Embed Size (px)
Citation preview
12/15/2015
1
Line-associated DVT, Calf Vein DVT
and Superficial Vein Thrombosis:
What to do.
Ian Del Conde, MD, FACC
Vascular Medicine and Cardiology
Miami Cardiac and Vascular Institute
HeartWell
December 12, 2015
Disclosures
CONSULTANT
Merck; New Haven Pharmaceuticals
ADVISORY BOARD
Merck, IC Sciences
SPEAKER’S BUREAU
Johnson & Johnson, BMS, Pfizer
12/15/2015
2
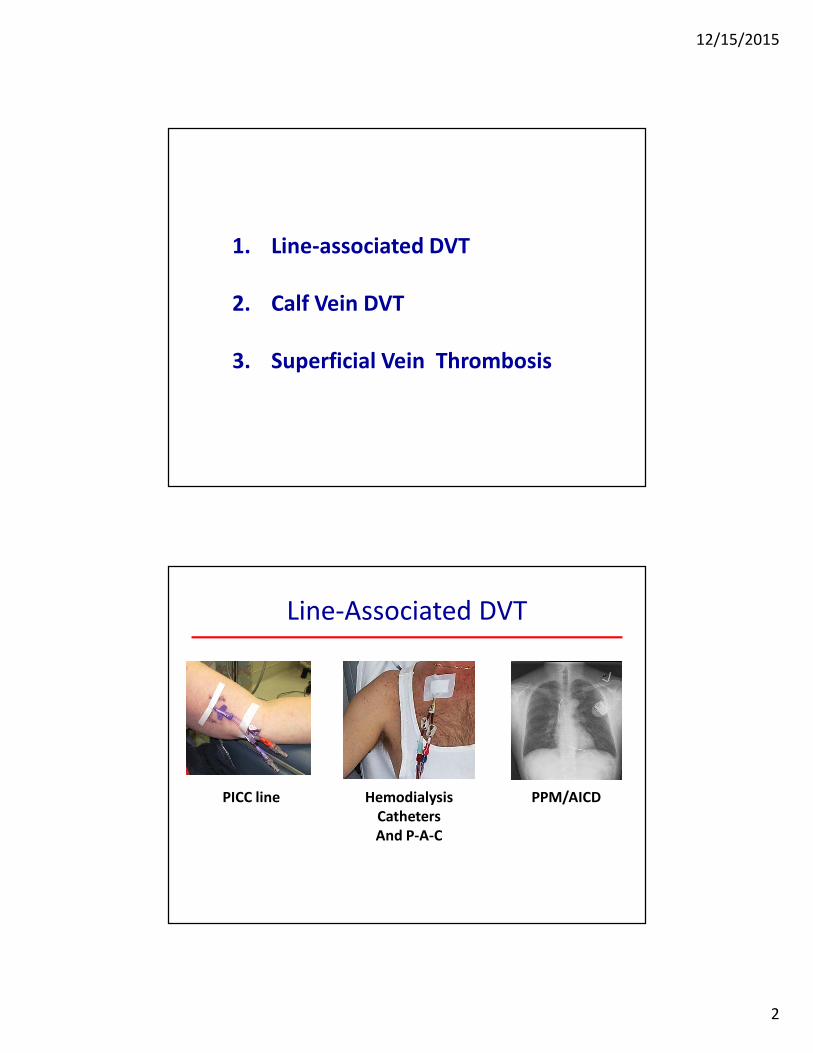
1. Line-associated DVT
2. Calf Vein DVT
3. Superficial Vein Thrombosis
Line-Associated DVT
PICC line Hemodialysis
Catheters
And P-A-C
PPM/AICD
12/15/2015
3
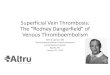
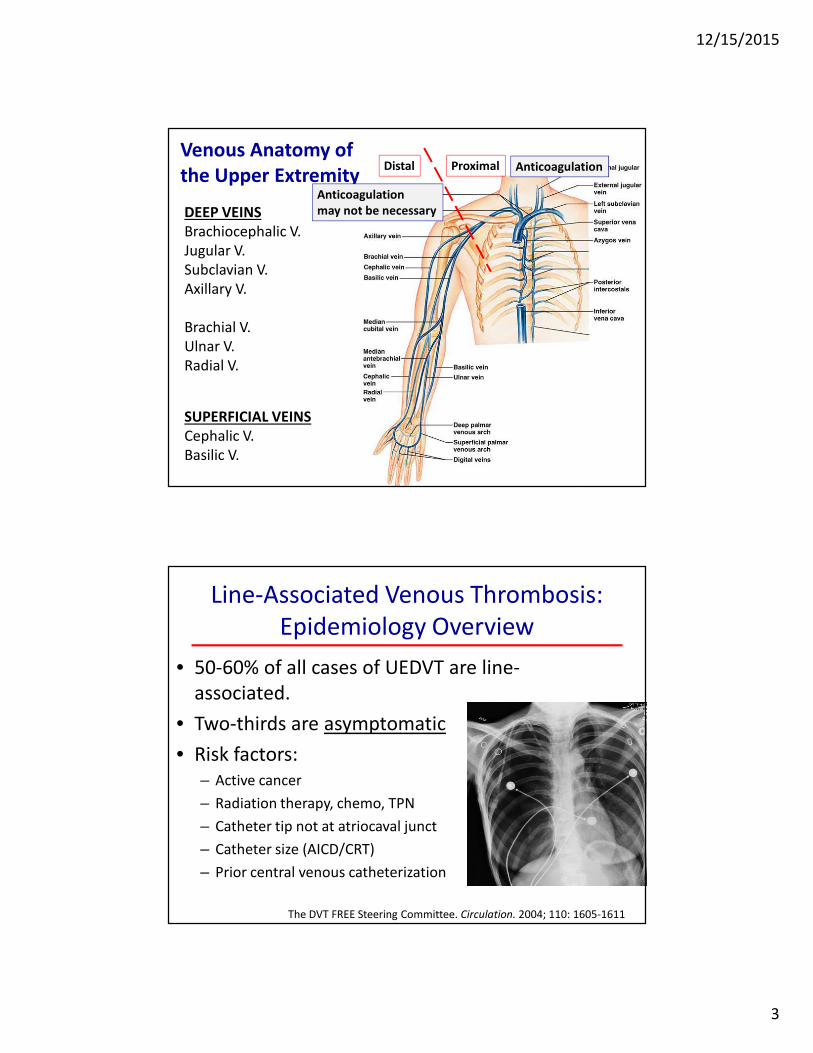
Venous Anatomy of
the Upper Extremity
DEEP VEINS
Brachiocephalic V.
