Embed Size (px)
Citation preview

CALIFORNIA STATE UNIVERSITY, NORTHRIDGE
Affordable Care Act: The Effects of Not Expanding Medicaid
A Graduate Project Submitted in Partial Fulfillment of the Requirements for the Degree of
Master of Public Administration, Health Administration
By
Judith Chandrasena
August 2021
ii
The Graduate Project of Judith Chandrasena is Approved:
____________________________________ ____________________________
Dr. David Powell Date
_________________________________________ ___________________________
Dr. Frankline Augustin Date
_________________________________________ ___________________________
Dr. Kyusuk "Stephan" Chung, Chair Date
California State University, Northridge

iii
Table of Contents
Signature Page………………………………………………………………………………….…ii
Abstract……………………………………………………………………………………………v
Introduction ..................................................................................................................................... 1
Literature Review............................................................................................................................ 4
Medicaid ..................................................................................................................................... 4
Medicaid Programs and Eligibility ............................................................................................. 4
Children's Health Insurance Program (CHIP) ........................................................................ 4
Basic Health Program ............................................................................................................. 5
Opt-Out States ............................................................................................................................. 6
Adopted ACA but Not Implement .............................................................................................. 8
Socioeconomic Consequences .................................................................................................... 9
Population Health...................................................................................................................... 10
If States were to Repeal ACA ................................................................................................... 11
Cost of Healthcare in Non-Expansion States ............................................................................ 14
Texas ..................................................................................................................................... 14
Wyoming............................................................................................................................... 15
Cost of Healthcare where ACA is Adopted .............................................................................. 17
California & New York ........................................................................................................ 17
Economic Effects of Medicaid Non-Expansion States on Hospitals ........................................ 20
Methodology ................................................................................................................................. 22
Methodology Chart ................................................................................................................... 24
Findings/Analysis ......................................................................................................................... 25
Positive Health Outcomes ......................................................................................................... 25
States' Economics and Politics .................................................................................................. 26
American Rescue Plan Act ....................................................................................................... 27
Policy Implications ....................................................................................................................... 30
Conclusion .................................................................................................................................... 33
References ..................................................................................................................................... 35
Appendix: List of Figures ............................................................................................................. 44

iv
Abstract
Affordable Care Act: The Effects of Not Expanding Medicaid
By
Judith Chandrasena
Master of Public Administration, Health Administration
One of The Affordable Care Act (ACA) 's main goals is to increase access in the United States
through insurance marketplace reforms, mandates, and Medicaid Expansion which started to take
effect in 2014. Medicaid Expansion offered coverage and affordability to all citizens, primarily to
those in poverty. States that did not expand Medicaid have gone through much scrutiny due to the
lack of coverage to its citizens and the lack of compensation to the hospitals and providers. The 12
states that opted out of the ACA failed to provide an alternate medical coverage plan for their
citizens. This literature review, through qualitative analysis, examined the socioeconomic,
population health, and economic effects on hospitals in non-expansion states through contrasting
the expansion and non-expansion of Medicaid through the country.

v
The consequences of opting out contributed to poor population health in that people are hesitant
to seek medical care for fear of incurring medical bills. Physicians and hospitals are in a bind
because they must render medical attention, knowing that they will not get adequate funding to
stay in business. The federal government purposefully withholds additional funding for Medicaid
as an incentive to try and get the 12 states to adopt slow but steady progress. Additional policy
efforts are needed to encourage non-expansion states to expand Medicaid.

1
Introduction
As of July 2021, 39 states (including DC) have adopted the Medicaid expansion, and 12
states have not adopted the expansion (U.S. Centers for Medicare & Medicaid Services, 2018).
The Obama administration explained that states who refused funding for Medicaid expansion
were making a political point. The 12 non-expansion states are Republican-led states (Leonard,
2015). Some lawmakers expressed that they do not trust the federal government about honoring
its commitment to keep up the level of support over the long term. The individual mandate –
which requires most people to maintain health insurance coverage or pay the penalty (Kamal et
al., 2018) of 10% cost is too much for their already-strained budgets (Leonard, 2015). In
addition, states believed that Washington should give them greater control over spending to
better fit coverage expansion within their states (Turner, 2013).
The Affordable Care Act (ACA) offers medical insurance to uninsured Americans,
including preventive and primary care services. The legislation is built on a multi-prong
framework - cost, access, and quality. First, the ACA promises to make health insurance
affordable to all Americans and covers 138% below the federal poverty level. Second, the Act
codified protections for preexisting conditions and eliminated patient cost-sharing for high-value
preventive services. Last, the law goes beyond coverage, requiring employers to provide
breastfeeding mothers with breaks at work, making calorie counts more widely available in
restaurants, and creating the Prevention and Public Health Fund. This law helps the Centers for
Disease Control and Prevention (CDC) and state agencies detect and respond to health
threats such as COVID-19 (Rapfogel et al., 2020).
Medicaid expansion ultimately contributes to population health improvement (Kino &
Kawachi, 2018. Vulnerable populations are particularly at risk for insufficient health insurance

2
coverage; people with lower incomes are often uninsured, and minorities account for over half of
the uninsured population. Inadequate health insurance coverage is one of the most significant
barriers to healthcare access, and the unequal distribution of the coverage contributes to
disparities in health. Out-of-pocket medical care costs may lead individuals to delay or forgo
needed care, such as doctor's visits, dental care, and medication. In addition, medical debt is
common among insured and uninsured individuals (Access to Health Services | Healthy People
2020, 2020).
This thesis comprises various literature reviews that focus on the 12 states that did not
adopt the ACA expansion. First, a brief definition of what Medicaid is is discussed. Then,
programs under Medicaid that provide health insurance coverage to children, the Children's
Health Insurance Program (CHIP), and the Basic Health Programs for adults that meet the
federal poverty level are assessed. States that opt-out of Medicaid expansion is looked at closely,
evaluating the effects of non-expansion. The findings exposed the cost of the uninsured to the
healthcare system and the vulnerability to population health. Medicaid expansion is associated
with a 4.4% to 4.7% reduction in state spending on traditional Medicaid. For example, Medicaid
spending on mental health care within the correctional system and a decrease in uncompensated
care range from 14% of the expansion cost in Kentucky to 30% in Arkansas (Ward, 2020). The
literature review showed how individual mandates affect enrollment decisions and assess the
effects of eliminating the penalty on enrollment, premiums, and the federal deficit (Eibner &
Nowak, 2019). The Supreme Court ruling allowed the states the choice to expand. The results of
states decisions are evident in every literature review. The burden of care has fallen on the states.
First, a brief description of what Medicaid is, the kind of programs under Medicaid, what states
did and did not adopt the ACA, the socioeconomic and overall population health, and the
3
economic consequences of the failure to adopt are provided. Next, a comparison is made
between states that adopted the ACA expansion and states that opt-out. The evidence showed the
differences in cost, access to healthcare for the vulnerable, and the difference in a healthier
population.
This research concludes by showing how expansion to Medicaid proves that individuals
with coverage improve overall health (Kagan & Catalano, 2019). First, the adoption of the ACA
reduces financial burdens significantly. Second, uninsured patients' costs are "absorbed" by the
federal government, localities, and states that support the operation of hospitals and clinics, both
through appropriations and implicit subsidies like Medicare and Medicaid. Lastly, philanthropic
donations are depleted (Institute of Medicine (US) Committee on the Consequences of
Uninsurance, 2003). Fourth, Medicaid expansion increases cost by increased usage of medical
resources. However, these factors still outweigh increased revenue by Medicaid expansion (Stan
Dorn et al., 2014).

4
Literature Review
Medicaid
Medicaid is a public insurance program created in 1965 and authorized by Title XIX of the
Social Security Act (Program History | Medicaid.gov, 2015). All states, the District of
Columbia, and the U.S. territories have Medicaid programs designed to provide health coverage
for low-income families and individuals, including children, parents, pregnant women, seniors,
and people with disabilities. Funding for Medicaid is a joint effort between the federal
government and states. Each state is responsible for how the program operates, provided that
they are operating within federal guidelines (Policy Basics: Introduction to Medicaid, 2020).
Medicaid Programs and Eligibility
Children's Health Insurance Program (CHIP)
In 2018, Medicaid provided health coverage for 97 million low-income Americans over
the course of the year. In any given month, Medicaid served 32 million children, 28 million
adults (mostly in low-income working families), 6 million seniors, and 9 million people with
disabilities, according to Congressional Budget Office (CBO) estimates (Policy Basics:
Introduction to Medicaid, 2020). The Children's Health Insurance Program (CHIP), signed into
law in 1997, provides health coverage to eligible children through both Medicaid and separate
CHIP programs. As of 2018, 9.6 million children are enrolled in the CHIP program (Benefits |
Medicaid.gov, 2013). CHIP ensures mandatory benefits. For example, Well-Baby and Well-
Child are mandatory in each state, and they have the flexibility to determine the periodicity
schedule that defines when those visits should occur (Benefits | Medicaid.gov, 2013). Most states
use the schedules recommended by the American Academy of Pediatrics or Bright Futures to

5
organize the periodicity schedule. The schedule mandates dental visits, behavioral health
benefits, and vaccines (Bright Futures, 2019).
After declines in enrollment from 2017 through 2019, total Medicaid/CHIP enrollment
grew to 81.0 million in February 2021, an increase of 9.8 million from enrollment in February
2020 (13.8%), right before the pandemic and when enrollment began to steadily increase as
shown in figure 1. Increases in enrollment reflect changes in the economy (as more people
experience income and job loss and become eligible and enroll in Medicaid and CHIP coverage)
and provisions in the Families First Coronavirus Response Act (FFCRA) that require states to
ensure continuous coverage to current Medicaid enrollees to access a temporary increase in the
Medicaid match rates. Enrollment may continue to grow even as the economy recovers from the
effects of the pandemic and the Medicaid Open Enrollment (MOE) remains in place (Corallo &
2020, 2020).
Figure 1
Basic Health Program
The Basic Health Program (BHP) enacted by the ACA in 2providesvide states the option to
establish health benefits to cover programs for low-income residents who would otherwise be
6
eligible to purchase coverage through the Health Insurance Marketplace (Benefits |
Medicaid.gov, 2013). This program provides affordable coverage for individuals whose income
fluctuates above and below Medicaid and CHIP levels. The income level required is 200% of the
federal poverty level (FPL), and consumers would otherwise qualify for subsidies in the
marketplace. In addition to meeting income requirements, BHP-eligible consumers must be state
residents, age 64 or younger, U.S. citizens or lawfully present immigrants, and ineligible for
other minimum essential coverage, including Medicaid, CHIP, and affordable insurance offered
by an employer. BHP consumers are enrolled in "standard health plans" that cover the ten
Essential Health Benefits required of QHPs in the marketplace. BHP premiums and out-of-
pocket cost-sharing may not exceed what would have been charged by the benchmark plan
(second-lowest-cost silver plan) in the marketplace, considering premium tax credits (PTCs) and
cost-sharing reductions (CSRs) for which consumers would have qualified (Dorn, November 25,
et al., 2014).
State and local officials will be responsible for reaching out to and enrolling more than 30
million individuals in publicly funded or subsidized health plans offered through state insurance
exchanges. Failure to meet enrollment goals will not only undermine the credibility and success
of the Patient Protection and Affordable Care Act (ACA) but, more importantly, will do little to
expand health insurance coverage and improve access to care among those at greatest need
(Martin & Parker, 2011).
Opt-Out States
The U.S. Supreme Court's ruling on the Affordable Care Act in 2012 allowed states to opt-out of
the health reform law's Medicaid expansion. Since that ruling, fourteen governors have

