Cardiovascular, Lymphatic and Systemic DiseasesReineer Jalon
College of Nursing Western Mindanao State University
y Cardiovascular &
Lymphaticy Bacterial y Septic shock y Rheumatic fever y
Parasitic y Schistosomiasis y Elephantiasis/Filariasis
y Systemic y Bacterialy Anthrax y Plague y Lyme disease
y Viral y Dengue fever y Parasitic y Malaria
Septic Shocky Sepsis or septic shock is a systemic inflammatory
response
secondary to a documented infection. Consequently, sepsis is a
continuum of detrimental host responses to infection that ranges
from sepsis to septic shock and Multiple Organ Dysfunction
Syndrome(MODS). y Shock refers to a state of inability to maintain
adequate tissue perfusion and oxygenation, ultimately causing
cellular, and then organ system dysfunction.
Septic Shocky Pathophysiologyy inflammatory mediators are the
key players in the pathogenesis. y The gram-positive and
gram-negative bacteria induce a variety
of proinflammatory mediators, including cytokines. Such
cytokines play a pivotal role in initiating sepsis and shock. The
bacterial cell wall components are known to release the cytokines;
these include lipopolysaccharide (gram-negative bacteria),
peptidoglycan (gram-positive and gram-negative bacteria), and
lipoteichoic acid (gram-positive bacteria) y An imbalance of
homeostatic mechanisms lead to disseminated intravascular
coagulopathy (DIC) and microvascular thrombosis causing organ
dysfunction and death
Septic Shocky The predominant hemodynamic feature of septic
shock is
arterial vasodilation. Diminished peripheral arterial vascular
tone may result in dependency of blood pressure on cardiac output,
causing vasodilation to result in hypotension and shock if
insufficiently compensated by a rise in cardiac output y Vasoactive
mediators cause vasodilatation and increase the microvascular
permeability at the site of infection. Nitric oxide plays a central
role in the vasodilatation of septic shock. Impaired secretion of
vasopressin also may occur, which may permit the persistence of
vasodilatation
Septic Shocky Etiologyy Most patients who develop sepsis and
septic shock have underlying
circumstances that interfere with the local or systemic host
defense mechanisms. The most common disease states predisposing to
sepsis are malignancies, diabetes mellitus, chronic liver disease,
chronic renal failure, and the use of immunosuppressive agents. In
addition, sepsis also is a common complication after major surgery,
trauma, and extensive burns. y Respiratory tract infection and
urinary tract infection are the most frequent causes of sepsis,
followed by abdominal and soft tissue infections. y The use of
intravascular devices is a notorious cause of nosocomiallyacquired
sepsis. y Multiple sites of infection may occur in 6-15% of
patients
Septic Shocky Etiologyy Lower respiratory tract infections are
the cause of septic shock
in 25% of patients. The following are common pathogens:y
Streptococcus pneumoniae y Klebsiella pneumoniae y Staphylococcus
aureus y Escherichia coli y Legionella species y Haemophilus
species y Anaerobes y Gram-negative bacteria y Fungi
Septic Shocky Etiologyy Urinary tract infections are the cause
of septic shock in 25% of
patients, and the following are the common pathogens:y E coli y
Proteus species y Klebsiella species y Pseudomonas species y
Enterobacter species y Serratia
Septic Shocky Etiologyy Soft tissue infections are the cause of
septic shock in 15% of patients, and the
following are the common pathogens:y y y y
S aureus Staphylococcus epidermidis Streptococci Clostridia
y GI tract infections are the cause of septic shock in 15% all
patients, and the
following are the common pathogens:y y y y y y y
E coli Streptococcus faecalis Bacteroides fragilis Acinetobacter
species Pseudomonas species Enterobacter species Salmonella
species
Septic Shocky Risk factorsy Extremes of age ( 70 y) y Primary
diseases y Liver cirrhosis y Alcoholism y Diabetes mellitus y
Cardiopulmonary diseases y Solid malignancy y Hematologic
malignancy y Immunosuppression y Neutropenia y Immunosuppressive
