-
Gut, 1984, 25, 526-530
Case reports
Sclerosing cholangitis and histiocytosis XH H THOMPSON, H A
PITT, K J LEWIN, AND W P LONGMIRE Jr
From the Departments ofSurgery and Pathology, UCLA School of
Medicine, Los Angeles, California, USA
SUMMARY Three patients with biopsy proven histiocytosis X who
developed a clinical andpathological picture compatible with
sclerosing cholangitis are reported. In one patient,operative
biopsy of the common bile duct revealed histiocytosis X in the
granulomatous/xanthomatous phase. At necropsy, however, only
fibrosis of the biliary tree was seen, a pictureconsistent with
sclerosing cholangitis. Fibrotic obstruction of the biliary tree
led to death fromliver failure in all three patients. The aetiology
of primary sclerosing cholangitis is unknown andmay be
multifactorial. Perhaps involvement of the biliary tree by
histiocytosis X is one cause.
Sclerosing cholangitis may be primary or related tocongenital
malformations of the biliary tract, ductcalculi, operative trauma,
or cancer of the bileducts.' Primary sclerosing cholangitis is
rare,2 andits aetiology unknown. Viral, bacterial and auto-immune
theories have been proposed,3 but evidencefor them is lacking. The
association betweensclerosing cholangitis and other diseases,
includingulcerative colitis, Crohn's disease, Riedel'sthyroiditis,
retroperitoneal fibrosis and pancreatitis,has been reported,4 5 but
the significance of theseassociations has yet to be determined.
Perhapsprimary sclerosing cholangitis has more than onecause, as
su6ggested by the very variable course ofthe disease.
Biliary obstruction in an adult resulting frominvolvement of the
intra- and extrahepatic biliarytree by histiocytosis X has been
reported recentlyfrom this institution.7 The patient has
subsequentlydied and further review of her clinical
course,radiology, and pathology reveals many featuresidentical to
those of primary sclerosing cholangitis.Review of our patients8 9
with a clinical picturecompatible with sclerosing cholangitis has
revealedtwo additional patients with histiocytosis X. Wereport here
the case histories of these three patientsand discuss the possible
nature of the associationbetween these two rare conditions.
Address for correspondence: Mr H H Thompson. MS. FRCS. Surgical
Unit.The London Hospital. Whitechapel, London El 1BB.Received for
publication 29 July 1983
526
Case reports
CASE 1A 44 year old woman was admitted with a history offatigue,
epigastric pain, and jaundice. Five yearspreviously she had
developed diabetes insipidusafter a road traffic accident. This
resolved over thenext two years. A vulval ulcer biopsied nine
monthsbefore admission was diagnosed as eosinophilicgranuloma.
Examination showed jaundice andseveral bluish nodules in the left
axilla, biopsy ofwhich also showed eosinophilic granuloma.Relevant
investigation results were: serum bilirubin42 ,umol/l, serum
aspartate aminotransferase (AST)167 u/l (normal
-
Sclerosing cholangitis
A-
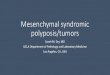
Fig. 1 Section ofcommon bileductfrom case 1 showing adense
inflammatory infiltrate inwall. The infiltrate is composedprimarily
of 'histiocytes' andeosinophils(H and E x40
originalmagnification)
trial of vinblastine were given but with no sympto-matic or
objective improvement. A cholangiogram,carried out 15 months after
her laparotomy, showeda stricture of the right hepatic duct. A
furtherlaparotomy was performed, the stricture dilated andthe T
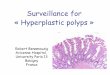
tube replaced. A postoperative cholangiogramrevealed sparse and
tenuous intrahepatic ducts (Fig.2). Despite this procedure, her
liver functiondeteriorated and she died of hepatic failure
fourmonths later. Necropsy showed advanced biliarycirrhosis and
dense fibrosis at the porta hepatis. Thediagnosis of histiocytosis
X would have been difficultto make from histopathological
examination of thenecropsy material.
