Embed Size (px)
Citation preview

Can we sustain
change for patients
with inoperable or
persistent/recurrent
CTEPH? Irene M Lang
Medical University of Vienna, Austria
Nick H Kim
University of California, San Diego,
CA, USA
ERS International
Congress 2015
Monday, 28 September
L.NL.MA.09.2015.0072
Disclosures (1)
Irene Lang has received research grants and speaker’s honoraria
from Abbott, Actelion, AOP Orphan Pharmaceuticals, Astra Zeneca,
Bayer HealthCare, Biotronik, Cordis, Daiichi-Sankyo, Euromed,
GSK, Medtronic, Novartis, Pfizer, Terumo, and United Therapeutics,
and is a board member of CTEPH.com and the International
CTEPH Association
Nick Kim has served as a consultant/speaker for Actelion and
Bayer HealthCare (steering committee member for the MERIT and
CHEST studies), and is a board member of CTEPH.com and the
International CTEPH Association
L.NL.MA.09.2015.0072
Disclosures (2)
This presentation includes discussion of riociguat in combination
with BPA in patients with CTEPH
To date, there have been no formal clinical trials of riociguat in
combination with BPA, nor is it approved for use in combination with
BPA
BPA, balloon pulmonary angioplasty.
L.NL.MA.09.2015.0072
Treatment algorithm for CTEPH
BPA, balloon pulmonary angioplasty.
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
aTechnically operable patients with non-acceptable risk/benefit ratio can be considered also for BPA. bIn some centers medical therapy and BPA are initiated concurrently.
Diagnosis confirmed by
CTEPH expert center
Lifelong anticoagulation
Operability assessment by a
multidisciplinary CTEPH team
Technically operable Technically non-operable
Targeted medical
therapy
Consider BPA in
expert centerb
Persistent severe
symptomatic PH
Consider lung
transplantation
Persistent
symptomatic PH
Non-acceptable
risk:benefit ratioa
Acceptable
risk:benefit ratio
Pulmonary
endarterectomy
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317
L.NL.MA.09.2015.0072
Pulmonary endarterectomy
The treatment of choice for CTEPH in eligible patients: potentially
curative1
Technically demanding procedure, requiring specialist training and
intensive postoperative care1,2
– Bilateral endarterectomy through the medial layer of the pulmonary
arteries
– Performed under deep hypothermic circulatory arrest
Effective and highly successful
– Substantial relief of symptoms; near normalization of hemodynamic
parameters1
– Low mortality in experienced centers1
– Cognitive function postsurgery not impaired3
1. Jenkins D. Eur Respir Rev 2015;24:263–71. 2. Jamieson SW et al. Ann Thorac Surg 2003;76:1457–64.
3. Vuylsteke A et al. Lancet 2011;378:1379–87.
L.NL.MA.09.2015.0072
The “operable” vs “non operable” patient
Lang IM and Madani M. Circulation 2014;130:508–18.
Copyright protected content.
Please view original content in the following reference:
Lang IM and Madani M. Circulation 2014;130:508–18.
L.NL.MA.09.2015.0072
Treatment algorithm for CTEPH
BPA, balloon pulmonary angioplasty.
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
aTechnically operable patients with non-acceptable risk/benefit ratio can be considered also for BPA. bIn some centers medical therapy and BPA are initiated concurrently.
Diagnosis confirmed by
CTEPH expert center
Lifelong anticoagulation
Operability assessment by a
multidisciplinary CTEPH team
Technically operable Technically non-operable
Targeted medical
therapy
Consider BPA in
expert centerb
Persistent severe
symptomatic PH
Consider lung
transplantation
Persistent
symptomatic PH
Non-acceptable
risk:benefit ratioa
Acceptable
risk:benefit ratio
Pulmonary
endarterectomy
Copyright protected content.
Please view original content in the following reference:
Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317
L.NL.MA.09.2015.0072
Riociguat as targeted medical therapy for
CTEPH
First evidence-based, medical therapy approved for patients in
WHO FC II to III with inoperable CTEPH, or persistent or recurrent
CTEPH after surgical treatment, to improve exercise capacity1
– Clinical evidence from CHEST: robust long-term (2 year) efficacy and safety
data2
– Reinforced by real-world data from the riociguat Early Access Study3
Highest recommendation (IB) in the 2015 ESC/ERS guidelines for
treatment strategies other than PEA4
WHO FC, World Health Organization functional class.
