Embed Size (px)
Citation preview
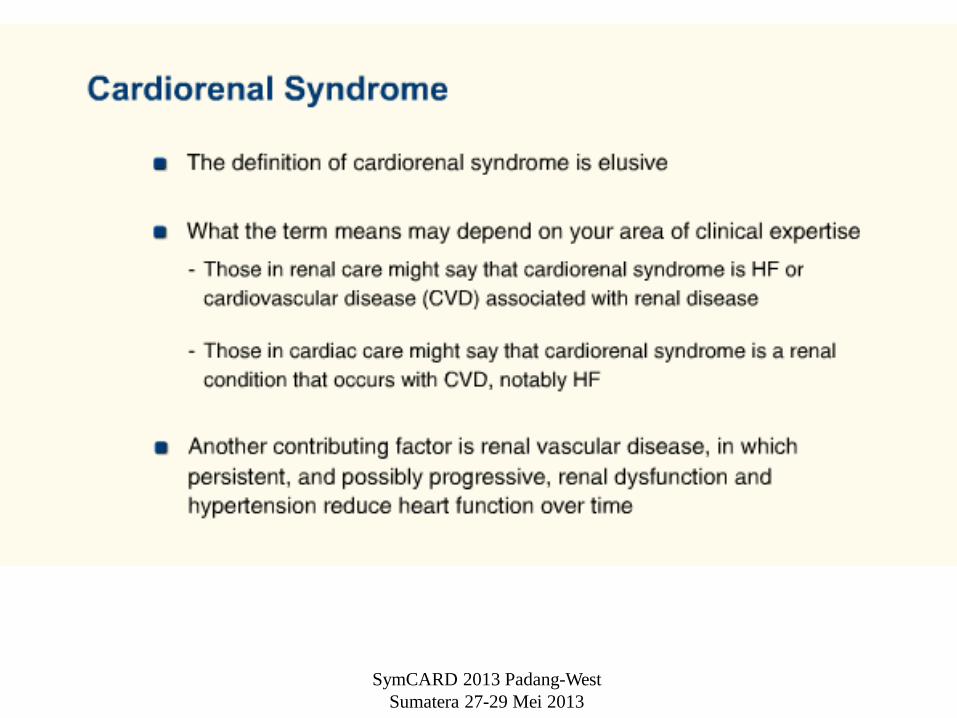
Cardiorenal Syndrome
Yerizal Karani SpPD, SpJP
SymCARD 2013 Padang-
West Sumatera 27-29 Mei 2013
• HF affects more than 5 million Americans, almost
one-half of them are rehospitalized for ADHF,
• Each year nearly 1 million pts are hospitalized
specifically for ADHF
• Prevalence of HF in US : 2.3%, 500 cases of HF /
year which can double or triple in the next 20 years
• In most patients with HF, a decrease in cardiac
contractility is associated with subendocardial
myocardial ischemia or renal impairment
SymCARD 2013 Padang-
West Sumatera 27-29 Mei
2013
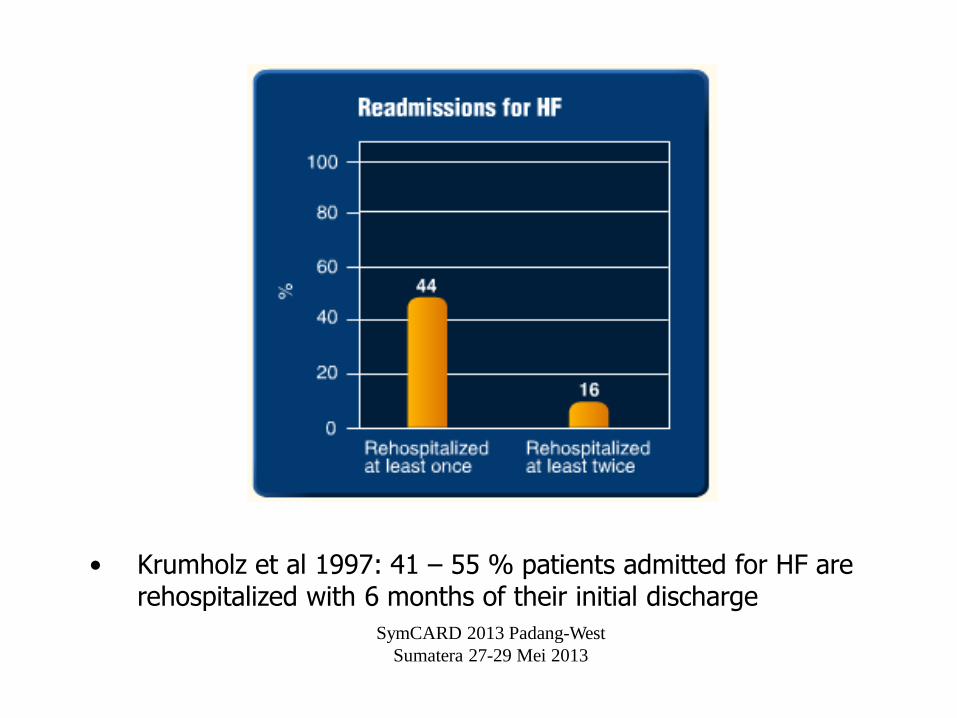
• Krumholz et al 1997: 41 – 55 % patients admitted for HF are rehospitalized with 6 months of their initial discharge
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-
West Sumatera 27-29 Mei
2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
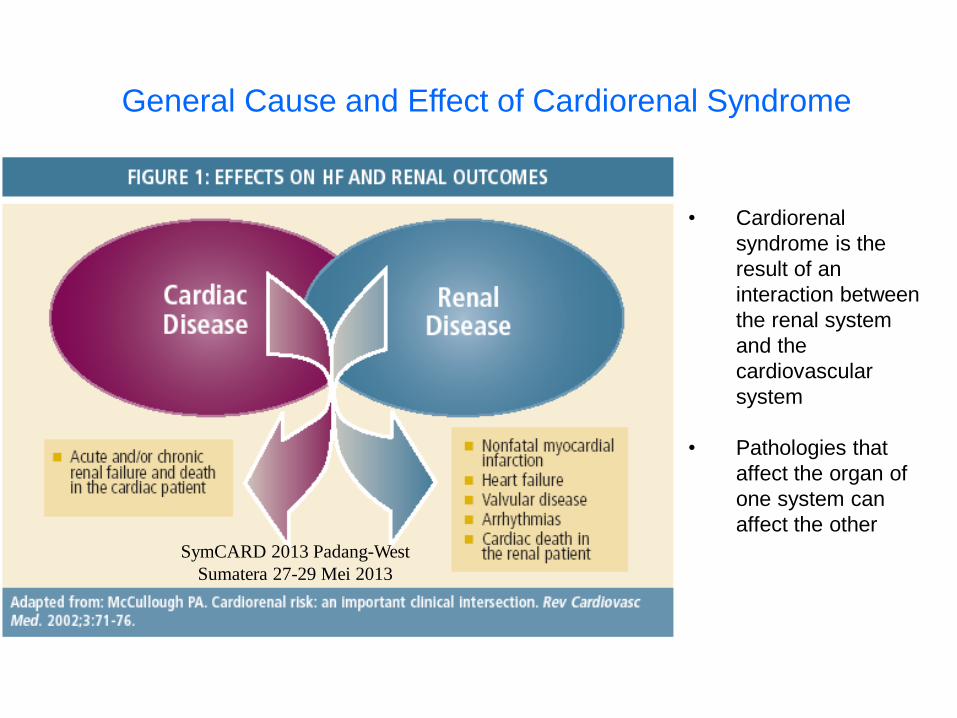
• Cardiorenal
syndrome is the
result of an
