Embed Size (px)
Citation preview

Cardiovascular DiseasesPathology
Medicine & Surgery
Bologna-University Medical School
Prof. Pier Paolo PiccalugaDepartment of Experimental, Diagnostic and Specialty Medicine
Institute of Hematology and Medical Oncology “L. and A. Seràgnoli”
Bologna University Medical School

Cardiovascular Diseases• Congenital heart diseases: principal alterations.
• Ischemic heart disease: anatomic alterations and histopathology of chronic ischemic heart disease and myocardial infarction (timing and evolution of morphologic changes, complications of myocardial infarction).
• Valvular heart disease: anatomic alterations and histopathology of rheumatic heart disease, aortic stenosis, mitral valve prolapse, infective endocarditis, non-bacterial thrombotic endocarditis.
• Myocardial diseases: anatomic alterations and histopathology of myocarditis and cardiomyopathies.
• Pericardial diseases: anatomic alterations and histopathology of pericarditis.
• Blood vessel diseases: anatomic alterations and histopathology of arteriosclerosis, atherosclerosis, aneurysms and vasculitis.
• Vascular tumors: classification and histopathological diagnosis.

Ischemic heart disease

Ischemic heart disease (IHD)Def. & general features
• IHD is a generic designation for a group of related syndromes resulting from myocardial ischemia - an imbalance between cardiac blood supply (perfusion) and myocardial oxygen demand.
• Although ischemia can result from increased demand (e.g., increased heart rate or hypertension), or diminished oxygen-carrying capacity (e.g., anemia, carbon monoxide poisoning), in the vast majority of cases IHD is due to a reduction in coronary blood flow caused by obstructive atherosclerotic disease Thus, IHD is also frequently called coronary artery disease (CAD).

Ischemic heart disease (IHD)Def. & general features
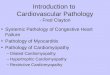
• Despite dramatic improvement over the past 3 to 4 decades, IHD in its various forms still represents the leading cause of death in Developed Countries
High income Low income

Clinical manifestations of IHD:(direct consequence of insufficient blood supply to the heart)
• There are four basic clinical syndromes of IHD:
– Angina pectoris (“chest pain”): the ischemia causes pain but is insufficient to lead to death of myocardium;
– Acute myocardial infarction (MI): the severity or duration of ischemia is enough to cause cardiac muscle death
– Chronic IHD with progressive heart failure
– Sudden cardiac death (SCD), can result from a lethal arrhythmia following myocardial ischemia.

Clinical manifestations of IHD:(direct consequence of insufficient blood supply to the heart)
• These syndromes are all relatively late manifestations of coronary atherosclerosis that begins early in life but manifests only after the vascular occlusions reach a critical stage.
• The term acute coronary syndrome is applied to three catastrophic manifestations of IHD: unstable angina, acute MI, and SCD

Ischemic heart disease (IHD)Pathogenesis
• Imbalance between perfusion and myocardial demand
• Ischemia also limits nutrients support and waste removal– It is less tolerated than simple hypoxia (anemia,
lung disease…)
• This may result from a combination of pre-existing ("fixed") atherosclerotic occlusion of coronary arteries and new superimposed thrombosis and/or vasospasm
→ Symptom onset depends not only on the extent and severity of fixed atherosclerotic disease but also critically on dynamic changes in coronary plaque morphology

• A lesion obstructing 70% to 75% or more of a vessel lumen - so-called critical stenosis -generally causes symptomatic ischemia (angina) only in the setting of increased demand
• A fixed 90% stenosis can lead to inadequate coronary blood flow even at rest.
• Importantly, if a coronary artery develops atherosclerotic occlusion at a sufficiently slow rate, it may be able to stimulate collateral blood flow from other major epicardial vessels;
– such collateral perfusion can then protect against MI even in the setting of a complete vascular occlusion.
Ischemic heart disease (IHD)Pathogenesis

