Embed Size (px)
Citation preview
Physiological amp Biochemical Process regulating Parturition
Physiological process in human pregnancy that result in initiation of parturition amp onset of labor poorly defined
Retreat from pregnancy maintenance amp uterotonin induction of parturition hypotheses
Mature human fetus source of initial signal for commencement parturitional process
One or more uterotonins initiation of human parturition ( myometrial R elevation)
Anatomical amp physiological consideration of myometrium Characteristics ndash advantage in efficiency of uterineCharacteristics ndash advantage in efficiency of uterine contractions amp delivery of fetuscontractions amp delivery of fetus ① ① degree of shortening of smooth m cells withdegree of shortening of smooth m cells with contractioncontraction magnitude greater than in striated m cells magnitude greater than in striated m cells ② ② forces can be exerted in smooth m cells inforces can be exerted in smooth m cells in any directionany direction ③ ③ not organized in same manner as skeletal mnot organized in same manner as skeletal m - thick amp thin filaments in long random bundles- thick amp thin filaments in long random bundles rarr rarr greater shortening amp force-generating capacitygreater shortening amp force-generating capacity ④ ④ multidirectional force generationmultidirectional force generation
Regulation of myometrial contraction amp Relaxation
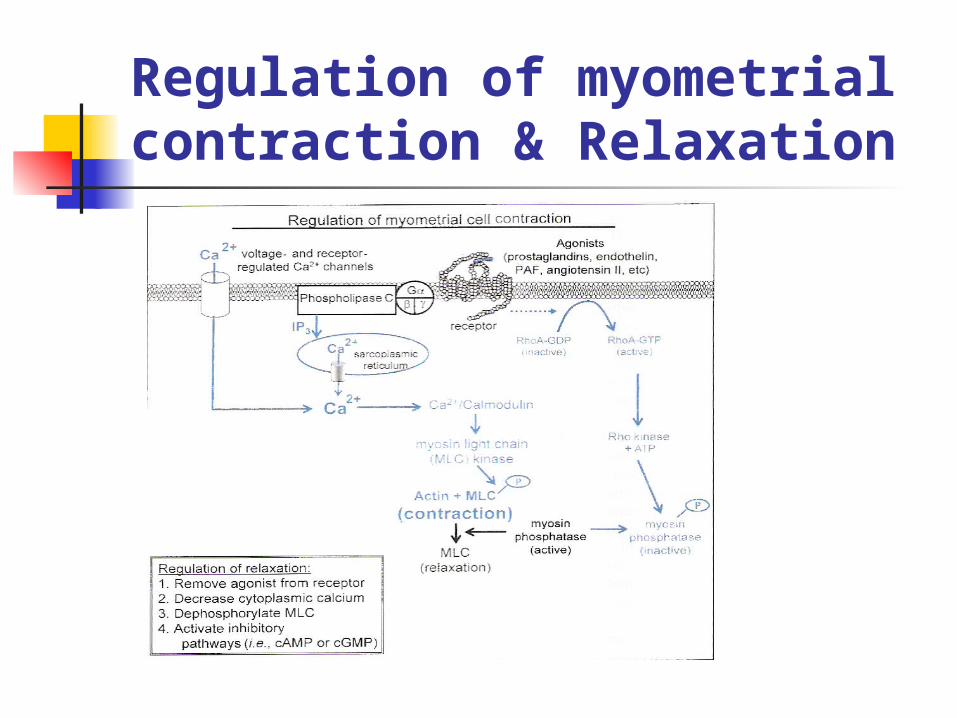
Regulation of myometrial contraction amp Relaxation Interaction of myosin amp actin activation of adenosine triphosp
hatase ATP hydrolysis force generation (by enzymatic phosphorylation of MLC)
Ca bind to calmodulin activate myosin light chain kinase increase in intracellular Ca2+ (transient)
Contraction prolonged inhibition of myosin phosphatase activity by Rho kinase
Uterine activity regulation of contraction ndashassociated protein (CAP) include channels associaeted with smooth m excitation amp contraction gap junction component uterotonic stimulatory or inhibitory R
Cellular signals transferred between cells through intercellular junctional channels
Communication is extabilished between myometrial cells by gap junctions that facilitate passage of electrical or ionic coupling current as well as metabolite coupling
Consist of two protein rdquohemi-channels ldquo termed connexons hexameric assemblage of type of protein called connexin
Conduit for exchange of small molecule Gap junctions optimal No electrical synchrony in myometriu
m coordination of contraction ( greater force during labor)
1] Myometrial Gap junctions
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Anatomical amp physiological consideration of myometrium Characteristics ndash advantage in efficiency of uterineCharacteristics ndash advantage in efficiency of uterine contractions amp delivery of fetuscontractions amp delivery of fetus ① ① degree of shortening of smooth m cells withdegree of shortening of smooth m cells with contractioncontraction magnitude greater than in striated m cells magnitude greater than in striated m cells ② ② forces can be exerted in smooth m cells inforces can be exerted in smooth m cells in any directionany direction ③ ③ not organized in same manner as skeletal mnot organized in same manner as skeletal m - thick amp thin filaments in long random bundles- thick amp thin filaments in long random bundles rarr rarr greater shortening amp force-generating capacitygreater shortening amp force-generating capacity ④ ④ multidirectional force generationmultidirectional force generation
Regulation of myometrial contraction amp Relaxation
Regulation of myometrial contraction amp Relaxation Interaction of myosin amp actin activation of adenosine triphosp
hatase ATP hydrolysis force generation (by enzymatic phosphorylation of MLC)
Ca bind to calmodulin activate myosin light chain kinase increase in intracellular Ca2+ (transient)
Contraction prolonged inhibition of myosin phosphatase activity by Rho kinase
Uterine activity regulation of contraction ndashassociated protein (CAP) include channels associaeted with smooth m excitation amp contraction gap junction component uterotonic stimulatory or inhibitory R
Cellular signals transferred between cells through intercellular junctional channels
Communication is extabilished between myometrial cells by gap junctions that facilitate passage of electrical or ionic coupling current as well as metabolite coupling
Consist of two protein rdquohemi-channels ldquo termed connexons hexameric assemblage of type of protein called connexin
Conduit for exchange of small molecule Gap junctions optimal No electrical synchrony in myometriu
m coordination of contraction ( greater force during labor)
1] Myometrial Gap junctions
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Regulation of myometrial contraction amp Relaxation
Regulation of myometrial contraction amp Relaxation Interaction of myosin amp actin activation of adenosine triphosp
hatase ATP hydrolysis force generation (by enzymatic phosphorylation of MLC)
Ca bind to calmodulin activate myosin light chain kinase increase in intracellular Ca2+ (transient)
Contraction prolonged inhibition of myosin phosphatase activity by Rho kinase
Uterine activity regulation of contraction ndashassociated protein (CAP) include channels associaeted with smooth m excitation amp contraction gap junction component uterotonic stimulatory or inhibitory R
Cellular signals transferred between cells through intercellular junctional channels
Communication is extabilished between myometrial cells by gap junctions that facilitate passage of electrical or ionic coupling current as well as metabolite coupling
Consist of two protein rdquohemi-channels ldquo termed connexons hexameric assemblage of type of protein called connexin
Conduit for exchange of small molecule Gap junctions optimal No electrical synchrony in myometriu
m coordination of contraction ( greater force during labor)
