Embed Size (px)
Citation preview

ASHNHA February–March 2012 1
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
ASHNHA FEBRUARY 2012
Care Closer to Home makes sure Veterans’ needs are front and center
Alaska Stat e Hosp ital and Nurs ing Homes As soc iat ion
Inside this issue:
Getting Healthy Sleep 2
Hospitals join forces for advanced nurse training 3
State moves on Health Exchange 4
Hospitals Connect eICUs 4
Meet Sara Bloom 5
News from DBH 6
Heffern tracks health care reform 8 Report: Hospitals fuel jobs 8
The State is seeking
a firm to develop a
Patient Center
Medical Homes
model strategy for
Medicaid program.
It expects to issue a
$300,000 one-year
contract in March.
Winter Meeting
Feb. 29-March 1,
Juneau
PRESIDENT’S REPORT / KAREN PERDUE
I t may be as simple as wanting a home-cooked meal, or as important as keeping one’s job. Perhaps it’s wanting to keep the driveway clear and the pipes from freezing at
home. Or just being happier staying busy in familiar surroundings instead of feeling iso-lated through separation. Whatever the personal reason, Alaska Veterans have more options to stay in Alaska for care thanks to the Care Closer to Home Program. And they’ve been doing so in record numbers. Since the Alaska VA Health System (AVAHS) initi-ated the program last year, out-of-state referrals have been reduced by half. The AVAHS provides health care to Alaska Veterans through a series of clinics located in Anchorage, Fairbanks, Kenai, Homer, Wasilla, and Juneau. Access to VA care for Alaska’s Veterans is excellent, with over 89% of enrolled Veterans residing in a Borough or Census Area that is home to an AVAHS clinic with primary care and primary mental health care. The AVAHS is a member of the Alaska Federal Health-care Partnership, and is a partner in the nationally recog-nized VA/DoD Joint Venture with the 673rd Medical Group on Joint Base Elmendorf-Richardson in Anchorage. If care is not available in an AVAHS facility or through a partner facility in Alaska, it is either pur-chased in the community or provided via referral to a VA facility elsewhere. The AVAHS initiated the “Care Closer to Home” program in May 2011. In consultation with individual Veterans, we sought to decrease the need to travel out of state for care. And we’re succeeding. In fiscal year 2009, the AVAHS offered out of state care to 591 Veterans and 545 in fiscal year 2010. Since initiating Care Closer to Home, 299 Veterans actually traveled for care in fiscal year 2011, 43% fewer than in fiscal year 2009. (Cont. p. 9.)
February-March 2012
Alex Spector, Director Anchorage VA Medical &
Regional Office Center
“We are glad to offer this opportunity to Alaska’s veterans to receive care
locally. Thank you to ASHNHA members for making the transition go so
smoothly.” Director Alex Spector

ASHNHA February–March 2012 2
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
Korbrien knows the value of a good night’s sleep
Andrew Korbel of Korbrien Medical Management believes in sleeping on the job. Or rather, his mission is to promote the quality delivery of sleep medicine so we don’t sleep on the job. Poor sleep is as bad for our health as poor nutrition and lack of exercise. Sleep is an active state. A body function central to every other system in the body. This is revealed in the co-morbidities of sleep disorders, such as 83% of patients with drug resistant hypertension, 77% of obese patients, 76% with congestive heart failure, 59% of patients with a pacemaker , 49% of patients with a trial fibrillation, and 48% of patients with diabetes*.
Improving sleep is Korbrien’s focus.
Kobrien Medical Management, based in Homer and Anchorage, is ASHNHA’s newest Associ-ate member. Working mostly with small and medium-sized hospitals, the company is an ex-pert in setting up sleep clinics and making them operational, administering the service as they do in several Alaska sites, or simply providing professional consultation and evaluation. The company is owned by Andrew Korbel and Dee O’Brien who together have 20 years of experience in setting up and managing Sleep Centers.
After a stint in the Marine Corps, Andrew earned his lab certification in 2001 in Austin, Texas, and began National Sleep Centers. The company, specializing in setting up sleep labo-ratories in rural hospitals, was the first in Austin to attain accreditation by the American Academy of Sleep Medicine.
