-
1Primary PCI VS Thrombolysis inSTEMI, Positional Statement
Primary PCI VS Thrombolysis inSTEMI, Positional Statement
Ahmed Magdy, MD, FACC, FSCAINational Heart
Institute
Change in Approach to AMIChange in Approach to AMI
19902002 20032011
AcuteMI
Lytic
AcuteMI
FacilitatedLytic/LMWH
Transfer for Cath with Lytic failureTransfer emergently all
patients
-
22007 focused update of the ACC/AHA STEMI guidelines
Reperfusion Therapy in STEMI
-
3Importance of Rapid Time toTreatment With Fibrinolysis in
STEMI
Importance of Rapid Time toTreatment With Fibrinolysis in
STEMI
33 55% %
44..00Ab
solu
te %
diff
eren
ce
Abso
lute
% d
iffer
ence
in
mor
talit
y at
in m
orta
lity a
t 35 35
day
sda
ys 33..55% %
2.5% 2.5%
1.8%1.8% 1.6% 1.6%
1.01.0
33..00
2.02.0
Time from onset of symptoms to treatment (hours)Time from onset
of symptoms to treatment (hours)
00..55% % 0.00.0 0 0 11 2 2 33 4 4 66 7 7 1212 12 12 2424
The Fibrinolytics Therapy Trialists collaborative group. The
Fibrinolytics Therapy Trialists collaborative group. LancetLancet.
. 19941994;; 343343::311311. .
PCI In-hospital Mortality vs Door to Balloon TimePCI In-hospital
Mortality vs Door to Balloon Time
12.214
4.96.1
8
4
6
8
10
12
In-hospDeath
N= 2,322
0
2
Door to Balloon Time (hours)
DeathRate
0-1.4 1.5-1.9 2.0-2.9 >3.0
Brodie BR, JACC 47, 2006
N=384 N=493 N=750 N=673
-
4(%)
(%)
DD
100100
8080
III. Timely Reperfusion1. Time is Myocardium
2. Infarct Size is Outcome
Symptom onset to hospArrival 2 hr Shift i t ith
BB
CC
AAExtent ofExtent ofMyocardial SalvageMyocardial Salvage
Mor
talit
y R
educ
tion
Mor
talit
y R
educ
tion
6060
4040
2020
Arrival 2 hr
Thrombolysis given, 2 hr
lysis induced reperfusion 3 hr onset to balloon 3 hr
Shifts in outcome with different ttt strategiesA to B no
benefitA to C BenefitB to C BenefitD to B HarmD to C Harm
Myocardial SalvageMyocardial Salvage0000 44 88 1212 1616 2020
2424
Time From Symptom Onset to Reperfusion Therapy, hTime From
Symptom Onset to Reperfusion Therapy, h
Critical TimeCritical Time--dependent Perioddependent
PeriodGoal: Myocardial SalvageGoal: Myocardial Salvage
TimeTime--independent Periodindependent PeriodGoal: Open
InfarctGoal: Open Infarct--Related ArteryRelated Artery
Gersh BJ, et al. Gersh BJ, et al. JAMAJAMA. .
20052005;;293293::979979..
Primary PCI vs Lysis for STEMI Meta-analysis of 23 trials
Primary PCI vs Lysis for STEMI Meta-analysis of 23 trials
PCI is better than LYSIS!
2468
10121416
PTCAThrombolytic
P=0.0003P
-
5Recent Influences of PracticeSalvage is Time Dependant
Recent Influences of PracticeSalvage is Time Dependant
Superiority of PPCI over fibrinolysis if Door-Superiority of
PPCI over fibrinolysis if Doorto-Balloon completed in a timely
fashion
Acknowledgement that Time Matters in PPCIg Recommendations for
time to reperfusion updated
Mortality rates with primary PCI as a function of PCI-related
time delay
ce in
ce
in
15 Circle sizes = sample size of the
P = 0.006
ute
Ris
k D
iffer
enc
ute
Ris
k D
iffer
enc
Dea
th
Dea
th (%
)(%
)
05
10
individual study.Solid line= weighted meta-regression.
