Embed Size (px)
Citation preview

Br Heart _J 1993;70:241-246
Reduction of mismatch of global ventilation andperfusion on exercise is related to exercisecapacity in chronic heart failure
Neal G Uren, Simon W Davies, John E Agnew, Andrew G Irwin, Sally L Jordan,Andrew JW Hilson, David P Lipkin
Departnent ofCardiologyN G UrenS W DaviesS L JordanD P LipkinDepartment ofMedical PhysicsJ E AgnewA G IrwinDepartment ofNuclear Medicine,Royal Free Hospital,LondonA JW HilsonCorrespondence to:Dr N G UrenMRC Cyclotron Unit,Hammersmith Hospital,London W12 OHS.
Accepted for publication8 February 1993
AbstractBackground-The inability to matchlung perfusion to ventilation because of areduced cardiac output on exercise con-tributes to reduced exercise capacity inchronic heart failure.Objective-To quantify ventilation toperfusion matching at rest and at peakexercise in patients with chronic heartfailure and relate this to haemodynamicand ventilatory variables of exercisecapacity.Design-Eight men in New York HeartAssociation class II underwent maximalbicycle ergometry with i gas anasis.Main outcome measures-On separatedays, ventilation and perfusion gammacamera imaging was performed at rest,and at 80% of previous peak exerciseheart rate during bicycle ergometry. Thevertical distribution of mismatchbetween ventilation and perfusion (V/Q)was estimated from subtracted profiles ofactivity (ventilation and perfusion) toderive a numerical index of global mis-match.Results-Maximal mean (SD) oxygenconsumption on bicycle ergometry was16-0 (4.5) ml min-' kg-'. There was areduction in the global V/Q mismatchindex from 23-96 (5.90) to 14-88 (7.90)units (p < 0.01) at rest and at peak exer-cise. Global V/Q mismatch index at peakexercise correlated negatively with maxi-mal minute ventilation (R = - 0 90, p <0-01) and with maximal mean arterialpressure (R = -0 79, p < 0.05), althoughno relation was seen with maximal oxy-gen consumption. The reduction inglobal V/Q mismatch index from rest topeak exercise correlated with maximaloxygen consumption (R = 0-88, p < 0.01),and with maximal minute ventilation(R = 0-87, p < 0.01).Conclusions-During exercise in patientswith chronic heart failure, there is areduction in the global V/Q mismatchindex. A lower global V/Q mismatchindex at peak exercise is associated withhigher maximal ventilation. The reduc-tion in global VIQ mismatch index onexercise correlates weli with maximalexercise capacity. This may imply thatthe inability to perfuse adequately allregions of lung on exercise and matchthis to ventilation is a factor determiniingexercise capacity in chronic heartfailure.
(Br Heart J 1993;70:241-246)
IntroductionIn chronic heart failure, patients ventilateduring maximal exercise, more than do nor-mal subjects at the same workload,1 2 leadingto an increased ratio of minute ventilation tominute production of carbon dioxide, com-pared with controls. It is widely believed thatthis inappropriate increase in ventilation maybe partly explained by an increase in physio-logical dead space secondary to a mismatchbetween ventilation and perfusion,'4 particu-larly as there is also a reduced cardiac outputin response to exercise in these patients.7 Asthe ventilatory equivalent for carbon dioxideproduction ratio correlates with maximal oxy-gen consumption in patients with chronicheart failure but not in normal subjects, it hasbeen postulated that a critical level of cardiacfunction is necessary to perfuse adequately alllung zones on exercise, thus avoiding signifi-cant mismatch between ventilation and perfusion.2
In our study, we have used radio isotopescanning to measure regional distribution oflung ventilation and perfusion at rest andduring maximal exercise in patients withchronic heart failure. From these data it ispossible to calculate a numerical index ofmismatch between global ventilation and per-fusion to find whether there is a direct rela-tion between the degree of mismatch betweenventilation and perfusion and exercise capac-ity as measured by oxygen consumption.
Patients and methodsPATIENT POPULATIONEight men with chronic heart failure, mean(SD) age 66 (7) years were enrolled in thestudy. Patients were excluded if there was ahistory of recent angina or ST segmentdepression (>0.1 mV) on the electrocardio-gram on exercise stress tests, or primary lungdisease judged by history, clinical examina-tion, chest x ray film, and pulmonary functiontests. Table 1 shows patient characteristics.Six of the patients had ischaemic heart dis-ease and two had idiopathic dilated car-diomyopathy as the cause of their chronicheart failure. All patients were classified asNew York Heart Association (NYHA) classII. Radionuclide gated ventriculography wasperformed before the study and the mean leftventricular ejection fraction was 30% (9%).The mean forced expiratory volume in onesecond was 2-5 (0 4) 1.