1. Bayer HealthCare. Adempas® EU Summary of Product Characteristics. July 2015. 2. Simonneau G et al. Eur Respir J 2014;44(Suppl.58):
1802; 3. McLaughlin V et al. Am J Respir Crit Care Med 2015;191:A4840. 4. Galiè N et al. Eur Heart J 2015:doi:10.1093/eurheart/ehv317.
Case study 1 Recurrent CTEPH
post-PEA
Nick H Kim
L.NL.MA.09.2015.0072
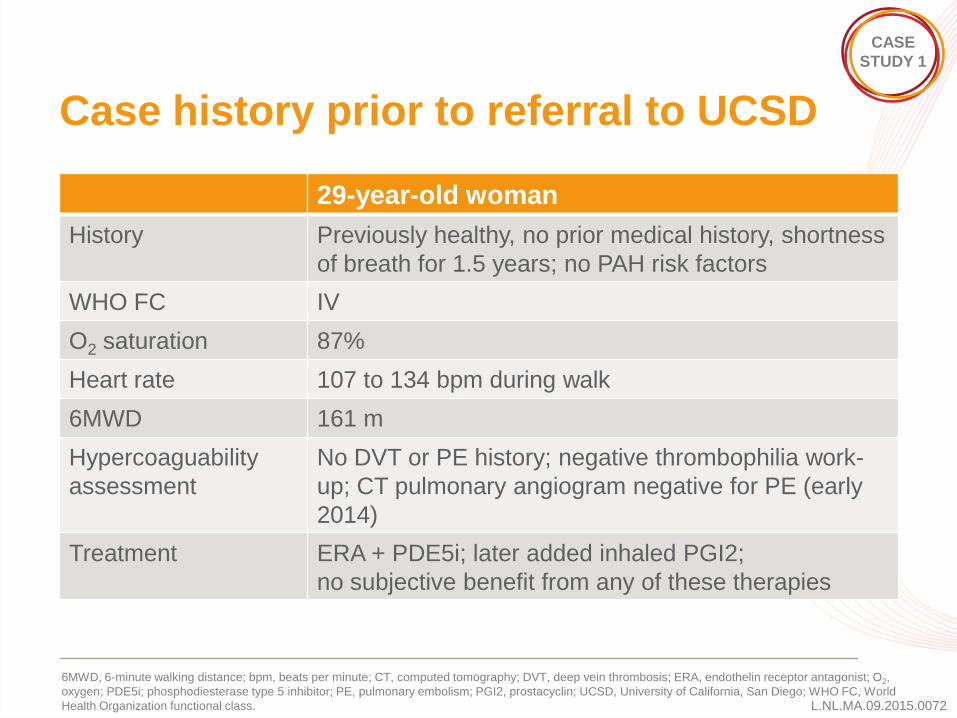
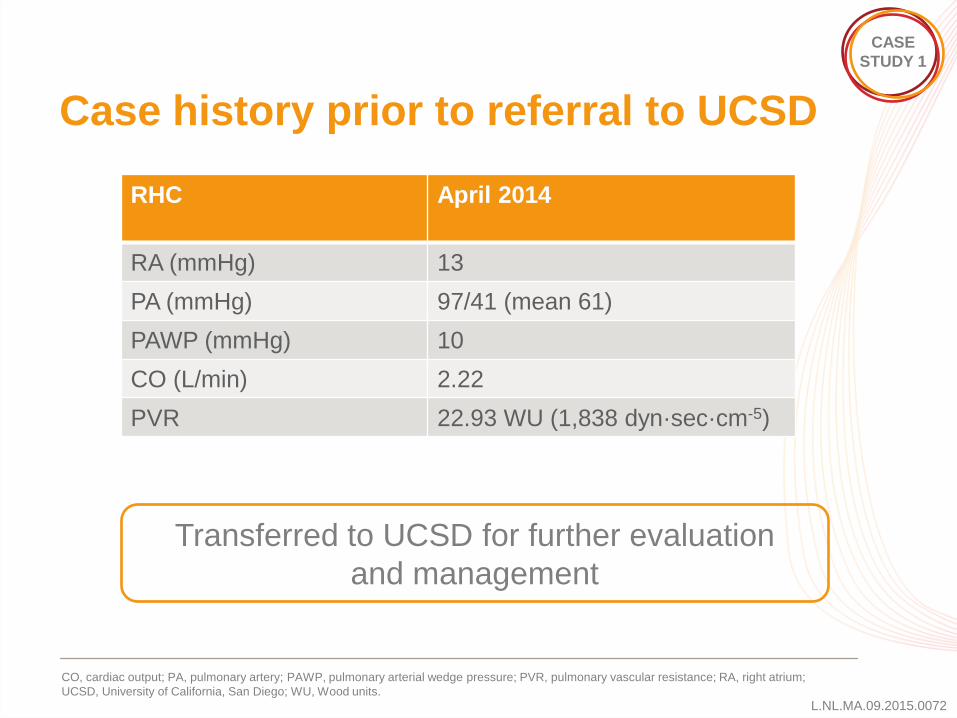
Case history prior to referral to UCSD
29-year-old woman
History Previously healthy, no prior medical history, shortness
of breath for 1.5 years; no PAH risk factors
WHO FC IV
O2 saturation 87%
Heart rate 107 to 134 bpm during walk
6MWD 161 m
Hypercoaguability
assessment
No DVT or PE history; negative thrombophilia work-
up; CT pulmonary angiogram negative for PE (early
2014)
Treatment ERA + PDE5i; later added inhaled PGI2;
no subjective benefit from any of these therapies
