Embed Size (px)
Citation preview
Cardivascular Causes of Sudden
Infant DeathAlpay Çeliker M.D.
Hacettepe University Pediatric Cardiology
DepartmentAnkara, Türkiye
Sudden Infant Death Syndrome
• Unexplained, unexpected death within the first year of life.There is no obvious cause of death on postmortem examination.
• Postulated Hypotheses:– Abnormal brain stem respiratory control of
arousal, dysautonomia, malignant cardiac arrhythmias
• Risk Factors:– Prematurity, siblings of SIDS victim, maternal drug
use, prone sleeping position, multiple gestations
• Laboratory Tests:– EEG, Pulse oximetry, ECG, Holter, sleep studies,
apnea monitorization
Causes of Cardiovascular Sudden
Death• Children With Known Heart Disease
– Aortic Stenosis– Congenital Heart BlockCongenital Heart Block– Cardiomyopathy & Myocarditis
• Children With Unknown Heart Disease– Hypertrophic Cardiomyopathy– Long QT SyndromeLong QT Syndrome– Wollf-Parkinson-White SyndromeWollf-Parkinson-White Syndrome– Primary Ventricular Tachycardia and Primary Ventricular Tachycardia and
Ventricular FibrillationVentricular Fibrillation

Sudden Cardiac Death
LQTS
Cathecolam inergic VT
Brugada Syndrom e
AV Blocks
W PW Syndrom e
ELECTRICAL DISORDERS
M yocarditis
Dilated Cardiom yopathy
Hypertrophic Cardiom yopathy
M YOCARDIAL DISORDERS
Aortic Stenosis
Coronary Anom alies
CONGENITAL ANOM ALIES
VT & VF

VT
VF
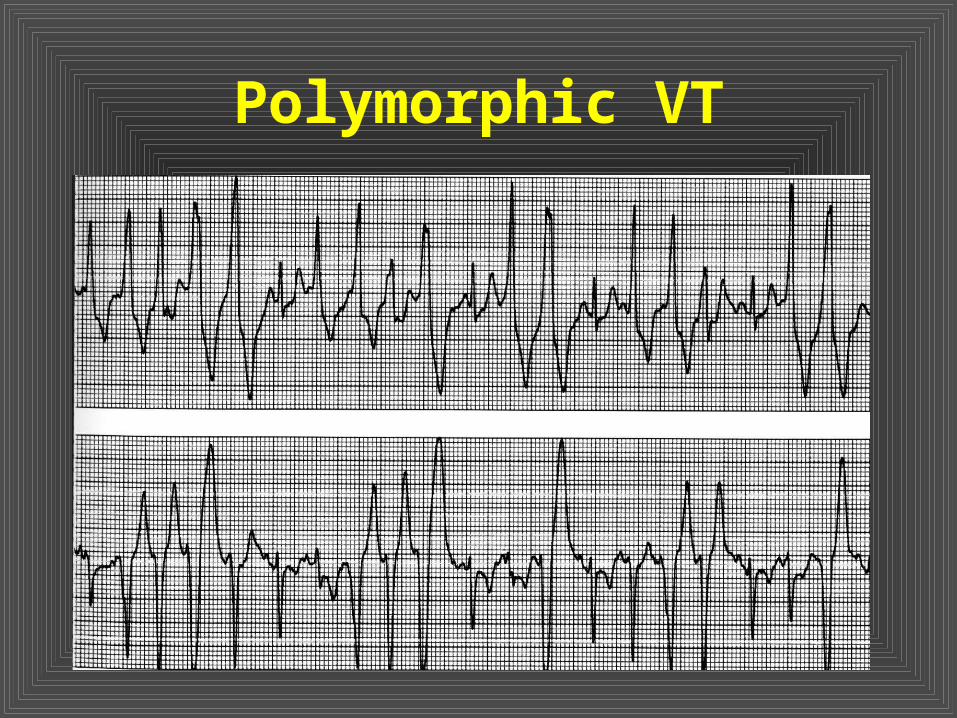
Polymorphic VT
Polimorphic Ventricular Tachycardia
• Congenital Long QT Syndrome
• Acquired Long QT Syndrome
• Cathecolaminergic Polimorphic VT
• Idiopatic VT & VF– Brugada Syndrome
– Normal ECG (Belhassen)
Long QT Syndrome: Prevalence &History
• On the basis of molecular genetics the prevalence of LQTS estimated to be one per 3000-4000 births.
• Description: 1957 (Jervell-Lange-Nielsen) and 1963-64 (Romano-Ward)
• “Registry”: 1979 (Moss&Schwartz)
• Genetic Analysis: 1991 (Keating)

Clinical Findings• SyncopeSyncope• Family historyFamily history• ECG FindingsECG Findings
– QT Interval ProlongationQT Interval Prolongation– Abnormal T MorphologyAbnormal T Morphology– Prolonged QT DispertionProlonged QT Dispertion– T wave AlternansT wave Alternans– Low Heart RateLow Heart Rate– AV BlocksAV Blocks
• GeneticsGenetics• ECHO Findings