Dee is a certified respiratory therapist, registered polysomnographic technician, and regis-tered sleep technician based on Homer. She began her career in sleep medicine in 2004 working for National Sleep Centers in Austin, Texas, performing nighttime sleep studies for
National Sleep Centers in satellite labs in three sites. She transitioned to Vice President of Lab Operations –managing 13 labs across Texas and Oklahoma.
Sleep medicine is an evolving field, with uneven quality and minimal national standards. There are roughly five physicians in Alaska boarded in Sleep Medi-cine. Korbrien’s focus is to ensure quality and consistency in sleep evaluations based on national standards. They work with existing sleep labs to improve technical skills or to set up a sleep lab at virtually no cost to the facility either on a permanent basis or quarterly until the operation is running smoothly.
“It’s a common misconception we encounter from hospital administrators,” Andrew says. “We can set up a full time or ‘on-demand’ sleep center, at no cost, for any facility with unused rooms. The ‘on-demand’ service is perfect for rural locations that might only need 6 sleep studies a month. The hospital pays a flat rate for the service, and bills the patient’s insurance as they would for any other outpatient diagnostic.”
South Peninsula Hospital was already performing about five sleep studies a month when the facility contracted with Korbrien to improve the sleep center’s performance. Registered sleep therapists and new diagnostic systems were brought in to improve quality and performance. Now referring physicians have increased confidence in the system and the center performs in excess of 20 sleep studies a month.
What’s ahead for sleep medicine? Home sleep studies for patients with limited co-morbidities are being embraced as a less expensive alternative- often 1/3 the cost of facility based tests. Payers such as Premera Blue Cross in Alaska will be paying for home studies for appropriate patients. For more information, contact Andrew Korbel at [email protected].
Andrew Korbel, RPSGT
Dee O’Brien, CRT, RPSGT
*References: 1. Logan at al. High prevalence of unrecognized sleep apnoea in drug-resistant hypertension. J Hypertens 2001;19:2271-2277, 2. O’Keeffe & Patterson. Evidence of supporting routine polysomnography before bariatric surgery. Obes Surg 2004; 3. Oldenburg et al. Sleep-disordered breathing in patients with symptomatic heart failure: a contemporary study of prevalence in and characteristics of 700 patients. Eur J Heart Fail 2007;9:251-257; 4. Garrigue et al. High prevalence of sleep apnea syndrome in patients with long-term pacing, the European multicenter polysomnographic study. Circulation. 2007;15:1-7; 5. Gami et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;1104:364-367; 6. Einhorn et al. Prevalence of sleep apnea in population of adults with type 2 diabetes mellitus. Endocr Pract 2007;13:355-362

ASHNHA February–March 2012 3
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
Hospitals join forces to train nurses
F acing a shortage of qualified perioperative nurses in Alaska,
six hospitals (see right) formed the Alaska Perioperative Nursing Con-sortium (APNC) to deliver advanced training and professional develop-ment for specialty nurses. Working together, they developed a training program based on an emerging best practice model of the NorthWest Pe-rioperative Consortium. Each facility sponsored students—some of whom were already working at their facili-ties in other capacities—for 17 weeks of training. Barbara Welte of Providence, and Jamie Britton of Fairbanks Memorial Hospital, are lead educators. Each nurse educator has assumed a portion of the teaching responsibilities and planning. Other nurse educators are: Peggy Robinson and Gail Augdahl (Alaska Regional) Merisue Bowerfind and Amber Nakazawa (Alaska Native Medical Center). Bartlett Regional Hospital’s Diane Bigge has assumed the responsibility for the preceptor training component of the pro-gram. APNC commended Tracey Jones and Diana Frawley, who came to Alaska to help the consortium with the feasibility study, for being such tremendous resources in support of Alaska’s efforts.
APNC welcomed 15 students and 6 Perioperative Nurse Educators on Monday, Feb; 13, the first day of a 17 week
Perioperative Nurse training. Graduation is in June.
Alaska Native Medical
Center
Alaska Providence Medical Center
Alaska Regional
Hospital
Bartlett Regional Hospital
Fairbanks Memorial
Hospital
PeaceHealth Ketchikan Medical Center
Consortium Members
Friends in Cordova (upper left) and Valdez (bottom right) shared their winter woes with us in pictures.
