Embed Size (px)
Citation preview

Carcinoma Renale: Posters Review
Elena Verzoni S.S. Oncologia Genitourinaria
Fondazione IRCCS Istituto Nazionale Tumori Milano

Adjuvant setting

Presented By Ronac Mamtani at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Presented By Ronac Mamtani at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Presented By Ronac Mamtani at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Presented By Ronac Mamtani at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
Presented By Ronac Mamtani at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care



Aim: to identify pharmacogenomic biomarkers associated with a benefit from adjuvant Sunitinib



Non clear cells

The most common non-clear cell variant is papillary RCC (10-15%) Different clinical phenotypes with both indolent (type 1) and aggressive tumors (type 2)

Aim: to determine the benefit of CN in synchronous metastatic papillary renal cell carcinoma using IMDC

HR adjusted for IMDC factors: 0.62 (95% CI 0.45-0.85; p 0.0031) HR adjusted for IMDC factors, age, bone mets (95% CI 0.39-0-78; p=0.0006)


Consider CN also in well selected pts with papillary RCC!


CREATE trial
• Prospective phase II trial
• Efficacy and safety of crizotinib in pts with advanced tumors with alterations leading to MET and/or ALK pathway
• Final clinical results of the Papillary RCC type I cohort (pathological central review)
• Primary endpoint: ORR per RECIST 1.1


Stage 1 success criteria were met -> 50% objective response

Conclusions
• Observed local misclassification rate: 35%!
• Crizotinib has clinically relevant activity in these patients
• Responses are also seen in MET -/MET? Pts
-> relevance of other alterations of MET or alternative pathways affected by crizotinib?

Presented By RamaprasadSrinivasan at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
• No consensus definition! • Choosing the right biomarker: feasibility vs predictive value

The cancer Genome Atlas Network

Which treatment after first line IO?

Abs.613
Abs.682
Presented at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

Abs 613 (Barata et al, Cleveland) Abs 682 (Shah et al, MD Anderson)
• 43 Patients after 1L IO (nivo/nivo ipi/nivo bev)
• Choice of II line TKIs:
- Pazopanib 12 (28%)
- Axitinib 16 (37%)
- Cabozantinib 15 (35%)
• ORR: 42%
• Toxicity was manageable with expected safety profile
Which treatment after first line IO?
• 33 Patients after 1L IO
• ORR: 77% • Toxicity was manageable with expected safety profile

Genomic Alterations

Abs 626

To assess the prognostic value of Genomic Alterations
• 65 pts IMDC + 33 from CTGA
• GA rates: 27% PRBM1, 17% BAP 1, 29% SETD2, 9% KDM5C, 8% TP53
• GA in BAP 1 or TP53 had the strongest association with OS (after adjusting for IMDC risk group and age)
• Poor risk AND GA in BAP 1 or TP53 -> worse OS

Abs 639

To integrate PBRM1-BAP1-TP53 mutation status into IMDC risk model
• N 354 pts (from Comparz trial)- Record 3 validation cohort (258)
• Mutation status for each gene
-> indipendently correlated with OS (TP53 and BAP1 –poor OS)
The annoted risk model alters risk status in over 1/3 of pts and improves accuracy of estimates outcomes in first line TKI population

Abs. 617
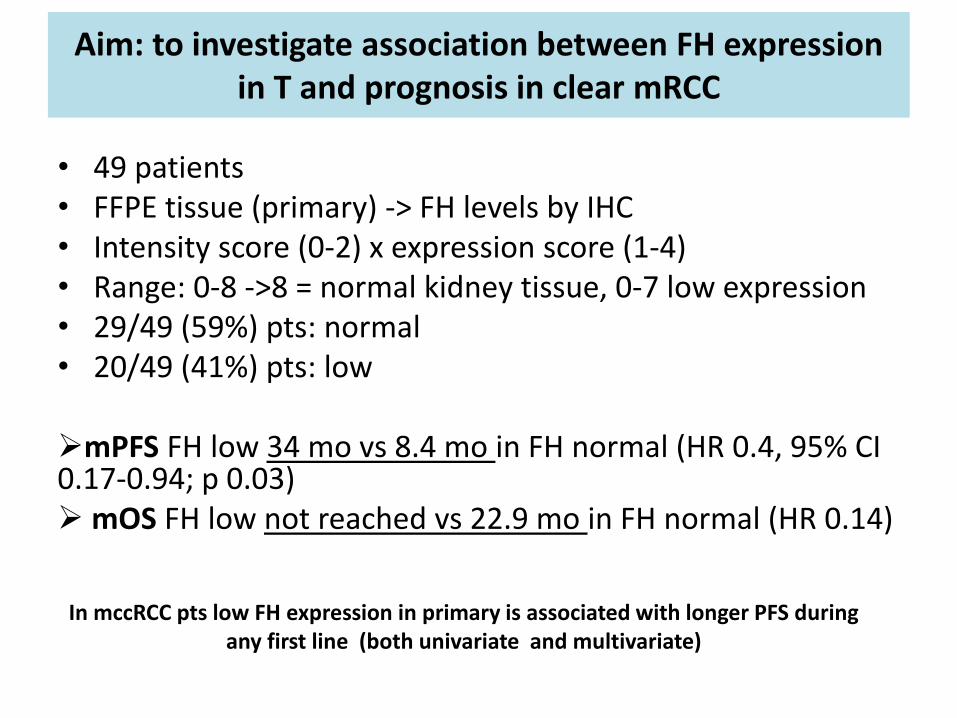
Aim: to investigate association between FH expression in T and prognosis in clear mRCC
• 49 patients • FFPE tissue (primary) -> FH levels by IHC • Intensity score (0-2) x expression score (1-4) • Range: 0-8 ->8 = normal kidney tissue, 0-7 low expression • 29/49 (59%) pts: normal • 20/49 (41%) pts: low mPFS FH low 34 mo vs 8.4 mo in FH normal (HR 0.4, 95% CI 0.17-0.94; p 0.03) mOS FH low not reached vs 22.9 mo in FH normal (HR 0.14)
In mccRCC pts low FH expression in primary is associated with longer PFS during any first line (both univariate and multivariate)

Immunotherapy “management”

Abs.616

To evaluate different expressions of PD1-PDL1-PDL2 in primary/mets
• 163 pt -> IHC
• The concordance rates between the primary and mets: 32.5%
• Higher detection rate in mets rather that in primary
• PD1 (T or M)-> poor prognostic factor for PFS
• PDL1 (T) -> poor prognostic factor for OS (HR 2.55)

Abs.654

• Retrospective analysis
• 90 pts received NIVO (44% II, 29%III, 27%>III)
• Non PD 35 pts
• PD 55 pts (91% RECIST or 9% clinical)
-> 20/55 pts (36% develop new sites of disease)
Brain (40%) Liver (20%) Soft tissue (20%) Locoregional (20%) Never: lung/pancreas/nodes

Take home messages
Adjuvant treatment is not standard of care (many factors could influence outcome)
CN should be considered also in well selected pts with papillary RCC
Be careful to evaluate PDL1 expression in Primary tumor
After first line IO -> TKIs work (prospective trial ongoing!)
Genomic alterations (PBRM1/BAP 1/TP53) have prognostic role and should be evaluated in every mRCC patients






