Syncope Attacks
• Syncope occurs due to “torsade de pointes” or ventricular fibrillation.
• Syncope develops during excitement or crying.– Especially during fear or excitement– Physical activity (swimming)
Syncope may occur during rest Syncope may occur during rest periods in LQTS3 type.periods in LQTS3 type.
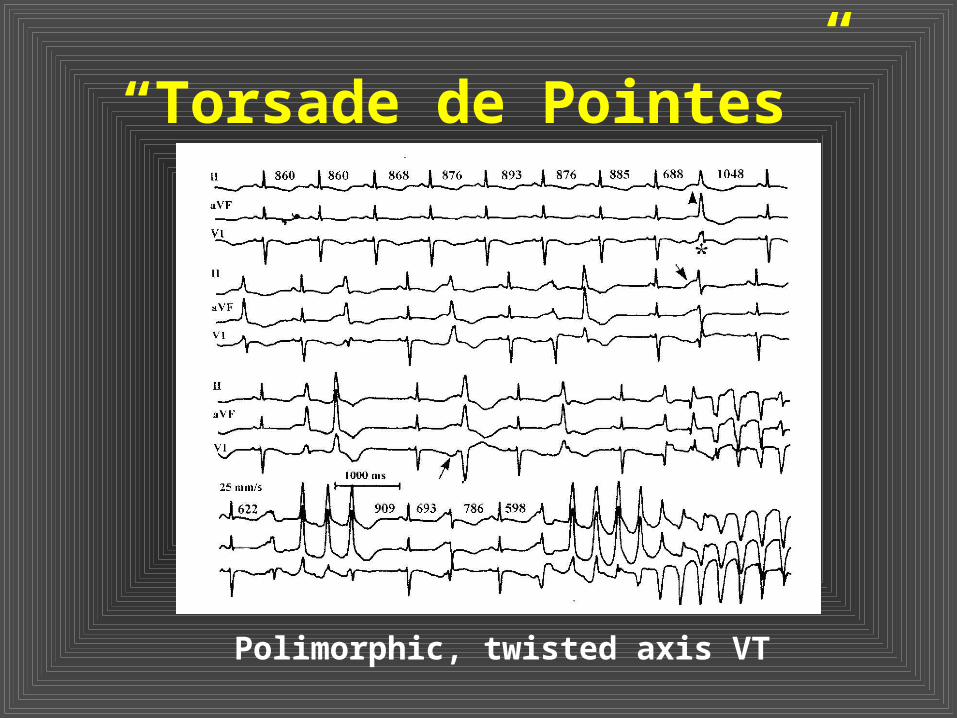
“Torsade de Pointes”
Polimorphic, twisted axis VT

Causes of Syncope
0
20
40
60
80
100
LQT1 LQT2 LQT3
STRESS
REST
QT Interval
• Corrected QT interval (QTc) can be measured by Bazzet formula.It should be measured from DII.
• It is abnormal if prolonged >440 msec. It is more pronounced in sick girls. There are some cases with normal QT interval (abnormal genotype, normal fenotype).
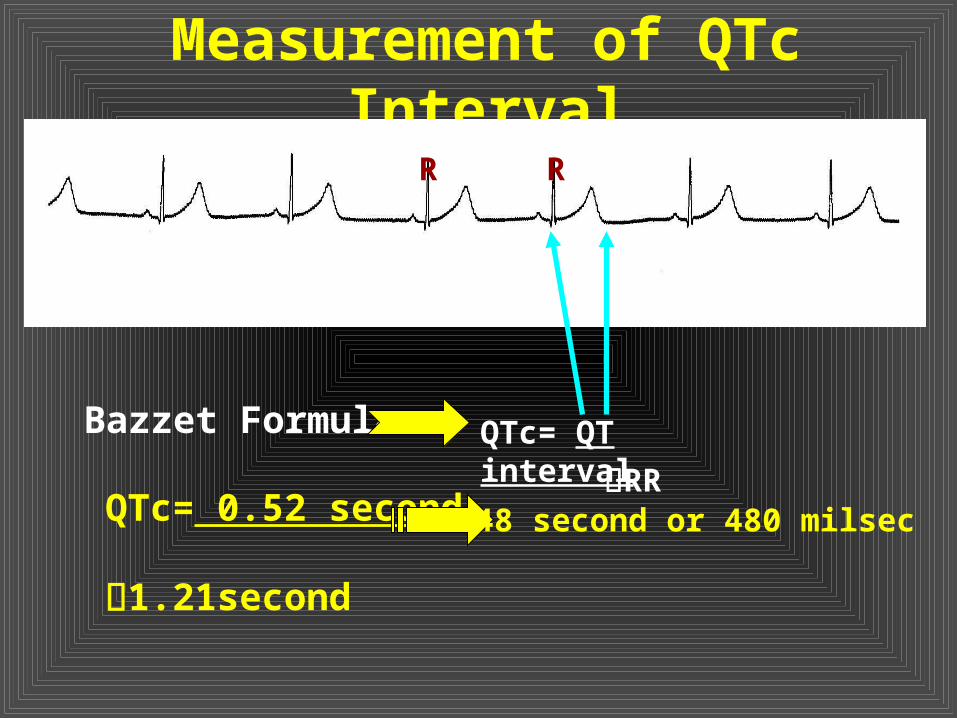
Measurement of QTc Interval
QTc= QT intervalBazzet Formula
RR
R R
QTc= 0.52 second 1.21second
0.48 second or 480 milsec

