Embed Size (px)
Citation preview

Cardiac output and pulmonary blood volume in dogs.
Comparison of three indicator-dilution methods
Gilbert0 Sanchez, M.D. Antonio C. Quiroz, M.D. George E. Bwch, M.D.* Nicholas P. DePtrsqade, M.D.
New Orleclns, I-u.
I n spite of limitations, but because of its convenience, the indicator-dilution
method is widely used in the estimation of cardiac output. According to the Stewart- Hamilton principle, If2 if a known concen- tration of indicator is injected rapidly into the central circulation, cardiac output can be estimated from the indicator time- concentration curve inscribed during con- tinuous sampling from a peripheral artery. Furthermore, the mean transit time of the indicator from the site of injection to the site of sampling multiplied by cardiac output represents the circulating blood volume between the two sites.
Several techniques for estimating pul- monary mean transit time have been described.a-6 These techniques differ pri- marily in the site in the circulation at which indicator is injected and withdrawn. However, since cardiac output as well as pulmonary mean transit time are esti- mated from the indicator time-concentra- tion curve, the various techniques differ not only in the calculation of pulmonary mean transit time but in the calculation of cardiac output as well.
The purpose of the present study was to compare cardiac output and pulmonary blood volume determined in each of 15 dogs by means of three indicator-dilution techniques as well as by the Fick principle.
Material and methods
Cardiac output and pulmonary blood volume were determined in 15 adult mon- grel dogs whose weight ranged from 16.2 to 20.0 kilograms. The dogs were anes- thetized lightly with intravenous urethane (1.5 Gm. per kilogram). After the insertion of an endotracheal tube the dogs were taped supine on a Aat fluoroscopic table and administered 100 per cent oxygen mixed with room air at a constant rate of 3 L. per minute.
Three red Kifa catheters of the same length, internal diameter, and volume (0.75 ml.) were positioned as follows: (1) in the pulmonary artery just distal to the pulmonic valve, (2) in the superior vena cava, and (3) in the femoral artery. A yellow Kifa catheter was passed trans- septally into the left atrium, With the aid of the pressure tracing and fluoroscopic
From the Department of Medicine, Tulane University School of Medicine, and the Charity Hospital of Louisiana, New means, La.
Supported by grants from the United States Public Health Service. Kowell A. Hillups Fund for Research in Heart Disease, and the Rudolph Matas Fund for the Kate Prewitt Hess Laboratory.
Received for publication June 29.1966. *Address: Department of Medicine, Tulane University School of Medicine, 1430 Tulane Ave., Sew Orlelrns, La.. 70111.
665

control, the tip of the catheter was po- sitioned carefully just at the atrial side of the mitral valve.
Dye-dilution curves were recorded by means of two similarly calibrated Gilford densitometers with single-stage amplifiers whose outputs were fed into D.C. ampli- fiers of a multichannel Electronics for 1,ledicine oscillographic recorder. Calibra- tions were made by passing known con- centrations of dye-labeled blood through the densitometers connected in series. The outputs of both densitometers were found to be linear, and a full-scale deflection was obtained with a dye concentration of 2.5 mg. per liter. Constant withdrawal at a rate of 0.42 ml. per second was made by use of a Harvard infusion-withdrawal pump (!lIodel 600-930).
Jndocyanine dye (Cardio-Green), 1.0 to 1.6 ml. of 1.25 mg. per ml. was intro- duced instantaneously into the circulation, using a Cornwall syringe with the auto- matic pipetting device removed. The exact amount of dye injected was de- termined by subtracting the volume of dye in the catheter from the total volume of dye injected. Cardiac output and mean transit time were calculated from the dye-dilution curves as described by Hamilton, Noore, Kinsman and Spur- ling.* Calculated catheter delays (transit time in seconds from the tip of the catheter to the cuvettes) were subtracted from the respective determinations of mean transit time.
