Embed Size (px)
DESCRIPTION
Calcium phosphate cements as bone drug delivery systems A review.pdf
Citation preview

Journal of Controlled Release 113 (2006) 102–110www.elsevier.com/locate/jconrel
Review
Calcium phosphate cements as bone drug delivery systems: A review
M.P. Ginebra ⁎, T. Traykova, J.A. Planell
Biomedical Engineering Research Centre (CREB), Division of Biomaterials, Biomechanics and Tissue Engineering,Department of Materials Science and Metallurgical Engineering, Technical University of Catalonia (UPC), Av. Diagonal 647, 08028 Barcelona, Spain
Received 22 November 2005; accepted 6 April 2006Available online 5 June 2006
Abstract
Since calcium phosphate cements were proposed, several formulations have been developed, some of them commercialised, and they haveproven to be very efficient bone substitutes in different applications. Some of their properties, such as the injectability, or the low-temperaturesetting, which allows the incorporation of different drugs, make them very attractive candidates as drug carriers. In this article, the performance ofcalcium phosphate cements as carriers of different types of drugs, such as antibiotics, analgesics, anticancer, anti-inflammatory, as well as growthfactors is reviewed.© 2006 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1032. Why calcium phosphate cements? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1033. Calcium phosphate cements as drug carriers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1044. Drug-release kinetics from calcium phosphate cements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1045. Calcium phosphate cements as carriers for antibiotics. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
5.1. Effect of antibiotic incorporation on the physico-chemical properties of CPC . . . . . . . . . . . . . . . . . . . . . . . . . 1055.2. Antibiotic release kinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1055.3. In vivo performance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
6. Calcium phosphate cements as carriers for other drugs: anti-inflammatory, analgesic and anticancer . . . . . . . . . . . . . . . . . 1067. Calcium phosphate cements as carriers for growth factors and other proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1078. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
Abbreviations: ACP, amorphous calcium phosphate; BMP, bone morphogenetic protein; CPC, calcium phosphate cement; DCP, dicalcium phosphate, CaHPO4;DCPD, brushite, dicalcium phosphate dihydrate CaHPO4·2H2O; HA, hydroxyapatite, Ca10(PO4)6(OH)2; MCPM, monocalcium phosphate monohydrate Ca(H2PO4)2·H2O; MRSA, Staphylococcus aureus resistant to Meticilin-Cefem; PLGA, poly(lactic-co-glycolic acid); PMMA, poly(methyl methacrylate); rhTGF-β1,human recombinant-transforming growth factor-β1; rhBMP-2, human recombinant-bone morphogenetic protein-2; SBF, simulated body fluid; α-TCP, alpha-tricalcium phosphate, α-Ca3(PO4)2; β-TCP, beta-tricaclium phosphate, β-Ca3(PO4)2; TTCP, tetracalcium phosphate, Ca4(PO4)2O; TGF, transforming growth factor;TGFβ-SF, superfamily of transforming growth factor-beta.⁎ Corresponding author. Tel.: +34 93 4011089; fax: +34 93 4016706.E-mail address: [email protected] (M.P. Ginebra).
0168-3659/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.jconrel.2006.04.007

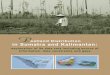
Fig. 1. Microstructure of an apatitic calcium phosphate cement after setting,showing the micro/nanoporous structure formed by the entanglement of theprecipitated crystals.
103M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
1. Introduction
The increased life expectancy in the developed countries hasled to a serious rise in the number of musculoskeletal disorders,such as osteoporosis and osteoarthritis. However, also thenumber of medications to treat and even prevent these diseaseshas expanded in recent years [1]. The development of new drugsand active substances, allows treating some of these diseaseseven in their initial stages.
A key issue in these treatments is to maximize the drugaccess to specific bone sites, and to be able to control therelease of drugs, in order to maintain a desired drugconcentration level for long periods of time without reachinga toxic level or dropping below the minimum effective level[2]. For this reason, a major effort has been done focused onthe development of materials that are capable of releasingdrugs by a reproducible and predictable kinetics. Althoughmost of these drug carriers are polymers, in the specific field ofthe pharmacological treatment of skeletal disorders, someinorganic materials can also play a role. Indeed, calciumphosphate based materials, which are bioactive, could have anadded value as drug carriers for the bone tissue. Moreover,another relevant property of calcium phosphates is their uniqueability to adsorb different chemical species on their surfaces.This property has been exploited for instance in thehydroxyapatite (HA) chromatography, which has proved tobe very efficient for the purification and separation of proteins,enzymes, nucleic acids and other macromolecules [3].Especially relevant is the application of HA chromatographyto the purification of bone growth factors [4]. Indeed, the greataffinity of HA for these various active molecules can beexploited within the field of the development of new matrixesfor drug delivery applications.
In this article we provide an insight in the application of onefamily of calcium phosphate based materials, namely calciumphosphate cements, as materials for controlled drug delivery.
2. Why calcium phosphate cements?
The possibility to obtain monolithic hydroxyapatite atambient or body temperature via a cementitious reaction wasput forward by LeGeros [5] and Brown and Chow [6] in theearly eighties. This was a significant step forward in the field ofbioceramics for bone regeneration, since it provided a materialwhich, in addition to being bioactive, was mouldable and hadthe capacity of self-setting in vivo, within the bone cavity [7,8].In addition, the development of injectable calcium phosphatecement formulations established good prospects for minimallyinvasive surgical techniques developed in recent years, lessaggressive than the classical surgical methods.
Since then, calcium phosphate cements have attracted muchattention and different formulations have been put forward[6,9–13]. In general, all CPC are formed by a combination ofone or more calcium orthophosphates, which upon mixing witha liquid phase, usually water or an aqueous solution, form apaste which is able to set and harden after being implantedwithin the body.
Currently many commercial products exist on the market [8].Most of them form hydroxyapatite upon setting, with lowcrystallinity and high specific surface, which can incorporatedifferent ions in its lattice depending on the composition of thestarting materials. In general it can be stated that the formationof hydroxyapatite through a cement reaction is a biomimeticprocess, in the sense that it takes place at body temperature andin a physiological environment. Indeed, the hydroxyapatiteformed in the setting of CPC is much more similar to biologicalapatites than ceramic hydroxyapatite. Other cement formula-tions give other reaction products upon setting, such as brushite.
As mentioned, cement setting is a result of dissolution andprecipitation process. The interlocking between precipitatedcrystals is responsible for cement hardening. Fig. 1 shows themicrostructure of an apatitic cement after setting. As it can beseen, CPCdevelop a highlymicro/nanoporous structure. Porositycan vary between 30% and 50%, depending on the processingconditions, e.g. liquid-to-powder ratio. The setting, rheologicaland mechanical properties of the CPC can be adjusted bymodifying different factors, such as the chemical composition ofreactants, particle size or presence of nucleating agents [14–17].CPC are therefore very versatile materials, which can be adaptedto the different clinical requirements of various applications.