therapy y Corticosteroid therapy y Intravenous drug abuse y
Compliment deficiencies y Asplenia
Septic Shocky Risk factorsy Major surgery, trauma, burns y
Invasive procedures y Catheters y Intravascular devices y
Prosthetic devices y Hemodialysis and peritoneal dialysis catheters
y Endotracheal tubes y Prior antibiotic treatment y Prolonged
hospitalization y Other factors - Childbirth, abortion, and
malnutrition
Septic Shocky s/sxTemperature greater than 38C or less than 36C
Heart rate greater than 90 Respiratory rate greater than 20 per
minute WBC count more than 12,000/L, Chills are a secondary symptom
associated with fever, which is a consequence of increased muscular
activity that produces heat and raises the body temperature. y
Sweating occurs when the hypothalamus returns to its normal set
point and senses the higher body temperature, stimulating
perspiration to evaporate excess body heat. y Alteration in mental
function often occurs: apprehension, anxiety, agitation, and,
eventually, coma are manifestations of severe sepsis. y
Hyperventilation with respiratory alkalosis is a common feature of
patients with sepsis secondary to stimulation of the medullary
respiratory center by endotoxins and other inflammatory mediators.y
y y y y
Septic Shocky Dxy PE, v/s y Observe patients for systemic signs
of inadequate tissue
perfusion. In the early stages of sepsis, cardiac output is well
maintained or even increased. The vasodilation may result in warm
skin, warm extremities, and normal capillary refill (warm shock).
As sepsis progresses, stroke volume and cardiac output fall, the
aeg start to manifest signs of hypoperfusion(cool skin, cool
extremities, and delayed capillary refill or cold shock) y CBC w/
dif count (Hgb, WBC, plt) y Assess renal and hepatic functions
(serum creatinine, BUN, ALT, AST, albumin)
Septic Shocky Tx y The principles in the management of septic
shock, based on
current literature, include the following components:Early
recognition Early and adequate antibiotic therapy Source control
Early hemodynamic resuscitation and continued support
Corticosteroids (refractory vasopressor-dependent shock) Proper
ventilator management with low tidal volume in patients with ARDS y
Vasopressor drugs: Dopamine, Epinephrine, Norepinephriney y y y y
y
Septic Shocky Nsg interventiony Assist Dr in mgt y Meds as
ordered y Admin oxygen as ordered y Assist in intubation y Aseptic
technique
Rheumatic Fevery Rheumatic fever causes
chronic progressive damage to the heart and its valves. y The
association between sore throat and rheumatic fever was not made
until 1880. y The dramatic decline in the incidence of rheumatic
fever is thought to be largely owing to antibiotic treatment of
streptococcal infection
Rheumatic Fevery Pathophysiologyy Acute Rheumatic Fever(ARF) is
a sequela of a previous group A
streptococcal infection, usually of the upper respiratory tract.
y The disease involves the heart, joints, CNS, skin, and
subcutaneous tissues. It is characterized by an exudative and
proliferative inflammatory lesion of the connective tissue,
especially that of the heart, joints, blood vessels, and
subcutaneous tissue
y Epidemiologyy As a sequela of beta-streptococcal exposure, ARF
occurs during
school years when streptococcal pharyngitis is most prevalent.
Similarly, prevalence is higher in the colder months of the year
when streptococcal pharyngitis is most likely to occur.
Rheumatic Fevery s/sxy Guidelines of diagnosis used by the
American Heart Association
include major and minor criteria (ie, modified Jones criteria).
In addition to evidence of a previous streptococcal infection, the
diagnosis requires 2 major Jones criteria or 1 major plus 2 minor
Jones criteria.
y Major criteriay Carditis: This occurs in as many as 40% of
patients and may
include cardiomegaly, murmur, congestive heart failure, and
pericarditis, with or without valvular disease. y Migratory
polyarthritis: This condition occurs in 75% of cases and is
polyarticular, fleeting, and involves the large joints.