CASE 2A 65 year old man was admitted with a recenthistory of
pruritus and jaundice. At laparotomy theliver appeared cirrhotic
and the extrahepatic bileducts were embedded in a mass of fibrous
tissue. Acholecystectomy was performed. The common ductcontained
'sludge' and its distal portion appearedoccluded. The common duct
was drained externally.Liver biopsy showed biliary cirrhosis. The
gallbladder, which contained no stones, showed themicroscopic
features of chronic cholecystitis.Biopsies from around the
extrahepatic bile ductswere reported as showing fibrosis and
chronicinflammation. Postoperatively, he complained ofpolydipsia
and polyuria.He was transferred to UCLA Medical Center. On
admission his serum bilirubin was 100 ,umol/l. Asecond
laparotomy confirmed the previous findings.In addition, an
operative cholangiogram showed
small, irregular right biliary radicles with non-visualisation
of the left intrahepatic biliary tree anddistal common bile duct. A
choledochojejunostomywas performed. After this operation, his
urineoutput greatly exceeded his fluid intake (in one day,
Fig. 2 T tube cholangiogram performed soon after
secondlaparotomy in case 1.
527
on April 3, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.25.5.526 on 1 M
ay 1984. Dow
nloaded from
http://gut.bmj.com/
-
Thompson, Pitt, Lewin, and Longmire Jr
intake 14 1, urine output 6 25 1). A diagnosis ofdiabetes
insipidus was made, but the cause notascertained. He died in liver
failure six months afterhis first laparotomy. Necropsy showed a
liverweighing 0*7 kg with the microscopic features ofbiliary
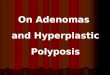
cirrhosis. Microscopic examination of theneurohypophysis showed
histiocytosis X (Fig. 3).
CASE 3A 17 year old girl with an 11 year history ofhistiocytosis
X involving lymph nodes, lung andskull, presented with episodes of
abdominal painand jaundice. A laparotomy was performed. Thegall
bladder was found to be fibrotic and thecommon duct strictured.
Both the gall bladder andthe bile ducts contained soft, black
stones. Acholecystectomy, choledocholithotomy, and
chole-dochojejunostomy were performed. Post-operatively, she
suffered from episodes ofcholangitis. Steroid therapy was
instituted. At theage of 19 years, her choledochojejunostomy
wasfound to be strictured and was revised.At the age of 21 years,
she was admitted to UCLA
Medical Center. Liver function tests at that timewere: serum
bilirubin 400 gmol/l, serum AST 193u/I, serum alkaline phosphatase
809 u/l. A furtherlaparotomy revealed a dense mass of fibrous
tissueat the porta hepatis, in which no bile duct could
beidentified. An attempt to perform a cholangio-jejunostomy failed
as no suitable duct foranastomosis could be identified after
amputating theleft lateral segment of the liver. Histology of
theresected liver showed secondary biliary cirrhosiswith no
features of histiocytosis X. She was
discharged from hospital but died soon after fromhepatic
failure. A necropsy was not performed.
Discussion
The three patients reported had both a clinicalpicture
consistent with sclerosing cholangitis andhistopathological
evidence of histiocytosis X. Twocases presented in adult life with
no evidence ofbone involvement. This is atypical of
histiocytosisX.10 The generic term. histiocytosis X, wasproposed by
Lichtenstein"1 to stress the histopatho-logical similarities
between the Hand-Schuller-Christian syndrome, Letterer-Siwe disease
andeosinophilic granuloma of bone. Otherauthorsl2 l3consider it
unwarranted to group themtogether and have proposed other
classifications,but none have gained widespread
acceptance.Histiocytosis X may be a misnomer as thepredominant cell
in the lesions is the Langerhanscell rather than the histiocyte.
Langerhans cellgranulomatosis has been suggested as an
alternativeterm. 14The liver is frequently involved in infants with
the
acute disseminated form of histiocytosis X(Letterer-Siwe
disease). 15 Pathological changesinitially consist of infiltration
of the portal tracts byhistiocytes, with fibrosis and cirrhosis
occurringsubsequently.16 Single case reports of children
withinvolvement of the extrahepatic bile ducts by histio-cytosis X
have been made.'5 17 18 In addition,LeBlanc et al9 described three
childhood cases, inone the common duct was affected and in two
therewas partial stenosis at the confluence of the left and
A.e'di .'.
