Embed Size (px)
Citation preview

Calcium Phosphate Cements loaded with Pantoprazole as Novel Bone Substitutes
By
Michel Victor Furtado Araújo
A thesis submitted in conformity with the requirements for the degree of Master of Science in Dentistry
Graduate Faculty of Dentistry
University of Toronto
© Copyright by Michel Victor Furtado Araújo 2008

Calcium Phosphate Cements loaded with Pantoprazole as Novel Bone Substitutes
Michel Victor Furtado Araújo, Master of Science, 2008
Faculty of Dentistry
University of Toronto
ABSTRACT
Calcium phosphate cements are produced by the mixing of calcium phosphate powders in
an aqueous solution resulting in a low-temperature synthesized hydroxyapatite. They have been
used as bone substitutes and drug delivery systems. The present work examined the possibility of
a machine-based modification to this process to derive a standardized preparation method of
calcium phosphate cements that could be loaded with Pantoprazole. To examine the
characteristics of these novel materials, the following analyses of hand- and machine-made
cements, with and without Pantoprazole were undertaken: in vitro surface characterization,
dissolution, hydroxyapatite conversion, Pantoprazole delivery, as well as in vivo reparative bone
formation and particulate degradation. The in vitro surface characterization, dissolution at
different pHs, and drug release analyses showed insignificant differences between hand- and
machine-prepared cements. However, machine-made cements showed increased hydroxyapatite
conversion, decreased dissolution at pH 7.4, and better in vivo outcomes than commercially
available bone-substitute particulate biomaterials.
ii

ACKNOWLEDGEMENTS
I could never have completed this thesis without the hard work and personal support of a
great many people. None of the experiments could have been run without the technical assistance
of many of my fellow scientists. Thanks to Battista Calvieri, Steven Doyle, Dr. Neil Coombs,
and Ilya Gourevich for their help with SEM; Dorthy Donn and Susan Carter for their help with
surgery; Dr. Stan Lugowski for his help with the AAS measurements; Dr. Srebri Petrov for his
help with the PXRD; and Lori Mockler for her kind help and departmental assistance from the
very beginning.
Financial support from Ontario Research and Development Challenge Fund (ORDCF)
and University of Toronto Scholarship, as well as material support from Biomet 3i are gratefully
acknowledged.
Thanks to my soccer teammates, who made the past two years much more enjoyable than
I would ever have imagined. Special thanks to my friends Anthony Capotosto, Pierre Grossi, and
Matthew Willis. Willis, your help goes beyond your excellent skills as a goalkeeper and I would
like to thank you for editing this work.
I am most grateful for the insightful recommendations of my committee members, Dr.
Paul Santerre and Dr. Phillip Watson, whose productive criticism helped to improve the quality
of this thesis.
I am eternally indebted to all the members of the Bone Interface Group, of which I am
honoured to be a part. Thanks to Krista Sider for her friendship and help with MicroCT; Liz for
her friendship; Limin Guan, whose friendship and help I’ll never forget; Patralika for always
being ready to cheer me up and for her help with the histology; Dave for becoming a good friend
and a funny, dirty Australian; Jane for being her great self and a most competent English editor;
Val for all her administrative work, friendship, and creative ideas; Padina, Yuko, Lorraine,
Elaine, Catalina, Alejandro, Hamideh, Rano, Rahul, and Nazlee for being part of one of the best
times of my life.
My kindest thanks to JED, whose patience and unconditional support guided me in this
project. Dr. Davies’ scientific knowledge is the reason I still believe in professional academia.
Living under his guidance for the last two-and-a-half years taught me that you can be a genius
and still very humble, you can be a leader without being harsh, and you can be both a supervisor
and a good friend. I will carry his mentorship and example with me for the rest of my life.
iii

I would also like to express my gratitude to Dr. Reynaldo Todescan and Dr. Vanessa
Mendes, members of the “Brazilian Connection”. Thanks to Reynaldo for his crucial guidance in
the beginning of my life in Toronto. Vanessa, I would never be where I am without your willing
help. Your character has been the source of my faith in people nowadays. You have become
more than a friend, you are now the sister I never had in Brazil.
Thanks to my family in Brazil, especially my in-laws, Laércio Couto and Maria José,
who started this dream 26 years ago. To my parents, Maria do Carmo and Antonio, my
grandmother Terezinha, and my brothers, Marco André, Marcelo and Mauro, for their never-
ending love and support. Special thanks to my beloved wife, Michelle Araújo, whose love and
support I try to deserve everyday. Words are just not enough to express the significance of
having you in my life.
Finally, I would like to dedicate this thesis to my wife and parents. You are the reason I
dream every night and work hard everyday!
iv

TABLE OF CONTENTS
ABSTRACT _____________________________________________________________________ ii
ACKNOWLEDGEMENTS_________________________________________________________ iii
LIST OF FIGURES ______________________________________________________________ vii LIST OF TABLES _______________________________________________________________ viii 1. INTRODUCTION _______________________________________________________________1
1.A Endosseous peri-implant healing ________________________________________________________ 1 1.A.1 Inflammation and blood clotting _____________________________________________________ 1 1.A.2 Provisional connective tissue matrix creation ___________________________________________ 2 1.A.3 Osteoconduction and bone formation _________________________________________________ 3 1.A.4 Bone remodelling ________________________________________________________________ 5
1.B Calcium phosphate cements ____________________________________________________________ 5 1.B.1 Preparation methods ______________________________________________________________ 6 1.B.2 Calcium phosphate cement reaction __________________________________________________ 7 1.B.3 Calcium phosphate cements as drug delivery systems (DDS)_______________________________ 8 1.B.4 In vivo behaviour of calcium phosphate cements _______________________________________ 10
1.C The effect of gastric proton pump inhibitors (PPI) on osteoclastic resorption _____________________ 12 1.C.1 Osteoclastic differentiation and acidic secretion through ion pumps ________________________ 12 1.C.2 Osteoclastic H+ATPase proton pump as a pharmacological target __________________________ 14 1.C.3 Mechanism of action of Pantoprazole ________________________________________________ 16
1.D Bone substitutes ____________________________________________________________________ 16 1.D.1 Autogenous grafts _______________________________________________________________ 17 1.D.2 Calcium phosphate ceramics _______________________________________________________ 18 1.D.3 Bioactive glass__________________________________________________________________ 20 1.D.4 Anorganic bone _________________________________________________________________ 20 1.D.5 Demineralized bone matrix ________________________________________________________ 21
1.E Rationale __________________________________________________________________________ 23 1.F Hypothesis _________________________________________________________________________ 24 1.G Objectives _________________________________________________________________________ 24
2. MATERIALS AND METHODS __________________________________________________25 2.A Preparation of particulate calcium phosphate cement________________________________________ 25
2.A.1 Grinding of the reagents __________________________________________________________ 26 2.A.2 Preparation of the liquid phase _____________________________________________________ 26 2.A.3 Hand-made calcium phosphate cements and Pant-calcium phosphate cements (H and HP)_______ 27
2.A.3.1 Mixing of the solid with the liquid phase _________________________________________ 27 2.A.4 Machine-made calcium phosphate cements and Pant-calcium phosphate cements (M and MP) ___ 27 2.A.5 Preparing particulate calcium phosphate cements_______________________________________ 27
2.B Characterization of hand- and machine-made calcium phosphate cements (H and M)_______________ 28 2.B.1 Particle size distribution, surface area, porosity, and pore size (Scanning Electron Microscopy)___ 28
2.B.1.1 Particle size distribution and total surface area _____________________________________ 29 2.B.1.2 Porosity and pore size ________________________________________________________ 29
2.B.2 In vitro degradation ______________________________________________________________ 30 2.B.2.1 Calcium concentration measurements (Atomic Absorption Spectroscopy)________________ 30
2.B.3 In vivo implantation______________________________________________________________ 31 2.B.3.1 Histomorphometric analysis (Micro-Computed Tomography) _________________________ 32
2.C Hand- and machine-made calcium phosphate cements with and without Pantoprazole ______________ 33 2.C.1 Powder X-ray diffraction (PXRD) analysis (H, M, HP, MP) ______________________________ 33 2.C.2 In vitro degradation (H, M, HP, MP)_________________________________________________ 34 2.C.3 Pantoprazole release kinetics (HP, MP) ______________________________________________ 34
2.C.3.1 Pantoprazole standard solutions and release kinetic curve ____________________________ 35 2.C.4 In vivo implantation______________________________________________________________ 35
v

2.C.4.1 Pilot study (Pantoprazole-, Omeprazole-, Concanamycin-, and Bafylomycin-calcium phosphate cements) _________________________________________________________________________ 35 2.C.4.2 Main study (MP x M, and MP x Empty defect)_____________________________________ 37 2.C.4.3 Experimental setup __________________________________________________________ 37 2.C.4.4 Histomorphometric analysis ___________________________________________________ 38 2.C.4.5 Histological processing _______________________________________________________ 38
2.D Other bone substitutes________________________________________________________________ 39 2.D.1 Anorganic bone (BioOssTM), Bioactive glass (BioGranTM), and Demineralized bone matrix (AllogenixTM) _______________________________________________________________________ 39 2.D.2 In vivo implantation _____________________________________________________________ 39
2.D.2.1 Histomorphometric analysis and histological processing _____________________________ 39 2.E Statistical analysis ___________________________________________________________________ 43
3. RESULTS _____________________________________________________________________44 3.A Characterization of hand- and machine-made calcium phosphate cements _______________________ 44
3.A.1 Particle size distribution and surface area (SEM) _______________________________________ 44 3.A.2 Porosity and pore size (FESEM) ____________________________________________________ 46 3.A.3 Calcium concentration analysis (AAS) _______________________________________________ 49 3.A.4 In vivo implantation (H x M)_______________________________________________________ 50
3.B Hand- and machine-made calcium phosphate cements with and without Pantoprazole ______________ 53 3.B.1 Time-dependent HA conversion (PXRD analysis) ______________________________________ 53
3.B.1.1 Pilot study _________________________________________________________________ 53 3.B.1.2 Main study _________________________________________________________________ 54
3.B.2 Calcium concentration analysis (AAS) _______________________________________________ 54 3.B.3 Drug release from calcium phosphate cements _________________________________________ 56
3.B.3.1 Pantoprazole standard solutions and release kinetic curve ____________________________ 56 3.B.4 In vivo implantation______________________________________________________________ 57
3.B.4.1 Pilot study (Pantoprazole-, Omeprazole-, Concanamycin-, and Bafylomycin-doped calcium phosphate cements) ________________________________________________________________ 57 3.B.4.2 MP x M ___________________________________________________________________ 60 3.B.4.3 MP x Empty defect __________________________________________________________ 64
3.C Other bone substitutes ________________________________________________________________ 66 3.C.1 MP, BioOssTM, BioGranTM, and AllogenixTM __________________________________________ 66
4. DISCUSSION __________________________________________________________________69 4.A Characterization of hand- and machine-made calcium phosphate cements (H and M) ______________ 69
4.A.1 Particle size distribution and surface area of M are not different from those of H. _____________ 69 4.A.2 M and H show overall similar porosity and pore size. ___________________________________ 70 4.A.3 M and H present similar in vitro dissolutions at different pHs._____________________________ 71 4.A.4 The particulate degradation rate and reparative bone remodelling are decreased for machined- compared to hand-prepared cements._____________________________________________________ 72
4.B Hand- and machine-made cements with and without Pantoprazole (H, M, HP, MP) ________________ 74 4.B.1 MP exhibit higher HA conversion and decreased dissolution at pH 7.4. _____________________ 74 4.B.2 MP and HP sustain the in vitro release of Pantoprazole until the drug starts to degrade.________ 76 4.B.3 Pantoprazole does not alter the in vivo degradation of calcium phosphate cements.____________ 77 4.B.4 MP provide an osteoconductive scaffold for bone formation and are completely resorbed in rat femoral defects after 16 weeks of implantation. _____________________________________________ 78
5. CONCLUSIONS _______________________________________________________________81 6. REFERENCES_________________________________________________________________82 7. APPENDICES _________________________________________________________________94
7.A In vivo implantation _________________________________________________________________ 94 7.A.1 Pilot study _____________________________________________________________________ 94 7.A.2 MP x BioOssTM x BioGranTM x AllogenixTM __________________________________________ 96
vi

LIST OF FIGURES
Figure 1.1 Intracellular events in osteoclastic resorption ____________________________________________ 13
Figure 2.1 Preparation methods of hand- and machine-made cements __________________________________ 25
Figure 2.2 Mixer Mill 301 and zirconium oxide jars and balls ________________________________________ 26
Figure 2.3 Rat femora model. Sequence of surgical stages ___________________________________________ 32
Figure 2.4 The principle of a MicroCT scan ______________________________________________________ 33
Figure 2.5 Pictures of BioOssTM, BiogranTM, and AllogenixTM _________________________________________ 39
Figure 2.6 MicroCT slice of a DBM sample. Marrow cavity with newly-formed bone and no visible material (demineralized bone matrix does not absorb x-rays) ________________________________________________ 41
Figure 2.7 Bone volume measurements for BAG samples ____________________________________________ 41
Figure 2.8 TMC measurement and overview of BAG particulate contours _______________________________ 42
Figure 3.1 SEM image of a H sample and the particle threshold analysis using the Image J Particle Analyzer tool 44
Figure 3.2 Particle size distribution of calcium phosphate cements_____________________________________ 45
Figure 3.3 Total surface area of hand- and machine-made calcium phosphate cements _____________________ 45
Figure 3.4 SEM image of a HM sample and the threshold of its porosity using the Image J Particle Analyzer tool 46
Figure 3.5 Porosity percentages of calcium phosphate cements _______________________________________ 47
Figure 3.6 SEM images of pore size measurements _________________________________________________ 48
Figure 3.7 Dissolution of H and M ______________________________________________________________ 49
Figure 3.8 MicroCT slices of H x M _____________________________________________________________ 51
Figure 3.9 Reparative bone volumes for M and H __________________________________________________ 52
Figure 3.10 Particulate volume for M and H ______________________________________________________ 52
Figure 3.11 HA conversion of hand-, machine-made, doped, and undoped calcium phosphate cements ________ 54
Figure 3.12 Dissolution of hand- and machine-made, doped and undoped- calcium phosphate cements in saline at pH 7.4 ____________________________________________________________________________________ 55
Figure 3.13 Standard curve and formula for known Pantoprazole solutions ______________________________ 56
Figure 3.14 Pantoprazole release from calcium phosphate cements ____________________________________ 57
Figure 3.15 Bone and particulate volumes of calcium phosphate cements _______________________________ 59
Figure 3.16 Bone volumes of MP and M _________________________________________________________ 61
Figure 3.17 Particle volumes of MP and M _______________________________________________________ 61
Figure 3.18 Histological sections of M and MP samples at 5 days and 2 weeks (FW=810µm)________________ 62
Figure 3.19 Histological sections of M and MP at 6 weeks (FW=810µm)________________________________ 63
Figure 3.20 Histological section of MP at 16 weeks (FW=142.3µm) ___________________________________ 64
Figure 3.21 µCT slices of MP and empty defects ___________________________________________________ 65
Figure 3.22 Bone volumes for BioOssTM, BioGranTM, AllogenixTM, and MP ______________________________ 67
Figure 3.23 Particle volumes for BioOssTM, BioGranTM, and MP ______________________________________ 67
Figure 3.24 Demineralized bone matrix area measurements __________________________________________ 68
Figure 7.1 µCT scans of calcium phosphate cements, OMP-, PANT-, and BAF-cements ____________________ 94
Figure 7.2 Threshold-based volumetric measurements of calcium phosphate cements ______________________ 95
Figure 7.3 SEM images of BioOssTM_____________________________________________________________ 96
Figure 7.4 Histological section of BioOssTM at 16 weeks post-operative (FW=5446µm) ____________________ 96
Figure 7.5 SEM images of BioGranTM ___________________________________________________________ 97
Figure 7.6 Histological section of BioGranTM at 16 weeks post-operative (FW=5446µm).___________________ 97
Figure 7.7 SEM images of AllogenixTM___________________________________________________________ 98
Figure 7.8 Histological section of AllogenixTM at 16 weeks post-operative (FW=5446µm). __________________ 98
vii

LIST OF TABLES
Table 3.1 Pore sizes of calcium phosphate cements _________________________________________________ 48
Table 3.2 Results from the quantitative Rietveld analysis of hand- and machine-made calcium phosphate cements (doped and undoped)_________________________________________________________________________ 53
viii

1
1. INTRODUCTION
1.A Endosseous peri-implant healing Bone is a mesoderm-derived vertebrate connective tissue that serves several functions.
The healing that occurs in a bony site is one of the most remarkable of all the body’s repair
processes, since it results, not in a scar, but in the actual regeneration of the tissue 1-3. This
process comprises a complex cascade of cellular and molecular events. After the injury-triggered
loss of tissue continuity, blood clots in the damaged tissue, leading to cytokines releases and to
an inflammatory response that favours angiogenesis and granulation tissue formation. This
fibrovascular stroma serves as a three dimensional matrix for osteogenic cell migration, which in
turn is responsible for bone formation, in other words, the “creation” of the original tissue 4.
Peri-implant healing in particular became the target of extensive investigations in the last
three decades, owing to the widespread use of dental implants 5. The course of endosseous
healing events differs significantly depending on circumstances such as the anatomical location
and severity of the trauma, as well as age and species 6. However, though it is known that these
events may occur simultaneously, this thesis emphasizes the following sequence: inflammation
and blood clotting, provisional connective tissue matrix creation, osteoconduction and bone
formation, and bone remodelling.
1.A.1 Inflammation and blood clotting
At the instant of injury (i.e., fracture, implant site preparation) the internal architecture of
the bone is interrupted, a trauma which leads to an alteration both in the vascularity and
mechanical properties of this connective tissue 7. Almost immediately following the trauma, an
inflammation phase begins and generally lasts from two to five days 8. The inflammatory
reaction is known to counteract the injurious agent and trigger a chain of events leading to the
healing of the implant site 9, 10. The disruption of the surrounding blood vessels causes
hemorrhage, which is followed by the release of adhesion mediators from endothelial cells.
These mediators, called Willebrand Factors (vWF), are responsible for the activation of platelets,
leading to cell shape rearrangement and the release of these cells’ storage granules’ contents
(degranulation). At this stage, activated platelets play a crucial role in peri-implant healing since
their degranulation will stimulate the proliferation and migration of distinct cell lineages, as well
as favour blood clot formation 4, 11. For instance, platelet-derived growth factor (PDGF) and
transforming-growth factor beta (TGF-β) have been proven to be both mitogenic for fibroblasts
and chemotactic factors for neutrophils, fibroblasts, osteogenic, and smooth muscle cells 6. In the

2adjacent tissue, coagulation factors convert prothrombin to thrombin, which in turn cleaves
fibrinopeptides to produce a fibrin framework that encloses the extravasated blood cells and
results in the formation of the hematoma or blood clot. The coagulated blood not only serves as a
reservoir of growth factors but also as a provisional scaffold in which osteogenic cells can
migrate 4.
1.A.2 Provisional connective tissue matrix creation
After the clotting, a new configuration of the injured tissue starts to evolve and the
intense cell activity begins transforming the hematoma into a temporary stroma for the upcoming
ossification. At this stage, hemostasis of the injured site is achieved by the co-incidence of
vasoconstriction of the interrupted ends of local blood vessels, limitation of blood access by the
constriction of local arterioles, blood coagulation, and clot retraction 12. Within the clot matrix,
macrophages, fibroblasts and new blood vessels are interdependent. Macrophages release growth
factors that stimulate the synthesis of extracellular matrix through fibroblasts, stroma which is
the support for cell and vascular growth, carrying nutrients to sustain cellular activity.
Eventually, this provisional matrix will be substituted by a collagen-rich matrix also synthesized
by fibroblasts. After seven to ten days, the transformation of some of the fibroblasts into
myofibroblasts creates contractile forces, which in turn results in wound contraction. This
contraction may represent an evolutionary means through which healing is accelerated by the
reduction of the wound’s size 6, 13.
Following hemostasis, the local lack of blood supply causes ischemia and necrosis. The
latter comprises a chain of feedback events and is a preamble to the recruitment of inflammatory
cells that will further degrade the blood plug. Specifically, clot demolition and cleaning is mainly
mediated by the phagocytic digestion exerted by neutrophils and macrophages which migrate
from the blood vasculature 6. Cytokines such as PDGF, TGF-β, platelet factor 4 (PF-4), tumor
necrosis factor alpha (TNF-α), and interleukin-1 (IL-1) are involved in the migration and passage
of phagocytic cells from the local vessels to the clot 14. At this point, the cellular activity is
greater in the core of the clot and oxygen demand exceeds supply. Therefore, the local pH is
lowered due to the increased anaerobic metabolism and becomes an important chemotactic factor
for endothelial and mesenchymal cells 15-17.
The local hypoxic environment is fundamental to the formation of new blood vessels in
the wound site (angiogenesis). Forming new blood vessels is crucial to maintaining high cellular
activity during bone regeneration because they supply oxygen, nutrients and a source for bone

3progenitor cells 18. This process is initiated predominantly in the post-capillary venules, where
endothelial cells migrate along the chemotactic gradient to form hollow capillary buds 16, 19, 20.
Mechanistically, venules and capillaries, which were initially constricted by the tissue trauma,
begin to dilate and become more permeable. Next, stimulated endothelial cells follow collagen
secretion by differentiated fibroblasts and lead to a new vascular sprouting towards the centre of
the clot or angiogenesis stimulus 14. The endothelial cells gradually divide and become tubular in
shape. When these tubular sprouts meet each other in the wound site, anastomoses are formed,
signing for blood flow to initiate in the newly created vasculature 21. The injured environment
now assumes a new configuration termed granulation tissue since the newly-formed vessels
appear as distinct granules when observed under light microscopy. The formation of granulation
tissue starts on approximately the fourth day and may last until the third week post-injury.
Finally, a provisional connective tissue matrix is established through the combined
fibroplasias and angiogenesis. The new vasculature mesh is supported by the constant activity of
fibroblasts which secrete collagen and proteoglycans while the vessels spread and anastomose.
Following the formation of the granulation tissue, osteogenic cells are stimulated and bone
deposition commences 18, 20.
1.A.3 Osteoconduction and bone formation
As described above, the signaling effects of soluble factors in the hematoma are of
considerable importance in osteogenesis. Certainly, new bone formation either on an old bone
surface or implant can only be observed after the recruitment and migration of osteogenic cells to
the endosseous healing site, a phenomenon called osteoconduction 6.
Osteoconduction is paramount to osteogenesis, not only in peri-implant healing, but also
during the normal bone remodelling events. It is composed of three main processes: (i) the
migration of bone progenitor cells through a transient matrix, (ii) the differentiation of the bone
progenitor cells, and (iii) the recruitment of functional differentiated cells to initiate the
formation of new bone 12.
During osteoconduction, pre-osteogenic cells are stimulated to migrate through a
provisional matrix, which could be represented by bone grafts, implants, or a blood clot. This
migration is dependent on the release of cell-derived soluble factors such as PDGF, TGF-β,
insulin-like growth factor (IGF) 22, and thrombin 23.

