Embed Size (px)
Citation preview

J Clin Pathol 1993;46:56-60
Inverted hyperplastic polyposis of the colon
N A Shepherd
AbstractAims: To describe and evaluate two appar-
ently unique cases of inverted hyper-plastic (metaplastic) polyposis of thecolon.Methods: The cases were analysed bystandard histopathological, histochemi-cal, and immunohistochemical techni-ques and the findings compared withthose of regular hyperplastic polyps of thecolorectum.Results: Both patients were middle-agedmen with concurrent adenocarcinoma ofthe proximal large intestine. The invertedpolyps numbered 18 and 12, measuredbetween 0 4 and 2*5 cm in diameter, andall were present in the proximal ascendingcolon. The polyps had characteristic mac-roscopic features: they were positioned onthe apex of mucosal folds and demon-strated surface pitting and mucus hyper-secretion. Histologically, inversion andmisplacement of hyperplastic epitheliumwas related to lymphoglandular com-
plexes. The polyps showed all the his-tochemical and immunohistochemicalfeatures of regular hyperplastic polyps.Conclusions: Inverted hyperplastic polypsare an unusual but distinctive polyp of theproximal colon, may be multiple, andshare the phenotypic changes of regularhyperplastic polyps. The pathogenesis ofepithelial inversion probably relates tomisplacement of epithelium through ana-
tomical defects in the muscular;s mucosaedue to mechanical forces. The polyps maymimic both adenomas and carcinomas.The neoplastic potential of invertedhyperplastic polyposis is likely to be very
low: one polyp only showed adenomatouschange.
(7 Clin Pathol 1993;46:56-60)
Department ofHistopathology,Gloucestershire RoyalHospital, GreatWestern Road,Gloucester, GL1 3NNN A ShepherdCorrespondence to:Dr N A ShepherdAccepted for publication13 July 1992
Hyperplastic (metaplastic) polyps are the com-monest polyp of the sigmoid colon and rectumin adults.' 2 Occasionally, multiple polyps are
present and in younger patients, particularlymen, the term hyperplastic (metaplastic) poly-posis has been applied.34 Hyperplastic polypsin the left colon and rectum are only very
occasionally associated with epithelial mis-placement or inversion of the epithelium intothe submucosa.' A distinctive form of invertedhyperplastic polyp has been described in whichepithelial misplacement was a characteristicfeature: the polyps were single, predominantlyin women, and concentrated in the rightcolon.'
Case reportsCASE 1
A 68 year old man presented with a threemonth history of anal bleeding and irondeficiency anaemia. There was no relevantmedical or family history. A barium enema andsubsequent colonoscopy demonstrated a cae-
cal tumour which was shown on biopsy to bean adenocarcinoma. There were two polyps,each 0 5 cm in diameter, in the distal colon:both were mildly dysplastic tubular adenomas.Elective right hemicolectomy was performed.The patient was followed up as an outpatientand remained well for nine months aftersurgery with no signs of tumour recurrence.
CASE 2
A 62 year old man presented as an emergencywith generalised abdominal pain, a high fever,and signs of small intestinal obstruction. Therewas no relevant medical or family history. Atemergency laparotomy a 5 cm appendicealmass was discovered with evidence of perfora-tion of the caecum and an acute generalisedperitonitis. There was extensive intraperitonealtumour spread. A palliative extended righthemicolectomy was performed with defunc-tioning ileostomy and mucus fistula. Despitethe extensive tumour, the patient remainedwell four months after surgery.
PathologyAll material was received fresh in the labo-ratory. Resection specimens were opened, pin-ned out on a corkboard, and fixed in 10%buffered formalin. Tissues were routinely pro-cessed through paraffin wax. Sections were cutat 4 ,um and stained with haematoxylin andeosin, periodic acid schiff, Perls's stain andhigh iron diamine alcian blue (HIDAB), thelatter according to the method of Spicer.6Sections were stained using the avidin-biotincomplex immunohistochemical method withthe monoclonal antibodies carcinoembryonicantigen (CEA: Dakopatts), IgA (a chain;Dakopatts), and secretory component (SC:ICRF, London). Sections with normal colonicmucosa, hyperplastic polyps, and carcinomaserved as positive controls. For negative con-
trols primary antibodies were excluded.
