Embed Size (px)
Citation preview

Preterm LaborPreterm Labor
Prof. Ryszard CzajkaProf. Ryszard Czajka
Chair and Department of Obstetrics and Chair and Department of Obstetrics and PerinatologyPerinatology

PRETERM BIRTH PRETERM BIRTH PTBPTB
PRETERM LABOR PRETERM LABOR PTLPTL
PRETERM DELIVERY PRETERM DELIVERY PTDPTD
PREMATURITYPREMATURITY
LOW-BIRTH WEIGHTLOW-BIRTH WEIGHT
PREMATURE NEWBORNPREMATURE NEWBORN
DYSTROPHIC NEWBORNDYSTROPHIC NEWBORN

Preterm Labor is defined as the presence of regular uterine contractions, occuring with a frequency of 10 minutes or less between 23 and 37 weeks gestation, with each contraction lasting at least 30 seconds

This uterine activity is accompanied by cervical effacement, cervical dilation and/or descent of the fetus into pelvis

However, variations of this definition are commonly used, so it is often difficult to know when a patient is really in PTL. This present a problem because treatment appears to be more effective when initiated early in the course of PTL; waiting for cervical changes to occur to establish a definitive diagnosis may limit successful therapy.

Symptoms and Signs of Preterm LaborSymptoms and Signs of Preterm Labor
Menstrual – like cramps Low, dull backache Abdominal pressure Abdominal cramping (with or without
diarrhoea) Increase or change in vaginal discharge
(mucus, watery, light bloody, discharge) Uterine contractions, often painless

Many preterm births are the result of Many preterm births are the result of deliberate intervention for a variety of deliberate intervention for a variety of pregnancy complication and hence pregnancy complication and hence have unavoidable perinatal have unavoidable perinatal complications. A major cause of complications. A major cause of preterm birth, however is PTL.preterm birth, however is PTL.

Because PTB is the most common cause Because PTB is the most common cause of perinatal morbidity and mortality, of perinatal morbidity and mortality, its prevention and treatment are major its prevention and treatment are major concerns in obstetric careconcerns in obstetric care

The consequences of PTL and PTB occur with increasing severity and frequency the earlier the gestational age of the newborn

Besides perinatal death in the very young fetus, common complications of PTL include – Respiratory Distress Syndrome (RDS,
hyaline membrane disease)
– Intraventricular hemorrhage
– Necrotizing enterocolitis
– Sepsis
– Seizures

Long-term morbidity associated with PTL and delivery includes– Bronchopulmonary dysplasia
– Developmental abnormalities

The significant impact of PTB is best summarized by this fact:The 10% of the babies born prematurely account for more than 50% of all perinatal morbidity and mortality in the United States.

In the consideration of the consequences of PTD, it is important to seperate the concepts of low-birth weight and prematurity

Prematuriy reflects gestational age, whereas low-birth weight is based on the single parameter of weight, usually 2500g or less

For example, a growth- restricted fetus (IUGR) of a hypertensive patient may weight well under 2500g at 40 weeks gestation

Such an infant is a low-birth weight infant but not preterm and will suffer the consequences associated with low-birth weight and maternal hypertension, but not of premature birth

Likewise, an infant of a diabetic mother may by delivered before term, weigh in excess of 2500g, and still have the significant perinatal morbidities of PTB.

Factors Associated with Preterm LaborFactors Associated with Preterm Labor
Dehydration Premature rupture of membranes
(PROM) Incompetent cervix
– Primary
– Secondary to surgery (e.g. cone biopsy of cervix)

Factors Associated with Preterm LaborFactors Associated with Preterm Labor
Infections
– Urinary
– Cervical
– Bacterial vaginosis
– Intra amniotic
Factors Associated with Preterm LaborFactors Associated with Preterm Labor
Placental abnormalitiesAbruptio placentae Placenta previa
Maternal smoking (strong implications)
Substance abuse Iatrogenic: induction of labor

Factors Associated with Preterm LaborFactors Associated with Preterm Labor
Excessive uterine enlargement: Hydramnios Multiple gestation Uterine distortion
– Leyomyomas– Septate uterus, uterine didelphis
and other anomalies

Risk factors of premature laborRisk factors of premature labor
1. Medical factors
2. Social factors
3. Demographic factors
4. Environmental factors

Risk factors of premature laborRisk factors of premature labor
Medical factors- medical history (preterm labor, spontaneous and
induced abortion, previous steelbirths)- medical factors variable arising during pregnancy a) uterine bleeding b) multiple pregnancy c) placenta previae d) preeclampsia e) urinal infections d) vaginal infections