7
announced that their states will not expand their Medicaid programs seen in figure 2. It is
estimated that 3.6 million fewer people would be insured, federal transfer payments to those
states could fall by $8.4 billion, and state spending on uncompensated care could increase by
$1 billion in 2016, compared to what would be expected if all states participated in the expansion
(Price & Eibner, 2013).
Figure 2
Status of State Action on the Medicaid Expansion Decision
In the states that have not expanded Medicaid, there is a coverage gap that leaves
about 2.5 million people ineligible for any sort of affordable coverage. And according to U.S.
Census data, the percentage of people below the poverty level who are uninsured is more than
twice as high in states that have not expanded Medicaid compared with states that have. Five
states — Texas, North Carolina, Florida, Georgia, and Tennessee — account for the lion's share
of the coverage gap population (healthinsurance.org, 2018). If Medicaid is expanded in North
Carolina, Gov. Roy Cooper's administration estimates that 624,000 residents would become
newly eligible for coverage. A significant number of them (estimates range
8
from 215,000 to nearly half a million) are currently in the coverage gap, with no realistic access
to health insurance at all unless Medicaid is expanded. The federal government paid the full cost
of expansion through 2016. In 2017, states began to pay 5 percent of the cost, and that will
increase to 10 percent by 2020. The states' portion will never exceed 10 percent, though. In
North Carolina, the state's cost to expand Medicaid is estimated at between $210 million and
$600 million per year (Norris, 2020).
Adopted ACA but Not Implement
Only one state decided to adopt the ACA but is hesitant to implement the expansion. On August
4, 2020, Missouri voters approved a ballot measure that added Medicaid expansion to the state's
Constitution and required the implementation of expansion coverage by July 1, 2021. However,
on May 13, 2021, Governor Mike Parson announced that the state's Department of Social
Services (DSS) was withdrawing its state plan amendment (SPA) submission and would not
implement expansion as scheduled due to a lack of funding: the ballot measure did not include a
revenue source and the state legislature excluded the program from its F.Y. 2022 budget.
Subsequently, on May 20, advocates filed a lawsuit against the DSS, arguing that the state's
refusal to expand Medicaid is unlawful per the initiated constitutional amendment and asking
that the court require expansion to go into effect on July 1, 2021. On June 23, a circuit court
judge ruled in favor of DSS, finding that the state's refusal to expand Medicaid is not unlawful
because the initiated amendment violated the state constitution by failing to provide a funding
source. However, on July 22, the Missouri Supreme Court overturned this decision, finding that
the initiated amendment did not violate the state constitution and instructing the lower court to
enter a judgment in favor of the plaintiffs. Pending this judgment, the timeline for Medicaid
9
expansion implementation remains unknown. Under the American Rescue Plan Act's incentive,
Missouri could receive an estimated $1.1 billion in additional federal funds over the next two
years for the traditional Medicaid program if the state implements the Medicaid expansion.
Language in the initiated constitutional amendment prohibited the imposition of any additional
burdens or restrictions on eligibility or enrollment for the expansion population.
(KFF, 2019).
Socioeconomic Consequences
Health insurance coverage helps increase access to health care services, including preventive and
primary care, and ultimately could contribute to population health improvement. The ACA
expansion was associated with a reduction in the uninsured rate while increasing the use of some
health services, such as outpatient visits and overnight hospital stays, as well as the use of
preventive services (e.g., screening visits and check-ups including cholesterol screening, Pap
smear tests, mammograms, and PSA tests) (Kino & Kawachi, 2018).
Access to health care among non-elderly Americans is strongly associated with
socioeconomic characteristics, including income, education, employment, and wealth. Compared
to Americans who are better off, those in lower socioeconomic strata are less likely to be insured
and more likely to avoid medical care due to cost, enter hospitals through emergency
departments and have twice as many avoidable hospitalizations. The poor use less health care in
spite of having greater medical needs. These health care access gaps are compounded by—and
may contribute to—the large and widening socioeconomic disparities in health and longevity in
the United States (Griffith et al., 2017).
The challenge in reaching medically underserved communities is that Medicaid
beneficiaries are more likely to live in medically underserved communities that frequently lack the
10
providers essential to building quality networks. Safety-net providers such as community health
centers and public and mission-driven hospital systems form the Medicaid managed care provider
network backbone, but they, too, experience staff shortages. One recent study reported that simply
by filling open positions, health centers could serve 2 million more patients.
Another challenge is those who have unstable eligibility and enrollment. Eligibility for
both Medicaid and the tax subsidies offered through the ACA's insurance marketplaces is closely
tied to family income. Even with the massive efforts now underway to streamline enrollment and
renewal, nothing can overcome the income fluctuations that can cause coverage shifts over time.
The risk of breaks in coverage remains, especially in states that have chosen not to expand Medicaid
eligibility. Therefore, the rule's emphasis on making it possible for health plans to participate in both
the Medicaid managed care market and the qualified health plan marketplace so that people can
remain enrolled in their plans represents a key opportunity for states (Rosenbaum, 2016).
Population Health
Population health is defined as the health outcomes of a group of individuals, including the
distribution of such outcomes within the group (Kindig & Stoddart, 2003). It is a relatively new
term with no agreement about whether it refers to a concept of health or a field of study of health
determinants. Discussions of population health involve many terms, such
as outcomes, disparities, determinants, and risk factors, which may be used imprecisely,
particularly across different disciplines, such as medicine, epidemiology, economics, and
sociology. Nonetheless, thinking and communicating clearly about population health concepts
are essential for public and private policymakers to improve the population's health and reduce
disparities (Chang et al., 2021).
11
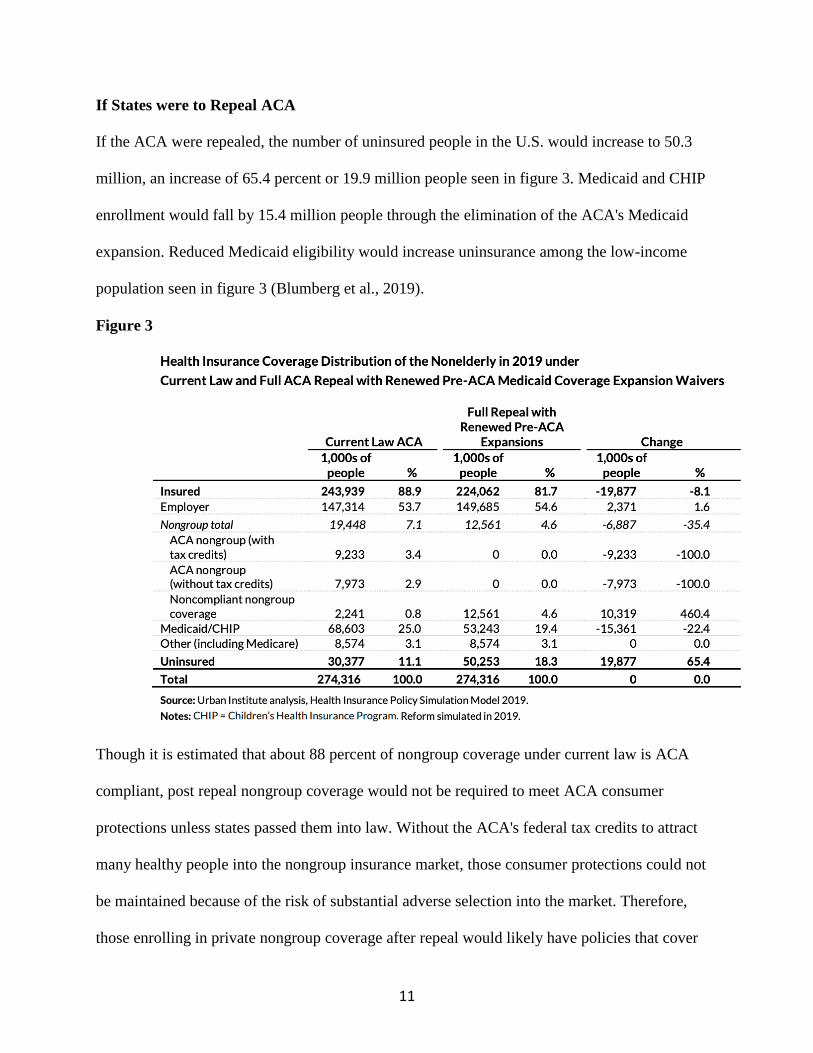
If States were to Repeal ACA
If the ACA were repealed, the number of uninsured people in the U.S. would increase to 50.3
million, an increase of 65.4 percent or 19.9 million people seen in figure 3. Medicaid and CHIP
enrollment would fall by 15.4 million people through the elimination of the ACA's Medicaid
expansion. Reduced Medicaid eligibility would increase uninsurance among the low-income
population seen in figure 3 (Blumberg et al., 2019).
Figure 3
Though it is estimated that about 88 percent of nongroup coverage under current law is ACA
compliant, post repeal nongroup coverage would not be required to meet ACA consumer
protections unless states passed them into law. Without the ACA's federal tax credits to attract
many healthy people into the nongroup insurance market, those consumer protections could not
be maintained because of the risk of substantial adverse selection into the market. Therefore,
those enrolling in private nongroup coverage after repeal would likely have policies that cover
12
significantly fewer benefits and require more out-of-pocket spending for services, five like
nongroup coverage before ACA implementation. These policies also would no longer be
required to cover preexisting conditions. Because of the elimination of guaranteed issues and
modified community ratings, many people with current or past health problems would be unable
to purchase the plans at any price, and others would be charged very high prices for insurance
policies, further decreasing coverage and increasing financial burdens (Blumberg et al., 2019).
The largest absolute increase in the number of uninsured people occurs in the largest states: 3.8
million more uninsured in California, 1.6 million more uninsured in Florida, and 1.7 million
more uninsured in Texas. The largest percentage increases in the uninsured would occur in the
states, with the largest increases in coverage under the ACA. For example, West Virginia and
Kentucky have large low-income populations and had high uninsurance rates before the ACA,
and both states expanded Medicaid eligibility in 2014 (Blumberg et al., 2019). Under a repeal,
the number of people uninsured in Kentucky would increase by 379,000, or 150.5 percent; in
West Virginia, the number of people uninsured would increase by 162,000, or 175.6 percent. The
uninsured in Montana, another ACA Medicaid expansion state, would increase by 176.8 percent,
or 112,000 people. States that did not expand Medicaid and/or did not have measures in place to
encourage high Marketplace enrollment would see much smaller changes in their number of
uninsured residents under repeal. For example, uninsurance in South Dakota would increase by
12,000 people, or 11.9 percent; uninsurance in Kansas would increase by 62,000 people, or 18.0
percent (Blumberg et al., 2019).