interaction between
the renal system
and the
cardiovascular
system
• Pathologies that
affect the organ of
one system can
affect the other
General Cause and Effect of Cardiorenal Syndrome
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
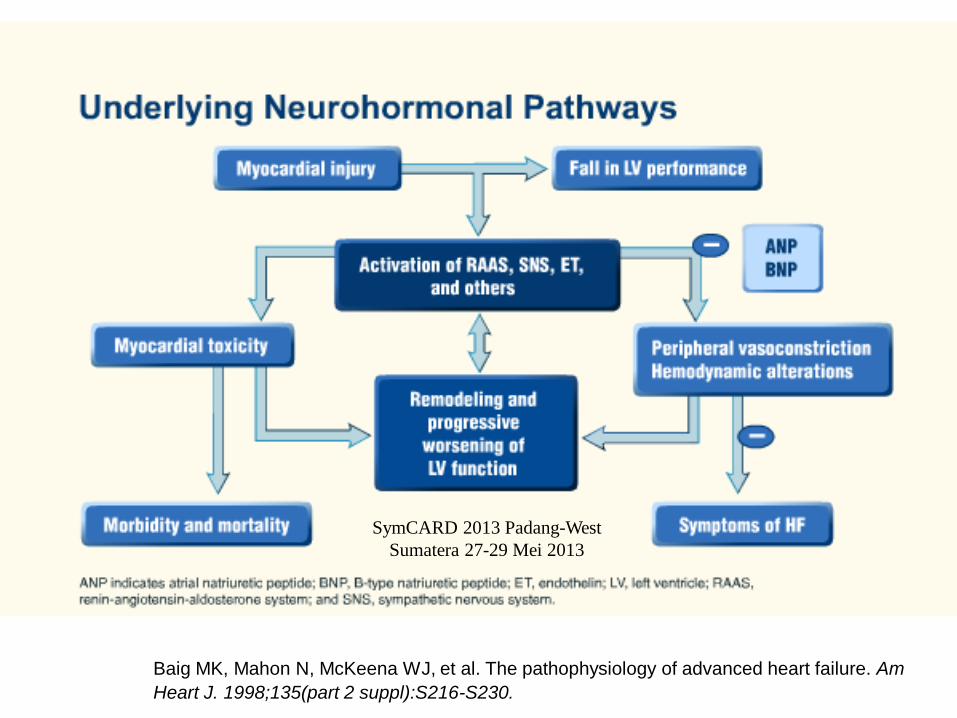
Baig MK, Mahon N, McKeena WJ, et al. The pathophysiology of advanced heart failure. Am
Heart J. 1998;135(part 2 suppl):S216-S230.
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
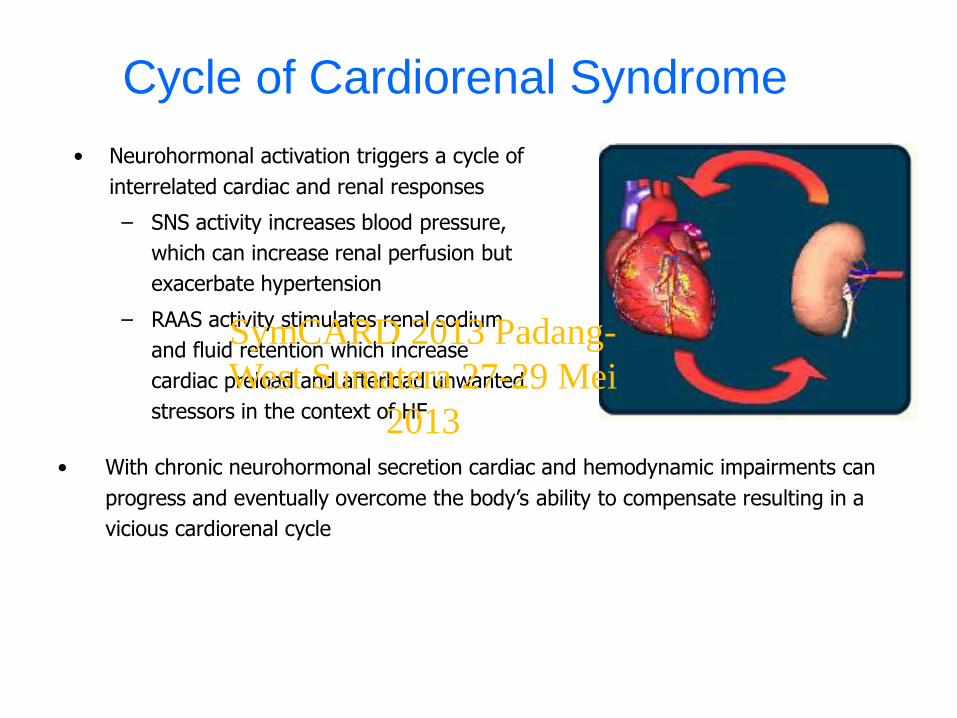
Cycle of Cardiorenal Syndrome
• Neurohormonal activation triggers a cycle of
interrelated cardiac and renal responses
– SNS activity increases blood pressure,
which can increase renal perfusion but
exacerbate hypertension
– RAAS activity stimulates renal sodium
and fluid retention which increase
cardiac preload and afterload unwanted
stressors in the context of HF
• With chronic neurohormonal secretion cardiac and hemodynamic impairments can
progress and eventually overcome the body’s ability to compensate resulting in a