CASE 1
The right hemicolectomy comprised 2 cm ofterminal ileum, caecum with a 9 cm appendix,and 13 cm of ascending colon. Arising inthe caecum was an ulcerating tumour6-8 x 6-3 cm (fig 1). In the ascending colonwithin 8 cm of the ileocaecal valve were a total
56 on 16 A
ugust 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.46.1.56 on 1 January 1993. D
ownloaded from

Inverted hyperplastic polyposis
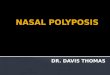
Figure 1 Case 1: theright hemicolectomyspecimen contains anulcerating tumour in thecaecum (below), a lipomain the proximal ascendingcolon (centre), andmultiple invertedhyperplastic polyps. Evenat this magnification thesurface puckering of thetwo largest polyps isevident.
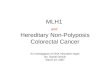
Figure 2 Case 2: three ofthe polyps from case 2. Thepolyps are paler than theadjacent mucosa withsurface pitting andpuckering. They areconsistently positioned onthe free edge of mucosalfolds.
4.
I.
of 12 polyps. They were all situated on thesurface of mucosal folds, orientated trans-versely and measured between 0 4 cm and2i4 cm (fig 1). The macroscopic appearancesof each polyp were similar: they appeared palerthan the adjacent mucosa and the surface ofthe polyp appeared pitted and puckered (fig 1).Several polyps showed evidence of mucus
hypersecretion, the surface being covered byviscid mucus. In the ascending colon imme-diately beyond the ileocaecal valve was a
submucosal lipoma 1-4 cm in diameter (fig1).
CASE 2
The specimen consisted of 11 cm of terminalileum, caecum with a 5 cm tumour massreplacing the appendix, and 55 cm of proximalcolon. The ileum appeared normal. The ileo-caecal valve showed lipohyperplasia. The entirecolonic serosa was covered by fibrinous exu-date with numerous small tumour nodules. Inthe proximal ascending colon were a total of 18polyps. These were transversely orientated onthe free edges ofmucosal folds. They measuredbetween 0 6 cm and 2 5 cm in diameter. Theyshowed very similar macroscopic appearancesto the polyps in specimen 1 (fig 2) with a pittedsurface and evidence of excessive mucus secre-tion. The polyps were strictly localised to theproximal 15 cm of the ascending colon andthere were no further mucosal lesions in themore distal colon.
Histological and histochemical findingsAll 30 polyps in both cases showed thearchitectural, cytological and proliferative fea-tures characteristic of hyperplastic polyp. Onepolyp in case 1 showed a focus of adenomatousepithelium with mild dysplasia adjacent tohyperplastic change, although despite serialsectioning, continuity could not be demon-strated. No other polyp showed such divergentfeatures. In all polyps there were exophyticcomponents characteristic of regular hyper-plastic polyp, but in addition all polyps of case2 and all but three of case 1 showed areas ofendophytic growth in which epithelium wasembedded in submucosal tissues deep to themuscularis mucosae. Some of these foci tookthe form of tubules with the characteristichyperproliferative basal region and serratedmaturing epithelium intimately mixed withsubmucosal connective tissues (figs 3 and 4).Other foci showed the same cellular contentbut the architecture was grossly distorted bymassive mucin hypersecretion and entrapmentwith the formation of submucosal mucin cysts(fig 5). Mucin hypersecretion was also evidentin the mucosal component of these polyps andresulted in a cap of haematoxyphilic mucin onthe surface of the polyp (fig 6). Apart from theone focus of tubular adenoma in a polyp ofcase 1, dysplastic features were entirely absent.In several foci of endophytic growth, partic-ularly those in which there was relatively earlyinversion, epithelial misplacement was clearlyrelated to lymphoglandular complexes (fig 3and 6).All inverted hyperplastic polyps showed the
same characteristic mucin histochemical andimmunohistochemical profile as that seen inclassic hyperplastic polyps.7-'Thus sialomucinwas strongly expressed (staining blue withHIDAB), and there was enhanced immunos-taining for CEA (fig 7) and diminished stainingfor SC and IgA in inverted hyperplastic polypscompared with normal colorectal mucosa.Haemosiderin was not demonstrated adjacentto any misplaced epithelium in the Perlspreparations. The presence of invasive adeno-carcinoma was confirmed in both cases. Thecaecal tumour of case 1 was a moderately
57 on 16 A
ugust 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.46.1.56 on 1 January 1993. D
ownloaded from

Shepherd
Figure 3 Case 1: an inverted hyperplastic polyp. Proliferative tubules are present withinthe submucosa. Part of a lymphoid follicle is present adjacent to the area of epithelialmisplacement, which is also seen within a lymphoid follicle (at left).