Ischemic heart disease (IHD)Pathogenesis
• Although only a single major coronary epicardial artery may be affected by atherosclerotic narrowing, two or all three arteries - left anterior descending (LAD), left circumflex (LCX), and right coronary artery (RCA) - can be concurrently involved.
• Clinically significant plaques can be located anywhere but tend to predominate within the first several centimeters of the LAD and LCX, and along the entire length of the RCA.
• Sometimes, secondary branches are also involved

Role of Acute Plaque Change
• In most patients, unstable angina, infarction, and many cases of SCD all occur because of abrupt plaque change followed by thrombosis, hence the term acute coronary syndrome. The initiating event is typically disruption of a plaque due to:
• Rupture, fissuring, or ulceration of plaques exposing highly thrombogenic plaque constituents or underlying subendothelial basement membrane.
• Hemorrhage into the core of plaques with expansion of plaque volume and worsening of the luminal occlusion.

Role of Acute Plaque Change II
• The events that trigger the abrupt plaque
changes are complex.
• They may be intrinsic to the structure of the
plaque or extrinsic to it.
• Basically, rupture reflects the inability of a
plaque to withstand mechanical stresses.

Role of Acute Plaque Change III
• Plaques that contain a large atheromatous core or those in which the overlying fibrous caps are thin are more likely to rupture and are therefore denoted as "vulnerable."
• Fissures frequently occur at the junction of the fibrous cap and the adjacent normal plaque-free arterial segment, a location at which the mechanical stresses are highest and the fibrous cap is thinnest.

Role of Acute Plaque Change IV
Extrinsic factors:
• Adrenergic stimulation - can elevate physical stresses on the plaque through systemic hypertension or local vasospasm.
• Intense emotional stress can also contribute to plaque disruption.

Role of Acute Plaque Change V
• Such acute changes often develop in plaques not initially critically stenotic or even symptomatic before rupture.
• Pathologic and clinical studies show that two-thirds of ruptured plaques are ≤50% stenotic before plaque rupture, and 85% have initial stenosis ≤70%.
• It is presently impossible to reliably predict plaque rupture in any given patient.

Role of Acute Plaque Change VI
• Accumulating evidence also indicates that plaque disruption with ensuing platelet aggregation and thrombosis are common, repetitive, and often clinically silent complications of atherosclerosis.
• Moreover, healing of subclinical plaque disruptions and overlying thrombosis is an important mechanism by which atherosclerotic lesions progressively enlarge.

Role of inflammation
• Inflammation plays an essential role at all stages of atherosclerosis, from inception to plaque rupture.
• Atherosclerosis begins with the interaction of endothelial cells and circulating leukocytes, resultingin T-cell and macrophage recruitment and activation.
• These cells subsequently drive smooth muscle cellproliferation, with variable amounts of extracellularmatrix (ECM) accumulating over an atheromatouscore of lipid, cholesterol, calcification, and necroticdebris.
• At later stages, destabilization of atheroscleroticplaque occurs through metalloproteinase secretion.

Role of Thrombosis
• Thrombosis associated with a disrupted plaque is critical to the pathogenesis of acute coronary syndromes.
• In the most serious extreme, completely obstructive thrombus over a disrupted plaque can cause a massive MI.
– Even partial luminal occlusion by thrombus can compromise blood flow sufficiently to cause a small infarction of the innermost zone of the myocardium (subendocardial infarct).
• Mural thrombus in a coronary artery can also embolize;
• Finally, organizing thrombi produce potent activators of smooth muscle proliferation, which can contribute to the growth of atherosclerotic lesions

Role of Vasoconstriction
• Vasoconstriction directly compromises lumen diameter; and by increasing local mechanical shear forces, it can potentiate plaque disruption.
• It can be stimulated by:
1. circulating adrenergic agonists,
2. locally released platelet contents,
3. an imbalance between endothelial cell relaxing factors (e.g., nitric oxide) versus contracting factors (e.g., endothelin)
4. mediators released from perivascular inflammatorycells.