vicious cardiorenal cycle
SymCARD 2013 Padang-
West Sumatera 27-29 Mei
2013
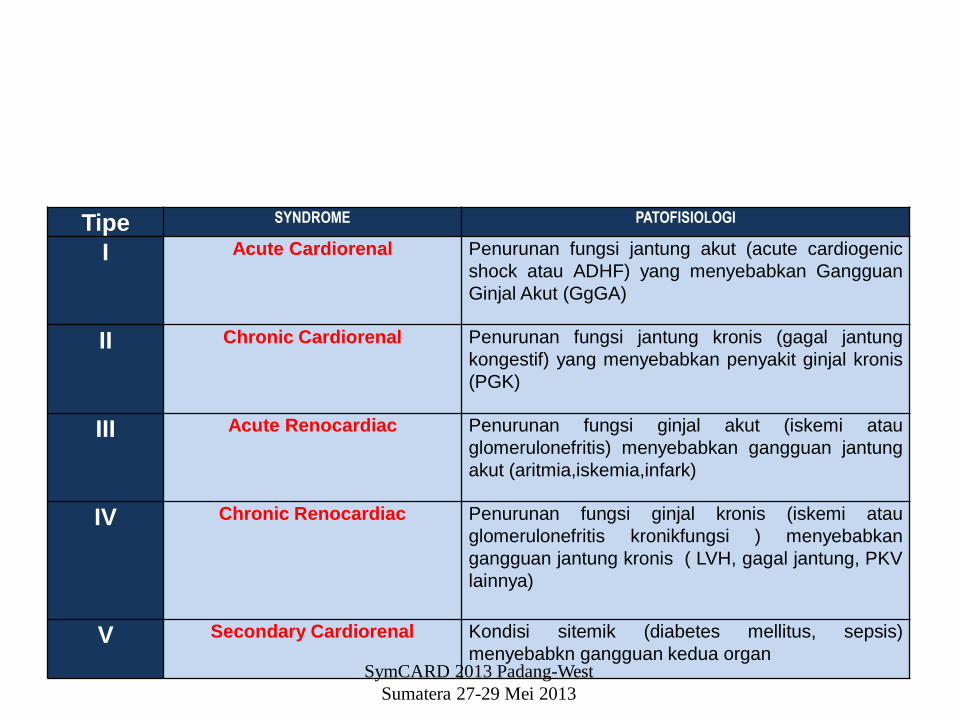
Tipe SYNDROME PATOFISIOLOGI
I Acute Cardiorenal Penurunan fungsi jantung akut (acute cardiogenic
shock atau ADHF) yang menyebabkan Gangguan
Ginjal Akut (GgGA)
II Chronic Cardiorenal Penurunan fungsi jantung kronis (gagal jantung
kongestif) yang menyebabkan penyakit ginjal kronis
(PGK)
III Acute Renocardiac Penurunan fungsi ginjal akut (iskemi atau
glomerulonefritis) menyebabkan gangguan jantung
akut (aritmia,iskemia,infark)
IV Chronic Renocardiac Penurunan fungsi ginjal kronis (iskemi atau
glomerulonefritis kronikfungsi ) menyebabkan
gangguan jantung kronis ( LVH, gagal jantung, PKV
lainnya)
V Secondary Cardiorenal Kondisi sitemik (diabetes mellitus, sepsis)
menyebabkn gangguan kedua organSymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
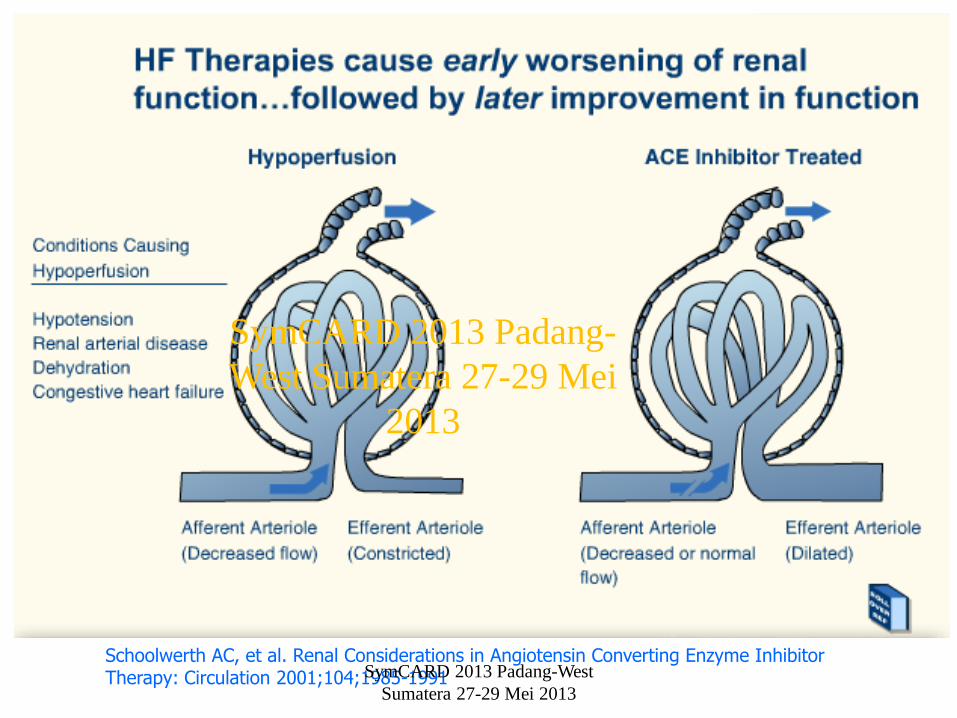