Jugular V.
Subclavian V.
Axillary V.
Brachial V.
Ulnar V.
Radial V.
SUPERFICIAL VEINS
Cephalic V.
Basilic V.
ProximalDistal Anticoagulation
Anticoagulation
may not be necessary
Line-Associated Venous Thrombosis:
Epidemiology Overview
• 50-60% of all cases of UEDVT are line-
associated.
• Two-thirds are asymptomatic
• Risk factors:
– Active cancer
– Radiation therapy, chemo, TPN
– Catheter tip not at atriocaval junct
– Catheter size (AICD/CRT)
– Prior central venous catheterization
The DVT FREE Steering Committee. Circulation. 2004; 110: 1605-1611
12/15/2015
4
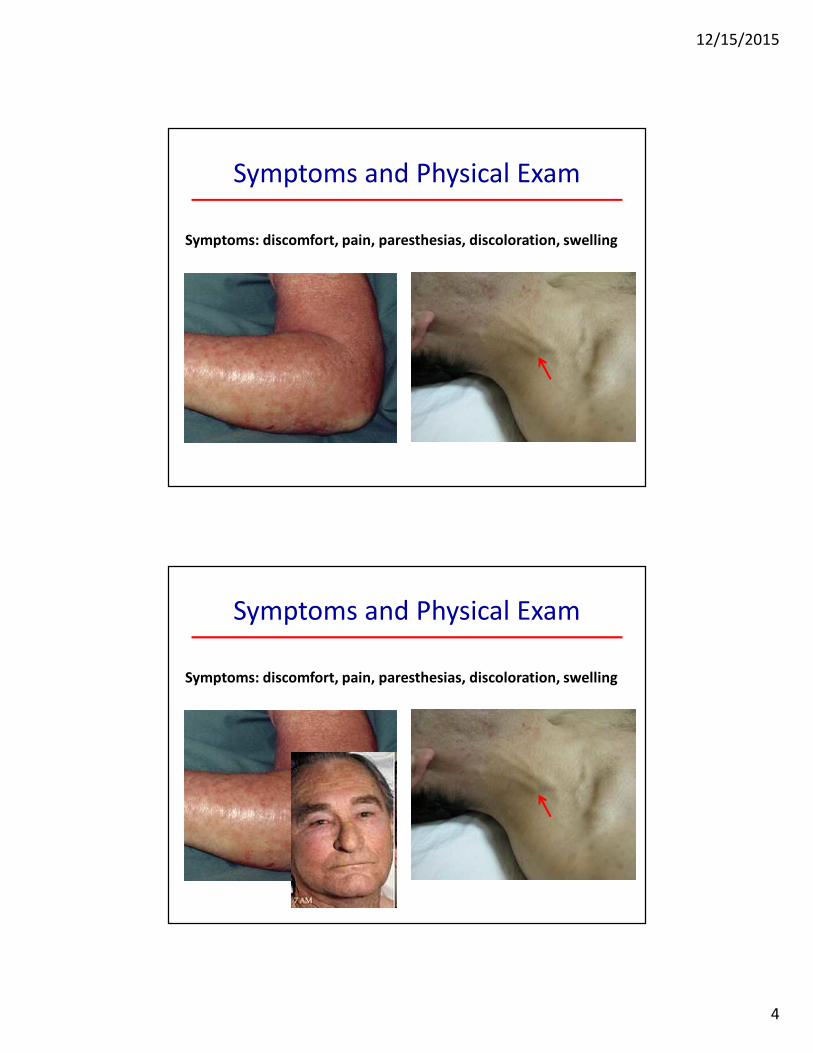
Symptoms and Physical Exam
Symptoms: discomfort, pain, paresthesias, discoloration, swelling
Symptoms and Physical Exam
Symptoms: discomfort, pain, paresthesias, discoloration, swelling
12/15/2015
5
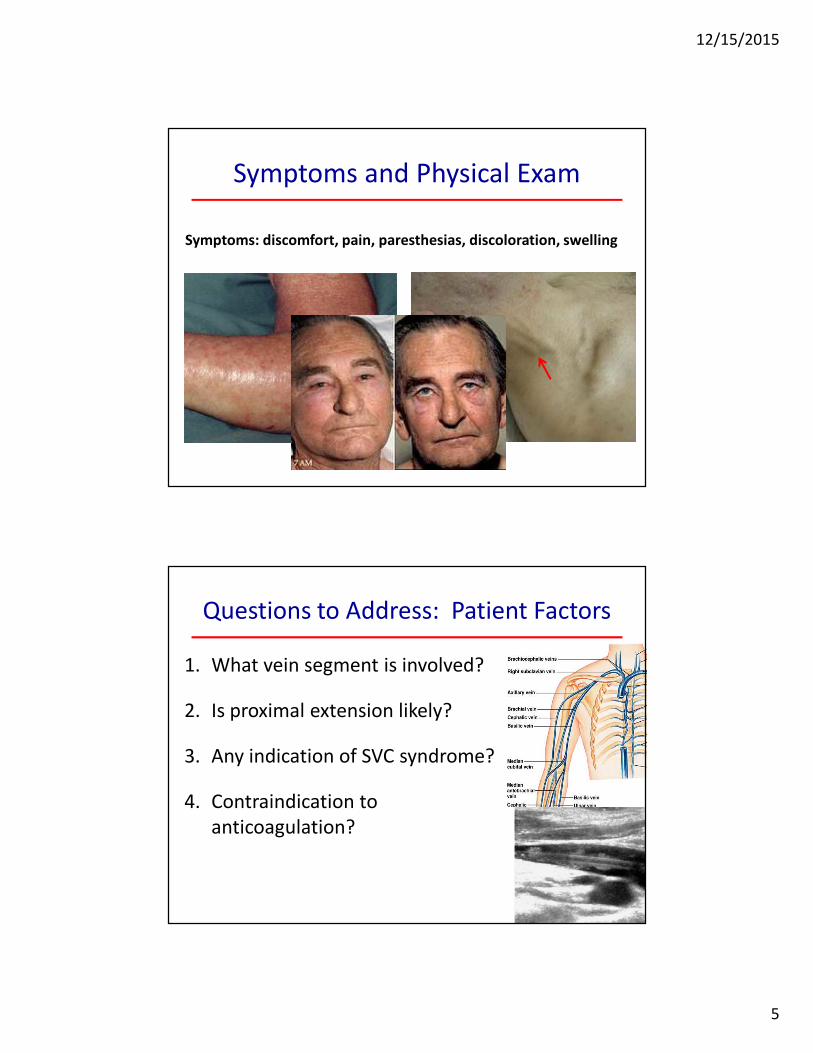
Symptoms and Physical Exam
Symptoms: discomfort, pain, paresthesias, discoloration, swelling
Questions to Address: Patient Factors
1. What vein segment is involved?
2. Is proximal extension likely?
3. Any indication of SVC syndrome?