STUDY PROTOCOLThe study was approved by the ethics com-mittee of the Royal Free Hospital and allpatients gave written informed consent.
241
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from
Uren, Davies, Agnew, Invin, Jordan, Hilson, Lipkin
Table I Patient characteristics
Age Weight Medication Vo,max LVEF FEV, FVC FEV,/FVCPatient (yr) (kg) Aetiology (daily) (ml min' kg') (%) CTR (% predicted) (% predicted) (%)1 52 75-7 DCM Frus 80mg 24-63 30 0 55 2-4 (83) 3 0 (77) 80
Ena 20 mgDig 0-25 mgAnsio 200 mg
2 64 93-8 DCM Frus 40 mg 11-70 45 0-57 2 0 (70) 2-8 (74) 71Ena 5 mg
3 64 73-7 EHD Frus 80 mg 19-59 24 0-59 3 1 (100) 41 (95) 76Cap 50 mgDig 0-25 mgISDN 20 mg
4 66 97-4 EHD Frus 40 mg 11-13 16 0-52 2-4 (83) 3-5 (84) 70Cap 75 mg
5 67 70 0 IHD Frus 40 mg 17-83 40 0-53 3-2 (92) 3-9 (85) 82Dig 0-25 mgAmio 200 mg
6 69 75 5 HID Frus 60 mg 14-69 23 0-61 2-7 (85) 3-5 (81) 77Cap 37-5 mgISDN 30 mg
7 73 67-0 EHID Dyazide I tablet 12-88 31 0-48 2-0 (61) 2-8 (65) 718 73 66-7 EHD Frus 80 mg 15-74 28 0-60 2-6 (79) 3-6 (84) 72
Lisin 5 mgMean(SD) 66(7) 77-4(11-8) 16-02 (4 54) 30 (9) 0-56 (0 04) 2-5 (0-4) 3-4 (0-5) 75 (5)
CTR, cardiothoracic ratio; DCM, dilated cardiomyopathy; FEV,, forced expiratory volume in one second, FVC, forced vital capacity; IHD, ischemic heart dis-ease; LVEF, radionuclide left ventricular ejection fraction; Vo,max, maximal oxygen consumption; Amio, amiodarone; Cap, captopril; Dig, digoxin; Dyazide,hydrochlorothiazid + triamterene; Ena, enalapril; Frus, frusemide; ISDN, isosorbide dinitrate; lisin, lisinopril.
Exercise testsPatients underwent exercise tests by bicycleergometry with a mechanically braked bicycleergometer (Monark-Crescent AB, Varberg,Sweden). An incremental protocol for thebicycle ergometer was used starting at 50 Wof work, increasing the workload by 10 Wmin-' as tolerated, maintaining the flywheelrate at 50 rev min-'. Patients took their usualmedications on the day of the exercise testsand all tests were performed in the morningat least two hours after eating. Heart rate,blood pressure, and respiratory rate weremeasured before exercise, every minute ofexercise, at peak exercise, and until valuesreturned to baseline.
Expired gases were analysed at rest until asteady state was achieved. Subjects wore amouthpiece with a low resistance HansRudolf spiral non-return valve and theamount of dead space in the circuit was esti-mated as 35 ml. Minute ventilation (VE, in1 min-'), oxygen consumption (Vo,, in mlmin-' kg-'), and carbon dioxide production(Vco,, in ml minr' kg-') were measured bythe argon dilution method every 10 secondsfrom a mixing box by an AirSpec MGA200mass spectrometer (Airspec, Bromley, Kent).8This output was linked by an analogue to dig-ital converter to an on line BBC micro com-puter. Values were corrected for atmosphericpressure, laboratory temperature, water-vapour pressure, and body weight. Ventil-atory variables were calculated over the 30seconds before and after the end of eachminute, and maximal (max) values derivedfrom the last 60 seconds of exercise. Arterialoxygen saturation was measured with anearlobe pulse oximeter (Radiometer,Copenhagen, Denmark).
During exercise, the magnitude of the sen-sation of dyspnoea was assessed with a handwritten 100 mm visual analogue scale (VAS),at the end of each three minute stage, at peakexercise, and at 15, 30, and 60 seconds theneach minute after exercise until valuesreturned to baseline.9
Ventilation and perfusion scanningVentilation and perfusion scanning was per-formed at rest and on exercise on separateoccasions within two weeks. Bicycle ergome-try was repeated in the Department ofMedical Physics according to the sameprotocol.