Different studies with CPCs have shown that they are highlybiocompatible and osteoconductive materials, which canstimulate tissue regeneration [18–24]. Most of the apatiticcements are resorbed via cell-mediated processes. In theseprocesses, osteoclastic cells degrade the materials layer by layer,starting at the bone–cement interphase throughout its inner part.
Some of the advantages brought out by the development ofCPC in comparison with the use of calcium phosphates in theform of ceramic granules or bulk materials can be summarizedas follows:
(a) In first place, the self-setting ability in vivo.(b) Their injectability, which allows cement implantation by
means of minimally invasive surgical techniques, lessaggressive than the traditional surgical techniques.

104 M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
(c) The perfect fit to the implant site, which assures goodbone–material contact, even in geometrically complexdefects. This allows for an optimum tissue–biomaterialcontact, necessary for stimulating the bone ingrowth,
(d) The fact that the setting reaction which takes place underin vivo conditions is a dissolution–precipitation process,resulting in most cases in a precipitated hydroxyapatitewith a high and interconnected microporosity, chemicallyand structurally similar to biological apatites. Thesefactors contribute to an increased reactivity of CPC ascompared to calcium phosphate ceramics.
(e) Lastly, as mentioned above, the low-temperature settingallows incorporation of different drugs: from antibioticsand anti-inflammatory drugs to growth factors which areable to stimulate certain biological responses. This aspectgives a great potential to this type of materials for thecontrolled drug delivery in target sites of the skeletalsystem.
3. Calcium phosphate cements as drug carriers
In general, a potential substrate to be used as drug carriermust have the ability to incorporate a drug, to retain it in aspecific target site, and to deliver it progressively with time inthe surrounding tissues. Additional advantages are provided ifthe material is injectable and biodegradable.
The possibility to use CPCs not only as bone substitutes butalso as carriers for local and controlled supply of drugs is veryattractive and can be useful in treatments of different skeletaldiseases, such as bone tumours, osteoporosis or osteomyelitis,which normally require long and painful therapies.
Unlike calcium phosphate ceramics employed as drugdelivery systems, where the drugs are usually absorbed on thesurface, in CPCs the drugs can be incorporated throughout thewhole material volume, by adding them into one of the twocement phases. This fact can facilitate the release of drugs formore prolonged times.
The studies about incorporation of drugs into CPC coverdifferent aspects. In the first place, it is necessary to verify thatthe addition of the drug (either to the liquid or the solid phasesof the cement) does not interfere in the setting reaction,modifying the physico-chemical properties, not only in terms ofthe setting and hardening mechanisms but also with respect tothe rheological behaviour. Secondly, it is necessary tocharacterize the kinetics of drug release in vitro. Subsequently,the effectiveness of the cement to act as carrier for drug deliveryin vivo, must be assessed. And finally, the clinical performanceof the drug delivery system must be evaluated.
During the last decade, several studies related to theapplication of both commercial and experimental CPCs asdrug carriers have been published. Major attention has beenpaid to antibiotics, due to their wide areas of application: eitheras prophylactics to prevent infections produced during surgicalinterventions, or in general in the treatment of bone infections.However, also anti-inflammatory of anticancer drugs or evenhormones has been studied. In addition, in the last years theincorporation in CPCs of some other substances or factors able
to stimulate bone regeneration, such as bone morphogeneticproteins (BMP) or transforming growth factors β (TGF-β), hasbeen considered.
4. Drug-release kinetics from calcium phosphate cements
The release of drugs from any drug delivery device dependson different factors such as the microstructure, the drugsolubility, the type of bond between the drug and the matrixwhich holds it, and the mechanism of degradation (if any) of thematrix. [25,26]. Generally speaking, CPC could be ascribed tothe category of diffusion-controlled devices, where the drug isincorporated into a non-biodegradable matrix, through which itshould diffuse. Indeed, although some CPC are resorbable, inmost of the CPC studied as drug-carriers, the rate of matrixdegradation (e.g. the cement itself) is much lower than the rateof drug liberation. For that reason it is possible to assume thatthe drug release is mainly controlled by the process of diffusionthrough the cement matrix and not by the degradation of thesame.
In CPC the drugs can be introduced either in the liquid phaseor in the powder phase. During cement setting, dissolution ofcalcium phosphates from the powder phase takes place, which isfollowed by precipitation of a new phase. The new phase is inmost cases precipitated hydroxyapatite, and it can be assumedthat the drug is dispersed in the matrix formed by the set cement.In this situation, normally the drug-release kinetics followsHiguchi's law [27], at least at the initial stages (until around60% drug is released):
Mt ¼ AM0½DCsð2C0−CsÞt�1=2 ð1Þwhere Mt is the amount of drug released for time t; M0 is thetotal amount of drug; A is the surface area of the device; D is thediffusion coefficient of the drug in the matrix; Cs is thesolubility of the drug in the matrix; C0 is the initialconcentration of the drug in the matrix.
If we consider that, in the case of CPC, the matrixcontaining the dispersed drug is very porous since it is formedby a mesh of interlocking of crystals which create an openmicro or even nanoporosity, the diffusion coefficient D of thematrix should be replaced by an effective diffusion coefficientDeff:
Deff ¼ D Ves
ð2Þ
where Deff is the effective diffusion coefficient; D′ is thediffusion coefficient of the crystals which form cement as such;ε is the cement porosity; τ is the tortuosity of the cement.
By substituting (2) in (1) we obtain:
Mt ¼ AM0D Ves
Csð2C0−eCsÞt� �1=2
ð3Þ
Therefore, it is clear that porosity and other microstructuralparameters of the cement (e.g. tortuosity), play an important rolein the kinetics of drug release. This dependence has been shownby Otsuka in several works [28–32] and confirmed by other

105M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
authors [33–35], in studies covering different CPC formulationsand different drugs.
It has to be pointed out, however, that in the cases when thedrug is poorly soluble, the release would not follow the law ofHiguchi, since it would be controlled by the dissolution of thedrug, the release being proportional to the time.