4. Contraindication to
anticoagulation?
12/15/2015
6
Questions to Address: Catheter Factors
1. Is the catheter still needed? (IV meds, blood draws, TPN, etc.)
2. Is the catheter functional?
3. Any evidence of infection?
Management of Catheter Associated UE DVT
Routine catheter removal is generally not
recommended
• Difficult access, continued need for
further IV access should be considered
• Must be able to anticoagulate the
patient
Removal is warranted in:
• Malfunctioning catheter, infection,
contraindication to anticoagulation,
persistent signs and symptoms despite
treatment.
12/15/2015
7
What do the Guidelines Say?
• Anticoagulate for as long as the catheter
remains in place.
• If the catheter is removed, and the DVT involves
the axillary or subclavian veins, anticoagulate
for 3 months (longer if the patient has cancer).
Calf Vein
Thrombosis
Opinions differ:
• Need to examine
calf veins?
• Need to treat?
12/15/2015
8
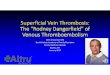
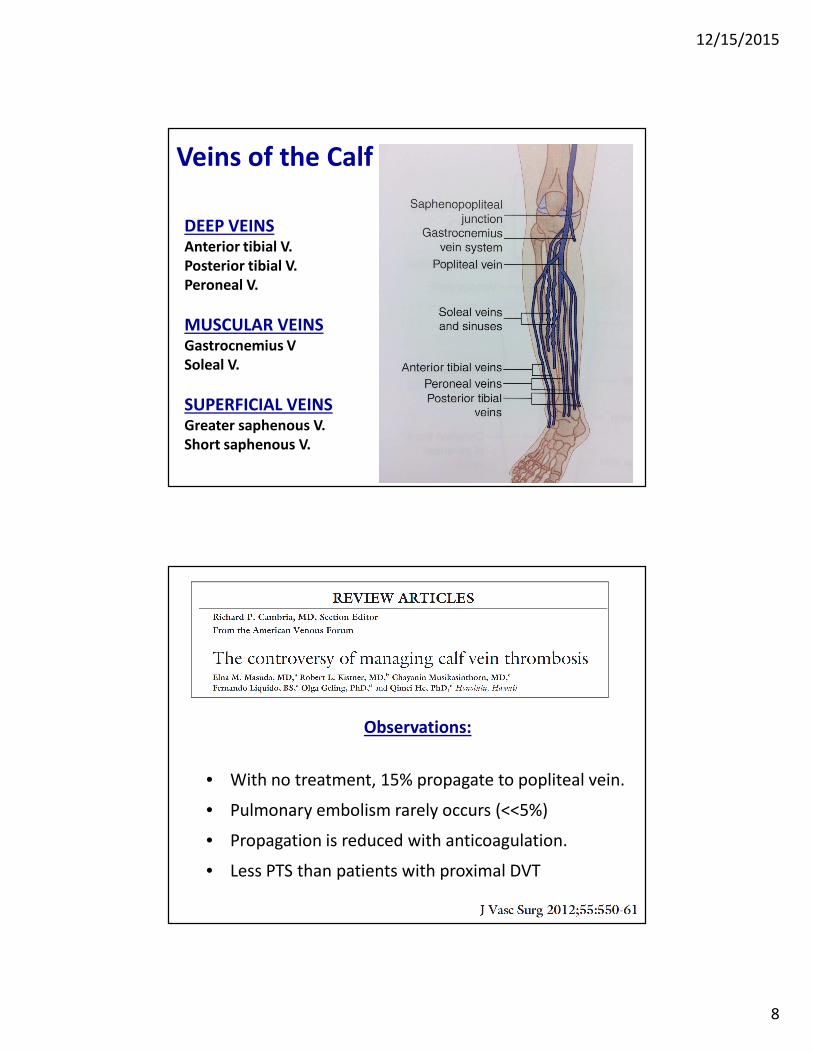
DEEP VEINSAnterior tibial V.