1] Myometrial Gap junctions
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Regulation of myometrial contraction amp Relaxation Interaction of myosin amp actin activation of adenosine triphosp
hatase ATP hydrolysis force generation (by enzymatic phosphorylation of MLC)
Ca bind to calmodulin activate myosin light chain kinase increase in intracellular Ca2+ (transient)
Contraction prolonged inhibition of myosin phosphatase activity by Rho kinase
Uterine activity regulation of contraction ndashassociated protein (CAP) include channels associaeted with smooth m excitation amp contraction gap junction component uterotonic stimulatory or inhibitory R
Cellular signals transferred between cells through intercellular junctional channels
Communication is extabilished between myometrial cells by gap junctions that facilitate passage of electrical or ionic coupling current as well as metabolite coupling
Consist of two protein rdquohemi-channels ldquo termed connexons hexameric assemblage of type of protein called connexin
Conduit for exchange of small molecule Gap junctions optimal No electrical synchrony in myometriu
m coordination of contraction ( greater force during labor)
1] Myometrial Gap junctions
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Cellular signals transferred between cells through intercellular junctional channels
Communication is extabilished between myometrial cells by gap junctions that facilitate passage of electrical or ionic coupling current as well as metabolite coupling
Consist of two protein rdquohemi-channels ldquo termed connexons hexameric assemblage of type of protein called connexin
Conduit for exchange of small molecule Gap junctions optimal No electrical synchrony in myometriu
m coordination of contraction ( greater force during labor)
1] Myometrial Gap junctions
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Estrogen amp progesteron R variety of cell surface R that can directly regulate contractile state of cell
Most of heptahelical R in myometrium Activation of adenylycyclase G-protein-medicated activation of phospholipase C [Ca2+]) uarramp myometial cell contraction uarr
In high concentration from maternal blood (endocrine) contiguous tissues or adjacent cells (paracrine) or direct synthesis in myometrial smooth m cell (autocrine) [Fig 6-16]
2] Cell surface R as regulator of myometrium
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
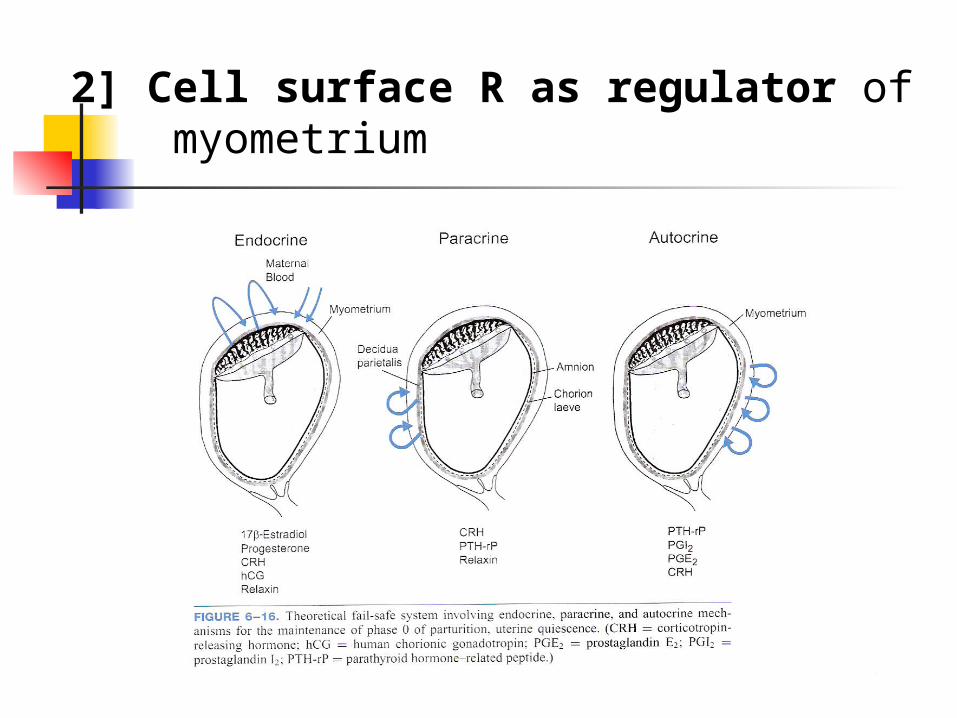
2] Cell surface R as regulator of myometrium
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Myometrial response to H can change during course of pregnancy
Imposition of quiescence (activation of adenylyl cyclase) or facilitation of contraction ( activation of phospholipase C amp increased [Ca+])
2] Cell surface R as regulator of myometrium
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
A Fail-Safe system that maintains Ut quiescence
Multiple process act independently amp cooperatively to estabilish ut quiescence
To sustain Ut quiescence of phase 0 biomolecular systems ( neural endocrine paracrine and autocrine )
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
A Fail-Safe system that maintains Ut quiescence Phase 0 of parturition amp its quiescent state fa
ctor Actions of estrogen amp progesterone via intrace
llular R Myometrial cell plasma membrane R ndashmediate
d increase in cAMP Generation of cGMP Other systems including modifications in myo
metrial cell ion channels
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
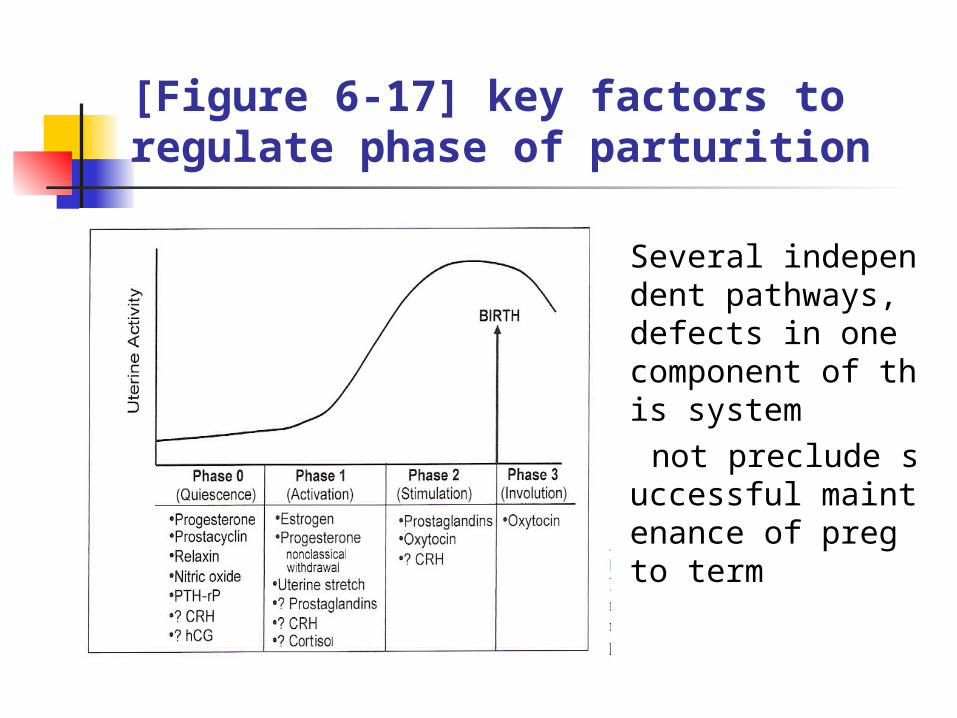
[Figure 6-17] key factors to regulate phase of parturition
Several independent pathways defects in one component of this system
not preclude successful maintenance of preg to term
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Progesterone amp Estrogen contributions to Phase 0 of parturition
Maintains Phase 0 of human parturition Removal of Progesterone ( Progesterone withdrawal)
progression of phase 0 into phase 1 of parturition Progesteron action
Successful maintenance of preg Biomolecular evidence or role of other agents not defined Maintain Phase 0 of human parturition
Estrogen action Promote progesteron responsiveness Ut quiescence In responsive tissues Estrogen R induces Progesteron R syn
thesis
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Steroid H Regulation of myometrial Cell-to-Cell communication
Progesteron Decrease expression of contraction associated proteins CAP grouping smooth m excitation contraction gap junction componen
ts uterotonic stimulatory R Inhibit expression of gap junctional protein connexin 43 Progesterone antagonist premature development of gap junction preter
m labor amp delivery Connexin 43 mRNA in human myometrial tissue increase before labor b
etween 37 ~40 wks Gap junction in myometrium increase But expression of connexin 43 protein not increase during gestation or
at labor in intracellular regulator of actual gap junction assembly at time of labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Heptahelical R that promote myometrial relaxation
Multiple process act independently amp cooperatively to estabilish ut quiescence
Associated with Gas-mediated activation of adenyly cyclase amp increased level of cAMP in myometrium
Part of fail-safe system to maintain Ut quiescence of phase 0 of parturition
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
B-adrenoreceptors
B-adrenoreceptors mediate Gas- stimulated increase in adenylyl cyclase increased level of cAMP
myometrial cell relaxation
Exact role of catecholamines in maintaining ut quiescence ill defined
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Luteinizing H (LH) amp chorionic gonadotropin(hCG)
LH amp hCG R in myometrium during preg greater before than during labor
Chorionic gonadotropin(hCG) activate adenylyl cyclase by plasma memb R Gas-linked system
decrease in contraction frequency amp force amp tissue-specific myometrial cell gap junctions
