Embed Size (px)
Citation preview

Cardiac Manifestations of Marfan Syndromein Infancy and Childhood
By CHAu PHoRNm uuL, M.D., AMNON RosENTAL, M.D.,AND ALExANDER S. NADAS, M.D.
SUMMARYThe clinical profile and course of 36 infants and children with Marfan syndrome is reviewed.
Cardiac abnormalities were present in 61% of the patients and were the major cause of death. Mi-tral regurgitation, the most frequently encountered cardiac lesion (47%), occurred in both malesand females, while aortic regurgitation was present only in males. Arrhythmias were observed infour patients, and congenital heart disease (atrial septal defect) was observed in one. A dis-tinguishing auscultatory feature was an apical mid or late systolic murmur preceded by singleor multiple clicks. A characteristic electrocardiographic pattern of S-T segment and T-wave changesin leads II, III, aVF, and left precordial leads was noted in 11 patients. The prognosis of chil-dren with Marfan syndrome and isolated mitral regurgitation was usually good, whereas patientswith combined mitral and aortic regurgitation had a rapidly deteriorating clinical course. Theoverall mortality in the group was 14%.
Additional Indexing Words:Mitral regurgitationElectrocardiographic patterns
Aortic regurgitation Mid-late systolic murmur
CARDIAC abnormalities, especially aneurysmsof the ascending aorta and aortic regurgita-
tion, have been recognized for decades as cardinalmanifestations of Marfan syndrome in the adult.Associated congenital heart disease,l lesions of themitral valve24 and pulmonary artery,57 andarrhythmias1' 5have been less frequently reported.The clinical and hemodynamic cardiac findings inchildhood Marfan syndrome have been limited toselected case reports of the more severe complica-tions resulting from the disease.2' 4, 8, 9
This paper reviews our entire experience withMarfan syndrome at The Children's HospitalMedical Center, Boston, between 1945 and 1970.The cardiac manifestations, course, and prognosisof the syndrome in childhood are presented.
From the Department of Cardiology of The Children'sHospital Medical Center, and the Department of Pediatricsof the Harvard Medical School, Boston, Massachusetts.
Supported in part by the U. S. Public Health ServiceGrant HE 10436-04 from the National Institutes of Health,Bethesda, Maryland, and a Grant-in-Aid from the AmericanHeart Association, New York, New York.
Address for reprints: Amnon Rosenthal, M.D., Depart-ment of Cardiology, The Children's Hospital MedicalCenter, 300 Longwood Ave., Boston, Massachusetts 02115.
Received August 22, 1972; revision accepted forpublication November 9, 1972.
Circulation, Volume XLVII, March 1973
Materials and MethodsThe diagnostic files of the Departments of Pediatrics,
Cardiology, Orthopedic Surgery, and Ophthalmologywere searched and the records of 36 patients classifiedas Marfan syndrome were obtained and reviewed. Abias inherent in this group of patients is that they donot represent a general population of children withMarfan syndrome but rather those selected for referralto this Medical Center. The diagnosis of Marfansyndrome and the patients' inclusion in the series werebased on clinical features of the disease. At least onephotograph was available for most of the patients.Features of Marfan syndrome noted include: increasedheight, arm span greater than height, long "spider"fingers, decreased subcutaneous fat, underdevelopedmusculature, hypermobility of joints, dolichocephaly,high-arched palate, eye defects (subluxation of lens,myopia), and spinal and thoracic abnormalities (ky-phosis, scoliosis, and sternal deformities). An adequatefamily history was obtained in 28 patients; only 13 ofthese had relatives with known or suspected Marfansyndrome. The incidence of positive family pedigree isconsiderably less than that reported by McKusick.l1The retrospective nature of this study, spanning 25years, may in part account for this difference. Two ofour patients were siblings. Forme fruste of the diseasewithout ocular manifestations or family history ofMarfan syndrome was not included in this study.Urinalysis for homocystine was negative in 12 patients.A history was obtained and physical examinationperformed by a pediatric cardiologist in all cases. Achest X-ray was obtained in 31 patients, electrocardio-gram in 32, and a phonocardiogram in 17. Cardiaccatheterization was performed in nine patients.
587
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

PH8ORNPHUTKUL ET AL.