For Cordova and Valdez, spring can’t
come too soon

ASHNHA February–March 2012 4
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
J uneau and Anchorage share a life-saving connection. On Feb. 14, 2012, Bartlett Hospital formed a life-saving partner-ship with Providence’s Electronic Care Unit (eICU) to provide additional around the
clock monitoring for critically ill patients. The eICU electronically ties Bartlett’s Critical Care unit to the eICU at Providence Alaska Medical Center through a patient monitor-ing system using 21st century telemedicine to help care for critically ill patients in mul-tiple hospitals from a single location. At the eICU, experienced critical care specialists continuously monitor patients’ vital signs, medications, test results and other data, and alert clinical staff at the bedside to potential problems before they occur and guide interventions. Through this partnership, Bartlett Regional Hospital’s patients have 24-hour electronic access to critical care specialists working jointly with local physicians and nurses to improve quality care for critically ill patients with two-way audio/video, real time bed-side support, vital signs monitoring, lab and medication review, and more.
Bartlett’s Director of Critical Care, Nancy White, believes the eICU will allow more pa-tients who would normally have to be transported to receive care on-site, with the comfort of family, friends and community nearby. Patients also won’t have to bear the high cost being evacuated, where charges can range from $46,000 to $120,000 depending on carrier and destination. Family mem-bers will not have to pay the high cost of airfare, lodging, meals, loss of work, etc., to accompany the patient to another facility. Bartlett’s patients do not have to pay extra for the eICU service. The Providence eICU system connects Providence Alaska Medical Center in Anchor-age, Providence Kodiak Island Medical Center, and Providence Seaside Hospital in Seaside, Oregon, and now Bartlett Regional Hospital in Juneau.
Bartlett & Providence connect for long distance care
ASHNHA WINTER MEETING February 29 - March 1, 2012
Legislative Briefing Lunch
ASHNHA overview with Sen. HSS Committee
Breakfast with Commissioner Bill Streur and Commissioner Becky Hultberg
Reception at the Governor’s Mansion
Alex Spector on a new VA initiative
ASHNHA overview to the House HSS Committee
Dr. Ward Hurlburt on public health challenges
Baranof Hotel, Juneau For Reservations, call:
Westmark Reservation Line @ 800-544-0970
Nurse Liesl Bland and patient
Providing around the clock care
State takes step toward Health
Insurance Exchange
The State of Alaska has hired Public Consulting Group (PGC) to recommend a viable plan for devel-oping and sustaining a Health Insurance Exchange in Alaska. PGC is currently advising 13 other states on health care reform planning. They will produce an integrated planning document of alternatives, cost estimates, timelines and recom-mendations for implementing and sustaining an Exchange in Alaska, while keeping in mind that the State of Alaska has taken the position that the indi-vidual mandate component of Health Care Reform is unconstitutional. PGC began work Jan. 1, 2012, on the one-year pro-ject. States have until January 1, 2013, to submit their
exchange plans to the federal government or risk hav-
ing the federal government do it for them. The deadline
for the exchanges to be working is Jan. 1, 2014.

ASHNHA February–March 2012 5
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
What is your title for ASHNHA and what do you do? Office Manager. I provide support to Karen Perdue: keep her calendar, make her travel ar-rangements, submit invoices and payroll to the accountant, work with vendors, prepare meet-ing materials for board meetings, write the minutes for the Executive Committee, order food for meetings, stock supplies. Where were you born? New York City What's the last movie you watched? The last good movie I [saw was] an independent called Another Year. What book are you currently reading? I just finished rereading Jane Eyre. What do you like most about your job? My autonomy. What's the most unusual job you've ever had? I briefly worked for a Christmas Tree farm in San Diego. How would you describe your work style? Self-management—as long as I know what needs to be done, I can budget my time accordingly. Tell us something about yourself that we'd be surprised to learn. I have a master’s degree in landscape architecture. What makes you tick? I love to make quilts and spend time out on the trails walking with my dogs.
Meet ASHNHA’s Sara Bloom
Best wishes to Robert Letson & Bride Cristol
Wedding Bells

ASHNHA February–March 2012 6
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
Note: This is an update from the Division of Behavioral Health’s Randall Burns, who manages the mental health emergency services for the State. ASHNHA will be starting a mental health committee in March. If you are interested in receiving updates or participating in the committee, please email [email protected] or Andrew Mayo at [email protected].