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Relaxin
Peptide H member of insulin like growth factor family of proteins A amp B chain
Secretion from corpus luteum
Greates amp peak at 1ngml 8wks ~12wks
Thereafter decline to lower lever until term
Activation of adenylyl cyclase amp promotes myometrial realxation effect cervical softening
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
CorticotropinndashReleasing H(CRH)
Myltiple isoforms their affinity amp coupling modified late in preg
Sythesized in PLamniondeciduamyometrium Increase final 6~8wks of preg Signal through cAMP or Calcium Relaxation or contraction of myometrial cell depending
on R isoform present CRH role of uterorelaxant during phase 0 amp uterotonin
in phases 1 amp 2 of parturition
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Parathyroid Hndashrelated protein (PTH-rP)
Initiate Gas-medated activation of adenylyl cyclase Expressd in myometriumamniondecidua amp trophobla
st PTH-rP expression in smooth m icreased by m stretch Function not establishedserve to maximize ut blood
flow durng myometrial contraction by vasorelaxant action
Facilitate maintenance of Ut tranquility
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Prostaglandins
Interact with family of 8 different heptahelical R
PG uterotoninsprostanoid sometimes can act as smooth m relaxant
Individual prostanoid diverse effect
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
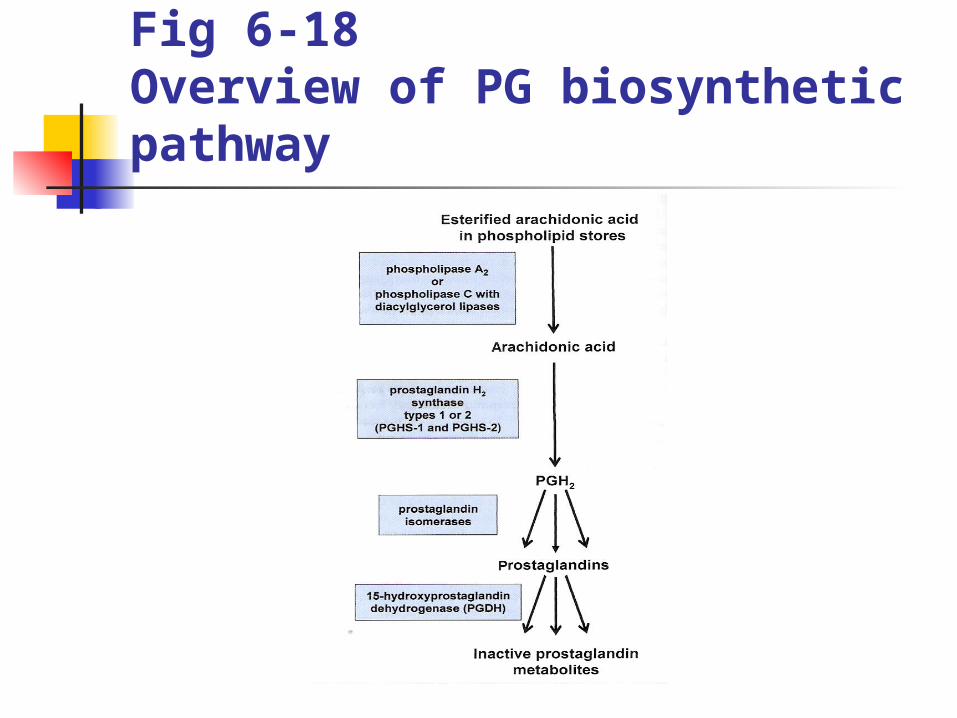
Fig 6-18Overview of PG biosynthetic pathway
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Prostaglandins
By action of phospholipase A2 or C Arachidonic acid act as substrate of type 1 amp type 2 P
G synthase (PGHS-1 amp -2) called COX ndash1 amp ndash2 Both convert Arachidonic acid to unstable endoperoxi
de PG G2 and then to PGH2target of many NSAIDs amp act as tocolytics to prevent preterm labor
PGH2 convert to active PG (PGE2PGF2 amp PGI2) PGDH Expression regulate in Ut rapidly incactivate PG
metabolites
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Prostaglandins
PG family of R classifed according to specificity of binding of given R to particular PG
DP(PGD2) amp IP (prostacyclin or PGI2) increase intracellular cAMP
FP R (PGF2a) increase intracellular Ca EP2 amp EP4 (PGE2) activate cAMP production PGE2 PGI2 maintain Ut quiescence by increasing cA
MP signaling PGE2PGD2PGI2 relaxation of vascular smooth m amp
vasodilation
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Prostaglandins
Either generation of specific PG or relative expression of various PG R determine responses of human myometrium
Change with gestation (32~35 wks vs 39~40wks ) Regional change in upper amp lower ut segment Prostanoid myometrial relaxation at one stage of pre
g amp regional myometrial contraction after initiation of parturition (in fundus)
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Atrial amp Brain natriuretic peptides amp cyclic guanosine monophosphate(cGMP)
Guanylyl cyclase activation increase intracellular level of cGMP promote smooth m relaxation
ANP amp BNP stimulate intracellular level of cGMP uarr BNP secreated by amnionANP expressed in PL Soluble form Guanylyl cyclase activated by nitric oxid
e penetrate pl membrane to enter cell NO react with iron in Guanylyl cyclase enzyme stimulat
e to produce cGMP act myometrial relaxation
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Accelerated Uterotonin degradation amp Phase 0 of parturition To stimulate myometrial cell refractoriness Activity of
enzymeuarr degrade or inactivate endogenoulsy produced uterotonins
Uterotonins (degredative enz) PG(PGDH) endothelin (enkephalinase) oxytocin (oxytocinase) histamine (diamine oxidase) catecholamines(catechol O-methlytransferase) angiotensin-II (angiotensinase) PAF(PAF ndashacetylhydrolase)
These enzyme increase by Progesteron action amp decrease late in gestation
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fail-safe system for Ut activation Phase 1 of parturition morphological amp functional change in myo
metrium amp Cx that prepare Ut for labor Development of uterotonin sensitivity improved intercellular com
municability via gap junctions Alteration incapacity of myometrial cell to regulate concentration
of cytoplasmic Ca2+
The process leading to enhance uterine responsiveness activation (by Chalis amp associates (2000))
As fuctional contractile capacity of myometrium amp Cx ripened phase1 merge into phase 2
Alteration in timing of these process cause preterm amp delayed labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
[Figure 6-17] key factors to regulate phase of parturition
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
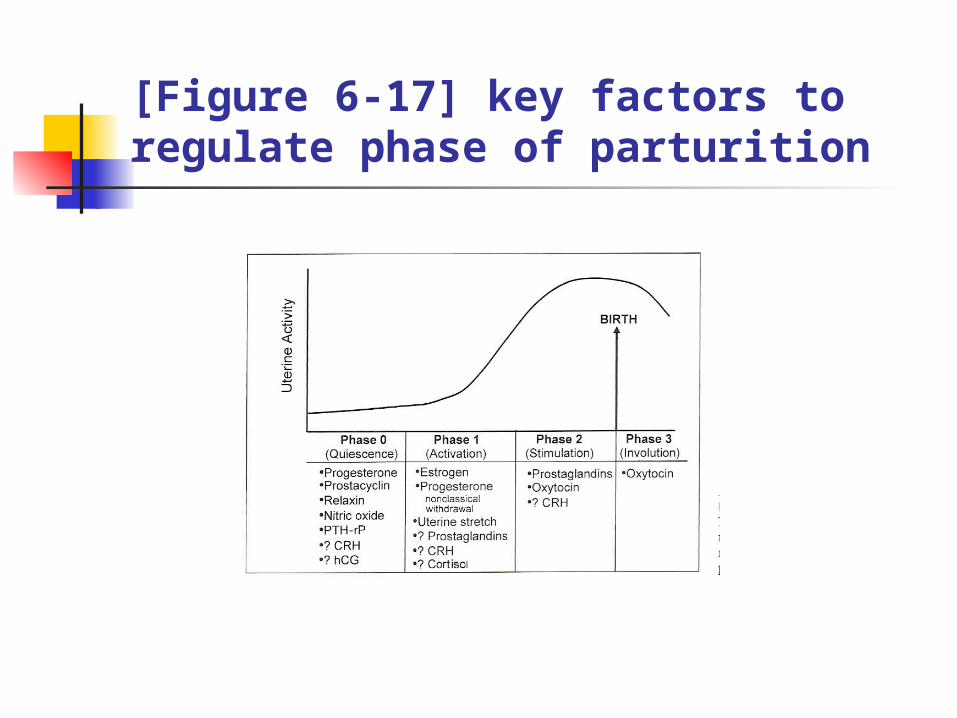
Classical Progesteron withdrawal not cause human parturition
In many species plasma progesterone level decrease Activation of Ut in preparation for labor Associated with increase in estrogen level in several s
pecies In primate plasma progesteron level not decrease be
fore labor only after delivery of PL decline Nonetheless morphological amp fuctional modification t
hat prepare Ut for labor occur in timely manner in human
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Classical Progesteron withdrawal not cause human parturition
In species Progesteron withdrawal can be blocked by administering Progesteron to mother
Conflicting reports whether or not Progesteron delay timely onset of parturition or prevent preterm labor
Majority of studies Progesteron cannot prevent preterm labor not appear to extend labor in control group
Progesteron metabolite 17-hydroxy progesteron (less potent than Progesteron )minimally decreased incidence of preterm labor in high ndashrisk group
additional research need
Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor

Progesteron R Antagonist amp human parturition RU 486 mifepristone less effective in inducing abortion or labor