Posterior tibial V.
Peroneal V.
MUSCULAR VEINSGastrocnemius V
Soleal V.
SUPERFICIAL VEINSGreater saphenous V.
Short saphenous V.
Veins of the Calf
Observations:
• With no treatment, 15% propagate to popliteal vein.
• Pulmonary embolism rarely occurs (<<5%)
• Propagation is reduced with anticoagulation.
• Less PTS than patients with proximal DVT
12/15/2015
9
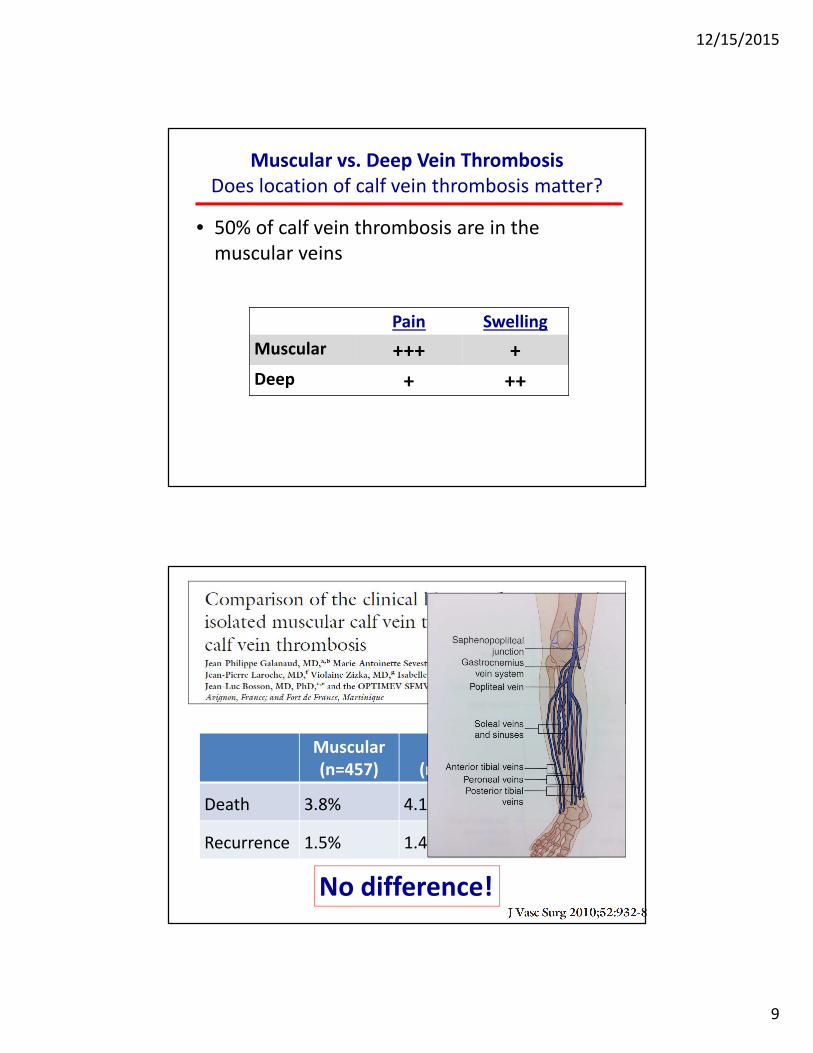
Muscular vs. Deep Vein Thrombosis
Does location of calf vein thrombosis matter?
• 50% of calf vein thrombosis are in the
muscular veins
Pain Swelling
Muscular +++ +
Deep + ++
Muscular
(n=457)
Axial
(n=222)
P value
Death 3.8% 4.1% 0.98
Recurrence 1.5% 1.4% 0.98
No difference!
12/15/2015
10
• Who to treat with anticoagulation?
• Symptomatic patients
• Risk factors for extension
• Full-dose anticoagulation,
(same as for prox. DVT)
Calf Vein Thrombosis: Bottom Line
2012 ACCP Guidelines
• Extensive
• > 2 veins
• Close to prox. veins
• > 7 mm in diameter
• Who to treat with anticoagulation?
• Symptomatic patients
• Risk factors for extension
• Full-dose anticoagulation,
(same as for prox. DVT)
• If anticoagulation is not prescribed, serial
duplex ultrasounds for 2 weeks.