N o doubt many of you have noticed that, compared to last winter, the census pressures on API have been minimal with respect to their acute care units. This has meant that unlike last year at this time (see the chart below for 2/15/12),
or in December and January of last year, your hospital emergency departments have not been filling up with behavioral health patients awaiting transfer to API or another evaluation site (a DET – designated evaluation and treatment site, like Fairbanks Memorial Hospital or Bartlett Regional Hospital).
API still has real pressures on its forensic and adolescent units (both just 10 beds and essentially always at capacity), but its larger two acute care units (25 beds each) have rarely been even half full over this winter season. This has meant that the state’s behavioral health crisis intervention system has been able to function relatively well in terms of getting patients to API more efficiently and quickly.
Substantially Revised Civil Commitment Court Forms Now in Use
This has been good news for all concerned, especially because of changes that have occurred to Alaska’s civil commitment procedures as a result of changes to the Alaska Court System’s involuntary commitment forms.
These changes came about because of pressure on the State’s emergency behavioral health (BH) delivery system from an Alaska Supreme Court case that has yet to be decided, but has been argued, and a lawsuit filed by the Disability Law Center (DLC) against the Alaska Department of Health & Social Services (DHSS). The DLC case was argued in June of last year and mostly decided on in December, although the case remains open in some regards.
As a result of these legal matters, DHSS / DBH decided to sit down with the DLC, the Alaska Public Defender Agency (PDA), the Alaska Court System (ACS), and the Alaska Department of Law (DOL) to see if we could find some solutions to the is-sues identified in the court cases and by the parties involved in providing services to the mentally ill.
A Status Report to the Court Now Required for Patients Not Transferred from EDs and Jails within 24 Hours
One of the major changes agreed to over almost a year’s worth of work, was a requirement in the Court’s REVISED Involun-tary Commitment Order that the State has to provide a status report to both the Court and the Public Defender if it appears likely that a patient is going to end up spending more than 24 hours in an ED bed or a jail cell because of difficulties trans-ferring that patient to a DET or DES* hospital for a court-ordered involuntary mental health evaluation. (Cont. p7.)
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
105%
1-F
eb
2-F
eb
3-F
eb
4-F
eb
5-F
eb
6-F
eb
7-F
eb
8-F
eb
9-F
eb
10-F
eb
11-F
eb
12-F
eb
13-F
eb
14-F
eb
15-F
eb
16-F
eb
17-F
eb
18-F
eb
19-F
eb
20-F
eb
21-F
eb
22-F
eb
23-F
eb
24-F
eb
25-F
eb
26-F
eb
27-F
eb
28-F
eb
API Midnight Census as a Percentage of Total Occupancy -A One Month Comparison
API 2011 API 2012 Maximum Capacity
80 Beds
News from the Division of Behavioral Health By Randall Burns

ASHNHA February–March 2012 7
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
(Cont. from p. 6) This is a “rolling” 24-hour notice re-quirement, meaning that every 24 hours until the pa-tient actually arrives at API or the DET or DES site, the State/ DHSS/DBH is required to inform both the court that issued the commitment order and the PDA of the patient’s status and whether and why (s)he may still be awaiting a transfer, and what (additional) efforts are being made to comply with / expedite the commitment order.
DBH is Gathering Data Regarding How the Emergency Services System is Functioning
While we understand, because of API’s ample adult acute bed availability, that Alaska hospitals, and espe-cially Alaska hospital Emergency Departments, are not nearly as pressured as last winter, we are very inter-ested in hearing from both the hospital Administrator/ CEO and the head of those EDs that were so impacted last winter, regarding your facility’s leadership regard-ing the State’s behavioral health emergency/crisis in-tervention system.
To that end, as some of you are aware, the Division hired researchers from UAA’s Center for Behavioral Health Research & Services (CBHRS) to update an earlier study of API admission and discharge practices, as well as to look at whether there was value in the data from some other existing databases, including the Providence Psychiatric Emergency Room (PPER), the ASHNHA / DHSS hospital database (including the available outpatient data), and the State’s AKAIMS database (collecting data on the clinical activities of the State’s many comprehensive behavioral health center grantees).