13
Figure 4
14
Cost of Healthcare in Non-Expansion States
Texas
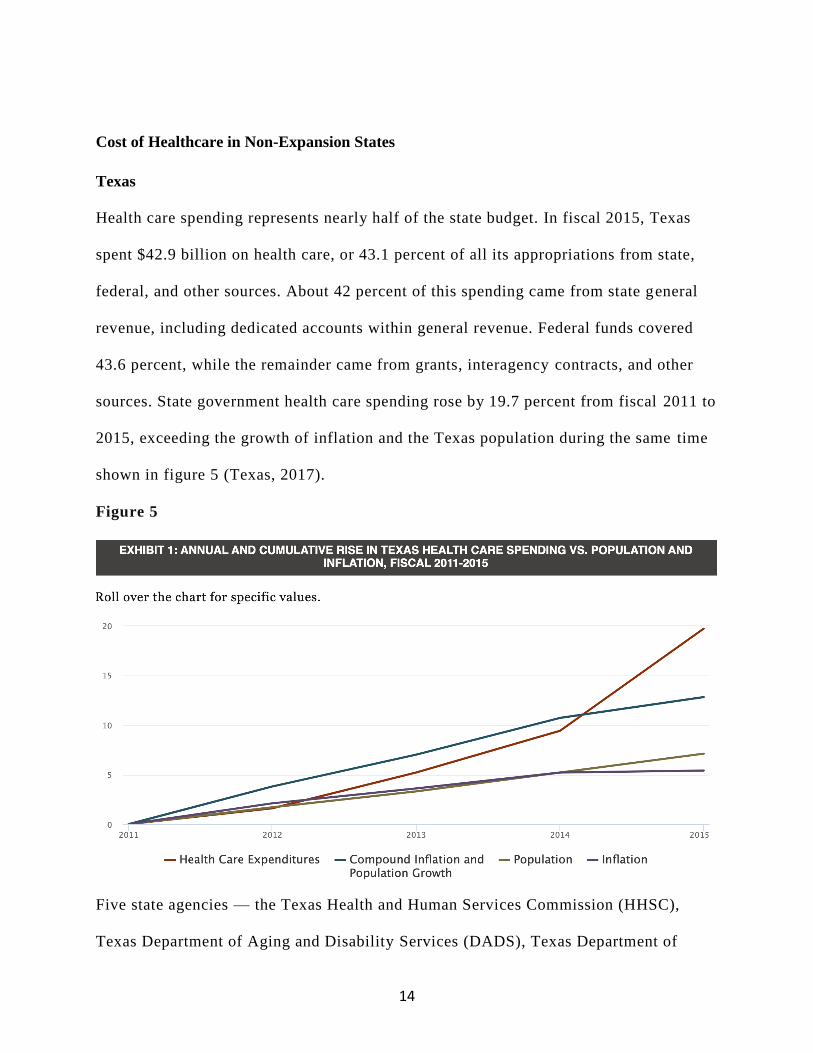
Health care spending represents nearly half of the state budget. In fiscal 2015, Texas
spent $42.9 billion on health care, or 43.1 percent of all its appropriations from state,
federal, and other sources. About 42 percent of this spending came from state general
revenue, including dedicated accounts within general revenue. Federal funds covered
43.6 percent, while the remainder came from grants, interagency contracts, and other
sources. State government health care spending rose by 19.7 percent from fiscal 2011 to
2015, exceeding the growth of inflation and the Texas population during the same time
shown in figure 5 (Texas, 2017).
Figure 5
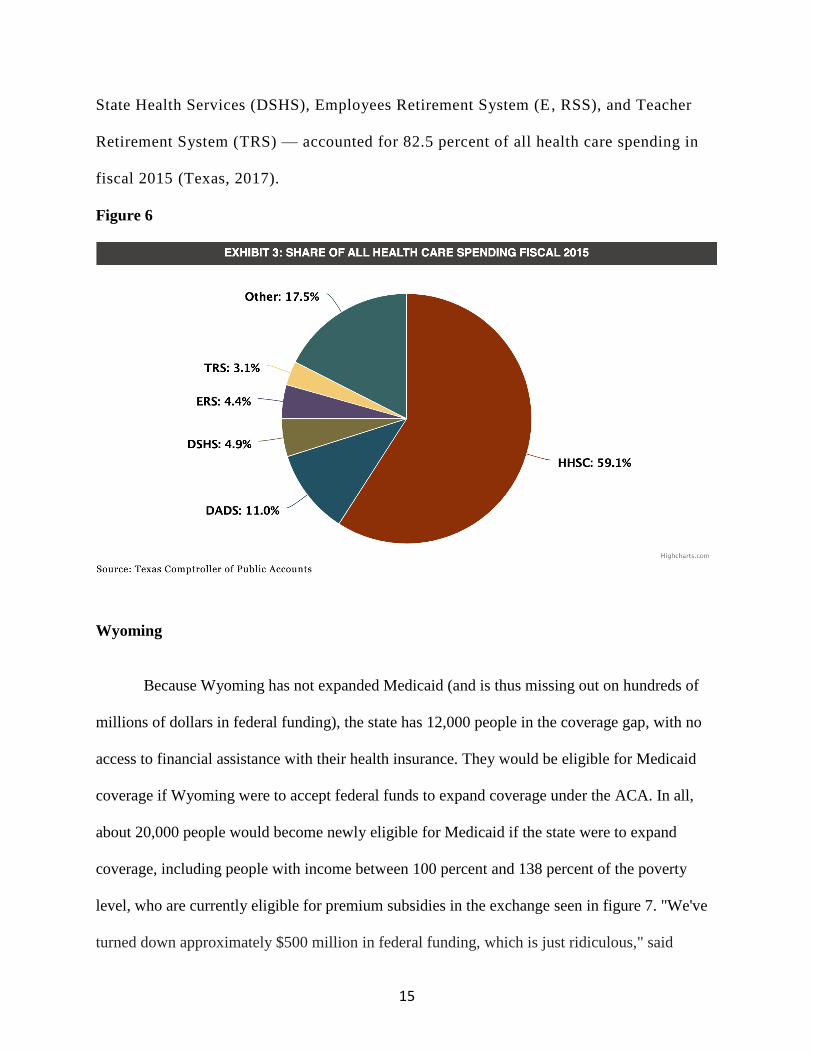
Five state agencies — the Texas Health and Human Services Commission (HHSC),
Texas Department of Aging and Disability Services (DADS), Texas Department of
15
State Health Services (DSHS), Employees Retirement System (E, RSS), and Teacher
Retirement System (TRS) — accounted for 82.5 percent of all health care spending in
fiscal 2015 (Texas, 2017).
Figure 6
Wyoming
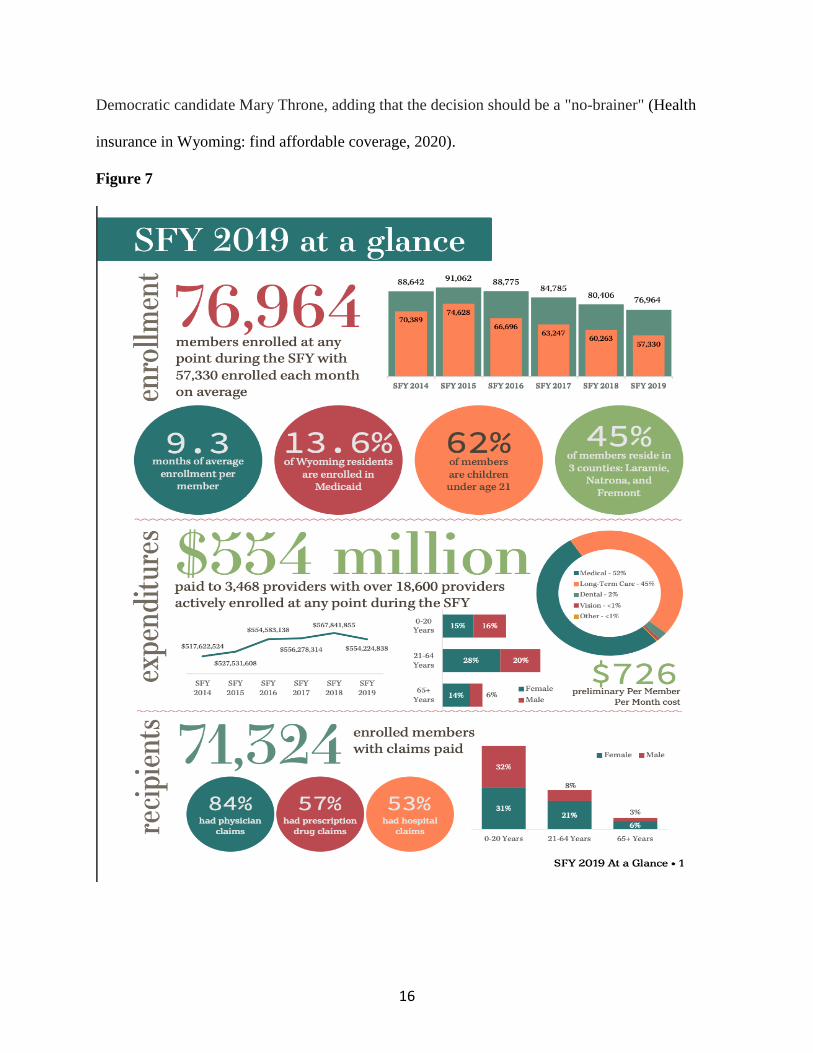
Because Wyoming has not expanded Medicaid (and is thus missing out on hundreds of
millions of dollars in federal funding), the state has 12,000 people in the coverage gap, with no
access to financial assistance with their health insurance. They would be eligible for Medicaid
coverage if Wyoming were to accept federal funds to expand coverage under the ACA. In all,
about 20,000 people would become newly eligible for Medicaid if the state were to expand
coverage, including people with income between 100 percent and 138 percent of the poverty
level, who are currently eligible for premium subsidies in the exchange seen in figure 7. "We've
turned down approximately $500 million in federal funding, which is just ridiculous," said
16
Democratic candidate Mary Throne, adding that the decision should be a "no-brainer" (Health
insurance in Wyoming: find affordable coverage, 2020).
Figure 7
17
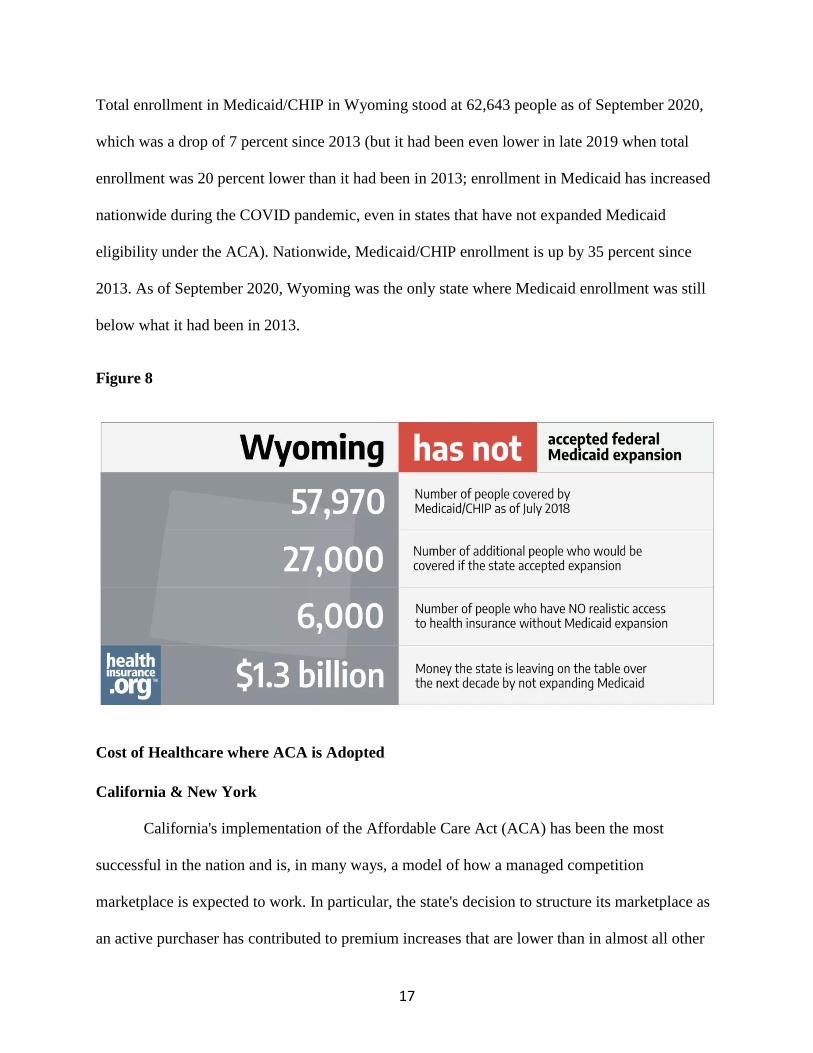
Total enrollment in Medicaid/CHIP in Wyoming stood at 62,643 people as of September 2020,
which was a drop of 7 percent since 2013 (but it had been even lower in late 2019 when total
enrollment was 20 percent lower than it had been in 2013; enrollment in Medicaid has increased
nationwide during the COVID pandemic, even in states that have not expanded Medicaid
eligibility under the ACA). Nationwide, Medicaid/CHIP enrollment is up by 35 percent since
2013. As of September 2020, Wyoming was the only state where Medicaid enrollment was still
below what it had been in 2013.
Figure 8
Cost of Healthcare where ACA is Adopted
California & New York
California's implementation of the Affordable Care Act (ACA) has been the most
successful in the nation and is, in many ways, a model of how a managed competition
marketplace is expected to work. In particular, the state's decision to structure its marketplace as
an active purchaser has contributed to premium increases that are lower than in almost all other