Cardiac output and pulmonary blood volume were determined in each of the 15 dogs, utilizing three previously described methods, as follows:
In Method 1,“~~ indicator was injected into the pulmonary artery (PA) and sam- pled from the left atrium (LA). Cardiac output (CO) and pulmonary mean transit time in seconds (XlTTp) were both calcu- lated from the indicator time-concentration curve inscribed. Pulmonary blood volume (Pl3\7) was calculated as follows:
PBV= (M’I‘TI~A to LA) X CO (1)
In Method II,5 indicator was introduced into the pulmonary artery and left atrium in rapid succession and sampled from the femoral artery after both injections. Car- diac output was calculated from the pul-
monary artery to femoral artery indicator time-concentration curve. Pulmonary mean transit time is equal to the difference l)e- tween the transit times from the pulmonary artery to the femoral artery and left atrium to femoral artery (FA), so that
r ,. I’RV = (M I.1 P?, I‘, 114 ) - (M’l‘?i’r.,\ ,U F.&)X CO (2)
In Method III,” indicator was introduced into the superior vena cava (WC) and sampled simultaneously from the pulmo- nary artery and left atrium. Cardiac out- put was calculated from the superior vena cava to left atrium indicator time-concen- tration curve. Pulmonary mean transit time is equal to the difference between the transit times from the superior vena cava to the left atrium and superior vena cave to pulmonary artery, so that
PBV= (M’I’Tsvc to J,A) - (M’ITsv~ t,, Y.A) x CO (3)
Cardiac output was also measured in each animal, using the direct Fick method. Accordingly, expired air was collected in a Douglas bag for 10 minutes, and samples of arterial and venous blood were obtained at the beginning and at the end of the lo-minute period. The volume of the expired air was measured with a Tissot gasometer, and the samples were analyzed for oxygen and carbon dioxide in duplicate by the Scholander method.7 The oxygen content of the samples of arterial and venous blood was determined in duplicate, utilizing the Roughton-Scholander micro- method.8
All measurements of cardiac output and pulmonary blood volume were related to body weight.
Results
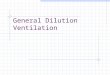
Cardiac output. There were no consistent differences among the cardiac output values determined by the three indicator- dilution methods (Fig. 1). Each of the indicator-dilution methods tended to yield higher values for cardiac output than did the direct Fick method (Fig. 2). However, there was no statistically significant dif- ference in cardiac output between the means of any of the methods regardless of how they were paired.
Pulmonary mean transit time. It can be seen from Fig. 3 that the values for pul- monary mean transit time determined by

00 I00 200 300
C.O. (cc. /min./Kg.) hfE,THODS Z, Ri-
MJJp (Ssc) METHODS l?-, ZZ’
Fig. 1. Cunrparison of wrdiac output x4ues de- tcrmined 1)~ the three indicator-dilrltioll methods.
C 0. (cc/m/n /Kg ) FI8.K (cc/Kg.)
FfCK ME THUD METHODS IT, iZ?
Fig. 2. Comparison of cardiac output values de- termined by the three indicator-dilution methods with that determined by the Fick method.
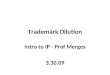
Fig. 4. Comparison of pulmonary blood volumes de- termined by the three indicator-dilution methods.
Methods 11 and III are in close agreement. Method I yielded consistently higher values for pulmonary mean transit time than did ;\iIethod II or lJIethod III. The difference between the means of Methods II and III was not statistically significant, whereas the differences between the means of RIethods I and II and Methods I and III were highly significant (p < 0.001).
Pulmonury blood volume. There was good agreement in pulmonary blood volumes between Llethods II and III (Fig. 4). Alethod I produced consistently higher
values for pulmonary blood volume than did either Method 11 or YIethod III (Fig. 4). The difference between the means of J’lethods II and III was not statistically significant, whereas the difference between the means of Methods I and II and YIeth- ods I and III xere highly significant (p < 0.001).
Discussion
Each of the four methods utilized in this study yielded comparable determinations of cardiac output. However, 31ethod I

produced consistently higher values for pulmonary mean transit time and pul- monary blood volume than did Method II or Method III. In addition, Riethod I resulted in much greater scatter in pul- monary mean transit time and pulmonary blood volume than did either Jlethod II or Method IIJ. For example, the standard error for the 15 determinations of pul- monary blood volume with Method I was hO.84, whereas for Methods II and III the standard errors were ho.48 and rtO.41: respectively.