In most cases it can be considered that CPC do not degradewhile drug is released, or, in other words, that the porosity of thematrix is maintained constant during drug delivery. However,some authors have shown certain degree of degradation of CPCduring drug liberation. For example, Otsuka [36] showed anincrease of porosity in a carbonated hydroxyapatite cementduring the release of indomethacin, which was ascribed to thecement degradation. In this case, the higher resorption rate ofthe cement was explained by the fact that the addition ofdifferent amounts of NaHCO3 to a TTCP/DCPD cementresulted in a carbonated apatite more soluble than thestoichiometric HA used in previous studies. Resorption ofcarbonated HA with time produced an increase of porosity,which increased the drug release rate. In summary, if porositydoes not remain constant, drug release kinetics does not followHiguchi's law, and the drug diffusion through the CPC matrix isnot any longer the only mechanism which controls drugliberation. In any case, it should not be omitted that duringrelease of drugs, the speed of resorption of the CPC matrixdepends on various factors, such as chemical composition,microstructure and crystallinity of the cement. In the case ofbrushite cements, the degradation rate is much higher than thatof apatite cements, and therefore is more important to considerthese phenomena.
As it was mentioned previously, Higuchi's law is valid forthe initial stage of drug release, being the mass of liberated drugproportional to
ffiffit
p. According to another model by Tung [37],
during the second stage, the release of drug is proportional tothe time, followed by a third stage at which the liberation isstabilized as the concentration of the antibiotic in theenvironment increases. In this model, the existence of thesecond stage would depend on the type of antibiotic and itssolubility. Although not described by the author, the releasekinetics of the second stage could be explained by a lowsolubility of the drug and hence a dissolution-controlled release,proportional to the time.
5. Calcium phosphate cements as carriers for antibiotics
In the field of application of CPCs for drug delivery, theantibiotics have been widely studied, due to their frequent use inthe treatment of infections of the skeletal system, or as aprophylactic strategy. One of the key factors for the success ofsurgical interventions aimed at the implantation of a prosthesisor of an osteoconductive material is the prevention frombacterial infections. Wound contamination, or postoperativeinfections following fracture repair, implantation of jointprosthesis or spine surgery, can cause serious problems. Forthis reason antibiotics are often provided as prophylactics, eitherorally or intravenously. However, the very little accessibility ofthe site of infection very often prolongs the treatment of bone
infections. A traditional method applied to control boneinfections is the implantation of poly-methylmethacrylatespheres (PMMA) loaded with gentamicin sulphate in theinfection site [38]. However, PMMA spheres are nonresorbableand must be removed after some months and replaced with newspheres or other substitute material, able to facilitate boneregeneration. Antibiotics can be also incorporated in calciumphosphate ceramic blocks, although their resorption rates areslow. Moreover, it is difficult to shape ceramics with complexform in order to be fitted into any type and size of bone defect.An alternative material that was proposed some decades agowas calcium sulphate hemihydrate (Ca2SO4·1/2H2O) which canbe used in form of cement, giving as reaction product calciumsulphate dihydrate (Ca2SO4·2H2O) [39]. The main drawbacksof this material come from its low mechanical strength and veryhigh resorption rate. In this context, the combination ofantibiotics with CPC can have enhanced properties whichovercome some of the previously mentioned drawbacks.
5.1. Effect of antibiotic incorporation on the physico-chemicalproperties of CPC
The setting reaction of the CPC can be affected or modifiedby introducing a drug either to the powder phase or to its liquidphase and, as a consequence, the physico-chemical andmechanical properties can change [33,34,40–42]. In general,in apatitic cements antibiotics tend to increase their setting timesand reduce the mechanical strength [40–42]. Takechi et al.studied the effect of incorporating flomoxef sodium in differentconcentrations (up to 10%) to the solid phase of a cementformed by TTCP and DCPA [40]. Since this antibiotic is verysoluble, it was assumed that it dissolved fast in the cement liquidphase. The authors noticed a strong reduction of mechanicalstrength when the amount of antibiotic added increased. Thisdecrease of mechanical strength was attributed to increasedporosity and to some inhibition of the setting reaction, assuggested by the presence of certain amount of reactants whenthe antibiotic quantity increased. The drug release followed thekinetics typical for these types of materials (as described in theprevious section), and after 72 h the total amount of liberatedantibiotic was between 55% and 60%.
In other cases, the modification of the CPC properties can bedue to some chemical interactions between the antibiotic and thecement. Indeed, the addition of tetracycline to an apatiticcement caused a strong reduction in mechanical propertieswhich was attributed to the ability of this antibiotic to chelateCa-atoms [41]. This was supported by the fact that whenantibiotic was introduced already complexed with calcium, theinteractions antibiotic–cement were limited. This allowed theaddition of bigger amounts of antibiotic without influencingsetting times and mechanical properties of the cement.
5.2. Antibiotic release kinetics
Hamanishi et al. [43] examined the incorporation ofvancomycin to a CPC formed by TTCP and DCPD for treatingosteomyelitis caused by MRSA. In in vitro studies they

106 M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
observed an effective release of vancomycin within 2 weeks, inthe case of CPCs containing 1% vancomycin, and within9 weeks for CPCs containing a higher content (5% vancomy-cin). In both cases, the released concentrations were higher thanthe effective concentration against different types of MRSA.The rate of drug release depended on the crystallinity of thecements, but for the two periods studied up to 95% of theantibiotic was liberated in both cases.
The antibiotic release kinetics of brushite cements, moreresorbable than apatitic cements, was analysed by addinggentamicine sulphate both in powder form and as a solution[33]. The reactants used for the cement were MCPM and β-TCP. Once again the rheological and mechanical properties ofthe cement changed by antibiotic addition, but in the oppositedirection of that reported by Takechi et al. They observed anincrease of the setting time, which was initially too short, as wellas an increase of mechanical strength, that was ascribed to thepresence of sulphate ions in the antibiotic. In the first few hours,drug release was very rapid following Higuchi's law. It wasproportional to
ffiffit
puntil 50% of antibiotic was released, and
drug release tended to stabilise beyond this value. The totalamount of antibiotic was released within 7 days, and nosignificant differences were observed depending on the way ofincorporation, as a powder or in solution.
An interesting aspect worth mentioning is the difference inthe rate of antibiotic release from CPC and from PMMA beads.In a comparative study, the release kinetics of three antibiotics,i.e. gentamicine, amikacine and ceftiofur incorporated either ina commercial TTCP/DCP cement or in PMMA spheres, wasanalysed [44]. The results after 30 days showed faster antibioticliberation from CPC than from the polymer. In both carriers, theconcentrations of liberated gentamicine and amikacine werehigher than the critical doses for preventing bacterial effects. Onthe other hand, the liberation of ceftiofur from both materialsremained within the right levels only during 7 days, beingtherefore inadequate when the bactericide effect has to beprolonged in time.