18
states. Relative concentrations of insurers and particularly of providers in the different rating
regions of the state are the fundamentals that matter most in the effort to bend the health
insurance cost curve (Weinberg & Kallerman, 2017).
The four largest states in the U.S.—California, Florida, New York, and Texas—fall into two
distinct categories. The first group is represented by California and New York, both of which are
operating their own health insurance marketplaces and have expanded eligibility for Medicaid to
adults who earn at or below 138 percent of the federal poverty level—about $16,000 for an
individual or $32,000 for a family of four.3 Florida and Texas, the second group, are using the
federal marketplace to enroll residents in health plans and have declined to expand Medicaid
eligibility. In this new analysis of data from the Commonwealth Fund Biennial Health Insurance
Survey, we find that there were larger shares of uninsured adults in Florida and Texas compared
with California and New York in 2014. In addition, adults in Florida and Texas were more likely to
report not getting needed care because of cost and having problems paying medical bills.
Figure 9

19
Young adults have experienced the largest gains in coverage nationally. According to the survey, by
2014, the national uninsured rate for 19-to-34-year-olds was 19 percent. This was down from 27
percent in 2010—the year adult children became eligible to remain on parents' health plans to age
26.8 There are differences among the four states. In New York, 14 percent of young adults were
uninsured in 2014, compared with 34 percent in Texas, 26 percent in Florida, and 23 percent in
California (Rasmussen et al., 2015).
There are also significant differences in coverage rates for adults with low incomes. Adults
with incomes below 100 percent of the federal poverty level—that is, $11,490 for an individual or
$23,550 for a family of four—are faring best in New York and California (figure 10). Thirteen
percent of low-income New Yorkers and 23 percent of low-income Californians are uninsured,
compared with 33 percent of low-income adults in Florida and 51 percent in Texas. Even before the
passage of the Affordable Care Act, both New York and California had established Medicaid
eligibility levels that were more generous than most states. And under the health reform law, both
states expanded eligibility for Medicaid up to 138 percent of poverty, while Florida and Texas did
not (Rasmussen et al., 2015).
Figure 10

20
Economic Effects of Medicaid Non-Expansion States on Hospitals
America's rural hospitals are in crisis. Small practices and pediatricians are in danger of
going out of business. University of North Carolina's Rural Health Research Program tracks that
they closed ten hospitals in 2020, and Texas, Nebraska, Wisconsin, and Pennsylvania's rural
areas have more low-income families who cannot afford the care they need. Policymakers need
to do better to bridge this gap before the change takes place for the better. The disparity will be
seen through the states, including rural areas. Low Medicaid reimbursement rates to hospitals
and healthcare providers do not make Medicaid expansion enticing for states. Patients do not
really benefit from the expansion due to the care. An agenda for reform shows that in-hospital
death rates for surgical patients show variation in outcomes based on coverage.
The death rates of Medicare, Medicaid, and uninsured patients were 97% higher than patients
with private insurance. The average hospital length of stay of privately insured patients was 7.38
days, Medicare stayed 19%, and Medicaid stayed 42% longer. Even though the length of stay
was longer, the outcomes were worse. Medicaid patients cost, on average, more than 26%.
(Antos et al., 2015) Low reimbursement causing poor outcomes is one of the reasons that
patients are skeptical about Medicaid. Expanding Medicaid will allow more plans in the
marketplace, giving more options and lower costs overall. Medicaid reimburses physicians only
61 cents on the dollar (Antos et al., 2015), which makes physicians opt-out of taking Medicaid
insurances, making specialists and primary care physicians unreachable for the patients who
need it. Patients on Medicaid do not have much choice other than to use the emergency room for
their needs; this goes back to putting the burden of free care on the hospitals. Hospitals such as
Northside hospital in Georgia are constantly trying to be innovative in Revenue cycle practice.
Non-for-profit hospitals offer financial assistance as charity to the community and their patients

21
who are covered for a certain period during which they qualify. They can get their tests,
including x-rays, C.T. scans, MRI, Ultrasound, and labs done at little or no cost. Any of the
outpatient testing, procedures, some surgeries, and all services that the hospital covers can be
covered under the charity status. Patients that make too much can go as self-pay and get a special
self-pay rate of 75% discount. Chartis Center for Rural Health deems 2019 the worst year for
rural hospital closures, with 19 hospitals closing and one out of four hospitals show early
warning signs of closure (Scott, 2020). Chartis studies hospitals in rural areas that are in danger
of closing to see if they are in non-expansion states. Medicaid expansion states decrease the
likelihood of closure by 62%. Texas, Tennessee, Oklahoma, Georgia, Alabama, and
Missouri refused to expand Medicaid and have a 75% hospital closure rate (Scott, 2020).
Hospitals such as Northside hospital in Georgia are constantly trying to be innovative in Revenue
cycle practice. The hospital is not-for-profit and offers financial assistance as a charity to the
community and its patients. This was the patient covered for a certain period of which they can
qualify, and they can get their tests, including X-rays, CT scans, MRI, ultrasound, and labs done
at little or no cost. Any of the outpatient testing, procedures, some surgeries, and all services that
the hospital covers can be covered under the charity status. Patients that make too much can go
as self-pay and get a special self-pay rate of 75% discount. This leaves a disparity in health
outcomes to disadvantage populations. Policymakers need to find a way to bridge this gap to see
results. Hospitals and hospital associates continue to rally for Medicaid expansion due to their
diminishing resources. Resources that have already been exhausted due to the
Emergency Medical Treatment and Labor Act of 1986 (EMTALA) (Allen, 2018). The
Congressional Budget Office (CBO) suggests that Medicaid would add very little or no costs to
the states compared to what the states would bear if there were no health reform at all (Angeles,