At bicycle ergometry, patients were posi-tioned directly in front of a gamma camera(IGE 400T) so as to ensure optimal views inthe posteroanterior plane. Heart rate andblood pressure were measured as before.Ventilation and perfusion scanning was per-formed at 80% of previous peak heart rate atergometry. This point was chosen because itallowed sufficient time to perform both venti-lation and perfusion scans before the end ofexercise at peak capacity. Ventilation scan-ning was performed with krypton-81m(81mKr) by the continuous inhalation tech-nique,'0 with inhalation through a two wayvalve. A dose of 3000 MBq s of 8'mKr wasdelivered through a standard reservoir con-nected by tubing to the patient's mouthpieceover 100 seconds until 300 000 counts werecollected, with the window of the camera setfor the 191 keV y rays of the 8'mKr.Consecutively, an additional 100 cm lengthof tubing was connected to create added deadspace (to ensure delivery at a later stage ofinspiration) with further delivery of 8lmKr over100 seconds. At the same time (80% of theprevious peak heart rate), 80 MBq oftechnetium-99m (99mTc) macroaggregatedalbumin was injected intravenously andcounts collected with the window of thecamera set for the 140 keV y rays of the9OmTc. Ventilation and perfusion scans wererecorded on a Nuclear Diagnostics computersystem (Nuclear Diagnostics, Gravesend,Kent) and analysed by means of vertical pro-file information transferred to a personalcomputer. The scans were performed by twoobservers (EA, AGI) independent of thesupervision of the exercise protocol (NGU,SLD.On another day, ventilation and perfusion
242
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from
Reduction ofmismatch ofglobal ventilation and perfusion on exercise is related to exercise capacity in chronic heartfailure
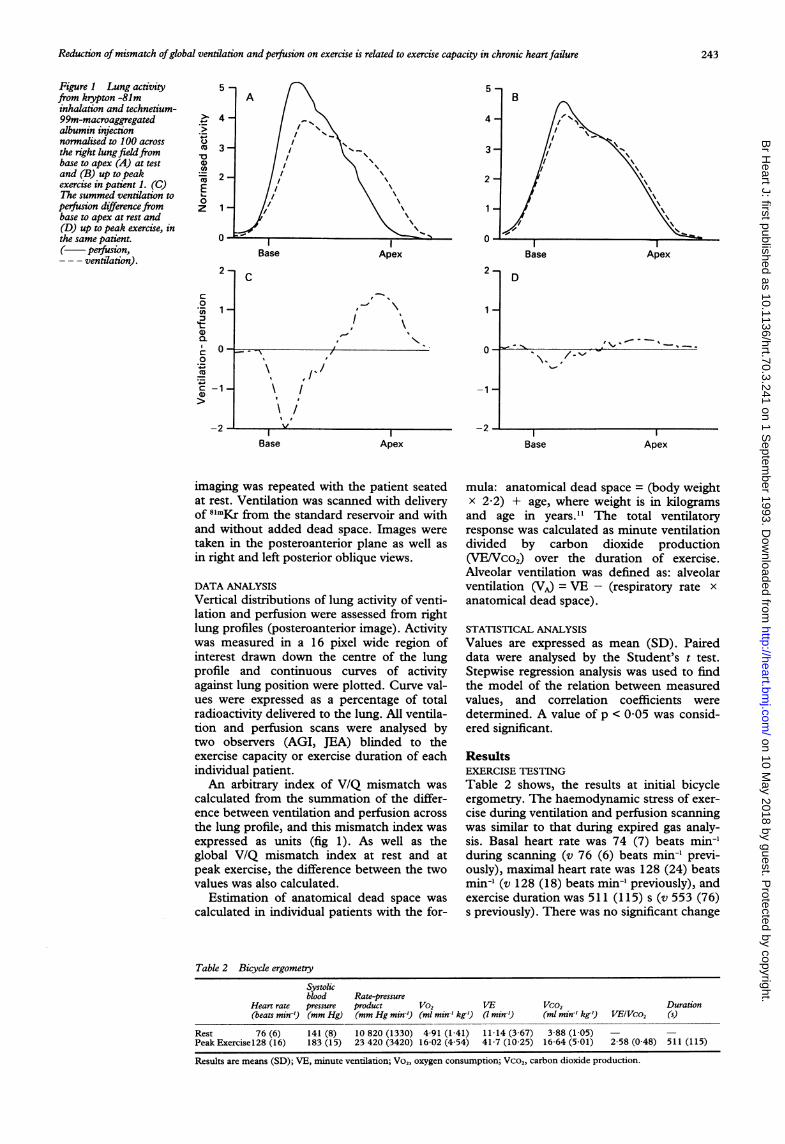
Figure 1 Lung activityfrom krypton -81minhalation and technetium-99m-macroaggregatedalbumin injectionnormalised to 100 acrossthe right lungfieldfrombase to apex (A) at testand (B) up to peakexercise in patient 1. (C)The summed ventilation toperfusion difference frombase to apex at rest and(D) up to peak exercise, inthe same patient.( perfusion,--- ventilation).
