Embed Size (px)
Citation preview

Candidati vaccinaliper la prevenzione
della meningite/sepsida GBS
Graziella Orefici
Difficulties in developing a GBS vaccine
• Reluctance to vaccinate women duringpregnancy
• Low prevalence rate of neonatal disease• Implausibility of performing traditional
efficacy trials
GBS disease in the years
• 1937 Fry reported 7 cases of puerperal sepsis
• 1960 Eikoff reported GBS as neonatal pathogen
• 1970s-80s GBS recognized as major cause of neonatal/puerperal disease
• 1990s surveillance revealed GBS to be importantpathogen in adults(immunocompromised and elderly)
comorbidities:diabetes,stroke,liver cirrosis,decubitus ulcer, breast cancer,urogenic bladder

GBS Disease – maternal
• Clinical presentation of the mother– bacteremia/sepsis – amnionitis– endometritis– urinary tract infection– cellulitis and fasciitis– wound infections
• Effect on the fetus– prematurity– low birthweight delivery– spontaneous abortion– stillbirth

GBS disease-Neonatal
• Early onset group B streptococcal disease (EOGBSD):• GBS is usually acquired peripartum.• The disease occurs within the first week after birth;• targets all infants but premature infants, are at greatest risk;• presents as bacteremia, respiratory distress, and
cardiovascular collapse;
• Late onset group B streptococcal disease (LOGBSD): • GBS may be acquired from the mother, from hospital staff
(intensive care nurseries), or from the community. • occurs from 1 week to 3 months after birth; • bacteremia and meningitis are prominent;

GBS infections in USIncidence Years 80-90 Years 2000
Early onset 1-3/1000 0.6/1000(mortality) (50%) (5%)
Late onset 0.7/1000 0.6/1000(30% reliquates)
(mortality) (17 %) (7 %)

Incidence of GBS disease in Europe in the 2000s
• Spain 0.3-0.7/1000 live births
• Germany 0.5 /1000
• UK 0.74 /1000
• Italy 0.4 /1000
• Czech Rep. 0.7-1/1000

Comparison of Studies Performed in Years 1983-1997
I (1983) II (1985) III (1995) IV (1997)
Mother-neonate
Pairs number 471 1516 6935 2300
Carriage:
M 42/471 (8.9%)
114/1516 (7.5%)
678/6935 (9.78%)
260/2300 (11.3%)
N 17/282 (6.02%)
64/1294 (4.9%)
308/6935 (4.4%)
208/2327 (4.8%)
Transmission 40.4% 45.1% 43.2% 41.5%
Infections - 4 (3.1‰) 3 (0.4‰) 1 (0.4‰)
Other studiesParea 1994. Retrospective study
60.000 pairs screened
0.8/000 incidence
17% mortality

Cases of Meningitis NotifiedYears 1995-2004
GBS Pn Men Hib Other Total
2004 24 263 318 13 252 870
2003 21 309 278 35 326 969
2002 31 235 223 42 346 877
2001 29 235 203 54 267 788
2000 25 232 224 50 283 814
1999 30 309 275 85 373 1064
1998 31 250 154 96 296 827
1997 23 231 182 100 318 854
1996 32 180 169 126 315 822
1995 34 180 200 118 294 826
GBS = Group B Streptococcus Men = Meningococcus
Pn = Pneumococcus Hib = H. influenzae b
CDC indications for intrapartum prophylaxisVaginal and rectal screening for all pregnant women at 37 W.
Prophylaxis indicatedPrevious infant with infectionGBS bacteriuria during pregnancyPositivity at GBS screeningUnknown GBS statusDelivery at <37 w.Amniotic membrane rupture > 18 hIntrapartum temperature>38°C
Prophylaxis non indicatedPrevious pregnancy with + screeningPlanned cesarean deliveryNegative screening
Surface components of GBS
• Group polysaccharide, non protective
• Type capsular polysaccharides (Ia,Ib,II,III,IV,V,VI,VII,VIII,), protective
• Surface proteins (C alpha and beta, Rib , Sip, C5 peptidase)
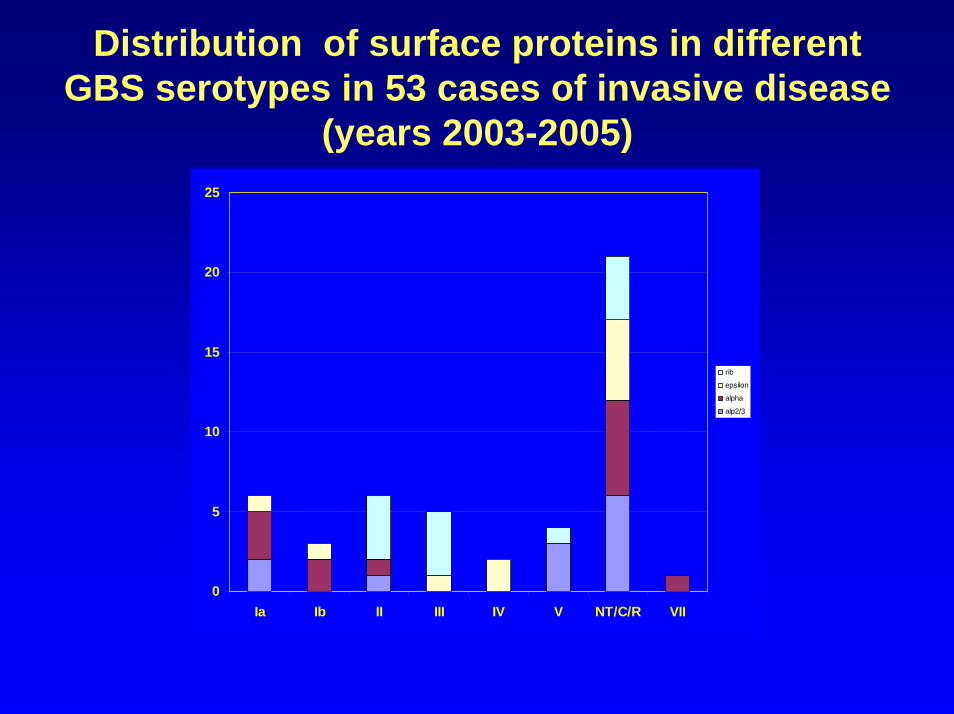
Distribution of surface proteins in differentGBS serotypes in 53 cases of invasive disease
(years 2003-2005)
0
5
10
15
20
25
Ia Ib II III IV V NT/C/R VII
rib
epsilon
alpha
alp2/3
Serotypes on GBS infections in US. years ’93-’99.(Shet et Ferrieri 2004)
• Six major serotypes are present both in neonataland adult disease:
• Ia,( Ib), II,III,(IV), V• Serotypes Ib and IV are not frequent in neonates• Serotypes VI and VIII are found in Japan but very
rarely in western countries
Development of GBS vaccinesin humans
• 1978 Type III CPS in adults to test safety
• 1988 Type III GBS in pregnant women