6MWD, 6-minute walking distance; bpm, beats per minute; CT, computed tomography; DVT, deep vein thrombosis; ERA, endothelin receptor antagonist; O2,
oxygen; PDE5i; phosphodiesterase type 5 inhibitor; PE, pulmonary embolism; PGI2, prostacyclin; UCSD, University of California, San Diego; WHO FC, World
Health Organization functional class.
CASE
STUDY 1
L.NL.MA.09.2015.0072
Case history prior to referral to UCSD
CO, cardiac output; PA, pulmonary artery; PAWP, pulmonary arterial wedge pressure; PVR, pulmonary vascular resistance; RA, right atrium;
UCSD, University of California, San Diego; WU, Wood units.
Transferred to UCSD for further evaluation
and management
CASE
STUDY 1
RHC April 2014
RA (mmHg) 13
PA (mmHg) 97/41 (mean 61)
PAWP (mmHg) 10
CO (L/min) 2.22
PVR 22.93 WU (1,838 dyn·sec·cm-5)
L.NL.MA.09.2015.0072
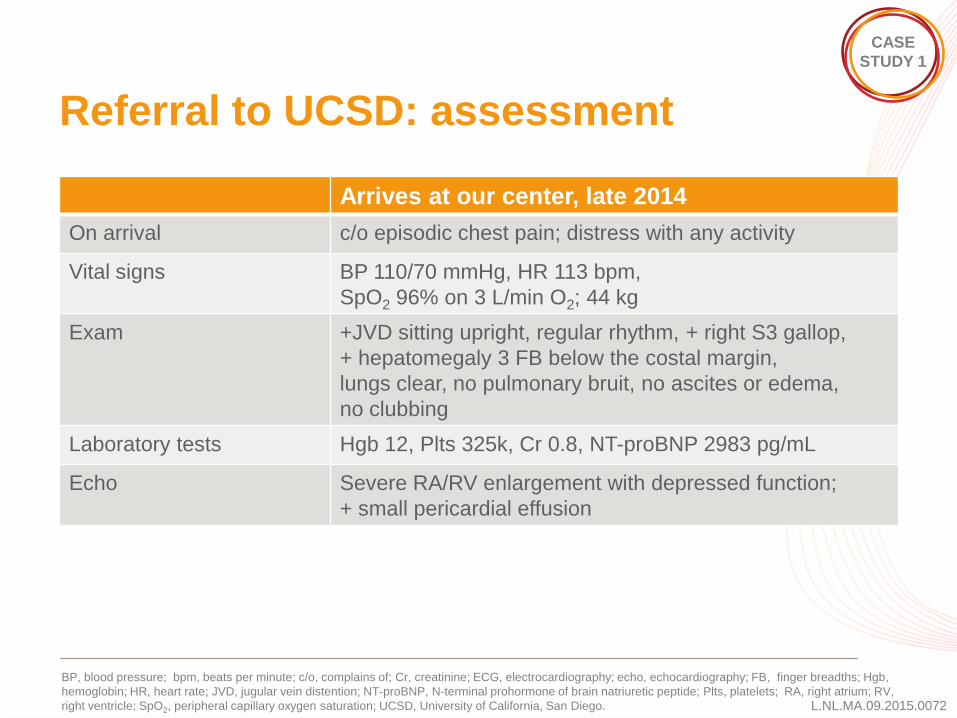
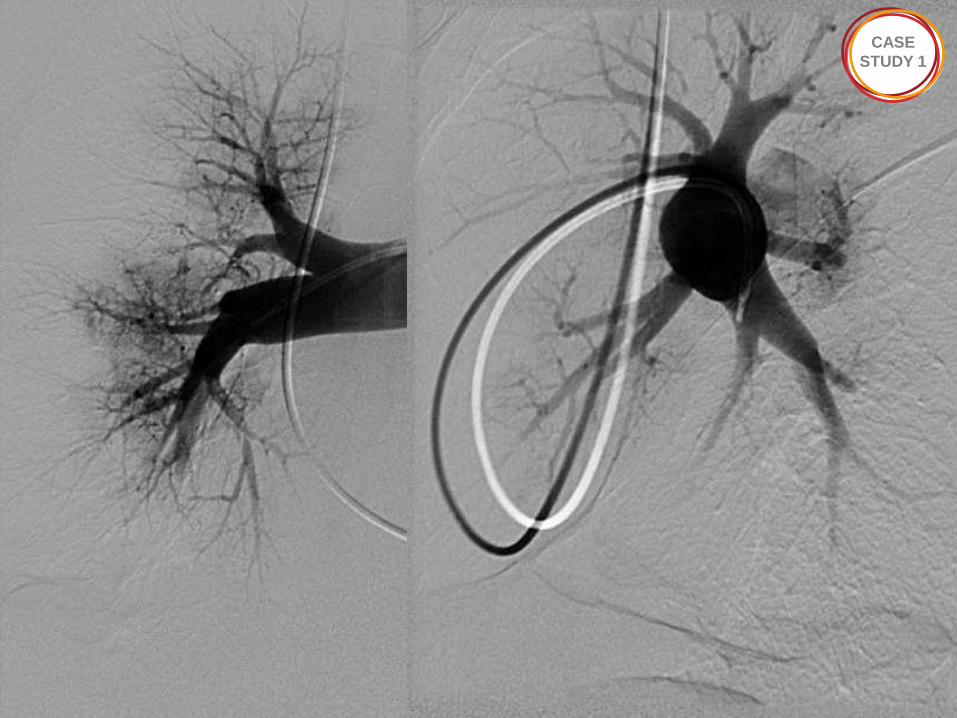
Referral to UCSD: assessment
Arrives at our center, late 2014
On arrival c/o episodic chest pain; distress with any activity
Vital signs BP 110/70 mmHg, HR 113 bpm,
SpO2 96% on 3 L/min O2; 44 kg
Exam +JVD sitting upright, regular rhythm, + right S3 gallop,
+ hepatomegaly 3 FB below the costal margin,
lungs clear, no pulmonary bruit, no ascites or edema,
no clubbing
Laboratory tests Hgb 12, Plts 325k, Cr 0.8, NT-proBNP 2983 pg/mL
Echo
Severe RA/RV enlargement with depressed function;
+ small pericardial effusion
BP, blood pressure; bpm, beats per minute; c/o, complains of; Cr, creatinine; ECG, electrocardiography; echo, echocardiography; FB, finger breadths; Hgb,
hemoglobin; HR, heart rate; JVD, jugular vein distention; NT-proBNP, N-terminal prohormone of brain natriuretic peptide; Plts, platelets; RA, right atrium; RV,
right ventricle; SpO2, peripheral capillary oxygen saturation; UCSD, University of California, San Diego.