Age and Sex & QTc (sec)
1-15 year Men Women
Normal <0.44 <0.43 <0.45
Borderline
0.44-0.46 0.43-0.45 0.45-0.47
Prolonged
>0.47 >0.46 >0.48
T Morpholgy• There are changes in T wave morphology beside
long QT interval.
• T wave may be biphasic or humped. These findings are generally seen in V2-V5 leads, and prominent in V3 and V4.
• This finding may be exaggrated after exercise test. Humps are generated by early after depolarization (EAD), and It is more common in symptomatic cases.
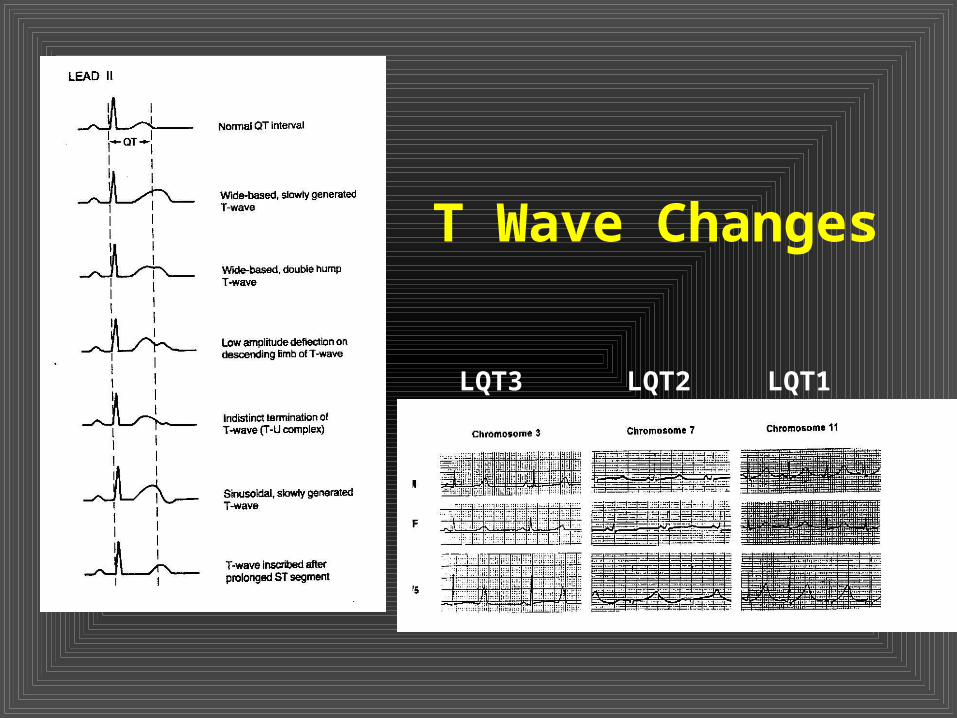
T Wave Changes
LQT1LQT3 LQT2
Heart Rate Abnormalities
• There is bradycardia. This feature is more apparent in children. Exercise test may also show inappropriately low heart rate increase.
• There may be >1.2 second pause without marked sinus arrhythmia and this may provoke TdP. After pauses some may see humps at T wave.

Molecular GeneticsType Inherita
nceGen Gen & Ion
ChannelTriggered causes
T Wave
LQT1 OD 11p5.5 KVLQT1, Iks Stress, swimming
Wide T
LQT2 OD 7q35-36
HERG, Ikr Stress, fear
Twave with hump and low volume
LQT3 OD 3p21-24
SCN5A, Na Channel
Sleeping Normal, Late T
LQT4 OD 4q25-27
? ? Sinusoidal T-U, AF
LQT5 OD 21q22 KCNE1 (minK), Iks
? ?
LQT6 OD 21q22 KCNE2 (MiRP1), Ikr
? ?
JLN* 1-2
OR 11p5.521q22
KVLQT1, Iks
KCNE1, Ikr
? ?
*: sensoryneural deafness