c
0CuCl
CI0._
a1)
0
CoCa
0
z
Base
2-
1-
Apex
2-C
1
0-1~~~~~~~~~~~~~~~0-0 -- -)/-
% I
\t I
/It f-1 \I
-2 - -IvIBase
Base Apex
D
O-_ - u , , ' -
-1-
-2 1- II
Apex Base Apex
imaging was repeated with the patient seatedat rest. Ventilation was scanned with deliveryof 8'mKr from the standard reservoir and withand without added dead space. Images were
taken in the posteroanterior plane as well asin right and left posterior oblique views.
DATA ANALYSISVertical distributions of lung activity of venti-lation and perfusion were assessed from rightlung profiles (posteroanterior image). Activitywas measured in a 16 pixel wide region ofinterest drawn down the centre of the lungprofile and continuous curves of activityagainst lung position were plotted. Curve val-ues were expressed as a percentage of totalradioactivity delivered to the lung. All ventila-tion and perfusion scans were analysed bytwo observers (AGI, JEA) blinded to theexercise capacity or exercise duration of eachindividual patient.An arbitrary index of V/Q mismatch was
calculated from the summation of the differ-ence between ventilation and perfusion across
the lung profile, and this mismatch index was
expressed as units (fig 1). As well as theglobal V/Q mismatch index at rest and atpeak exercise, the difference between the twovalues was also calculated.
Estimation of anatomical dead space was
calculated in individual patients with the for-
mula: anatomical dead space = (body weightx 2 2) + age, where weight is in kilogramsand age in years.'1 The total ventilatoryresponse was calculated as minute ventilationdivided by carbon dioxide production(VE/Vco,) over the duration of exercise.Alveolar ventilation was defined as: alveolarventilation (VA) = VE - (respiratory rate xanatomical dead space).
STATISTICAL ANALYSIS
Values are expressed as mean (SD). Paireddata were analysed by the Student's t test.Stepwise regression analysis was used to findthe model of the relation between measuredvalues, and correlation coefficients weredetermined. A value of p < 005 was consid-ered significant.
ResultsEXERCISE TESTING
Table 2 shows, the results at initial bicycleergometry. The haemodynamic stress of exer-
cise during ventilation and perfusion scanningwas similar to that during expired gas analy-sis. Basal heart rate was 74 (7) beats min-'during scanning (v 76 (6) beats min-' previ-ously), maximal heart rate was 128 (24) beatsmin-' (v 128 (18) beats min-' previously), andexercise duration was 511 (115) s (v 553 (76)s previously). There was no significant change
Table 2 Bicycle ergometry
Systolicblood Rate-pressure
Heart rate pressure product Vo, VE Vco, Duration(beats min-9 (mm Hg) (mm Hg min') (ml min-' kg') (7 min-') (ml min-' kg') V/EIVco, (s)
Rest 76 (6) 141 (8) 10 820 (1330) 4-91 (1-41) 11-14 (3-67) 3-88 (1-05) - -
Peak Exercisel28 (16) 183 (15) 23 420 (3420) 16-02 (4 54) 41-7 (10-25) 16-64 (5-01) 2-58 (0 48) 511 (115)
Results are means (SD); VE, minute ventilation; Vo5, oxygen consumption; Vco,, carbon dioxide production.