in later preg effective in ripening Cx amp increase myometrium sensitivity to uterotonins
(Chwalisz amp Garfield1994) Decreased circulating progesterone by inhibitioning enzyme 3B-h
ydroxysteroid degydrogenase induced labor
Inhibition of progesterone action important for activation phase of parturition
But there is lsquohiddenrsquo or unique form of fuctional progesteron withdrawal that end ut quiescence
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fuctional Progesteron withdrawal in human parturition Unique mechanisms to inhibit progesterone action in human
Late gestational decrease in activity of progesteron R expression that cause fuctional withdrawal
Changes in relative expression of progesterone R or of its two isoforms shift in relative ratio of PR-A to PR-B(active isoform) within myometrium
Activity of Progesteron R for gene transcription in late gestation coactivator darr co-repressor uarr
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Oxytocin R Oxytocin R increase in myometrium during phase 1 o
f parturition Progesterone amp estradiol primary regulator of Oxytoci
n R expression Estradiol increase in myometrial Oxytocin R Progesterone increase in myometrial Oxytocin R degra
dation inhibit oxytocin R activation at cell surface maintain Ut quiescence through inhibition of myomet
rial oxytocin response
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fetal contributions to initiation of parturition
After growth amp maturation of vital organs fetus provide initial signal that set parturitional process
Via fetal brain pituitary gl adrenal gl Fetal blood to placenta
Unlikely initial signal for phase 1 of parturition is uterotonin
But Ut first must be prepared for labor before uterotonin optimally effective
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Role of Ut strecth in parturition In association with fetal growth significant increase in myometri
al tensile stress amp amnionic fluid pressure
Studies in rat models strecth was required for normal induction of specific contraction-associated pretein(CAPs)
Stretch expression of gap junction proteinuarrconnexin 43 amp oxytocin R
Twin preg amp hydramnios(Uterine stretch occur) at much greater risk of preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Role of Ut strecth in parturition
Cell signaling systems used by stretch to regulate myometrial cell mechanotransduction
Activation of cell surface R or ion channels signaling through extracellular matrix through release of autocrine molecule that act dire
ctly on myometrial cell
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fetal endocrine Cascades Leading to parturition
Placental-Pituitary ndashadrenal axis role in timing of human parturition
Activation of human fetal hypothalamic-Pituitary ndashadrenal axis critical component of normal parturition
Steroid product of fetal adrenal gl effect on placenta amp memb promote myometrium quiescent ---gt contractile state
Key component CRH (corticotropin-releasing H)
Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor

Action of CRH on fetal adrenal Gland Weigh same amp similar size in adult Daily production of steroid 100~200 mgday Steroidogenic fuction different from adult
Fetal cortisol level increase during last wks of gestation Increased DHEA-S production increase in maternal estrogens
(estriol) Increase in adrenal activity in contrast fetal adrenocorticotropic H
(ACTH) do not increase until stress of actual labor ACTH levels do not increase during last gestation Growth and differentiation of fetal adrenal gland influenced by facto
rs secreted by placenta Fetal zone of adrenal gland rapid involution immediately after birth
when placenta derived factors no longer available
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Action of CRH on fetal adrenal Gland
CRH of placental origin one of critical component that facilitate fetal adrenal hypertrophy amp increase steroidogenesis late in gestation
Ability of CRH to regulate adrenal gland amp of adrenal to regulate placental production of CRH feed-forward endocrine cascade late in gestation
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fig 6-19 Placental-fetal adrenal endocrine cascade
Maternal estrogen
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
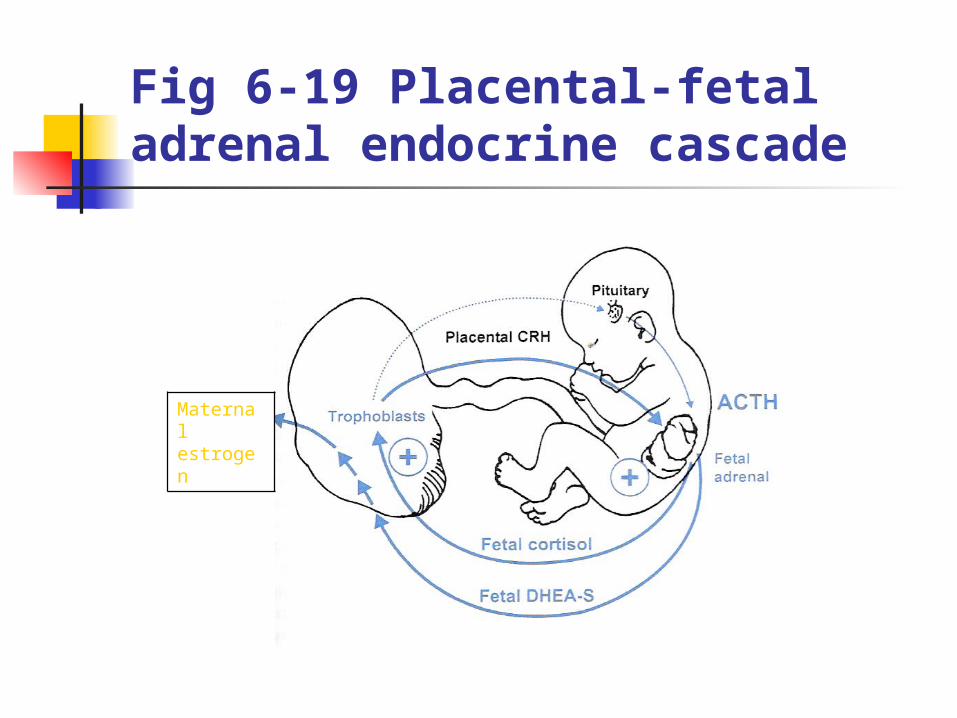
Placental CRH production Unlike hypothalamic CRH cortisol stimulate placental
CRH feed-forward endocrine cascade until separation of fetus from placenta at delivery
Rise in CRH as well as fetal adrenal steroidogenesis in late gestation
Maternal plasma CRH low in first trimester rising from midgestation to term
In last 12 wks CRH level rise exponentially peaking during labor then falling after delivery
Amnionic fluid levels of CRH increase in late gestation
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Placental CRH production Late pregnancy CRH-BP level in both maternal plasm
a amp Amnionic fluid decline CRH level increasing bioavailable CRH level increasing Various Complications CRH concentration in fetal pla
sma amp amnionic fluidmaternal plasma increasing over normal gestation
PL source for stress-associated increase in CRH fetal adrenal cortisol synthesis
Supranormal level of umbilical cord blood cortisol occurred in stressed neonates
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Potential Roles of CRH in timing of parturition Roles of PL CRH in regulation of parturition1Enhance fetal cortisol production((+) feedback on PL produce mor
e CRH) Modulate myometrial contractility
2Cortisol affect myometrium indirectly by stimulating membranes to increase PG synthesis
3CRH stimulate featal adrenal C19-steroid synthesis increased substrate for PL aromatization
Elevation in estrogens shift estrogen-to-progesterone ratio promote expression of contractile protein in myometrium
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fetal anomalies amp delayed parturtion Hypoestrogenism prolonged gestation