62 min
BenefitFavors PCI
BenefitFavors PCIHH
0 20 40 60 80 100PCI-Related Time Delay (door-to-balloon - door
to needle)
Abs
olu
Abs
olu
-5
Nallamothu BK, Bates ER. Am J Cardiol. 2003;92:824-6
HarmFavors Lysis
HarmFavors Lysis
For Every 10 min delay to PCI: 1% reduction in mortality
difference towards lytics
-
6*PPCI Better > Pre-Hospital Lysis > In-Hospital Lysis
*PPCI Better > Pre-Hospital Lysis > In-Hospital Lysis
*Transfer for PCI is better than LYSIS! (In a timely manner)
*Transfer for PCI is better than LYSIS! (In a timely manner)
-
7Assessing Reperfusion Options for Patients with STEMI1
Assessing Reperfusion Options for Patients with STEMI1
STEP 1: Assess time from symptom onset, risk of STEMI, risk of
thrombolysis, time for transport to PCI lab
STEP 2: Determine whether fibrinolysis or invasive strategy is
preferred*
FibrinolysisFibrinolysis preferred if:preferred if: Invasive
strategy preferred if:Invasive strategy preferred if: Early
presentation (3 hours) Late presentation (>3 hours)Late
presentation (>3 hours) Diagnosis of STEMI is in doubtDiagnosis
of STEMI is in doubt
*If presentation is
-
8PCI post thrombolysis in STEMI:PCI post thrombolysis in
STEMI:
Prehospital TL+ immediate transfer
Delayed PCIb f di h immediate transfer
Rescue PCIfor failed TL
-
9PCI post thrombolysis in STEMI: RATIONALE
PCI post thrombolysis in STEMI: RATIONALE
1 Ri k f reocclusion hi h1. Risk of reocclusion high2. Early
angiographic risk stratification3. High likelihood of residual
complex
stenosis despite successful TL Rxstenosis despite successful TL
Rx
REACT: 6 month Primary compositeREACT: 6 month Primary
composite(Death, MI, CVA, or severe heart failure)
Rescue PCI is better than Lysis!!
31.0
15.3
29.8
15
20
25
30
35
%
The primary composite endpoint of death, MI, CVA or severe heart
failure at 6 months was significantly lower in the rescue PCI group
compared
p
-
10
PCI i b tt th
PCI i b tt this better than
Facilitated PCI????
is better than Facilitated PCI
????
-
11
-
12
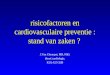
Primary, secondary and bleeding end points in FINESSE
Primary, secondary and bleeding end points in FINESSE
End pointsEnd points Primary Primary PCI (%) PCI (%)
AbciximabAbciximab+PCI%) +PCI%)
(abcixima/(abcixima/reteplase)reteplase)--facilitated PCI
facilitated PCI (%)(%)
p, p, combined+ combined+ PCI vs PCI vs primary PCI primary
PCI
p, combin p, combin +PCIvs +PCIvs abciximababciximab--facilitate
facilitate (%) (%)
Primary end Primary end point* point*
10.710.7 10.510.5 9.89.8 NSNS NSNS
AllAll--cause cause mortality mortality
4.54.5 5.55.5 5.25.2 NSNS NSNS
Complications Complications of MI of MI
8.98.9 7.57.5 7.47.4 NSNS NSNS
Death Death 4.54.5 5.55.5 5.25.2 NSNS NSNS
TIMI major TIMI major bleeding bleeding
2.62.6 4.14.1 4.84.8 0.0250.025 NSNS
TIMI minor TIMI minor bleeding bleeding
4.34.3 6.06.0 9.79.7
-
13
Immediate PCIImmediate PCIImmediate PCI is better than
LYSIS +/- Delayed PCI!
Immediate PCI is better than
LYSIS +/- Delayed PCI!