ResultsDiagnosis of Marfan SyndromeThe diagnosis of Marfan syndrome was estab-
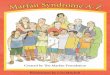
lished in 36 patients (20 females and 16 males).The median age at the initial diagnosis was 6 8/12years (range: birth-15 10/12 years). The diagno-sis was made twice in infancy; once at birth(because of congenital dislocation of the hips) andin the other at 3 months of age (because of adislocated lens). Twenty-six cases (72%) werediagnosed before the age of 10 years (fig. 1).Eye defects (subluxation of the lens, myopia)
were present in 27 patients (75%) and severekyphoscoliosis in 19 (53%). The extracardiacfeatures resulted in the initial diagnosis of Marfansyndrome in 31 (86%) of the patients. In only fivepatients (14%) did the cardiac evaluation lead tothe initial diagnosis of Marfan syndrome; of these,two had mitral regurgitation, one paroxysmal atrialtachycardia, and two no significant heart disease(NSHD).
Diagnosis and Distribution of Cardiac LesionsFourteen patients (39%) of the total group had
no significant heart disease; they had only a grade1-2/6 physiologic systolic ejection murmur withnormal chest X-ray and electrocardiogram whenlast examined. Valvar lesions were present in 21patients and included mitral regurgitation (MR) in17, pure aortic regurgitation (AR) in one, andcombined MR and AR in three. One patient had
,oo _ "0AA
75 /
Cumulative Percent 50- /
0 5 10 15 20Age (Years)
Figure 1
Cumulative distribution by age at initial diagnosis of Mar-fan syndrome (A) and heart disease (B) in 36 patients.
attacks of paroxysmal atrial tachycardia withoutother clinical evidence of cardiovascular disease.The distribution of valvar lesions, according to
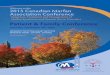
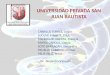
sex, revealed that of the 20 females, 12 had MR andnone had AR. Of the 16 male patients, five had MR,one AR, and three both AR and MR (fig. 2).
Dilatation of the ascending aorta was recognizedon plain chest X-rays or angiograms in all threepatients with combined MR and AR, four of thepatients with pure MR, and in three patientswithout significant valvar lesions. In the patientwith isolated AR, the aortic dilatation could not beappreciated on plain chest X-ray. A dissectinganeurysm of the ascending aorta occurred in onepatient with MR and AR. None of the patients hada history of rheumatic fever and only one hadcongenital heart disease (atrial septal defect).Cardiac involvement was noted on the initial visit
in 15 patients. Six patients developed cardiovascularlesions during the follow-up period. The age atwhich the initial diagnosis of MR was made rangedfrom 3 months to 15 8/12 years with a median of 6%years. The patient with isolated AR was diagnosedat 2 8/12 years. Of the three patients withcombined MR and AR, one developed AR at 6 6/12years and MR at 9 8/12; a second patient developedAR and MR between 11 and 16 years of age; thethird developed MR at 4 7/12 years and ARassociated with a dissecting aortic aneurysm at196/12 years.
Symptoms and Physical FindingsMost patients were asymptomatic throughout the
follow-up period. Symptoms and cardiac abnormal-ities noted on physical examination were related tothe type and severity of the cardiac lesion.
Mitral Regurgitation. There were only three(18%) symptomatic patients among 17 with pureMR. One, with severe MR, developed congestivecardiac failure at the age of 9 months and died withsevere pulmonary infection. Another, also withmoderately severe MR, developed atrial fibrillationat 14 5/12 years and the third patient had recurrentpalpitation for 2 years, but no arrhythmia could bedocumented.
All the patients had a grade 2/6 or louder, apical,mid-to-late systolic murmur. An apical pansystolicregurgitant murmur with late systolic accentuationwas noted in three patients. Single or multiplemidsystolic clicks often preceding the apical systolicmurmur occurred in 12 patients. A third heart
Circulaion, Volume XLVII, March 1973
588
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

MARFAN SYNDROME
20
15 KNumber of Patients 10 _
0Male
J No Significant Heart Disease
EJ Aortic Regurgitation
E Mitral Regurgitation
m Mitral and Aortic Regurgitation
Female
Figure 2
Distribution of cardiac valvar lesions by sex in 36 patients with Marfan syndrome. Note the absence ofaortic regurgitation in girls with Marrfan syndrome.
sound was heard in four patients. An apicalmiddiastolic rumble was audible in one patient with
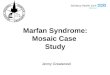
severe MR. The auscultatory findings were con-firmed by phonocardiography in 14 patients (fig. 3).
Carotid A.
SM.Apex A1#4l ,
HFSI x
ECGCx X
X XECG [
Figure 3
Phonocardiogram in a patient with mild mitral regurgitation. Note the late systolic murmur (SM) andclicks (X).
Circulation, Volume XLVII, Marcb 1973
589
...........
...........1
'I
if .1
.,4,owmi .s 1
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

PHORNPHUTKUL ET AL.