Fetal anencephaly adrenal hypoplasia placental sulfatase deficiency
Fetal anencephaly prolong human gestation (anomalous brain-pituitary-adrenal fuction)
Fetal adrenal gland hypoplasia onset of labor delayed
Fetal adrenal gland important for timely onset of parturtion
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fail-safe system for Success of phase 2 of Parturition
Phase 2 of Parturition Ut contraction that bring progressive cervical dilatation amp delivery
Formation of uterotonins most likely cause of initiation of labor
OxytocinPGserotoninhistaminePAF angiotensin II
Activate Gzi or Gaq-mediated processes increase myometrial cell [Ca2+]
Stimulate smooth m contraction through such G-protein coupling
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Oxytocin amp Phase 2 of Parturition During phase 1 of Parturition 50-fold or more increase in No of
myometrial Oxytocin R Uterine contractile responsiveness to Oxytocin increase Nanopeptide synthesized in magnocellular neurons of supraoptic
amp paraventricular neurons Oxytocin proH transport Carrier protein (neurophysin) along axo
ns to neural lobe of post pituitary gl in membrane bound vesicles for storage and later release
Oxytocin proH converted enzymatically to oxytocin during transport
Oxytocin not cause initiation of parturition but one of several participants in effectiveness of active labor
Oxytocin act by way of heptahelical R activate phospholipase
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition Striking increase in No of Oxytocin R in myometrial amp decidual tis
sues near end of gestation Oxytocin act on decidual tissue to promote PG release Oxytocin synthesized directly in decidual amp extraembryonic fetal ti
ssues amp in placenta Evidence in support of important role for Oxytocin during 2nd stag
e labor amp puerperium Oxytocin level increase
(1) during 2nd stage labor (end of phase 2 of parturition) (2) In early postpartum period (3) Breast feeding (phase 3 of parturition)
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Role of Oxytocin in Phase 2 amp Phase 3 of Parturition This timming of increased Oxytocin release role for O
xytocin at end of labor amp during puerperium After completion of Ut phase 2persistent contraction
=gtprevent postpartum hemorrhage
Oxytocin infusion in women promote increased level of mRNA in myometrium of genes that encode proteins essential for Ut involution
Oxytocin action at end of labor amp during phase 3 of parturition Ut involution
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
PGampPhase2 of Parturition PGF2a PGE2 involved in Phase 2 of Parturition process of labor 1Level of PG in amnionic fluid maternal plasma amp maternal urin
e increased during labor(Keirse1979) 2Tx of PG cause abortion or labor at all stage gestation (Novy amp
Liggins1980) 3PGH synthase type 2(PGHS-2) inhibitor delay time of onset of s
pontaneous labor amp sometimes arrest preterm labor 4PG Tx of myometrial smooth m in vitro cause contraction PG effectiveness of myometrial contractions of active labor once
labor is initiated
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Ut events regulating PG production Result of an inflammatory response that signal event l
eading to active labor Lowermost pole of fetal membranes structurally modif
ied in formation of forebag of amnionic sac Before labor fetal membranes cotiguous with amp attac
hed to ut decidua vera thin amp poorly developed As lower pole of amnionic sac pulled away from wall
of Ut fragment of decidua parietalis torn away but remain attached rather firmly to outer surface of chorion laeve
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fig 6-20] Sagittal view of exposed forebag amp attached decidual fragment after Cx dilatation during labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Ut events regulating PG production As Cx opendforebag presents through Cx in upper vagina
Surface area of exposed forebag increases as cervical dilatation progresses during phase 2 of parturition
Traumatized devascularized decidual tissue fragmnets that torn away from Ut form irregular lining on outer surface of forebag present in vagina
Forebag tissues bathed continoulsy by vaginal fluid contain large numberampvariety ofmicroorganismbacterial toxins in large amount amp PG amp cytokines
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
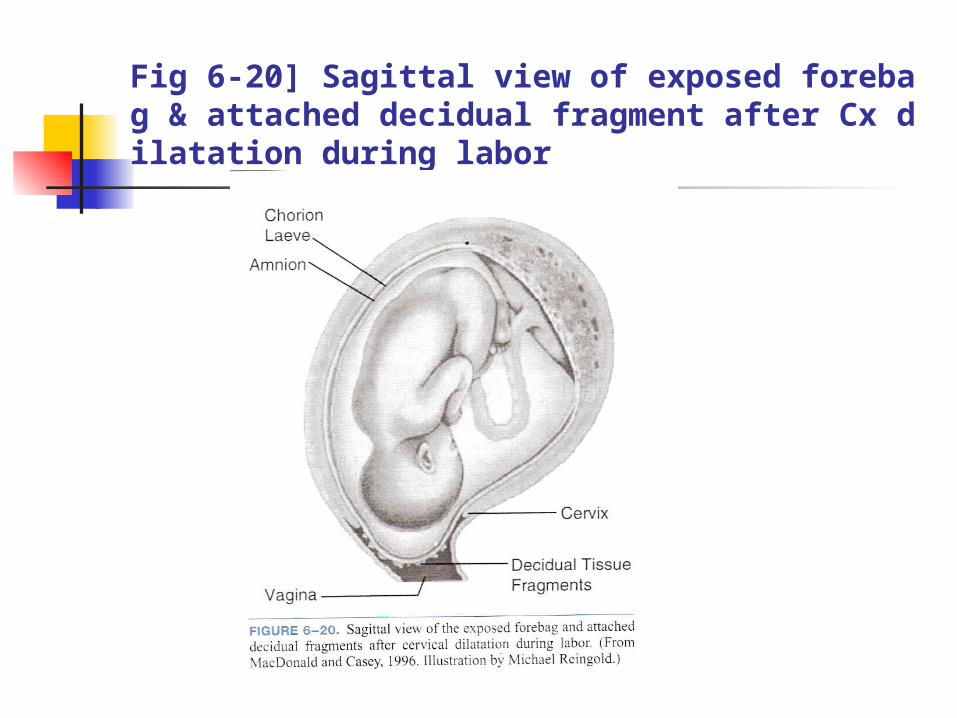
Ut events regulating PG production Taruma to decidual tissues in formation of forebag Devascularization of decidual fragments that pulled a
way from Ut Action of vaginal fluid inflammatory response in decid
ual fragment of forebag During labor level of cytokine in forebag much greater
than in upper compartment of amnionic sac Cytokine produced in forebag enhance level of PG pr
ouduce by amnion higer level of PG in forebag
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Figure 6-21] mean values of PGF2aPGFMPGF2a+PGFM ampPGE2
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Fig 6-22]PG recoverd from vaginal fluid before amp during labor PGE2PGF2a PGFM
PG synthesized in forebag tissues released into vagina
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
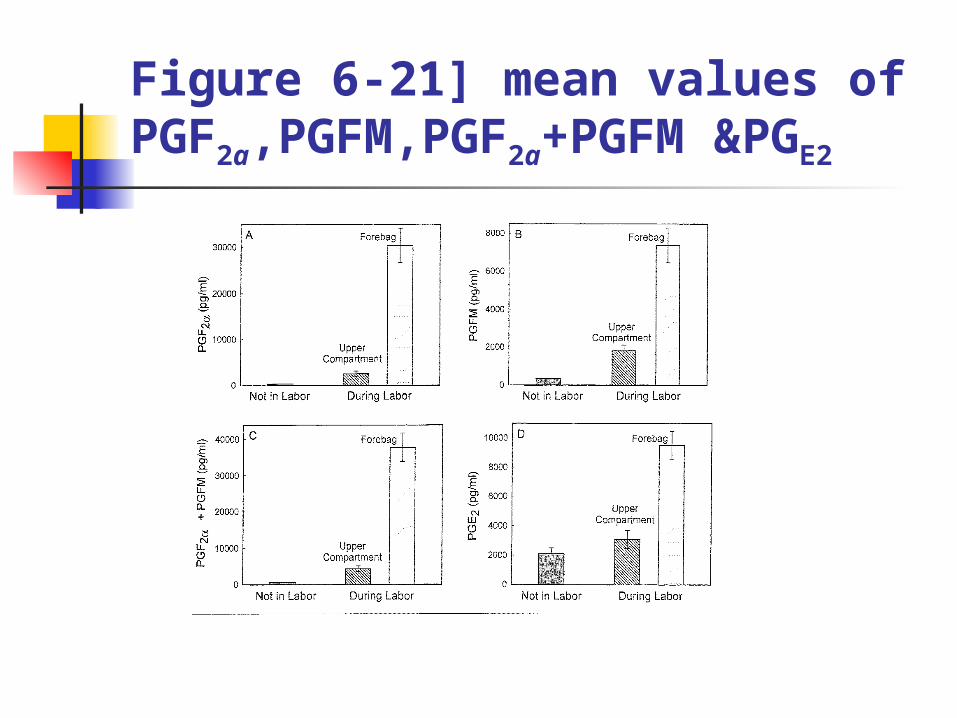
Ut events regulating PG production Inflammatory mediators facilitate cervical dilatation amp
alteration to lower uterine segment Cytokine amp chemokine
further extracellular matrix degradation increase level of hyaluronic acid cause influx of leukocyte into area
Cytokine amp PG degrade extracellular matrix weakening fetal membrane
rapid change in Cx
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
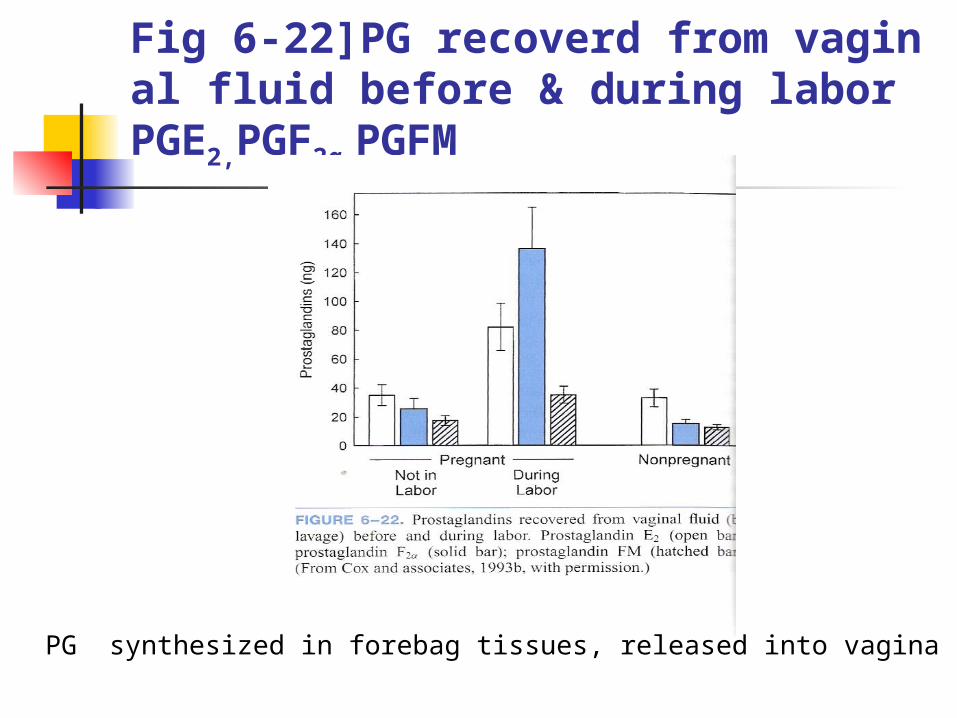
Platelet-Acitvating Factor(PAF) Heptahelical family of transmembrane R amp act to increase myo
metrial cell calcium promte Ut contraction When cervical dilatation exposure of traumatized forebag tiss
ues to vaginal fluids inflammatory process PAF produced in leukocytes PAF ndashacetylhydrolase present and possesses high specific activit