22
2012). Expanding Medicaid will ensure reimbursement for hospitals. CBO predicts that 17
million more people will be covered in expansion, reducing the state's costs for uncompensated
care and other programs alike. The federal government will pick up the bulk of the costs of
Medicaid expansion, which is favorable for states and for their residents in need of insurance
(Angeles, 2012). Federal law mandates in the ACA for nonprofit hospitals to increase
community benefits in exchange for their "lucrative" tax status. According to research, they are
still very stagnant in going so. Tax-exempt hospitals spent an average of 7.6% in 2010 of their
total spending on community benefits, while the total operating costs increased to 8.1% by 2014.
The bulk of this sending went toward non-reimbursed patient care such as charity. Boston
University professors test that Gary Young from Boston University says that this is not easy for
hospitals to do since their focus has been on treatment and not prevention (Connor, 2018).
Methodology

23
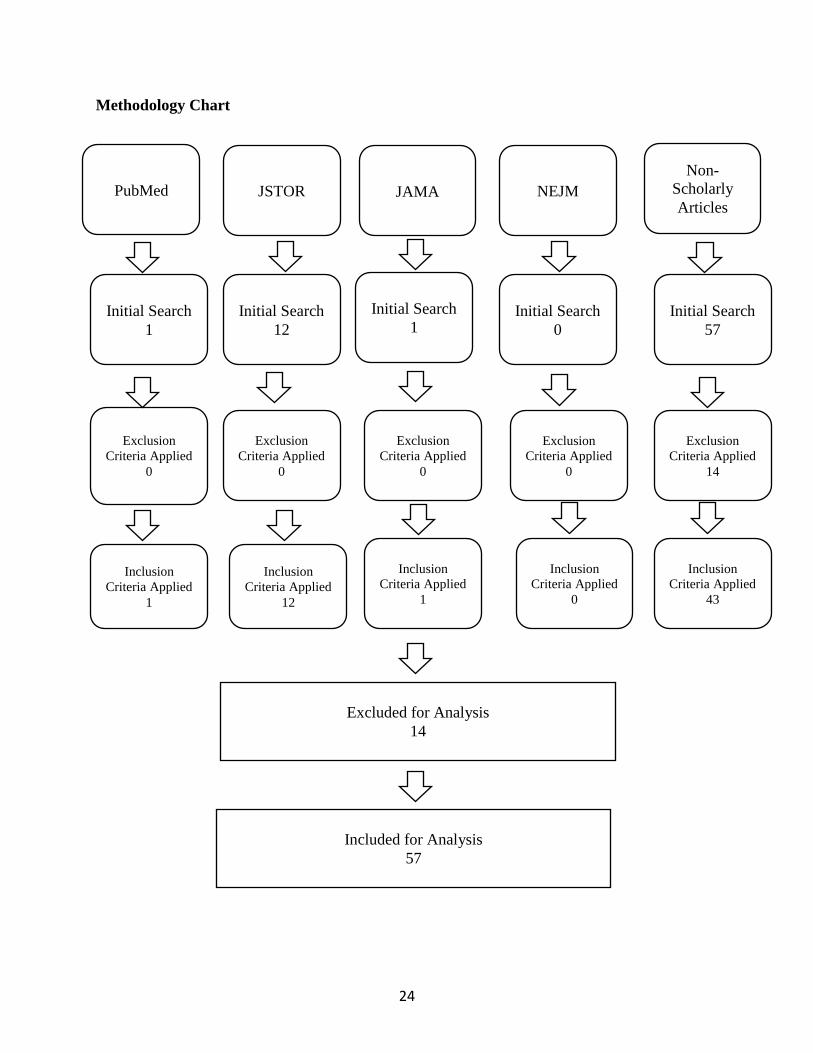
This study is a qualitative analysis of archival data from peer-reviewed journal articles.
From 1992 through July 2021, four academic databases, PubMed, JSTOR, JAMA, and NEJM,
were searched to identify relevant literature, and 43 news articles, interviews, and official
government websites were searched for more recent data. The inclusion criteria was based on the
search keyword terms were "Affordable Care ACT, mandate, healthcare cost," "Expansion AND
States. In addition, search filters were added to refine the results. Exclusions were any articles
that didn't dive into the results of Medicaid non-expansion. Articles that were focused on specific
illness and disease were also omitted due to the title of the thesis. Search filter criteria were
English language, academic journal publications, peer-reviewed, and published in 1990 for
classic articles and 2014 through 2021 for more relevant data. JAMA database was used only for
a health policy subject because PubMed did not offer that subject filter. 57 articles were included
for analysis and 14 were excluded for analysis.
Figure 11
24
Methodology Chart
PubMed JSTOR JAMA NEJM
Non-
Scholarly
Articles
Initial Search
1
Exclusion
Criteria Applied
0
Inclusion
Criteria Applied
1
Initial Search
0
Initial Search
12
Initial Search
57
Exclusion
Criteria Applied
0
Exclusion
Criteria Applied
0
Exclusion
Criteria Applied
0
Exclusion
Criteria Applied
14
Inclusion
Criteria Applied
12
Inclusion
Criteria Applied
43
Inclusion
Criteria Applied
0
Inclusion
Criteria Applied
1
Initial Search
1
Excluded for Analysis
14
Included for Analysis
57
25
Findings/Analysis
Medicaid has been a source of official insurance for low-income children, parents, elderly, and
disabled individuals to improve health outcomes. Medicaid expansion with the Affordable Care
Act (ACA) authorized states to extend Medicaid levels for all adults with income up to 138
percent of Federal Poverty Level (FPL). Medicaid is the largest health insurer in the country with
66 million approximately. (Manatt, Phelps & Phillips, LLP. 2019). Medicaid was associated with
improved medical outcomes, such as access to care, higher preventative care, and screenings,
decreased hospital and Emergency utilization and decreased infant mortality rates. People were
more confident within their health care practices since the cost was not the biggest issue (Manatt,
Phelps & Phillips, LLP, 2019). Medicaid expansion in the remaining states would insure over 14
million people who are uninsured. Due to the current economic crisis due to the COVID
pandemic, people with no insurance are afraid to seek medical attention. In economic crisis,
people who have lost their jobs can still get coverage if Medicaid were expanded. This will
allow them the peace of mind to seek medical attention with chronic diseases such as diabetes,
hypertension, and heart disease (Schubel, 2020).
Positive Health Outcomes
Medicaid expansion gives peace of mind and body to citizens. ACA has improved
access to care and utilization of services among the low-income population. Improved access to
care and utilization have led to an increase in early diagnosis, which leads to better outcomes of
chronic disease. States that expanded Medicaid have seen improvements in access to medications
and
services for behavioral and mental health conditions (Antonisse et al., 2018).
A study in Maryland showed that a year after expansion, there was a small but statistical
26
difference in more emergent cases in the emergency room rather than using it as a primary care
facility. Another study showed a decline in the length of stay for Medicaid patients. There are
many studies showing positive self-reported outcomes of individuals who have had lifesaving
treatments and care that could not have afforded care prior to expansion. An Ohio study post-
expansion showed a decrease in medical debt since enrolling in Medicaid. Antonisse et al.,
2018).
States' Economics and Politics
Since the 2016 elections, "repeal and replace" bills have been a point of
contention in Congress. Though they are aimed at changing Medicaid and its details, they have
still kept Medicaid expansion in place. The replace and Repel bill would not repeal the ACA's
expansion of the Medicaid program, it will reduce the cost to the federal government. It is to
allow states to maintain the higher initial federal funding till 2020 (Flood et al, 2017). It will be
impossible and a threat to any party or group of people that will rescind coverage for over 12
million newly covered Medicaid beneficiaries since then. This has been the reason for the failure
of all "repeal and replace" bills.
States' residents pay over $3 trillion dollars in federal income taxes. The federal
the government keeps the money for federally funded activities and sends back funding to
the state governments through Medicaid and other programs. This process is
called "financial migration". In 2018, it was projected that 55 percent of all federal