Calf Vein Thrombosis: Bottom Line
• Extensive
• > 2 veins
• Close to prox. veins
• > 7 mm in diameter
2012 ACCP Guidelines
12/15/2015
11
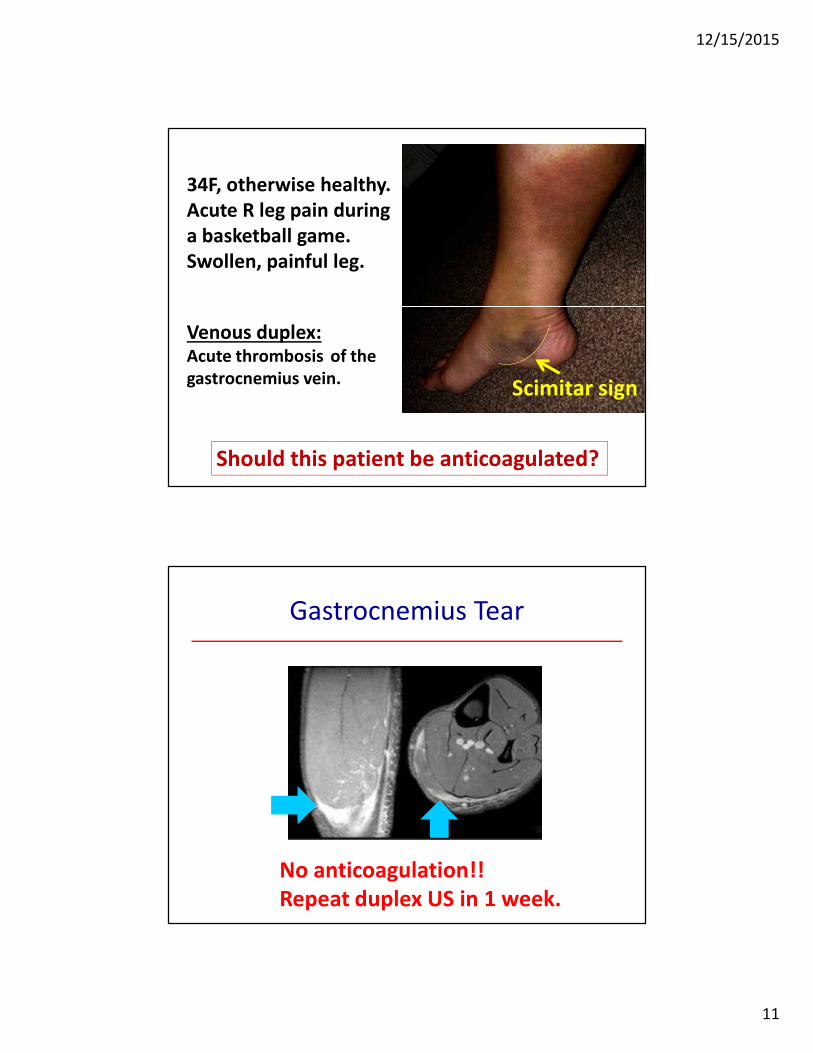
34F, otherwise healthy.
Acute R leg pain during
a basketball game.
Swollen, painful leg.
Venous duplex:Acute thrombosis of the
gastrocnemius vein.
Should this patient be anticoagulated?
Scimitar sign
Gastrocnemius Tear
No anticoagulation!!
Repeat duplex US in 1 week.
12/15/2015
12
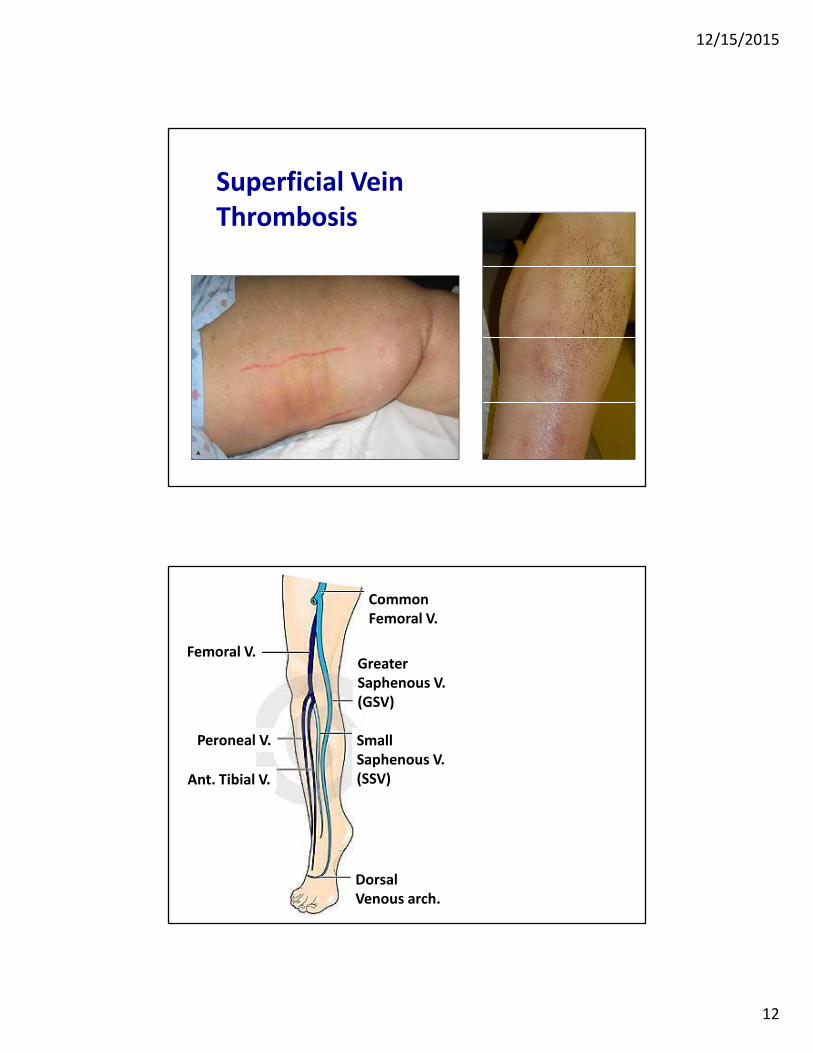
Superficial Vein
Thrombosis
Femoral V.
Peroneal V.
Ant. Tibial V.
Greater
Saphenous V.
(GSV)
Common
Femoral V.
Small
Saphenous V.
(SSV)
Dorsal
Venous arch.