-
14
SIAM SIAM 3 3 Event Free SurvivalEvent Free Survival
(Death, Re(Death, Re--infarction, Intervention,
Ischemia)infarction, Intervention, Ischemia)
SIAM SIAM 3 3 Event Free SurvivalEvent Free Survival
(Death, Re(Death, Re--infarction, Intervention,
Ischemia)infarction, Intervention, Ischemia)
-
15
Pharmacoinvasive (Facilitated) PCI
Pharmacoinvasive (Facilitated) PCI(Facilitated) PCI
is better than Lytic +Rescue PCI
(Facilitated) PCI is better than Lytic +
Rescue PCI
-
16
-
17
Comments on CARESSComments on CARESS
Again use of potent antiplatelet agent Again use of potent
antiplatelet agent (abciximab), platelets inactivated at time of
PCI, (In ASSENT IV < 10% use!!)
Bleeding reassuring as pts > 75yo excluded Median time from
TL Rx to PCI 212 minMedian time from TL Rx to PCI 212 min
Post-Lysis PCI studiesPost-Lysis PCI studies
50 660 GRACIAGRACIA--11SIAM IIISIAM III CAPITAL MICAPITAL MI
CARESSCARESS
25.6
50.6
2124.4
20
30
40
50 PCI"Conservative"N=N=14361436
9 11.64.1
11.1
0
10
20
refractIs/D/MI/TLR
D/MI/Revasc D/MI/UA/stoke refract Is/D/MI
P=0.001 P=0.0008 P=0.04 P=0.001
-
18
CommunityCommunityHospitalHospitalEmergencyEmergency
TNK + ASA + Heparin / Enoxaparin + ClopidogrelTNK + ASA +
Heparin / Enoxaparin + Clopidogrel
PharmacoinvasivePharmacoinvasiveStrategyStrategy
High Risk ST Elevation MI within High Risk ST Elevation MI
within 12 12 hours of symptom onsethours of symptom onset
Standard TreatmentStandard Treatment
PCI CentrePCI Centre
EmergencyEmergencyDepartmentDepartment
CathCath / PCI within 6 hrs / PCI within 6 hrs regardless of
regardless of
reperfusion statusreperfusion status
Cath and Rescue Cath and Rescue PCI PCI GP IIb/IIIa GP
IIb/IIIa
InhibitorInhibitor
gygyUrgentUrgent Transfer to PCI CentreTransfer to PCI
Centre
Assess chest pain, STAssess chest pain, ST
resolutionresolutionat at 6060--90 90 minutes after
randomizationminutes after randomization
Failed Reperfusion*Failed Reperfusion* Successful
ReperfusionSuccessful Reperfusion
Elective Cath Elective Cath PCIPCI
>> 2424 hrs laterhrs laterPCI CentrePCI CentreCath LabCath
Lab
reperfusion statusreperfusion status InhibitorInhibitor >
> 24 24 hrs laterhrs later
* ST segment resolution < 50% & persistent chest pain, or
hemodynamic instability* ST segment resolution < 50% &
persistent chest pain, or hemodynamic instability
Repatriation of stable patients within 24 hrs of PCI
Randomization stratified by age (Randomization stratified by age
(75 75 vs. > vs. > 7575) and by enrolling site) and by
enrolling site
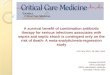
141416161818 1616..66
% of Patients% of Patients
Primary Endpoint: Primary Endpoint: 3030--Day Death, reDay
Death, re--MI, MI, CHF, Severe Recurrent Ischemia, CHF, Severe
Recurrent Ischemia,
Shock Shock
446688
101012121414
1010..66
Standard PCI > 24 hrs (n=496)Standard PCI > 24 hrs
(n=496)
OR=0.537 (0.368, 0.783); p=0.0013
0022
00 55 1010 1515 2020 2525 3030Days from RandomizationDays from
Randomization
Invasive < 6 hrs (n=508)Invasive < 6 hrs (n=508)
n=496n=496n=508n=508
422422468468
415415466466
415415463463
414414461461
414414460460
412412457457
-
19
SummarySummary Pharmacoinvasive Strategy of routine early
PCI within 6 hrs after thrombolysis is associated with a 6%
absolute (46% relative) ( )reduction in the composite of death,
re-MI, recurrent ischemia, HF and shock
is not associated with any increase in transfusions, severe
bleeding despite high
f GP IIb/III i PCIuse of GP IIb/IIIa in PCI Benefit seen despite
high cath/PCI rates in
Standard Treatment group (including ~40% rescue PCI)
-
20
Observational prospective database (July 2007
Thrombolysis catching up with PCI in STEMI, especially in
lower-risk patientsThrombolysis catching up with PCI in
STEMI, especially in lower-risk patients
to December 2009) of patients with STEMI admitted to 73 Belgian
hospitals: 25 hospitals had PCI facilities and 48 hospitals did
not.