243
I---l
I
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from
Uren, Davies, Agnew, Irvin, Jordan, Hilson, Lipkin
0
0 R -090, p <0.01'I-
0
20 30 40 50 60 70Maximal minute ventilation (1.min-1)
B |R = 079, p <0*05 |
03 ~~~0
0
0
100 110 120 130 140 150Maximal mean arterial pressure (mm Hg)
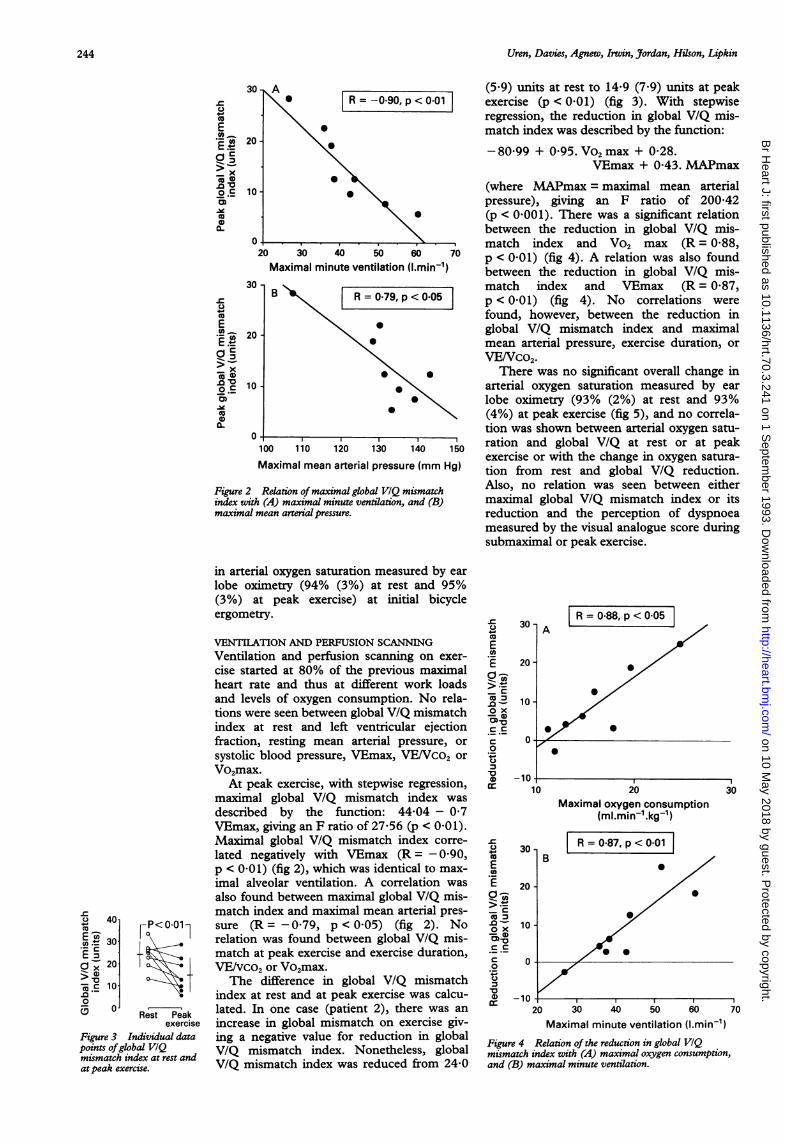
Figure 2 Relation ofmaximal global VIQ mismatchindex with (A) maximal minute ventilation, and (B)maximal mean arterial pressure.
Rest Peakexercise
Figure 3 Individual datapoints ofglobal VIQmismatch index at rest andat peak exercise.
in arterial oxygen saturation measured by earlobe oximetry (94% (3%) at rest and 95%(3%) at peak exercise) at initial bicycleergometry.
VENTILATION AND PERFUSION SCANNINGVentilation and perfusion scanning on exer-cise started at 80% of the previous maximalheart rate and thus at different work loadsand levels of oxygen consumption. No rela-tions were seen between global V/Q mismatchindex at rest and left ventricular ejectionfraction, resting mean arterial pressure, orsystolic blood pressure, VEmax, VE/Vco2 orVo2max.
At peak exercise, with stepwise regression,maximal global V/Q mismatch index wasdescribed by the function: 44 04 - 0'7VEmax, giving an F ratio of 27-56 (p < 0 01).Maximal global V/Q mismatch index corre-lated negatively with VEmax (R = - 0 90,p < 0-01) (fig 2), which was identical to max-imal alveolar ventilation. A correlation wasalso found between maximal global V/Q mis-match index and maximal mean arterial pres-sure (R = -079, p < 0 05) (fig 2). Norelation was found between global V/Q mis-match at peak exercise and exercise duration,VE/vco2 or Vo2max.The difference in global V/Q mismatch
index at rest and at peak exercise was calcu-lated. In one case (patient 2), there was anincrease in global mismatch on exercise giv-ing a negative value for reduction in globalV/Q mismatch index. Nonetheless, globalV/Q mismatch index was reduced from 24-0
(5 9) units at rest to 14-9 (7 9) units at peakexercise (p < 0 01) (fig 3). With stepwiseregression, the reduction in global V/Q mis-match index was described by the function:-80-99 + 0.95. Vo2 max + 0-28.