12/15/2015
13
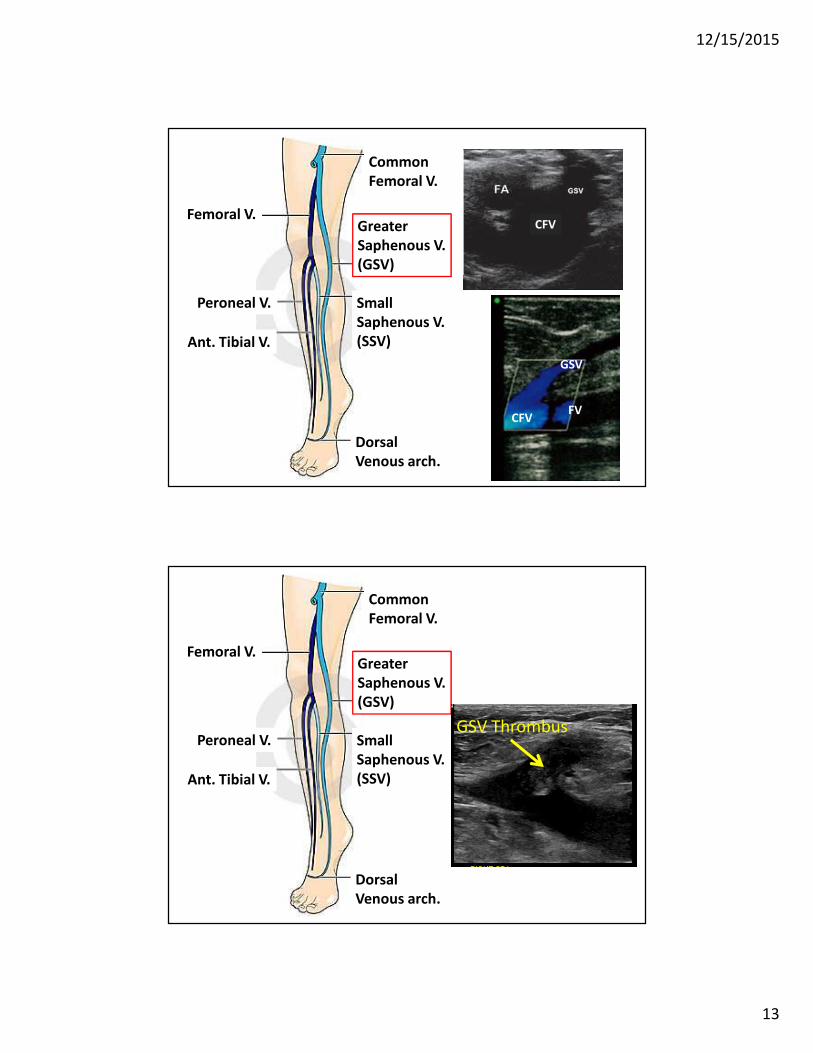
Femoral V.
Peroneal V.
Ant. Tibial V.
Greater
Saphenous V.
(GSV)
Common
Femoral V.
Small
Saphenous V.
(SSV)
Dorsal
Venous arch.
GSV
FVCFV
CFV
Femoral V.
Peroneal V.
Ant. Tibial V.
Greater
Saphenous V.
(GSV)
Common
Femoral V.
Small
Saphenous V.
(SSV)
Dorsal
Venous arch.
GSV Thrombus
12/15/2015
14
Femoral V.
Peroneal V.
Ant. Tibial V.
Greater
Saphenous V.
(GSV)
Common
Femoral V.
Small
Saphenous V.
(SSV)
Dorsal
Venous arch.
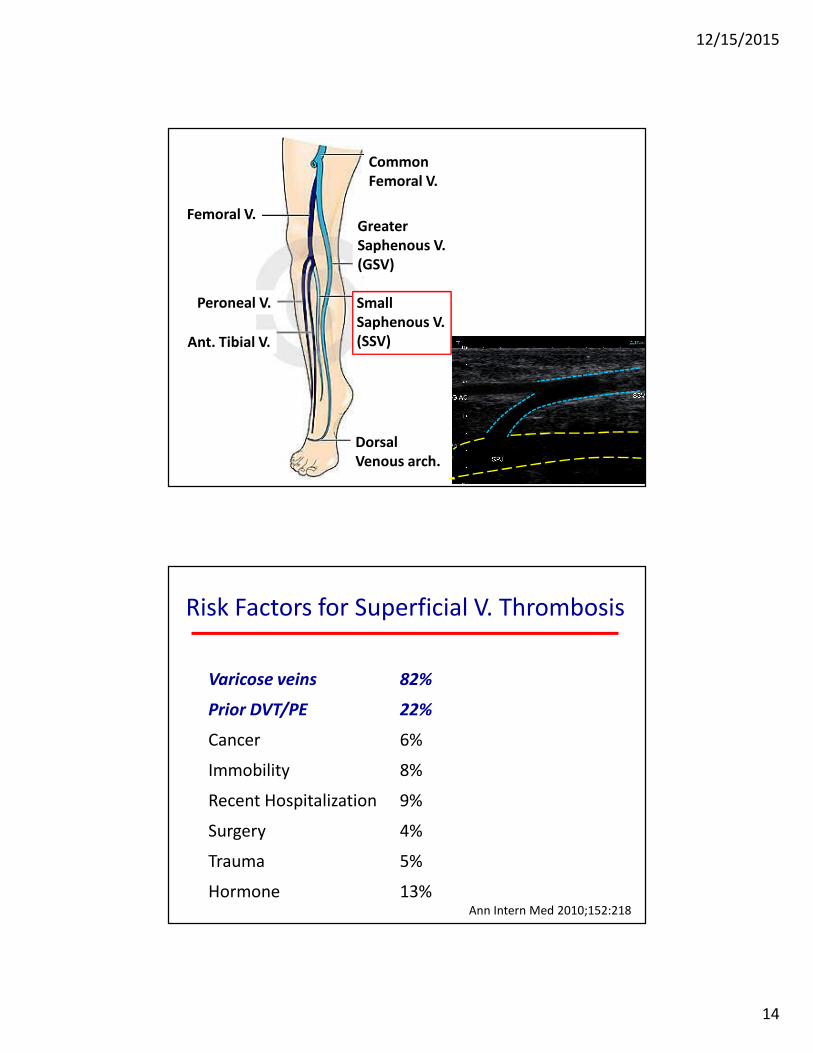
Varicose veins 82%
Prior DVT/PE 22%
Cancer 6%
Immobility 8%
Recent Hospitalization 9%
Surgery 4%
Trauma 5%
Hormone 13%
Risk Factors for Superficial V. Thrombosis