Figure 4 Case 1: theintimate associationbetween hyperplasticepithelial tubules andsubmucosalfatty tissues.
JFe,:r t: 3
+ jl s,
Jw . t 1:
B SR w.. t...fi....* , ,¢.?t'::
..^*._,. ,.lF': 4 :.
... {.K..
i..> .R>..;%go._ .:
_ .*
*[email protected] / * _ e- .: * as.^
_ - J X
*s t w' * wjS X * ilF¢3,P- .. /^S :::..t
g*9 sillt:
Wj¢t kY _Sa i'- *... :: . . . 0: .... - -.<S ' n.. .,.. z;; , f6F fujjijA 8
., J .,
differentiated Dukes B adenocarcinoma withextensive extramural venous spread but noevidence of spread to the peritoneal surface. Incase 2 the appendiceal tumour was a poorlydifferentiated adenocarcinoma, with evidenceof serosal pathology and transcoelomic spread.
DiscussionSobin's description of solitary inverted hyper-plastic polyps emphasises their right-sided
colonic preponderance, the predominance offemale patients, and their histological mimicryof both adenomas and carcinomas of thecolon.5 This study clearly shows that suchpolyps can be multiple and appear to bepredominantly situated in the proximalascending colon: in neither case was thereevidence of similar polyps in the more distalcolon. This study further shows a characteristicmacroscopic appearance with a puckered andpitted surface (presumably the result of under-lying epithelial misplacement), surface mucushypersecretion, and underlying mucous cysts.The latter feature parallels those of colitiscystica profunda in which epithelial misplace-ment in solitary ulcer syndrome and alliedconditions results in submucosal mucouscysts. '0In this study the inverted hyperplastic polyps
showed morphological, histochemical, andimmunohistochemical features identical withthose of regular hyperplastic polyps of the
791sigmoid colon and rectum. They appear torepresent the same dysmature and hyper-mature colonic mucosal lesion39 and, likeregular hyperplastic polyps, inverted hyper-plastic polyps are concentrated on the apices ofthe mucosal folds. The prime differencebetween regular hyperplastic polyps and theirright-sided equivalents is the frequency ofepithelial misplacement and mucus hyper-secretion. Another striking feature of theseascending colonic polyps is their relativelylarge size. Most regular hyperplastic polypsmeasure under 0 5 cm,3 while Sobin recordsexamples of inverted hyperplastic polyps meas-uring 1-5 cm in diameter,5 and in this studyseveral measured in excess of 2 cm. Could theinversion be solely the result of the size of thesepolyps?This is most unlikely as both small andlarge polyps showed the features of inversion inthis study and epithelial misplacement is not afeature of giant hyperplastic polyposis. "What is the cause of the epithelial inversion?