Rheumatic Fevery Subcutaneous nodules (ie,
Aschoff bodies): These nodules occur in 10% of patients and are
edematous, fragmented collagen fibers. They are firm, painless
nodules on the extensor surfaces of the wrists, elbows, and
knees.
Rheumatic Fevery Erythema marginatum: This
condition occurs in about 5% of cases. The rash is serpiginous
and long lasting. y Chorea (also known as Sydenham chorea and "St
Vitus dance"): This characteristic movement disorder occurs in
5-10% of cases. Sydenham chorea consists of rapid, purposeless
movements of the face and upper extremities. Onset may be delayed
for several months and may cease when the patient is asleep
Rheumatic Fevery Minor criteriay Clinical findings include
arthralgia, fever and previous history of
ARF y Laboratory findings include elevated acute phase reactants
(eg, erythrocyte sedimentation rate, C reactive protein), a
prolonged PR interval, and supporting evidence of antecedent group
A streptococcal infections (ie, positive throat culture or rapid
streptococcal screen and an elevated or rising streptococcal
antibody titer).
Rheumatic Fevery Dx y Jones criteria y Streptococcal antibody
tests disclose preceding streptococcal infection. y Isolate group A
streptococci via throat culture y cx y Mitral stenosis; carditis;
CHF y Tx y Penicillin G benzathine IM y Prednisone (glucocorticoid)
y Naproxen (NSAID) y Haloperidol may be helpful in controlling
chorea
Rheumatic Fevery Nsg interventions y Antibiotics as ordered;
completing the course of antibiotics minimizes the risk of
developing ARF (and subsequently rheumatic heart disease) y
Salicylates and anti-inflam agents y Emphasize importance of
long-term cardiac reevaluation and regular prophylactic antibiotics
y Maintain hydration y Control joint pain and inflam w/ massage y
Limit physical exercise in child w/ carditis y Monitor sx of cx
(pulmonary HPN, CHF, thromboemboli, valvular dse, arrhythmias
Schistosomiasisy Also Bilharziasis or snail fever, is a
human disease syndrome caused by infection from one of several
species of parasitic trematodes of the genus Schistosoma. This is a
major source of morbidity and mortality for developing countries in
Africa, South America, the Caribbean, the Middle East, and Asia. y
Most human schistosomiasis is caused by Schistosoma haematobium,
Schistosoma mansoni, or Schistosoma japonicum.
Schistosomiasisy Pathophysiologyy Acute schistosomiasis (ie,
Katayama fever) is a serum sicknesslike
illness that develops after several weeks in some, but not most,
individuals with new schistosomal infections. It may correspond to
the first cycle of egg deposition and is associated with marked
peripheral eosinophilia and circulating immune complexes. It is
most common with S japonicum and S mansoni infections and is most
likely to occur in heavily infected individuals after primary
infection. Symptoms usually resolve over several weeks, but the
syndrome can be fatal. Early treatment with cidal drugs may
exacerbate this syndrome and necessitate concomitant glucocorticoid
therapy.
Schistosomiasisy Pathophysiologyy Mild maculopapular skin
lesions may develop in acute
infection within hours after exposure to cercariae. Significant
dermatitis is rare with the major human schistosomal pathogens,
probably because the invading and developing cercariae are
minimally immunogenic. However, abortive human infection with
schistosomal species that rely on other primary hosts may cause
marked dermatitis or swimmer's itch. This self-limited process may
recur more intensely with subsequent exposures to the same
species.