Ann Intern Med 2010;152:218
12/15/2015
15
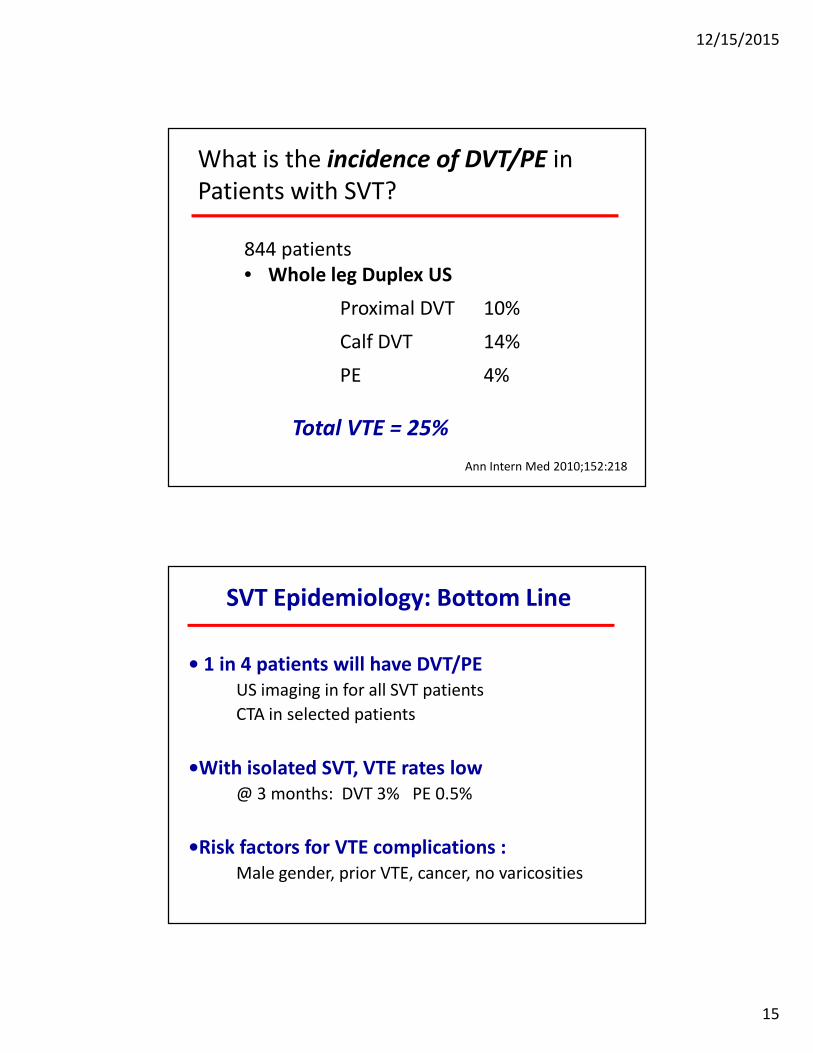
What is the incidence of DVT/PE in
Patients with SVT?
844 patients
• Whole leg Duplex US
Proximal DVT 10%
Calf DVT 14%
PE 4%
Total VTE = 25%
Ann Intern Med 2010;152:218
• 1 in 4 patients will have DVT/PE
US imaging in for all SVT patients
CTA in selected patients
•With isolated SVT, VTE rates low
@ 3 months: DVT 3% PE 0.5%
•Risk factors for VTE complications :
Male gender, prior VTE, cancer, no varicosities
SVT Epidemiology: Bottom Line
12/15/2015
16
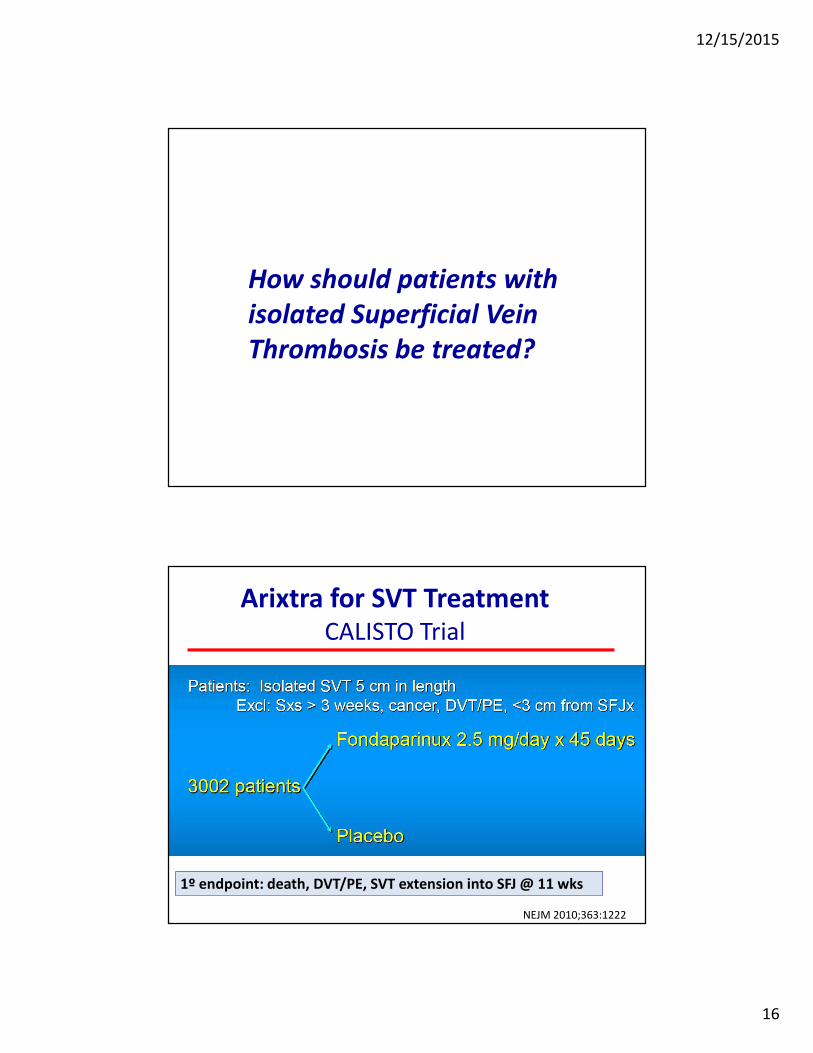
How should patients with
isolated Superficial Vein
Thrombosis be treated?