VEmax + 0 43. MAPmax
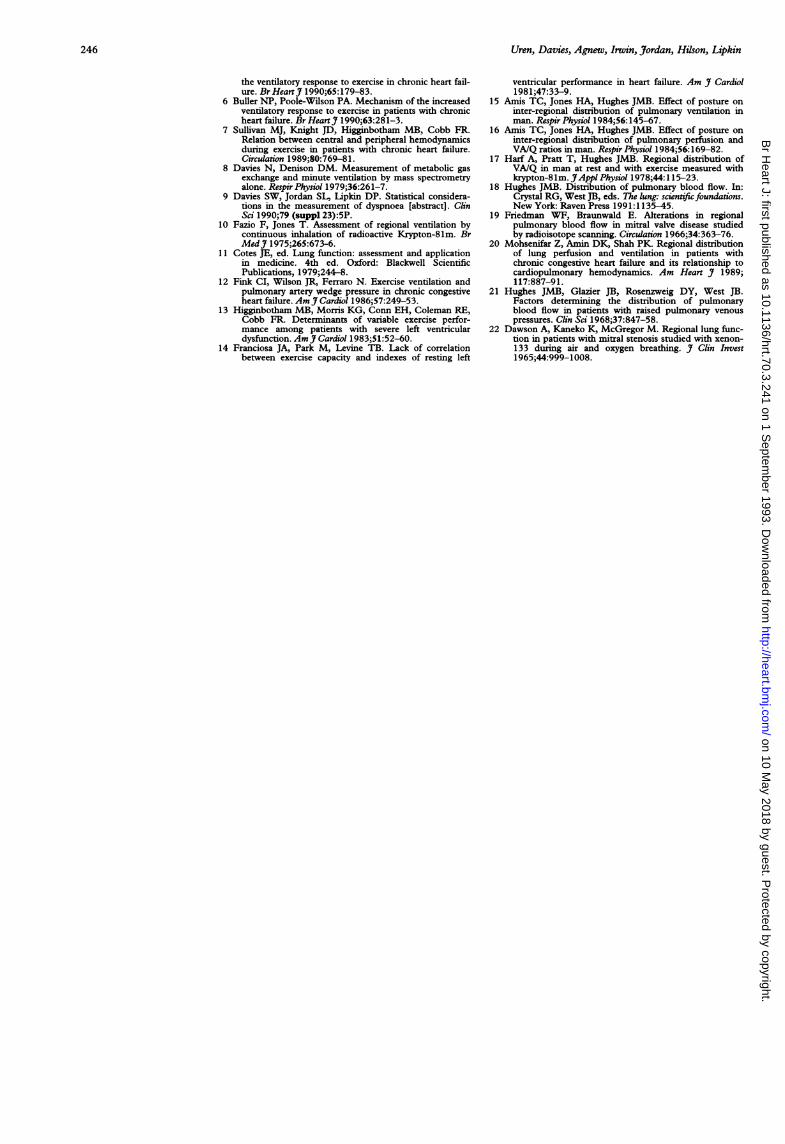
(where MAPmax = maximal mean arterialpressure), giving an F ratio of 200-42(p < 0 001). There was a significant relationbetween the reduction in global V/Q mis-match index and Vo2 max (R = 0-88,p < 0-01) (fig 4). A relation was also foundbetween the reduction in global V/Q mis-match index and VEmax (R = 0-87,p < 0-01) (fig 4). No correlations werefound, however, between the reduction inglobal V/Q mismatch index and maximalmean arterial pressure, exercise duration, orVE/Vco2.
There was no significant overall change inarterial oxygen saturation measured by earlobe oximetry (93% (2%) at rest and 93%(4%) at peak exercise (fig 5), and no correla-tion was shown between arterial oxygen satu-ration and global V/Q at rest or at peakexercise or with the change in oxygen satura-tion from rest and global V/Q reduction.Also, no relation was seen between eithermaximal global V/Q mismatch index or itsreduction and the perception of dyspnoeameasured by the visual analogue score duringsubmaximal or peak exercise.
0
E._LE
-
cc
'E
.0
00-50
_ C
E0
-c
.0
ox
cc
CC
0E._E.
.0_
D00
30.
20
10
0
20
R=0.88,p<0.05 |
20Maximal oxygen consumption
(ml.min-l.kg-1)
B
30
R = 0-87, p < 0-01
0
0S
30 40 50 60Maximal minute ventilation (l.min-1)
70
Figure 4 Relation of the reduction in global VIQmismatch index with (A) maximal oxygen consumption,and (B) maximal minute ventilation.
3C
04-0
E.E m 20a r- 2_> x
DE 0.00o.E 1C
.beco
0
0-
30
U0
E
D - 12(x
Co
0
0.