The UAA Center is developing a set of key informant interview questions for the leadership (administrative and clini-cal) of the various providers active in the State’s behavioral health emergency response system, including hospitals and BH centers.
The Division looks forward to your participation. The results of this qualitative portion of the Center’s work will be available (without attribution) by late summer.
DBH Wants to Hear from Hospital Leadership
As important stakeholders, we wanted to let hospital administrators and ED directors know that they may soon be hearing from Center staff asking to set up an appointment for a key informant interview.
The responses to these set questions will be codified and de-identified and compiled as a part of the Center’s qualitative portion of their research into API and its impact on the State’s statewide emergency services system.
We have provided this article for use in the ASHNHA newsletter in order to apprise you in advance of this upcoming interview process and to specifically and respectfully request your hospital’s cooperation with CBHRS staff, should they call your office.
Although a specific number of key informants have been selected, mostly from those hospitals we know from experi-ence and data send the most patients to API (or the other DET or DES sites), if any hospital administrator or ED director wishes to be sure that they are interviewed, please send me an email or give me a call and we will be sure that you are called.
The Division looks forward to your participation. The results of this qualitative portion of the Center’s work will be available by late summer.
Randall Burns can be contacted by telephone at 907.269.5948, or via email at [email protected].
ASHNHA
2012 Legislative Priorities
We support:
Full funding for Medicaid
Additional funding for trauma designation
Psychiatric Residency Funding
HB 78 Providing for incentive payments of
loan repayments to health care providers
Workforce Development Funding
Senate Bill 5 Expansion of Denali Kid Care
to 200% of poverty level
Anchorage Tribal Nursing Home

ASHNHA February–March 2012 8
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
With the US Supreme Court set to hear oral arguments on the Affordable Health Care Act in March, things are moving fast. Sandra Heffern is working with the Alaska Health Reform Coalition and is keeping her finger on health reform. Sandra has worked on health and human service issues in Alaska for more than 30 years. She will track and synthesize the changes for ASHNHA and its partner organizations, along with in-depth analysis of perti-nent topics. In her prior life as CEO and owner of EHD Enterprises, Sandra assisted health and human ser-vice organizations focus on system analysis and design, advocacy and organizational capacity building. She is the founder of Job Ready, an Anchorage-based company that assisted indi-viduals with disabilities in the community. Sandra has a Master’s degree in rehabilitation ad-ministration from the University of San Francisco. Like most Alaskans, when Sandra is not having fun working at something she loves, she is playing in Alaska’s great outdoors. She has a cabin in the woods, enjoys snow machining, fish-ing (as long as someone else baits her hook), and hiking. As soon-to-be Chair of the Anchor-age Chamber of Commerce, Sandra looks forward to the commissioning of the USS Anchorage in September. Sandra lives in Anchorage with her family, including two school-age children.
Sandra Heffern tracks health care reform
Alaska’s Hospitals & Nursing Homes provide good jobs, fuel economic growth
ASHNHA’s 2012 Report on Hospitals & Nursing Homes in Alaska is now available online (www.ashnha.com). The document is get-ting good reviews from legislators and policy makers. It summa-rizes the employment picture, rural challenges of care delivery, uncompensated care and cost issues.