Outcome was in-hospital mortality, and patients were stratified
into low intermediate andwere stratified into low, intermediate,
and high risk according to TIMI score.
Arch Intern Med 2011; 171: 544-9
-
21
Thrombolysis catching up with PCI in STEMI, especially in
lower-risk
patients
Thrombolysis catching up with PCI in STEMI, especially in
lower-risk
patients
There were 5 295 eligible patients in the There were 5,295
eligible patients in the registry, 4,574 (86.4%) were treated with
primary PCI and 721 (13.6%) received thrombolysis. Of those
receiving thrombolysis, 603 (83.6%) underwent subsequent
invasive
l i TIMI i k l ievaluation. TIMI risk scores were low in 1,934,
intermediate in 2,382, and high in 979.
Arch Intern Med 2011; 171: 544-9
In hospital mortality was similar in the two
Thrombolysis catching up with PCI in STEMI, especially in
lower-risk patientsThrombolysis catching up with PCI in
STEMI, especially in lower-risk patients
In-hospital mortality was similar in the two groups, 5.9% (PCI)
vs. 6.6%, and after adjustment for baseline risk profile the
difference was significant only in the high-risk group
-
22
The authors conclude that in current practice
The authors conclude that in current practice
thrombolysis is normally followed by invasive y y yintervention,
immediate PCI only has an advantage for in-hospital mortality in
patients at high risk.
Early thrombolysis followed by later invasive l ti t b i t d l d
PCIevaluation seems to be superior to delayed PCI
when door to balloon time is over 60 minutes.
In summary: European GLIn summary: European GL
-
23
(From 2007 STEMI Update, Section 5)(From 2007 STEMI Update,
Section 5)
1. Facilitated PCI using regimens other than full-dosefib i l ti
th i ht b id dfibrinolytic therapy might be considered as a
reperfusion strategy when all of the following are present: a.
Patients are at high risk, b. PCI is not immediately available
within 90 yminutes, c. Bleeding risk is low (younger age, absence
of poorly controlled hypertension, normal body weight). (Level of
Evidence: C)
2009 Joint STEMI/PCI Focused Update2009 Joint STEMI/PCI Focused
Update Class IIa1. It is reasonable for high-risk* patients who
receive
fibrinolytic therapy as primary reperfusion therapy at a non PCI
capable facility to be transferred asnonPCI-capable facility to be
transferred as ASAP to a PCI-capable facility where PCI can be
performed either when needed or as a pharmaco-invasive
strategy.
Consideration should be given to initiating a preparatory
antithrombotic (anticoagulant plus antiplatelet) regimen before and
during patient transfer to the catheterization laboratory
(14,15).
(Level of Evidence: B)
-
24
Both Discourage Facilitated Reperfusion Both Endorse Newer
Anticoagulants
" bl " t f
Latest European and US STEMI Guidelines Compared and
Contrasted
Latest European and US STEMI Guidelines Compared and
Contrasted
both note it would be "reasonable" to perform early angiography
for risk stratification in patients not undergoing primary PCI, but
the ESC goes a step further by supporting routine angiography (with
PCI if indicated) 3 to 24 hours after successful fibrinolysis based
on several recent studies, including the GRACIA trials.
What conclusions can we make!What conclusions can we make!
PCI centers should do PCI (in a timely manner
-
25