y in macrophage (in large number of decidua) Myometrium may be protected from PAF action by PAF ndashacetylh
ydrolase
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Endothelin-1 Endothelin A R in smooth m cell increase in intracellul
ar calcium by linkage to both Gaq- G ai- subunit of G proteins
Endothelin-1 produced in myometrium
Endothelin-1 also synthesized in amnion Transported to myometrium without degradation
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
AngiotensinII AT2 nonpregnant women
AT1 pregnant women
During pregnancyvascular smooth m express AT2R is refractory to pressor effect of angiotensin II
In myometrium near termangiotensin II another component of uterotonin systemacting to promote increased myometrial cell calcium
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
CRHhCGPTH-rP Switch from cAMP formation to increased myometrial
cell calcium
Oxytocin attenuate CRH-stimulated accumulation of cAMP in myometrial tissue
CRH augment contraction ndashinducing potency of oxytocin
CRH increase myometrial contractile force in response to PGF2a
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Contribution of intrauterine tissues to parturition
Membrane decidua important tissue shell around fetus that serves as physical immunological metabolic shield that protect against untimely initiation of parturition
Late in gestation fetal membrane change amp act to prepare for labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Amnion
Tensile strength of membranes resistance to tearing and rupture
Resistant to penetration by leukocytes microorganism neoplastic cell from maternal compartment
Selective filter to prevent fetal particulate-bound lung and skin secretions from reaching maternal compartment
Maternal tissues protected from constituents in amnionic fluid that adversely affect decidual or myometrial function
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Amnion
Several bioactive peptides amp PG which cause myometrial relaxation or contraction are synthesized in amnion
Increase in amnion PG biosynthetic capability late in gestation
Amnion increase its activity for phospholipase A2 amp PGHS-2 late in gestation
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Chorion laeve Protective tissue providing immunological acceptance Enriched with enzyme inactivate uterotonin such as P
G dehydrogenaseoxytocinase During most of gestation PG produced by amnion r
elease into amnionic fluid or metabolized by adjacent chorion
Exact role of fetal membrane derived peptide or PG in initiation of parturition under debate
Important for process of labor amp in involution (phase 2 amp 3)
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Decidua parietalis Central question Whether decidual activation preced or follow o
nset of labor
Process of decidual activation localized to exposed decidual fragment lining forebag
Traumahypoxia exposure of forebag decidua to endotoxin lipopolysaccharidemicroorganismIL-1B in vaginal fluid provoke inflammatory reaction
series of cytokine increase production utertonins (principally PG) or act directly in myometrium to cause contraction
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Regulation of phase 2 of parturitionSummary Multiple process contribute to success of phase 2(act
ive labor)
Variety of myometrial heptahelical R promote Ut quiescence
But another group inhibit cAMP formation or activate phospholipase C or A2 or both
Source of regulatory ligand for teses R varies from endocrine H such as oxytocin to locally produced PG
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Physiology amp Biochemistry of preterm labor
Conditions lead to preterm delivery Complications of pregnancy that jeopardize fetal healt
hamp sometimes maternal heath mandate preterm delivery 25
Preterm premature rupture of fetal membranes (PPROM) followed by preterm delivery 25
Spontaneous preterm labor with intact fetal membrane 50
Cx of preg threaten fetal health Maternal HTN severe DMfailure of fetal growth multiple pre
g abrutio placenta
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Preterm premature rupture of fetal membranes (PPROM)
Spontaneous rupture of fetal membranes that occur before 37 wks complete weeks before onset of labor
Major predisposing cause intrauterine infection Pathogenesis of PPROM increased apoptosis of cellular compo
nents of fetal membrane as well as elevation in specific proteases in membrane amp amnionic fluid
Much of tensile strength of fetal membranes provided by extracellular matrix within amnion
Interstitial amnionic collagen(type I III) produced in mesenchymal cell structual component most important for its strength
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Preterm premature rupture of fetal membranes (PPROM) 1Degradation of collagen
Matrix metalloproteinase (MMP) family of proteinase normal tissue remodeling amp particularly degradation of collagen
MMP-2MMP-3MMP-9 members found in higher concentraion in amnionic fluid in PPROM
Activity of MMP regulated by tissue inhibitor of matrix metalloproteinase(TIMP)
In lower concentraion in amnionic fluid in PPROM Elevation of MMP at time when protease inhibitor expression dro
p Alter tensile strength of amnion Increase incidence of PPROM
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Preterm premature rupture of fetal membranes (PPROM)
2Higher degree of cell death Markers of apoptosis increased in membrane with PP
ROM compared with normal term membranes Activation of collagen breakdown amp cell death weak
ening amnion Survey of 18 independent studies (1979~2000) of 14
62 women with PPROM (+) culture of amnionic fluid in PPROM 13
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Preterm premature rupture of fetal membranes (PPROM)
Studies performed to address prophylatic antimicrobial Tx to prevent PPROM
Evidence early Tx of some asymptomatic lower genital tract infection active periodontal inflammation reduce incidence of PPROM amp preterm birth (conflicting study)