ASHNHA February–March 2012 9
ANCHORAGE 943 West 6th Avenue, Anchorage, AK 99501 tel 907.646.1444 JUNEAU 426 Main Street, Juneau, AK 99801 tel 907.586.1790 www.ashnha.com
(Cont. from p. 1)
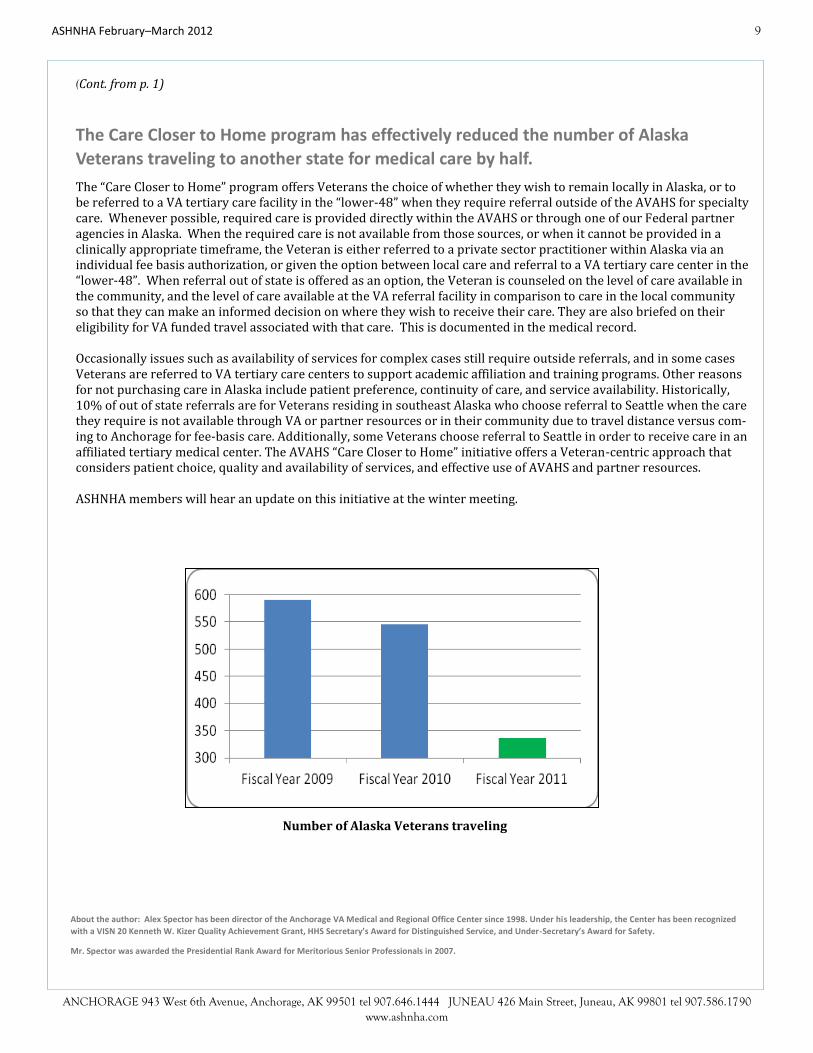
The Care Closer to Home program has effectively reduced the number of Alaska
Veterans traveling to another state for medical care by half.
The “Care Closer to Home” program offers Veterans the choice of whether they wish to remain locally in Alaska, or to be referred to a VA tertiary care facility in the “lower-48” when they require referral outside of the AVAHS for specialty care. Whenever possible, required care is provided directly within the AVAHS or through one of our Federal partner agencies in Alaska. When the required care is not available from those sources, or when it cannot be provided in a clinically appropriate timeframe, the Veteran is either referred to a private sector practitioner within Alaska via an individual fee basis authorization, or given the option between local care and referral to a VA tertiary care center in the “lower-48”. When referral out of state is offered as an option, the Veteran is counseled on the level of care available in the community, and the level of care available at the VA referral facility in comparison to care in the local community so that they can make an informed decision on where they wish to receive their care. They are also briefed on their eligibility for VA funded travel associated with that care. This is documented in the medical record. Occasionally issues such as availability of services for complex cases still require outside referrals, and in some cases Veterans are referred to VA tertiary care centers to support academic affiliation and training programs. Other reasons for not purchasing care in Alaska include patient preference, continuity of care, and service availability. Historically, 10% of out of state referrals are for Veterans residing in southeast Alaska who choose referral to Seattle when the care they require is not available through VA or partner resources or in their community due to travel distance versus com-ing to Anchorage for fee-basis care. Additionally, some Veterans choose referral to Seattle in order to receive care in an affiliated tertiary medical center. The AVAHS “Care Closer to Home” initiative offers a Veteran-centric approach that considers patient choice, quality and availability of services, and effective use of AVAHS and partner resources. ASHNHA members will hear an update on this initiative at the winter meeting.
About the author: Alex Spector has been director of the Anchorage VA Medical and Regional Office Center since 1998. Under his leadership, the Center has been recognized
with a VISN 20 Kenneth W. Kizer Quality Achievement Grant, HHS Secretary’s Award for Distinguished Service, and Under-Secretary’s Award for Safety.
Mr. Spector was awarded the Presidential Rank Award for Meritorious Senior Professionals in 2007.
Number of Alaska Veterans traveling