Parameters to be evaluated
• Type of polysaccharide• Protein carrier• Type of conjugation• Adjuvant• Effect of repeated dose• Type of IG produced• Duration of immunity

Development of GBS vaccine in animals
• 1990 TT-III conjugate vaccine (Wessels et al., J ClinInvest)
• 1993 TT- Ia (Wessels et al,Infect and Immunity)
• 1994 tetravalent conjugate vaccine (Paoletti et al,Infect and Immunity)
• 1995 TT-V (Wessels et al,J Infect dis)
• 1996 TT-III in baboons (Paoletti et al,Infect and Immunity)
• 1999 TT-VI and TT-VIII (Paoletti et al,J Infect Dis)
• 2002 TT-IV and TT-VII (Paoletti et al ,J infect Dis)
Development of GBS vaccinesin humans
• 1978 Type III CPS in adults to test safety (J Clin Invest)
• 1988 Type III GBS in pregnant women (New Engl J Med)
• 1996 TT-III for safety and immunogenicity (Kasper et al,J Clin Invest)
• 2000 TT-II (Baker et al, J Infect Dis)
• 1999 Bivalent TT-Ia and TT-Ib for safety and immunogenicity ( Baker et al,J infect Dis )
• 2003 TT-III in 30 healthy pregnant women (Baker et al ,Vaccine)
• 2004 TT-V in healthy women (Baker et al ,J Infect Dis)

May the proportion of women with Ab < protective threshold be reduced by
immunization?
4 wks after immunization % women >1 µg/mlPS :from 10% to 55%TT-PS : from 10% to 90% (J Clin Invest 1996)
With bivalent TT-Ia + TT-Ib, 8 wksimmunization:
from 40% to 90% >1 µg /mlfrom 10% to 65% > 5 µg/ml (J Infect dis 1999)

Maternal and cord serum anti type III GBS antibodies in healthy and EOD subjects . (Lyn F.C. et al 2004)
70% cases in newborns with <05 µg/ml20% btwn 0.5-1 µg/mlFew cases > 1 µg/ml
Cord/ M. ratio:80% NN > 34 W20% NN < 34 W
In NN > 34 w.Risk : 31%lower if mother > 0.5 µg/ml
88% lower if mother >5 µg/ml

Other GBS vaccine candidateson study
• GBS surface proteins (Larsson et al,vaccine 1999)
• GBS surface proteins conjugated to CPS (Cheng et al,Infect &Immunity 2002)
• DNA vaccines for“in utero” vaccination(Gerdts et al,Vaccine 2004)
• Mucosal CT-GBS vaccines (Shen et al, Infect & immunity 2001)
• New protein vaccines from genome information

Target population
• Pregnant women at III trimester pregnancy (90% EO prevention?)
• Non pregnant teenage girls (longevity of functional antibodies?Prevention in < 33 w.gestationneonates?)
• Elderly at risk persons?

Conclusions
• Vaccination can be useful to improveprevention in E.O and to prevent L O GBS disease (but neonatal protective Ablevels not firmly established for eachserotype)
• Vaccination in teenage or in pregnantwomen may be not more expensivethan the general screening ( but long term immunity is to be defined)

• Some of TT-conjugated vaccines havealready passed Phase I and II sperimentationand might be used in target population in a short time provided that legal obstacle are removed

Further studies
• Epidemiological surveillance of new serotypes
• Better knowledge of the immune responsefor different serotypes
• Studies on new types of vaccines and vaccination
• Studies on population target for vaccination

Roberta CretiLucilla BaldassarriSimona RecchiaMonica ImperiMarco PataracchiaGiovanna Alfarone
Christina vonHunolstein
Laura Parisi
Alberto Berardi