Risk factors of premature laborRisk factors of premature labor - maternal diseases a) diabetes mellitus b) epilepsia c) hypertension d) EPH – gesthosis (PIH) e) Urinary disease f) Uterine malformation g) Myoma uterine h) Incompetence cervix i) Fetal malformation j) Pathology of placenta k) Infections

Risk factors of premature laborRisk factors of premature labor Social factors
– low socioeconomic status smoking Demographic factors -Young (below 18) and old (over 35) maternal age -Multiparity Unmarried status Environmental factors - physical factors (radiation, jonization, termical factors,
magnetism), vibration, noisy, chemical factors

Risk factors of premature laborRisk factors of premature labor Psychogenic factorsPsychogenic factors- - family or own diseases- death of family member- stressful of life events- stressful with husband and parents- stressful with unmarried status- bad of residence- work/fatigue- anxiety- past of obstetrical history- arising symptoms of premature labor - insufficient of obstetrical care
Prevention of Preterm DeliveryPrevention of Preterm Delivery
In Europe premature birth remains primary cause of neonatal morbidity and mortality.
Early identification of high risk pregnancies through various screening methods as well as specific markers for preterm delivery is crucial.

Prevention of Preterm DeliveryPrevention of Preterm Delivery Ascending infections play an important role in the pathogenesis of Ascending infections play an important role in the pathogenesis of
preterm delivery, and thus have to receive adequate diagnostic attention. preterm delivery, and thus have to receive adequate diagnostic attention. In the scope “step-by-step concept” of markers, the vaginal pH is most In the scope “step-by-step concept” of markers, the vaginal pH is most
easily measured. Vaginal pH is an important indicator of abnormalities easily measured. Vaginal pH is an important indicator of abnormalities of vaginal flora and predisposition to ascending infections. of vaginal flora and predisposition to ascending infections.
Trichomonas and bacterial vaginosis can be detected in native sample; Trichomonas and bacterial vaginosis can be detected in native sample; IIf other infections are suspected, vaginal bacteriology is to be carried out.f other infections are suspected, vaginal bacteriology is to be carried out. According to recent publications, specific pathogens are closely are According to recent publications, specific pathogens are closely are
closely associated with preterm delivery closely associated with preterm delivery – (syphilis, gonorrhea, bacterial vaginosis), (syphilis, gonorrhea, bacterial vaginosis), – whereas correlation of preterm delivery with other pathogens (beta-whereas correlation of preterm delivery with other pathogens (beta-
Streptococcus, Ureaplasma, Mycoplasma, Chlamydia, Trichomonas) Streptococcus, Ureaplasma, Mycoplasma, Chlamydia, Trichomonas) is still disputed.is still disputed.

Prevention of Preterm DeliveryPrevention of Preterm Delivery
Fibronectin is also a predictive factor for Fibronectin is also a predictive factor for imminent preterm delivery. imminent preterm delivery.
EElevated CRP values may indicate levated CRP values may indicate beginning infectionbeginning infection
Prevention of Preterm DeliveryPrevention of Preterm Delivery Pathogenesis of Preterm Delivery Vaginal pH Vaginal Wet Smear Cultures - beta Streptococcus - Ureaplasma urealyticum - Mycoplasma hominis - Chlamydia Trachomatis - Trichomonas vaginalis - Gardnella vaginalis Cervical – Vaginal Oncofetal Fibronectin C-Reactive Protein

Evaluation of a patient in Evaluation of a patient in suspected preterm laborsuspected preterm labor
Once a patient describes symptoms ans signs suggestive of PTL, evaluation should be prompt
External elctronic fetal monitoring Abdominal palpation by experienced
personnel The status of the cervix should be
determined by visualization with speculum or gentle digital examination

Evaluation of a patient in Evaluation of a patient in suspected preterm laborsuspected preterm labor
Serial digital examinationSerial digital examination Ultrasound examinationUltrasound examination
– Gestational ageGestational age
– AFIAFI
– Placental locationPlacental location
– Cervix dilationCervix dilation