Angina Pectoris
• Angina pectoris is intermittent chest pain caused by transient, reversible myocardial ischemia.
1. Typical or stable angina is episodic chest pain associated with exertion or some other form of increased myocardial oxygen demand (e.g., tachycardia or hypertension due to fever, anxiety, fear). – Usually associated with a fixed atherosclerotic narrowing (≥75%) of one or
more coronary arteries.
– The myocardial oxygen supply may be sufficient under basal conditions but cannot be adequately augmented to meet any increased requirements.
– The pain is usually relieved by rest (reducing demand) or by administering agents such as nitroglycerin

Angina Pectoris
2. Prinzmetal, or variant angina is angina occurring at rest due to coronary artery spasm. Although such spasms typically occur on or near an existing atherosclerotic plaque, completely normal vessels can be affected. The etiology is not clear, but Prinzmetal angina typically responds promptly to the administration of vasodilators such as nitroglycerinView drug information or calcium channel blockers.

Angina Pectoris
3. Unstable angina is characterized by increasing frequency of pain, precipitated by progressively less exertion; the episodes also tend to be more intense and longer lasting than stable angina.
– Associated with plaque disruption and superimposed partial thrombosis, distal embolization of the thrombus, and/or vasospasm.
– Unstable angina is the harbinger of more serious, potentially irreversible ischemia (due to complete luminal occlusion by thrombus) and is therefore sometimes called pre-infarction angina.

Miocardial Infarction
• MI is necrosis of heart muscle resulting from ischemia.
• One-third die-half before they can reach the hospital.
• Approximately 10% of MIs occur in people younger than 40 years, and 45% occur in people younger than age 65.
• Men are at significantly greater risk than women, although the gap progressively narrows with age. In general, women are remarkably protected against MI during their reproductive years. Nevertheless, menopause-and presumably declining estrogen production-is associated with exacerbation of coronary atherosclerosis.

Pathogenesis
• Any form of coronary artery occlusion can cause acute MI,
– angiographic studies demonstrate that most MIs are caused by acute coronary artery thrombosis.
• In most cases, disruption of an atherosclerotic plaque results in the formation of thrombus.
– Vasospasm and/or platelet aggregation can contribute but are infrequently the sole cause of an occlusion.
– Sometimes, particularly with infarcts limited to the innermost (subendocardial) myocardium, thrombi may be absent. In these cases, severe diffuse coronary atherosclerosis significantly limits coronary vessel perfusion, and a prolonged period of increased demand (e.g., due to tachycardia or hypertension) may be sufficient to cause necrosis of myocytes most distal to the epicardial vessels.

• The evidence for this series of events derives from
(1) autopsy studies of patients dying with acute MI,
(2) angiographic studies demonstrating a high frequency of thrombotic occlusion early after MI,
(3) the high success rate of therapeutic thrombolysis and primary angioplasty, and
(4) the demonstration of residual disrupted atherosclerotic lesions by angiography after thrombolysis.
• Interestingly, coronary angiography performed within 4 hours of the onset of MI shows a thrombosed coronary artery in almost 90% of cases. However, when angiography is delayed until 12 to 24 hours after onset of symptoms, occlusions are observed in only 60% of patients, even without intervention. Thus, at least some occlusions seem to clear spontaneously as a result of lysis of the thrombus and/or relaxation of spasm

Myocardial Response to Ischemia
• Coronary artery obstruction blocks the myocardial blood supply, leading to
– functional,
– biochemical,
– morphologic consequences.
• Within seconds of vascular obstruction, cardiac myocyte aerobic glycolysis ceases, leading to inadequate ATP production and accumulation of potentially noxious breakdown products (e.g., lactic acid).
• The functional consequence is a striking loss of contractility, occurring within a minute or so of the onset of ischemia.

Myocardial Response to Ischemia II
Ultrastructural changes (rapidly apparent):
1. myofibrillar relaxation,
2. glycogen depletion,
3. cell and mitochondrial swelling.
• However, these early changes are potentially reversible, and myocardial cell death is not immediate.
Only severe ischemia lasting at least 20 to 40 minutes causes irreversible injury and myocyte death:
– predominant pattern is coagulation necrosis.