Schistosomiasisy Epidemiologyy Highly endemic in Regions VIII,
X, XI and XII
y Inc periody 2-6wk
y MOTy skin penetration of infective cercariae through
wading, swimming in infested waters y Not transmissible from
person to person
Schistosomiasisy s/sxy Swimmers itch: itchiness w/in 24h;
redness; and
pustule formation at the point of entry of cercariae lasting
2-3d y diarrhea; abdominal pain y Katayama fever: fever;
generalized lymphadenopathy; hepatosplenomegaly 2-3wk after initial
infx and last for 1-2mo
Schistosomiasisy Dx y S/E: ID of eggs y Liver & rectal bx y
Cx y portal cirrhosis; cor pulmonale (hypertrophy of LV resulting
fr lung dse); myocardial damage y Tx y Praziquantel PO y Nsg
interventions y Proper disposal of excreta y Avoid wading in
infested waters y Elimination of intermediate host y Maintain
nutrition
Elephantiasisy or Lymphatic Filariasis, is a rare disorder of
the lymphatic
system caused by parasitic worms such as Wuchereria bancrofti
and Brugia malayi, all of which are transmitted by mosquitos(Aedes
poicilus, Culex fatigans, Anopheles flavirostris). y Inflammation
of the lymphatic vessels causes extreme enlargement of the affected
area, most commonly a limb or parts of the head and torso. It
occurs most commonly in tropical regions.
Elephantiasisy Pathophysiology y larvae from the mosquito
migrate to the
lymphatics, where they develop into threadlike adult worms
within 6 to 12 mo. Gravid adult females produce microfilariae that
circulate in blood.
Elephantiasisy Epidemiologyy Phil stat: 2.5/100,000 pop y
Distribution: Cam norte/sur, Sorsogon, Quezon,
Albay, Mindoro, Bohol, Samar, Palawan, Sulu, TawiTawi, Basilany
MOTy Bite of mosquito
y Dxy Fresh blood smear y Bentonite Flocculation Test
Elephantiasisy s/sxy Acute: fever, malaise,
chills y Chronic: lymphadenitis, swelling of scrotum, lymphatic
channel affected; eosinophilia
Elephantiasisy Txy Diethylcarbamazine
citrate (Beltrazan) y AH or corticosteroid y Surgicaly Nsg
interventionsy Meds as ordered y Vector control y Health education
in
endemic areas
Anthraxy The term anthrax means coal in
Greek, and the disease is named after the appearance of its
cutaneous form. Anthrax is described in the Old Testament, by the
poet Virgil, and by the Egyptians. At the end of the 19th century,
Robert Koch's experiments with anthrax led to the original theory
of bacteria and disease. y Anthrax is caused by inhalation, skin
exposure, or gastrointestinal (GI) absorption. Disease caused by
inhalation is usually fatal, and symptoms usually begin days after
exposure. This delay makes the initial exposure to Bacillus
anthracis difficult to track
Anthraxy Can be grown in
laboratories and is a potential biowarfare agent
Anthraxy Pathophysiology y Virulence depends on the bacterial
capsule and the toxin complex. The capsule is a poly-D-glutamic
acid that protects against leukocytic phagocytosis and lysis.
Anthrax toxins are composed of 3 entities: a protective antigen, a
lethal factor, and an edema factor. The protective antigen is an
83-kd protein that binds to cell receptors within a target tissue.
Once bound, a fragment is cleaved free to expose an additional
binding site. This site can combine with edema factor to form edema
toxin or with lethal factor to form lethal toxin. Edema toxin acts
by converting adenosine triphosphate (ATP) to cyclic adenosine
monophosphate (cAMP). Cellular cAMP levels are increased, leading
to cellular edema within the target tissue. Lethal factor is not
well understood, but recent work suggests that it may inhibit
neutrophil phagocytosis, lyse macrophages, and cause release of
tumor necrosis factor and interleukin 1.