Schoolwerth AC, et al. Renal Considerations in Angiotensin Converting Enzyme Inhibitor Therapy: Circulation 2001;104;1985-1991SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-
West Sumatera 27-29 Mei
2013
Common Comorbidity of CKD
• DM
• Poorly controlled hypertension
• Elevated triglyceride levels
• Decreased HDL level
• Increased Lp(a)
• Peripheral Vascular Disease
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
Other Clinical Factors to Consider
• In addition to the types of comorbidities present, other general factors to consider are
• Patient age
• Duration of cardiac and renal impairments
• Drug therapies
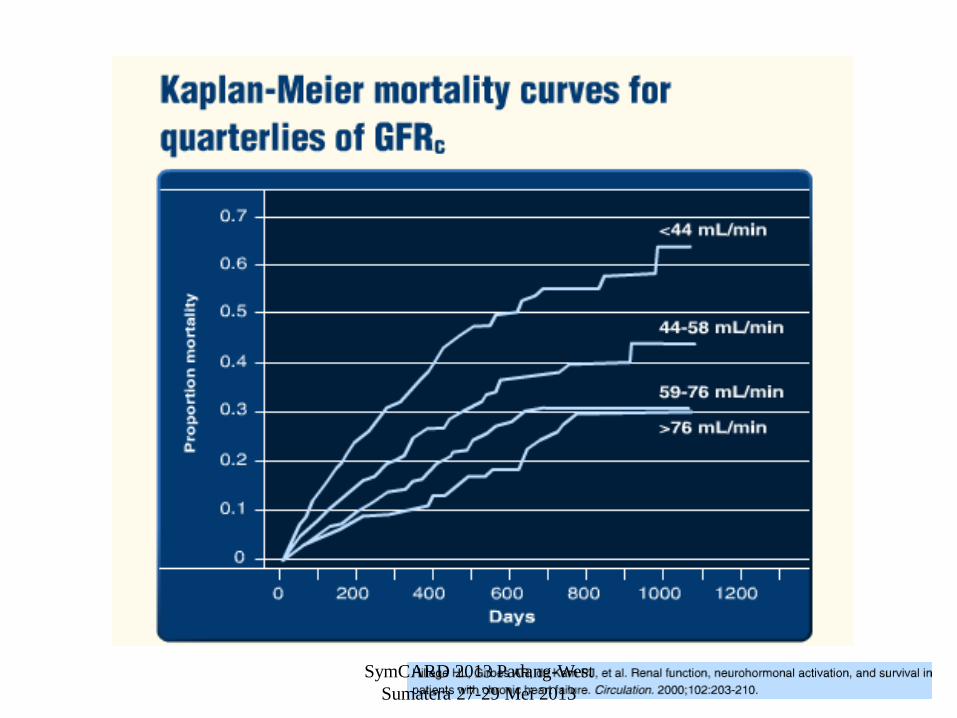
• Specific factors to consider in cardiorenal syndrome include
– Creatinine level
– Glomerular filtration rate (GFR)
• Clinical studies have shown that creatinine levels and GFR are predictive of ortality risk in patients with HF
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
• Forman DE, Buttler J Wang Y. et al. Incidence, predictors at admissions & impact of worsening renal function among
patients hospitalized with heart failure. JACC 2004;43:61-67
• Krumholz, Chen YT. Correlation and impact on outcoumes of worsening renal functions in patiens >65yo with HF. Am J
Cardiol 2000:85 (9):1110-3
Specific Factor : Creatinine Level
• In a prospective study of 412 patients hospitalized for HF,
– 75% had creatinine elevations of >0.1 mg/dL
– 24% had creatinine elevations of > 0.5 mg/dL
• Large Creatinine increases predicted the highest mortality risks
– However, even minor changes were associated with adverse
outcomes
– Large elevations were more important predictors than single
baseline measures
• In clinical practice, definitions of worsening renal function differ
– Absolute creatintie increase form >0.1 to >0.5 mg/dL
– Increase of 25% from baseline creatinine values
How we define worsening renal function will affect the number of
patients we identify as being at risk for mortality
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
Treatment of Patients with Cardiorenal Syndrome
• No evidence from clinical HF trials.