4The migrating cells then start a differentiation process that results in the secretion of the
new or de novo bone matrix. Having ceased their migration process, these cells are eventually
buried by the matrix they secrete and are called osteocytes since. Thus, for the bone formation
process to continue, new undifferentiated bone cells must be consistently engaged. In this matter,
osteoconduction becomes crucial for the continuous renewal of progenitor cells during the bony
tissue metabolism24, 25.
During the bone formation, differentiating osteogenic cells first secrete globular
accretions of a matrix devoid of collagen called cement line. These afibrillar layers are found at
the interface of secondary osteons with the surrounding tissue and may also be seen at the bone-
implant interface 26. This first laid layer provides nucleation sites for calcium phosphate nano-
crystals, which nucleate and grow within the organic matrix. After the deposition of the cement
line matrix, the osteogenic cells differentiate into mature secretory and fully functional cells,
namely osteoblasts, which elaborate the collagenous extracellular matrix assembled as fibers.
Finally, the collagenous fibers undergo calcification and are separated from the underlying
substratum by a calcified non-collagenous matrix 4, 27.
Osteogenesis in a peri-implant environment results from two distinct mechanisms:
Distance osteogenesis and Contact osteogenesis. The first occurs when bone matrix is deposited
from the host bone towards the implant surface, while the second occurs when bone matrix is
deposited from the implant surface to the host bone 16, 20, 28. Juxtaposition of bone to the implant
surface is a result of Distance and Contact osteogenesis concurrently.
Distance osteogenesis is triggered when micro-damage to the bone at the prepared site
occurs. In particular, reports from the literature show that despite optimal surgical technique,
approximately 1mm of compact bone adjacent to the osseous wound site undergoes necrosis
post-operatively 13, 29, a phenomenon also displayed in the fracture healing process.
Contact osteogenesis is a result of osteoconduction and bone formation, and occurs when
the first layer of bone is directly secreted onto the implant’s surface. Although both osteogenesis
processes occur simultaneously, contact osteogenesis is more likely to achieve favourable
results. After the deposited bone matures, the remodelling process assures the self-regeneration,
and adaptation to stress, of the bony tissue.

51.A.4 Bone remodelling
Bone remodelling is the process of bone resorption (osteoclastic activity) followed by
bone formation (osteoblastic activity) and is characterized by the changing of both the
dimensions and orientation of the bone matrix 20.
This process reflects the functional adaptation of the bone structure to load. Generally,
the remodelling pattern of the preexisting bone dictates the remodelling pattern that will develop
after implant insertion 16, 20. Thus, compact bone is replaced by compact bone and sparse
trabecular bone is replaced by sparse bony contacts 16. During the remodelling stages, several
cytokines, growth factors (IGFs, TGF-b1, FGF, BMP, EGF, PDGF, etc.) and hormones (PTH)
participate in cell proliferation at remodelling sites 20.
1.B Calcium phosphate cements Calcium phosphate cements were first described in the 1980s and are biomaterials
obtained from the mixture of equimolar amounts of calcium phosphate powders in aqueous
solutions at or below room temperature 30. They can be formulated in different shapes such as in
situ setting injectable cements, porous blocks, and particulate implants. In addition, they are
regarded as bone substitutes/fillers since the main end product of the reaction is hydroxyapatite,
a biocompatible calcium phosphate compound 31, 32.
Calcium phosphate cements are mouldable, injectable, bioresorbable, osteoconductive,
and serve as local delivery devices for active agents. They fit any defect size or shape right after
their fabrication process, an advantage in light of the limitations of prefabricated calcium
phosphate ceramics 33. These cements fulfill a structural role at the implant site and then, over
time, are degraded and replaced by bone during the bone remodelling process. They are also
osteoconductive, in that they provide a scaffold for bone ingrowth 34. Finally, their high surface
area not only offers a scaffold onto which bone matrix can be laid, but also increases their
capability as potent drug carriers 35. However, as with other bone biomaterials, the characteristics
of calcium phosphate cements are strictly related to their preparation methods. In this context,
the shape, size, surface area, porosity, pore size, biocompatibility, and biological reactivity of
these biomaterials may depend upon how their synthesis is conducted.

61.B.1 Preparation methods
Brown and Chow 36 developed the first formulation of calcium phosphate cements. Since
the main end product of their reaction is a hydroxyapatite synthesized at room temperature,
different formulations of these cements have been prepared and analyzed as potential grafting
materials which would overcome some of the disadvantages of ceramic hydroxyapatites 37.
Conventionally, calcium phosphate cements are prepared by the mixing of ground calcium
phosphate powders with a liquid phase, such as water, phosphate solution or even phosphoric
acid 33, 37-41. Dicalcium phosphate anhydrous (DCPA) and tetracalcium phosphate (TTCP) make
up the most widely used solid phase of these cements, while buffered phosphate solutions
account for the most common liquid phase.
Dicalcium phosphate (DCPA – CaHPO4) was first found as a soil mineral in the island of
Moneta in 1882 and, consequently, it is also known as monetite. This calcium phosphate is an
acidic compound and its solubility depends upon the solvent’s pH. However, it is less soluble in
water than tetracalcium phosphate. Tetracalcium phosphate (TTCP – Ca4(PO4)2O) or
hilgenstockite, the other solid reagent for the calcium phosphate cements’ reaction, was
discovered by G. Hilgenstock in 1883. It is a basic compound highly soluble in aqueous solution 42.
In the calcium phosphate cements’ preparation process, the reagent powders are first
ground using machinery, and then they are mixed with a liquid phase using a spatula or stirring
rod 33, 34, 36, 38, 40, 43-45. Generally, DCPA is ground in a non-aqueous medium to a particle size
range of 0.3 to 4µm, while TTCP is dry milled to a particle size of 1 to 10µm. To prevent water
uptake, the ground DCPA is dried at 80ºC until desiccated and subsequently mixed with ground
TTCP. The mixed calcium phosphate powders are then stored in a vacuum desiccator at 60ºC 37.
These milling procedures are thought to promote an improved reaction between the reagents and
aim for a controlled setting reaction 46 and the creation of better drug delivery systems 40, 47.
In summary, the hard cements are the result of equimolar amounts of the ground and pre-
mixed calcium phosphate powders mixed in an aqueous solution. The characteristics of these
cements vary according to the specific solid to liquid ratio of their component parts. In general,
the higher the solid to liquid ratio, the shorter the setting time, the higher the mechanical
properties, and the lower the porosity of calcium phosphate cements 40, 47.

71.B.2 Calcium phosphate cement reaction
The setting reaction between DCPA and TTCP in an aqueous environment depends on
the hydration rates of the acid and basic salts, followed by the neutralization of the by-products.
Since these salts present different solubility rates in different milieu, pH changes have a
substantial effect on the hydration of the reagents.
A simplified diagram of the DCPA/TTCP system for the calcium phosphate cements
setting reaction is shown below:
1) Hydration of the reagents:
CaHPO4(s) + H2O(l) Ca+2(aq) + HPO4-2
(aq)
Ca4(PO4)2O(s) + H2O(l) 4Ca+2(aq) + 2PO4-3 (aq) + 2OH- (aq)
2) Precipitation of the reacted species:
5Ca+2(aq) + 3PO4-3(aq) + OH-(aq) Ca5(PO4)3OH
In the same aqueous environment, TTCP dissolves faster than DCPA and the result is a
drastic increase in pH. At a basic pH, the dissolution of DCPA is accelerated and, even though
both reagents have their hydration process stimulated, crystallization into hydroxyapatite is only
attained when a supersaturation of the dissolved species occurs. At this point, the mixture’s pH
can be as high as 10.6. However, the dissolution of DCPA leads to a drop in pH and balances the
ion concentration in the solution, leaving the reaction in a steady state. This state is kept as long
as the rate of dissolution of DCPA and TTCP exceeds the rate of hydroxyapatite formation 46, 48.
Finally, the hardening of the cement results from the interlocking of hydroxyapatite crystals,
which creates an exquisite porous scaffold 47.
Clearly, the hydration of both TTCP and DCPA plays an important part in the hardening
of calcium phosphate cements. However, the rate-determining step for the above-described
reaction is the dissolution of DCPA, since it is the phosphate supplier for the formation of
hydroxyapatite 46, 49. Several strategies have thus been developed which aim the increase of the
dissolution of DCPA during the cements’ reaction. For instance, the use of small DCPA particles
mixed with large TTCP particles would increase the specific surface area of the DCPA,
accelerating its hydration. Another alternative, described by Liu et al. (2003), would be reducing
the particle size of TTCP, which would thus dissolve even faster, promoting a steeper increase in
pH and accelerating the dissolution of DCPA. Therefore, the particle size of DCPA and TTCP

8certainly has crucial effects on the properties of calcium phosphate cements 46. Other strategies
to tune the characteristics of calcium phosphate cements have also been attempted. For instance,
the decrease of the powder size and liquid to powder ratio, as well as the adding of calcium or
phosphate ions and apatite nanocrystals, would result in faster setting time. A decrease in the
liquid to powder ratio and the adding of reinforcing fibres, on the other hand, would decrease the
cements’ porosity and increase their mechanical properties 40.
Overall, the main end product of the calcium phosphate cements’ reaction is a
hydroxyapatite which has low crystallinity and exhibits greater similarity than ceramic apatites to
biological apatites 44, 46, 47. In addition, this hydroxyapatite has a porosity ranging from 30% to
50% with pores up to 10µm in size 47, thus offering the additional benefit of acting as drug
delivery systems.
1.B.3 Calcium phosphate cements as drug delivery systems (DDS)
DDS have been used clinically to dramatic effect in treating patients with diseases such
as diabetes and osteomyelitis 51-54. Though most drug delivery devices are polymers, some
inorganic materials are capable of acting as carriers for the treatment of skeletal disorders such as
bone tumors, osteoporosis, and osteomyelitis. Indeed, calcium phosphate cements may represent
valuable alternatives as delivery systems thanks to their bioactivity, increased surface area and
porosity, as well as their capacity to adsorb different chemical species 35, 43, 47, 55-59.
Different from calcium phosphate ceramics, which can only adsorb drugs onto their
surfaces, calcium phosphate cements can be fully saturated with active agents by adding the drug
to one of the two cement phases. However, when incorporated into the cements’ matrix, some
drug classes may change certain of these biomaterials’ physico-chemical and mechanical
properties. One great challenge is thus predicting the drug-cement in vivo behaviour based on in
vitro drug delivery studies. Moreover, as bioactive bone substitutes, calcium phosphate cements
are subjected to surface changes after implantation, which can alter the release profile of the drug 47.
The release profile of drugs from any carrier is dependent on factors such as
microstructure, drug solubility, type of drug-matrix bond, and the process of matrix degradation
(if any). In this context, calcium phosphate cements are generally described as diffusion-
controlled devices, where the drug diffuses from a non-biodegradable matrix. However, it is only
so because the rate of the cements’ degradation is generally much lower than the delivery rate of

9the drug. Drugs can be added to either the solid or the liquid phase of calcium phosphate cements
and, since hydroxyapatite is the main end product of the cements’ reaction, it is inferred that the
active agent is distributed in the porous mesh of interlocking apatitic crystals formed by the hard
cement. Scholars have tested different calcium phosphate cements’ formulations with several
drugs and attested that their release kinetics are not only dependent on the drug’s solubility, but
also directly related to the cements’ microstructural characteristics such as porosity and
tortuosity 47.
Implanted calcium phosphate cements serve as a means to target and deliver agents
locally to a site with the intention of accelerating and promoting desired biological responses. As
local delivery devices, they have the advantages of sustaining the release, whilst minimizing the
concentrations of the drug in the bloodstream and other organs; and the reduction of potential
side effects produced by systemic administration 60. These biomaterials have been adapted to act
as delivery devices for an array of pharmacological agents, cytokines and growth factors 55.
Certain pharmacological agents were highly soluble and released quickly when
incorporated into the cements’ matrix. Bohner et al. (1997) prepared gentamicin-doped calcium
phosphate cements and found a high antibiotic release rate within 7 days of implantation.
Attempting to decrease of the drug delivery rate, the authors combined polyacrylic acid (PAA) to
the drug-doped cement 35. Similarly, other authors have used sodium alginate and polymers such
as chitosan to retard drug liberation 60, 61. Different from soluble antibiotics, growth factors have
shown a delayed release from calcium phosphate cements. This fact may be caused by the
affinity of these polypeptides to calcium phosphates, which may have trapped them inside the
cements’ matrix 47.
Pharmacological agents that stimulate reparative bone formation have also been
incorporated into calcium phosphate cements. Among them, transforming growth factor beta
(TGF-β), a polypeptide involved in bone regeneration, was combined with these biomaterials and
implanted using different animal models. Both an increased local bone mass and a stimulated
resorption of the growth factor-doped cements were observed 62, 63. However, it was the loading
of the macrolide antibiotic Bafilomycin to calcium phosphate cements which led not only to a
massive peri-implant bone formation, but also to a controlled resorption of the implants 64.
As described in this section, several factors interfere with the incorporation of drugs into
the calcium phosphate cements’ matrix. To assess the performance of these compounds, it is first
necessary to evaluate whether the addition of the active agent (irrespective of the phase in which

10it is added) alters the setting reaction, subsequently changing the properties of the cements. Next,
an in vitro release kinetics study must be conducted followed by an in vivo analysis of the
effectiveness of implanted drug-cements. Finally, a translation of the above-mentioned assays to
the clinical reality must be targeted 47.
1.B.4 In vivo behaviour of calcium phosphate cements
Biocompatibility, osteoconductivity, and bioresorbability are all features of calcium
phosphate cements that make them attractive bone substitute candidates. Specifically, since the
main product of the cements’ reaction is a hydroxyapatite which mimics the inorganic phase of
bone and teeth, they are not recognized as foreign materials by the host 31, 48. Moreover, when
compared to calcium phosphate ceramics in particulate or lithomorph shapes, calcium phosphate
cements offer the advantages of: (i) being injectable and able to harden in vivo, (ii) fitting
implant beds of various shapes, (iii) forming a complex scaffold with interconnected micropores,
and (iv) being capable of carrying a wide variety of active agents 47.
However, the pore sizes of calcium phosphate cements range from a nanoscale to 10µm
with limited interconnectivity while natural bone has a highly interconnected macropore
structure with pores sizes from 100 to 400µm. Therefore, cellular invasion through the cements’
scaffold is constrained and cell-implant interaction is restricted to their surface 32.
One strategy for incorporating macropores into the matrix of calcium phosphate cements
is to add large polyssacharides to their chemical reaction. After the cements are hardened, they
are soaked in an aqueous solution to dissolve the polyssacharides which leaves large,
interconnected voids within the cements’ structure 48. Another alternative could be the forcing of
gas flux to calcium phosphate cements while they are setting. The gas flux would create bubbles
within the cement and these bubbles would be trapped in the biomaterial’s scaffold after their
hardening 65. Although intended to improve the in vivo performance of the calcium phosphate
cements, these techniques also aggravate one of these biomaterials’ key limitations: their low
mechanical properties 48. As a result of these properties, these biomaterials have essentially been
used in sites that do not bear loads 66. To decrease their brittleness, reinforcing fibres and
polymers were added to these cements’ matrix as a part of a periodontal disease model, yielding
promising results 44.
Calcium phosphate cements used in skeletal defects in different animal models have
shown the absence of a fibrous capsule and direct bone deposition onto the cements’ surface 67,

1168. Indeed, the application of implanted calcium phosphate cements loaded with osteogenic
inducers has shown encouraging results. Injectable calcium phosphate cement pastes carrying
recombinant human bone morphogenetic protein 2 (rhBMP-2) displayed accelerated bone
healing in canine and non-human primate osteotomy studies 69, 70. In a model using rat femora, a
faster fracture consolidation was also reported, following the use of a ß–tricalcium phosphate-
calcium phosphate cement loaded with rhBMP-2 71.
One of the most appealing characteristics of calcium phosphate cements is their
resorbability in vivo. Upon implantation, these cements act as osteoconductive scaffolds but, in
time, degrade and are replaced by bone during the remodelling process 31, 72. The products of the
cements’ degradation are Ca+2 and PO4-3 ions, which are easily excreted or recycled by the body.
The degradation of calcium phosphate cements occurs by the combination of two
processes: dissolution in the in vivo fluidic environment and cell-mediated resorption mainly by
osteoclasts. The in vivo dissolution of these biomaterials is strictly related to their composition
and particle size 32. Nevertheless, apatitic cements are generally degraded through osteoclastic
activity. In this resorption process, osteoclasts gradually degrade calcium phosphate cements
from their surface to their core 47. Cell-mediated resorption is advantageous since it mimics the
natural process of bone turn-over, in which osteoclasts resorb bone and osteoblasts subsequently
secrete bone matrix 67, 68.
A variety of characteristics may influence bone substitution. Among them are: the age,
sex, and general metabolic health of the host, as well as the particle size, porosity, chemical
composition, crystallinity, and powder to liquid ratio of the cement. Taking these variables into
consideration, the complete resorption and substitution of calcium phosphate cements may take
from 3 to 36 months. Additional studies are needed in order to describe the degradability of these
materials in clinical models 37.
Indeed, a major concern is related to the absence of controls over the implanted cements’
degradation rate. Ideally, the implant should stay un-resorbed to perform its osteoconductive role
until a stable tissue from the host is able to take over. However, some preparations of calcium
phosphate cements resorb at too great a rate to stabilize the implant bed, whilst other
formulations take too long to be resorbed and restrain the biological function. Several techniques
have been employed to control the degradation of these biomaterials but with restricted success.
Promising outcomes were generated when Bafilomycin A1 was incorporated to implanted

12calcium phosphate cements, which significantly decreased the resorption rate of the cements and
promoted a large deposition of peri-implant bone 64.
Overall, the number of in vivo studies is still low, and most of them have been performed
in small animals, with the intrinsic limitations for results extrapolation to humans 57.
1.C The effect of gastric proton pump inhibitors (PPI) on osteoclastic resorption
1.C.1 Osteoclastic differentiation and acidic secretion through ion pumps
Before bone resorption starts, osteoblasts play an important role in osteoclastic
differentiation and activation. For instance, the bone-forming cells express a membrane-bound
ligand called receptor activator of nuclear factor κ B ligand (RANKL), which is recognized and
bound by an osteoclastic receptor, the receptor activator of nuclear factor κ B (RANK) 73. This
coupling activates a concatenation of intracellular events that promote osteoclast activation.
Once bound, RANK’s cytoplasmic domain recruits a TNF receptor associated factor–6 (TRAF6) 74, which serves as a promoter for transcription factors to upregulate osteoclastic activation genes 75. These transcription factors, namely nuclear factor κ B (NFκB) and activator protein-1 (AP1),
migrate to the nucleus and stimulate the expression of genes required for resorption activity, such
as cathepsin K, tartrate resistant acid phosphatase (TRAP), and integrin β3 74. As a regulatory
mechanism to prevent osteoclastic overstimulation, osteoblasts also express a soluble factor,
called osteoprotegerin (OPG), which limits the binding between RANK and RANKL 76, 77.
Activated osteoclasts have distinct but related metabolic mechanisms to resorb both the
inorganic and organic phase of bone. Bone resorption is initiated when osteoclasts create an
acidic environment by secreting protons through vacuolar proton pumps (V-ATPases). Once on
the surface of the bone, osteoclasts form a sealed micro-environment between their apical
membrane and the surface. After the establishment of this sealed microenvironment, or
“resorption pit”, vacuoles in the osteoclast cytoplasm migrate and fuse to the apical membrane.
These osteoclast vacuoles store pro-proteolytic enzymes as well as integral pumps. The fusion of
these vacuoles releases pro-proteolytic enzymes into the resorption pit and inserts the integral
pumps into the membrane. During this process, the surface area of the membrane increases and
is referred to as the ruffled border 78.
A member of the V-Type proton-ATPase pump (H+ATPase) class is one of the key
integral pumps inserted into the ruffled border. This H+ATPase pump depends upon energy to
expel protons from the cytoplasm into the resorption pit. Mechanistically, the reaction between

13CO2 and H2O is catalyzed by a cytosolic carbonic anhydrase and produces H2CO3. H2CO3 is then
dissociated into HCO3- and protons which exit into the resorption pit. The release of these
protons lowers the pH to the extent that hydroxyapatite becomes soluble. This acidic
environment also activates pro-proteolytic enzymes like cathepsin K and TRAP (tartrate-resistant
acid phosphatase), enzymes which will cleave the underlying collagen matrix 58, 79. Additionally,
an electrical gradient is created as the protons are delivered into the resorption pit. As a result,
Cl- diffuses freely along its specific ion channels in the ruffled border in an attempt to balance
the electrical gradient. Through these diverse strategies, osteoclasts resorb the inorganic and
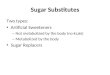
organic phases of bone (Figure 1.1) 78.
HCO3-
Figure(CAII)througCl- ioncombinis solu
HCO3- H++
Ca2+Ca2+
Ca2+
Ca2+
Cl-
ATP ADP + PATP ADP + PH+
CAIICAII
H
CO2 + H2O
Cl-
NucleusNucleus
NucleusNucleusNucleusNucleus
IntegrinsIntegrins
Cll
Bone/Implant
HC
1.1 Intracellular events in osteoclastic resorption. Cytoplasmic carbonic anhydrase II converts H2O and CO2 into HCO3
- and H+. Next, hydrogen ions are expelled from the cell h proton pumps in the ruffled border whereas HCO3
- ions are exchanged by extracellular s. The Cl- ions diffuse freely along their specific ion channels in the ruffled border and e with H+ in the resorption pit, which creates an acidic pH, at which point hydroxyapatite
ble.