Evaluation of a patient in Evaluation of a patient in suspected preterm laborsuspected preterm labor
Urinalysis Investigation of clinical or subclinical
infection:
– White blood cells
– CRP
– Bacteriological culture
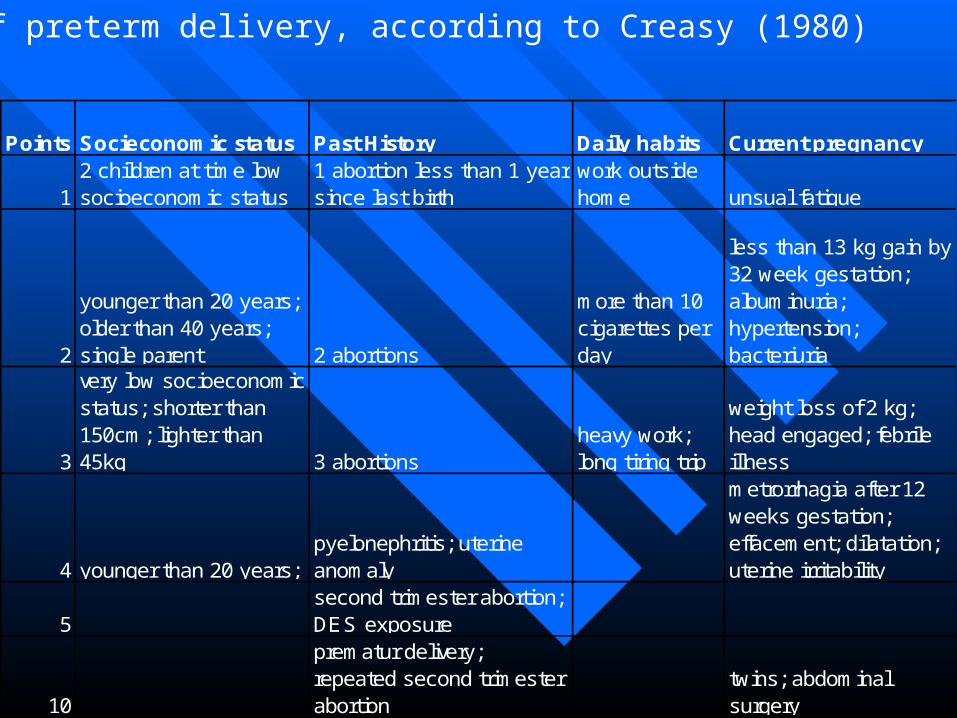
Points Socieconomic status Past History Daily habits Current pregnancy
12 children at time low socioeconomic status
1 abortion less than 1 year since last birth
work outside home unsual fatigue
2
younger than 20 years; older than 40 years; single parent 2 abortions
more than 10 cigarettes per day
less than 13 kg gain by 32 week gestation; albuminuria; hypertension; bacteriuria
3
very low socioeconomic status; shorter than 150cm; lighter than 45kg 3 abortions
heavy work; long tiring trip
weight loss of 2 kg; head engaged; febrile illness
4 younger than 20 years; pyelonephritis; uterine anomaly
metrorrhagia after 12 weeks gestation; effacement; dilatation; uterine irritability
5second trimester abortion; DES exposure
10
prematur delivery; repeated second trimester abortion
twins; abdominal surgery
Risk of preterm delivery, according to Creasy (1980)

Points Background Reproductive history Way of life Clinical signs
1
2 or more children without household help; low socioeconomic level
1 curettage; short interval between previous pregnancies (1 year between delivery and 2nd pregnancy) work outside home unusual fatigue
2
not married; aged less than 20 years; aged more than 40 years 2 curettages
more than 3 flights of stairs without elevator
less than 5 kg weight gain at 32 week; albuminuria; hypertension
3
very low socioeconomic level (poverty); less 1,50m; less than 45kg
3 or more curettages; cylindrical uterus
long daily commuting; unusual exertions; tiring work
bleeding during 1st trimester; thinned lower segment of uterus
4 less than 18 years pyelonephritis extensive travel
bleeding during 2nd trimester; shortened cervix; opened inner cervical os; uterine contractions
Preterm birth risk score (According to Papiernik)

Agents Used in Treating Preterm LaborAgents Used in Treating Preterm Labor
- adrenergic agents (phenoterol) Magnesium sulfate Calcium channels blockers
(werapamil) Oxytocin receptor blockers
(tractocile)

Administration of Magnesium Administration of Magnesium Sulfate for Preterm LaborSulfate for Preterm Labor
1. 6g MgSO4 are mixed in 100-150 ml of D5W and infused over 15-20 minutes as a loading dose.
2. 40g MgSO4 are mixed in 1000 ml of D5W, providing an MgSO4 concentration of 1 g MgSO4 in 25 ml of solution
3. Using a piggyback infusion via an infusion pump, the physician usually begins infusion at 2g/hr (50ml/hr) and increases it in 0,5 g/hr increments as needed.