Current research being focused on certain mediators of this process that accumulate in amnionic fluid amp may provide early markers for women at risk for PPROM
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Spontaneous preterm labor More common cause
multifetal pregnancy bleeding intrauterine infection placental infarction premature cervical dilatation cervical incompetence uterine fundal abnormalities fetal anomalies
Maternal illness ( nonobstetrical infection) Autoimmune disease Gestational hypertension
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Spontaneous preterm labor
Actual process of preterm labor final step result from premature uterine activation that initiate weeks before onset of labor
Result from premature initiation of phase 1 of parturition
(Cervical ripening amp myometrial activation)
Major cause of spontaneous preterm labor uterine distention maternal-fertal stress infection
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Uterine distention Ut stretch play important role in normal process of my
ometrial activation in prepartion for labor Multifetal gestation or hydramnios Early uteirne distention initiate expression of contracti
on-associated protein(CAP) in myometrium CAP gene influenced by strecth coding for gap junctio
n protein(such as connexin 43) for oxytocin R amp for PG synthase
Excessive uterine strecth premature loss of myometrial quiescence
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Uterine distention Exhibit early activation of placental-fetal endocrine ca
scade Early rise in maternal CRH amp estrogen level further en
hance expression of myometrial of myometrial CAP genes
Cervical length important risk factor in multifetal pregnancies
Uterine stretch amp endocrine activity in multifetal gestation initiate sequence of event shift in timming of uterine activation including premature cervical ripening
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Maternal-fetal stress Complexities of measuring stress and other
moderating psychosocial factor that lead to stress contribute to difficulty of defining its exact role in preterm birth
Studies showing correlation between maternal psychological stress amp placental-adrenal endocrine axis potential mechanism for stress-induced preterm birth
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Maternal-fetal stress Last trimester marked by rising maternal serum level of placental
-derived CRH increase adult and fetal adrenal steroid hormone production i
ncluding initiation of fetal cortisol biosynthesis Maternal amp fetal cortisol further increase placental CRH secretio
n develop feed-forward endocrine cascade CRH stimulate fetal adrenal DHEA-S biosynthesis increase mate
rnal circulating estrogens (estriol) Premature rise in cortisol amp estrogen cause early loss of uterine
quiescence
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Maternal-fetal stress
Preterm labor is associated with early rise in maternal circulating CRH (Holzman2001)
Level of CRH in term amp preterm women similar
However women destined for preterm labor rise in CRH that occurs 2 to 6 weeks earlier (McLean amp coworker1995)
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Maternal-fetal stress Several studies early rise of serum estriol in women preterm lab
or (Heine co-workers2000) Premature rise in estrogen alter myometrial quiescence
Associated with maternal fetal biological stress response Several studies CRH or estriol level activated in preterm birth du
e to infection amp multifetal pregnancies (Gravett amp collegue2000)
Thus activation of this axis activation of phase I of parturition Further study will be needed to define exact biochemical role of
CRH estrogens amp cortisol in preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Infection amp preterm labor
Administration to animal of bacteria or bacterial endotoxin cause abortion or perterm delivery which is accompanied by decidual hemorrhage and necrosis
40 of preterm labor caused by intrauterine infection
Incidence of (+) culture of amnionic fluid during preterm labor 10~40 (Average13)
Morel likely to develope chorioamnionitis amp PPROM than women with negative culture
More neonate complication
The earlier onset of perterm labor the greater likelihood of documented amnionic fluid infection
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Infection amp preterm labor
Associate Chorioamnionitis with preterm labor (Chellam amp Rushton1985Goldenberg amp
associates2002) Microbe invade maternal tissue only not amnionic fl
uid Endotoxin stimulate amnionic cell to secrete cytokin
e that enter amnionic fluid Explain association between amnionic fluid cytokine
s and preterm labor microbe not detectable in amnionic fluid
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Infection amp preterm labor
Infection-mediated preterm delivery preventable by antimicrobial Tx
However debate on effectiveness of antimicrobial prophylaxis
Effectiveness of antimicrobial prophylaxis to prevent spontaneous preterm birth recommneded in only a few situation to prevent spontaneous preterm delivery
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Sources for intrauterine infection
1 transplacental transfer of maternal systemic infection
2 Retrograde flow of infection from peritoneal cavity via fallopian tube
3 Ascending infection with bacteria form vagina amp Cx
Lower pole of fetal membrane-decudual junction embraces orifice of cervical canal which anatomically patent to vagina Passageway for microorganisms to enter intrauterine tissue
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Sources for intrauterine infection
Categorize intrauterine infection into four stage (Goncalves amp co-workers 20002)
stage I microbial invasion that include bacterial vaginosis
stage II Decidual infection stage III Amnionic infection stage IV Fetal systemic infection Progression of these stages increase effect on preter