Epithelial misplacement is seen in severalsituations in polyps and other lesions of theintestines. Torsion with mucosal necrosis is thepathogenetic mechanism of epithelial mis-placement (pseudo-invasion) in pedunculatedadenomas, particularly of the sigmoid colon. 2The absence of haemosiderin in areas ofinversion argues against this mechanism as acause of epithelial misplacement in hyper-plastic polyps. Colitis cystica profunda insolitary ulcer syndrome of the rectum andother conditions in which mucosal prolapse isthe pathogenetic mechanism is the result ofmucosal erosion and regeneration.'° "'1 Suchinflammatory changes are not observed ininverted hyperplastic polyps. In Peutz-Jegherssyndrome up to 10% of small intestinal polypsshow epithelial misplacement. ' Obstructiveforces with intussusception lead to raisedintraluminal pressures and the likely result ofthis is that the excessive epithelium of thepolyps is forced through anatomical defects inthe wall of the intestine."' In inverted hyper-plastic polyps the epithelial misplacement isseen closely related to lymphoglandular com-plexes, structures which are associated with an
58
... 3F '
,,.,
on 16 August 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.46.1.56 on 1 January 1993. Dow
nloaded from

Inverted hyperplastic polyposis
Ar
0 tof01
iig
'V!~~~~~~'4# _ ...,.~ ~ ~
Figure S Case 2: a typical large submucosal mucin cyst.
Jej
4~~~~~~~~~~%-
Figure 6 Case 2: epithelial misplacement confined to an enlarged lymphoid folliclewithin the submucosa. Mucin hypersecretion is well seen both within the dilated misplacedepithelial glands and over the surface of the lesion.
anatomical defect in the muscularis muco-sae.16 Although lymphoglandular complexesare plentiful in the ascending colon, they arerelatively fewer in number here than in thedistal colon'6 and these alone cannot accountfor the preferential localisation of these lesionsto the ascending colon. Nevertheless, the mostfeasible mechanism for the development ofinverted hyperplastic polyps would seem to bemild traction forces, due to the presence of thelesions on the apices of the mucosal folds,leading not to mucosal erosion but to epithelialmisplacement through these pre-existingdefects in the muscularis mucosae.
Hyperplastic polyposis of the sigmoid colonand rectum is rare and its neoplastic potentialis a matter of controversy.3 4 17 Evidenceagainst significant carcinogenic potential ofhyperplastic polyposis is provided by the recentobservation of regression and disappearance ofhyperplastic polyposis after surgical removal ofrectal cancers, suggesting that the cancers wereresponsible for, and trophic to, the polyps.'8
Figure 7 Case 2: enhanced immunostaining for CEA isseen in the hyperplastic surface epithelium (upper left) andthe misplaced epithelium (below) compared with thenormal colonic mucosa (upper right) (CEAimmunohistochemistry).
Just one polyp in the cases under study showedadenomatous change. Such mixed hyperplas-tic-adenomatous polyps are thought to beassociated with malignant potential,'9 20 butnothing is known of the risk factors for thecondition.2' There is some evidence to suggestthat larger hyperplastic polyps are more likelyto show foci of dysplastic/adenomatous epithe-lium.7 Both cases in this study were associatedwith proximal large intestinal carcinomas butboth patients were within the expected agerange of such tumours and one at least had aconsiderably enhanced risk by having twodistal colonic adenomas. The inevitable con-clusion is that the malignant potential ofinverted hyperplastic polyposis is very low andprimarily relates to the presence or absence ofan associated adenomatous component.Can the term polyposis be justified for these
two cases? In general the term is reserved forsyndromes in which large numbers of polypsare present within the bowel. However, somepolyposis syndromes, in particular Peutz-Jeghers and juvenile polyposis, may be asso-ciated with relatively low numbers of polyps.Indeed, 10 or more polyps of the juvenile typeis an accepted definition for juvenile poly-posis." 2 Inverted hyperplastic polyposiswould seem an appropriate term, although it isrecognised that these polyps represent a dis-tinctive form of hyperplastic polyp with acharacteristic endophytic growth patternrather than a separate entity. The recognitionof the characteristic macroscopic and histo-logical features of these polyps will ensure that
59
on 16 August 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.46.1.56 on 1 January 1993. Dow
nloaded from

Shepherd
there is no confusion with other polyposissyndromes and will avoid erroneous diagnosesof adenoma and carcinoma of the proximalcolon.
1 Arthur JF. The structure and significance of metaplasticnodules in the rectal mucosa. Clin Pathol1968;21:735-43.
2 Goldman H, Ming S, Hickok DF. Nature and significanceof hyperplastic polyps of the human colon. Arch pathol1970;89:349-54.