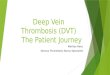
Arixtra for SVT TreatmentCALISTO Trial
NEJM 2010;363:1222
1º endpoint: death, DVT/PE, SVT extension into SFJ @ 11 wks
12/15/2015
17
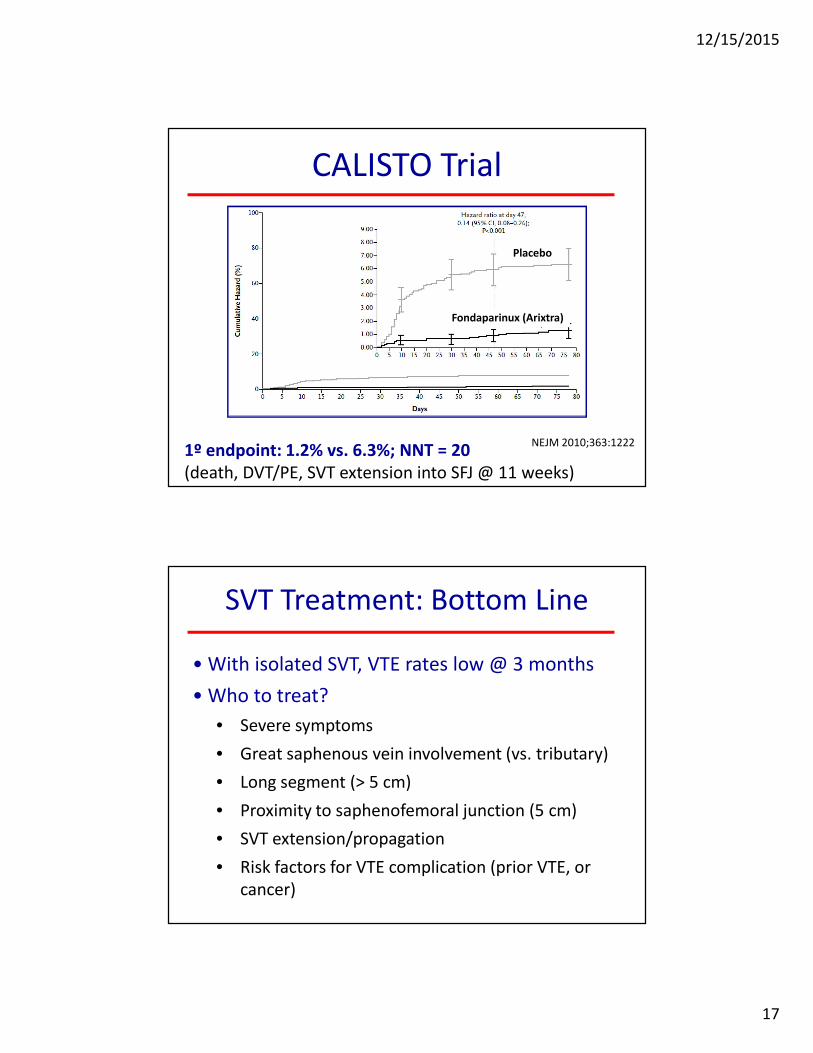
1º endpoint: 1.2% vs. 6.3%; NNT = 20
(death, DVT/PE, SVT extension into SFJ @ 11 weeks)
NEJM 2010;363:1222
CALISTO Trial
Fondaparinux (Arixtra)
Placebo
• With isolated SVT, VTE rates low @ 3 months
• Who to treat?
• Severe symptoms
• Great saphenous vein involvement (vs. tributary)
• Long segment (> 5 cm)
• Proximity to saphenofemoral junction (5 cm)
• SVT extension/propagation
• Risk factors for VTE complication (prior VTE, or
cancer)
SVT Treatment: Bottom Line
12/15/2015
18
• How to treat?
Arixtra 2.5 mg QD (prophy dose)
Prophylactic does LMWH
Novel Anticoagulant?
• How long to treat?
6 weeks
SVT Treatment: Bottom Line
•Lower limb SVT ≥ 5 cm in length, we suggest
prophylactic fondaparinux or LMWH for 45
days over no anticoagulation (Grade 2B).
•We suggest fondaparinux 2.5 mg daily over
prophylactic LMWH (Grade 2C).
2012 ACCP Guidelines: Superficial Vein Thrombosis
ACCP Guidelines 2012