assistance to state and local governments derived through the federal match program for
Medicaid (Allen, 2018). The states that have chosen not to expand Medicaid have
been primarily Republican governors and lawmakers. Kaiser Family Foundation (KFF) reports
studies positive budget savings, revenue gains, and overall economic growth. During FY 2010-
27
2015, the federal government paid 100% of the costs related to transportation, education, or
other state programs related to Medicaid expansion (Guth et al., 2020).
The goal of the Trump administration was to repeal the ACA, and it set out to cut expansion of
low-income adults and impose "rigid" caps on the federal government's Medicaid spending.
Despite Trump's determination to repeal the ACA, Congress rejected many of his proposals in
2017 (Center on Budget and Policy Priorities. 2020).
Trump's administration proposed rules in 2019 that aimed to make it hard for the states to
pay for their share of Medicaid costs. These rules can significantly change the costs and
coverages of Medicaid in the states. In 2019, a proposal to lower the poverty line would
cause millions of people to lose their coverage and receive less help from federal aid programs.
(Center on Budget and Policy Priorities. 2020). In 2018, Trump gave states the authority to pay
premiums for health coverage in the marketplace, knowing very well that higher premiums will
lower Medicaid participation. States were given full authority to take away coverage from low
income people who could not afford to pay their premiums (Center on Budget and Policy
Priorities. 2020). This causes more fear within the low-income population, causing them to flee
from any coverage and again turn to the emergency room for service.
American Rescue Plan Act
American Rescue Plan Act (ARP) is part of the COVID-19 relief package that became law
March 11, 2021. The ARP contains many provisions which increase coverage, expand benefits,
and adjust federal financing of Medicaid programs to states (Musumeci, 2021). In addition to the
already 90% federal funding, they can now get another 5% increase for two years. The new
incentive is available for the 12 states that have not expanded Medicaid, as well as Oklahoma
and Missouri, which are expected to expand Medicaid by July 21, 2021. An additional 10%
28
increase can be matched if the states incorporate more senior and people with disability
resources, which allow them to live and function in the community (Musumeci, 2021). The ARF
coverage provisions are:
1. Mandatory coverage of Covid-19 vaccines.
2. Option to extend post-partum coverage to 12 months.
3. Community cased mobile crisis intervention service.
4. Extension of 100% federal financing to Urban Indian and Native Hawaiian health
Systems.
5. Medicaid during the Covid-19 emergency period.
6. Covid-19 relief funds for rural provides. (Musumeci, 2021).
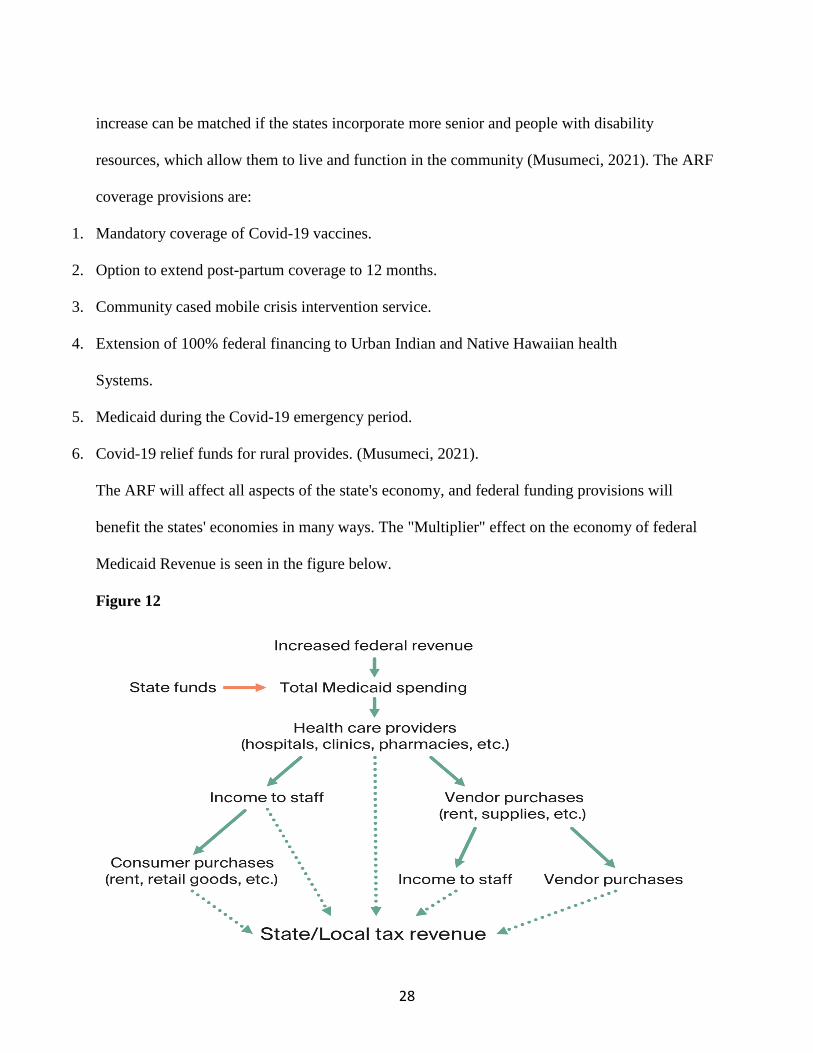
The ARF will affect all aspects of the state's economy, and federal funding provisions will
benefit the states' economies in many ways. The "Multiplier" effect on the economy of federal
Medicaid Revenue is seen in the figure below.
Figure 12
29
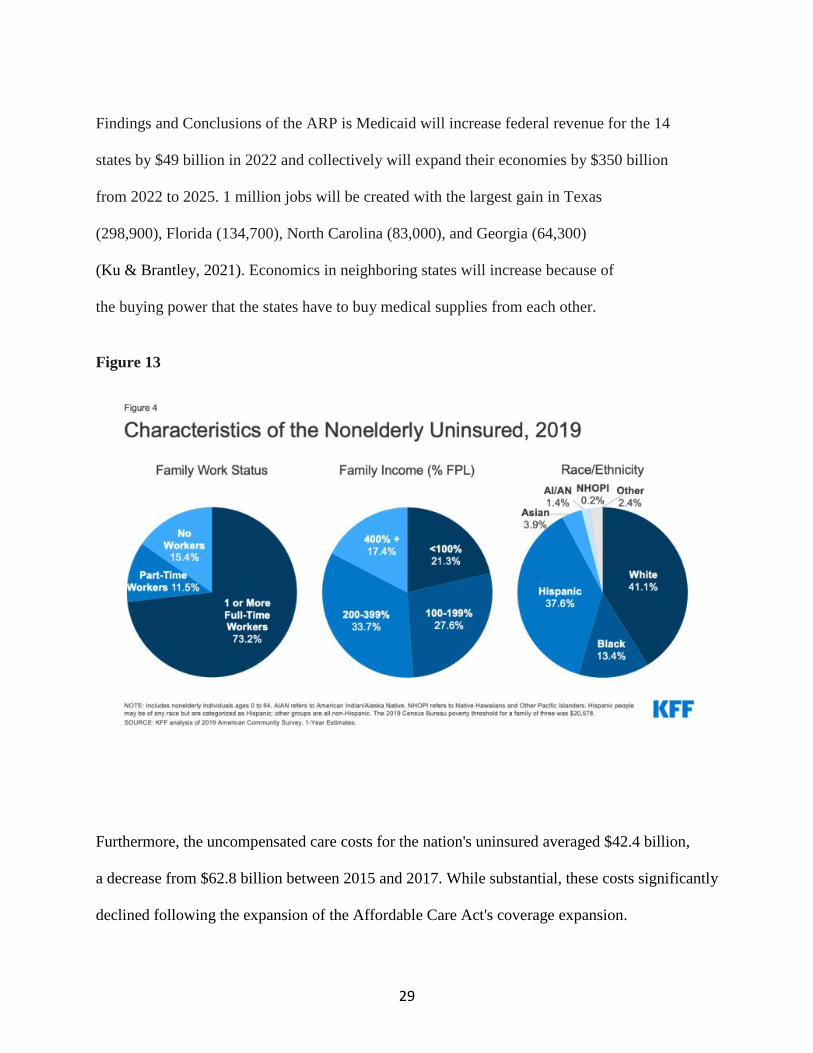
Findings and Conclusions of the ARP is Medicaid will increase federal revenue for the 14
states by $49 billion in 2022 and collectively will expand their economies by $350 billion
from 2022 to 2025. 1 million jobs will be created with the largest gain in Texas
(298,900), Florida (134,700), North Carolina (83,000), and Georgia (64,300)
(Ku & Brantley, 2021). Economics in neighboring states will increase because of
the buying power that the states have to buy medical supplies from each other.
Figure 13
Furthermore, the uncompensated care costs for the nation's uninsured averaged $42.4 billion,
a decrease from $62.8 billion between 2015 and 2017. While substantial, these costs significantly
declined following the expansion of the Affordable Care Act's coverage expansion.
30
However, with the rise in the number of uninsured since 2017, provider uncompensated care
costs associated with caring for the uninsured have likely increased. Between 2017 and 2019, the
number of uninsured grew by an estimated 1.5 million (Coughlin et al., 2021).
\
31
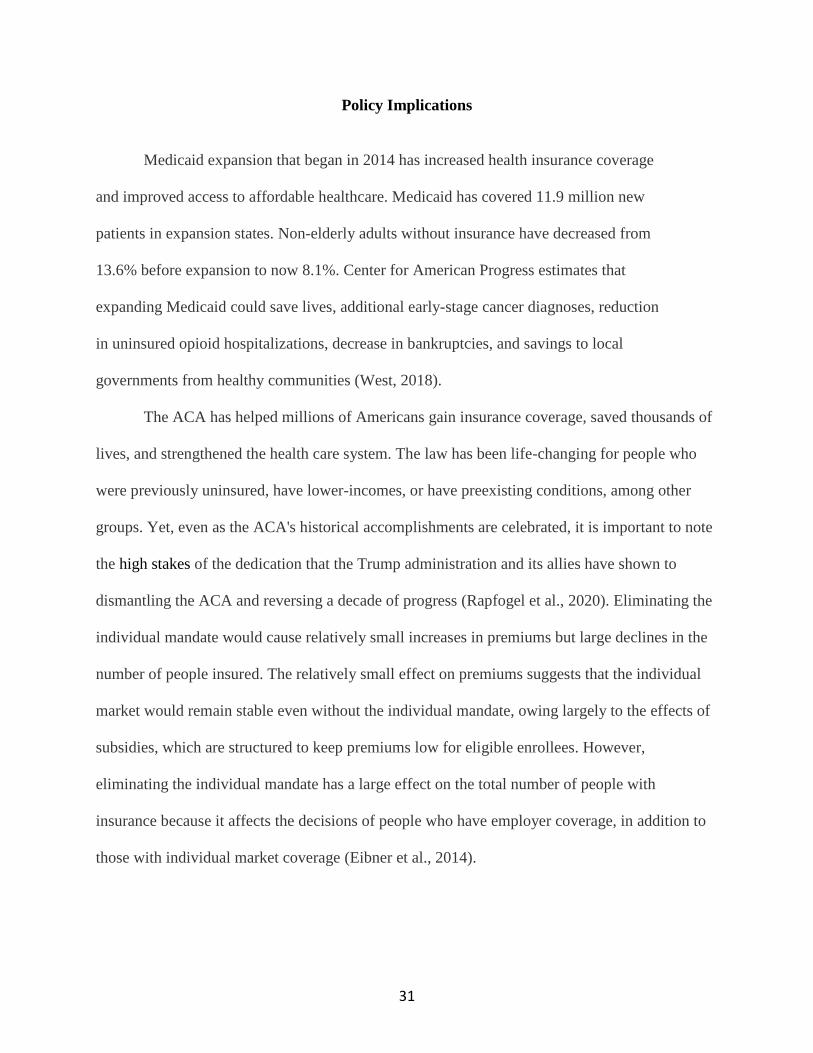
Policy Implications
Medicaid expansion that began in 2014 has increased health insurance coverage
and improved access to affordable healthcare. Medicaid has covered 11.9 million new
patients in expansion states. Non-elderly adults without insurance have decreased from
13.6% before expansion to now 8.1%. Center for American Progress estimates that
expanding Medicaid could save lives, additional early-stage cancer diagnoses, reduction
in uninsured opioid hospitalizations, decrease in bankruptcies, and savings to local
governments from healthy communities (West, 2018).
The ACA has helped millions of Americans gain insurance coverage, saved thousands of
lives, and strengthened the health care system. The law has been life-changing for people who
were previously uninsured, have lower-incomes, or have preexisting conditions, among other
groups. Yet, even as the ACA's historical accomplishments are celebrated, it is important to note
the high stakes of the dedication that the Trump administration and its allies have shown to
dismantling the ACA and reversing a decade of progress (Rapfogel et al., 2020). Eliminating the
individual mandate would cause relatively small increases in premiums but large declines in the
number of people insured. The relatively small effect on premiums suggests that the individual
market would remain stable even without the individual mandate, owing largely to the effects of
subsidies, which are structured to keep premiums low for eligible enrollees. However,
eliminating the individual mandate has a large effect on the total number of people with
insurance because it affects the decisions of people who have employer coverage, in addition to
those with individual market coverage (Eibner et al., 2014).