• Inhibitors of RAAS are cornerstone of management of LVs dysfnction, prevent progressive renal dysfunction in diabetic.
• ACE inhibitors elevations in creatinine, potasium
Rise in creatinine levels after initiation of ACE achieve the greatest benefit from their use
Discontinuation of ACE inh because of renal dysfunction high mortality risk (57% over an 8.5 month of study)
Continue ACE I despite a rise in creatinine, as long as renal dysfunction does not steadily deteriorate and severe hyperkalemia dos not develop
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
Diuretics
• Aggressive diuresis associated with worsening renal
function
• High diuretic dosis have been associated with
increased mortality rates
Diuretic resistance and concomitant worsening renal
dysfunction necessitate high doses of diuretics,
marker rather than a mechanism for poor outcome
• Positive inotropic agents facilitate diuresis
• Dopamine effect is severely limited in advance
heart failure
• Intravenous vasodilators improve hemodynamics,
less improve renal function
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
poor
perfusion
VOLUME
OVERLOAD
LOW
COP
INCREASED
BP
HEART
FAILURE
Clamping down
Sodium retention
RENAL
FAILURE
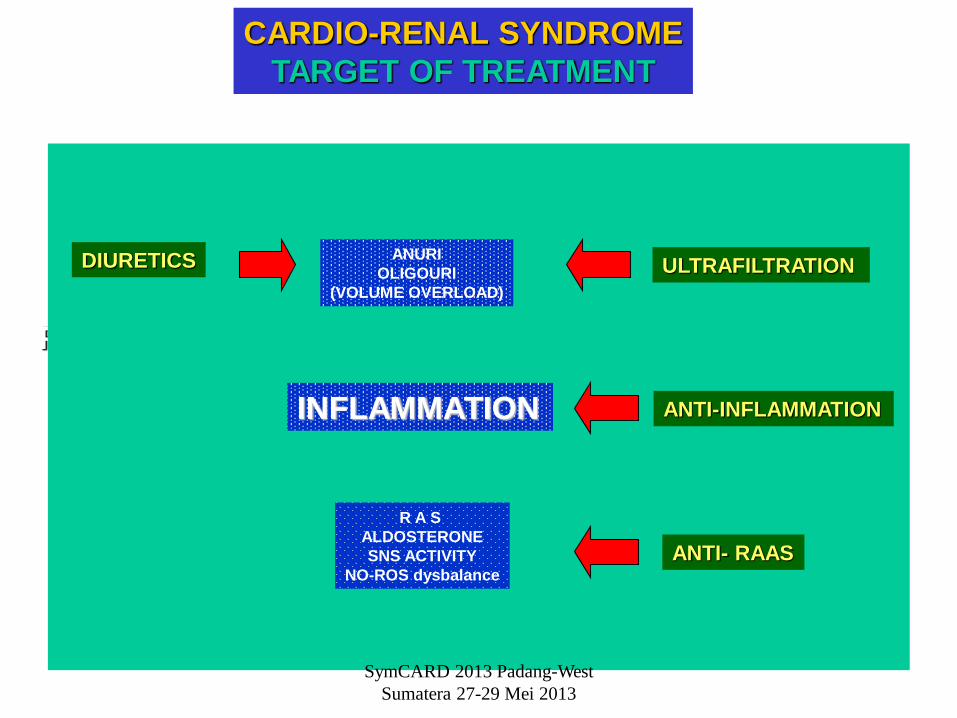
CARDIO-RENAL SYNDROME
TARGET OF TREATMENT
ANURI
OLIGOURI
(VOLUME OVERLOAD)
INFLAMMATION
R A S
ALDOSTERONE
SNS ACTIVITY
NO-ROS dysbalance
DIURETICS ULTRAFILTRATION
ANTI-INFLAMMATION
ANTI- RAAS
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
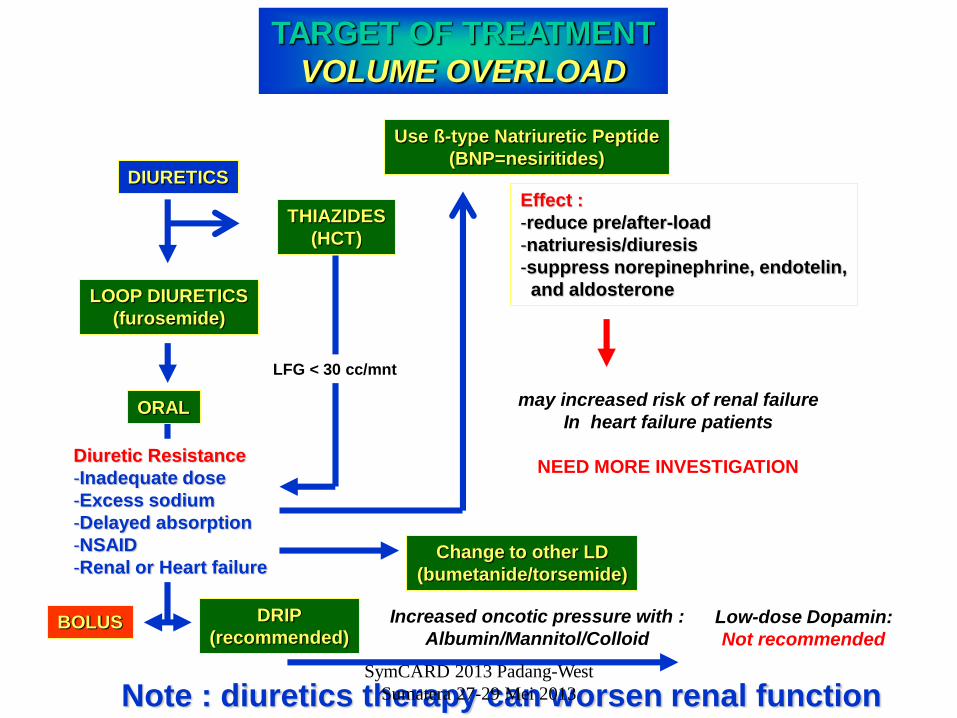
TARGET OF TREATMENT
VOLUME OVERLOAD
DIURETICS
LOOP DIURETICS
(furosemide)
ORAL
DRIP
(recommended)BOLUS
Diuretic Resistance
-Inadequate dose
-Excess sodium
-Delayed absorption
-NSAID
-Renal or Heart failure
THIAZIDES
(HCT)
LFG < 30 cc/mnt
Note : diuretics therapy can worsen renal function
Change to other LD
(bumetanide/torsemide)
Use ß-type Natriuretic Peptide
(BNP=nesiritides)
Increased oncotic pressure with :
Albumin/Mannitol/ColloidLow-dose Dopamin:
Not recommended
Effect :
-reduce pre/after-load
-natriuresis/diuresis
-suppress norepinephrine, endotelin,
and aldosterone
may increased risk of renal failure
In heart failure patients
NEED MORE INVESTIGATION
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
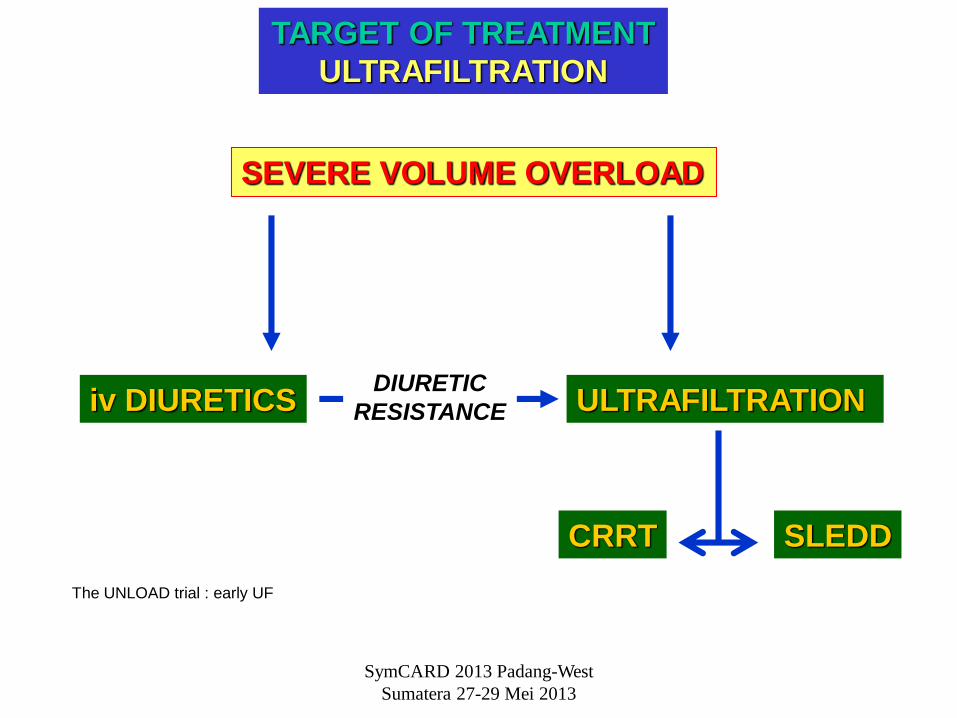
TARGET OF TREATMENT
ULTRAFILTRATION