Aortic Regurgitation. Isolated aortic regurgitationwas diagnosed in only one child. He was asympto-matic when seen at 2 8/12 years and did not returnfor follow-up. On examination the heart sounds werenormal but he had a grade 3/6 blowing diastolicmurmur at the lower left sternal border.Combined Mitral and Aoitic Regurgitation. All
three patients with combined AR and MR weresymptomatic with progressive exercise intoleranceand fatigue. The cardiac auscultatory findings werethose of moderate-to-severe MR and AR. A thirdheart sound was present in all three patients andone had a fourth heart sound as well.One patient eventually developed acute pulmo-
nary edema at 165/12 years and died immediatelyafter mitral and aortic valve replacement. Anotherpatient died suddenly at home at the age of 11years. The cause of death could not be established.The third patient developed dissection of an aorticaneurysm at age 19 6/12 years and died in theimmediate postoperative period.Abnormalities of the Great Arteries. Dilatation of
the ascending aorta was noted in all patients withcombined MR and AR, four patients with pure MR,and three patients with NSHD. In the only patientwith pure AR, dilatation of the aorta could not beappreciated on plain chest X-rays.The pulmonary artery appeared prominent in
three asymptomatic patients in the absence ofclinical evidence of pulmonary artery hypertension,regurgitation, or a left-to-right shunt.
Arrhythmias. There were four patients witharrhythmias. Two had atrial arrhythmias, one hadparoxysmal atrial tachycardia with NSHD, and inthe other atrial fibrillation complicated moderatelysevere mitral regurgitation. Two patients hadmultifocal premature ventricular beats. Symptomswere related to the severity of the associated heartdisease or the arrhythmia.
Congenital Heart Disease. The diagnosis of anatrial septal defect was confirmed by cardiaccatheterization in one patient. The lesion wasassociated with mild MR. This patient wasasymptomatic during the follow-up period. Perti-nent cardiovascular physical findings includeda widely split fixed second sound, a grade 2/6systolic ejection murmur at the left upper sternalborder, and a midsystolic murmur of mitralregurgitation at the apex.Growth Pattern. The growth pattern of children
with Marfan syndrome is often that of acceleratedrate of maturation for height and average orretarded maturation for weight.10 In four of 16
males and two of 17 females, there was a delay ( >1SD from the mean) in height maturation; all of thesehad associated severe valvar heart disease, severescoliosis, or both. Among the seven patients withthe poorest weight gain (>2 SD), six had severeheart disease and one severe scoliosis. In theabsence of severe scoliosis the presence of retardedgrowth in children or adolescents with Marfansyndrome should therefore strongly suggest exten-sive or severe cardiac involvement.
Cerebrovasculkr Accidents. Two patients re-covered from a moderately severe stroke. Thecerebrovascular accident was due to a subarachnoidhemorrhage in one case, and probably due tothrombosis of a middle cerebral artery in the secondcase.
ElectrocardiogramOne hundred twenty-four electrocardiograms
from 32 patients were available for analysis. Thefindings are summarized in table 1.Mean electrical QRS axis in the frontal plane was
normal in most patients. Right-axis deviation waspresent in the patient with an atrial septal defect.Three patients, two with MR and one withcombined AR and MR, had an indeterminate QRSaxis, and one patient with AR had a superior frontal-plane axis. All the patients with abnormal axes hadvery severe scoliosis and/or pectus deformities(pectus excavatum).Conduction abnormalities were common. Six
patients had first-degree atrioventricular block. Ofthese, three had MR, one MR and AR, and twoNSHD. In addition to these, one patient hadparoxysmal atrial tachycardia, and another hadintermittent atrial fibrillation complicating severeMR. The Q-Tc interval was prolonged (> 0.45 sec)in only three patients.
Left atrial hypertrophy was present in five patientswith MR (isolated or in association with AR) andin the patient with paroxysmal atrial tachycardia.Left ventricular hypertrophy was present in four ofthe 21 patients with valvar lesions. Bight atrial orright ventricular hypertrophy was not present inany of the patients.
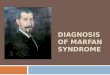
Inverted T waves, frequently associated withdepression of the S-T segment, were noted in leadsII, III, aVF, and across the left precordium in 11patients. Mitral regurgitation was present in eightof the 11 patients. The ST-T wave changes in theleft precordial leads were intermittent in twopatients with MR (one of whom also showedchanges in the standard leads) (fig. 4).