CASE
STUDY 1
13
CASE
STUDY 1
14
CASE
STUDY 1
15
CASE
STUDY 1
16
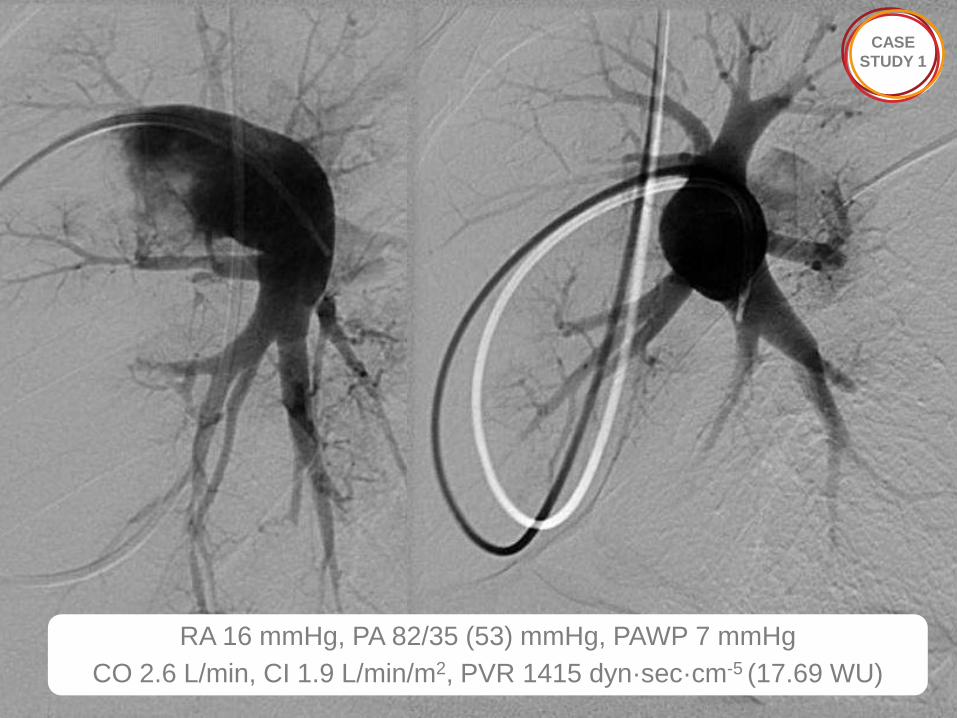
RA 16 mmHg, PA 82/35 (53) mmHg, PAWP 7 mmHg
CO 2.6 L/min, CI 1.9 L/min/m2, PVR 1415 dyn·sec·cm-5 (17.69 WU)
CASE
STUDY 1
L.NL.MA.09.2015.0072
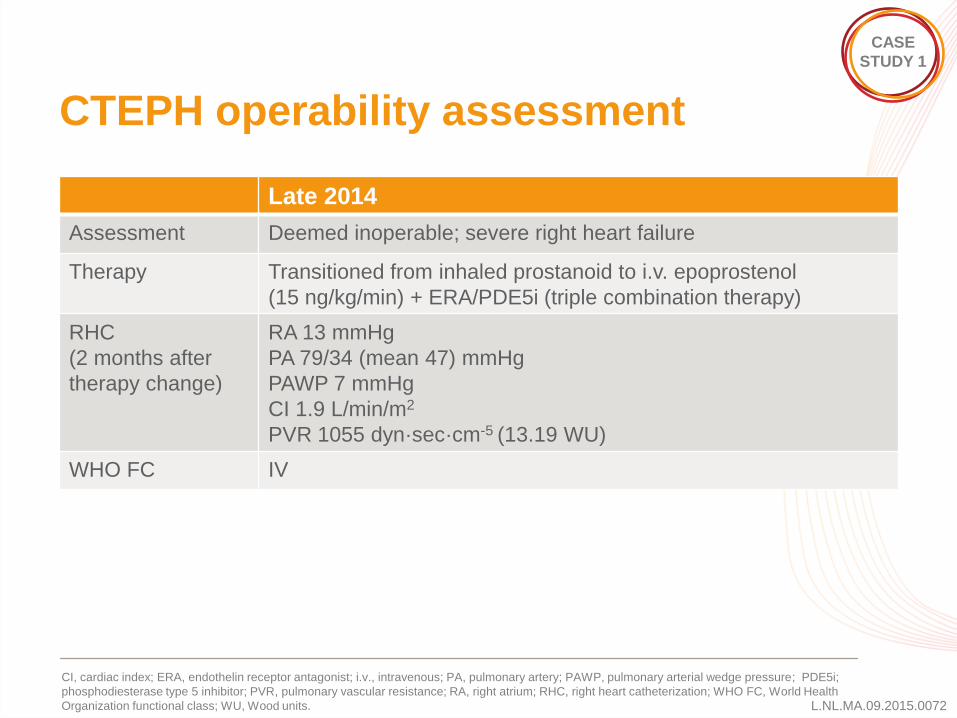
CTEPH operability assessment
Late 2014
Assessment Deemed inoperable; severe right heart failure
Therapy Transitioned from inhaled prostanoid to i.v. epoprostenol
(15 ng/kg/min) + ERA/PDE5i (triple combination therapy)
RHC
(2 months after
therapy change)
RA 13 mmHg
PA 79/34 (mean 47) mmHg
PAWP 7 mmHg
CI 1.9 L/min/m2
PVR 1055 dyn·sec·cm-5 (13.19 WU)
WHO FC IV
CI, cardiac index; ERA, endothelin receptor antagonist; i.v., intravenous; PA, pulmonary artery; PAWP, pulmonary arterial wedge pressure; PDE5i;
phosphodiesterase type 5 inhibitor; PVR, pulmonary vascular resistance; RA, right atrium; RHC, right heart catheterization; WHO FC, World Health
Organization functional class; WU, Wood units.
CASE
STUDY 1

L.NL.MA.09.2015.0072
What would you recommend now?
1. Lung transplantation
2. Transition to other medications
3. PEA
4. Hospice referral
PEA, pulmonary endarterectomy.
CASE
STUDY 1
VOTE NOW!

CASE
STUDY 1
20
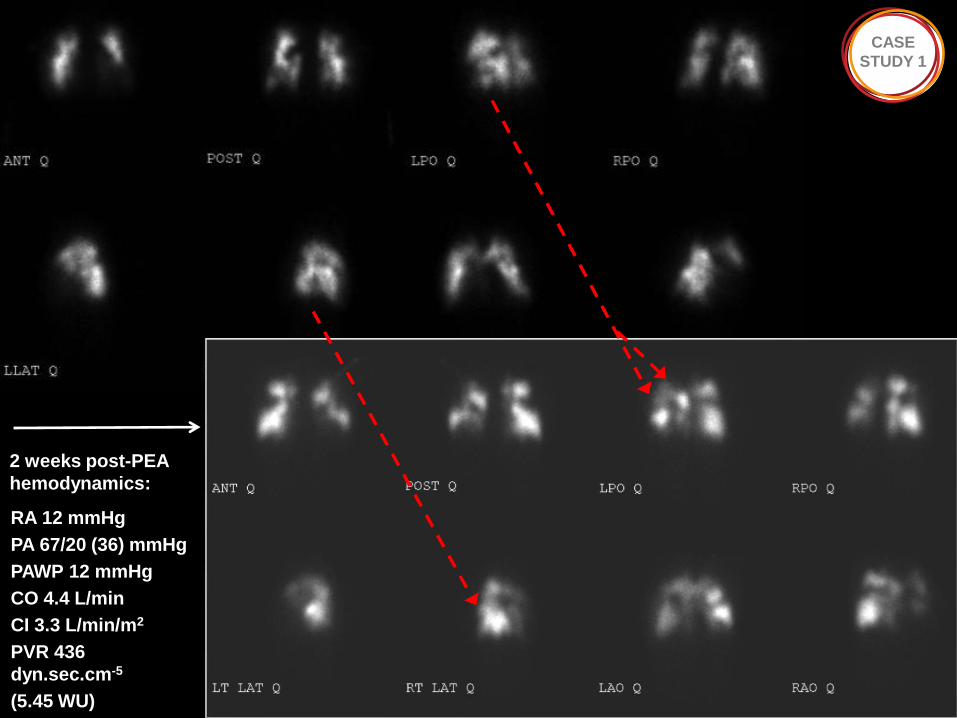
RA 12 mmHg
PA 67/20 (36) mmHg
PAWP 12 mmHg
CO 4.4 L/min
CI 3.3 L/min/m2
PVR 436
dyn.sec.cm-5
(5.45 WU)
CASE
STUDY 1
2 weeks post-PEA
hemodynamics:
L.NL.MA.09.2015.0072
Follow-up at 2 months after PEA
Off all meds except warfarin, spironolactone, and prednisone taper