In the cases where antibiotic release is considered to beexcessively fast, a possible strategy is to incorporate somepolymers in the CPC, in order to retard drug liberation. In thissense some studies have been carried out aiming at theformation of a gel into the cement pores, which served asmatrix for the antibiotic. Takechi et al. added sodium alginate orchitosan [40,45]. Chitosan is found to stimulate bone formation,osteoconductivity, endochondral ossification and membranousosteoinduction. Thus, by combining sodium alginate andchitosan with the cement, a slight decrease of antibiotic releaseat the initial stage was observed, and liberation was maintainedto slightly higher levels to those obtained in commercial CPC.Bohner et al. [34] applied a similar strategy by addingpolyacrylic acid (PAA) to brushite cement, and likewisegentamicine delivery was prolonged in time, especially whenPAA had a high molecular weight. It was hypothesized that atthe initial stage the release kinetic would be controlled viadiffusion through pores (proportional to
ffiffit
p), and subsequently,
at the second stage, it would be controlled by the dissociation ofgentamicine sulphate from the complex formed with PAA
following a first order kinetics. Depending on the amount ofadded PAA, the quantity of released gentamicine variedbetween 58% and 100%. A constant delivery during 8 dayswas achieved by using high molecular PAA, which practicallymeant release of 100% antibiotic.
5.3. In vivo performance
In vivo release of vancomycin was studied by Hamanishi etal. [43]. CPC were loaded with 1%, 2% and 5% of vancomycinand implanted in tibial condyles of rabbits. After 3 weeks theconcentration of vancomycin in bone marrow was 20 timeshigher than the minimum value clinically required, in thecement with 5% vancomycin. Nevertheless, higher antibioticconcentrations seemed to delay bone ingrowth on the implantand thin fibrous capsules were formed.
In another in vivo study, Stallmann et al. [46] examinedand compared the effect of adding gentamicine and theantibicrobian peptide hLF1-11 (a fragment of human lacto-ferrin) to a commercial CPC based in TTCP and DCP. Thesematerials were thereafter implanted in the femoral channel ofrabbits, vaccinated with Staphylococcus aureus. The develop-ment of osteomyelitis was reduced for both drugs, but thisreduction was more effective in the case of the gentamicine-loaded CPC.
6. Calcium phosphate cements as carriers for other drugs:anti-inflammatory, analgesic and anticancer
Besides their application as antibiotic carriers, CPC can beappropriate matrixes for the incorporation of other drugs withpotential application in the musculoskeletal system.
As already mentioned, it is important to consider allpossible effects of drug addition on the setting reaction of theCPC. Ginebra et al. studied the effect of the incorporation ofan amino salicylic acid derived methacrylamide in an apatiticα-TCP-based cement [47]. Salicylic acid is an analgesic andanti-inflammatory, and moreover has a calcium complexationability. Strong effects were observed both in the rheologicaland mechanical properties. The injectability was improved,but simultaneously a decrease in the reaction rate of thecement was observed. The mechanical strength increased, by25% in compression and by 80% in flexion, which wasattributed to decreased porosity and smaller precipitatedcrystals.
Otsuka et al. [32] carried out an in vitro study about therelease kinetics of aspirin from a TTCP/DCP/HA cement. Therate of drug liberation was found to increase with higherporosity of cement, which can be easily controlled by liquid-to-powder ratio. Thus, the authors confirmed that kinetics of drugrelease followed a modified Fick's law, which was controlled bydrug diffusion through pores.
Indomethacin is an anti-inflammatory, non-steroidal drugwith wide application in different pathologies of muscle–skeletal system, such as chronical joint rheumatism. Otsuka etal. published different studies regarding the incorporation ofindomethacin in an apatite cement based in TTCP, DCPD and

107M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
HA [29,30,36,48]. Different concentrations of indomethacinwere combined with CPC and analyzed in vitro in simulatedbody fluid (SBF) as well as in phosphate buffer solution (PBS).In both cases the kinetics followed Higuchi's law, and theamount of drug released increased with the amount of drugincorporated in the cement. The release of indomethacin wasmuch slower in SBF than in PBS. This was attributed to theformation of an HA layer on the surface upon immersing inSBF, since the cement is a bioactive material [49]. This HAlayer reduced cement porosity and intervened the drug diffusionto the surrounding fluid. There was a particular case whereindomethacin release from CPCs did not follow Higuchi's law,i.e. when sodium bicarbonate was added to the cement, due tothe increase of the CPC resorption rate [36].
In vivo studies [30,48] were made where the cement wasimplanted subcutaneously in rats and the concentration ofindomethacin in the plasma was measured. Initially indo-methacin release was very fast. After 1 day it started todecrease and in total it prolonged for 3 weeks. The higherthe initial amount of drug in the cement, the higher theamount of liberated indomethacin. A relevant result was thatthe half-life of indomethacin in plasma was much higherwhen drug was introduced via cement implantation, ratherthan when it was injected subcutaneously. The liberation ofthe drug was prolonged over one month when it was addedin the cement. By comparing the concentrations of releaseddrug in vivo and in vitro, a linear relation at the initial stagewas observed, but liberation in vivo was much slower thanliberation in vitro during the last stage of the study. Thiscould be due to some surface changes in the cement causedby the formation of an apatite layer due to the bioactivecharacter of the CPC, or by other changes due to proteinadsorption or cell activity.
Mercaptopurine is a drug used in the therapy of sometumours, due to its ability to inhibit the proliferation of tumoralcells. Otsuka et al. studied its incorporation to a CPC based inTTCP and DCPD [28,31]. The setting reaction was not affected.In vitro release of mercaptopurine showed a similar behaviourto that observed for indomethacin. A clear dependence betweenrelease rate and cement porosity was also observed, which canbe easily controlled by modifying the liquid-to-powder ratio ofthe cement paste [31].
Estradiol is a feminine sexual hormone with estrogenicactivity, which can be used in the treatment of symptoms causedby the deficit of estrogens during menopause, such as mineralresorption and bone loss. Otsuka et al. studied the rate of releaseof estradiol in vitro, incorporated in CPC and immersed in SBF,and in vivo, by subcutaneous implantation in rats [50,51]. Therate of estradiol liberation in vitro was inversely proportional tocalcium concentration in solution. Consistently, in vivo releaseof estradiol was faster in rats which had lower concentrations ofvitamin D and Ca, compared to healthy rats, suggesting theautoregulatory mechanism of estradiol liberation. The bonemass of the recovery model rats was greater after the experimentthan before, suggesting that the severity of osteoporosis in theseanimals could be reduced by the implantation of this estradiol-loaded apatite cement.