141.C.2 Osteoclastic H+ATPase proton pump as a pharmacological target
It is evident that the acidification process is only attained through the combined activity
of several ion pumps and channels. Within these structures, the osteoclastic H+ATPase has the
critical role of translocating protons and has been the target of several active agents aimed at the
inhibition of bone resorption.
Proton translocating V-ATPases are the major electronic pumps of vacuolar membranes
and are ubiquitous components of eukaryotic organisms. In humans, H+-ATPases were first
identified in the stomach as being responsible for the acidification of the gastric lumen. Later,
H+-ATPases were identified in several locations within the gastrointestinal system from the
esophagus 80 to the colon 81, skin, brain, lung, kidney 82, prostate 83, placenta 84 and bone 85.
Given the ubiquitous nature these pumps, the major therapeutic challenge concerning V-
ATPase inhibitors is to develop agents that discriminate between the osteoclastic enzyme and the
other essential V-ATPases. The discovery of novel and selective inhibitors of the osteoclastic V-
ATPases has been restrained by the high complexity and the incomplete structural knowledge of
the pump 58.
Nevertheless, several agents that inhibit the activity of the H+-ATPase have been
identified. Among them, Bafilomycin and Concanamycin have been employed to inhibit the H+-
ATPase on osteoclasts with potencies in the nanomolar range 86. These drugs are isolated from
the fermentation of Streptomyces spp and belong to the macrolide antibiotics class. Bafilomycin
A1 and Concanamycins are characterized by the presence of a vinylic methoxy at position 2 and
by a long side chain bearing a hemiketalic ring 58. Bafilomycin A1 binds tightly to one or more
subunits in the transmembrane Vo domain of the enzyme complex and exerts its inhibitory
effect. However, this therapeutic agent does not produce any covalent modification.
Consequently, the biochemistry and the physiological roles of V-ATPases have been widely
studied through the use of Bafilomycin A1 58, 87.
Initially, Bafilomycin and Concanamycin were considered specific osteoclast inhibitors.
However, it was subsequently discovered that Bafilomycin inhibited H+-ATPase activity in
membrane vesicles of bone and kidney 88. Furthermore, Bafilomycin and Concanamycin were
also discovered to inhibit other ATPase pump classes with potencies in the micromolar range 86,
88. As a result of this non-specific characteristic, neither Bafilomycin nor Concanamycin can be
applied systemically in human settings as osteoclast inhibitors, since their administration in

15animals has caused inhibition of essential V-ATPases, leading to the systemic alteration of
cellular physiology and high toxicity 58. For these reasons, Bafilomycin and Concanamycin are
not Food and Drug Administration (FDA) regulated drugs.
The above-cited studies yielded encouraging evidence to indicate that acid pumps
isolated from different tissues could have different pharmacological properties. This opened the
way to novel and effective inhibitors of bone resorption lacking unwanted side effects. It has
been suggested that the osteoclast V-ATPase could potentially be useful as an anti-osteoporotic
agent 58.
A class of substituted benzimidazoles known as Proton Pump Inhibitors (PPI) was proven
to inhibit the activity of H+K+-ATPases. Examples of these drugs are Omeprazole and
Pantoprazole, which are employed clinically in the treatment of gastroesophageal reflux disorder
(GERD) 78, 89. Although the mechanisms of acid secretion for osteoclasts and gastric parietal
cells differ, PPIs were considered potential means of controlling bone resorption. Indeed,
Omeprazole-like inhibitors were shown to bind a cysteine residue in the catalytic subunit of the
V-ATPases, inhibiting proton transport of membrane vesicles in osteoclast and kidney cultures in
vitro 58. In addition, after implantation in rat femora, Pantoprazole-loaded calcium phosphate
cements inhibited the osteoclastic resorption without interfering in the peri-implant bone
resorption rate 78.
Pantoprazole, specifically, has been proposed for the treatment of acid-related disorders 89, 90. Though it has the same inner structure as other PPIs 89, its binding to H+K+-ATPases
appears to be more specific 91. In spite of its irreversible proton pump inhibition 90, 92,
Pantoprazole is apparently well tolerated and 89-92 offers the advantage of minimal drug
interaction risk 90-92. The duration of its effects depends on the rate of proton pump regeneration
and not on the duration of drug circulation in the body 89. Therefore, it may be of clinical benefit
to patients taking other drugs 91. An inactive state of the drug is administered, which at the low
pH quickly becomes an active unstable intermediate. In this active state, the drug binds to free
thiol groups present on the luminal side of the catalytic α-subunit of the H+K+-ATPase 78,
preventing the exit of protons into the resorption pit. Moreover, Pantoprazole has been
successfully employed as an osteoclast inhibitor when administered in vitro 93.Therefore,
evidence of both in vivo and in vitro experimentation has shown the potential of PPI drugs as
anti-resorptive agents.

161.C.3 Mechanism of action of Pantoprazole
Gastric parietal cells use H+K+-ATPases to secrete H+ in exchange for K+. The electrical
potential generated by the exertion of H+ favours the diffusion of Cl- anions into the lumen
through membrane channels. In addition, K+ is transported along with its chemical gradient from
the cytoplasm back to the lumen by cationic channels, replenishing the extracellular K+ source.
This series of events acidifies the stomach lumen to a pH as low as 1-2 94.
Like other PPI drugs, Pantoprazole is a substituted 2-pyridyl methylsulfinyl
benzimidazole with a backbone structure and a methylsulfinyl link, which is the region
responsible for their inhibitory action 94. Upon administration, Pantoprazole irreversibly binds
and inhibits the H+K+-ATPase on the apical membrane of parietal cells. As described above,
Pantoprazole is an inactive pro-drug which turns into an unstable active agent in low pH. This
transformation is the result of a two-step protonation, after which Pantoprazole becomes a
reactive cationic sulfenamide. This sulfenamide is able to bind to luminal free cysteine residues
on the side-chain of the gastric H+K+-ATPase creating a disulfide bridge between the drug and
the proton pump 95.
The H+K+-ATPase cysteine residues contain thiol groups that result from the oxidation of
the enzyme’s catalytic α-subunit 94 and reside in K+ binding regions. The bridging between
Pantoprazole and the H+K+-ATPase blocks the binding of K+ to its target on the proton pump,
impeding the shifting of the protein to different configurations. Once the pump is arrested in a
static position, the proton translocation across the membrane is irreversibly inhibited and the
acidification of the extracellular environment is prevented 95. As a consequence, the only way for
the parietal cells to recover their function is to synthesize new H+K+-ATPases. In order to
renovate their proton pumps, the cells have to take up and degrade the non-functional proteins as
well as synthesize and incorporate sound pumps into their membrane. Pantoprazole does not alter
these cellular processes and the activity of the drug is kept until the cells are able to recycle their
proton pumps 96, 97.
1.D Bone substitutes Finding a suitable bone substitute has been the target of several studies for more than a
century. In the past, bone defects were usually allowed to heal through their filling with blood
clot. However, bone grafting techniques began to be adopted to stimulate bone healing and, in
1889, the use of a muriatic acid-decalcified ox bone to fill skeletal defects caused by tumor

17removal or osteomyelitis was first reported 98, 99. Today, autogenous grafts are the “gold
standard” 31, 100, 101 for bone replacement procedures since they have all three elements of an
“ideal” bone substitute: osteoconductivity, osteoinductivity, and osteogenic cells 102, 103.
However, autografts also have disadvantages such as morbity of the donor site, prolonged pain,
risk of infection, graft availability, and cosmetic defects 31, 104-107.
Considerable focus has thus been placed on the development of new alternatives to
autografts. Ideally, synthetic bone substitutes should be biocompatible, osteoconductive,
osteoinductive, bioresorbable, structurally similar to bone, remodelled during bone turnover,
easy to use and cost-effective, and promote minimal fibrotic reaction 99, 102, 108. Also, synthetic
bone grafts should not involve undue pain or fracture, excessive blood loss, the transmission of
disease, immunogenic response, or cosmetic defects 99. As a result, a wide range of biomaterials
is currently available (e.g. calcium phosphate ceramics [CaPC], bioactive glasses [BAG],
anorganic bone [AB], demineralized bone matrix [DBM]).
1.D.1 Autogenous grafts
Since it was initially hypothesized that periosteum supported osteogenesis, it was
believed that autografts remained “alive” when grafted and their periosteum was necessary for
osteogenesis. Subsequently, different types of bone were shown to have varying osteogenic
potential, with cancellous iliac bone containing the highest and cortical bone the lowest
osteogenic capacity 99.
Although autografts and xenografts carry antigenic factors which may cause an
immunogenic response, the former are known to be highly biocompatible. Upon implantation,
autogenous bone is resorbed and substituted by a stable host tissue through angiogenesis and the
recruitment of mesenchymal cells 99. However, some cases have been reported which show
resorption of autografts without subsequent bone formation, resulting in gaps within the material.
In such cases, the gaps would have acted as stress points, increasing the risk of fractures and/or
deformities, needing more surgical intervention 109, 110. Indeed, in some cases autograft
disadvantages outweight the advantages. The harvesting of autologous bone grafts, which can be
retrieved from sites such as ilium, rib, fibula, or tibia, always requires extra surgery, and thus
additional morbidity. For instance, complications including pelvic instability, fatigue, fracture,
and iliac fistula were observed in individuals having undergone bone harvesting from the iliac
crest. A 20-year survey on 118 autografts harvested from the iliac crest, Cockin et al. (1971)
reported minor and major post-operative complications. Harvest site pain, hypersensitivity, and

18buttocks anesthesia represented the minor post-operative complaints and accounted for 6% of the
patients. Major complaints such as herniation, subluxation of the hip, or paresthesia were found
in 3 to 4% of the patients 111. Another study with records of 239 grafting patients noted a major
complication rate of 8.6% and a minor complication rate of 20.6% 112. Harvesting autologous
bone from the iliac crest has been shown not only to increase the operative time, but also to
result in residual pain and cosmetic problems. These prolonged surgical procedures are usually
associated with other complications such as hematoma, blood loss, infection, arterial and ureteral
injuries, and chronic pain 102. In fact, post-operative pain lasting up to three months was recorded
in 15% of patients subjected to iliac crest harvesting and the reported discomfort was believed to
be proportional to the invasiveness of the surgical procedure 108.
1.D.2 Calcium phosphate ceramics
Due to their chemical composition, calcium phosphate compounds are ideal when it
comes to biocompatibility 41, 113-115. Their utility in bone-bonding may, for example, improve
cementless fixation of orthopaedic prostheses 116. Because of their poor fatigue behaviour,
however, they should not be subjected to loads 117.
Tricalcium phosphate (TCP) and hydroxyapatite (HA) ceramics have different chemical
and structural compositions. These ceramics are calcium phosphate materials sintered at very
high temperatures (between 700 and 1300°C) to form a highly crystalline structure 108, 118, 119. Of
these ceramics, it is HA which better approximates to the chemical composition of bone 115. In
addition, HA has been characterized as a bioactive (bone bonding) but non-biodegradable bone
replacement material.
These materials have shown great biocompatibility and direct bone to implant contact,
but still display problematic brittleness 108. The resorption of ceramic hydroxyapatite is believed
to be slow (1 to 2% per year) and a result of surface macrophage attack, which creates a
roughened surface and forms an apatitic layer similar to the biological apatite. The new surface
then serves as a substrate onto which bone is deposited. However, these dense materials are too
brittle and degrade too slowly to be considered for orthopedic procedures.
Ceramic or non-ceramic hydroxyapatites are available in porous or solid, block or
granule form 108. The use of block forms of porous HA to reconstruct mandibular ridges has
involved a high degree of failure and although the use of granular HA has been suggested, this

19material still presents problems because of its relative insolubility. Conversely, particulate HA
used in dental and craniomaxillofacial applications have shown biocompatibility, absence of
antigenic response, availability, and low infection risk. These materials also yielded favourable
results when used as graft extenders for autogenous bone. However, besides their insolubility,
some additional complications included erosion, particulate migration, and overfill 99, 108. Owing
to their lack of resorption and particulate migration, HA ceramics are not broadly used for
orthopedic situations. On the other hand, several coatings with these ceramics have been used to
enhance early stabilization of metallic orthopedic implants. In addition, rough and smooth
surface polymers coated with HA were tested in vivo. It was reported that smooth coating
allowed bone attachment to exposed particulate HA only, whereas for the rough HA coating a
mechanical interdigitation between bone and the material was found 99.
Tricalcium phosphate ceramics are preferred as biodegradable bone replacements 120,
although their degradation is through rapid dissolution rather than osteoclast resorption. Thus,
TCP ceramics exhibit an overly fast biodegradation rate when used to promote alveolar ridge
augmentation, and in an attempt to slow this biodegradation rate, composites consisting of HA
and TCP (biphasic calcium phosphates – BCP) have been elaborated 121. Manipulating the
TCP:HA ratio provides a means of influencing the biodegradation rate. Therefore, ceramics with
higher amounts of TCP presented greater biodegradation. Accordingly, Lee et al. (1988), showed
that some commercially available BCPs with a higher TCP quantity dissolved more rapidly in
vitro 122.
Materials and interfacial factors may influence biodegradation. Material aspects include
particle size, TCP to HA ratio 41, 122, 123 and conditions of HA or TCP synthesis; while interfacial
factors comprise the composition of grain boundaries, stability when subjected to body fluid, and
porosity of surface. Increased density and high crystallinity also lead to dissolution resistance
and long-lasting stability. In contrast, interface activity and bone ingrowth are enhanced by
ultrastructure complexity and porous formation 115.
Overall, calcium phosphate ceramics present a similar composition to bone and possess
the advantages of being bone-bonding and biocompatible. However, HA ceramic particles
present a very slow resorption rate in vivo whereas particles of TCP show a fast biodegradation
rate.

201.D.3 Bioactive glass
First developed in the 1970s, bioactive glasses consist of sodium oxide, calcium oxide,
phosphorus pentoxide and silicon dioxide (silicate). The resorbability of these materials can be
tailored according to the proportions of their constituents, solubility being increased with the
increase of sodium oxide content. When a bioactive glass is exposed to an aqueous environment,
a silica-rich gel layer is formed, on which calcium and phosphate ions interact to form
hydroxyapatite 102, 108, 124. Bioglass does not trigger an immunogenic response 125 and it is known
to be non-cytotoxic 126-129.
Upon implantation, bioglass granules are modified by the ionic exchange with the
implanted site fluid 129, a modification which leads to further protein adsorption on the surface of
the material 130, 131. This protein adsorption is essential for the biocompatibility of the biomaterial
and, consequently, for bone deposition onto the surface of the implant 129. In spite of the bonding
properties of bioactive glasses, inherent limited mechanical properties restrict them to alveolar
ridge augmentation and non-weight-bearing sites 99. Mechanical strength is higher for pre-
fabricated bioglass implants than for ceramic HA. Thus, the presence of these bioglass blocks
may hinder further drilling and shaping which may result in fracture 99, 102, 108.
A known and widely used commercial bioglass (BioGranTM) is resorbable 132 and has
irregular particles with a 90 to 355µm size range 127, 131-133. The bioactive glass calcium
phosphate layer was shown to be osteoclastic-resorbed while cracks on the granules’ surface
favour in situ dissolution of the silica-gel core 106, 134. Nevertheless, particles of this material
were found in the implantation site as long as 12 months after implantation 106. Therefore, there
is a concern related to the resorption time-frame and density of these materials for clinical
applications.
1.D.4 Anorganic bone
Anorganic bone is a biocompatible synthetic biomaterial generated from the treatment of
bovine bone. The material is subjected to a strong alkaline solution and a subsequent heating at
300ºC which aims to remove its organic contents 135.
BioOssTM (anorganic bone, Geistlich Biomaterials, Wolhusen, Switzerland) is a well-
known bone substitute product in the dental field. It has been commonly used in a particulate
shape for void filling applications and alveolar ridge augmentation 136-139. Clinically, this
particulate material is tightly packed into the implantation bed to serve as a framework onto

21which bone matrix is then laid 137, 138, 140. However, upon compression the interconnectivity
within the particulate material decreases, limiting the space available for the occurrence of
angiogenesis.
Several authors have shown that BioOssTM provides a scaffold for new bone formation
and may be removed from the recipient site by the process of bone remodelling 101, 136, 140-144.
However, although BioOssTM reportedly has properties such as micro/macroporosity and
osteoconductivity, its resorption rate in vivo is still controversial. Thus, in the case of the material
staying un-resorbed for an extended period, the increased particle to bone ratio would be liable to
create micro-fracture-inducing stress-points within the bone 136-138, 140, 144. Indeed, orthodontic
movement experiments have revealed that sites filled with BioOssTM were favourable for tooth
movement after 12 months 136. Others have demonstrated that the degradation of this anorganic
bovine bone takes as long as 3-4 years after implantation 137-139, 145.
Overall, anorganic bovine bone is known to be osteoconductive and has been widely used
in the dental field to fill bone defects. It is believed to undergo resorption and be replaced in the
course of the bone remodelling process. However, in spite of BioOssTM’s broad use, its resorption
rate in vivo is still very slow, which could hinder site preparation for future metallic implant
placement and contact osteogenesis.
1.D.5 Demineralized bone matrix
As reviewed by Van de Putte and Urist (1965), the use of different formulations of
demineralized bone matrix (DBM) as osteogenic inducers dates back to the late 19th century 146.
However, owing to the different preparation protocols and models used, a great variety of results
were reported 99.
Today, DBM is obtained from the acidic treatment (generally with HCl) of a donor
cortical bone followed by its sterilization through gamma radiation (less than 1.5 MRad) at 60ºC.
The remnant of this treatment includes osteoinductive growth factors, non-collagenous proteins
and collagen type I. Among them, the osteoinductive growth factors, particularly bone
morphogenetic proteins (BMPs), are considered responsible for mesenchymal cell recruitment
and differentiation in vivo 100, 102, 104, 147. Nevertheless, the concentration of these osteoinductive
factors in DBM is believed to be very low 104.
Clinically, DBM is available as a freeze-dried powder, crushed granules or chips, flexible
strips, gel, malleable putty or paste. These materials have low mechanical properties and are

22most useful in mechanically stable sites. They have been applied with satisfactory results in
large, contained, stable skeletal defects and mainly as a graft extender for autogenous bone rather
than as a bone substitute 100, 102.
One disadvantage of DBM is its tendency to yield greatly variable osteoinductive results 129, 148. Although many immunological, chemical, and osteoinductive tests are still conducted
with DBM, many of these bone matrices have not been examined in clinically relevant animal
models, partly because this is not an FDA requirement. Despite this lack of data, DBM has been
used to improve spine fusion, graft non-unions, lesions in joint implants, and treatment of benign
cysts 147.

231.E Rationale
Calcium phosphate materials can be used in the repair of bony and periodontal defects, in
alveolar ridge augmentation, in maxillofacial reconstruction, and as bone-filling agents 40, 149. In
this context, calcium phosphate cements are made by the reaction of one or more calcium
phosphate compounds in a liquid phase to form HA, resulting in a self-hardening material that
sets at or below physiological temperatures. Therefore, these materials represent a potentially
valuable alternative as bone substitutes/fillers 34, 35, 36, 38, 40, 43, 149. Experiments from the Bone
Interface Group have reported varied percentages of HA conversion, which is possibly related to
the preparation process and/or the drug incorporated into the cements’ matrix (section 3.B.1.1).
Upon in vivo implantation, calcium phosphate cements are osteoconductive 34 and
biologically resorbable 31, 34, 47, 57, 72. However, they dissolve at a fast rate in physiological
conditions, which limits their functionality in vivo. New perspectives regarding the resorbability
of these materials have arisen with a new synthesis method for amorphous calcium phosphates
via milling, which may synthesize calcium phosphate granules and porous blocks with very high
surface areas. These obtained materials are potentially very biologically reactive 31, 35, 40, 43, 44, 46,
47, 57. In particular, calcium phosphate cements serve as a means of targeting and delivering
agents locally to a site with the intention of accelerating and promoting desired biological
responses. These cements have been adapted to act as DDS for an array of pharmacological
agents, cytokines and growth factors 35, 43, 47, 55-59. Drug-loaded calcium phosphate cements have
demonstrated less resorption and increased reparative bone formation compared to undoped
cements three weeks after implantation (section 3.B.4.1). Thus, PPI-loaded cements
demonstrated not only inherent biocompatibility and osteoconductivity, but also the ability to
retard bone resorption through a drug delivery mechanism which tuned their degradation rate as
closely as possible to that of natural bone turnover.
The main purpose of this work is, therefore, to standardize the preparation methods of
calcium phosphate cements, both in their mechanical preparation and in their loading with
Pantoprazole, in order to extend their functional longevity in situ while allowing resorption
throughout the course of bone remodelling process.

241.F Hypothesis
That when Pantoprazole is incorporated into the matrix of machine-activated calcium
phosphate cements, the in vivo lifespan of these biomaterials is extended, allowing them to be
resorbed and replaced by new bone during the bone remodelling process.
1.G Objectives To standardize the preparation methods of calcium phosphate cements, both in their
mechanical preparation and in their loading with Pantoprazole, in order to extend their functional
longevity in situ while allowing resorption throughout the course of bone remodelling process
by:
a) Assessing and comparing, through a threshold analysis of SEM images, the
particle size distribution, total surface area, porosity, and pore size of hand- and machine-made
calcium phosphate cements (H and M);
b) Identifying and quantifying, through powder x-ray diffraction analysis, the end
products of H and M, with and without Pantoprazole (HP and MP);
c) Describing, through calcium trace element analysis using Atomic Absorption
Spectroscopy (AAS), the dissolution profiles of H and M in solutions at three different pHs (5.0,
6.4, and 7.4). In addition, the dissolution profiles of H, M, HP, and MP in saline at pH 7.4 were
also assessed;
d) Describing, through UV absorbance analysis using spectrophotometry, the in vitro
release of Pantoprazole from particulate HP and MP in saline at pH 7.4;
e) Quantifying, through MicroCT evaluation, the reparative bone formation and
particulate degradation of H, M, MP, BioOssTM, BioGranTM, and AllogenixTM (DBM) in rat
femora defects after several intervals.