Molecular Abnormalities in LQTS

Genetics I• Molecular analysis should be done
in patients and their families.• Molecular analysis is very helpful in
asymptomatic carriers.• Genetic analysis can reveal
molecular diagnosis in 30-50 percent of patients, since many of the genes responsible for LQTS have not been known nowadays. Molecular diagnosis may take several months.
Genetics II
• Gene-specific treatment can be used after genetic analysis. In LQTS3, mexiletine (Na channel blocking agent) may lessen QT interval and attacks.
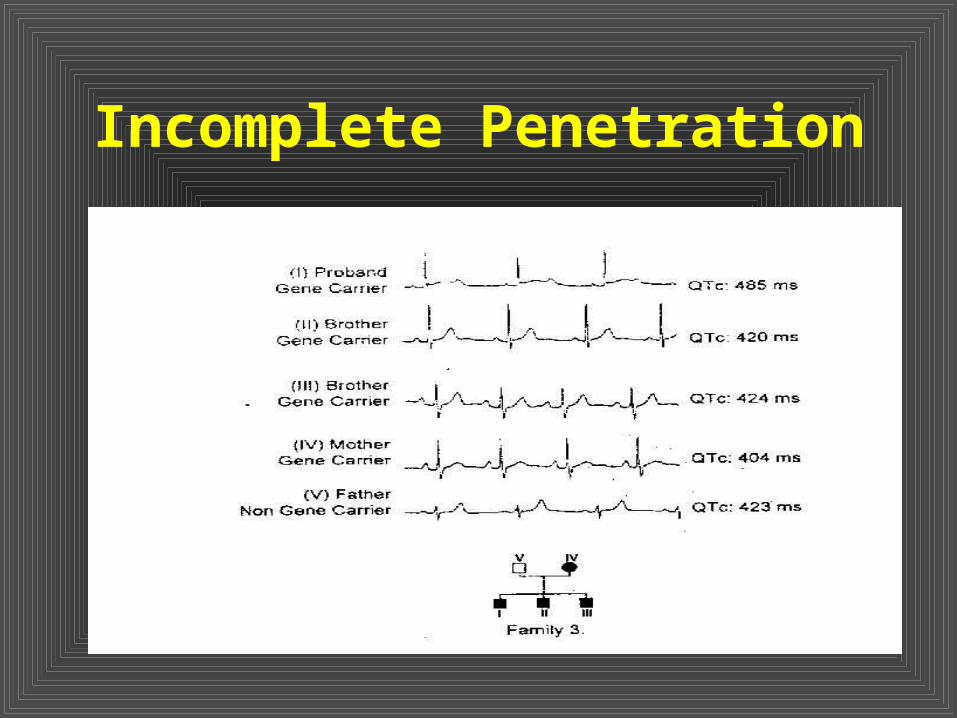
• Incomplete penetration is very common.Ventricular arrhtyhmia can be seen in some conditions in these patients.
• Some drugs may cause prolonged QT interval in these cases. QT interval would be normal if this drug will be stopped.
Incomplete Penetration
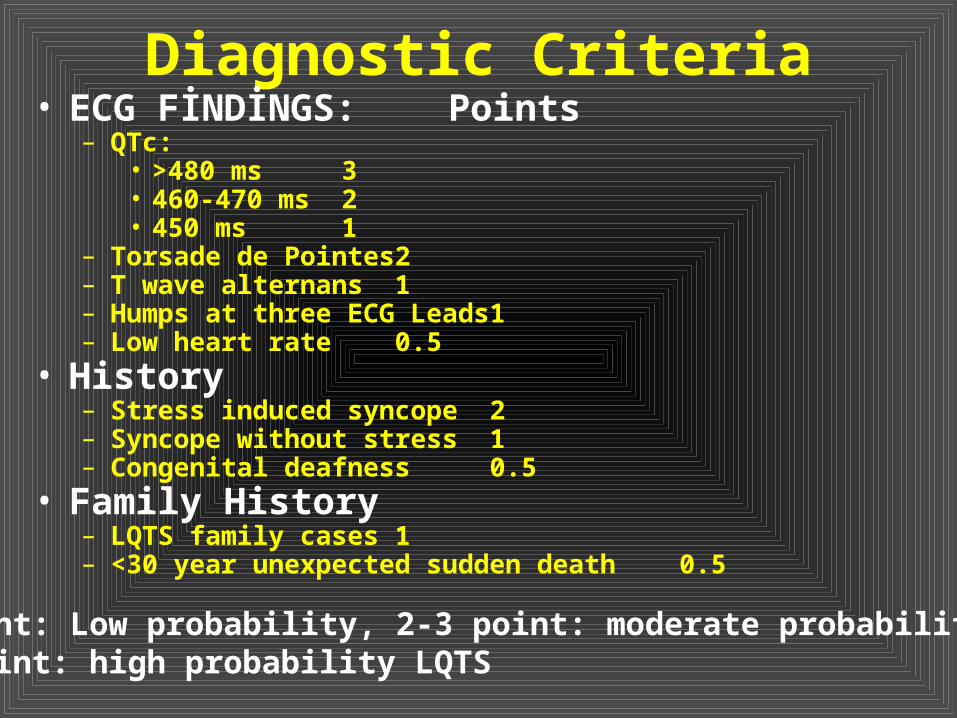
Diagnostic Criteria• ECG FİNDİNGS:
Points– QTc:
• >480 ms 3 • 460-470 ms 2 • 450 ms 1
– Torsade de Pointes 2 – T wave alternans 1 – Humps at three ECG Leads 1 – Low heart rate 0.5
• History– Stress induced syncope 2– Syncope without stress 1– Congenital deafness 0.5
• Family History– LQTS family cases 1– <30 year unexpected sudden death 0.5
<1 point: Low probability, 2-3 point: moderate probability LQTS, >4 point: high probability LQTS
Treatment
blockage• Permanent pacemaker implantation• Left Cardiac Sympatethic Denervation• ICD (Implantable Cardiac Defibrillator)• Gene specific treatment • Avoid of drugs that prolongs QT
interval

Long QT ve Second Degree Type II AV Block

Drugs Should be Avoided !!!
• Drugs causes QT Interval Prolongation:– Fenotiasins: Haldol, klorpromazin vs– Tricyclic Antidepressants: İmipramin, lityum– Makrolide Antibiotics: Erithromisin, azitromisin,
cetocanazole– Nonsedative Antihystamins: Terfenadine, astemizol– Class I AA Drugs: Quinidin, procainamide, dysopyramide– Class III AA Drugs: Sotalol, amiodarone– Gastric Motility Agents: Cisapride
• Stimulants stimulants, metylksantins, metilphenidate
• Drug Abuse and Addicts– Nicotine, cocaine, amphetamine, marihuana, LSD,
fensyklydine

Pentamidine
Procainamide
Hypokalemia
SIDS and Long QT Syndrome
• Schwartz et al. demonstrated a correlation between QT prolongation and SIDS.!!!
• In the first 48 hours there is a transient QT prolongation (fewer than two to three per 1000), secondary to fetal-maternal eletrolyte fluxes and transient alterations in autonomic control. ECG screening should be done after a few days of life.
• The efficacy of therapeutic interventions in infants with prolonged QT interval is impossible to predict. Since many of these prolongations are due to transient autonomic instability.
Schwartz PJ. Et al.Prolonged QT
And SIDS. New Eng. J Med.330; 709, 1998.
Long QT and SIDS
• 34.462 healthy newborn enrolled and 33.064 could be followed for one year.
• 12 lead ECG’s were obtained at the third or fourth day of life, and RR, QT and QTc intervals were measured from lead II.
• 1408 children were lost to follow-up when their families moved.
Schwartz PJ. Et al.Prolonged QT And SIDS.
• During one year of follow-up there were 34 deaths; 24 due to SIDS and 10 due to other causes.
• The incidence of SIDS was 0.7 per 1000. Most deaths due to SIDS occurred in the second and third month of life.
• There was no difference between SIDS and others regarding sex.
• No victim of SIDS had a family history of LQTS.
Schwartz PJ. Et al.Prolonged QT And SIDS