7. Calcium phosphate cements as carriers for growthfactors and other proteins
Growth factors are a large group of polypeptides, able totransmit signals which affect cellular activity [52]. Amongthem, the superfamily of β-transforming growth factors (TGFβ-SF) is especially relevant for bone regeneration. It includesthe transforming growth factors β1, β2, β3 (TGF-β1, β2 and β3),and the bone morphogenetic proteins (BMP) among otherproteins. It is known that they play a role as activating agents forthe complex cascades of biological phenomena responsible forbone formation, and therefore they can accelerate boneingrowth. A special feature of the subfamily of BMPs is that,on the contrary to the other growth factors of the TGF-βSF,BMPs are osteoinductive. This means that BPMs can activatethe differentiation of pluripotential cells to bone forming cells,thus leading to bone formation even outside bone tissue.
In the last years the recombination techniques have madepossible the industrial production of human growth factors inbig quantities and high purity. However, it is necessary to haveavailable materials which allow for the controlled administra-tion of these factors at adequate therapeutic levels, and theirvectoring towards local tissue targets and cells. In fact, it isknown that injection of this type of substances alone cannotinduce tissue formation and regeneration, since protein diffusesvery fast from the implantation site. For that reason it isnecessary to select new materials which can act as substrates orcarriers for these biologically active factors. CPC possess agreat potential, because they set at room temperature, arebiocompatible and osteoconductive. Indeed, the idea ofincorporating growth factors into CPCs arose with the aim ofimproving or increasing the osteoconductive capacity ofcements.
TGF-β are multipotential regulators of bone cells metabo-lism and are capable of favouring bone formation in vivo,depending on their concentration and way of application, asshown in many studies. It has been shown also that TGF-β1
stimulates proliferation of osteoblasts and collagen synthesis invitro [53], and can increase the thickness of cortical bone whenapplied adjacent to periosteum in vivo [54]. Some studies invitro demonstrated that combinatory use of these factors withcalcium phosphate ceramics resulted in improved bone growthdue to adsorption of big doses of rhTGF-β1 on the ceramicsurface [55,56]. Nevertheless, the use of resorbable CPC canallow for a homogeneous distribution of the growth factor notonly on the surface but in the whole bulk of the cement, thusmaking it possible the growth factor release for a moreprolonged time, while degradation of the cement takes place,activating simultaneously the new bone formation.
Recently, Blom et al. studied the effect of the incorporationof human recombinant TGF-β1 (rhTGF-β1) in a CPC, based inα-TCP, TTCP and DCPD, on the first stages of bone formationin vitro, using primary rat bone cells [57]. The growth factorwas incorporated in the cement during setting, and resultsshowed that the addition of rhTGF-β1 stimulated the differen-tiation of pre-osteoblastic cells in vitro. Other studies analysedthe effect of growth factor addition on the physico-chemical and

108 M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
mechanical properties of two different cement formulations[58,59], demonstrating that CPCs with TGF did not differ fromconventional cements, in terms of the setting parameters.Preclinical studies in animals proved as well the stimulatingeffect of TGF on bone growth [60]. In contrast to whathappened in most cases with the antibiotics, the drug releasekinetics of this osteogenic factor was quite slow. In bothcements an initial elution in the first days was followed by astabilization of the released amount after this time. These resultssuggested that the growth factor was released only from thesuperficial layer, in contact with the surrounding medium, andnot from the whole volume of the CPC. This was confirmed bythe fact that the enlargement of the area in contact with themedium by fragmentation, resulted in another burst or rhTGF-β1 release. This behaviour can be related to the high bindingaffinity of the protein for calcium phosphate ceramics, and putsforward a different kinetics from that described for otherconventional drugs.
A similar trend was observed when human recombinantBMP-2 loaded poly(DL-lactic-co-glycolic acid) (PLGA) micro-spheres were mixed with a CPC [61]. Release of rhBMP-2 wasvery limited (mean of 3.1% after 28 days under neutralconditions), much slower than the release of the protein in themicrospheres alone (18% after 28 days). This was attributed tothe physical entrapment of the microparticles within thenanoapatitic porous cement. According to the authors, thenanoporosity of the CPC not only did not facilitate the release ofthe protein, but may have further limited it because of the highbinding affinity of the protein for CPC.
The in vivo performance of BMP-2 was assessed bySeeherman et al. in a complete series of works where differentinjectable osteogenic factor/carrier combinations was reviewedin different large animal models [62–65]. Among all the carriersstudied, a commercial resorbable CPC, based in ACP andDCPD, was considered to be the best carrier in terms of bonehealing after 10 weeks, in a fibular osteotomy, in a non-humanprimate model. One of the main advantages of this carrier is thatit can be implanted by a single percutaneous injection. Bonehealing was accelerated by approximately 40%, as compared tountreated osteotomy sites. Ohura et al. obtained analogousresults by incorporating different amounts of recombinanthuman BMP (rhBMP-2) to a cement formed by β-TCP, MCPM,calcium sulphate hemihydrate and granules of β-TCP, aftersetting [66], and implanting it in critical fractures in a rabbitmodel. One of the main advantages of employing this CPCs as acarrier with respect to other ceramics already used for the samepurpose [67] was supposed to be the faster rate of resorption ofthis cement. In the fractures filled with cement with theoptimum rhBMP-2 concentration, bone formed very rapidly,and after 3 weeks the fracture was already consolidated. Most ofthe cement cylinders were resorbed, except from the β-TCPgranules, and were completely replaced by new bone in6 weeks. By the ninth week, the torsion resistance was 99%recovered. None of the fractures consolidated when theunloaded cement was used as a filling material. In conclusion,the CPC turned out to be an adequate substrate for delivery ofrhBMP-2. Similar results are reported by Kamegai et al. [68].
Other proteins which have a relevant function in bone tissueand which have been incorporated in CPC aiming at improvingtheir biological and mechanical properties are collagen I andosteocalcin [69]. Osteocalcin is a non-collagenous proteinfound in the extracellular bone matrix, which plays an importantrole in the biomineralization process. The addition ofosteocalcin to an apatitic cement obtained from a mixture ofα-TCP, DCP, calcium carbonate and HA seeds modified themicrostructure by reducing the size of precipitated hydroxyap-atite crystals. On the other side osteocalcin modified the cellularresponse in vitro of the osteosarcoma cell line SAOS-2,improving their initial adhesion, but without significant effecton cell proliferation.
Incorporation of insulin and bovine albumin in a CPC basedin TTCP and DCP was studied by Otsuka et al [70], in the caseof albumin as a model protein to test protein release. Theirresults showed that these polypeptide drugs do not disturb thesetting reaction of cement. Moreover, their release in aphosphate solution went on more than 3 weeks, following theHiguchi's law.