... i ..o
Fig. 3 Section ofneurohypophysis from case 2showing an
inflammatoryinfiltrate containingcharacteristic 'histiocytes'
withfolded grooved nuclei (H and Ex 160 original magnification)
._ /
528
on April 3, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.25.5.526 on 1 M
ay 1984. Dow
nloaded from
http://gut.bmj.com/
-
Sclerosing cholangitis 529
right hepatic ducts. This latter appearance isfrequently seen in
primary sclerosing cholangitis.8Also cholangiography in those
patients with histio-cytosis X and cholestasis shows an appearance
of theintrahepatic ducts similar to that seen in primarysclerosing
cholangitis.19
In addition to the reports in children, Parker andLichtenstein2
described an adult with involvementof the extrahepatic ducts by
histiocytosis X, butwithout biliary obstruction. Histiocytosis X
andbiliary obstruction has been reported7 in an adultwhose case
history and necropsy findings areincluded in this paper (case 1).
In this patient, theinitial biopsies of the tissue encasing
theextrahepatic bile ducts showed histiocytosis X.Microscopic
examination of tissue taken from thissite at necropsy, however,
revealed only chronicinflammation and fibrosis. In case 2, the
thickenedgastrohepatic ligament was biopsied at twolaparotomies. On
both occasions, the tissue wasreported as showing chronic
inflammation andfibrosis. No features of histiocytosis X were
present.This diagnosis was only made after postmortemexamination of
the neurohypophysis. In case 3,histological confirmation of
histiocytosis X wasmade from cervical lymph node and
mandibularbiopsies at age 6 and 10 respectively. At age 17,
abiliary stricture was found at her first laparotomy.Subsequently,
she sclerosed the whole of her biliarysystem. No biopsies were
taken from the bile ductsor from the tissue surrounding
them.Engelbreth-Holm et alP described four histo-
pathological stages through which a lesion of histio-cytosis X
may progress: (i) a hyperplastic orproliferative phase, (ii) a
granulomatous phase, (iii)a xanthomatous phase and (iv) a fibrous
phase.Once a lesion has entered the last phase, it loses
thehistological features which permit the diagnosishistiocytosis X
to be made. In case 1, the biopsytaken at the first laparotomy
showed the lesionencasing the bile ducts to be in the
granulo-matous/xanthomatous phase, whereas examinationof the same
tissue obtained at necropsy showed it tobe in the fibrous phase.
Perhaps the fibrosissurrounding the bile ducts in case 2 represents
thefibrous phase of a histiocytosis X lesion.
Different authors' 8 22 have used different criteriafor
inclusion of patients under the diagnosis ofprimary sclerosing
cholangitis. Case 1 had clinicaland radiological features of
primary sclerosingcholangitis, but would be excluded from having
thisdiagnosis by some authors because the biliaryobstruction was
due to involvement of the biliarysystem by histiocytosis X. This
diagnosis was madebecause the biopsy was taken while the lesion was
inthe granulomatous/xanthomatous phase. It is
conceivable that this diagnosis would have beensubstituted by
that of primary sclerosing cholangitisif the biopsy had been taken
later, when the lesion'had entered the fibrous phase. Case 2 could
beconsidered a classic example of primary sclerosingcholangitis,
fulfilling the most rigid criteria22 neces-sary for making the
diagnosis. Case 3, at age 17, hadstones in both the gall bladder
and the bile ducts.These stones were soft and black and may
haveresulted from stasis in a strictured biliary systemrather than
have been the cause of the sclerosingcholangitis.One may speculate
as to whether some cases of
primary sclerosing cholangitis are caused byinvolvement of the
biliary tree by histiocytosis X.The characteristic
histopathological features ofhistiocytosis X may not be appreciated
because thelesion has entered the fibrous phase at the time
ofbiopsy. It is likely that more than one causal agentmay result in
a clinical picture consistent withprimary sclerosing cholangitis.
Perhaps involve-ment of the bile ducts by histiocytosis X
representsone pathogenic mechanism for the development ofprimary
sclerosing cholangitis. Until more is knownabout the aetiology of
these two diseases, however,the nature of their association must
remainspeculative.
References
1 Longmire WP Jr. When is cholangitis sclerosing? Am JSurg 1978;
135: 312-20.
2 Glenn F. Whitsell JC. Primary sclerosing cholangitis.Surg
Gynecol Obstet 1966; 123: 1037-46.
