-
8/12/2019 Neonatal Chole Stasis
1/23
Neonatal Cholestasis
Jenny Bergquist, M.D.August 5, 2005
-
8/12/2019 Neonatal Chole Stasis
2/23
Definition: Neonatal Cholestasis
Prolonged conjugated hyperbilirubinemia
in the newborn period
Conjugated hyperbilirubinemia
Conjugated bilirubin >1mg/dL if TB < 5mg/dL >20% Total
Bilirubin if TB is >5 mg/dL
Caused by a group of hepatobiliary
diseases occuring within the first 3 monthsof life
Occurs in 1:2500 live births
-
8/12/2019 Neonatal Chole Stasis
3/23
Neonatal Cholestasis
NASPGHAN Recommendations Evaluate infants with jaundice at the
2
week visit Up to 15% of infants are jaundiced at 2 weeks,the
majority due to breast milk jaundice
Timely and accurate diagnosis is crucial forsuccessful treatment
and favorable prognosis
Breast-fed infants may have an evaluationdelayed until 3 weeks
if: Normal exam
No h/o dark urine or light stools
Reliably monitored
-
8/12/2019 Neonatal Chole Stasis
4/23
Differential Diagnosis:
Obstructive Cholestasis Biliary Atresia
* accounts for 30% of all cases of neonatalcholestasis
Choledochal cysts
Gallstones
Alagille syndrome
Neonatal sclerosing cholangitis Cystic fibrosis
Tumor
-
8/12/2019 Neonatal Chole Stasis
5/23
Differential Diagnosis:
Hepatocellular Cholestasis Idiopathic neonatal hepatitis
Diagnosis based on liver biopsy findings: giant cell
hepatitis
Was thought to account for ~40% of neonatal cholestasis(with new
diagnostic techniques, % is probably ~10-20%)
60-70% resolve without sequelae
Infectious
Viral: TORCH, CMV, HIV, viral hepatitis Bacterial: sepsis,
syphilis, UTI
Genetic/metabolic
Alpha-1-antitrysin deficiency, galactosemia, tyrosinemia,
hypothyroid, PFIC, CF Toxic/secondary causes
TPN associated cholestasis
-
8/12/2019 Neonatal Chole Stasis
6/23
History Congenital infections
Prenatal ultrasound ABO incompatibility
Neonatal infection
UTI Dietary history
Weight gain
vomiting
Stool pattern
Delayed: CF,hypothyroid
Diarrhea: infx,metabolic disease
Stool and urine color Excessive bleeding
Irritability or lethargy
+family history
-
8/12/2019 Neonatal Chole Stasis
7/23
Physical Exam Weight measurement
General appearance
Ill-appearing: infection, metabolic disease Well-appearing:
biliary atresia
Fundoscopic exam (congenital infection)
Cardiac murmur
Abdominal exam Ascites, abd wall veins, liver, spleen
Stool/urine for color
Skin exam Bruising, petechiae
Dysmorphic features
Broad nasal bridge, triangular facies, deep set eyes
(Alagille)
-
8/12/2019 Neonatal Chole Stasis
8/23
Laboratory Studies Total and direct bilirubin
LFTs + GGTP
Detects liver cell or bile duct injury PT/PTT, glucose,
albumin
Assessment of biosynthetic capacity of liver
CBC, urine and blood culture
Viral serologies
(TORCH infections + HBsAg, CMV, HIV if indicated)
UA for reducing substances
TFTs Alpha-1-antitrypsin
Sweat chloride or mutation analysis for CF gene
-
8/12/2019 Neonatal Chole Stasis
9/23
NASPGHAN Recommendations:
Imaging Studies Ultrasound: initial study recommended
for patients with cholestasis of unknownetiology Evaluates for
anatomic abnormalities
Liver Biopsy Recommended for mostinfants with
cholestasis of unknown etiology Differentiates b/w extra and
intrahepatic processes,
disorders of physiology from anatomy and candetermine need for
surgical vs. medical intervention
Scintigraphy (HIDA), ERCP, MRCP
-
8/12/2019 Neonatal Chole Stasis
10/23
Biliary Atresia 1:8,000-15,000 live births
Accounts for 30% of all cases ofcholestasis in infants
Female>Male
Asians>African Americans>Caucasian Most frequent cause of
chronic end-stage
liver disease in children
Leading indication for liver transplantationin the pediatric
population (40-50% of allliver transplants)
-
8/12/2019 Neonatal Chole Stasis
11/23
Biliary Atresia: pathogenesis Bile duct obstruction due to
inflammation
and fibrous obliteration Perinatal or classic type (70-85%):
obstruction begins afterbirth. Signs/symptomsdevelop within ~2-4
weeks of age. No
associated abnormalities Embryonic type (15-30%):
obstructive
process begins in utero. Cholestatic symptoms
present at birth. Associated with congenitalanomalies: Situs
inversus, polysplenia, malrotation, cardiac
anomalies