Circulatson, Volume XLVII, March 1973
590
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

MARFAN SYNDROME
Table 1
Electrocardiographic Data
NSH1-D AR MR MR + AR TotalData (N = 11) (N 1) (N = 17) (N -3) (N -32)
QRS axis:0 to 900 11 14 2 27Rtight-axis deviation 1 (ASD) 1Superior axis 1 - 1Perpendicular to frontal plane 2 1 3
10 A-V block 2 3 1 6Atrial fibrillation - - 1 1Paroxysmal atrial tachycardia 1 1Multifocal venitricular extrasystoles 2 2LAH 1 3 2 6LVH 3 1 4ST-T wave changes in II, III, aVF 1 1 8 1 11Prolonged Q-Tc interval (> 0.45 sec) 2 1 3
Abbreviations: NSHD - Ino significant heart disease; AR - aortic regurgitation; MR - mitral regurgita-tion; LAH = left atrial hypertrophy; LVH - left ventricular hypertrophy.
Chest X-raySkeletal abnormalities such as kyphoscoliosis
and/or pectus deformity were noted in the plainchest X-ray in most patients. Cardiac size andindividual chamber enlargement were difficult toassess due to distortion of the cardiac silhouettefrom its usual position by the chest or spine
1957-Age 6 years
deformnity. Dilatation of the ascending aorta wasnoted in all the patients with MR and associatedAR, four patients with MR, and three patients withno significant valvar disease. The pulmonary arteryappeared prominent (in the absence of clinicalevidence of pulmonary artery hypertension, regur-gitation, or a left-to-right shunt) in three patients.
~~~~~~~~~~~~~~~~~~.
t---aVR aVL- aVF V4R V5R Vl
1969-Age 18 years
4-7T~~~~~~~~~~. -.. : -;i.;i.+..!r:... ..
+I:.. ta4-*2*-*-*.!:I't t- ',*, *-......S
tis ;t tj 4 [.... t... {t~~~~~~~~~~~~~A l4a+ s._. ;..F+& S}++sv t -4.oF
$ ' ,' ']* *]- I jise-aVRI atV'9,' .|i. 4F+-.,-.-a.}W:o~~~~V V4R_ ,.s|ev--a -4St- _
Figure 4
Electrocardiogram in a patient with Marfan syndro me and mild mitral regurgitation. Note the inter-mittent nature of the T-wave changes in leads II, III, aVe, and V6.
Circulation, Volume XLVII, March 1973
:. .+: ...::1. ....-fr
V2 V4
rV444___.
14.sV6.
591
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

PHORNPHUTKUL ET AL.
Cardiac Catheterization
Eleven cardiac catheterizations were performedin nine patients. Five patients had MR, three MRand AR, and one MR associated with an atrialseptal defect. There were no fatalities associatedwith the catheterization nor were there any vascularcomplications in the vessels involved. One patientwith MR, AR, and dissecting aneurysm of the aortadeveloped ventricular fibrillation during the aorticangiogram and was successfully countershocked.
Right atrial pressures were normal and none ofthe patients had tricuspid regurgitation. A left-to-right intracradiac shunt was detected in the patientwith an ASD. In patients with angiographicevidence of mitral regurgitation, an elevated meanleft atrial or pulmonary artery wedge pressure witha prominent v wave was observed in two, and mildpulmonary artery hypertension in one patient. Anincrease in LVED (>12 mm Hg) was present inall the patients with significant MR and/or AR. Themean cardiac index was normal, 4.2 liters/min/m2(range 2.5-6.2 liters/mmin/M2). Selective angiogra-phy revealed mild MR in two, severe MR in two,and combined MR and AR in three. Markeddilatation of the sinuses of Valsalva and dilatationof the ascending aorta were present in five patients(fig. 5).
Prognosis
Cardiovascular complications were the cause ofdeath in four cases. One patient died at 9 months ofage with severe MR, congestive heart failure, andpneumonia. An ll-year-old boy with moderate MRand AR died suddenly at home. Three patients diedin the immediate postoperative period; one follow-ing aortic and mitral valve replacement, the secondafter aortic valve replacement and plication of adissecting aortic aneurysm, and the third, a patientwith NSHD, of cardiac arrest during a spinal fusionfor severe scoliosis.
Pathology
Autopsy was performed in two patients. In theinfant with severe MR, examination of the heartshowed marked left atrial and ventricular hypertro-phy. The mitral valve was thickened, its edgesrolled, and there was redundant mitral valve tissue.The chordae tendineae were elongated and theposterior papillary muscle arose low in the leftventricular apex. Redundant tricuspid valve leafletswere present. The pulmonary and aortic valves aswell as the aorta were normal.