(transient lung injury)
WHO FC II; oxygen 2 L/min with exertion
SBP 110s, HR 90s; No JVD, accentuated P2, no S3, wound healed,
lungs clear, no hepatomegaly, no edema
Shortness of breath with activity, chest pain
Started riociguat for persistent symptomatic CTEPH after PEA
HR, heart rate; JVD, jugular vein distension; PEA, pulmonary endarterectomy; SBP, systolic blood pressure; WHO FC,World Health Organization functional
class. 21
CASE
STUDY 1
L.NL.MA.09.2015.0072
Longer term follow-up after PEA
On riociguat TID: early subjective benefit
4 month visit: off oxygen, WHO FC I
No limitations; cleared to return home after
securing riociguat
Now back home, over 6 months after PEA
and 4 months on riociguat: WHO FC I
PEA, pulmonary endarterectomy; TID, three times daily; WHO FC, World Health Organization functional class. 22
CASE
STUDY 1
Sustained, improved activities of daily living with
riociguat for persistent CTEPH post-PEA
Case study 2 Inoperable CTEPH
Irene M Lang
L.NL.MA.09.2015.0072
Case study
38-year-old woman
History Dyspnea on exertion since 2013, arterial
hypertension, pulmonary embolism July 2013 and
June 2014
CASE
STUDY 2
November 2014: referred to Medical University of
Vienna for evaluation of PH
Confidential patient information: slides not shown
L.NL.MA.09.2015.0072
Unresolved issues in CTEPH
Optimal path toward timely and accurate diagnosis of CTEPH
L.NL.MA.09.2015.0072
Do you have resources to follow the current
guidelines for CTEPH?
1. Yes: we have access to V/Q scan, pulmonary angiography (either