3 Williams GT, Arthur JF, Bussey HJR, Morson BC. Meta-plastic polyps and polyposis of the colorectum. Histo-pathology 1980;4: 155-70.
4 Bengoechea 0, Martinez-Penuela JM, Larrinaga B, ValerdiJ, Borda F. Hyperplastic polyposis of the colorectum andadenocarcinoma in a 24 year old man. Am Surg Pathol1987;11:323-7.
5 Sobin LH. Inverted hyperplastic polyps of the colon. AmSurg Pathol 1985;9:265-72.
6 Spicer SS. The use of various cationic reagents in his-tochemical differentiation of mucopolysaccharides. Am JClin Pathol 1961;5:393-407.
7 Franzin G, Zamboni G, Scarpa A, Dina R, lannucci A,Novelli P. Hyperplastic (metaplastic) polyps of the colon.A histological and histochemical study. Am J Surg Pathol1984;8:687-98.
8 Jass JR, Faludy J. Immunohistochemical demonstration ofIgA and secretory component in relation to epithelial celldifferentiation in normal colorectal mucosa and meta-plastic polyp: a semiquantitative study. Histochem1985;17:373-80.
9 Jass JR, Filipe MI, Abbas S, Wilson Y, Lovell D. Amorphologic and histochemical study of metaplasticpolyps of the colorectum. Cancer 1984;53:510-15.
10 Wayte DM, Elwig EB. Colitis cystica profunda. Am J ClinPathol 1967;48: 159-69.
11 Summer HW, Wasserman NF, McClain CJ. Giant hyper-
plastic polyposis of the colon. Dig Dits Sci 1981;26:85-9.12 Muto T, Bussey HJR, Morson BC. Pseudocarcinomatous
invasion in adenomatous polyps of the colon and rectum.J Clin Pathol 1973;26:25-31.
13 du Boulay CEH, Fairbrother J, Isaacson PG. Mucosalprolapse syndrome - a unifying concept for solitary ulcersyndrome and allied conditions. J Clin Pathol 1983;36:1264-8.
14 Madigan MR, Morson BC. Solitary ulcer of the rectum.Gut 1969;19:871-8.
15 Shepherd NA, Bussey HJR, Jass JR. Epithelial misplace-ment in Peutz-Jeghers polyps: a diagnostic pitfall. Am JSurg Pathol 1987;11:743-9.
16 O'Leary AD, Sweeney EC. Lympho-glandular complexes ofthe colon: structure and distribution. Histopathology1986;10:267-84.
17 Cappell MS, Forde KA. Spatial clustering of multiplehyperplastic, adenomatous and malignant colonic polypsin individual patients. Dis Colon Rectum 1989;32:641-52.
18 Kusunoki M, Fujita S, Sakanoue Y, et al. Disappearance ofhyperplastic polyposis after resection of rectal cancer. DisColon Rectum 199 1;34:829-31.
19 Cooper HS, Patchefsky AS, Marks G. Adenomatous andcarcinomatous changes within hyperplastic colonic epi-thelium. Dis Colon Rectum 1979;22:152-6.
20 Gebbers J-O, Laissue JA. Mixed hyperplastic and neoplasticpolyp of the colon. An immunohistological study. VirchowsArch 1986;410:189-94.
21 Fenoglio-Preiser CM, Lantz PE, Listrom MB, Davis M,Rilke FO. Polyposis In:Gastrointestinal pathology. An atlasand text. NewYork: Raven Press, 1989:503.
22 Sachatello CR, Hahn IS, Carrington CB. Juvenile gastro-intestinal polyposis in a female infant. Report of a caseand review of the literature of a recently recognisedsyndrome. Surgery 1974;75:107-13.
23 Shepherd NA, Bussey HJR. Polyposis syndromes - anupdate. In: Williams GT, ed. Current topics in pathology.Gastrointestinal Pathology. Berlin: Springer-Verlag,1990:323-52.
60
on 16 August 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.46.1.56 on 1 January 1993. Dow
nloaded from