8. Conclusions
It has been shown that the research carried out in the pastdecade put forward the great potential of CPC as carriers forcontrolled release and vectoring of drugs in the skeletal system.Especially encouraging are the results obtained with osteogenicfactors for bone regeneration applications. However, one mustadmit that the industrial use of CPC for drug delivery is not easyfor two main reasons. First, implant companies selling CPC donot have the know-how to deal with drugs, whereaspharmaceutical companies do not have any know-how withCPC, and often do not have any interest in working with suchsmall markets. Second, infections are not always produced bythe same bacteria. Therefore, it would be of importance topropose a system that could be combined with many differentdrugs, in such a way that the surgeon could choose the drug justbefore implantation. However, as it has been shown, variousdrugs have various effects on CPC properties, and thisrepresents a serious drawback for the implementation of thistechnology. A lot of work has still to be done to establish thegeneral laws that control the release profile of these types ofmaterials, in order to be able to adjust them to differenttherapeutical needs and to obtain reproducible and predictabledrug delivery systems.
Acknowledgements
The authors thank the Science and Technology SpanishMinistry for funding this work through project CICYTMAT2002-04297. T. Traykova is grateful to the SpanishMinistry of Education for her grant SB2003-0352.
References
[1] National Osteoporosis Foundation, Physician's Guide to Prevention andTreatment of Osteoporosis, Exempta Medica, Belle Mead, NJ, 1998.

109M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
[2] D.G. Arkfield, E. Rubenstein, Quest for the holy grial to cure arthritis andosteoporosis: emphasis on bone drug delivery systems, Adv. Drug Deliv.Rev. 57 (2005) 934–944.
[3] A. Tiselius, S. Hjerten, O. Levin, Protein chromatography on calciumphosphate columns, Arch. Biochem. Biophys. 65 (1956) 132–136.
[4] M.R. Urist, Y.K. Huo, A.G. Brownell, W.M. Hohl, J. Buyske, A. Lietze, P.Tempst, M. Hunkapiller, R.J. DeLange, Purification of bovine bonemorphogenetic protein by hydroxyapatite chromatography, Proc. Natl.Acad. Sci. 81 (1984) 371–375.
[5] R. LeGeros, A. Chohayeb, A. Shulman, Apatitic calcium phosphates:possible dental restorative materials, J. Dent. Res. 61 (1982) 343.
[6] W.E. Brown, L.C. Chow, A new calcium phosphate setting cement, J.Dent. Res. 62 (1983) 672.
[7] F.C.M. Driessens, M.G. Boltong, I. Khairoun, E.A.P. De Maeyer, M.P.Ginebra, R. Wenz, J.A. Planell, R.M.H. Verbeeck, Applied aspects ofcalcium phosphate bone cement, in: D.L. Wise, D.J. Trantolo, K.U.Lewandrowski, J.D. Gresser, M.V. Cattaneo (Eds.), Biomaterials Engi-neering and Devices: Human Applications. Vol. 2: Orthopaedic, Dentaland Bone Graft Applications, Humana Press, Totowa, NJ, 2000,pp. 253–260.
[8] M. Bohner, U. Gbureck, J.E. Barralet, Technological issues for thedevelopment of more efficient calcium phosphate bone cements: a criticalassessment, Biomaterials 26 (2005) 6423–6429.
[9] A. Tofighi, S. Mounic, P. Chakravarthy, C. Rey, D. Lee, Setting reactionsinvolved in injectable cements based on amorphous calcium phosphate,Key Eng. Mater. 192–195 (2000) 769–772.
[10] B. Constantz, et al., Skeletal repair by in situ formation of the mineralphase of bone, Science 267 (1995) 1796–1799.
[11] M. Freche, J.L. Lacout, Z. Hatim, 1999. Method for preparing abiomaterial based on hydroxyapatite, resulting biomaterial and surgicalor dental use. FR Patent No. 2776282.
[12] F.C.M. Driessens, M.G. Boltong, O. Bermudez, M.P. Ginebra, E.Fernández, J.A. Planell, Effective formulations for the preparation ofcalcium phosphate bone cements, J. Mater. Sci., Mater. Med. 5 (1994)164–170.
[13] M.P. Ginebra, E. Fernandez, E. De Maeyer, R.M.H. Verbeeck, M.G.Boltong, J. Ginebra, F.C.M. Driessens, J.A. Planell, Setting reaction andhardening of an apatitic calcium phosphate cement, J. Dent. Res. 76 (4)(1997) 905–912.
[14] M.P. Ginebra, M.G. Boltong, E. Fernández, J.A. Planell, F.C.M. Driessens,Effect of various additives and of the temperature on some properties of anapatitic calcium phosphate cement, J. Mater. Sci., Mater. Med. 6 (1995)612–616.
[15] M.P. Ginebra, F.C.M. Driessens, J.A. Planell, Effect of the particle size onthe micro and nanostructural features of a calcium phosphate cement: akinetic analysis, Biomaterials 25 (2004) 3453–3462.
[16] E. Fernández, M.G. Boltong, M.P. Ginebra, F.C.M. Driessens, O.Bermúdez, J.A. Planell, Development of a method to measure the periodof swelling of calcium phosphate cements, J. Mater. Sci. Lett. 15 (1996)1004–1005.
[17] M.P. Ginebra, E. Fernández, F.C.M. Driessens, J.A. Planell, The effectof Na2HPO4 addition on the setting reaction kinetics of an α-TCPcement, in: R.Z. LeGeros, J.P. LeGeros (Eds.), Proceedings of the 11thInternational Symposium on Ceramics in Medicine, . Bioceramics, vol.11, World Scientific Publishing Co. Pte. Ltd., Singapore, 1998,pp. 243–246.
[18] K. Kurashina, et al., In vivo study of calcium phosphate cements:implantation of an α-tricalcium phosphate/dicalcium phosphate dibasic/tetracalcium phosphate monoxide cement paste, Biomaterials 18 (1997)539–543.
[19] D. Apelt, F. Theiss, A.O. El-Warrak, K. Zlinszky, R. Bettschart-Wolfisberger, M. Bohner, S. Matter, J.A. Auer, B. Von Rechenberg, Invivo behavior of three different injectable hydraulic calcium phosphatecements, Biomaterials 25 (7–8) (2004) 1439–1451.
[20] J.A. Jansen, J.E. de Ruijter, H.G. Schaeken, J.P.C. van der Waerden, J.A.Planell, F.C.M. Driessens, Evaluation of tricalciumphosphate/hydroxyap-atite cement for tooth replacement: an experimental animal study, J. Mater.Sci., Mater. Med. 6 (1995) 653–657.
[21] C.D. Friedman, P.D. Costantino, S. Takagi, L.C. Chow, Bonesourcehydroxyapatite cement: a novel biomaterial for cranofacial skeletal tissueengineering and reconstruction, J. Biomed. Mater. Res., Appl. Biomater.43 (1998) 428–432.
[22] S. Larsson, T.W. Bauer, Use of injectable calcium phosphate cement forfracture fixation: a review, Clin. Orthop. Relat. Res. 395 (2002) 23–32.