Unknown etiology: genetic, viral and hostimmune factors have
been postulated
-
8/12/2019 Neonatal Chole Stasis
12/23
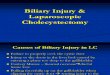
Variations in Biliary Atresia
http://www.emedicine.com/cgi-bin/foxweb.exe/makezoom@/em/makezoom?picture=\websites\emedicine\ped\images\Large\2780Figure1.jpg&template=izoom2
-
8/12/2019 Neonatal Chole Stasis
13/23
Clinical Features History: Variable degrees of persistent
jaundice,
dark urine, light colored stools, +/-poor appetite
* Usually W e l l - A p p e a r i n g * Physical:
Hepatomegaly, +/- splenomegaly appear well-nourised
Usually with decreased fat stores and lean body mass Enlarged
abdomen from HSM may give impression ofnormal weight for age
Scleral icterus, abdominal wall veins (caput medusa)
Labs: Total bilirubin rarely is >12mg/dL; CB is usually
-
8/12/2019 Neonatal Chole Stasis
14/23
Imaging Studies Ultrasound
Absent gallbladder, triangular cord sign Low sensitivity;
operator dependent Evaluates for other anatomic abnormalities
Hepatobiliary scintigraphy (HIDA) High sensitivity: normal
uptake, but no excretion of
radionuclide tracer into biliary system or bowel in virtually
all
patients with BA (exceptions in very early disease) However,
failure of excretion may be seen in both BA and
neonatal hepatitis Sensitivity and Specificity increase with
phenobarbital
administration
ERCP Invasive, not readily available, technically difficult in
infants Intraoperative use is most common to confirm diagnosis
and
document site of obstruction
MRCP May become an important tool for diagnosis Further studies
are required
-
8/12/2019 Neonatal Chole Stasis
15/23
Triangular Cord Sign
-
8/12/2019 Neonatal Chole Stasis
16/23
Diagnosis Percutaneous Liver Biopsy: most reliable test
for diagnosing biliary atresia
Biopsy interpretation is pathologist dependent
Accurate diagnosis made in 90-95% of cases
Liver biopsies made early in the course of disease (
-
8/12/2019 Neonatal Chole Stasis
17/23
Surgical Management Kasai Procedure: resection of the
obliterated bile duct w/ creation of aRoux-n-Y
hepatoportoenterostomy
Timing of procedure predicts the
prognosis 90 days- bile flow returned in ~20% cases Usually
require a liver transplant within one year
The experience of the centerperforming the Kasai if one of the
mostimportant factors determinig surgicaloutcome
-
8/12/2019 Neonatal Chole Stasis
18/23
-
8/12/2019 Neonatal Chole Stasis
19/23
Post-operative Management Prophylactic Abx to prevent
cholangitis
Ursodiol: enhance bile flow No special diet needed unless
concern
with poor bile drainageMCT formula
(ie Alimentum, Pregestimil)
Fat-soluble vitamins: A, D, E, K
+/- short term, high dose steroid therapy
-
8/12/2019 Neonatal Chole Stasis
20/23
If Kasai Fails?
+/- support for revision of Kasai procedure if fails
Despite clinical improvement after a Kasai, 70-80% pts
willeventually require liver transplantation
Indications for Liver Transplant:
operation not successful in restoring bile flow initially(~20%)
late referrals (generally >120 days) develop end-stage liver dz
despite bile drainage (ie
portal htn, recurrent cholangitis, ascites, growth failure)
Liver Transplant results: one-yr survival rates >90% b/c
reduced size allografts
and living-related donors
-
8/12/2019 Neonatal Chole Stasis
21/23
Post-Kasai Complications Early: Ascending Cholangitis (50%) can
lead to
ongoing bile duct injury & re-obstruction
fever, dec. bile secretion, worsening jaundice,leukocytosis
Late: Portal Hypertension
bleeding esophageal varices, ascites,
hypoalbuminemia,fat-soluble vit def., malabsorbtion of
long-chaintriglycerides, encephalopathy
Long term, malignancies screened for Hepatoblastoma,
hepatocarcinoma, cholangiocarcinoma
-
8/12/2019 Neonatal Chole Stasis
22/23
What happened to our patient? Kasai Procedure on 8/16/04
Complicated by cholangitis x 2 wks Portal hypertension
Esophogeal varicessclerotherapy x 2
1/05: TB 32.3/ conjugated bilirubin 18.6
Now on the transplant list awaiting a
liver
-
8/12/2019 Neonatal Chole Stasis
23/23
Take-Home Message! Any Jaundice>2 weeks requires
investigation
ALWAYS ask for fractionated bilirubin
(Total + Direct bilirubin)
Early diagnosis and referral (