Myocardial Response to Ischemia III
• If myocardial blood flow is restored anywhere along this timeline (reperfusion), cell viability may be preserved.
• This provides the rationale for early clinical detection of acute MI, and prompt intervention by angioplasty or thrombolysis, to restore blood flow to the at-risk areas.
• Ischemic but still viable myocardium can be salvaged by early reperfusion.

Myocardial Response to Ischemia IV
• Myocardial ischemia also contributes to arrhythmias, probably by causing electrical instability (irritability) of ischemic regions of the heart.
• Although massive myocardial damage can clearly cause a fatal mechanical failure, SCD in the setting of myocardial ischemia is most often (80% to 90% of cases) due to ventricular fibrillation caused by myocardial irritability.

Myocardial Response to Ischemia V
• Irreversible injury of ischemic myocytes first occurs in the subendocardial zone. Not only is this region the last area to receive blood delivered by the epicardial vessels, the relatively higher intramural pressures there further compromise blood inflow.

Myocardial Response to Ischemia VI
• With more prolonged ischemia, a wave-front of cell death moves through the myocardium to involve progressively more of the transmural thickness of the ischemic zone, so that an infarct usually reaches its full size within 3 to 6 hours.
Any intervention in this time frame can
potentially limit the final extent of necrosis.

Morphology
• Nearly all transmural infarcts (defined as involving ≥50% of the myocardial wall thickness) affect at least a portion of the left ventricle and/or ventricular septum.
• Roughly 15% to 30% of MIs affecting the posterior or postero-septal wall also extend into the adjacent right ventricular wall.
• Isolated right ventricle infarcts, however, occur in only 1% to 3% of cases.
• Even in transmural infarcts, a narrow rim (∼0.1 mm) of viable subendocardial myocardium is preserved by diffusion of oxygen and nutrients from the ventricular lumen.

MI distribution based on vascularinvolvement
• Left anterior descending artery (40% to 50%): anterior left ventricle, anterior septum, and apex circumferentially.
• Right coronary artery (30% to 40%): posteriorleft ventricle, posterior septum, and right ventricular free wall in some cases.
• Left circumflex artery (15% to 20%): lateral leftventricle except the apex

Gross anatomy
• The gross and microscopic appearance of an MI depends on the interval of time since the original injury
• Areas of damage undergo a progressive and highly characteristic sequence of morphologic changes.
• Myocardial necrosis proceeds invariably to scar formation without any significant regeneration.
Time Gross Features
Reversible Injury
0-½ hr None
Irreversible Injury
½-4hr None
4-12hr Occasionally dark mottling
12-24hr Dark mottling
1-3 days Mottling with yellow-tan infarct center
3-7 days Hyperemic border; central yellow-tan softening
7-10 days Maximally yellow-tan and soft, with depressed
red-tan margins
10-14 days Red-gray depressed infarct borders
2-8wk Gray-white scar, progressive from border
toward core of infarct
>2mo Scarring complete

Gross anatomy
• Early recognition of acute MIs can be challenging
• MIs less than 12 hours old are usually not grossly apparent.
• Infarcts more than 3 hours old can be visualized by exposing heart slices to vital stains (e.g., triphenyl tetrazolium chloride, a substrate for lactate dehyrogenase in viable heart).
Time Gross Features
Reversible Injury
0-½ hr None
Irreversible Injury
½-4hr None
4-12hr Occasionally dark mottling
12-24hr Dark mottling
1-3 days Mottling with yellow-tan infarct center
3-7 days Hyperemic border; central yellow-tan softening
7-10 days Maximally yellow-tan and soft, with depressed
red-tan margins
10-14 days Red-gray depressed infarct borders
2-8wk Gray-white scar, progressive from border
toward core of infarct
>2mo Scarring complete

Gross anatomy II
• Because dehydrogenases are depleted in the area of ischemic necrosis (they leak through damaged cell membranes) an infarcted area is revealed as an unstained pale zone
• Old scars appear white and glistening.