[23] E.M. Ooms, J.G.C. Wolke, M.T. van de Heuvel, B. Jeschke, J.A. Jansen,Histological evaluation of the bone response to calcium phosphate cementimplanted in cortical bone, Biomaterials 24 (6) (2003) 989–1000.
[24] P. Torner, Bone tissue repair by osteotransduction with a calciumphosphate cement. An experimental study. PhD Thesis from the Dept ofSurgery, Faculty of Medicine. Universitat de Barcelona, Barcelona, Spain(2001).
[25] E. Mathiowitz (Ed.), Encyclopaedia of Controlled Drug Delivery, JohnWiley and Sons, New York, 1999.
[26] B.D. Ratner, A.S. Hoffman, F.J. Schoen, J.E. Lemons (Eds.), BiomaterialsScience. An Introduction to Materials in Medicine, 2nd Edition, AcademicPress, San Diego, CA, 2004.
[27] T. Higuchi, Mechanism of sustained-action medication. Theoreticalanalysis of release of solid drugs dispersed in solid matrices, J. Pharm.Sci. 52 (1963) 1143–1149.
[28] M. Otsuka, Y. Matsuda, Y. Suwa, J.L. Fox, W.I. Higuchi, A novel skeletaldrug delivery system using self-setting calcium phosphate cement 5: drug-release behaviour from a heterogeneous drug-loaded cement containing ananticancer drug, J. Pharm. Sci. 83 (11) (1994) 1565–1568.
[29] M. Otsuka, Y. Nakahigashi, Y. Matsuda, J.L. Fox, W.I. Higuchi, Y.Sugiyama, Effect of geometrical cement size on in vitro indomethacinrelease from self-setting apatite cement, J. Control. Release 52 (3) (1998)281–289.
[30] M. Otsuka, Y. Nakahigashi, Y. Matsuda, J.L. Fox, W.I. Higuchi, Y.Sugiyama, A novel skeletal drug delivery system using self-setting calciumphosphate cement VIII: the relationship between in vitro and in vivodrug release from indomethacin-containing cement, J. Control. Release 43(2–3) (1997) 115–122.
[31] M. Otsuka, Y. Matsuda, J.L. Fox, W.I. Higuchi, Novel skeletal drugdelivery system using self-setting calcium phosphate cement 9: effects ofthe mixing solution volume on anticancer drug-release from homogeneousdrug-loaded cement, J. Pharm. Sci. 84 (6) (1995) 733–736.
[32] M. Otsuka, Y. Matsuda, Y. Suwa, J.L. Fox, W.I. Higuchi, A novel skeletaldrug-delivery system using self-setting calcium-phosphate cement 4.Effects of the mixing solution volume on the drug-release rate ofheterogeneous aspirin-loaded cement, J. Pharm. Sci. 83 (2) (1994)259–263.
[33] M. Bohner, J. Lemaitre, P. VanLanduyt, P.Y. Zambelli, H.P. Merkle, B.Gander, Gentamicin-loaded hydraulic calcium phosphate bone cement asantibiotic delivery system, J. Pharm. Sci. 86 (5) (1997) 565–572.
[34] M. Bohner, J. Lemaitre, H.P. Merckle, B. Gander, Control of gentamicinrelease from a calcium phosphate admixed poly(acrylic acid), J. Pharm.Sci. 89 (10) (2000) 1262–1270.
[35] T. Suzuki, K. Arai, H. Goto, M. Hanano, J. Watanabe, K. Tomono,Dissolution tests for self-setting calcium phosphate cement-containingnifedipine, Chem. Pharm. Bull. 50 (6) (2002) 741–743.
[36] M. Otsuka, Y. Matsuda, Z. Wang, J.L. Fox, W.I. Higuchi, Effect of sodiumbicarbonate amount on in vitro indomethacin release from self-settingcarbonated-apatite cement, Pharm. Res. 14 (4) (1997) 444–449.
[37] I.C. Tung, In-vitro drug release of antibiotic-loaded porous hydroxyapatitecement, Artif. Cells Blood Substit. Immobil. Biotechnol. 23 (1) (1995)81–88.
[38] K. Klemm, Antibiotic bead chains, Clin. Orthop. 295 (1993) 63–76.[39] L.F. Peltier, R.H. Jones, Treatment of unicameral bone cysts by curettage
and packing with plaster-of-paris pellets, J. Bone Jt. Surg., Am. 60A(1978) 820–822.
[40] M. Takechi, Y. Miyamoto, K. Ishikawa, M. Nagayama, M. Kon, K.Asaoka, K. Suzuki, Effects of added antibiotics on the basic properties ofanti-washout-type fast-setting calcium phosphate cement, J. Biomed.Mater. Res. 39 (2) (1998) 308–316.
[41] Ratier, I.R. Gibson, S.M. Best, M. Freche, J.L. Lacout, F. Rodriguez,Behaviour of a calcium phosphate bone cement containing tetracycline

110 M.P. Ginebra et al. / Journal of Controlled Release 113 (2006) 102–110
hydrochloride or tetracycline complexed with calcium ions, Biomaterials22 (2001) 897–901.
[42] Y. Huang, C.S. Liu, H.F. Shao, Z.J. Liu, Study on the applied properties oftobramycin-loaded calcium phosphate cement, Key Eng. Mater. 192-1(2000) 853–860.
[43] C. Hamanishi, K. Kitamoto, S. Tanaka, M. Otsuka, Y. Doi, T. Kitahashi, Aself-setting TTCP–DCPD apatite cement for release of vancomycin,J. Biomed. Mater. Res., Appl. Biomater. 33 (3) (1996) 139–143.
[44] M.T. Ethell, R.A. Bennett, M.P. Brown, K. Merritt, J.S. Davidson, T. Tran,In vitro elution of gentamicin, amikacin and ceftiofur from polymethyl-methacrylate and hydroxyapatite cement, Vet. Surg. 29 (5) (2000)375–382.
[45] M. Takechi, Y. Miyamoto, Y. Momota, T. Yuasa, S. Tatehara, M.Nagayama, K. Ishikawa, K. Suzuki, The in vitro antibiotic release fromanti-washout apatite cement using chitosan, J. Mater. Sci., Mater. Med. 13(10) (2002) 973–978.
[46] H.P. Stallmann, C. Faber, A.L.J.J. Bronckers, A.V.N. Amerongen, P.I.J.M.Wuisman, Osteomyelitis prevention in rabbits using antimicrobial peptidehLF-11 or gentamicin-containing calcium phosphate cement, J. Anti-microb. Chemother. 54 (2) (2004) 472–476.