In the patient who died following plication of adissecting aneurysm, examination of the heartshowed a massively dilated left atrium and left
Figure 5
Aortic angiogram (anteroposterior and lateral projections) in a patient with Marfan syndrome showingmoderately dilated sinuses of Valsalva. The dilatation cannot be appreciated on the plain chest X-rayssince the structures are within the cardiac silhouette.
Circulation, Volume XLVII, Marcb 1973
592
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

MARFAN SYNDROME
ventricle. Jet lesions were noted in the left atrium.The mitral valve was thickened and rolled but theattachments were normal. The tricuspid andpulmonic valves were normal. The aortic valveleaflets were thickened, the sinuses of Valsalva were
markedly dilated, and dissecting ascending andproximal descending aortic aneurysms were present.
Discussion
Marfan syndrome is a heritable disorder ofconnective tissue affecting predominantly the mus-
culoskeletal, cardiovascular, and ocular systems.The general clinical features of the syndrome andthe cardiovascular manifestations in adults havebeen extensively reviewed.10"11 The cardiac mani-festations of the syndrome during childhood are
usually more subtle and less severe than those inadults, yet they represent the major cause of deathfrom the disease in this age group. Five of our
patients (14%) died, and four of these deaths were
directly attributed to cardiovascular disease.The perinatal period in children with Marfan
syndrome is usually uneventful and the diagnosis,except in cases with known family history, isuncommonly made during infancy (fig. 1). Thediagnosis of Marfan syndrome should be suspectedin infants with isolated mitral regurgitation,4congenital dislocation of the hips,'2 ocular'3 or
orthopedic3 deformities.During childhood most patients exhibit an
accelerated rate of maturation for height and an
average maturation for weight.'0 Patients withdelayed height maturation and very poor weightgain usually had severe cardiac disease and/orkyphoscoliosis. This suggests that severe cardiac or
musculoskeletal deformities significantly interferewith the growth and development of these children.The absence of an accelerated growth pattern in a
child with mitral regurgitation should also, there-fore, not exclude the diagnosis of Marfan syndromeif this is supported by other clinical evidence.
Careful evaluation revealed that 61% of childrenwith Marfan syndrome in our series had an
associated cardiac abnormality (fig. 1). The inci-dence of cardiovascular complications in largegroups of patients with Marfan syndrome haspreviously been reported to be 32%,13 40%,14 and inone series 30 6O%.15 The incidence of cardiovascularcomplications will depend on the age at the initialexamination and will be greater in older childrenand adults. In a recent review'6 of the lifeexpectancy and causes of death in Marfan syn-
drome, cardiac problems led to 52 of 56 deaths of
Circulation, Volume XLVII, March 1973
known causes. The most common cardiac lesion inthe pediatric age group is mitral regurgitation and,in contrast to adults with this syndrome, saccularand dissecting aneurysms of the ascending aorta arerare. Mitral regurgitation was present in 47% of ourcases, aortic regurgitation in 11%, and an aneurysmof the ascending aorta in only one patient (3%).Girls with Marfan syndrome developed mitralregurgitation but no aortic regurgitation. Bycontrast, mitral regurgitation, aortic regurgitation,or combined lesions were present in boys (fig. 2).The reasons for this distribution of valvar lesionsaccording to sex remain unexplained except for theknown predilection of males to aortic diseases(aortic stenosis, coarctation of the aorta, etc) .
Mitral regurgitation usually is an isolated, mildlesion which does not result in any symptoms. Itmay, rarely however, be severe and lead tocongestive heart failure,4 8 saccular aneurysm of theanterior leaflet,17 atrial arrhythmias," 5 or becomethe focus for bacterial endocarditis.1 18, 19 Thedevelopment of aortic regurgitation, however, isusually indicative of more severe cardiac involve-ment and subsequent progressive clinical deteriora-tion.1" Aortic regurgitation may occur as an isolatedlesion or in association with dissecting aneurysm ofthe ascending aorta, or sometimes in combinationwith MR. The prevalence of left heart lesions inMarfan syndrome suggests that although theabiotrophic changes in the elastic tissue fibers aregenetically determined, the severity of the cardio-vascular lesion may in part result from mechanicalfactors.4 14 15 The aortic regurgitant lesion probablydevelops secondary to dilatation of the aortic ringand valve cusps or in association with a dissectingaortic aneurysm. We frequently looked for rheumat-ic valvulitis, but it was not documented in any ofour cases.The murmur of MR in Marfan syndrome is
usually an apical, late systolic murmur accompaniedby mid or late systolic clicks (fig. 3). Whenpansystolic in nature it tends to have a late systolicaccentuation. It is very similar to the mitralregurgitation murmur in the "prolapsed mitral valvesyndrome" and "papillary muscle dysfunction syn-drome."20 Barlow et al.2' and Ronan et al.22 haveclearly demonstrated that apical late systolic mur-murs or pansystolic murmurs with late accentuation,associated with mid-late systolic clicks are dueto mild mitral incompetence. The regurgitant mitralmurmur in patients with Marfan syndrome hasbeen attributed to prolapse of the mitral valveleaflet into the left atrium due to unusually long or
593
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

PHORNPHUTKUL ET AL.