32
Figure 14
Congress must keep lowering Medicaid funding for states that refuse to adopt and implement the
ACA. Congressional Democrats and President Joe Biden have vowed to find a path to convince
the last 12 states — Alabama, Florida, Georgia, Kansas, Mississippi, Missouri, North Carolina,
South Carolina, South Dakota, Tennessee, Texas, and Wyoming — to expand eligibility or
directly extend affordable insurance options to their residents. Biden's COVID-19 relief package,
the American Rescue Plan, offered more federal money to states that opted into the expansion
(Luthra, 2021).

33
Conclusion
States that refuse to expand Medicaid wreak havoc on the insurance markets (Rapfogel, Calsyn,
et al., 2020). Without coverage, people cannot get both the preventive and curative care they
need. Rising uninsured rates during the COVID-19 pandemic would be particularly dire, as the
uninsured may not only risk their own lives by avoiding treatment but also unwittingly spread
the coronavirus without adequate and affordable care. The ACA is a lifeline for employees of
small businesses and the self-employed. Prior to the ACA, most uninsured workers were self-
employed or working at small businesses and had few affordable, comprehensive coverage
options. Since the ACA was enacted, the uninsured rate for small-business employees has
dropped by nearly 10 percentage points (Rapfogel, Calsyn, et al., 2020).
Insurance companies must now spend at least 80 percent of insurance premiums
on medical care and improvements. The ACA also aims to prevent insurers from making
unreasonable rate increases. Insurance coverage is not free by any means, but people now
have a wider range of coverage options. Preexisting conditions, such as cancer, made it
difficult for many people to get health insurance before the ACA. Most insurance
companies would not cover treatment for these conditions. They said this was because the
illness or injury occurred before you were covered by their plans (Roland, 2015).
Under the ACA, you cannot be denied coverage because of a preexisting health
problem. The ACA covers many screenings and preventive services. These usually have
low copays or deductibles. The hope is that if you are proactive in your healthcare, you
can avoid or delay major health problems later. Healthier consumers will lead to lower
costs over time. For example, a diabetes screening and early treatment may help prevent
costly and debilitating treatment later.
34
"The ACA is going to help all Americans have higher quality and less costly healthcare in the
decades to come," says Dr. Christopher Lillis, an internist in Virginia and a member of Doctors
for America (Roland, 2015).
ACA has many aspects that will enhance the health outcomes of Americans and improve
U.S. healthcare. States must adopt this expansion and allow the marketplace to work itself
through allowing for better prices of medical supplies, medical coverage, and prescriptions. The
states will continue to flourish as they are able to be funded for several other programs as a stem
of the expansion. The states will not be responsible for the bulk of the costs as originally thought
by the lawmakers and stakeholders alike.
35
References
Allen, K. (2018, December 20). Medicaid Expansion Considerations For Non-Expansion States.
Health Management Associates. https://www.healthmanagement.com/blog/35exas35to-
expansion-considerations-non-expansion-states/
Ammula, M. (2021, May 6). Building on the Evidence Base: Studies on the Effects of Medicaid
Expansion, February 2020 to March 2021. KFF.
https://www.kff.org/35exas35to/report/building-on-the-evidence-base-studies-on-the-
effects-of-medicaid-expansion-february-2020-to-march-2021/
Antos, J., Capretta, J. C., Chen, L. J., Gottlieb, S., Levin, Y., Miller, T. P., Ponnuru, R., Roy, A.,
Wilensky, G. R., & Wilson, D. (2015). Accept Terms and Conditions on JSTOR.
Www.jstor.org.
https://www.jstor.org/stable/pdf/resrep24612.7.pdf?ab_segments=0%2Fbasic_search_gsv
Barofsky, J. (2021, February 25). What are the effects of not expanding Medicaid? Brookings.
https://www.brookings.edu/blog/usc-brookings-schaeffer-on-health-
policy/2015/02/20/what-are-the-effects-of-not-expanding-medicaid/
Barrilleaux, C., & Rainey, C. (2014). The Politics of Need: Examining Governors’ Decisions to
Oppose the “Obamacare” Medicaid Expansion. State Politics & Policy Quarterly, 14(4),
437–460. https://www.jstor.org/stable/24710976
Béland, D., Rocco, P., & Waddan, A. (2016). Obamacare Wars: Federalism, State Politics, and
the Affordable Care Act. In JSTOR. University Press of Kansas.
http://www.jstor.org/stable/j.ctt1ckpbtp.11
Benefits | Medicaid.gov. (2013). Medicaid.gov.
https://www.medicaid.gov/chip/benefits/index.html
36
Blumberg, L. J., Buettgens, M., Holahan, J., & Pan, C. W. (2019, March 18). State-by-State
Estimates of the Coverage and Funding Consequences of Full Repeal of the ACA. Urban
Institute. https://www.urban.org/research/publication/state-state-estimates-coverage-and-
funding-consequences-full-repeal-aca
Bright Futures. (2019). Aap.org. https://brightfutures.aap.org/Pages/default.aspx
Buehler, J. W., Snyder, R. L., Freeman, S. L., Carson, S. R., & Ortega, A. N. (2018). It’s Not
Just Insurance: The Affordable Care Act and Population Health. Public Health Reports
(1974-), 133(1), 34–38.
https://www.jstor.org/stable/26374234?Search=yes&resultItemClick=true&search
Chang, J., Lai, A., Gupta, A., Nguyen, A., Berry, C., Shelley, D., Graffigna, G., Palamenghi, L.,
Savarese, M., Castellini, G., Barello, S., Walker, D., Yeager, V., Lawrence, J.,
Mcalearney, A., Eccleston-Turner, M., Upton, H., Ci, M., Schalkwyk, V., & Maani, N.
(2021). Identifying Opportunities to Strengthen the Public Health Informatics
Infrastructure: Exploring Hospitals’ Challenges with Data Exchange International
Collaboration to Ensure Equitable Access to Vaccines for COVID-19: The ACT-
Accelerator and the COVAX Facility. A Multidisciplinary Journal of Population Health
and Health Policy, 99(2).
Corallo, B., & 2020. (2020, November 5). Analysis of Recent National Trends in Medicaid and
CHIP Enrollment. KFF. https://www.kff.org/coronavirus-covid-19/issue-brief/analysis-
of-recent-national-trends-in-medicaid-and-chip-enrollment/
Coughlin, T. A., Samuel-Jakubos, H., & 2021. (2021, April 6). Sources of Payment for
Uncompensated Care for the Uninsured. KFF. https://www.kff.org/uninsured/issue-
brief/sources-of-payment-for-uncompensated-care-for-the-uninsured/
37
Courtemanche, C., Marton, J., Ukert, B., Yelowitz, A., Zapata, D., & Miron, J. (2018). Accept
Terms and Conditions on JSTOR. Www.jstor.org.
https://www.jstor.org/stable/pdf/resrep26220.pdf?ab_segments=0%2Fbasic_searc
Custer, W. (2013). The Economic Impact of Medicaid Expansion in Georgia.
https://www.issuelab.org/resources/14733/14733.pdf
Dinan, J. (2014). Implementing Health Reform: Intergovernmental Bargaining and the
Affordable Care Act. Publius, 44(3), 399–425. https://www.jstor.org/stable/24734665
Dorn, S., Mcgrath, M., & Holahan, J. (2014a). Urban Institute | Social and Economic Policy
Research. Urban Institute. https://www.urban.org
Dorn, S., Mcgrath, M., & Holahan, J. (2014b). What Is the Result of States Not Expanding
Medicaid? Timely Analysis of Immediate Health Policy Issues.
https://www.urban.org/sites/default/files/publication/22816/413192-What-is-the-Result-
of-States-Not-Expanding-Medicaid-.PDF
Dorn, S., November 25, J. T. P., & 2014. (2014, November 25). The ACA’s Basic Health
Program Option: Federal Requirements and State Trade-Offs. KFF.
https://www.kff.org/health-reform/report/the-acas-basic-health-program-option-federal-
requirements-and-state-trade-offs/
Dranove, D., Garthwaite, C., & Ody, C. (2016). Uncompensated Care Decreased At Hospitals In
Medicaid Expansion States But Not At Hospitals In Nonexpansion States. Health Affairs,
35(8), 1471–1479. https://doi.org/10.1377/hlthaff.2015.1344
Eibner, C., Eibner, C., Saltzman, E., & Saltzman, E. (2014). How Does the ACA Individual
Mandate Affect Enrollment and Premiums in the Individual Insurance Market? Rand.org;
RAND Corporation. https://www.rand.org/pubs/research_briefs/RB9812z4.html

