•Prevention of preterm birth
–37 weeks
–35 weeks
–32 weeks
•Prolongation of pregnancy
•Neonatal morbidity and mortality

Safety
•Fetal
•Neonatal
•Infant
•Maternal

ProgesteroneProgesteroneDeficiency StateDeficiency StateProgesteroneProgesterone
Deficiency StateDeficiency State
Common Terminal Common Terminal PathwayPathway
Common Terminal Common Terminal PathwayPathway
Preterm LaborPreterm LaborPreterm LaborPreterm Labor

Obstet Gynecol 2003;102:1115-6

Obstet Gynecol 2003;102:1115-6


Quiescence
Weeks 0 36 40
Quiescence
Weeks 0 24 4028
The preparatory stage of labor
The preparatory stage of labor

ProgesteroneProgesteroneDeficiency StateDeficiency StateProgesteroneProgesterone
Deficiency StateDeficiency State
Common Terminal Common Terminal PathwayPathway
Common Terminal Common Terminal PathwayPathway
Preterm LaborPreterm LaborPreterm LaborPreterm Labor
Uterine Uterine Pathologic State Pathologic State
(infection, (infection, vascular, vascular, uterine)uterine)
Uterine Uterine Pathologic State Pathologic State
(infection, (infection, vascular, vascular, uterine)uterine)
Common Terminal Common Terminal PathwayPathway
Common Terminal Common Terminal PathwayPathway
Preterm LaborPreterm LaborPreterm LaborPreterm Labor