redundant chordae tendineae or a very dilatedmitral valve ring.4' 8 The insufficiency results fromthe elongated chordae which allow one leaflet toovershoot the other8 or, rarely,, it may be secondaryto rupture of the chordae.2 18 Mitral incompetencemay also be due to deformity of the valve margin bynodularity and fibromyxomatous excrescences.'1 Themidsystolic clicks have been postulated to result fromsnapping of the elongated17 or fibrous22 chordae butmay also be related to the sudden distension of theprolapsed mitral leaflet. The high left ventricularpressure could snap redundant or loose chordaetaut and produce a click. Midsystolic clicks werenot heard in the absence of an apical systolicmurmur suggesting that they are of intracardiacorigin.The electrocardiographic tracings in seven of our
patients with isolated mitral regurgitation, mid-to-late systolic murmur, and clicks, reveal myocardialischemic changes in the posterior-inferior cardiacregion (fig. 4), supporting the hypothesis that theapical systolic murmur and clicks may in somepatients be secondary to papillary muscle dysfunc-tion.23 Similar observations have been made inpatients with coronary artery disease.20Although mitral and aortic regurgitation are the
dominant cardiac abnormalities seen in pediatric pa-tients with Marfan syndrome, our group includedone patient with dissecting aortic aneurysm, threewith a solitary dilated main pulmonary artery, andone with paroxysmal atrial tachycardia. Dissectinganeurysms and rupture of the pulmonary artery5 6and/or aorta24 have also been reported in childhood.Contrary to other published reports which suggest astrong association between Marfan syndrome andcongenital cardiovascular malformations,'3 we en-countered only one patient with an atrial septal de-fect. In a review of 28 autopsied cases,' an atrialseptal defect was said to be present in six (21%),aortic stenosis or coarctation in two (7%),and a patent ductus arteriosus in one (3.5%).The necropsy descriptions on individual pa-tients, however, suggest that most of the inter-atrial communications were due to an incom-petent foramen ovale rather than an atrial septaldefect. Fifteen percent of patients with an atrialseptal defect, 1.5% of patients with coarctationof the aorta, and 12% of patients with pulmonicstenosis were reported by Paul Wood to haveMarfan syndrome.25 While the prevalence ofcongenital cardiovascular malformations in Marfansyndrome is probably less than previously sus-pected, there are numerous case reports of the
syndrome associated with coarctation of theaortal" 17, 26-29 or atrial septal defect' suggesting adefinite relationship between these malformationsand Marfan syndrome. A variety of other lesionssuch a patent ductus arteriosus,6 7 ventricular septaldefect,'14 18, 30 tetralogy of Fallot, 4 31 and pulmo-nary stenosis32 have been reported.The chest roentgenogram is usually not helpful in
detecting mild increase in cardiac size and greatvessel enlargement because the severe sternal andspine deformities frequently result in cardiacdisplacement and rotation. Since the sinuses ofValsalva are within the cardiac silhouette, dilatationor aneurysms of these structures are usually notrecognized in the plain chest X-ray unless they arevery large."The classical electrocardiographic finding of a
first-degree atrioventricular block" 4' 5 and S-T andT-wave changes in leads II, III, and AVF33 wereobserved in 19% and 34% of our patients, respective-ly. The occurrence of first-degree atrioventricularblock does not appear to be related to the presenceof aortic regurgitation as suggested by McKusick.14The S-T and T-wave changes in the standard leadsare often accompanied by similar changes in theleft precordial leads and are usually, but notalways, associated with clinically apparent mitralregurgitation (table 1). In two of our patients thesechanges were intermittent (fig. 4). Prolongation ofthe Q-Tc interval has also been reported'8 but thiswas noted in only two of our patients with MR andone patient with MR and AR. QRS-axis abnormali-ties may be secondary to cardiac malrotationinduced by the skeletal deformities. The develop-ment of ventricular and atrial hypertrophy isrelated to the severity of the cardiac lesion.'Increased magnitude of left ventricular voltages,however, may occur in the absence of any leftventricular hypertrophy in some patients with avery thin chest wall.