25
2. MATERIALS AND METHODS
2.A Preparation of particulate calcium phosphate cement Traditional calcium phosphate cements have been developed as injectable materials
which set in vivo. However, in the present work these cements were formulated in a particulate
shape and used as bone substitutes. The cements were obtained from an equimolar (0.0005mol)
mixture of two calcium phosphate powders with a phosphate solution, with a powder to liquid
ratio (P/L) fixed at 2.0 78. The chosen powder reagents were dicalcium phosphate anhydrous
(CaHPO4 - DCPA) and tetracalcium phosphate (Ca4(PO4)2O - TTCP) while the liquid phase was
a 0.2M solution of Na2HPO4 and NaH2PO4 in a 4:1 ratio (vol/vol). In addition, the proton pump
inhibitor Pantoprazole was incorporated into calcium phosphate cements as an attempt to control
their biological resorption. It was believed that, as the cements are resorbed and the incorporated
PPI is delivered, the osteoclastic resorption would be frustrated and the implanted particulate
would present a delayed degradation rate. A summarized description for the preparation of hand-
and machine-made cements, with and without Pantoprazole is shown in figure 2.1.
Hard cements
DCPA CaHPO4
Pantoprazole
TTCP Ca4(PO4)2O
HPO4-
OH-Ca2+ 4Ca2+2PO43-
Phosphate solution
Ca5(PO4)3OHPantoprazole
24h 37º C
100% hum.
5% CO2
H / M
HM / MM
Particulate cements 90-355µm
Figure 2.1 Preparation methods of hand- and machine-made cements. Calcium phosphate powders, with or without Pantoprazole, were mixed in a phosphate solution. The resultant compound was then mixed either using a spatula (H) or the Mixer Mill 301 (M), and allowed to set for 24 hours in the incubator. Finally, the set cements were crushed, either with a pestle and mortar (H or M) or with the Mixer Mill 301 (HM or MM), into a particulate material which was sieved to a particle size range of 90-355µm.

262.A.1 Grinding of the reagents
Prior to the preparation of hand- and machine-made calcium phosphate cements, the
DCPA and TTCP powders were ground with the objective of obtaining more reactive cements. A
99.0% pure DCPA powder (Sigma, St. Louis, MO) was weighed and wet-ground with 100%
ethanol using a Mixer Mill machine (MM301, Retsch, Burlington, ON). Thus, 5g of DCPA and
5ml of 100% ethanol were put in a 45mL zirconium oxide jar with a 20mm zirconium oxide ball
(Figure 2.2). The system was then subjected to a vibrational frequency of 30 revolutions per
second for 25 minutes. In order to promote ethanol evaporation, the resultant paste was allowed
to dry for 24 hours in a fume hood and the dried powder, with a final particle size range of 0.6-
20µm, was stored in a desiccator at 60ºC. TTCP powder with purity greater than 95% (Clarkson
Chromatography Products Inc., South Williamsport, PA) was also weighed and wet-ground with
100% ethanol using the same protocol described for DCPA. However, since the mix of small
particles of DCPA and median particle sizes of TTCP was described to result in cements with
optimal hydroxyapatite (HA) conversion, fast setting time, a microporous structure, and adequate
mechanical strength 46, the grinding time of TTCP was reduced to 20 minutes. In order to
promote ethanol evaporation, the resultant paste was allowed to dry for 24 hours in a fume hood
and the dried powder, with a final particle size range of 2-35µm, was stored in a desiccator at
60ºC to prevent water uptake.
Figure 2.2 Mixer Mill 301 and zirconium oxide jars and balls (illustrations from manufacturers catalogue)
2.A.2 Preparation of the liquid phase
The liquid component consisted of a 0.2M solution of Na2HPO4 (Sigma, St. Louis, MO)
and NaH2PO4 (Sigma, St. Louis, MO) in a 4:1 ratio (vol/vol) with a final pH of 7.4. First, double
distilled water solutions of 0.2M of Na2HPO4 and NaH2PO4 were prepared and stored in

27sterilized 500mL glass jars. Second, these solutions were mixed in a ratio of 4:1 to yield a final
pH of 7.4 78.
2.A.3 Hand-made calcium phosphate cements and Pant-calcium phosphate cements (H
and HP)
2.A.3.1 Mixing of the solid with the liquid phase
As described above, an equimolar mixture of DCPA and TTCPA was used for the
calcium phosphate cement formulation. For each 0.25g of solid phase, 0.068g of DCPA and
0.183g of TTCP, as well as 125µL of liquid phase, were employed to achieve a powder to liquid
ratio of 2.0.
For the preparation of hand-made calcium phosphate cements, the weighed calcium
phosphate powders (0.068g of DCPA and 0.183g of TTCP) were placed in a sterilized glass dish
and mixed with a glass stirring-rod for 30 seconds. Next, 125µL of the neutral phosphate
solution was added to the powders and the phases were mixed thoroughly for 3 minutes to a
paste-like consistency. For the preparation of Pantoprazole-doped cements, 12.5µg of
Pantoprazole sodium salt (Apotex, Canada) was added to the solid phase.
2.A.4 Machine-made calcium phosphate cements and Pant-calcium phosphate cements
(M and MP)
In the literature, calcium phosphate cements are often described as being prepared
through the mixing of ground calcium phosphate powders with a liquid phase, such as water, a
phosphate solution or even phosphate acid 33, 37-41. The traditional preparation process involves
grinding the powders using machinery, but mixing the solid with the liquid phase by hand 33, 34,
38, 40, 36, 43-45. The mixing is thus dependent on the individual’s own technique and is not
reproducible. For this reason, in the present work, the mixing of the solid phase with the neutral
phosphate solution was done in a 45ml Zirconium oxide jar with a 20mm zirconium oxide ball,
for 30 seconds at a vibrational frequency of 20 revolutions per second, using the MM301. The
final material is thus designated “machine-made” calcium phosphate cement (M).
2.A.5 Preparing particulate calcium phosphate cements
The final paste-like cements for both machine- and hand-made calcium phosphate
cements were stored and allowed to set in the incubator at 37˚C, with 5% CO2 and 100% relative
humidity, for 24 hours. After the allotted time, the hardened cements were ground into particles
using a pestle and mortar and the particulate material was sieved into a size range of 90 to

28355µm. This range was used since particles any larger would inhibit quick osteoclastic resorption
(owing to their large surface areas) and particles any smaller would be resorbed at too great a
rate by osteoclasts. The smallest particles (90µm) were included since they were considered too
big to be engulfed by macrophages during the initial stages of inflammation and could therefore
favour osteoconduction until remodelled through bone turnover. Finally, particulate Pant-
calcium phosphate cements (HP and MP) and calcium phosphate cements (H and M) were stored
in glass vials, labeled and γ-sterilized at 2.5Mrads.
2.B Characterization of hand- and machine-made calcium phosphate cements (H and M) Cements prepared using the conventional, manual technique and the novel, machine-
based protocol were characterized using the following methods.
2.B.1 Particle size distribution, surface area, porosity, and pore size (Scanning Electron
Microscopy)
In addition to the calcium phosphate cements prepared according to the methods
described in section 2.A, hardened hand- and machine-made calcium phosphate cements ground
using a pestle and mortar (H and M; as described in section 2.A.5) and using the MM301
machine (for 1 minute at 30 revolutions per second - HM and MM) were randomly selected and
their particle size distribution, surface area, porosity, and average pore size were assessed (n=5).
For the particle size distribution and surface area analyses of the calcium phosphate
cements, a Hitachi S3400 model SEM with an accelerating voltage of 15kV was used. Particulate
cements were mounted on standard stubs and, after image calibration and focus, pictures were
taken at a specific magnification (x40) and the software Image J 1.37v (National Institute of
Health, US) was used to calculate the particle size distribution and the total surface area for each
sample.
A Hitachi S-5200 model of cold field-emission scanning electron microscope (FESEM)
with a spot size varying from 0.4 to 1.5mm and an accelerating voltage of 7.0kV was used for
the porosity and pore size analyses of the calcium phosphate cements. The particulate materials
(0.5-0.7mg) were carbon-coated, affixed to an aluminum stub using conductive carbon paint
(Structure Probe, Inc.), and placed in a standard holder HS-5200 for the FESEM. Image J 1.37v
was used to calculate the porosity and pore size for each sample.

29
2.B.1.1 Particle size distribution and total surface area
For both particle size distribution and total surface area analyses of the calcium
phosphate cement groups (H, M, HM, MM – n=5), SEM images at x40 magnification were
scaled using Image J software. In the total surface area study, all particles in the sample were
selected using specific thresholds and their total area was measured by the Image J Particle
Analyzer.
In the particle size distribution study, the areas of the particles were measured and
converted into linear values using the Image J Particle Analyzer. Since the particulate material
has an average size range of 90 to 355µm, 6 particle size groups were chosen as follows: (1) 90-
130µm (6,358.0 to 13,273.26µm2); (2) 130-160µm (13,273.26 to 20,106.24µm2); (3) 160-200µm
(20,106.24 to 31,416.0µm2); (4) 200-230µm (31,416.0 to 41,547.66µm2); (5) 230-300µm
(41,547.66 to 70,686.0µm2); (6) 300-355µm (70,686.0 to 98,980.04µm2).
It was discovered that, during the preparation of calcium phosphate cements, a few
particles smaller than 90µm had become trapped in the sieves during the sieving process.
Therefore, particles smaller than 90µm (6,358.0µm2) were excluded from the study.
2.B.1.2 Porosity and pore size
Images at 2K, 10K, and 20K were scaled using Image J. Regions of interest with
40x40µm, 8.5x8.5µm, and 4.0x4.0µm respectively were cropped for each magnification. Next,
the pores of each sample were selected using specific thresholds and their areas were quantified
using the Image J Measure tool.
In order to measure the pore sizes of the calcium phosphate cements groups, images at
three different magnifications were scaled using Image J. In the micropores (pores bigger than
1µm) analysis, cropped areas of 40x40µm and 15x15µm were used for images at 2K and 5K
magnifications, respectively, while a region of interest of 4.0x4.0µm (20K images) was drawn
for the nanopores (pores smaller than 1µm) analysis. Special care was taken not to overlap
cropped areas, so that the same pores were not measured twice. The feature “invert LUT” was
used as a guide for the drawing of at least 10 pores per cropped region (50 pores per group per
magnification). In addition, four linear measurements per pore were taken and averaged using
the Image J Measure tool.

30
2.B.2 In vitro degradation
Particulate hand- and machine-made calcium phosphate cements (H and M) were
prepared as outlined in section 2.A and analyzed according to their degradation in solutions with
different pHs after specific intervals. Since this degradation study relied upon calcium trace
analysis and calcium is a ubiquitous element, all vials were cleaned following a protocol which
eliminated the possibility of contamination 150. Additionally, all procedures were undertaken in a
laminar flow fume hood to avoid the samples’ coming into contact with the lab environment.
Five samples (0.013g each) of each group were soaked in clean 15mL falcon tubes with
10mL (1:1000 w/v) sodium phosphate buffer solutions at different pHs (7.4, 6.4 and 5.0).
Previously cleaned polyethylene jars were chosen to store 2L of each buffer solution
which were prepared using 0.2M Na2HPO4 (BioShop), 0.1M Citric acid (Sigma), and double
distilled water (DDH2O). The pH of each jar was adjusted to the desired 5.0, 6.4, and 7.4 values
by adding a DDH2O solution of either 0.1M Ultrex Grade HCl (JT Baker, Phillipsburg, NJ) or
0.1M NaOH in a drop-wise fashion and measuring the pH of the solution until the correct pH
was obtained. The 0.1 M NaOH DDH2O solution was prepared by weighing and adding NaOH
pellets (Baker Analyzed ACS Reagent, JT Baker, Phillipsburg, NJ) to DDH2O.
2.B.2.1 Calcium concentration measurements (Atomic Absorption Spectroscopy)
After immersion, the samples were stored in the incubator at 37ºC for 1, 2, 3, and 4
weeks. At the one-, two-, three- and four-week marks, 10mL of the buffer solution was retrieved
from the Falcon tubes and transferred to clean 30mL Nalgene bottles. Next, 200µl of a 1+1
Ultrex Grade HCl (JT Baker, Phillipsburg, NJ): DDH2O solution was added to each sample and
the bottles were stored at 4ºC until their calcium concentration was measured. Measurement was
conducted using Atomic Absorption Spectroscopy analysis at the Institute of Biomaterials and
Biomedical Engineering at the University of Toronto. During Atomic Absorption
Spectrophotometry (AAS) analysis, a flame was used to atomize metal ions in solutions. A light
beam was then shot through the resultant vapour and the amount of light absorbed by the
investigated element was measured. Finally, the concentration of the metal was calculated using
the principle of proportionality between the absorbed light and the concentration of the studied
element. A Varian 850 (Palo Alto, CA) Atomic Absorption Spectrophotometer with an

31approximate calcium concentration detection limit of 0.005ppm was used to measure the trace
amount of Ca element present in the above-described solutions.
2.B.3 In vivo implantation
Fifteen male Wistar rats (200-250g) were anaesthetized by inhalation of Isofluorane in
nitrous oxide and oxygen (900 mL total flow rate - 5% for induction and 2-2.5% as
maintenance). Buprenorphin (0.01-0.15 mg/kg) was administered subcutaneously as analgesic
both prior to and after the surgery. Next, 12mg of hand- and machine-made calcium phosphate
cement particles (H and M) was implanted in bilateral bone defects created in the distal aspect of
the femora using a 2.3mm dental burr under constant saline irrigation (n=5). A Teflon membrane
was used to cover the defect and prevent the washing out of the particles. After implantation, the
femoral muscle wall was repositioned and sutured using a biodegradable suture (4-0
PolysorbTM, Syneture, US), and the skin was closed with 9-millimeter wound clips (Becton
Dickinson, MD, US). To ensure that the volume was identical for all samples and to prevent the
leaching out of particles, custom-made stainless steel syringes with end tips matching the
diameter of the defects were used to deliver the implants into the defects (Figure 2.3). This
protocol was approved by the Ethics Committee of Animal Research at the University of
Toronto.
During the post-operative period, the animals were monitored on a daily basis in the
animal care facilities of the Department of Comparative Medicine and Faculty of Dentistry of the
University of Toronto. Five animals were euthanized by cervical dislocation after CO2 exposure
at each of the 1-, 2- and 3-week marks post-operation (sum total: 15 rats). The rats’ femurs were
harvested, trimmed, and fixed in 10% neutral formalin. Finally, they were submitted to non-
destructive histomorphometric analysis (MicroCT).

32
Figure 2.3 Sequence of surgic(D) loading of stainless steel syTeflon membrane and suture.
2.B.3.1 Histomorphome
MicroCT scans of each
(MicroCT40, Scanco Medical,
were placed in poly-methyl-me
70kVp and 114µA. The specim
resolution of 6µm, and acquisi
each (per 180º of rotation), 0º a
averaging. The scanning time f
The final 3D images w
thickness. After scanning and r
cavity was drawn at different d
the final drawings could be mo
quantification of both bone and
segmentation of these material
analyzing the gray-level distrib
calcium phosphate cements we
were divided by an averaged d
consistently related to the defe
A
al stages: (A) exposure of feringe with particulate mate
tric analysis (Micro-Comp
femur were conducted with
Basserdorf, Switzerland) (F
tacrylate (PMMA) holder w
ens were scanned in high-r
tion files were obtained at 1
ngle increment, 300ms of i
or each specimen was appr
ere composed of 500-700 ax
econstruction, a region of in
epths (approximately every
rphed and render a 3D ROI
particulate material volum
s using different threshold v
ution. However, threshold v
re kept the same for each ti
efect size (10.23 mm3), so t
ct volume.
B
E
mur, (B) and (C) drillingrial, (E) closure of the def
uted Tomography)
a microtomography syst
igure 2.4). All trimmed f
ith distilled water and sc
esolution mode with an X
000 projections with 2,04
ntegration time, and 1 fra
oximately 2.1 hours.
ial-cut slices, each one w
terest (ROI) comprising
50 slices) of the 3D data
. Within the new-designe
es (in mm3) was possible
alues, which were determ
alues for hand- and mach
me interval. In addition, a
hat the measurements wer
C
D
of defect, ect with
em
emur samples
anned at
, Y, and Z
8 samples
me
ith 6µm in
the marrow
set, so that
d ROI, the
through the
ined by
ine-made
ll volumes
e

33
Figure 2.4 The principle of a MicroCT scan. (i) From a tungsten tube, X-rays are shot through a sample on a rotatory stage. Next, a Charged-Coupled Device (CCD) camera captures the photoelectrical signals, which are serialized into images and reconstructed by the µCT40 software (Source: Mohr et al., 2003).
2.C Hand- and machine-made calcium phosphate cements with and without Pantoprazole This section proposes the assessment of hand- and machine-made, Pantoprazole-doped
and undoped-calcium phosphate cements. Specifically, calcium phosphate cements were
examined with respect to their HA conversion, dissolution in saline (pH=7.4), Pantoprazole
release kinetics, and in vivo implantation.
2.C.1 Powder X-ray diffraction (PXRD) analysis (H, M, HP, MP)
The measurement of the HA conversion percentage of the prepared hand- and machine-
made calcium phosphate cements, undoped (H and M) and doped with Pantoprazole (HP and
MP), was performed using Powder X-ray Diffraction (PXRD) analysis 34, 39, 44, 50, 56, 57, 151, 152.
First, 2g of each calcium phosphate cements sample (n=3) was prepared as described in
section 2.A and stored in 1.5mL eppendorf tubes. After 1, 3, 5, and 10 days, and 1, 2, 3, 4, 5, 6,
7, and 8 weeks, the eppendorfs were submerged in liquid nitrogen (N2 at -80ºC) to arrest the
cements’ reaction. The frozen samples were then sent to the Department of Chemistry of the
University of Toronto for quantitative PXRD analysis.
The samples were run using a normal front packing technique on a Bruker AXS D8
Discovery Microdiffraction system with Cu kα point-focus x-ray source operating at 40
kV/40µA. The system was equipped with a curved primary graphite monochromator and 2D
proportional detector (GADDS). The data were collected on two frames at 1200s exposure,
which cover a range of 20-58 degrees. The 2D diffraction images were then integrated with a

34step size of 0.005º 2-theta and converted to standard I vs. 2-theta diffraction patterns. The phase
identification was done by Diffrac Plus™ data processing software Eva™ v. 8.0 and
Search/Match™ routine. This qualitative phase composition was established by comparison with
the reference PXRD patterns stored in the U of T Chemistry Department PDF-2 Database (2001)
via Search-Match™ software. The profile fitting applications such as Rietveld refinement,
quantitative and microstructure analyses were performed using Topas™ v. 2.1 software. The
Rietveld method is well known and widely accepted in the field as providing a full and complete
compositional analysis of the material. The structural information of all components being
presented in the analyzed materials is needed for input. Using an appropriate algorithm, the
software calculates point-by-point the individual diffraction patterns for components, extracts the
individual reflections from the overlap diffraction profile, and then matches every calculated
point against the corresponding point of the observed pattern's profile. During the refinement
least square procedure, all refined parameters have their values changed until a best fit is
achieved. The Rietveld refinement procedure intrinsically calculates all refinable data as overall
parameters with their mean values.
2.C.2 In vitro degradation (H, M, HP, MP)
In this model, 0.013g of calcium phosphate cements from the batch described in section
2.C.1 were analyzed according to their degradation in saline at pH 7.4 (n=3). The samples were
immersed in 15mL falcon tubes with saline and the calcium (Ca) concentrations were measured
at intervals of 2, 4, and 8 hours, 1, 3, 5 and 10 days, and 1, 3, 4, 8, and 12 weeks. This analysis
was performed using an Atomic Absorption Spectroscopy (AAS), as outlined in section 2.B.2.1.
2.C.3 Pantoprazole release kinetics (HP, MP)
A Synergy HT spectrophotometer (Bio-Tek, US) was used to analyze the release profile
of Pantoprazole incorporated into hand- and machine-made calcium phosphate cements. In
addition, the reading and quantification of the examined solutions was done using the KC4
v.3.1/rev1.4 software (Kineticalc for Windows, Bio-Tek Instruments Inc., US).
The particulate material (each sample containing 12.5µg of the drug) was immersed in
vials with 1mL of saline and stored in an incubator at 37ºC for 2, 4, and 8 hours, 1, 3, 5 and 10
days, and 1, 3, 4, 8 and 12 weeks (n=5). The shortest intervals were chosen to enable analysis of
the burst effect of delivery from the cements’ matrix 153, 154. Intervals of 1, 3, 4, 8 and 12 weeks
were chosen because they corresponded to those used in the in vivo experiments, assays from

35which parallel analyses could be made. As previously described by Queiroz et al. 2005 155, after
each interval, the vials were centrifuged at 4,500rpm for 5 minutes and 200µL of the supernatant
was removed and placed in 96 well plates for the ultra violet (UV) absorbance reading, according
to Pantoprazole’s wavelength absorbance peak (292nm).
2.C.3.1 Pantoprazole standard solutions and release kinetic curve
Solutions with known concentrations of Pantoprazole were prepared through serial
dilutions of a matrix solution of Pantoprazole:saline with a concentration of 20ug/ml. Since the
total amount of Pantoprazole in each sample was 12.5µg, the chosen concentrations for the
standard solution were: 0.75, 1.0, 2.0, 4.0, 5.0, 7.0, 8.0, 9.0, 11.0, 12.0, 13.0, 15.0, 16.0, 17.0,
19.0, and 20.0µg/ml.
The standard solutions were then analyzed using a spectrophotometer at 292nm, the
appraisal of which allowed for the design of a standard curve and a formula for the drug release
profile. Finally, a curve for the drug delivery from hand- and machine-prepared cements was
plotted.
2.C.4 In vivo implantation
2.C.4.1 Pilot study (Pantoprazole-, Omeprazole-, Concanamycin-, and Bafylomycin-
calcium phosphate cements)
In a pilot study, particulate calcium phosphate cements loaded with different drugs were
prepared using the hand technique as follows:
The solid phase of these cements consisted of an equimolar mixture of DCPA and TTCP.
Bafilomycin (BAF), Omeprazole (OMP) or Pantoprazole (PANT) was incorporated into the
cements’ matrix. The liquid component consisted of a 0.2M solution of Na2HPO4 and NaH2PO4
in a 4:1 ratio (vol/vol). For the drugs that are not phosphate or water soluble, DMSO
(Dimethylsulfoxide) was used as solvent. Therefore, DMSO solutions of BAF and OMP as well
as a phosphate solution of PANT were prepared. For each 25mg of powder, 125µL of liquid was
employed in order to achieve a powder-liquid ratio of 2.0. Control (undoped) calcium phosphate
cement particles were also prepared. Solid and liquid components were mixed in order to obtain
paste-like cements. These cements were then kept in an incubator at 37°C with 5% CO2 and
100% humidity for 24 hours. Next, they were allowed to dry at room temperature for another 48