Anthraxy Epidemiology y A zoonotic dse; spores can remain viable
in soil for yrs y Livestock can become infected and can transmit
infx to humans on contact w/ infected animals or animal products
(hides, hair, wool, meat) y Inc period y Less than 2 wk y MOT y
Ingestion, inhalation or ingestion
Anthraxy s/sxy Cutaneous: pruritic papule
or vesicle which enlarges and ulcerates in 1-2d; a central black
aschar forms (malignant pustule); lesion is painless but w/
surrounding edema y Inhalational: fever; chills; non-productive
cough; chest pain; headache; myalgia; malaise; pleural effusion;
septic shock y GI: N&V; anorexia; abdominal pain; ascites;
hematemesis; bloody diarrhea
Anthraxy Dxy CXR y G/S and culture of blood, pleural fluid, CSF,
skin
discharges, tissue bx specimeny Txy Penicillin y
Ciprofloxacin
Anthraxy Nsg interventions/considerationsy Standard precaution y
Meds as ordered y Post-exposure prophylaxis y Anthrax vaccine
y Prognosisy high mortality for inhalational and GI anthrax
Plaguey The plague has caused more fear and terror than perhaps
any other
infectious disease in the history of humankind. It has laid
claim to nearly 200 million lives and has brought about monumental
changes, such as the end of the Dark Ages and the advancement of
clinical research in medicine. y AlexandreYersin isolated the
plague bacillus, developed an antiserum to combat the disease, and
postulated its connection with fleas and rats during the epidemic
of 1894. The plague bacillus was named Yersinia pestis in his
memory. y Although, the plague has been considered a disease of the
Middle Ages, recent interest has been spurred by concerns over its
use as a potential biological weapon. Aerosolized Y pestis, causing
primary pneumonic plague, has been recognized by bioterrorism
experts as having one of the highest potentials for adverse public
health impacts.
Plaguey In addition to the concern over its use in acts of
terrorism, there
are further reasons that may cause a dramatic increase in the
number of plague cases worldwide in the years to come. One reason
may be the climatic change brought about by global warming. This
change is ideal for increasing the prevalence of Y pestis in the
host population. A recent study has estimated a more than 50%
increase in the plague host prevalence with an increase of 1 degree
centigrade of the temperature in spring.Another reason may be the
increasing population explosion worldwide, which is bringing humans
into ever-increasing contact with wildlife. Lastly, the dramatic
population increase will contribute to conditions of overcrowding
and poor sanitationconditions ripe for plague hosts and vectors to
flourish in.
Plaguey Pathophysiology y Three forms of the plague exist:
bubonic plague,
pneumonic plague, and septicemic plague. The bubonic form of the
plague involves the pathognomonic "bubo" and is caused by
deposition of the bacillus in the skin by the bite of an infected
vector. If the vector is a flea, bacillus proliferates in the
flea's esophagus, preventing food entry into the stomach. To
overcome starvation, the flea begins a blood-sucking rampage.
Between its attempts to swallow, the distended bacillus-packed
esophagus recoils, depositing the bacillus into the victim's
skin.
Plaguey Pathophysiology y The bacillus invades nearby lymphoid
tissue,
producing the famous bubo, an inflamed, necrotic, and
hemorrhagic lymph node. Spread occurs along the lymphatic channels
toward the thoracic duct, with eventual seeding of the vasculature.
Bacteremia and septicemia ensue. The bacillus potentially seeds
every organ, including the lungs, liver, spleen, kidneys, and
rarely even the meninges
Plaguey Pathophysiologyy The most virulent form, pneumonic
plague, results from direct
inhalation of the bacillus, which occurs from close contact of
infected hosts or from aerosolized bacteria such as may occur if
used as a biological weapon. A severe and rapidly progressive
multilobar bronchopneumonia ensues with subsequent bacteremia and
septicemia. Secondary pneumonic plague is caused when an infected
patient seeds his or her lungs and airways. y The third type of
plague is a primary septicemic plague. This is hypothesized to
occur when the bacillus is deposited in the vasculature, bypassing
the lymphatics. Early dissemination with sepsis occurs but without
the formation of a bubo. This usually is observed in bites to the
oral, tonsillar, and pharyngeal area and is believed to occur
because of the vascularity of the tissue and short lymphatic
distance to the thoracic duct.