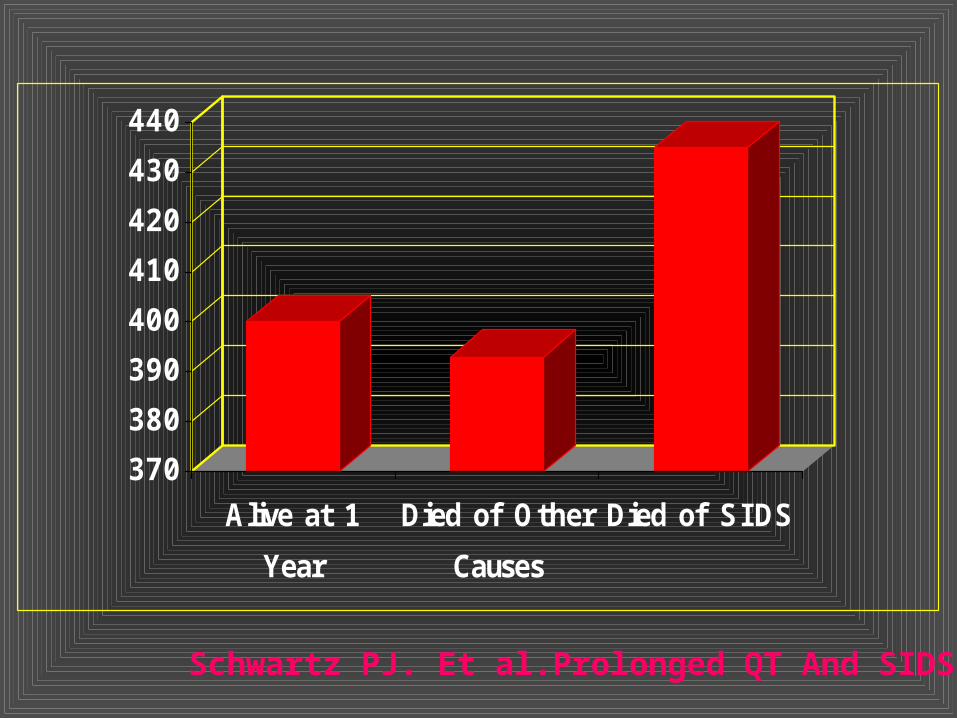
ECG Findings• Heart rate were not different
between groups.• QTc
– SIDS: 43545 msec– NonSIDS Deaths: 39324 msec
(p<0.05 )– Survivors: 40020 msec (p<0.05)– 12 of 24 infants who died of SIDS (50
percent) had a QTc greater than 440 msec.
Schwartz PJ. Et al.Prolonged QT And SIDS
370
380
390
400
410
420
430
440
Alive at 1
Year
Died of Other
Causes
Died of SIDS
Schwartz PJ. Et al.Prolonged QT And SIDS
• Schwartz et al. N Eng. J Med. 1999.
• They showed SCN5A mutation in this resusiated sudden death case.
Prevention of SIDS
• Assessment of family history• ECG recordings at 2-3 weeks
after birth.• If QTc> 470 msec after second
ECG, blockers may be used.
Schwartz PJ. Schwartz PJ.
!!!!???
-------------------