36hours and subsequently crushed into particles (90-355µm). The final particulate material was
then labeled and γ-sterilized.
Control and test materials were placed into bilateral 2.3mm diameter distal femoral
defects in 200-250g male Wistar rats. Implants were left for either 1 or 3 weeks (n=3). Following
the allotted time, animals were euthanized by cervical dislocation after exposure to CO2. Femora
were harvested and fixed in 10% buffered formaldehyde. Samples were then trimmed and
scanned for MicroCT (µCT - GE) quantitative analysis of the volume of particles and bone
formation.
MicroCT scans were conducted with the GE eXplore Locus SP MicroCT System, which
has a fixed tungsten anode as the x-ray source, an x-ray tube with maximum potential of 90kVp
and maximum current of 180µA combined to a maximum power of 8w. A built-in CCD camera
and a thin film cesium scintillador are used for data acquisition and data sets are generated with
isotropic resolution (GE Healthcare, 2005). All particulate samples were placed in a 15mm
diameter holder with distilled water and scanned using a 0.02” Aluminum filter at 80kVp and 80
µA (6.4w). The densities of the samples were calibrated following to the GE protocol using a
calibration object included in the GE sample holder which contained air, water, and
hydroxyapatite. This calibration tool converted the Arbitrary Digital Units (ADUs) into
Hounsfield Units (HUs). The MicroCT settings for the scan of the particulate material were:
scan time of 2 hours, 2x2 binning, 4 frame averaging, 1700ms view exposure time, and 360º
rotation, at a 16µm effective pixel size. The resulting 3 dimensional volumes were reconstructed
at 32µm effective pixel size (2x2 binning) using the GE eXplore Reconstruction Utility.
MicroView (GE) software was used for the volumetric analysis. The densities of the particles
and bone were then calibrated (particles=20000HUs/ bone= 16000HUs) and their volumes in
mm3 were calculated according to the Bone Analysis Application of the Micro View (GE)
software. The region of interest selected was comprised by the area delimited by the defect
created and the resulting 3 dimensional images were analyzed in the Microview (GE) software
for quantification of the volume of the particles and reparative bone at each time point.
For the MicroCT quantitative analysis, the volumes of the remnant particles and bone
activity were measured and compared to the volume of an averaged defect volume. The volume
of the defect was calculated considering the defect as a cylinder and was used as a standardized
value (100%) with which particles and bone formation volumes were compared. Microview GE
software was used to calculate the above-mentioned volumes through the threshold of different

37regions of interest according to their densities, particulate calcium phosphate cements’ density
being higher than that of the bone.
Statistical analysis was performed using R (The R Foundation for Statistics Computing
Version 2.3.0). Differences among groups were compared using ANOVA, followed by post-hoc
TukeyHSD. P values lower than 0.05 were considered significant.
2.C.4.2 Main study (MP x M, and MP x Empty defect)
As approached in the pilot study, an issue of particular relevance to the clinical
applicability of doped calcium phosphate cements is their ability to inhibit osteoclastic
resorption. Therefore, in this in vivo experiment, the degradation time frame and reparative bone
formation of MP and M were compared. In the case of the doped calcium phosphate cements
presenting an extended degradation profile, it was essential to ascertain how long the cements
would stay un-resorbed in the defect. Thus, the objective was to survey the in vivo degradation
process of the doped and undoped machine-made calcium phosphate cements using µCT and
histological analyses. The same surgical protocol outlined in section 2.B.3 was employed for this
in vivo study.
2.C.4.3 Experimental setup
A two-stage experimental setup was designed to examine the degradation rate and bone
formation of machine-made pantoprazole calcium phosphate cements (MP) and machine-made
calcium phosphate cements (M), as well as to determine the in vivo longevity of MP.
In the first stage, MP and M were bilaterally implanted in rats femora and analyzed after
5 days and 1, 2, 3, 4, 5, 6, and 7 weeks (n=5). The first 3 intervals (5 days, 1, and 2 weeks) were
chosen so as to show when the in vivo degradation began, while the later intervals (3, 4, 5, 6, and
7 weeks) were chosen so as to show the degradation course of the doped and undoped calcium
phosphate cements.
In the second stage, particulate MP were implanted in one femur while the contra lateral
femur was left empty. The histomorphometric and histological analyses were conducted after 2,
4, 6, 8, 10, 12, 14, and 16 weeks (n=5). This second experiment aimed to pinpoint the time at
which the particulate material was completely resorbed as well as whether the particulate
material would impair the defect’s closure.

382.C.4.4 Histomorphometric analysis
The quantitative analysis of this study was carried out under the same conditions as those
described in section 2.B.3.1.
2.C.4.5 Histological processing
According to the histomorphometric analysis, the most representative samples for each
interval were chosen for the histological analysis. A modified version of the Osteo-Bed Bone
Embedding Kit protocol for small samples was used (Donath Technique - Exakt Products
Histology, US).
Briefly, the trimmed samples were placed in specimen glass vials and washed in running
water for 1 hour. Next, the samples were dehydrated at room temperature in increasingly
concentrated ethanol solutions: 70% for 2 days, 1 change after the first hour; 95% for 3 days, 1
change daily; 100% for 3 days, 1 change daily. Then, the samples were infiltrated with the
monomer Osteo-Bed I for 6 days (1 change after 3 days) under vacuum at room temperature.
Finally, the samples were embedded in Osteo-Bed III (1.4g benzoyl peroxide /100mL monomer)
for 6 days (1 change after 3 days) under vacuum at 4ºC before being placed in the oven at
progressively higher temperatures (35ºC for 3 days, 50ºC for 3 days, and 60ºC for 1 day) to
allow the resin to set.
After setting, the glass vials were broken and the resin blocks were ground and polished.
The blocks were then glued to back-up slides and cut at the region of interest with a 200µm
diamond saw (E300). To smooth the surfaces of the specimens, P800 and P1000 grinding papers
were used with a micro grinder-polisher (Exakt 400CS) featuring a water-cooled system. Once
the surface of the each block was parallel to its respective back-up slide (the dimensions of three
sites of each block were equal to each other to within 0.002mm or less), a final slide was glued to
the block. To remove the back-up slide, a cut was made through the block, parallel to, and
200µm from, the final slide. Next, the specimens were polished with P4000 polishing paper until
a smooth surface was obtained. Finally, the polished slides, with a thickness of 30-40µm, were
subjected to the staining protocol.
In the staining procedure, a drop of Toluidine Blue:DDH2O solution at 1% was poured on
the specimens, which were kept in the oven at 50ºC for 30 minutes. The excess stain was
removed by quickly washing the samples in running water. Images in different magnifications

39were retrieved using a Leitz Aristoplan microscope, Q imaging Micropublisher 5.0 RTV digital
camera, and Openlab 4.0.4 software.
2.D Other bone substitutes
2.D.1 Anorganic bone (BioOssTM), Bioactive glass (BioGranTM), and Demineralized bone
matrix (AllogenixTM)
Attempts to develop efficient bone substitutes have resulted in the development of several
products. Among them are: Bioactive Glass (BAG), Anorganic Bone (AB), and Demineralized
Bone Matrix (DBM). To assess whether the particulate MP produced better in vivo outcomes
than AB, BAG and DBM, the degradation and reparative bone formation of these bone
substitutes were assessed using the experimental design outlined in section 2.B.3. For this
purpose, three commercially available bone substitutes were tested: BioOssTM (AB), BioGranTM
(BAG), and AllogenixTM (DBM). BioOssTM is commercially provided in particles with a size
range of 250µm to 1mm; BioGranTM has the shape of glass beads with a size range of 90 to
355µm; and AllogenixTM is available in putty form (Figure 2.5).
Figure 2.5 Pictures of BioOssTM, BiogranTM, and AllogenixTM
2.D.2 In vivo implantation
In this experiment, AB, BAG, and DBM were bilaterally implanted in rat femora and
MicroCT (quantitative) as well as histological (qualitative) analyses were conducted 3, 6, 12, and
16 weeks post-operative (n=5). The results from the quantitative and qualitative assessments
were compared to those for MP described in section 2.C.4.1.
2.D.2.1 Histomorphometric analysis and histological processing
The MicroCT and histological analyses of AB, BAG, and DBM, followed the same
procedures as those described in sections 2.B.3.1 and 2.C.4.3, respectively.

40However, since the DBM putty is not visible in the MicroCT images, the
histomorphometric evaluation of this group was done using the histology slides. Thus, two slides
per sample per interval were selected and DBM area values were measured using the Image J
Measure tool. However, DBM bone volume measurements were conducted using the traditional
MicroCT thresholds (Figure 2.6).
In addition, BioGranTM’s core showed thresholds very similar to those of reparative bone,
which represented a limitation for the radiodensity segmentation of bone and particulate
volumes. As a result, at every 3 slices in the reconstructed image, each particle was contoured
and excluded, so a threshold for the measurement of reparative bone volume was possible
(Figure 2.7). For the measurement of the particulate volume, traditional marrow contours
(outlined in 2.B.3.1) were drawn and a low threshold was chosen to calculate the Total Mineral
Content (TMC = bone volume + particle volume) of the samples. Finally, the bone volume
values were subtracted from the TMC ones, the result of which was considered the volume of
BAG (Figure 2.8).

41
Figure 2.6 MicroCT slice of a DBM sample. Marrow cavity with newly-formed bone and no visible material (demineralized bone matrix does not absorb x-rays).
Figure 2.7 Bone volume measurements for BAG samples.

42
Figure 2.8 TMC measurement and overview of BAG particulate contours

432.E Statistical analysis
Statistical analyses were performed using the computer software Statistical Analysis
System (SAS Institute Inc., NC, USA). Differences among groups were compared using
ANOVA analysis of variance followed by Tukey adjustment for multiple comparisons (used
when ANOVA showed statistical differences and two or more treatments were being analyzed).
Specifically, statistical analysis by ANOVA was used to compare the difference among the mean
values of all groups without discrimination (e.g., machine, hand, pestle and mortar, and
MM301). In case one group of values was significantly different from other, Tukey adjustment
for multiple comparisons was used to separate each group and pinpoint the factor responsible for
the statistical difference (e.g., the mixing protocols, the grinding techniques, or the combination
of both). P values lower than 0.05 were considered significant.

443. RESULTS
3.A Characterization of hand- and machine-made calcium phosphate cements 3.A.1 Particle size distribution and surface area (SEM)
A quantitative analysis of SEM images was conducted to describe the particle size
distribution of hand- and machine-made calcium phosphate cements, ground with pestle and
mortar or the MM301 machine (Figure 3.1). The particulate material was divided into six groups
according to its particle size. Neither the different preparation methods nor the grinding
procedures influenced the particle size distribution of calcium phosphate cement groups, which
showed particle sizes mainly in the range of 90 to 200µm (Figure 3.2). Nor was any statistical
significance found in the different mixing (hand- and machine) or grinding procedures (MM301
and PM – pestle and mortar). In addition, the total surface area of hand- and machine-made
cements was similar for all groups, as shown in figure 3.3.
A B
Figure 3.1 (A) SEM image of a H sample and (B) the particle threshold analysis using the Image J Particle Analyzer tool.

45
Particle size distribution of calcium phosphate cements05
101520
253035
4045
90-130 130-160 160-200 200-230 230-300 300-355
Size ranges (um)
Perc
enta
ge
HM MM H M
Figure 3.2 Particle size distribution of calcium phosphate cements. For all groups, approximately 80% of the particles showed a size range of 90-200µm (n=5).
Surface area of calcium phosphate cements
32.37
23.46
25.70
20.60
0 5 10 15 20 25 30 35 40 45
Gro
ups
Percentage
HM MM H M
Figure 3.3 Total surface area of hand- and machine-made calcium phosphate cements. All groups presented similar total surface area values (n=5).

46
3.A.2 Porosity and pore size (FESEM)
The porosity of hand- and machine-made calcium phosphate cements was measured
through the analysis of FESEM images using the Image J Measure tool (Figure 3.4). Both
calcium phosphate cements ground using the MM301 (HM and MM) and those mixed manually
and ground using a pestle and mortar (H) showed similar porosity values. However, the cements
mixed by the MM301 and ground using a pestle and mortar (M) had a statistically higher
porosity percentage compared to those mixed by hand and ground using the MM301 (HM)
(Figure 3.5). The conducted statistical analyses (ANOVA followed by Tukey adjustment – p =
0.0482) identified the grinding procedure (pestle and mortar) as the factor which caused such
difference.
B
A
Figure 3.4 (A) SEM image of a HM sample and (B) the threshold of its porosity using the Image J Particle Analyzer tool.

47
Fp
m
I
w
a
d
d
n
s
w
o
c
T
Porosity of calcium phosphate cements
14.9716.00 16.20
18.47
0
5
10
15
20
Groups
Poro
sity
(%)
HM MM H M
igure 3.5 Porosity percentages of calcium phosphate cements. M samples showed higher orosity values than HM (ANOVA and Tukey adjustment for multiple comparisons - p=0.0482).
The pore sizes of calcium phosphate cements were measured and divided into 2 groups:
icropores (pores larger than or equal to 1µm) and the nanopores (pores smaller than 1µm).
mages at 2K and 5K magnifications were used to measure the micropores, whereas those at 20K
ere used to measure nanopores. Four linear measurements of each pore were drawn and
veraged to define the final pore size for each sample (Figure 3.6). As shown in Table 3.1, the
ifferences in the measurements of micropores were insignificant for all groups.
In the case of the nanopores, the only comparison that did not show nanopore size
iscrepancies was that between the cements mixed using the MM301 (M and MM). The
anopores values of all hand-made cements (H and HM) and the other groups (M and MM) were
tatistically different. Overall, the grinding procedure did not interfere in the nanopore sizes
ithin the machine-prepared cements. On the other hand, both the grinding and the combination
f grinding and mixing strategies influenced the nanopore values when the hand-prepared
ements were compared to each other and to the machine-made cements (ANOVA followed by
ukey adjustment – p = 0.0001).

48
NANOPORES (µm) MICROPORES (µm) HM 0.13 ± 0.02 4.21 ± 0.81 MM 0.22 ± 0.03 3.95 ± 0.84
H 0.28 ± 0.04 4.26 ± 0.23 M 0.22 ± 0.04 3.68 ± 0.05
Table 3.1 Pore sizes of calcium phosphate cements. Cements mixed using the MM301 showed similar nanopores values. Statistical significance was found between the hand-prepared cements and the other groups (p= 0.0001).
A
B
Figure 3.6 SEM images of pore size measurements. (A) Cropped region for a HM sample at 2K, (B) Same sample viewed after application of Image J “invert LUT” tool, (C) and (D) Micropore size drawings and measurements, (E) and (F) Nanopore size drawings and measurements.
F
D C
E

493.A.3 Calcium concentration analysis (AAS)
Two samples of H (4 weeks) were excluded from this study because they presented
extremely high calcium concentrations, possibly the result of particulate material carried from
the Falcon tubes to the Nalgene bottles, which were submitted to AAS analysis.
Results of the hand- and machine-made cements dissolution experiments are shown in
figure 3.7. Calcium concentrations decreased with the increase of the pH (dissolution at pH 5.0 >
pH 6.4 > pH 7.4). At pH 5.0, all samples presented high dissolution values with a decreasing
trend from the first to the second weeks and increased calcium concentrations from the second to
the fourth weeks. At pH 6.4, H showed similar dissolution values through all the intervals. On
the other hand, M exhibited significantly higher calcium concentrations after 1 and 2 weeks of
immersion. At pH 7.4, except for M, which displayed increased dissolution in the 2-week
interval, the particulate materials presented low and consistent calcium concentration for all
intervals.
Figure 3.7 Dissolution of H and M. Calcium concentrations decreased as the pH increased. During the first 2 weeks at pH6.4, the cements prepared using the MM301 showed a higher calcium concentration (n=5).
Dissolution of calcium phosphate cements
1.0
10.0
100.0
1000.0
5.0 6.4 7.4
pH
[Ca]
(ug/
ml)
H(1w) M(1w) H(2w) M(2w)H(3w) M(3w) H(4w) M(4w)

50
3.A.4 In vivo implantation (H x M)
At 1 week post-operative, peri-implant osteogenesis was observed in all samples,
irrespective of mixing technique. This bone was found directly surrounding the implant within
the marrow cavity and was distinct from distal trabecular bone. At 2 weeks post-operative, bone
volumes were higher for the machine-prepared cements (M). However, by 3 weeks the reparative
bone observed at 1 week had partly resorbed and had similar values for all samples (Figure 3.9).
Although the mean volumetric values were similar, machine-prepared cements showed a
decreased reparative bone remodelling rate (65%) compared to hand-prepared cements (77%)
from the first to the third experimental week. For all intervals, peri-implant bone was found on
the surface and within the implants, creating a bony net in the marrow cavity. The criteria for the
threshold analyses of samples at 1 week are shown in figure 3.8.
A consistent degradation pattern of the particulate calcium phosphate cements was found
at all tested intervals. At 1, 2, and 3 weeks post-operative, particulate H and M presented
significant degradation with similar volumes. However, as was the case with the bone volumetric
analysis, M presented a particulate degradation rate of 55% while H degraded 63% from the first
to the third week after implantation (Figure 3.10).

D
H
51
Figure 3.8 MicroCT slices of H x M. (A) and (B) Reparative bone formation of H at 1week; (C) and (D) Particulate volume of H at 1 week; (E) and (F) Reparative bone formation of M at 1week; (G) and (H) Particulate volume of M at 1 week.
C
G
B
F
A
E

52Bone volume of calcium phosphate cements
0.460.43 0.34
0.150.16
0.10
0.00
0.10
0.20
0.30
0.40
0.50
0.60
1w 2w 3w
Intervals
Volu
me
(mm3 )
M H
77%
65%
Figure 3.9 Reparative bone volumes for M and H. After 1 week and 3 weeks, M and H showed similar bone formation mean values but different remodelling rates.
Figure 3.10 Particulate volume for M and H. At all intervals, M and H showed similar volume values but different degradation rates from the first to the third week (n=5).
Particle volume of calcium phosphate cements
0.11
0.08
0.060.04 0.05
0.03
0.000.020.040.060.080.100.120.140.160.18
1w 2w 3w
Intervals
Volu
me
(mm3 )
M H
63% 55%

53
3.B Hand- and machine-made calcium phosphate cements with and without Pantoprazole
3.B.1 Time-dependent HA conversion (PXRD analysis)
3.B.1.1 Pilot study
Before testing the hand- and machine-made cements proposed in this work, cements
doped with Pantoprazole (PANT), Omeprazole (OMP), and Tetracycline (TC) were prepared by
different individuals (1 and 2) and sent for PXRD analysis for identification and quantification of
the final products of the calcium phosphate cements’ reaction.
As shown in Table 3.2, the machine-made calcium phosphate cements displayed a
substantially higher HA conversion rate when compared to all hand-made cements, except for
TC-cement. Similarly, TC-cement converted into more HA than both TC-PANT- and PANT-
cements. Overall, a great variability in the conversion of calcium phosphate cements into HA
was observed, which served as a basis for further comparisons between hand- and machine-made
cements.
Calcium phosphate cements %TTCP %DCPA %HA OMP-cement (1) 58.0 19.0 23.0 OMP-cement (2) 54.0 34.0 12.0 TC-cement (2) 13.0 --- 87.0
TC-PANT-cement (1) 46.0 30.0 24.0 TC-PANT-cement (2) 26.0 25.0 49.0
PANT-cement (1) 13.0 30.0 57.0 H (1) 57.0 29.0 14.0 H (1) 70.4 29.6 ---
M-Oct06 13.0 --- 87.0 M-Dec06 10.0 --- 90.0
Table 3.2 Results from the quantitative Rietveld analysis of hand- and machine-made calcium phosphate cements (doped and undoped).

54
3.B.1.2 Main study
The cements prepared by the machine technique had a more stable, statistically increased
HA conversion rate compared to those prepared by hand at all intervals analyzed. Interestingly,
the cements loaded with Pantoprazole showed a consistently higher HA percentage compared to
the undoped cements (Figure 3.11).
HA conversion of calcium phosphate cements
0
30
60
90
120
1d 3d 5d 7d 10d 2w 3w 4w 5w 6w 7w 8w
Intervals
% H
A
H HP M MP
Figure 3.11 HA conversion of hand-, machine-made, doped, and undoped calcium phosphate cements. The machine-prepared cements presented higher HA conversion at all intervals studied (n=3).
3.B.2 Calcium concentration analysis (AAS)
One sample of H at 10 weeks, one of M at 4 weeks, and all samples of MP at 4 and 12
weeks were excluded from this study because they presented extremely high calcium
concentrations. Again, this might have been a result of delivery of the particulate material from
the Falcon tubes to the Nalgene bottles, which were sent to AAS analysis.
Calcium concentration values at 2 hours were similar for most of the groups, except for
MP, which showed significantly decreased dissolution values compared to H and M. However, at
4 hours the only group that presented discrepant higher calcium readings was M. From 8 hours to

552 weeks and from 8 to 10 weeks, MP showed consistently decreased calcium concentrations
compared to the other groups. Generally, the cements loaded with Pantoprazole showed
diminished dissolution rates compared to the undoped ones. On the other hand, M presented
overall higher calcium concentrations when analyzed together with H.
Interestingly, the dissolution profiles of the machine-made cements showed more stable,
ascending values up to the 4-week interval, from which point the calcium measurements dropped
until the 12-week interval. Meanwhile, the dissolution outlines for the hand-made cements
showed a variable profile, with peaks and valleys throughout the whole experiment (Figure
3.12).
Dissolution of calcium phosphate cements
0
5
10
15
20
25
30
2h 4h 8h 1d 3d 5d 7d 10d 2w 4w 8w 10w 12w
Intervals
[Ca]
(ug/
ml)
H HP M MP
Figure 3.12 Dissolution of hand- and machine-made, doped and undoped- calcium phosphate cements in saline at pH 7.4. Machine-made cements displayed a more stable dissolution profile. MP consistently showed lower calcium concentration than the other groups.