[47] M.P. Ginebra, A. Rilliard, E. Fernández, C. Elvira, J. San Román, J.A.Planell, Mechanical and rheological improvement of a calcium phosphatecement by the addition of a polymeric drug, J. Biomed. Mater. Res. 57 (1)(2001) 113–118.
[48] M. Otsuka, Y. Nakahigashi, Y. Matsuda, J.L. Fox, W.I. Higuchi, A novelskeletal drug delivery system using self-setting calcium phosphate cement7: effect of biological factors on indomethacin release from the cementloaded on bovine bone, J. Pharm. Sci. 83 (11) (1994) 1569–1573.
[49] T. Kokubo, H. Kim, M. Kawashita, Novel bioactive materials withdifferent mechanical properties, Biomaterials 24 (2003) 2161–2175.
[50] M. Otsuka, K. Yoneoka, Y. Matsuda, J.L. Fox, W.I. Higuchi, Y. Sugiyama,Oestradiol release from self-setting apatitic bone cement responsive toplasma-calcium level in ovariectomized rats and its physicochemicalmechanism, J. Pharm. Pharmacol. 49 (12) (1997) 1182–1188.
[51] M. Otsuka, Y. Matsuda, A.A. Baig, A. Chhettry, W.I. Higuchi, Calcium-level responsive controlled drug delivery from implant dosage forms totreat osteoporosis in an animal model, Adv. Drug Deliv. Rev. 42 (2000)249–258.
[52] M.E. Nimni, Polypeptide growth factors: targeted delivery systems,Biomaterials 18 (1997) 1201–1225.
[53] M. Centrella, J. Massague, E. Canalis, Human platelet-derived transform-ing growth factor β stimulates parameters of bone growth in fetal ratcalvaria, Endocrinology 119 (1986) 2306–2312.
[54] M. Noda, J.J. Camilliere, In vivo stimulation of bone formation bytransforming growth factor β, Endocrynology 124 (1989) 2991–2994.
[55] C. Bosch, B. Melsen, R. Gibbons, K. Vargervik, Human recombinanttransforming growth factor beta 1 in healing of calvarial bone defects,Craniofac. Surg. 7 (1996) 300–310.
[56] M. Lind, S. Overgaard, K. Soballe, T. Nguyen, B. Ongpipattanakul, C.Bunger, Transforming growth factor-beta 1 enhances bone healing tounloaded tricalcium phosphate coated implants: an experimental study indogs, J. Orthop. Res. 14 (1996) 343–350.
[57] E.J. Blom, J. Klein-Nulend, C.P.A.T. Klein, K. Kurashina, M.A.J. vanWaas, E.H. Burger, Transforming growth factor-β1 incorporated duringsetting in calcium phosphate cement stimulates bone cell differentiation invitro, J. Biomed. Mater. Res. 50 (2000) 67–74.
[58] E.J. Blom, J. Klein-Nulend, J.G.C. Wolke, K. Kurashina, M.A.J. vanWaas, E.H. Burger, Transforming growth factor-beta 1 incorporation in analpha-tricalcium phosphate/dicalcium phosphate dihydrate/tetracalciumphosphate monoxide cement: release characteristics and physicochemicalproperties, Biomaterials 23 (4) (2002) 1261–1268.
[59] E.J. Blom, J. Klein-Nulend, J.G.C. Wolke, M.A.J. van Waas, F.C.M.Driessens, E.H. Burger, Transforming growth factor-beta 1 incorporationin a calcium phosphate bone cement: material properties and releasecharacteristics, J. Biomed. Mater. Res. 59 (2) (2002) 265–272.
[60] E.J. Blom, J. Klein-Nulend, L. Yin, M.A.J. van Waas, E.H. Burger,Transforming growth factor-β1 in calcium phosphate cement stimulatesbone regeneration, J. Dent. Res. 79 (2000) 255.
[61] P.Q. Ruhe, E.L. Hedberg, N.T. Padron, P.H. Spauwen, J.A. Jansen, A.G.Mikos, rhBMP-2 release from injectable poly(DL-lactic-co-glycolic acid)/calcium-phosphate cement composites, J. Bone Jt. Surg. 85 (2003) 75–82.
[62] D.D. Lee, A. Tofighi, M. Aiolova, P. Chakravarthy, A. Catalano, A. Majad,D. Knaack, Alpha-BSM®: a biomimetic bone substitute and drug deliveryvehicle, Clin. Orthop. Relat. Res. 367 (1999) S396–S405 (Suppl.).
[63] H.J. Seeherman, R. Li, J.M. Wozney, A review of preclinical programdevelopment for evaluating injectable carriers for osteogenic factors,J. Bone Jt. Surg., A 85 (2003) 96–111.
[64] R.B. Edwards III, H.J. Seeherman, J.J. Bogdanske, J. Devitt, R. Vanderby,M.D. Markee, Percutaneous injection of recombinant human bonemorphogenetic protein-2 in a calcium phosphate paste accelerates healingof a canine tibial osteotomy, J. Bone Jt. Surg., A 86 (2004) 1425–1438.
[65] H.J. Seeherman, M. Bouxsein, H. Kim, R. Li, X.J. Li, M. Aiolova, J.M.Wozney, Recombinant human bone morphogenetic protein-2 delivered inan injectable calcium phosphate paste accelerates osteotomy-site healing ina nonhuman primate model, J. Bone Jt. Surg., A 86 (2004) 1961–1973.
[66] K. Ohura, C. Hamanishi, S. Tanaka, N. Matsuda, Healing of segmentalbone defects in rats induced by a β-TCP-MCPM cement combined withrhBMP-2, J. Biomed. Mater. Res. 44 (1999) 168–175.
[67] M.R. Urist, A. Lietze, E. Dawson, β-Tricalcium phosphate delivery systemfor bone morphogenetic protein, Clin. Orthop. 187 (1984) 277–280.
[68] A. Kamegai, N. Shimamura, K. Naitou, K. Nagahara, N. Kanematsu, M.Mori, Bone formation under the influence of bone morfogenetic protein/self-setting apatite cement composite as delivery system, Bio-Med. Mater.Eng. 4 (1994) 291–307.
[69] B. Knepper-Nicolai, A. Reinstorf, I. Hofinger, K. Flade, R. Wenz, W.Pompe, Influence of osteocalcin and collagen i on the mechanical andbiological properties of Biocement D, Biomol. Eng. 19 (2–6) (2002)227–231.
[70] M. Otsuka, Y. Matsuda, Y. Suwa, J.L. Fox, W.I. Higuchi, Novel skeletaldrug-delivery system using self-setting calcium phosphate cement. 3.Physicochemical properties and drug-release rate of bovine insulin andbovine albumin, J. Pharm. Sci. 83 (1994) 255–258.