38
Flood, J., & Records, J (2017). Analysis of the House of Republican Repeal and replace Bills for
the Affordable Care Act.
https://www.crowell.com/NewsEvents/AlertsNewsletters/all/Analysis-of-the-House-
Republican-Repeal-and-Replace-Bills-for-the-Affordable-Care-Act
Fishman, E., & Weissfeld, J. (2019, October 15). Medicaid Policy And Partisan Politics: A New
Dynamic. https://www.healthaffairs.org/do/10.1377/hblog20191015.597909/full/
Griffith, K., Evans, L., & Bor, J. (2017). The Affordable Care Act Reduced Socioeconomic
Disparities In Health Care Access. Health Affairs, 36(8), 1503–1510.
https://doi.org/10.1377/hlthaff.2017.0083
Health insurance in Wyoming: find affordable coverage. (2020). Healthinsurance.org.
https://www.healthinsurance.org/states/38exas38t/
healthinsurance.org. (2018, November 19). Medicaid expansion definition. Healthinsurance.org;
healthinsurance.org. https://www.healthinsurance.org/glossary/38exas38to-expansion/
Hsieh, H.-M., & Bazzoli, G. J. (2012). Medicaid Disproportionate Share Hospital Payment: How
Does It Impact Hospitals’ Provision of Uncompensated Care? Inquiry, 49(3), 254–267.
http://www.jstor.org/stable/23480516
Institute of MedicineU.S.S.) Committee on the Consequences of Uninsurance. (2003). Hidden
Costs, Values Lost: Uninsurance in America. In PubMed. National Academies
PressU.S.S.). https://www.ncbi.nlm.nih.gov/books/NBK221662/
January 21, A. D. P., & 2021. (2021, January 21). The Coverage Gap: Uninsured Poor Adults in
States that Do Not Expand Medicaid. KFF. https://www.kff.org/38exas38to/issue-
brief/the-coverage-gap-
39
Kagan, J., & Catalano, T. J. (2019). Medicaid. Investopedia.
https://www.investopedia.com/terms/m/39exas39to.asp
KFF. (2019, August 2). Status of State Medicaid Expansion Decisions: Interactive Map. The
Henry J. Kaiser Family Foundation. https://www.kff.org/39exas39to/issue-brief/status-of-
state-medicaid-expansion-decisions-interactive-map/
KHN, M. B. (2018, January 9). The Consequences Of Not Expanding Medicaid: A Significant
Increase In Hospital Closures. Kaiser Health News. https://khn.org/morning-
breakout/the-consequences-of-not-expanding-medicaid-a-significant-increase-in-hospital-
closures/
Kindig, D., & Stoddart, G. (2003). What Is Population Health? American Journal of Public
Health, 93(3), 380–383. https://doi.org/10.2105/ajph.93.3.380
Kino, S., & Kawachi, I. (2018). The impact of ACA Medicaid expansion on socioeconomic
inequality in health care services utilization. PLOS ONE, 13(12), e0209935.
https://doi.org/10.1371/journal.pone.0209935
Kodjak, A. (2015, October 15). States That Declined To Expand Medicaid Face Higher Costs.
NPR.org. https://www.npr.org/sections/health-shots/2015/10/15/448729327/states-that-
Ku, L., & Brantley, E. (2021, May 20). Economic and Employment Effects of Medicaid
Expansion Under ARP | Commonwealth Fund. Www.commonwealthfund.org.
https://www.commonwealthfund.org/publications/issue-briefs/2021/may/economic-
employment-effects-medicaid-expansion-under-arp
Lanford, D., & Quadagno, J. (2016). Implementing ObamaCare: The Politics of Medicaid
Expansion under the Affordable Care Act of 2010. Sociological Perspectives, 59(3), 619–
639. http://www.jstor.org/stable/26339045
40
Luthi, S. (2017). Reports Show Medicaid Expansion Increasing Coverage & Affordability.
Inside CMS, 20(16), 13–14.
https://www.jstor.org/stable/26707663?ab_segments=0%2Fbasic_se%20%20%20%20%
20%20arch_gsv2
Luthra, S. (2021, July 9). When states don’t expand Medicaid, women suffer. The 19th.
https://19thnews.org/2021/07/when-states-don’t-expand-medicaid-women-suffer/
Manatt, Phelps & Phillips, LLP. (2019, February). Medicaid’s Impact on Health Care Access,
Outcomes and State Economies. RWJF.
https://www.rwjf.org/en/library/research/2019/02/40exas40to-s-impact-on-health-care-
access-outcomes-and-state-economies.html
Markus, A. R., Gianattasio, K., Luo, E. (Qian), & Strasser, J. (2019). Predicting the Impact of
Transforming the Medicaid Program on Health Centers’ Revenues and Capacity to Serve
Medically Underserved Communities. The Milbank Quarterly, 97(4), 1015–1061.
https://doi.org/10.1111/1468-0009.12426
Martin, L. T., & Parker, R. M. (2011). Insurance Expansion and Health Literacy. JAMA, 306(8).
https://doi.org/10.1001/jama.2011.1212
Norris, L. (2020, September 14). North Carolina and the ACA’s Medicaid expansion.
Healthinsurance.org. https://www.healthinsurance.org/40exas40to/north-carolina/#2019
Policy Basics: Introduction to Medicaid. (2020, April 14). Center on Budget and Policy
Priorities. https://www.cbpp.org/research/health/introduction-to-medicaid
Price, C. C., & Eibner, C. (2013). For States That Opt Out Of Medicaid Expansion: 3.6 Million
Fewer Insured And $8.4 Billion Less In Federal Payments. Health Affairs, 32(6), 1030–
1036. https://doi.org/10.1377/hlthaff.2012.1019

41
Program History | Medicaid.gov. (2015). Medicaid.gov. https://www.medicaid.gov/about-
us/program-history/index.html
Raftery, E. (2016). Obama Offers To Extend Full Medicaid Funding To Nonexpansion States.
Inside CMS, 19(3), 7–7.
https://www.jstor.org/stable/26705555?ab_segments=0%2Fbasic_search_%20gsv2
Rapfogel, N., Calsyn, M., & Seeberger, C. (2020, October 1). The Chaos of Repealing the
Affordable Care Act During the Coronavirus Pandemic. Center for American Progress.
https://www.americanprogress.org/issues/healthcare/news/2020/10/01/490916/chaos-
repealing-affordable-care-act-coronavirus-pandemic/
Rapfogel, N., Gee, E., & Calsyn, M. (2020, March 23). 10 Ways the ACA Has Improved Health
Care in the Past Decade. Center for American Progress.
https://www.americanprogress.org/issues/healthcare/news/2020/03/23/482012/10-ways-
aca-improved-health-care-past-decade/
Rasmussen, P. W., Collins, S. R., Beutel, S., & Doty, M. M. (2015, March 15). Health Care
Coverage and Access in the Nation’s Four Largest States | Commonwealth Fund.
Www.commonwealthfund.org. https://www.commonwealthfund.org/publications/issue-
briefs/2015/apr/health-care-coverage-and-access-nations-four-largest-states
RevCycleIntelligence. (2016, April 8). Does Medicaid Expansion Improve Revenue of
Hospitals? RevCycleIntelligence. https://revcycleintelligence.com/news/does-medicaid-
expansion-improve-revenue-of-hospitals
Roland, J. (2015, June 15). The Pros and Cons of Obamacare. Healthline; Healthline Media.
https://www.healthline.com/health/consumer-healthcare-guide/pros-and-cons-
obamacare#cons

42
Rosenbaum, S. (2016, May 6). The Medicaid Managed Care Rule: The Major Challenges States
Face | Commonwealth Fund. Www.commonwealthfund.org.
https://www.commonwealthfund.org/blog/2016/42exas42to-managed-care-rule-major-
challenges-states-face
Scott, D. (2020, February 18). 1 in 4 rural hospitals is vulnerable to closure, a new report finds.
Vox. https://www.vox.com/policy-and-politics/2020/2/18/21142650/rural-hospitals-
closing-medicaid-expansion-states
Searing, A. (2020, May 12). Expanding Medicaid Would Help Keep Rural Hospitals Open in 14
Non-Expansion States. Center for Children and Families.
https://ccf.georgetown.edu/2020/05/12/expanding-medicaid-would-help-keep-rural-
hospitals-open-in-14-non-expansion-states/
Sunkara, V., & Rosenbaum, S. (2016). The Constitution and the Public’s Health: The
Consequences of thU.S.S. Supreme Court’s Medicaid Decision in NFIB v Sebelius.
Public Health Reports (1974-), 131(6), 844–846. https://www.jstor.org/stable/26374030
Texas. (2017). Counting the Cost of Texas Health Care. Texas.gov.
https://comptroller.texas.gov/economy/fiscal-notes/2017/march/health-care.php
Tolbert, J., Singer, N., Dec 13, A. D. P., & 2019. (2019, December 13). Key Facts about the
Uninsured Population. KFF. https://www.kff.org/uninsured/issue-brief/key-facts-about-
the-uninsured-
Turner, G, Roy, A (2013). Why States Should not Expand Medicaid. https://galen.org/2013/why-
states-should-not-expand-medicaid/
U.S. Centers for Medicare & Medicaid Services. (2018). Affordable Care Act (ACA).
HealthCare.Gov. https://www.healthcare.gov/glossary/affordable-care-act/
43
Ward, B. (2020, May 5). The Impact of Medicaid Expansion on States’ Budgets | Commonwealth
Fund. Www.commonwealthfund.org.
https://www.commonwealthfund.org/publications/issue-briefs/2020/may/impact-
medicaid-expansion-states-budgets
Weinberg, M., & Kallerman, P. (2017). ACA Exchange Competitiveness In California. Risk
Management and Insurance Review, 20(2), 173–188. https://doi.org/10.1111/rmir.12078
Weirich, M., & Benson, W. (2019). Rural America: Secure in a Local Safety Net? Generations:
Journal of the American Society on Aging, 43(2), 40–45.
https://www.jstor.org/stable/26760113?ab_segments=0%2Fbasic_search_
44
Appendix: List of Figures
Corallo, B., & 2020. (2020, November 5). Analysis of Recent National Trends in Medicaid and
CHIP Enrollment. KFF. https://www.kff.org/coronavirus-covid-19/issue-brief/analysis-
of-recent-national-trends-in-medicaid-and-chip-enrollment/
Policy Basics: Introduction to Medicaid. (2020, April 14). Center on Budget and Policy
Priorities. https://www.cbpp.org/research/health/introduction-to-medicaid
Blumberg, L. J., Buettgens, M., Holahan, J., & Pan, C. W. (2019, March 18). State-by-State
Estimates of the Coverage and Funding Consequences of Full Repeal of the ACA. Urban
Institute. https://www.urban.org/research/publication/state-state-estimates-coverage-and-
funding-consequences-full-repeal-aca
Texas. (2017). Counting the Cost of Texas Health Care. Texas.gov.
https://comptroller.texas.gov/economy/fiscal-notes/2017/march/health-care.php
Health insurance in Wyoming: find affordable coverage. (2020). Healthinsurance.org.
https://www.healthinsurance.org/states/wyoming/
Rasmussen, P. W., Collins, S. R., Beutel, S., & Doty, M. M. (2015, March 15). Health Care
Coverage and Access in the Nation's Four Largest States | Commonwealth Fund.
Www.commonwealthfund.org. https://www.commonwealthfund.org/publications/issue-
briefs/2015/apr/health-care-coverage-and-access-nations-four-largest-states

45
Ku, L., & Brantley, E. (2021, May 20). Economic and Employment Effects of Medicaid
Expansion Under ARP | Commonwealth Fund. Www.commonwealthfund.org.
https://www.commonwealthfund.org/publications/issue-briefs/2021/may/economic-
employment-effects-medicaid-expansion-under-arp
Antos, J., Capretta, J. C., Chen, L. J., Gottlieb, S., Levin, Y., Miller, T. P., Ponnuru, R.,
Roy, A., Wilensky, G. R., & Wilson, D. (2015). Accept Terms and Conditions on JSTOR.
Eibner, C., Eibner, C., Saltzman, E., & Saltzman, E. (2014). How Does the ACA Individual
Mandate Affect Enrollment and Premiums in the Individual Insurance Market? Rand.org;
RAND Corporation. https://www.rand.org/pubs/research_briefs/RB9812z4.html





