Gross anatomy III
• By 12 to 24 hours after MI, an infarct can usually be grossly identified by a reddish blue discoloration caused by stagnant, trapped blood.
• Progressively thereafter, an infarct becomes more sharply delineated as a yellow-tan, softened area;
Time Gross Features
Reversible Injury
0-½ hr None
Irreversible Injury
½-4hr None
4-12hr Occasionally dark mottling
12-24hr Dark mottling
1-3 days Mottling with yellow-tan infarct center
3-7 days Hyperemic border; central yellow-tan softening
7-10 days Maximally yellow-tan and soft, with depressed
red-tan margins
10-14 days Red-gray depressed infarct borders
2-8wk Gray-white scar, progressive from border
toward core of infarct
>2mo Scarring complete

Gross anatomy IV
• By 10 to 14 days infarcts become rimmed by hyperemic (highly vascularized) granulation tissue.
• Over the succeeding weeks the MI evolves to a fibrous scar
Time Gross Features
Reversible Injury
0-½ hr None
Irreversible Injury
½-4hr None
4-12hr Occasionally dark mottling
12-24hr Dark mottling
1-3 days Mottling with yellow-tan infarct center
3-7 days Hyperemic border; central yellow-tan softening
7-10 days Maximally yellow-tan and soft, with depressed
red-tan margins
10-14 days Red-gray depressed infarct borders
2-8wk Gray-white scar, progressive from border
toward core of infarct
>2mo Scarring complete

Microscopic anatomy
• The microscopic appearance also undergoes a characteristic sequence of changes
• Typical features of coagulative necrosis become detectable within 4 to 12 hours of infarction.
• "Wavy fibers" can also be present at the edges of an infarct; these reflect the stretching and buckling of noncontractile dead fibers
• Sublethal ischemia can also induce myocyte vacuolization. These are large cleared intracellular spaces, probably containing water; such myocytes are still alive but are poorly contractile.

Microscopic anatomy II
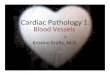
Coagulative
necrosis along
with wavy fibers,
Widened spaces
contain edema
fluid and scattered
neutrophils
Dense PMN
leukocytic
infiltrate in
area of 2- to
3-day-old MI
Granulation
tissue
(loose
collagen
and
abundant
capillaries)
Well-healed myocardial infarct with replacement of
the necrotic fibers by dense collagenous scar

Microscopic anatomy III
• Acute inflammation (typically most prominent 1-3 days after MI),
• Macrophages to remove necrotic myocytes and neutrophil fragments (most pronounced 5-10 days after MI).
• The infarcted zone is progressively replaced by granulation tissue (most prominent 2-3 weeks after MI),
• Dense collagenous scar is formed. In most instances scarring is well advanced by the end of the sixth week

Microscopic anatomy IV
• The efficiency of repair depends on the size of the original lesion.
– Healing requires the migration of inflammatory cells and ingrowth of new vessels that can access infarcts only from the intact vasculature at the infarct margins. Thus, an MI heals from its borders toward the center, and a large infarct may not heal as readily or as completely as a small one.
• Once an MI is completely healed, it is impossible to distinguish its age (i.e., the dense fibrous scars of 8-week-old and 10-year-old lesions look similar).

Changes in an Infarct due to Reperfusion
• The current therapeutic goal in acute MIs is to salvage the maximal amount of ischemic myocardium by restoration of tissue perfusion as quickly as possible. Such reperfusion is achieved by thrombolysis, balloon angioplasty (with or without stenting), or coronary arterial bypass graft.

Changes in an Infarct due to Reperfusion
• While preservation of viable (but at-risk) heart can improve both short- and long-term outcomes, reperfusion is not a completely innocuous process.
– there is a distinct entity of reperfusion injury that can incite greater local damage than might have otherwise occurred without rapid restoration of blood flow.
• Reperfusion injury is mediated in part by oxygen free radicals generated by the increased number of infiltrating leukocytes facilitated by reperfusion.
• Reperfusion-induced microvascular injury causes not only hemorrhage but also endothelial swelling that occludes capillaries and may prevent local blood flow (called no-reflow).