Plaguey Epidemiology y From 1967-1993, the World Health
Organization has reported an annual average of 1666 cases of the
plague. y MOT y Bite of vector, rat flea Xenopsylla cheopis y
Contact w/ infected tissue or body fluid y inhalation
Plaguey s/sx y Fever ; chills; myalgias; sore y y y y y y y
throat; malaise Enlarged, painful, swollen lymph node(bubo)
Abdominal pain Nausea, vomiting (bloody at times) Constipation,
diarrhea, and black or tarry stools Cough, which may be productive
of bloody sputum Shortness of breath Stiff neck
Plaguey Dx y CBC: elevated WBC y U/A: hematuria, proteinuria y
ABG: hypoxia and/or acidosis y G/S, culture of blood, sputum or
bubo aspirate y Tx y Gentamicin IV/IM y supportive y Nsg
considerations y Meds as ordered y Universal precaution (goggles,
gloves, gown; mask if pneumonic)
Lyme Diseasey is a multi-system infection
commonly affecting the skin, CNS, heart and joints caused by the
spirochete Borrelia burgdorferi.The bacterium is inoculated into
the skin by a tick bite. The tick is almost always of the genus
Ixodes.
Lyme Diseasey Pathophysiologyy Once in the skin, the spirochete
can (1) be overwhelmed and
eliminated by host defense mechanisms; (2) remain viable and
localized in the skin where it produces the pathognomonic skin
lesion, or erythema migrans (EM); or (3) disseminate through the
lymphatics or blood. Hematogenous dissemination can occur within
days to weeks of initial infection; the organism can travel to the
skin, heart, joints, CNS, and other parts of the body.
Lyme Diseasey Epidemiologyy In 2001, the CDC reported
17,029 cases and, in 2002, that number rose to 23,763a 40%
increase.Year-to-year variation can be significant. More than 95%
of cases come from 12 states (Connecticut, Delaware, Maine,
Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New
York, Pennsylvania, Rhode Island, and Wisconsin). Even within these
states, incidence can be quite variable from county to county and
even neighborhood to neighborhood.
y MOTy Vector-borne
Lyme Diseasey s/sxy Bulls eye rash (EM) usually
found in moist parts of the body, usually ascribed as rounded
rings of rash
Lyme Diseasey Dxy Aeg hx y Dermatologic findings:Classic EM is
an erythematous papule or
macule that occurs at the site of the tick bite (1-33 d later;
average, 7-10 d). Often, a central punctum is found at the site.
The size varies enormously (as large as 70 cm; average, 16 cm) and
depends on disease duration. EM usually is flat, round, or oval and
monocyclic but non-pruritic. y Elevated IgM
Lyme Diseasey Txy y y y
Amoxicillin Doxycycline Cefuroxime Erythromycin
y Nsg interventionsy Ascertain if the aeg was exposed to deer
ticks y Instruct aeg to wear light colored clothing when going to
the
forest/ woods or have himself/herself vaccinated y When bitten
by a tick, remove it by exerting slow steady upward pull and avoid
squeezing it
Denguey Dengue has been called the most important mosquito-
transmitted viral disease in terms of morbidity and mortality.
Dengue fever is a benign acute febrile syndrome occurring in
tropical regions. In a small proportion of cases, the virus causes
increased vascular permeability that leads to a bleeding diathesis
or disseminated intravascular coagulation (DIC) known as dengue
hemorrhagic fever (DHF). In 2030% of DHF cases, the patient
develops shock, known as the dengue shock syndrome (DSS).
Worldwide, children younger than 15 years comprise 90% of DHF
subjects; however, in the Americas, DHF occurs in both adults and
children
Denguey Dengue is a homonym for the
African ki denga pepo, which appeared in English literature
during an 1827-28 Caribbean outbreak. The first definite clinical
report of dengue is attributed to Benjamin Rush in 1789, but the
viral etiology and its mode of transmission via mosquitoes were not
established until the early 20th century. y EA: DEN-1, DEN-2,
DEN-3, DEN-4, Chikungunya virus
Denguey Pathophysiology y Dengue viral infections frequently are
not apparent. Classic
dengue primarily occurs in nonimmune, nonindigenous adults and
children. Symptoms begin after a 5- to 10-day incubation period.