Long QT Syndrome & SIDS
Major Drawbacks• International studies have failed to demonstrate
any excess of SIDS in families with known LQTS. • The incidence of SIDS is rare in some countries.• The incidence of sudden death decreased by
changing of sleep position, cessation of parental smoking.
• There is no proven relationship between the prolonged QT and molecular diagnosis.
• Problems of screening methods.• There is no consensus on diagnosis and
treatment.
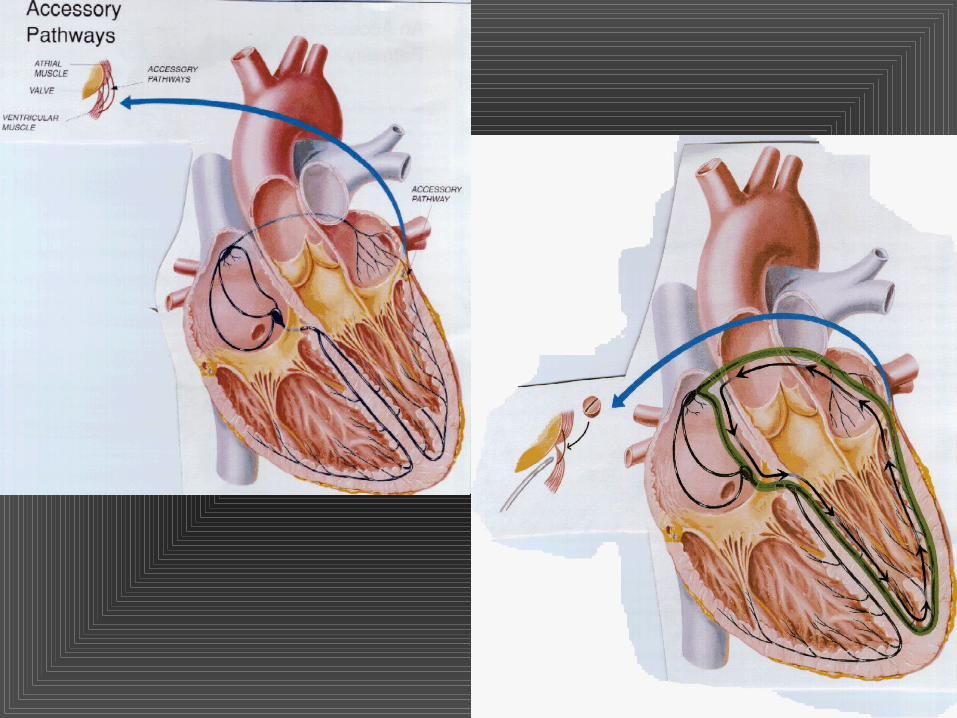
Wolf-Parkinson-White Syndrome
• The incidence in children is 0.1 %.• If there is a rapidly conducting
accessory pathway, atrial fibrillation may cause to VF.
• Some proarrhythmic (new arrhythmia caused by antiarrhythmic drugs) antiarrhythmic drugs may also cause this complication.
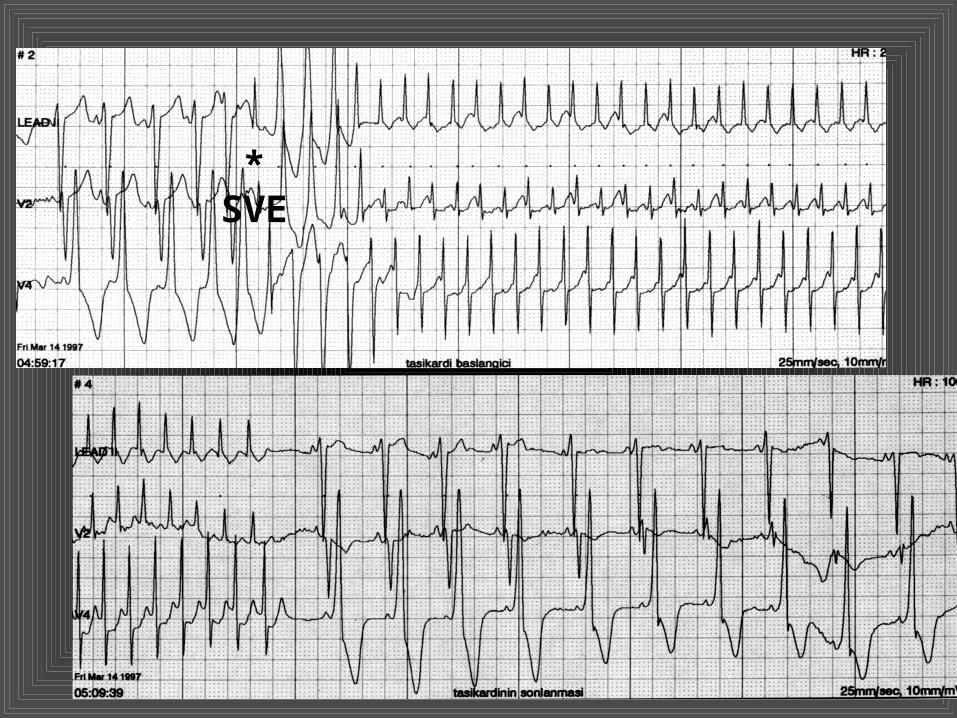
*SVE
WPW Syndrome and VF
• Atrial fibrillation is more common in patients with this syndrome.
• If accessorry pathway refractory period is less than 220 msec, there is a risk of ventricular fibrillation during atrial fibrillation.
• Some drugs, that prolongs AV conduction may provoke VF during AF due to rapid conduction via AP.
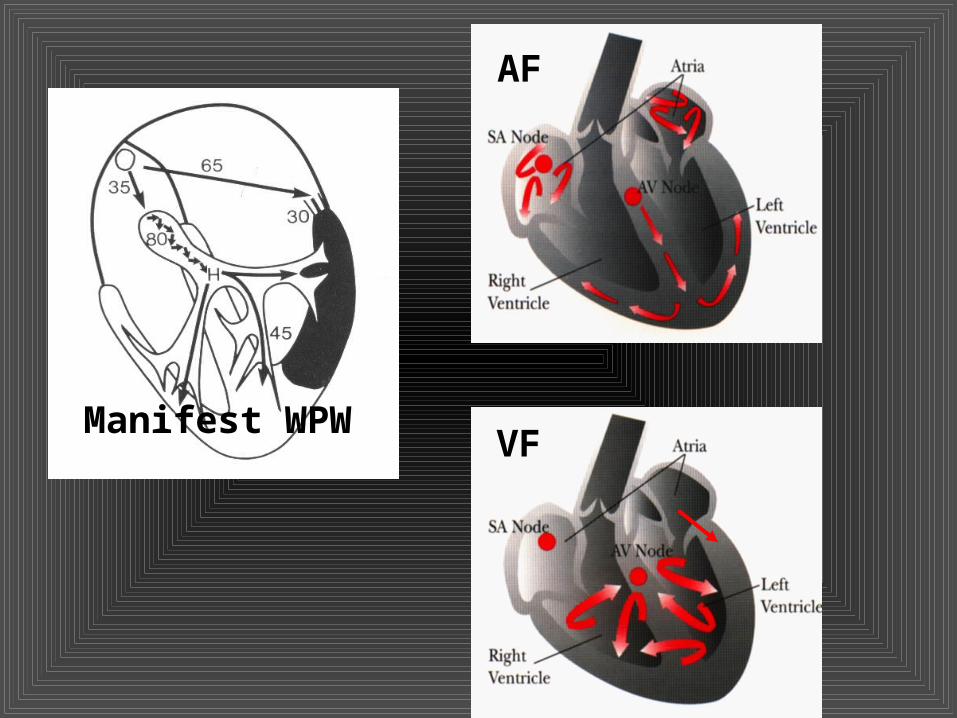
Manifest WPW
AF
VF