• A reperfused infarct usually has hemorrhage because the vasculature injured during the period of ischemia is leaky after flow is restored.
• Irreversibly damaged myocytes subjected to reperfusion also show contraction band necrosis. Contraction bands are intensely eosinophilic transverse bands composed of hypercontracted sarcomeres (massive Ca++ arrival).
Changes in an Infarct due to Reperfusion

• It should be noted that despite timely reperfusion and salvage, ischemic (but viable) myocardium can show profound dysfunction.
• Abnormalities in cellular biochemistry may persist for several days after ischemia and lead to a noncontractile state (stunned myocardium). Such stunning can produce a state of transient reversible cardiac failure that may require pump assistance to support the patient until cardiac function returns.
Changes in an Infarct due to Reperfusion

Consequences and Complications of MI
• In-hospital death rate has declined to an overall rate of between 10% and 13% today (and to ∼7% for patients receiving aggressive reperfusion therapy).
• Unfortunately, half of the deaths associated with acute MI occur in individuals who never reach the hospital; such patients generally die within 1 hour of symptom onset-usually as a result of arrhythmias.
• The variables associated with a poor prognosis include advanced age, female gender, diabetes mellitus, and previous MI.

Consequences and Complications of MI
• The risk of developing complications and the prognosis after MI depend on
1. infarct size,
2. site,
3. fractional thickness of the myocardial wall that is damaged (subendocardial or transmural infarct).
• Nearly 75% of MI patients will experienceone or more complications

Consequences and Complications of MI
• Large transmural infarcts have a higher probability of cardiogenic shock, arrhythmias, and late CHF.
• Patients with anterior transmural infarcts are at greatest risk for free-wall rupture, expansion, mural thrombi, and aneurysm.
• Posterior transmural infarcts are more likely to be complicated by serious conduction blocks, right ventricular involvement, or both;

Consequences and Complications of MI
• Overall, however, patients with anterior infarcts have a substantially worse clinical course than those with posterior infarcts.
• Long-term prognosis after MI depends on many variables, the most important of which are the quality of left ventricular function and the extent of vascular obstructions in vessels that perfuse the remaining viable myocardium. The overall total mortality within the first year is about 30%. Thereafter, there is a 3% to 4% per year mortality

Contractile dysfunction
• A MI affects left ventricular pump function approximately proportional to its size.
• Typically, there is some degree of left ventricular failure, with hypotension, pulmonary vascular congestion, and fluid transudation into the pulmonary interstitial and alveolar spaces.
• Severe "pump failure" (cardiogenic shock) occurs in 10% to 15% of patients after acute MI, generally with a large infarct (often >40% of the left ventricle).
• Cardiogenic shock has a nearly 70% mortality rate and accounts for two-thirds of in-hospital deaths

Arrhythmias
• Following a MI, many patients developarrhythmias, which undoubtedly are responsible for many of the sudden deaths.
• MI-associated arrhythmias include
– sinus bradycardia,
– heart block,
– tachycardia,
– ventricular premature contractions or ventricular tachycardia,
– ventricular fibrillation

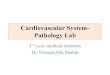
Myocardial rupture
• Rupture complicates somewhere between 1% and 5% of MIs but is a frequent cause (7% to 25%) of MI-associated demise.
• (1) rupture of the ventricular free wall, with hemopericardium and cardiac tamponade, usually fatal
• (2) rupture of the ventricular septum, leading to a new VSD and left-to-right shunt
• (3) papillary muscle rupture, resulting in severe mitral regurgitation.
1
2
3

Myocardial rupture
• Rupture can occur at almost any time after MI but is most common 3 to 7 days after infarction;
• it is at this point in the healing process that lysis of the myocardial connective tissue is maximal and the granulation tissue has not deposited sufficient collagenous matrix to buttress the wall.
• Risk factors for free-wall rupture include age older than 60 years, female gender, pre-existing hypertension, lack of left ventricular hypertrophy, and no previous MI (pre-existing scarring tends to prevent myocardial tearing).

