Embed Size (px)
DESCRIPTION
not pharmacological prevention of deep venous thrombosis
Citation preview

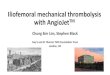
not-‐pharmacological periopera0ve profilaxys

general methods mobiliza(on hydra(on
elas(c compression caval filters pneuma(c compression
mechanical prophylaxis
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

moderate risk
high risk
very high risk
Preven&on and management of venous thromboembolism in the surgical pa&ent: op&ons by surgery type and individual pa&ent risk factors, The American Journal of Surgery, Vol 199, Jan 2010
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

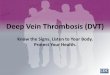
Knudson Ann Surg 2004; 240:490-‐498
INJURED PATIENT
High Risk Factors (Odds ra0o for VTE = 2 – 3) • Age ≥ 40 • Pelvic fx • Lower extremity fx • Shock • Spinal cord injury • Head Injury (AIS ≥ 3)
Very High Risk Factors (Odds ra0o for VTE = 4 -‐ 10)
• Major opera0ve procedure • Venous injury • Ven0lator days > 3 • 2 or more high risk factors
Does the pa0ent have contraindica0ons for Heparin?
Does the pa0ent have contraindica0ons for Heparin?
Yes No
Yes No
Mechanical Compression
LMWH*
* Prophylac0c dose
LMWH* and Mechanical Compression
Mechanical Compression and serial CFDI
OR Temporary IVC filter
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

We recommend that mechanical methods of thromboprophylaxis be used primarily in pa0ents at high risk for bleeding (Grade 1A), or possibly as an adjunct to an0coagulant – based thromboprophylaxis (Grade 2A).
For pa0ents receiving mechanical methods of thromboprophylaxis, we recommend that careful a_en0on be directed toward ensuring the proper use of, and op0mal adherence with, these methods (Grade 1A).
Kearon et al. AnJthromboJc Therapy for Venous Thromboembolic Disease: American
College of Chest Physicians Evidence-‐Based Clinical PracJce Guidelines (8th EdiJon). Chest 2008; 133; 454-‐545
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

Rimozione quotidiana per ispezione cute se riduzione significativa mobilità, integrità della cute compromessa e ridotta sensibilità 2-3 volte giorno specie talloni e prominenze ossee. Ensure that patients who develop oedema or postoperative swelling have their legs re-measured and anti-embolism stockings refitted. Use anti-embolism stockings that provide graduated compression and produce a calf pressure of 14–15 mmHg. Se collaborante coinvolgere il paziente ad indossarle in modo corretto mopnitorando la comprensione Se collaborante coinvolgere il paziente ad indossarle in modo corretto mopnitorando la comprensione
For general surgery pa0ents with mul0ple risk factors for VTE who are thought to be at par0cularly high risk, we recommend that a pharmacologic method … be combined with the op0mal use of a mechanical method (ie, graduated compression stockings [GCS] and/or IPC) (Grade 1C).
For general surgery pa0ents with a high risk of bleeding, we recommend the op0mal use of mechanical thromboprophylaxis with properly fi_ed GCS or IPC (Grade 1A). When bleeding risk decreases, we recommend that pharmacologic prophylaxis be s u b s 0 t u t e d f o r o r a d d e d t o me c h a n i c a l prophylaxis (Grade 1C).
Kearon et al. AnJthromboJc Therapy for Venous Thromboembolic Disease: American College
of Chest Physicians Evidence-‐Based Clinical PracJce Guidelines (8th EdiJon). Chest 2008; 133; 454-‐545
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

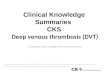
SCD
foot impulse devices
sequen0al compression devices
SCD
FP
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

graduated compression stockings
SCD AES
G C S
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

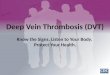
DVT anamnesis/suspect
controindicazioni SCD
conges0ve heart failure/pulmonary edema Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

bone lesions
edema
not treated -‐ infected sores
recent sutures
fasci0s, gangrene
arterial bypass graging skin gag
vasculopathies neuropathies
obesity malforma0ons
edema
foot pumps !
controindicazioni AES/SCD
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care

Offer VTE prophylaxis to pa0ents undergoing gastrointes0nal surgery who are assessed to be at increased risk of VTE or pa0ents undergoing bariatric surgery
S t a r t a t admi s s ion , con0nue un0l pa0ent n o l o n g e r h a s significantly reduced mobility.
Choose any one of: AES, foot impulse devices, IPC … Base choice on individual factors including clinical condi0on, surgical procedure and pa0ent preference. Add pharmacological prophylaxis if low risk of major bleeding
Venous thromboembolism – reducing the risk, NICE guidelines 2007
Velia Marta Antonini, Parma University Hospital - I° Department of Anesthesia and Intensive Care