SEVERE VOLUME OVERLOAD
iv DIURETICSDIURETIC
RESISTANCE ULTRAFILTRATION
CRRT SLEDD
The UNLOAD trial : early UF
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013
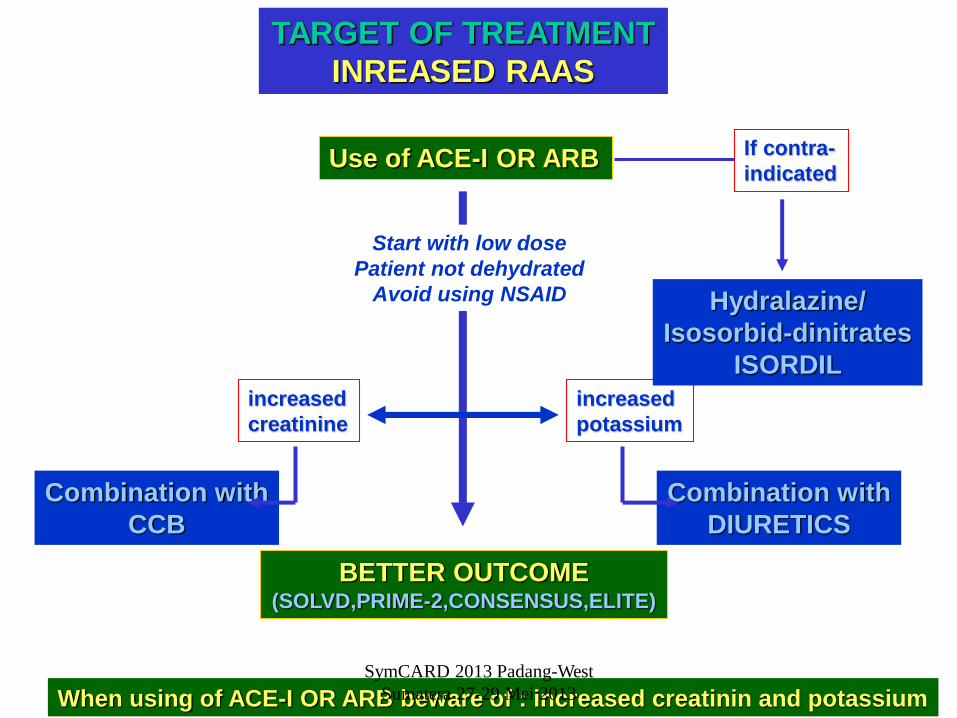
TARGET OF TREATMENT
INREASED RAAS
Use of ACE-I OR ARB
Start with low dose
Patient not dehydrated
Avoid using NSAID
When using of ACE-I OR ARB beware of : increased creatinin and potassium
BETTER OUTCOME(SOLVD,PRIME-2,CONSENSUS,ELITE)
increased
potassium
increased
creatinine
Combination with
CCB
Combination with
DIURETICS
If contra-
indicated
Hydralazine/
Isosorbid-dinitrates
ISORDIL
SymCARD 2013 Padang-West
Sumatera 27-29 Mei 2013




![Cardiorenal biomarkers in acute heart failure · characterized as cardiorenal syndrome.[10,11] Ronco et al.,[11] proposed the definition for cardiorenal syndrome as, “disorders](https://img.pdfslide.us/doc/110x75/5f0c081e7e708231d43369b5/cardiorenal-biomarkers-in-acute-heart-failure-characterized-as-cardiorenal-syndrome1011.jpg)



![[AIESEC UNAND 1415] Summer Market Research Analysis in UNAND](https://img.pdfslide.us/doc/110x75/55d58aa2bb61eb61078b45fe/aiesec-unand-1415-summer-market-research-analysis-in-unand.jpg)