56
3.B.3 Drug release from calcium phosphate cements
3.B.3.1 Pantoprazole standard solutions and release kinetic curve
The standard release curve of known concentrations of Pantoprazole is shown in figure
3.13. Hand- and machine-made cements showed similar release profiles which sustained the drug
delivery for 5 days. However, after 5 days the solutions appeared dark-yellowish and clumps
appeared in the bottom of the eppendorfs (Figure 3.14). This interval coincides with the period in
which the UV readings of Pantoprazole are higher than the total amount of the drug incorporated
into the cements. Therefore, it is suggested that the Pantoprazole was denatured on account of its
long-term instability in saline solution.
Pantoprazole standard curve
y = 1.1473Ln(x) + 2.1817R2 = 0.9755
0
1
2
3
4
5
6
0 2 4 6 8 10 12 14 16 18
Concentration (ug/ml)
Abs
orba
nce
Figure 3.13 Standard curve and formula for known Pantoprazole solutions.

57
Pantoprazole release from calcium phosphate cements
12.7
8.18.4
5.175.583.514.19
3.643.373.33
3.35
15.6
9.49.6
5.656.08
4.274.43.873.413.41
3.33
0
2
4
6
8
10
12
14
16
18
2h 4h 8h 1d 3d 5d 10d 2w 4w 8w 10w
Intervals
Abs
orba
nce
HP MP
Figure 3.14 Pantoprazole release from calcium phosphate cements. A sustained released occurred for 5 days, after which interval Pantoprazole became denatured (red line).
3.B.4 In vivo implantation
3.B.4.1 Pilot study (Pantoprazole-, Omeprazole-, Concanamycin-, and Bafylomycin-
doped calcium phosphate cements)
A preliminary study with loaded calcium phosphate cements was conducted which aimed
to examine the influence of the drug incorporation on the in vivo behaviour of these cements.
MicroCT scans of this pilot study are shown in section 7.A.1.
Bone formation was found in all samples. Moreover, direct bone-particulate contact was
observed at 1 and 3 weeks. At 1 week post-operative, statistically higher particulate volumes
were found on PANT-doped cements compared to cement particles doped with BAF and small
amounts of BAF and OMP particles were found. These diminished volumes were possibly due to

58the particulate leaching from the bone defect. In addition, bone formation for all samples was
greater than the volume of the defects. The differences between bone volume of OMP after 1 and
3 weeks and control after 1 and 3 weeks were statistically significant.
At 3 weeks, all PPI groups presented proportionally, delayed particle degradation rate
when compared to the control samples. From the first to the third week, control samples showed
considerable particle and bone degradation rates (82.2% and 84.6%, respectively) whereas PPI-
doped particles maintained a controlled degradation rate for both particles and bone volumes.
BAF-loaded particle volume decreased 30.5% from the first to the third week. The
volume of new-formed bone for this sample diminished 44%. PANT decreased 23.1% and
62.6% in particle and bone activity volumes, respectively. Particles doped with OMP diminished
17.7% in particle volume and 61.7% in bone volume (Figure 3.15). Some samples, however,
showed a diminished particle volume. It is likely that this occurred from the washing out of
particles from the defect, which was a limitation of the surgical protocol since at the time of this
experiment the standardized stainless steel syringes described in section 2.B.3 were being
designed.
This study has indicated that PPI-doped cements, when delivered in particulate form, led
to a delayed degradation rate compared to the undoped samples. In addition, PPI samples were
also able to modulate the degradation of the materials at a controlled rate compared to the
controls. Based on these outcomes, further analyses of calcium phosphate cements,
Pantoprazole-calcium phosphate cements, and other commercially available biomaterials were
proposed.

Bafilomycin volume percentage
3.90 2.71
100 100123.98
58.22
020406080
100120140160180
1 week 3 weeks
Time points
Perc
enta
ge ParticlesDefectBone activity
Pantoprazole volume percentage
27.54 21.19
100 100.00116.95
83.90
0
20
40
6080
100
120
140
1 week 3 weeks
Time points
Perc
enta
ge ParticlesDefectBone activity
59
1.1.1.1
Figure 3.15 Bone and particulate volumes of calcium phosphate cements. Drug-loaded cements showed delayed degradation and increased reparative bone mass.
ParticlesDefectBone activity
ParticlesDefectBone activity
Omeprazole volume percentage
7.2 5.93
100 100
132.63
50.85
020406080
100120140160
1 week 3 weeks
Time points
Control volume percentage
19.073.39
100 100
127.12
43.64
020406080
100120140160180
1 week 3 weeks
Time points
Pecre
ant
gePe
rcen
age
t

603.B.4.2 MP x M
In the first stage of the in vivo implantation, MP and M were bilaterally implanted in rat
femora. Next, qualitative histological analyses using toluidine blue staining as well as
histomorphometric measurements for reparative bone and particulate using µCT were conducted.
Bone formation was found in all samples analyzed. MP samples showed increased mean
reparative bone volumes when compared to M at all intervals studied. However, the 5-day
(p=0.0312) and 5-week (p=0.0372) marks were the only one at which this difference was
statistically significant (Figure 3.16).
Similarly, particulate volumes of MP and M showed similar values without statistical
difference throughout the whole experimental period (Figure 3.17).
Toluidine Blue-stained resin-embedded sections of calcium phosphate cements showed a
large peri-implant bone deposition from 5 days to 2 weeks, from which point the bone
progressively remodelled until 6- to 7-week mark (Figure 3.18). At 7 weeks, only a thin mantle
of bone covered the surface of the particulate implants, which were replaced by bone over time
(Figure 3.19). The volumetric analyses of MP and M followed the same criteria shown in section
3.A.4 (Figure 3.10).

61
Figure 3.16 Bone volumes of MP and M. Particulate cements showed comparable bone volumes from 1 to 4 weeks and from 6 to 7 weeks.
igure 3.16 Bone volumes of MP and M. Particulate cements showed comparable bone volumes from 1 to 4 weeks and from 6 to 7 weeks.
Bone volume of calcium phosphate cements
0.36
0.63
0.47
0.640.610.62
0.57
0.380.32
0.26 0.270.17
0.240.16 0.13
0.00.10.20.30.40.50.60.70.80.9
5d 1w 2w 3w 4w
Intervals
Volu
me
(mm3 )
0.11
5w 6w 7w
MP M
Particle volume of calcium phos
0.160.18
0.160.18
0.15
0.17
0.120.14
0.12 0.1
0.00
0.05
0.10
0.15
0.20
0.25
5d 1w 2w 3w 4w
Intervals
Vol
ume
(mm3 )
phate cements
2
0.100.09
0.080.07
0.050.05
5w 6w 7w
Figure 3.17 Particle volumes of MP and M. ANOVA analysis of variance showed no statistical difference between the tested groups during the course of 7 weeks. Figure 3.17 Particle volumes of MP and M. ANOVA analysis of variance showed no statistical difference between the tested groups during the course of 7 weeks.
MP M

62
Figure 3.18 Histological sections. (A) M samples at 5 days and 2 weeks; (B) MP samples at 5 days and 2 weeks (FW=810µm).
A
B

63
C
Figure 3.19 Histosurrounding parti
c
D
logical sections at 6 weeks. (C) M and (D) MP: thin mantle of bone les (FW=810µm).

64
3.B.4.3 MP x Empty defect
In the second stage of the implantation of calcium phosphate cements, particulate MP
were unilaterally implanted in rat femora while the contra lateral sites were left empty. Empty
defects were considered completely healed when no trabecular bone was found in the marrow
cavity and total cortical bridging had occurred. The majority of empty defects showed healing in
the interval between 4 and 6 weeks. Similarly, MP-filled defects had their cortical bone closed at
6 weeks, with a net of trabecular bone still remaining surrounding the particles in the bone
marrow (Figure 3.21). At 16 weeks, MP particles were completely resorbed and the marrow
cavity was completely empty, which was confirmed by the histological examination (Figure
3.20). The volumetric analyses of empty defects and MP samples followed the same criteria
shown in section 3.A.4 (Figure 3.10).
Figure 3.20 Hthe marrow caat high resolut
istological section of MP at 16 weeks: particulate material resorbed completely in vity and some particles (dark dots) can only be seen embedded in the cortical bone ion (FW=142.3µm).

65
Figure 3.21 µCT slices 4 weeks; (B), (C), and (D) MP sparticulate volumes; (E) MP samremodelled with degradation of
A
of Mampl
par
B
C
pe
D
t
E
P and empty defects. (A) Defect’s closure in empty femur at le at 6 weeks: defect healing with cortical bridging, bone and at different depths at 16 weeks: reparative bone completely iculate implants.

66
3.C Other bone substitutes
3.C.1 MP, BioOssTM, BioGranTM, and AllogenixTM
The results of the volumetric analyses of BioOssTM, BioGranTM, and AllogenixTM were
compared with those of MP samples in the first and second stages of the in vivo implantation
experiments. SEM images and histological sections are shown in section 7.A.2.
In the quantitative bone measurements, shown in figure 3.22, all groups presented similar
volumes until 12 weeks. At 3 weeks post-operative, although MP showed increased values, the
reparative bone volumes showed insignificant differences among the groups. At 6 weeks post-
operative, BioGranTM showed statistically higher bone volumes compared to AllogenixTM
(p=0.0108). At 12 weeks post-operative, MP displayed statistically lower bone volumes
compared to all other biomaterials, BioGranTM presenting the highest volume (p=0.0463 for
BioOssTM x MP; p=0.0047 for BioGranTM x MP; p=0.0063 for AllogenixTM x MP). At 16 weeks
post-operative, MP bone volumes had almost completely remodelled whereas the other materials
still presented increased values (p=0.0325 for BioOssTM x MP; p=0.0006 for BioGranTM x MP;
p=0.0402 for AllogenixTM x MP). Particulate measurements of BioOssTM, BioGranTM, and MP are
shown in figure 3.23. At all intervals, the particulate volumes of BioOssTM and BioGranTM were
substantially higher than that of MP. At 3 weeks post-operative, similar volumes of BioOssTM
and BioGranTM were found (p=0.9801), while the comparison of these biomaterials with MP
revealed statistical significance (p=0.0002, for both BioOssTM x MP and BioGranTM x MP). At 6
weeks post-operative, BioOssTM and BioGranTM still presented comparable volumes (p=0.3104)
while MP particulate volume preserved its low values (p=0.0027 for BioOssTM x MP; p=0.0315
for BioGranTM x MP). At 12 weeks post-operative, BioOssTM and BioGranTM showed a slow
degradation rate with similar values (p=0.0875), whereas MP had almost completely resorbed
(p=0.0001 for BioOssTM x MP; p=0.0019 for BioGranTM x MP). Finally, at 16 weeks post-
operative, increased volumes of BioOssTM and BioGranTM were still found in the defects, while
MP particulate had completely remodelled. In contrast to literature reports 106, 134, BioGranTM
granules showed decreased cracks at all intervals. Area measurements for AllogenixTM
histological sections were conducted through the Image J Measure tool. Results of this analysis
showed increased putty values (3.35mm2 at 3weeks and 2.10mm2 at 16 weeks) and a decreased
degradation rate from 3 to 16 weeks (37.3%) (Figure 3.24).

67Bone volume of MP and commercially available biomaterials
0.0
0.1
0.2
0.3
0.4
0.5
3w 6w 12w 16w
Intervals
Vol
ume
(mm3 )
BioOss BioGran Allogenix MPFigure 3.22 Bone volumes for BioOssTM, BioGranTM, AllogenixTM, and MP. BioOssTM, BioGranTM, AllogenixTM displayed higher bone volume values than seen in the normal medullary cavity, with little sign of reparative bone remodelling while MP showed an increased remodelling profile until the 16-week mark.
Particle volume of MP and commercially available biomaterials
0.0
0.1
0.2
0.3
0.4
0.5
0.6
3w 6w 12w 16w
Intervals
Volu
me
(mm3 )
BioOss BioGran MPFigure 3.23 Particle volumes for BioOssTM, BioGranTM, and MP. At all intervals, significant smaller volumes were found for MP when compared to BioOssTM and BioGranTM. BioOssTM and BioGranTM showed little sign of degradation while MP was completely degraded in the period between the 14th and the 16th experimental weeks.

68
Area of Allogenix
0.0
0.1
0.2
0.3
0.4
0.5
0.6
3w 6w 12w 16w
Intervals
Are
a (m
m2 )
Allogenix Figure 3.24 Demineralized bone matrix area measurements. Increased values and a decreased degradation rate of the material were found. As AllogenixTM is not radio-opaque, these area measurements were derived from histological sections, as explained in the text.

69
4. DISCUSSION
4.A Characterization of hand- and machine-made calcium phosphate cements (H and M) The proposed experiments aimed to compare the characterization of calcium phosphate
cements prepared using the conventional, manual technique (H) and the novel, machine-based
method (M). The means of preparing calcium phosphate cements described herein is based on
the following logic: the manual-based method is dependent on the technique of the individual
preparing it and, therefore, is not reproducible. Machine-prepared cements (M), however, are
reproducible and displayed greater and more consistent hydroxyapatite (HA) conversion (section
3.B.1.1). Therefore, machine technology represents a standardized and controllable means of
obtaining calcium phosphate cements.
4.A.1 Particle size distribution and surface area of M are not different from those of H.
Measurements of particle size distribution, surface area, porosity, and pore sizes of four
calcium phosphate cement groups (as assessed by deriving data from SEM images as described
in section 2.B.1) were conducted using the Image J software.
Particle size distribution and surface area are interdependent characteristics which
influence the behaviour of bone substitutes. Particle size, surface area, porosity, and pore sizes of
calcium phosphate cements can all be adjusted. Varying (i) the powder to liquid ratio, (ii) the
particle sizes of the reagents, (iii) the proportions of the starting powders, (iv) the composition of
the reactants and (v) the aqueous solution, is one way. Adding nucleating agents to the setting
reaction is another 40, 46, 47. In addition, the milling of calcium phosphate cements may result in
materials with increased surface area and biological reactivity 40. As part of the premise of this
work, it was anticipated that machine-prepared cements would yield smaller particle sizes,
increased surface areas, higher porosity, and decreased pore sizes compared to hand-prepared
cements. However, the results have shown that neither the mixing techniques (hand mixing and
MM301) nor the grinding strategies (pestle and mortar and MM301) produced a difference in the
particle size distribution and surface area of the tested cements.
In the literature, the detailing of the hand-mixing techniques used to prepare calcium
phosphate cements is imprecise 33, 45, 156. These descriptions fail to convey a basic understanding
of how much mechanical activation was put into the material’s reaction, since a paste-like
consistency can occur almost immediately during the mixing. In contrast, as outlined in section
2.A.3.1, the solid and liquid phases of the hand-made cements tested in this work were
thoroughly mixed in a glass dish for 3 minutes using glass stirring-rods. Hence, since the starting

70chemistry was the same for all cements analyzed and based on the results shown herein, it
appears that the thorough hand-mixing of the cements and the machine-based protocol produced
similar activation effects on the materials.
4.A.2 M and H show overall similar porosity and pore size.
Microstructural features such as porosity and pore size have been accounted responsible
for the rate of drug delivery from calcium phosphate cements. Although it varies depending on
the starting wet chemistry, the porosity of the cements is usually higher than 30% while their
pore sizes is normally in a nano to micron scale 57. Porosity is usually obtained through the
calculation of the relative density of cement blocks. In the relative density calculation, a
measured density and an apparent density are assessed, the former being obtained by experiment
(helium pycnometry) and the latter being a result of calculations of the geometry and mass of the
blocks. The relative density is obtained by dividing the apparent density by the measured density 34, 156. The limitation of this methodology stems from the assumption (necessary to the
calculation of the blocks’ mass) that the whole calcium phosphate solid is composed of only one
product, hydroxyapatite in this case. In actual fact, the cement reaction could exhibit two or more
final products.
In the present work, calcium phosphate cement groups had their porosity quantified
through the analysis of SEM images. The percentage of pore surface area was quantified relative
to the total image area. This methodology is similar to that described by Gautier et al. (2000),
except that those authors examined SEM images of slices of calcium phosphate cement blocks.
They found a porosity range of 33.93±4.29 (for cements prepared by wet granulation) to
63.40±14.36 (for cements prepared by isostatic compression) 55. The findings of the present work
indicated a lowered porosity percentage for all groups (HM= 14.97%, MM=16%, H=16.2%,
M=18.47%). The difference may be attributable to this work’s analysis of the surface of the
cements as opposed to either the whole solid 34, 156 or several layers within a block of material 55.
The porosity comparison showed a higher porosity for M compared to HM (p=0.0438).
According to the statistical analyses (ANOVA + Tukey), the ground procedure (pestle and
mortar) accounted for the different values. Nevertheless, the isolated difference between M and
HM might have been the result of an uncontrolled and non-standardized pestle and mortar
technique used in the fabrication of M.
For the pore size measurements of HM, MM, H, and M, two groups were chosen:
micropores, for pores ≥1µm; and nanopores, for pores <1µm. This division was geared towards

71enabling a comparison with the literature reports 47, 57 and providing a better description of the
results through separated statistical analyses. Ideally, for a bone substitute to allow cellular in-
growth it should present interconnected pores with diameters ranging from 100 to 400µm.
Although the pore sizes of calcium phosphate cements are outside this range (nano scale to
10µm) 32, 149, 157, a cement with increased porosity and decreased pore sizes presents a more
complex surface topography, which should stimulate platelet degranulation and accelerate bone
healing 2, 3, 158.
Pore measurements of hand- and machine-made cements were in accordance with the
literature, varying from 130±2nm to 4.26±0.23µm. The micropore assessment did not display
significant differences among all studied groups, with values ranging from 3.68±0.05µm to
4.26±0.23µm (p=0.118). On the other hand, while the machine-made cements (M and MM)
presented similar nanopore values (0.22±0.03µm, p=0.1365), the hand-prepared groups (H and
HM) showed significantly different nanopore sizes compared to each other and to the other
groups (p<0.0001). According to ANOVA and Tukey analyses, the grinding technique and the
combination of the mixing and grinding strategies caused these differences. Interestingly, within
H and HM the nanopore sizes were significantly different, with HM presenting nanopores of
0.13±0.02µm and H having nanopores of 0.28±0.04µm (p<0.0001). Again, this might have been
due to the non-standardized hand technique used to fabricate these cements. This outcome is
clear evidence of the variability introduced when the hand technique is applied to prepare
calcium phosphate cements.
4.A.3 M and H present similar in vitro dissolutions at different pHs.
As with other ambient temperature produced apatites, calcium phosphate cements are
believed to be degraded mainly by cell activity such as osteoclastic resorption 31, 34, 47, 58, 72.
Accordingly, it is also inferred that calcium phosphate cements are partly degraded in vivo
through the dissolution of soluble end products of the cement reaction, often represented by the
un-reacted reagents DCPA and TTCP. Since the dissolution of both reagents is pH-dependent,
the body fluid’s ionic potential has a critical effect on the degradation rate of calcium phosphate
cements. The physiological pH is generally 7.4, which decreases within the extracellular
compartment (pH=6.4) 159 and becomes acidified in specific resorption spots (e.g., macrophage
subcellular milieu, pH=5.0) 160. Specifically, the dissolution of DCPA is facilitated in basic pH,
while TTCP is highly soluble in aqueous and acidic milieux 42. During the cement reaction,

72TTCP dissolves first and increases the pH of the system, which promotes the dissolution of
DCPA.
The in vitro dissolution of hand- and machine-made cements (H and M) was examined by
the immersion of these materials in solutions at different pHs (5.0, 6.4, and 7.4). AAS analysis
was conducted to measure the calcium concentrations of these solutions at specific intervals (1,
2, 3, and 4 weeks). As shown in section 3.B.1.1, the machine-prepared cements were converted
into more HA. Since HA is more stable than DCPA and TTCP in all three pHs (HA is soluble at
pHs 4.5-5.0), it was expected that the higher the HA content in the calcium phosphate cements,
the lower the calcium concentration in solution would be. As expected, the calcium
concentrations decreased with the increase of the pH (pH 5.0 > pH 6.4 > pH 7.4) at all intervals.
The increased calcium concentration of the cements at pH 5.0 was likely due to the complete
dissolution of the sub-products DCPA and TTCP and a substantial dissolution of the HA. The 1-
week interval at pH 5.0 showed increased dissolution values of H and M compared to 2, 3, and 4
weeks. Because the solutions could not be periodically changed to maintain a steady pH, as
suggested by Holy et al. (1999) 161, it was expected that at 1 week they would present a more
stable pH compared to the pHs at 2, 3, and 4 weeks. The reason for this increased dissolution
could be the stability of the solution for this initial interval (pH is closer to 5.0 than at 2, 3, and 4
weeks). The pHs were not periodically measured since the use of the pH meter probe would
contaminate the solutions with calcium, which in turn would interfere in the trace analysis done
by AAS.
Except for the first 2 weeks at pH 6.4 and at the 2-week interval at pH 7.4, the dissolution
of H and M revealed similar values. Based on these findings, it is suggested that the surface
characteristics, which were similar for both H and M, played a more important role in the in vitro
dissolution of these cements than their conversion into HA. Moreover, since M were expected to
present lower calcium concentration values, it is argued that the increased HA conversion of
these cements effectively interfered with their in vitro dissolution.
4.A.4 The particulate degradation rate and reparative bone remodelling are decreased for
machined- compared to hand-prepared cements.
The particle size and surface area of H and M have a direct influence on their degradation
rate and ability to act as osteoconductive biomaterials. In this context, the protocol used to
prepare M was suggested as a way to increase their surface area, consequently improving their
osteoconductivity. It was speculated that particulate size and surface area would influence the

73rate of occurrence, and even the occurrence itself, of phagocytosis of the cements by
macrophages. Macrophages and osteoclasts are derived from blood-borne monocytes. They are
responsible for the in vivo resorption of calcium phosphate cements, and increase in size during
either resorptive activity or in some diseases (e.g. Paget’s disease, periodontal disease, cancer) 162-164. Human osteoclasts have been reported to have diameters of 50µm-200µm 163, while
macrophage sizes varied from 200-400µm2 (22-44µm in diameter) in a mouse atherosclerosis
model 165. Macrophages are usually involved in the clearance of inflammatory debris through the
engulfment of foreign biomaterial particles, whereas osteoclasts resorb calcium phosphate
cements through an acidic secretion capable of dissolving the most stable product of the cement
reaction cascade: HA 59, 79, 166. On the contrary, HA ceramics have been reported to present a
slow osteoclastic resorption, which is a result of the high temperature sintering, and resultant
increased grain size, of these materials 99, 108. Therefore, the small crystallite size range of
calcium phosphate cements is critically important to their degradation, and their small particle
size range (from 90-200µm) is considered not to constrain their degradation through either
dissolution or cellular resorption. Particle degradation volumes for H and M showed similar
values for all intervals tested. The increased degradation within the first interval can be explained
by the decreased pH of the early healing milieu as well as the intense resorption activity of
macrophages and osteoclasts during this period. However, the degradation rate for M was 65%
and H degraded 77% from the first to the third week.
Another characteristic of great relevance in bone healing is the surface topography of
implanted materials. Specifically, biomaterials with complex surface topography have been
shown to accelerate healing, and favour bone-bonding through mechanical interdigitation of the
first bone matrix laid down by osteogenic cells (the cement line) and the submicron-scale
undercuts on the surface of the material 2, 167. Though the porosity and pore size of H and M were
not ideal for cell/vascular in-growth, their micron-scale surface with pore sizes in a
submicron/micron range were thought likely to accelerate endosseous healing (refer to SEM
images of H and M in figures 3.1, 3.4, and 3.6). Histomorphometric analyses were conducted to
measure the reparative bone formation achieved by implanted H and M at 1, 2, and 3 weeks post-
operative. At 2 weeks, peri-implant bone volumes were larger for M compared to H (p = 0.0311).
However, at 1 and 3 weeks the bone volumes were not significantly different. Nevertheless, from
the first to the third week, the remodelling rate for the reparative bone of H samples was 63%
while that of M samples was 55%. Together with the particulate degradation rates of M and H,