DHF/DSS usually occurs during a second dengue infection in persons
with preexisting actively or passively (maternally) acquired
immunity to a heterologous dengue virus serotype. Illness begins
abruptly with a minor stage of 2-4 days' duration followed by rapid
deterioration. Increased vascular permeability, bleeding, and
possible DIC may be mediated by circulating dengue antigen-antibody
complexes, activation of complement, and release of vasoactive
amines. In the process of immune elimination of infected cells,
proteases and lymphokines may be released and activate complement
coagulation cascades and vascular permeability factors.
Denguey Epidemiology y Phil stat: 29.8/100,000 pop y Source:
infected persons y Common during rainy season y Infants and
children mostly affected generally 0-9yo y Inc period y 4-6d (min
3d, max 10d) y MOT y Day biting female mosquitoes (Aedes aegypti,
Aedes albopictus)
Denguey s/sx y Grade Iy Fever; (+) tourniquet test; non-specific
sx; abdominal sign; Hermans
sign (petechiae)
y Grade II y Grade I + bleeding (epistaxis, melena, gingival
bleeding, coffee ground vomitus) y Grade III y Grade II +
circulatory collapse (hypotension, rapid & weak pulse, cold
clammy skin y Grade IV y Grade III + shock w/ undetectable BP &
P
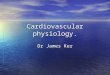
DengueA child with dengue hemorrhagic fever or dengue shock
syndrome may present severely hypotensive with disseminated
intravascular coagulation (DIC), as this severely ill PICU patient
did. Crystalloid fluid resuscitation and standard DIC treatment are
critical to the child's survival
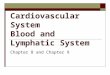
DengueDelayed capillary refill may be the first sign of
intravascular volume depletion. Hypotension usually is a late sign
in children. This child's capillary refill at 6 seconds was delayed
well beyond a normal duration of 2 seconds.
Denguey Dx y Tourniquet test y CBC: leukopenia,
thrombocytopenia, low hct y Dengue blot test y Tx y Symptomatic and
supportive y No specific antiviral tx y Avoid aspirin
Denguey Nsg interventions y Monitor for signs of bleeding and
fall in BP y Epistaxis: lean forward y Gingival bleeding: ice chips
y Hematemesis: NPO y Prognosis y Grade I & II: good y Grade
III: guarded y Grade IV: serious, high mortality rate
Malariay Term malaria is derived fr Lt mal(bad) and aria(air) y
Infection transmitted by female Anopheles mosquito, caused y y y y
y y
by Plasmodium falciparum(most fatal), P. vivax, P. ovale, P.
malariae. at high risk are pregnant women and children Sexual cycle
in mosquito; asexual cycle in human rbc Pf: malignant tertian
malaria Pv: benign tertian malaria Po: benign tertian malaria Pm:
quartan malaria
Malariay Pathophysiologyy The degree of damage to the tissue
depends mainly on the
parasitic concentration y Red cell changes:y Low deformability y
High adhesion y High fragility y Low oxygen transport
y Hemolysis leading to anemia y Rupture of infected and
non-infected RBC (blackwater fever) y Organ damage: spleen, liver,
brain, kidneys
MalariaEpidemiologyPhil stat: 52/100,000 pop
Inc periodPf: 10-13d Pm: 27-37d or up to yrs Po: 11-26d Pv:
12-21d
MOTbite of female Anopheles
Malariay s/sxy Stages y Cold: chilling: 10-15min (hot water bath
on soles) y Hot: 41deg fever (TSB, antipyretics) y Diaphoretic
(increase fluids, rest)
y Dxy symptomatic y Malarial smear (peak of fever) y IFA
Malariay Txy Chloroquine + Sulfadoxine/Pyrimethamine (CQ+SP) 1st
line
drug in the tx of probable malaria and confirmed Pf y
Artemether-Lumefantrine (Co-ArtemTM) 2nd line drug; given only to
microscopically confirmed Pf which did not respond to CQ+SP y
Quinine + Tetracycline/Doxycycline 3rd line drug; should be given
to those who did not respond to Co-Artem or if CQ+SP is not
available y N.B.: Tetracycline and Doxycycline are conrtaindicated
for pregnant women and children under 8yo; instead give Quinine w/
Clindamycin