Cardiac catheterization and selective angiogra-phy are useful in assessing the severity of thecardiac involvement. Dilatation of the aorticannulus and sinuses of Valsalva has been demon-strated by angiography to occur at a very earlyage.9 Catheterization is indicated in patients withhemodynamically significant lesions. It should beundertaken in all preoperative patients to quanti-tate the severity of the regurgitant lesion, outlinethe anatomy of the great arteries, and detect thepossible coexistence of a congenital cardiovascularmalformation. Complications resulting from cardiaccatheterization are rare.
Circulation, Volume XLVII, March 1973
594
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

MARFAN SYNDROME
Surgical experience with cardiac abnormalities inMarfan syndrome has been limited and the resultsof treatment have been generally poor.4 34 Therehave been few successful attempts of mitral and/oraortic valve replacement.17' 35, 36 Two of our pa-tients died in the immediate postoperative periodfollowing valve replacement. In view of the primaryconnective tissue defect in this syndrome, replace-ment of the mitral and aortic valve is preferable toplication. Postoperative death is usually the resultof arrhythmia, pulmonary complications, or dissec-tions in the aortic wall.The care and treatment of a child with Marfan
syndrome require a cooperative effort between alarge number of medical specialties frequentlyavailable only in a medical center. Particularlyimportant is the care provided by the pediatrician,orthopedic surgeon, physiotherapist, ophthalmolo-gist, cardiologist, and genetic counselor. Death inchildhood is usually due to congestive heartfailure,3 4 intercurrent infection,1' 18 or rupture of avascular structure.37 Early recognition of thissyndrome in childhood may improve the prognosis.Patients with mitral incompetence, even if hemo-dynamically insignificant, should be regarded assusceptible to bacterial endocarditis. The develop-ment of an aortic regurgitant murmur in thepatient with mitral regurgitation may be regardedas a poor prognostic sign and the patient should befollowed more closely. The use of beta-blockingagents such as propranolol has been suggested inthese patients.16 Further clinical investigation andsurgical experience, however, will be necessary todetermine whether the basic connective tissuedefect precludes successful long-term medicaland/or surgical results.
References1. MARVEL RJ, CENOVESE PD: Cardiovascular disease in
Marfan's syndrome. Amer Heart J 42: 814, 19512. SIMPSON JW, NoRA JJ, McNAMARA DG: Marfan's
syndrome and mitral valve disease: Acute surgicalemergencies. Amer Heart J 77: 96, 1969
3. HOHN AR, WEBB HM: Cardiac studies of infant twinswith Marfan's syndrome. Amer J Dis Child 122: 526,1971
4. RAGHIB G, JUE KL, ANDERSON RC, EDWARDS JE:Marfan's syndrome with mitral insufficiency. Amer JCardiol 16: 127, 1965
5. BAER RW, TAUSSIG HB, OPPENHEIMER EH: Congeni-tal aneurysmal dilatation of the aorta associated witharachnodactylia. Bull Johns Hopkins Hosp 72: 309,1943
6. TUNG HL, LIEBOW AA: Marfan's syndrome: Observa-tion at necropsy with special reference to medio-
Circulation, Volume XLVII, March 1973
necrosis of the great vessels. Lab Invest 1: 382,1952
7. ANDERSON M, PRArr-THOMAs HR: Marfan's syndrome.Amer Heart J 46: 911, 1953
8. BOWDEN DH, FAVARA BE, DONAHUE JL: Marfan'ssyndrome: Accelerated course in childhood associatedwith lesions of mitral valve and pulmonary artery.Amer Heart J 69: 96, 1965
9. PAPAIOANNOU AC, AGusTsSON MW, GASUL BM: Earlymanifestation of the cardiovascular disorders inMarfan's syndrome. Pediatrics 27: 255, 1961
10. McKusicic VA: Heritable Disorders of ConnectiveTissue, ed 3. St. Louis, C. V. Mosby Co, 1966
11. GASUL BM, ARCILLA RA, LEv M: Heart Disease inChildren. Philadelphia, J. B. Lippincott Co, 1966
12. HELDRICH F JR, WRIGHT CE: Marfan's syndrome:Diagnosis in the neonate. Amer J Dis Child 116:419, 1967