Pericarditis
• A fibrinous or hemorrhagic pericarditis usually develops within 2 to 3 days of a transmural MI and typically spontaneously resolves with time
• It is the epicardial manifestation of the underlying myocardial inflammation.

Infarct expansion
• Because of the weakening of necrotic muscle, there may be disproportionate stretching, thinning, and dilation of the infarct region (especially with anteroseptal infarcts); this is often associated with mural thrombus

Ventricular aneurysm
• A late complication, aneurysmsof the ventricular wall most commonly result from a large transmural anteroseptal infarct that heals with the formation of thin scar tissue
• Complications of ventricular aneurysms include mural thrombus, arrhythmias, and heart failure, but rupture of the fibrotic wall does not occur

Papillary muscle dysfunction
• As mentioned above, dysfunction of a papillary muscle after MI occurs rarely as a result of rupture. More frequently, postinfarct mitral regurgitation results from ischemic dysfunction of a papillary muscle and underlying myocardium, and later from papillary muscle fibrosis and shortening, or ventricular dilation

Others
Mural thrombus
• With any infarct, the combination of a local loss of contractility (causing stasis) with endocardial damage (causing a thrombogenic surface) can foster mural thrombosis and, potentially, thromboembolism
Progressive late heart failure

Chronic Ischemic Heart Disease
• Chronic IHD, also called ischemic cardiomyopathy,is essentially progressive heart failure as a consequence of ischemic myocardial damage.
• In most instances there is a history of MI.
• Chronic IHD usually results from post-infarction cardiac decompensation that follows exhaustion of the hypertrophy of the viable myocardium. In other cases severe obstructive coronary disease may be present without prior infarction, but with diffuse myocardial dysfunction
• Severe, progressive heart failure, angina and MI. Arrhythmias are common

Morphology
• Hearts from patients with chronic IHD are usually enlargedand heavy from left ventricular dilation and hypertrophy.
• Invariably there is moderate to severe atherosclerosis of the coronary arteries, sometimes with total occlusion.
• Discrete, gray-white scars of healed infarcts are usually present.
• The endocardium generally shows patchy, fibrous thickening, and mural thrombi may be present.
• The major microscopic findings include:
– myocardial hypertrophy,
– diffuse subendocardial myocyte vacuolization,
– fibrosis from previous infarcts.

Sudden Cardiac Death (SCD)
• Affecting some 300,000 to 400,000 individuals annually in the United States, SCD is most commonly defined as unexpected death from cardiac causes either without symptoms or within 1 to 24 hours of symptom onset (different authors use different time points).
• Coronary artery disease is the most common underlying cause, and in many adults SCD is the first clinical manifestation of IHD.

In younger victims other nonatherosclerotic causes are:
• Congenital coronary arterial abnormalities
• Aortic valve stenosis
• Mitral valve prolapse
• Myocarditis or sarcoidosis
• Dilated or hypertrophic cardiomyopathy
• Pulmonary hypertension
• Hereditary or acquired abnormalities of the cardiacconduction system.
– autosomal dominant long-QT syndrome, due to mutations in various cardiac ion channels.
• Isolated myocardial hypertrophy, hypertensive or of unknown cause.
• Increased cardiac mass is an independent risk factor for SCD;

Morphology
• Severe coronary atherosclerosis with critical (≥75%) stenosis involving one or more of the three major vessels is present in 80% to 90% of SCD victims;
– acute plaque disruption is found in only 10% to 20% of these.
• Healed MI is present in about 40%, but in those who were successfully resuscitated from sudden cardiac arrest, new MI is found in only 25% or less.
• Subendocardial myocyte vacuolization indicative of severe chronic ischemia is common.
• Only a minority (10% to 20%) of cases of SCD are of nonatherosclerotic origin.
The ultimate mechanism of SCD is most often a
lethal arrhythmia, such as ventricular
fibrillation.

Prof. Pier Paolo Piccaluga
Department of Experimental, Diagnostic and Specialty Medicine
Institute of Hematology and Medical Oncology “L. and A. Seràgnoli”Bologna University Medical School
051-2144043
www.unibo.it