Congenital Heart Block I
• These babies have been diagnosed due to low heart rates. But most of them do not need pacemaker implantation. Close follow-up is mandatory to avoid the sudden cardiac death.
• Pacemaker Indications (Class I):– No CHD, awake heart rate <65 bpm– CHD, awake heart rate <55 bpm– Heart failure– Prolonged QT Interval
Congenital Heart Block II
• Mothers of babies with congeniatl AV block should be evaluated for antinuclear antibodies.
• QT interval measurement is very important, since Long QT Syndrome may be the cause of AV block. Prolonged repolarisation results with AV block.
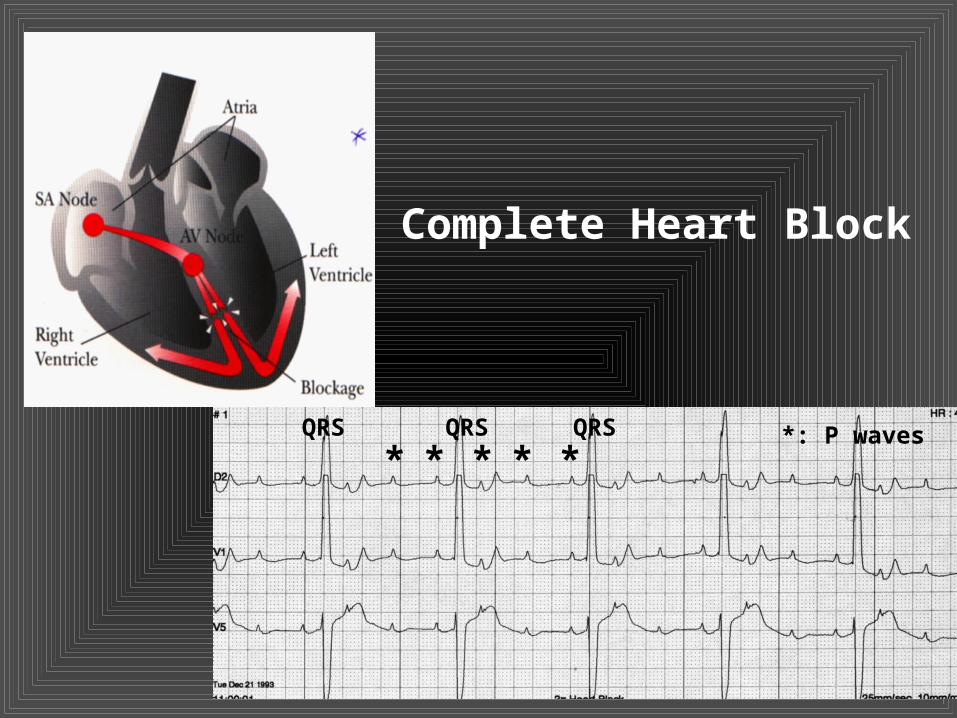
* * * * *QRS QRS QRS *: P waves
Complete Heart Block
Permanent Pacemaker
Dilated Cardiomyopathy & Myocarditis
• The etiology of DCM is idiopathic. Only 2-15 % of the children with DCM has biopsy proven myocarditis.
• There are familial DCM cases. • Histologic features classically include
myocyte hypertrophy, degeneration and varying degrees of interstitial fibrosis.
• There is ventricular dilation and decreased left ventricular systolic function.