74this is evidence of more stable materials produced through the machine technique, although the
mean values were statistically insignificant.
Indeed, similar mean values for reparative bone and particulate degradation of H and M
were expected since the materials showed very similar surface characteristics. On the other hand,
despite the greater, and more consistent, HA conversion of M, an in vivo significance of the
increased HA content in the final biomaterial was not observed. Thus, while the M process
resulted in a more consistent reaction product which made the processing route more
reproducible, it may be necessary, in the future, to alter the initial reactants in order to achieve a
consistent, but different, end product (e.g. DCPA, TTCP, ß-TCP) in order to witness an
observable change in the biological reaction to the cement upon implantation in vivo. This may,
in turn, result in a changed osteoconductivity, increased bone formation, or modulated and
controllable degradation rate.
4.B Hand- and machine-made cements with and without Pantoprazole (H, M, HP, MP) Pantoprazole was included on the basis of results obtained from previous experiments
within the Bone Interface Group: in the first set of experiments, a macrolide antibiotic
(Bafilomycin A1) with the ability to inhibit the osteoclastic proton pump was incorporated into
calcium phosphate cement rods and generated not only a means of controlling the resorption of
these materials, but also an increase in peri-implant bone volume in a rat femoral model 64. In a
second set of experiments, using the same rodent model, the incorporation of Pantoprazole and
Omeprazole into cement rods helped control the degradation of the implanted materials 78.
In the present work, the evaluation of hand- and machine-made calcium phosphate
cements (H and M) and their loading with Pantoprazole (HP and MP) comprised the following
assays: (i) the HA conversion and dissolution profile of these cements in saline (pH 7.4), (ii) the
release profile of Pantoprazole from calcium phosphate cements (HP and MP), (iii) the effect of
Pantoprazole on the in vivo degradation of machine-made cements, and (iv) the comparison of
the degradation rate and reparative bone formation of MP against BioOss™ (anorganic bone),
BioGran™ (Bioactive glass), and Allogenix™ (Demineralized bone matrix).
4.B.1 MP exhibit higher HA conversion and decreased dissolution at pH 7.4.
In order to compare the HA conversion rates of H, M, HP, and MP, these cements were
snap-frozen to stop their reaction at specific intervals, and analyzed by x-ray diffraction analysis
(PXRD). According to these measurements, HA, DCPA, TTCP, and beta-tricalcium phosphate

75(ß-TCP) were the end products of the reaction. Across all intervals tested, DCPA showed varied
quantities as an end product of the reaction (4-47%), TTCP presented amounts from 4% to 16%,
and minimal ß-TCP amounts were found (0.4 to 14%). As described by Liu et al. (2003) and
Miyamoto et al. (1997), the amount of DCPA in the final cement was the main determinant for
the HA conversion 46, 49. Accordingly, this experiment showed that for the cements with less
DCPA as an end product, a higher HA amount was found. For all intervals analyzed, the
machine-made cements (M and MP) presented statistically higher HA contents than the hand-
made cements (H and HP). MP presented an initial HA percentage of 73% at 1 day and 88% at 8
weeks, which was statistically significant (p<0.0001) compared to M (62% at 1 day, 70% at 8
weeks), the second highest in HA conversion. ANOVA combined with TUKEY post-hoc
analysis identified both the mixing technique and the adding of Pantoprazole as causal factors for
the HA conversion differences among the groups. Interestingly, the doped cements showed
consistent, increased HA percentages compared to all other materials. Interestingly, a similar
effect was described by Zhang et al. (2006) after the incorporation of mannitol into self-setting
calcium phosphate scaffolds. Different concentrations of mannitol increased the HA conversion
of these materials until a steady rate was reached. It was hypothesized that the fast dissolution of
mannitol formed micropores, which increased the surface area of the cement and improved the
hydration rates of DCPA and TTCP 45. In the case of Pantoprazole, the drug may have helped the
hydration of the cement reactants by interfering in the pH changes of the setting reaction.
A dissolution analysis of H, HP, M, and MP in saline at pH 7.4 was also conducted. It
was expected that a higher conversion into HA would make calcium phosphate cements capable
of being degraded mainly through the osteoclastic activity as opposed to through dissolution in
vivo. Lower calcium concentration values would thus be found in solution with the cements with
higher HA content (MP in this case). Indeed, results showed that the cements with higher HA
amount (MP) did display decreased dissolution values than the other cements. No difference was
found among H, HP, and M at all intervals. In contrast, at almost all intervals, the comparison
between MP and the other groups showed a statistically significant difference. In cases where the
differences were not statistically significant, borderline values were found (p=0.0608 against M
at 10 weeks). From these findings it can be inferred that an increase in the number of samples
analyzed could show significance in these differences. Overall, although at 10 weeks all groups
presented similar dissolution profiles, the cements with increased HA conversion (MP) showed
decreased calcium concentrations during all intervals analyzed.

76Interestingly, M and MP showed gradually ascending dissolution values until the 4-week
mark, after which point they descended to a plateau through the final intervals of the experiment.
Conversely, uneven dissolution profiles with calcium concentration peaks and valleys were
found for H and HP. The saline solutions used had an initial pH of 5.5, which was calibrated to
pH 7.4 using HCl and NaOH solutions. One limitation of this model is the impossibility of
maintaining a stable pH for all solutions over such long intervals. Therefore, it is possible that
pH changes occurred in these solutions during the experiment. If so, varied calcium
concentration values for the presumably less stable cements (H and HP) might have been caused
by the possible pH changes of the saline solutions.
4.B.2 MP and HP sustain the in vitro release of Pantoprazole until the drug starts to
degrade.
Major advances have been made in the development of new materials to be used for the
delivery of drugs to a local area of interest. Two advances include: achieving the sustained
release of a therapeutic agent while minimizing the concentrations of the drug in the bloodstream
and other organs; and reducing the potential side-effects produced by systemic administration 61.
In particular, implanted calcium phosphate cements are a means of locally targeting and
delivering agents to a site with a view to accelerating and promoting desired biological
responses.
The release of a PPI from hand- and machine-made calcium phosphate cements was
assessed. Specifically, MP and HP were immersed in saline (pH 7.4) and the concentration of
Pantoprazole was measured using its UV absorbance through spectrophotometric analysis. The
UV absorbance of Pantoprazole was measured at 292 nm and the final concentration of the
cement/saline system was 12.5µg/ml. A comparison between the absorbance values of
Pantoprazole standard solutions and those of MP and HP described the release kinetics of the
drug from the cements. The analysis of Pantoprazole standard solutions showed that the
absorbance values increased with the increase of the drug concentration until a plateau was
reached. UV absorbance evaluation of Pantoprazole from saline solutions with HP and MP
revealed similar kinetics, with no burst effect and a sustained release of the drug within the first 5
days analyzed (between 2.0 µg/ml at 2 hours and 10 µg/ml ate 5 days). However, after 5 days the
absorbance values of Pantoprazole began to increase significantly, reaching values higher than
its initial concentration. This timing is coincident with the formation of yellowish clumps on the
bottom of the vials and a change in the colour of the solution. Pantoprazole is acid-labile and

77several methods have been described to measure efficiently the UV absorbance of this drug in
solution 168-170. As a result, the stability of Omeprazole and Pantoprazole solutions was tested and
it was found that the best UV resolution and a maximal stability of 48 hours were attained when
a basic solution (pH 9.0) was used 170. The storage of OMP at pH 7.5-10.0 was recommended for
4 days at room temperature 171. Therefore, since the drug was stored in a saline solution at 37ºC
for a prolonged time, it was hypothesized that it had denatured after 5 days in solution, which
caused increased UV absorbance readings. Overall, HP and MP served as efficient drug carriers,
maintaining the release of Pantoprazole at stable concentrations until the drug became denatured.
4.B.3 Pantoprazole does not alter the in vivo degradation of calcium phosphate cements.
Since the in vivo outcomes of the implantation of hand- and machine-made calcium
phosphate cements had shown similar results, only machine-made cements were tested in this
experiment (M and MP). Pantoprazole salt was incorporated into the solid phase of MP aiming to
evenly distribute the drug within the cement matrix. This drug is highly soluble in aqueous
solutions and was expected to be released before the complete degradation of the cements in the
femoral defects. Along with the drug solubility, the microstructural characteristics of the cement
(porosity, tortuosity) were also expected to interfere in the drug delivery. Based on the increased
HA conversion of MP, and on the fact that Pantoprazole would inhibit osteoclastic resorption, it
was thought that MP degradation would take longer than that of M.
MP and M were bilaterally implanted in rat femora and their in vivo outcomes (reparative
bone and particulate volumes) were calculated at 5 days and 1-7 weeks post-operative. Except
for the 5-day and 5-week intervals, µCT data of peri-implant bone volumes of M and MP
showed similar values. Similarly, the degradation rates of the particulate cements revealed no
statistical differences. It was hypothesized that these similar values for bone and particulate
volumes could be the result of two factors:
(i) The instability of Pantoprazole. It was expected that most of Pantoprazole’s delivery
would happen as the cements were being resorbed by the osteoclasts, in which case, the drug
would perform its proton pump inhibition function in an acidic milieu (as it occurs in GERD).
However, since Pantoprazole is highly soluble at physiological pH, its rapid delivery within the
implantation bed (with a pH of approximately 7.4) may have hindered its functionality.
(Pantoprazole is acid-labile and may be denatured after 5 days in physiological pH, as discussed
in section 4.B.2.)

78(ii) Pantoprazole reacted with the cement to form HA. As discussed in 4.B.1, calcium
phosphate cements with Pantoprazole displayed a higher HA conversion. This effect was
suggestive of an interference by the drug on the cement reaction, possibly through a pH change.
Thus, since Pantoprazole is acid-labile and was involved in an acid-base reaction, it is
hypothesized that, after reacting with the cement reagents, the drug lost its ability to function as a
PPI.
4.B.4 MP provide an osteoconductive scaffold for bone formation and are completely
resorbed in rat femoral defects after 16 weeks of implantation.
Once implanted, calcium phosphate cements perform their osteoconductive function and
are gradually degraded through both dissolution of their soluble components and osteoclastic
resorption. Of the two processes, the osteoclastic resorption is the more beneficial since it
resembles the natural bone turnover. In a first experimental stage, MP was unilaterally implanted
in rat femora while the contra-lateral side was left empty. This assay aimed to describe the
degradation profile of MP as well as to indicate whether these cements would impair the healing
of the defect. The results showed that the empty defects healed completely in the period between
the 4th and 6th weeks post-operative. Complete healing was assessed by the bridging of the
cortical bone and the absence of reparative trabecular bone within the marrow. Therefore, for MP
to not represent a constraint on normal healing, it would delay (as do all other bone fillers) but
not prevent the closure of the defect. In other words, it should offer an osteoconductive scaffold
for bone matrix to be secreted, but not stay un-resorbed beyond the point at which a stable host
tissue is able to respond properly to the trauma. Indeed, the defects filled with MP had their
cortical bone bridged at 6 weeks, but a highly interconnected trabecular reparative bone was
found within the marrow cavity until the 12th week post-operative. By the 16th week post-
operative the particulate cement had completely resorbed.
In a second experiment, the reparative bone formation and degradation rate of MP was
compared to that of commercially available materials (BioOss™, BioGran™, and Allogenix™).
Specifically, histomorphometric measurements of these materials were taken at 3, 6, 12 and 16
weeks post-operative.
At 3 weeks, MP showed the highest bone volume, followed by BioGran™, BioOss™, and
Allogenix™, in that order. However, theses differences were not statistically significant. At 6
weeks, BioGran™ samples presented the highest values for bone volume, which was significant
only when compared to Allogenix™ samples (p=0.0108). At 12 weeks, BioGran™, BioOss™, and

79Allogenix™ showed similar bone volumes, whereas MP showed significant bone remodelling
(p=0.0463 for BioOss™ x MP; p=0.0047 for BioGran™ x MP; p=0.0063 for Allogenix™ x MP).
At 16 weeks, increased bone values of BioOss™, BioGran™, and Allogenix™ were found,
whereas MP bone volumes had almost completely remodelled (p=0.0325 for BioOss™ x MP;
p=0.0006 for BioGran™ x MP; p=0.0402 for Allogenix™ x MP). On the other hand, BioOss™,
BioGran™ and Allogenix™ presented little to no bone remodelling throughout the whole
experiment. During early peri-implant healing, osteoconductive materials stimulate the
recruitment and migration of osteogenic cells, which deposit bone matrix onto these material
surfaces. An ideal biomaterial would stimulate increased bone formation during early endosseous
healing but, over time, should be remodelled by the joint activity of osteoclasts and osteoblasts.
BioOss™, BioGran™, and Allogenix™ displayed biocompatibility and osteoconductivity,
invoking bone formation at 3 and 6 weeks post-operative. However, at the 12- and 16-week
marks BioOss™, BioGran™, and Allogenix™ showed increased bone volumes, which is
characteristic of incomplete or absent remodelling.
The particulate volume of MP, BioOss™, and BioGran™ was measured using microCT
analysis, while the area of DBM was obtained from histological sections, since DBM is not
radiodense enough to be visualized through microCT. At 3 weeks, the volumes of BioOss™ and
BioGran™ were similar and substantially higher than those of MP. At 6, 12, and 16 weeks
BioOss™ volumes were almost kept the same, whereas a gradual slow degradation was found for
BioGran™. BioOss™ and BioGran™ showed statistically higher volumes than MP for all intervals
analyzed. At 16 weeks, MP particles could not be found in the marrow cavity for the majority of
the samples. Results of the Allogenix™ area analysis showed consistently high values with a low
degradation rate from 3 to 6 weeks. However, although the degradation rate of the putty material
increased from 6 to 16 weeks, high volumes of DBM were still found at 16 weeks post-operative.
BioOss™, BioGran™, and Allogenix™ have all shown to be osteoconductive with
increased bone volume at all intervals studied. In contrast, these materials displayed a poor in
vivo resorbability. BioOss™’ slow degradation rate may be attributable to its high temperature
sintering process and increased particle size (250-1000µm). On the other hand, the degradation
rate of BioGran™ depends on cracks that are eventually formed in the implanted glass granules
and, since the present experiment revealed that only a small amount of the implanted glasses had
cracked, a slow in situ degradation was found. Finally, since Allogenix™ is not porous and does
not favour cellular in-growth, the resorption of this material may have occurred by osteoclastic

80activity only on its surface, which may explain its slow degradation (refer to figure 7.8, where an
increased amount of the material with little sign of degradation is seen).
The results presented herein showed that low volumes of particulate MP could stimulate
similar reparative bone volumes to those of high material volumes of BioOss™, BioGran™, and
Allogenix™. MP is a particulate material mainly composed of a HA formed at room temperature.
It presents particle sizes ranging from 90-355µm, high surface area, increased porosity, and a
nano-microporous structure. These MP materials were able to promote an increased reparative
bone formation yet were resorbed within the 16-week experimental period. These improved in
vivo outcomes (compared to BioOss™, BioGran™, and Allogenix™) may be a result of the
combination of their complex surface topography, decreased particle size, and low temperature
synthesized HA (which presents faster degradation than ceramic HA).

81 5. CONCLUSIONS
From the work reported herein, it can be concluded that:
Despite the changes instituted in cement preparation, the majority of surface
characteristics and the dissolution rates at different pHs did not differ among the
cement groups examined.
One exception to the above was that machine-made cements displayed less
variability in surface porosity than hand-made cements.
Machine-prepared cements showed a less variable, and increased, HA conversion;
a more stable, and decreased, in vitro dissolution at pH 7.4; and decreased bone and
particulate degradation rates than hand-made cements.
Hand- and machine-prepared cements showed similar, and sustained,
Pantoprazole release profiles until the drug denatured.
The incorporation of Pantoprazole to calcium phosphate cements did not affect
the in vivo behaviour of these biomaterials.
Machine-prepared cements showed increased early bone formation but an
improved degradation compared to three currently available commercial bone
substitute materials tested.

82 6. REFERENCES 1. Einhorn, T. A. The cell and molecular biology of fracture healing. Clin Orthop Relat Res, S7-21 (1998). 2. Cohen, I. K., Diegelmann, R. F. & Lindblad, W. J. Wound healing- Biochemical & Clinical aspects (1992). 3. Davies, J. E. Bone bonding at natural and biomaterial surfaces. Biomaterials 28, 5058-67 (2007). 4. Davies, J. E. Understanding peri-implant endosseous healing. Journal of Dental Education 8, 932-949 (2005). 5. Iacono, V. J. Dental implants in periodontal therapy. J Periodontol 71, 1934-42 (2000). 6. Davies, J. E. & Hosseini, M. M. Histodynamics of endosseous wound healing (ed. Davies, J. E.) (em squared, Toronto, 2000). 7. Simmons, D. J. Fracture healing perspectives. Clin Orthop Relat Res, 100-13 (1985). 8. Malcolm, A. J. Basics of fracture healing (ed. Gregg, P. J., Stevens, J., Worlock, P. H.) (Blackwell Science Ltd., Oxford, 1996). 9. Anderson, J. M. The cellular cascades of wound healing (ed. Davies, J. E.) (em squared, Toronto, 2000). 10. Cornell, C. N. & Lane, J. M. Newest factors in fracture healing. Clin Orthop Relat Res, 297-311 (1992). 11. Klinger, M. H. F. Platelets and inflammation. Anat Embryol 196, 1-11 (1997). 12. Hosseini, M. M. in On the relationship between osteoconduction and surface texture during peri-implant osteogenesis. Institute of Biomaterials and Biomedical Engineering (University of Toronto, Toronto, 2002). 13. Bieber, E. J. & Wood, M. B. Bone Reconstruction. Clinics in Plastic Surgery 13, 645-655 (1986). 14. Broughton, G., Janis, J. E. & Attinger, C. E. The basic science of wound healing. Plast Reconstr Surg 117(7), 12S-34S (2006). 15. Cardaropoli, G., Araujo, M. & Lindhe, J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J Clin Periodontol 30, 809-18 (2003). 16. Listgarten, M. A. Soft and hard tissue response to endosseous dental implants. Anat Rec 245, 410-25 (1996).

83 17. Amler, M. H. The time sequence of tissue regeneration in human extraction wounds. Oral Surg Oral Med Oral Pathol 27, 309-18 (1969). 18. Chau, J. in Development of an outer cortical bone model for the investigation of bone/implant healing. Institute of Biomaterials and Biomedical Engineering (University of Toronto, Toronto, 2007). 19. Carano, R. A. & Filvaroff, E. H. Angiogenesis and bone repair. Drug Discov Today 8, 980-9 (2003). 20. Franchi, M., Fini, M., Gianluca, G. & Vittoria, O. Peri-implant osteogenesis in health and osteoporosis. Micron 36, 630-44 (2005). 21. Patan, S. Vasculogenesis and angiogenesis as mechanisms of vascular network formation, growth and remodeling. J Neurooncol 50, 1-15 (2000). 22. Lind, M. Growth factor stimulation of bone healing. Effects on osteoblasts, osteomies, and implants fixation. Acta Orthop Scand Suppl 283, 2-37 (1998). 23. Karp, J. M. et al. Thrombin mediated migration of osteogenic cells. Bone 37, 337-48 (2005). 24. Aubin, J. E. in Bone Engineering (ed. Davies, J. E.) 19-30 (em squared incorporated, Toronto, 2000). 25. Sodek, J., Cheifetz, S. in Bone Engineering (ed. Davies, J. E.) 31-43 (em squared incorporated, Toronto, 2000). 26. Davies, J. E., Nagai, N., Takeshita, N., Smith, D. C. in The bone-biomaterial interface (ed. Davies, J. E.) 285-294 (em squared, Toronto, 1991). 27. Davies, J. E. In vitro modeling of the bone/implant interface. Anat Rec 245, 426-45 (1996). 28. McKee, M. D. & Nanci, A. Osteopontin at mineralized tissue interfaces in bone, teeth, and osseointegrated implants: ultrastructural distribution and implications for mineralized tissue formation, turnover, and repair. Microsc Res Tech 33, 141-64 (1996). 29. Roberts, W. E. Bone tissue interface. J Dent Educ 52, 804-9 (1988). 30. Brown, W., Chow, I. C. Combinations of sparingly soluble calcium phosphates in slurries and paste as mineralizers and cements. US patent 4612053 (1987). 31. Apelt, D. et al. In vivo behavior of three different injectable hydraulic calcium phosphate cements. Biomaterials 25, 1439-51 (2004). 32. LeGeros, R. Z. & LeGeros, J. P. Calcium phosphate bioceramics: past, present and future. Kev Engineering Materials 240-242, 2-10 (2003).