catheter, CT, or MRI), and a CTEPH team for operability
assessment
2. No: we do not have access to V/Q scan or pulmonary angiography
3. No: we do not have access to a CTEPH team for operability
assessment
4. We use our own guidelines (disagree with what’s published!)
CT, computed tomography; V/Q, ventilation/perfusion; MRI, magnetic resonance imaging.
VOTE NOW!
L.NL.MA.09.2015.0072
Unresolved issues in CTEPH
Optimal path toward timely and accurate diagnosis of CTEPH
Operability versus opinion?
Role of medical therapy (bridge) in operable CTEPH
Place for BPA in the treatment of CTEPH
BPA, balloon pulmonary angioplasty.
L.NL.MA.09.2015.0072
What is your top priority of interest in
CTEPH?
1. Access or establishment of a PEA program
2. Further exploring/expanding medical therapy for CTEPH
3. Establishing BPA in your center
4. Receiving more CTEPH referrals (we don’t see enough)
VOTE NOW!
BPA, balloon pulmonary angioplasty; PEA, pulmonary endartectomy.
L.NL.MA.09.2015.0072
Summary
CTEPH patients should be evaluated for surgical eligibility by a
multidisciplinary team of experts using high-quality imaging
technologies
Riociguat is an alternative for patients who are inoperable or have
persistent CTEPH after PEA, which can improve exercise capacity,
hemodynamics, functional class, and RV function
Whilst there are clear guidelines for the management of CTEPH,
there is still much work ahead to address the unanswered questions
that remain
PEA, pulmonary endartectomy; RV, right ventricle.

Thank you