Dilated Cardiomyopathy
Dilated Cardiomyopathy & Myocarditis
• Fibrosis of ventricular myocardium may occur, resulting in an irritable focus that causes ventricular arrhythmias.
• In Holter monitoring 46 % of patients had arrhythmias. Ventricular arrhytmias are more common than atrial arrhythmias.
• If there is a serious ventricular arrhythmia, amiodarone should be the drug of choice to prevent sudden death.
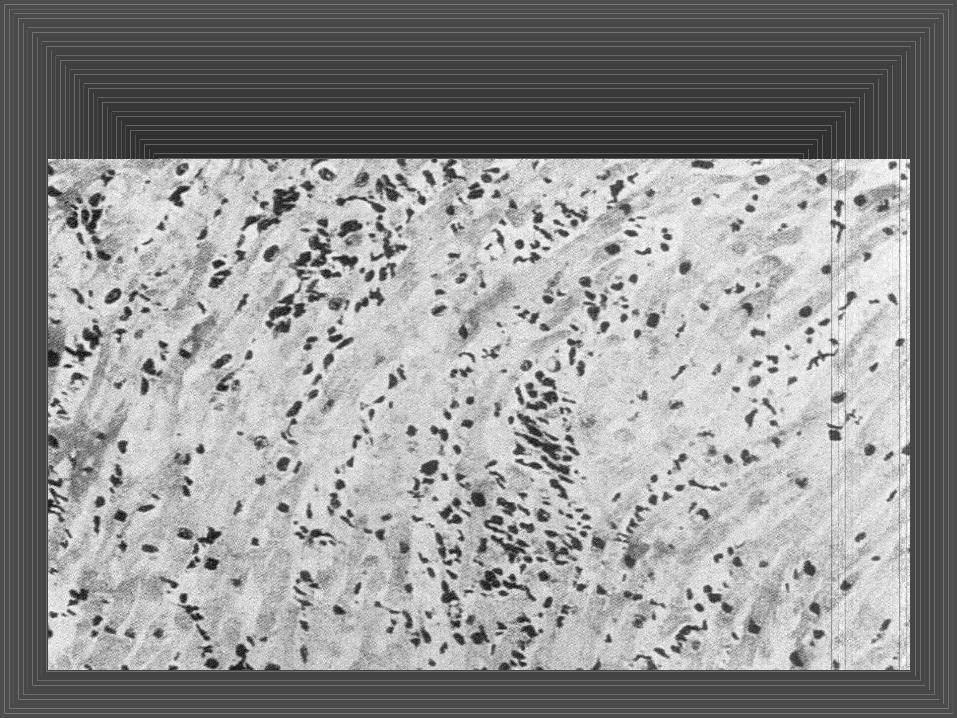
Myocarditis
• Acute or myocarditis have been reported as pathologic findings in up to 42 % of patients with SCD.
• Some patients may have subtle findings such as tachycardia and low-grade ventricular ectopy.
• Occasionally AV block may develop during myocarditis.
Hypertrophic Cardiomyopathy
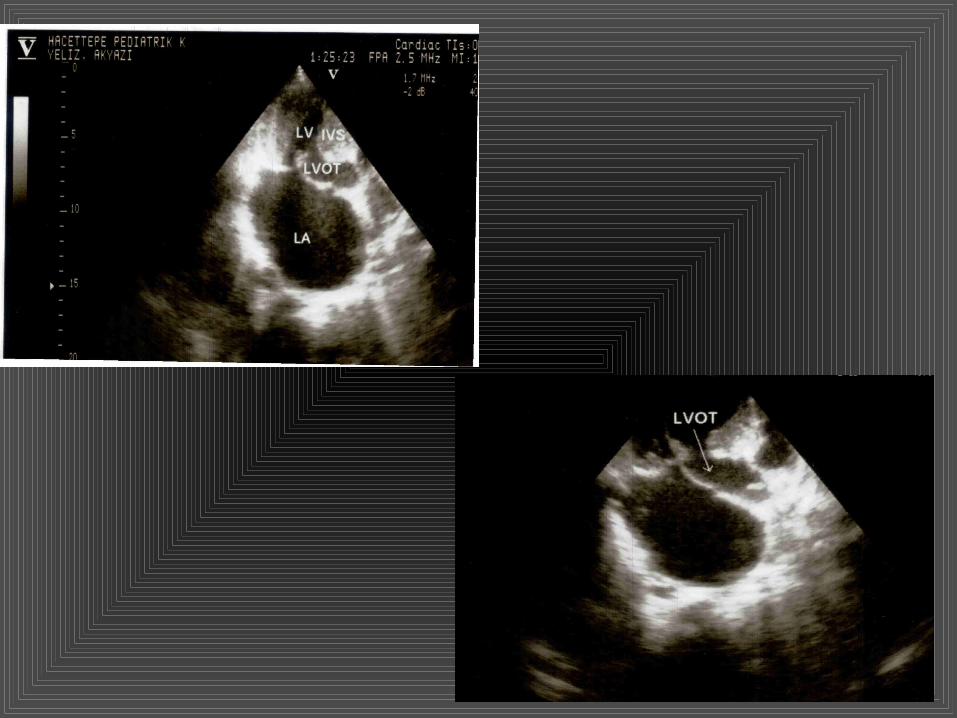
• It is the most common hereditary cardiac disease.
• Left ventricular outflow tract obstruction and diastolic dysfunction are the main pathophysiologic abnormalities.
• The histologic features consistent with with HCM include myocyte hypertrophy with great variation in size and shape, cardiac muscle cell disarray, fibrosis and abnormalities of small intramural coronary arteries.
Hypertrophic Cardiomyopathy

Hypertrophic Cardiomyopathy
• Muscle cell disarray may be a reason for ventricular arrhythmias.
• Any kind of supraventricular and ventricular arrhythmias may occur in patients with HCM.
• HCM is the most common cause of sudden cardiac death in young adults.
• The prognosis of infants who present before one year of age continues to be dismal.
• Amiodarone has been suggested as an effective medication for the treatment of rhythm problems. Sometimes ICD implantation is required to prevent sudden death due to VF.
Aortic Stenosis
• The incidence of sudden death is 5.4 % in patients with AS.
• The development of myocardial ischemia is thought to be the initiating factor for terminal ventricular arrhythmias in patients with severe AS.
• Syncope, chest pain, dyspnea, left ventricular strain on ECG, severe LVOT obstruction were identified as risk factors for SCD.
Coronary Artery Anomalies
• These anomalies may be diagnosed during postmortem examination.
• Types of anomalies:– Anomalous origin of left coronary artery from Anomalous origin of left coronary artery from
pulmonary artery (ALCAPA)pulmonary artery (ALCAPA)– Left main coronary artery from the right sinus
Valsalva– Acute angle takeoff of a coronary artery– Intramural coronary artery– Single right coronary artery
• ALCAPA is the mostcommon type that presents symptoms during infancy.