3 Fee HJ. Gewirtz H. Schiller J. Longmire WP Jr.Sclerosing
cholangitis and primary biliarv cirrhosis - adisease spectrum? Ann
Surg 1977; 186: 589-93.
4 Whelton MJ. Sclerosing cholangitis. Clin Gastroenterol1973; 2:
163-73.
5 Chapman RWG. Marborgh BA. Rhodes JM et al.Primary sclerosing
cholangitis: a review of its clinicalfeatures. cholangiography. and
hepatic histology. Gut1980; 21: 870-7.
6 Wiesner RH. LaRusso NF. Clinicopathologicalfeatures of the
syndrome of primary sclerosingcholangitis. Gastroenterology 1980;
79: 200-6.
7 Jones MB. Voet R, Pagani J. Lotysch M. O'Connell T.Loretz RL.
Multifocal eosinophilic granulomainvolving the common bile duct:
histologic andcholangiographic findings. Gastroenterologv 1981;
80:384-9.
8 Thompson HH. Pitt HA. Tompkins RK. Longmire WPJr. Primary
sclerosing cholangitis: a heterogenousdisease. Ann Surg 1982; 196:
127-36.
9 Pitt HA. Thompson HH. Tompkins RK. Longmire WPJr. Primary
sclerosing cholangitis: results of an aggres-sive surgical
approach. Ann Surg 1982: 196: 259-68.
on April 3, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.25.5.526 on 1 M
ay 1984. Dow
nloaded from
http://gut.bmj.com/
-
530 Thomtipson, Pitt, Lewin, and Longmire Jr
10 Cheyne C. Histiocytosis X. J Bone Joint Surg (Br)1971. 53:
366-82.
11 Lichtenstein L. Histiocytosis X: integration ofeosinophilic
granuloma of bone 'Letterer-Siwe'disease and Schiuller-Christian'
disease as relatedmanifestations of a single nosologic entity.
Arc/i Pathol1953: 56: 84-102.
12 Vogel JM. Vogel P. Idiopathic histiocytosis: a discus-sion of
eosinophilic granuloma. the Hand-Schiiller-Christian svndrome and
the Letterer-Siwe syndrome.Semin Hematol 1972: 9: 349-69.
13 Daneshbod K. Kissane JM. Idiopathic
differentiatedhistiocvtosis. Am J Clini Pathol 1978; 70: 381-9.
14 Lieberman PH. Jones CR. Filippa DA. Langerhanscell
(eosinophilic) granulomatosis. J Invest Dermatol1980: 75: 71-2.
15 Averv ME. McAfee JG. Guild HG. The course andprognosis of
reticulo-endotheliosis (eosiniphilicgranuloma. Schuller-Christian
disease and Letterer-Siwe disease): a studv of fortv cases. Am J
Med 1957:22: 636-52.
16 Grosfeld JL. Fitzgerald JF, Wagner VM, Newton WA,Baehner RL.
Portal hypertension in infants andchildren with histiocytosis X. Am
J Surg 1976; 131:108-13.
17 Hampton AO. Case records of the MassachusettsGeneral
Hospital. N Engl J Med 1942; 226: 393-5.
18 Heitner R, Mouton S. Rabinowitz L, Rosen EU. Type1
histiocytosis X presenting as biliary atresia. A casereport. S Afr
Med J 1978; 53: 768-70.
19 LeBlanc A. Hadchouel M. Jehan P. Odievre M,Alagille D.
Obstructive jaundice in children withhistiocytosis X.
Gastroenterology 1981; 80: 134-9.
20 Parker JW. Lichtenstein L. Severe hepatic involvementin
chronic disseminated histiocytosis X. Report of acase with
necropsy. Am J Clin Pathol 1963; 40: 624-32.
21 Engelbreth-Holm J. Teilum G. Christensen E.Eosinophil
granuloma of bone - Schuller-Christian'sdisease. Acta Med Scand
1944; 118: 292-312.
22 Cutler B, Donaldson GA. Primary sclerosingcholangitis and
obliterative cholangitis. Am J Surg1969; 117: 502-1 1.
on April 3, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.25.5.526 on 1 M
ay 1984. Dow
nloaded from
http://gut.bmj.com/