The higher values of pulmonary blood volume for Method I, as compared to those for Method II or Method III, are obviously due to the longer mean transit times obtained with Method I. The pro- longed mean transit times obtained with h’lethod I were most likely due to the fact that the dye was injected into the pul- monary artery and did not traverse ;I mixing chamber before it was sampled. It is interesting that the mean transit time determined by RIethod III agreed well with that determined by Method II. In nlethod III the right ventricle is the mixing chamber, and in YIethod II the left ven- tricle is the mixing chamber. Thus, in so far as the present study is concerned, the right ventricle was as adequate as the left ventricle as a mixing chamber.
Pulmonary blood volume in dogs de- termined by direct bleed-out was found to be 8.0 ml. per kilogram.g Thus, Methods II [mean 8.03 ml. per kilogram) and III (mean 8.71 ml. per kilogram) were in closer agreement with the direct bleed-out determinations than was hlethod I (mean 13.6 ml. per kilogram).
From these experiments it would appear that determinations of pulmonary blood volume by the indicator-dilution method are more accurate when dye is injected in rapid succession into the pulmonary artery and left atrium and sampled from the femoral artery (Method II), or when dye is injected into the superior vena cava and sampled simultaneously from the pulmo- nary artery and left atrium (Method III), than when dye is injected into the pul- monary artery and sampled from the left atrium (Method I). Method III has the advantage of requiring only a single injec-
tion of dye. This is particularI>. import;illl in experiments which require rapid de- terminations of pulmonary blood volurn~=.
Conclusion Three indicator-dilution methods for
determining cardiac output and pulmonary blood volume were compared in 15 dogs. Injection of dye into the pulmonary artery and sampling from the left atrium (I2Iethod I) yielded consistently longer pulmonary mean transit times and higher pulmonary blood volumes than did injection of dye into the pulmonary artery and left atrium ivith sampling from the femoral artery (Rlethod II) or single injection of dye into the superior vena cava with simultaneous sampling from the pulmonary artery and left atrium (Rfethod III). Although meas- urements of cardiac output determined by the three indicator-dilution methods as well as by the Fick principle were in good agreement, there was considerable scatter among the individual values in all methods.
1.
2.
1 . .
4.
5.
6.
7.
8.
9.
REFERENCES
Stewart, G. N.: The pulmonary circulation time, quantity of blood In lungs and output of blood. Am. 1. Phvsiol. 58:20. 1921. Hamilton, iV. 6, Moore, J. W., Kinsman, J. M., and Spurling, R. G.: Studies on circulation; further analysis of injection method, and of changes in hemodynamics under physiological and pathological conditions, Am. J. Physiol. 99:534, 1932. Hyman, A. I,., and *Myers, W. S.: Hemody- namic changes following pulmonary emboliza- tion, Circulation 26:73.5-1662. - Levinson. G. E.. Frank. M. I.. and Hellems. H. K. : The pulmonary vascular volume in man: Measurement from atrial dilution curves, AM. HEAKT J. 67:734,1964. Milnor, W. R., Jose, A. D., and McGaff, C. J.: Pulmonary vascular volume, resistance and compliance in man, Circulation 22:130, 1960. De Freitas, F. M., Faraco, E. Z., Nedel, N., De Azevedo, D. F., and Zaduchliver, J.: De- termination of pulmonary blood volume by single intravenous injection of one indicator in patients with normal and high pulmonary vascular pressure, Circulation 30:370, 1964. Scholander, P. F.: Analyzer for accurate esti- mation of respiratory gases in one-half cubic centimeter samples, J. Biol. Chem. 167:235, 1947. Roughton, F. J. W., and Scholander, P. F.: Micro gasometric estimation of the blood gases. I. Oxygen, J. Biol. Chem. 148:541, 1943. Plum&, L.: La circulation pulmonaire chez le chien, Arch. Internat. Physiol. 1:176, 1905.