m birth amp neonatal morbidity
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Sources for intrauterine infection Pathogenesis of infection- induced preterm labor (fig 6-23) Microorganism originating in vagina or cervix after ascending co
lonize decidua and possibly fetal membranes then may enter amnionic sac
Lipopolysaccharide or other toxin elaborated by these bacteria induce cytokine production in cell within decidua membrane or fetus itself
Lipopolysaccharide amp cytokine increase provoked PG release from fetal membrane decidua
Rise in cytokines amp PG influence both cervical ripening amp loss of myometrial quiescence with resultant myometrial stimulation (Challis2002Keelan2003)
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Pathogenesis of infection- induced preterm labor (fig 6-23)
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Microbes associated with preterm birth
Gardnerella vaginalis Fusobacterium Mycoplasma hominis Ureaplasma urealyticum are detected more commonly in amnionic fluid of preterm labor
Further studies needed to better define intrauterine site of infection most influence timing of delivery why some pregnant women appear more susceptible to microbe
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Intrauterine inflammatory response to infection
Initial inflammatory response elicited by bacterial toxin in mediated by specific R on mononuclear phagocytes decidual cells trophoblast
Toll-like R present in placenta on trophoblast cell as well as fixed amp invading leukocytes
Influence of ligand such as bacterial lipopolysaccharide R increase local release of chemokine cytokines PG as part of inflammatory response
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
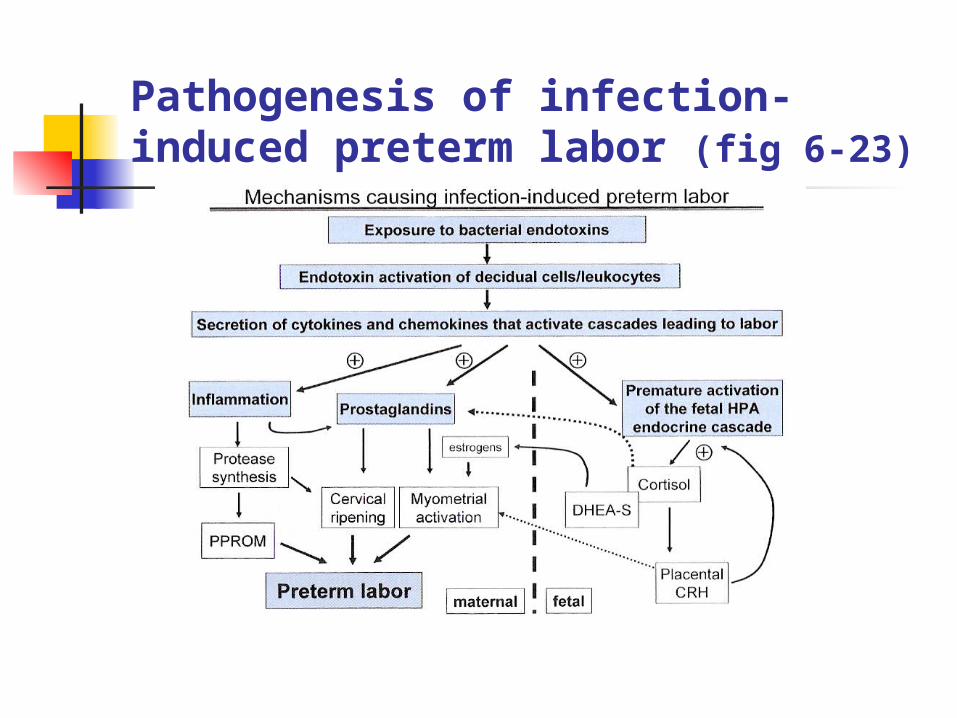
Intrauterine inflammatory response to infection
Lipopolysaccharide stimulation IL-1 promote increase synthesis of other cytokines( TNF-AIL-6 IL-8)
Proliferation activation migration of leukocyte Modification in extracellular matrix protein Mitogenic amp cytotoxic effect including fever amp acute phase respons
e
IL-1promote PG formation in many tissues including myometriumdecidua amnion
Appear to be cascade of event once inflammatory response in initiated that can result in preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Origin of cytokines in intrauterine infection Transfer of cytokine from decidua across membranes into amnionic fluid
severely limited
Thus cytokine produced in maternal decidua amp myometrium have effect on that side whereas cytokine produced in membrane or in cell within amnionic fluid not tranferred to maternal tissue
In most cases of inflmmation resulting from infection resident and invading leukocyte produce bulk of cytokine
Leukocyte (neutrophilmacrophageT lymphocyte) infiltrate Cx lower Ut segment fundus at time of labor
Invading Leukocyte major source if cytokine at time of labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Origin of cytokines in intrauterine infection
In term laboring Ut both invading leukocyte amp certain parenchymal cell produce cytokine
Primary source of myometrial cytokines including IL-1 IL-6 IL-8 TNF-a (in decidua both stromal cell amp invading leukocytes in Cx glandular amp surface epithelial cell)
IL-8 critical cytokine in cervical ripening produced in both epithelial amp stromal cell of Cx
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Origin of cytokines in intrauterine infection Cytokine in Amnionic fluid amp their association with preterm labor
has been well documented But exact cellular origin not well defined Amnionic fluid IL-1 probably not arise from amnion tissue fetal u
rineor fetal lung secretion but most likely secreted by mononuclear phagocyte or neutrophils activated amp recruited into amnionic fluid
IL-1 in amnionic fluid likely generated in situ from newly recruited cell
Amount of amnionic fluid IL-1 would be determined by number of leukocyte recruited their activational status or effect of amnionic fluid constituent on their rate of IL-1 secretion
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Origin of cytokines in intrauterine infection Leukcocyte infiltration regulated by fetal membrane synthesis of specific chemoki
nes
In term labor increased amnionic fluid concentration of potent chemoattractant and monocyte-macropage activatior monocyte chemotactic protein-1(MCP-1)
Level of MCP-1 much higher in forebag compared with upper compartment
In preterm labor significantly higher than in normal term amnionic fluid
MCP-1 may be the factor that initiate fetal leukocyte infiltration of placenta amp membrane
MCP-1may act as marker of intra-amnionic infection amp inflammation
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Summary of infection amp preterm labor Intrauterine infection cause significant number
of cases idiopathic spontaneous preterm labor
Variety of site for intrauterine infection amp similarities between inflammatory response of preterm amp term labor difficult to determine proportion of pregnancies that end prematurely due to infection
Mechanistically infection induced preterm labor as process causing early initiation of phase 1 of parturition
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Summary of infection amp preterm labor Initial exposure to bacterial endotoxin leading to prod
uction of cytokines
In Cx theses cytokine cause of infiltration of leukocyte amp ripening
Activation of proteases in Cx promote Cx dilatation amp weaken fetal membranes PPROM
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor
Summary of infection amp preterm labor Transfer of bacteria or cytokine into fetal circulation premature activation of CRH amp placentalndashadrenal end
ocrine cascade loss of myometrial quiescence
Continued leukocyte infiltration proinflammatory cytokine further increase PG within maternal decidua amp myometrium act as uterotonin
preterm labor