13. RADOs A: Marfan's syndrome (arachnodactyly coupledwith dislocation of the lens). Arch Ophthal(Chicago) 27: 477, 1942
14. McKusIcK VA: The cardiovascular aspects of Marfan'ssyndrome: A heritable disorder of connective tissue.Circulation 11: 321, 1955
15. GOYETTE EM, PALMER PW: Cardiovascular lesions inarachnodactyly. Circulation 7: 373, 1963
16. MURDOCH JL, WALuz BA, HALPERN BL, KuzMA JW,McKusicy. VA: Life expectancy and causes of deathin the Marfan syndrome. New Eng J Med 286: 804,1972
17. EDYNAK GM, RAWSON AJ: Ruptured aneurysm of themitral valve in a Marfan-like syndrome. Amer JCardiol 11: 674, 1963
18. KErIH JD, RowE RD, VLAD P: Heart Disease inInfancy and Childhood, ed 2. New York, TheMacmillan Co, 1966
19. BOWERS D, LIM DW: Subacute bacterial endocarditisand Marfan's syndrome. Canad Med Ass J 86: 455,1962
20. PHILLIPS JH, BURCH GE, DEPASQUALE NP: Thesyndrome of papillary muscle dysfunction. Ann InternMed 59: 508, 1963
21. BARLOW JP, PococK WA, MARCHAND P, DENNY M:The significance of late systolic murmurs. Amer HeartJ 66: 443, 1963
22. RONAN JA, PERLOFF JK, HARVERY WP: Systolic clicksand the late systolic murmur. Amer Heart J 70: 319,1965
23. EHLERS KH, ENGLE MA, LEVIN AR, GROSSMAN H,FLEMING RJ: Left ventricular abnormality with latemitral insufficiency and abnormal electrocardiogram.Amer J Cardiol 26: 333, 1970
24. WONG FL, FRIEDMAN W, YAKOVAC W: Cardiaccomplication of Marfan's syndrome in a child: Reportof a case with rapidly progressive course terminatingwith rupture of a dissecting aneurysm. Amer J DisChild 107: 404, 1964
25. WOOD P: Diseases of the Heart and Circulation, ed 3.Philadelphia, J. B. Lippincott Co, 1968
26. ELDRIDGE R: Coarctation in the Marfan's syndrome.Arch Intern Med (Chicago) 113: 342, 1964
595el
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

PHORNPHUTKUL ET AL.
27. UYEYAMA H, KoNDO B, KAMINS M: Arachnodactylyand cardiovascular disease. Amer Heart J 34: 580,1947
28. FIscHL AA, RUTHERG J: Clinical implications ofMarfan's syndrome. JAMA 146: 704, 1951
29. COFFEY JH, BARKER DE, FRIEDLANDER JH: Dissectinganeurysm with Marfan's syndrome. Texas Med 51:79, 1955
30. TOBERT LE JR, BMCHALL RB: Marfan's syndrome withinterventricular septal defect found at autopsy.Ochsner Clin Rep 2: 48, 1956
31. LINDEBOOM GA, WnrmRVELD-BRANDON ER: Dilatationof the aorta in archnodactyly. Cardiologia (Basel)17: 217, 1950
32. VANBUCHEM FSP: Cardiovascular disease in arachno-dactyly. Acta Med Scand 161: 197, 1958
33. BOWERS D: An electrocardiographic pattern associatedwith mitral valve deformity in Marfan's syndrome.Circulation 23: 30, 1961
34. SmAx: HD, RESSALLAT MM: Surgical correction ofmitral insufficiency in Marfan's syndrome. J ThoracCardiovasc Surg 55: 493, 1968
35. ELLIs PR, CooLEY DA, DEBAKEY HE: Clinicalconsiderations and surgical treatment of annulo-aorticectasia: Report of successful operation. J ThoracCardiovasc Surg 42: 363, 1961
36. MULLER WH JR, DAMMANN JF JR, WARREN WD:Surgical correction of cardiovascular deformities inMarfan's syndrome. Ann Surg 152: 506, 1960
37. CooLEY DA, BLOODWELL RD, HALLMAN GL: Aneur-ysm of the ascending aorta with aortic valvularinsufficiency. Arch Surg (Chicago) 42: 596, 1966
Circulation, Volume XLVII, March 1973
596
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from

CHARLIE PHORNPHUTKUL, AMNON ROSENTHAL and ALEXANDER S. NADASCardiac Manifestations of Marfan Syndrome in Infancy and Childhood
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1973 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.47.3.587
1973;47:587-596Circulation.
http://circ.ahajournals.org/content/47/3/587Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer in the
Permissions in the middle column of the Web page under Services. Further information about this process is availableOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 22, 2018
http://circ.ahajournals.org/D
ownloaded from