40
E o 30._C
C- 20
Q.:. 10..00
A
rP< 0.01Ilr -l±
244
3
D 4
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from

Reduction of mismatch ofglobal ventilation and perfusion on exercise is related to exercise capacity in chronic heartfailure
DiscussionPrevious work has suggested that theincreased ventilation of exercise in chronicheart failure may occur as a response to anincrease in physiological dead space.2-6 Inthese patients there is a linear inverse relationbetween minute ventilation over carbon diox-ide production (VENco2) and maximal oxy-gen consumption.1 12 As correction forventilation of anatomical dead space onlyreduces the gradient of the inverse relation byone third, it has been suggested thatincreased physiological dead space, that is anincreased V/Q mismatch, accounts for mosthyperpnoea, and that this mismatch corre-lates directly with maximal oxygen consump-tion.6By contrast, Davies and coworkers showed
that there was no such correlation betweenVE/vco2 and maximal oxygen consumptionin normal healthy subjects5 and there seemedto be a curvilinear relation between VEIVco2and maximal oxygen consumption, whencombining this with data from patients withchronic heart failure. It was suggested thatthe point of inflection of this curve repre-sented a threshold of severity of chronic heartfailure beyond which VEIVco2 increased dueto V/Q mismatch, and that this might be dueto insufficient cardiac function to perfuse alllung zones.5The results of this study indicate that it is
possible to show V/Q mismatch in chronicheart failure patients at rest with a simplemethod of quantitation. As with many otherresting measurements of cardiorespiratoryfunction in chronic heart failure patients"'34V/Q mismatch at rest does not correlate withsubsequent exercise capacity. The degree ofglobal mismatch at peak exercise, however, isinversely related to maximal minute ventila-tion. On exercise, there is a tendency toreduce this mismatch, and this correlates wellwith exercise capacity measured by maximaloxygen consumption, as well as with maximalminute ventilation. The increase in meanarterial pressure at peak exercise, which maybe a measure of the ability adequately to per-fuse all regions of the pulmonary vascularbed, also correlated with the reduction inglobal V/Q mismatch. Thus although we can-not prove a causal relation it is possible thatthe ability to increase cardiac output to per-fuse the lungs adequately and match theincrease in alveolar ventilation on exercise iswhat partly determines the delivery of oxygento exercising muscles.
Gravity is a considerable influence onregional ventilation and perfusion in the nor-mal lungs, with a gradient in flow from theapex to the base,'1'7 with reduced arterialpressure at the apices, as well as a central toperipheral reduction in pulmonary bloodflow. Regional perfusion is also dependent onthe arteriolar resistance and hypoxic vasocon-striction.'8 On exercise, there is a consider-able increase in recruitment of additionalvascular channels in the pulmonary circula-tion and widespread pulmonary vasodilata-tion to accommodate the increase in
pulmonary blood flow. Chronic heart failureresults in redistribution of pulmonary bloodflow away from dependent areas at rest to theapices,'9 with an inability to increase the pro-portion of upper zone perfusion on exerciseby contrast with controls.20 This lack ofchange in perfusion to the upper zones mayreflect the inability to reduce mismatch onexercise in patients with more severe heartfailure. Furthermore, as this is only partiallyrelieved by increasing lung volume,2' or
22oxygen, it may be that there are structuralor functional alterations in these areas thatcompound a reduced regional lung perfusionon exercise through an inadequate cardiacoutput.
LIMITATIONS OF THE STUDYA potential limitation of this study is thatventilation and perfusion scanning was per-formed separately from expired gas measure-ment. This obviated the use of an arbitrarylevel of oxygen consumption as the startingpoint for scanning during sub-maximal exer-cise. Both the heart rate response to exerciseand exercise duration were not significantlydifferent from that during expired gas analy-sis, implying similar exercise haemodynamics.As scanning was initiated at this point,patients were also performing different work-loads that could contribute to differentdegrees of cardiovascular work. Although it ispossible that patients with worse heart failurewere able to exercise for less time and couldnot reduce V/Q mismatch for this reason, thisstill does not exclude the inability to reducemismatch as a possible limiting factor in exer-cise.
CONCLUSIONSIt is possible to measure V/Q mismatch inpatients with chronic heart failure at rest andon exercise with vertical lung profiles of 8'mKrgas inhalation and intravenous 99mTc. Onexercise, global V/Q mismatch tends todiminish. The ability to reduce this mismatchcorrelates well with maximal exercise capacityas assessed by maximal oxygen consumptionand with maximal minute ventilation, and toa lesser extent with maximal mean arterialpressure. This implies that the inability toperfuse all regions of lung adequately on exer-cise through a reduced cardiac output is oneof the factors determining exercise capacity inchronic heart failure.We thank Ian Watson at the MRC Cyclotron Unit,Hammersmith Hospital, London for providing hot generatorsfor this study.
1 Weber KT, Kinasewicz GT, Janicki JS, Fishman AP.Oxygen utilisation and ventilation during exercise inpatients with chronic stable congestive heart failure.Circulation 1982;65: 1213-23.
2 Wilson JR, Ferraro N. Exercise intolerance in patientswith chronic left heart failure: relation to oxygen trans-port and ventilatory abnormalities. Am J Cardiol1983;51:1358-63.
3 Rubin SA, Brown HV. Ventilation and gas exchange dur-ing exercise in severe chronic heart failure. Am RevRespir Dis 1984;129:S63-4.
4 Sullivan MJ, Higginbotham MB, Cobb FR. Increasedexercise ventilation in patients with chronic heart fail-ure: intact ventilatory control despite haemodynamicand pulmonary abnormalities. Circulation 1988;77:552-9.
5 Davies SW, Emery TM, Watling ML, Wannamethee G,Lipkin DP. A critical threshold of exercise capacity in
C 1001oo0
90 -
CDx.-1 ,7u%_ /U J
Rest Peakexercise
Figure 5 Individual datapoints of arterial oxygensaturation at rest and atpeak exercise.
245
I-A-4-
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from
Uren, Davies, Agnew, Invin, Jordan, Hilson, Lipkin
the ventilatory response to exercise in chronic heart fail-ure. BrHeartj 1990;65:179-83.
6 Buller NP, Poole-Wilson PA. Mechanism of the increasedventilatory response to exercise in patients with chronicheart failure. Br HeartJ 1990;63:281-3.
7 Sullivan MJ, Knight JD, Higginbotham MB, Cobb FR.Relation between central and peripheral hemodynamicsduring exercise in patients with chronic heart failure.Circulation 1989;80:769-81.
8 Davies N, Denison DM. Measurement of metabolic gasexchange and minute ventilation by mass spectrometryalone. Respir Physiol 1979;36:261-7.
9 Davies SW, Jordan SL, Lipkin DP. Statistical considera-tions in the measurement of dyspnoea [abstract]. ClinSci 1990;79 (suppl 23):5P.
10 Fazio F, Jones T. Assessment of regional ventilation bycontinuous inhalation of radioactive Krypton-81m. BrMedJ 1975;265:673-6.
11 Cotes JE, ed. Lung function: assessment and applicationin medicine. 4th ed. Oxford: Blackwell ScientificPublications, 1979;244-8.
12 Fink CI, Wilson JR, Ferraro N. Exercise ventilation andpulmonary artery wedge pressure in chronic congestiveheart failure. AmJCardiol 1986;57:249-53.
13 Higginbotham MB, Morris KG, Conn EH, Coleman RE,Cobb FR. Determinants of variable exercise perfor-mance among patients with severe left ventriculardysfunction. Am Cardiol 1983;51:52-60.
14 Franciosa JA, Park M, Levine TB. Lack of correlationbetween exercise capacity and indexes of resting left
ventricular performance in heart failure. Am J7 Cardiol1981;47:33-9.
15 Amis TC, Jones HA, Hughes JMB. Effect of posture oninter-regional distribution of pulmonary ventilation inman. Respir Physiol 1984;56:145-67.
16 Amis TC, Jones HA, Hughes JMB. Effect of posture oninter-regional distribution of pulmonary perfusion andVA/Q ratios in man. Respir Physiol 1984;56: 169-82.
17 Harf A, Pratt T, Hughes JMB. Regional distribution ofVA/Q in man at rest and with exercise measured withkrypton-81m. JAppM Physiol 1978;44:115-23.
18 Hughes JMB. Distribution of pulmonary blood flow. In:Crystal RG, West JB, eds. The lung: scientific foundations.New York: Raven Press 1991:1135-45.
19 Friedman WF, Braunwald E. Alterations in regionalpulmonary blood flow in mitral valve disease studiedby radioisotope scanning. Circulation 1966;34:363-76.
20 Mohsenifar Z, Amin DK, Shah PK. Regional distributionof lung perfusion and ventilation in patients withchronic congestive heart failure and its relationship tocardiopulmonary hemodynamics. Am Heart 1989;117:887-91.
21 Hughes JMB, Glazier JB, Rosenzweig DY, West JB.Factors determining the distribution of pulmonaryblood flow in patients with raised pulmonary venouspressures. Clin Sci 1968;37:847-58.
22 Dawson A, Kaneko K, McGregor M. Regional lung func-tion in patients with mitral stenosis studied with xenon-133 during air and oxygen breathing. Clin Invest1965;44:999-1008.
246
on 10 May 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.70.3.241 on 1 Septem
ber 1993. Dow
nloaded from





