84 33. Ishikawa, K., Takagi, S., Chow, L. C. & Suzuki, K. Reaction of calcium phosphate cements with different amounts of tetracalcium phosphate and dicalcium phosphate anhydrous. J Biomed Mater Res 46, 504-10 (1999). 34. Lilley, K. J., Gbureck, U., Wright, A. J., Farrar, D. F. & Barralet, J. E. Cement from nanocrystalline hydroxyapatite: effect of calcium phosphate ratio. J Mater Sci Mater Med 16, 1185-90 (2005). 35. Bohner, M., Lemaitre, J., Merkle, H. P. & Gander, B. Control of gentamicin release from a calcium phosphate cement by admixed poly(acrylic acid). J Pharm Sci 89, 1262-70 (2000). 36. Brown, W. E. & Chow, L. C. A new calcium phosphate setting cement. J. Dent. Res. 62, 672 (1983). 37. Ambard, A. J. & Mueninghoff, L. Calcium phosphate cement: review of mechanical and biological properties. J Prosthodont 15, 321-8 (2006). 38. Fukase, Y., Eanes, E. D., Takagi, S., Chow, L. C. & Brown, W. E. Setting reactions and compressive strengths of calcium phosphate cements. J Dent Res 69, 1852-6 (1990). 39. Frayssinet, P. et al. Tissue reaction against a self-setting calcium phosphate cement set in bone or outside the organism. J Mater Sci Mater Med 11, 811-5 (2000). 40. Bohner, M., Gbureck, U. & Barralet, J. E. Technological issues for the development of more efficient calcium phosphate bone cements: a critical assessment. Biomaterials 26, 6423-9 (2005). 41. Kohri, M., Miki, K., Waite, D. E., Nakajima, H. & Okabe, T. In vitro stability of biphasic calcium phosphate ceramics. Biomaterials 14, 299-304 (1993). 42. Elliot, J. C. Structure and chemistry of the apatites and other calcium orthophosphates (Elsevier, Amsterdam, London, New York, Tokyo, 1994). 43. Hamanishi, C., Kitamoto, K., Ohura, K., Tanaka, S. & Doi, Y. Self-setting, bioactive, and biodegradable TTCP-DCPD apatite cement. J Biomed Mater Res 32, 383-9 (1996). 44. Xu, H. H., Quinn, J. B., Takagi, S. & Chow, L. C. Processing and properties of strong and non-rigid calcium phosphate cement. J Dent Res 81, 219-24 (2002). 45. Zhang, Y., Xu, H. H., Takagi, S. & Chow, L. C. In-situ hardening hydroxyapatite-based scaffold for bone repair. J Mater Sci Mater Med 17, 437-45 (2006). 46. Liu, C., Shao, H., Chen, F. & Zheng, H. Effects of the granularity of raw materials on the hydration and hardening process of calcium phosphate cement. Biomaterials 24, 4103-13 (2003). 47. Ginebra, M. P., Traykova, T. & Planell, J. A. Calcium phosphate cements as bone drug delivery systems: a review. J Control Release 113, 102-10 (2006).

8548. Chow, I. C. Calcium phosphate cements: cehmistry, properties, and applications. Materials Research. Society Symposim Proceedings 599, 27-37 (2000). 49. Miyamoto, Y. et al. Tissue response to fast-setting calcium phosphate cement in bone. J Biomed Mater Res 37, 457-64 (1997). 50. Visentin, L. et al. A selective inhibitor of the osteoclastic V-H(+)-ATPase prevents bone loss in both thyroparathyroidectomized and ovariectomized rats. J Clin Invest 106, 309-18 (2000). 51. Trehan, A. & Ali, A. Recent approaches in insulin delivery. Drug Dev Ind Pharm 24, 589-97 (1998). 52. Saudek, C. D. Novel forms of insulin delivery. Endocrinol Metab Clin North Am 26, 599-610 (1997). 53. Irsigler, K., Kritz, H. & Lovett, R. G. Controlled drug delivery in the treatment of diabetes mellitus. Crit Rev Ther Drug Carrier Syst 1, 189-280 (1985). 54. El-Ghannam, A., Ahmed, K. & Omran, M. Nanoporous delivery system to treat osteomyelitis and regenerate bone: gentamicin release kinetics and bactericidal effect. J Biomed Mater Res B Appl Biomater 73, 277-84 (2005). 55. Gautier, H., Merle, C., Auget, J. L. & Daculsi, G. Isostatic compression, a new process for incorporating vancomycin into biphasic calcium phosphate: comparison with a classical method. Biomaterials 21, 243-9 (2000). 56. Ratier, A. et al. Setting characteristics and mechanical behaviour of a calcium phosphate bone cement containing tetracycline. Biomaterials 22, 897-901 (2001). 57. Ginebra, M. P., Traykova, T. & Planell, J. A. Calcium phosphate cements: competitive drug carriers for the musculoskeletal system? Biomaterials 27, 2171-7 (2006). 58. Farina, C. & Gagliardi, S. Selective inhibitors of the osteoclast vacuolar proton ATPase as novel bone antiresorptive agents. Drug Discov Today 4, 163-172 (1999). 59. Barroug, A. & Glimcher, M. J. Hydroxyapatite crystals as a local delivery system for cisplatin: adsorption and release of cisplatin in vitro. J Orthop Res 20, 274-80 (2002). 60. Takechi, M., Miyamoto, Y., Ishikawa, K., Nagayama, M., Kon, M., Asaoka, K., Suzuki, K. Effects of added antibiotics on the basic properties of anti-washout-type fst-setting calcium phosphate cement. J. Biomed. Mater. Res. 39, 308-316 (1998). 61. Takechi, M., Miyamoto,Y., Momota, Y., Yuasa, T., Tatehara, S., Nagayama, M., Ishikawa, K., Suzuki, K. The in vitro antibiotic release from anti-washout apatite cement using chitosan. J. Mater. Sci., Mater. Med. 13, 973-978 (2002).

8662. Blom, E. J., Klein-Nulend, J., Yin, L., van Waas, M. A. & Burger, E. H. Transforming growth factor-beta1 incorporated in calcium phosphate cement stimulates osteotransductivity in rat calvarial bone defects. Clin Oral Implants Res 12, 609-16 (2001). 63. Steffen, T., Stoll, T., Arvinte, T. & Schenk, R. K. Porous tricalcium phosphate and transforming growth factor used for anterior spine surgery. Eur Spine J 10 Suppl 2, S132-40 (2001). 64. Rzeszutek, K., Sarraf, F. & Davies, J. E. Proton pump inhibitors control osteoclastic resorption of calcium phosphate implants and stimulate increased local reparative bone growth. J Craniofac Surg 14, 301-7 (2003). 65. del Real, R. P., Ooms, E., Wolke, J. G., Vallet-Regi, M. & Jansen, J. A. In vivo bone response to porous calcium phosphate cement. J Biomed Mater Res A 65, 30-6 (2003). 66. Okada, E., Maruyama, Y. & Hayashi, A. Nasal augmentation using calcium phosphate cement. J Craniofac Surg 15, 102-5 (2004). 67. Schliephake, H., Gruber, R., Dard, M., Wenz, R. & Scholz, S. Repair of calvarial defects in rats by prefabricated hydroxyapatite cement implants. J Biomed Mater Res A 69, 382-90 (2004). 68. Yuan, H., Li, Y., de Bruijn, J. D., de Groot, K. & Zhang, X. Tissue responses of calcium phosphate cement: a study in dogs. Biomaterials 21, 1283-90 (2000). 69. Seeherman, H. J., Bouxsein, M., Kim, H., Li, R., Li, X. J., Aiolova, M. et al. Recombinant human bone morphogeneticprotein-2 delivered in an injectable calclium phosphate paste accelerates osteotomy-site healing in a non-human primate model. J Bone Jt Surg A 86, 1961-1973 (2004). 70. Seeherman, H. J., Li, R., Wozney, J. M. A review of preclinical program development for evaluating injectable carriers for osteogenic factors. J Bone Jt Surg A 85, 96-111 (2003). 71. Ohura, K., Hamanishi, C., Tanaka, S., Matsuda, N. Healing of segmental bone defects in rats induced by a B-TCP-MCPM cement combined with rhBMP-2. J Biomed Mater Res 44, 168-175 (1999). 72. Ooms, E. M., Wolke, J. G., van de Heuvel, M. T., Jeschke, B. & Jansen, J. A. Histological evaluation of the bone response to calcium phosphate cement implanted in cortical bone. Biomaterials 24, 989-1000 (2003). 73. Chambers, T. J. Regulation of the differentiation and function of osteoclasts. J Pathol 192, 4-13 (2000). 74. Boyle, W. J., Simonet, W. S. & Lacey, D. L. Osteoclast differentiation and activation. Nature 423, 337-42 (2003). 75. Troen, B. R. Molecular mechanisms underlying osteoclast formation and activation. Exp Gerontol 38, 605-14 (2003).

87 76. Udagawa, N. Mechanisms involved in bone resorption. Biogerontology 3, 79-83 (2002). 77. Udagawa, N. et al. Osteoblasts/stromal cells stimulate osteoclast activation through expression of osteoclast differentiation factor/RANKL but not macrophage colony-stimulating factor: receptor activator of NF-kappa B ligand. Bone 25, 517-23 (1999). 78. Sheraly, A. R. in Use of gastric proton pump inhibitors to modulate osteoclast-mediated resorption of calcium phosphate cements. (University of Toronto, Toronto, 2005). 79. Farina, C. et al. Novel bone antiresorptive agents that selectively inhibit the osteoclast V-H+-ATPase. Farmaco 56, 113-6 (2001). 80. Altman, K. W., Haines, G. K., 3rd, Hammer, N. D. & Radosevich, J. A. The H+/K+-ATPase (proton) pump is expressed in human laryngeal submucosal glands. Laryngoscope 113, 1927-30 (2003). 81. Fejes-Toth, G. & Naray-Fejes-Toth, A. Immunohistochemical localization of colonic H-K-ATPase to the apical membrane of connecting tubule cells. Am J Physiol Renal Physiol 281, F318-25 (2001). 82. Verlander, J. W., Moudy, R. M., Campbell, W. G., Cain, B. D. & Wingo, C. S. Immunohistochemical localization of H-K-ATPase alpha(2c)-subunit in rabbit kidney. Am J Physiol Renal Physiol 281, F357-65 (2001). 83. Pestov, N. B. et al. Identification of the beta-subunit for nongastric H-K-ATPase in rat anterior prostate. Am J Physiol Cell Physiol 286, C1229-37 (2004). 84. Johansson, M., Jansson, T., Pestov, N. B. & Powell, T. L. Non-gastric H+/K+ ATPase is present in the microvillous membrane of the human placental syncytiotrophoblast. Placenta 25, 505-11 (2004). 85. Baron, R., Neff, L., Louvard, D. & Courtoy, P. J. Cell-mediated extracellular acidification and bone resorption: evidence for a low pH in resorbing lacunae and localization of a 100-kD lysosomal membrane protein at the osteoclast ruffled border. J Cell Biol 101, 2210-22 (1985). 86. Drose, S. & Altendorf, K. Bafilomycins and concanamycins as inhibitors of V-ATPases and P-ATPases. J Exp Biol 200, 1-8 (1997). 87. Farina, C. & Gagliardi, S. Selective inhibition of osteoclast vacuolar H(+)-ATPase. Curr Pharm Des 8, 2033-48 (2002). 88. Mattsson, J. P., Vaananen, K., Wallmark, B. & Lorentzon, P. Omeprazole and bafilomycin, two proton pump inhibitors: differentiation of their effects on gastric, kidney and bone H(+)-translocating ATPases. Biochim Biophys Acta 1065, 261-8 (1991). 89. Poole, P. Pantoprazole. Am J Health Syst Pharm 58, 999-1008 (2001).

8890. Cheer, S. M., Prakash, A., Faulds, D. & Lamb, H. M. Pantoprazole: an update of its pharmacological properties and therapeutic use in the management of acid-related disorders. Drugs 63, 101-33 (2003). 91. Jungnickel, P. W. Pantoprazole: a new proton pump inhibitor. Clin Ther 22, 1268-93 (2000). 92. Fitton, A. & Wiseman, L. Pantoprazole. A review of its pharmacological properties and therapeutic use in acid-related disorders. Drugs 51, 460-82 (1996). 93. Tuukkanen, J. & Vaananen, H. K. Omeprazole, a specific inhibitor of H+-K+-ATPase, inhibits bone resorption in vitro. Calcif Tissue Int 38, 123-5 (1986). 94. Horn, J. The proton-pump inhibitor: similarities and differences. Clinical Therapeutics 22, 266-280 (2000). 95. Shin, J. M., Cho, Y. M. & Sachs, G. Chemistry of covalent inhibition of the gastric (H+, K+)-ATPase by proton pump inhibitors. J Am Chem Soc 126, 7800-11 (2004). 96. Nishioka, K., Nagao, T. & Urushidani, T. Correlation between acid secretion and proton pump activity during inhibition by the proton pump inhibitors omeprazole and pantoprazole. Biochem Pharmacol 58, 1349-59 (1999). 97. Shin, J. M. & Sachs, G. Differences in binding properties of two proton pump inhibitors on the gastric H+,K+-ATPase in vivo. Biochem Pharmacol 68, 2117-27 (2004). 98. Senn, N. On the healing of aseptic bone cavities by implantation of antiseptic decalcified bone. Amer. J. Med. Sci. 98, 219-243 (1889). 99. Damien, C. J., Parsons, J. R. Bone graft and bone graft substitutes: a review of current technology and applications. Journal of Applied Biomaterials 2, 187-208 (1991). 100. Finkemeier, C. G. Bone-grafting and bone-graft substitutes. J Bone Joint Surg Am 84-A, 454-64 (2002). 101. Hurzeler, M. B., Quinones, C. R., Kirsch, A., Gloker, C., Schupbach, P., Strub, J. R., Caffesse, R. G. Maxillary sinus augmentation using different grafting materials and dental implants in monkeys. Part I. Evaluation of anorganic bovine-derived bone matrix. Clin Oral Implants Res 8, 476-86 (1997). 102. Giannoudis, P. V., Dinopoulos, H. & Tsiridis, E. Bone substitutes: an update. Injury 36 Suppl 3, S20-7 (2005). 103. Bloemers, F. W. et al. Autologous bone versus calcium-phosphate ceramics in treatment of experimental bone defects. J Biomed Mater Res B Appl Biomater 66, 526-31 (2003). 104. Ludwig, S. C., Kowalski JM, Boden SD. Osteoinductive bone graft substitutes. Eur Spine J 9, 119-125 (2000).

89105. Perry, C. R. Bone repair thecniques, bone graft, and bone grafts substitutes. . Clinical Orthopaedics and related research 360, 71-86 (1999). 106. Cordioli, G., Mazzocco, C., Schepers, E., Brugnolo, E. & Majzoub, Z. Maxillary sinus floor augmentation using bioactive glass granules and autogenous bone with simultaneous implant placement. Clinical and histological findings. Clin Oral Implants Res 12, 270-8 (2001). 107. Hallman, M., Sennerby, L., Zetterqvist, L. & Lundgren, S. A 3-year prospective follow-up study of implant-supported fixed prostheses in patients subjected to maxillary sinus floor augmentation with a 80:20 mixture of deproteinized bovine bone and autogenous bone Clinical, radiographic and resonance frequency analysis. Int J Oral Maxillofac Surg 34, 273-80 (2005). 108. Moore, W. R., Graves, S. E. & Bain, G. I. Synthetic bone graft substitutes. ANZ J Surg 71, 354-61 (2001). 109. Bahn, S. L. Plaster: A bone substitute. Oral Surg., Oral Med., Oral Path 21, 672-681 (1966). 110. Baker, R. D., Terry, B. C., Davis, W. H., Connole, P. W. Long-term results of alveolar ridge augmentation. J. Oral Surg. 37, 486-489 (1979). 111. Cockin, J. Autologous bone grafting complications at the donor site. J. Bone Jt. Surg. 53B, 153 (1971). 112. Younger, E. M., Chapman, M. W. Morbidity at bone graft donor sites. J. Orthop. Trauma 3, 192-195 (1989). 113. Klein, C. P., Patka, P., van der Lubbe, H. B., Wolke, J. G. & de Groot, K. Plasma-sprayed coatings of tetracalciumphosphate, hydroxyl-apatite, and alpha-TCP on titanium alloy: an interface study. J Biomed Mater Res 25, 53-65 (1991). 114. Sharpe, J. R., Sammons, R. L. & Marquis, P. M. Effect of pH on protein adsorption to hydroxyapatite and tricalcium phosphate ceramics. Biomaterials 18, 471-6 (1997). 115. Osborn, J. F. & Newesely, H. The material science of calcium phosphate ceramics. Biomaterials 1, 108-11 (1980). 116. Geesink, R. G., de Groot, K. & Klein, C. P. Chemical implant fixation using hydroxyl-apatite coatings. The development of a human total hip prosthesis for chemical fixation to bone using hydroxyl-apatite coatings on titanium substrates. Clin Orthop Relat Res, 147-70 (1987). 117. Kitsugi, T. et al. Four calcium phosphate ceramics as bone substitutes for non-weight-bearing. Biomaterials 14, 216-24 (1993). 118. Einhorn, T. A. Enhancement of fracture-healing. J Bone Joint Surg Am 77, 940-56 (1995). 119. Hulth, A. Current concepts of fracture healing. Clin Orthop Relat Res, 265-84 (1989).

90120. Rejda, B. V., Peelen, J. G. & de Groot, K. Tri-calcium phosphate as a bone substitute. J Bioeng 1, 93-7 (1977). 121. Ellinger, R. F., Nery, E. B. & Lynch, K. L. Histological assessment of periodontal osseous defects following implantation of hydroxyapatite and biphasic calcium phosphate ceramics: a case report. Int J Periodontics Restorative Dent 6, 22-33 (1986). 122. Lee, D. A. in Dissolution characterization of commercially available hydroxylapatite particulate (The University of Alabama at Birmingham, 1988). 123. Klein, C. P., Driessen, A. A., de Groot, K. & van den Hooff, A. Biodegradation behavior of various calcium phosphate materials in bone tissue. J Biomed Mater Res 17, 769-84 (1983). 124. Brink, M. in Bioactive glass with a large working range (Abo Akademi, Finland, 1997). 125. Lai, W., Garino, J. & Ducheyne, P. Silicon excretion from bioactive glass implanted in rabbit bone. Biomaterials 23, 213-7 (2002). 126. Shimizu, Y. et al. Bone remodeling with resorbable bioactive glass and hydroxyapatite. Implant Dent 6, 269-74 (1997). 127. Furusawa, T., Mizunuma, K., Yamashita, S. & Takahashi, T. Investigation of early bone formation using resorbable bioactive glass in the rat mandible. Int J Oral Maxillofac Implants 13, 672-6 (1998). 128. Froum, S., Cho, S. C., Rosenberg, E., Rohrer, M. & Tarnow, D. Histological comparison of healing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: a pilot study. J Periodontol 73, 94-102 (2002). 129. Mendes, V. C. in Evaluation of bone repair in cavities filled in by bioactive glass or DFDBA: biomechanical, microscopic and histometric analysis in dogs. Faculty of Dentistry (Universidade Estadual Paulista, Araçatuba, 2004). 130. Radin, S., Ducheyne, P., Rothman, B. & Conti, A. The effect of in vitro modeling conditions on the surface reactions of bioactive glass. J Biomed Mater Res 37, 363-75 (1997). 131. Schepers, E., Barbier, L. & Ducheyne, P. Implant placement enhanced by bioactive glass particles of narrow size range. Int J Oral Maxillofac Implants 13, 655-65 (1998). 132. Orthovita & Implant Innovations, I. (1998). 133. Furusawa, T. & Mizunuma, K. Osteoconductive properties and efficacy of resorbable bioactive glass as a bone-grafting material. Implant Dent 6, 93-101 (1997). 134. Huygh, A., Schepers, E. J. G., Barbier, L., Ducheyne, P. Microchemical transformation of bioactive glass particles of narrow size range, a 0-24 months study. Journal of Materials Science: Materials in Medicine 13, 315-320 (2002).

91135. Tapety, F. I., Amizuka, N., Uoshima, K., Nomura, S. & Maeda, T. A histological evaluation of the involvement of Bio-Oss in osteoblastic differentiation and matrix synthesis. Clin Oral Implants Res 15, 315-24 (2004). 136. Araujo, M. G., Carmagnola, D., Berglundh, T., Thilander, B. & Lindhe, J. Orthodontic movement in bone defects augmented with Bio-Oss. An experimental study in dogs. J Clin Periodontol 28, 73-80 (2001). 137. Skoglund, A., Hising, P. & Young, C. A clinical and histologic examination in humans of the osseous response to implanted natural bone mineral. Int J Oral Maxillofac Implants 12, 194-9 (1997). 138. Zitzmann, N. U. & Scharer, P. Sinus elevation procedures in the resorbed posterior maxilla. Comparison of the crestal and lateral approaches. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85, 8-17 (1998). 139. Dies, F., Etienne, D., Abboud, N. B. & Ouhayoun, J. P. Bone regeneration in extraction sites after immediate placement of an e-PTFE membrane with or without a biomaterial. A report on 12 consecutive cases. Clin Oral Implants Res 7, 277-85 (1996). 140. Berglundh, T. & Lindhe, J. Healing around implants placed in bone defects treated with Bio-Oss. An experimental study in the dog. Clin Oral Implants Res 8, 117-24 (1997). 141. Camelo, M. et al. Clinical, radiographic, and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int J Periodontics Restorative Dent 18, 321-31 (1998). 142. Hammerle, C. H., Chiantella, G. C., Karring, T. & Lang, N. P. The effect of a deproteinized bovine bone mineral on bone regeneration around titanium dental implants. Clin Oral Implants Res 9, 151-162 (1998). 143. Klinge, B., Alberius, P., Isaksson, S. & Jonsson, J. Osseous response to implanted natural bone mineral and synthetic hydroxylapatite ceramic in the repair of experimental skull bone defects. J Oral Maxillofac Surg 50, 241-9 (1992). 144. Wetzel, A. C., Stich, H. & Caffesse, R. G. Bone apposition onto oral implants in the sinus area filled with different grafting materials. A histological study in beagle dogs. Clin Oral Implants Res 6, 155-63 (1995). 145. Valentini, P., Abensur, D., Densari, D., Graziani, J. N. & Hammerle, C. Histological evaluation of Bio-Oss in a 2-stage sinus floor elevation and implantation procedure. A human case report. Clin Oral Implants Res 9, 59-64 (1998). 146. Van de Putte, K. A. & Urist, M. R. Osteogenesis in the interior of intramuscular implants of decalcified bone matrix. Clin Orthop Relat Res 43, 257-70 (1965). 147. Peterson, B., Whang, P. G., Iglesias, R., Wang, J. C. & Lieberman, J. R. Osteoinductivity of commercially available demineralized bone matrix. Preparations in a spine fusion model. J Bone Joint Surg Am 86-A, 2243-50 (2004).

92148. Haas, R., Haidvogl, D., Donath, K. & Watzek, G. Freeze-dried homogeneous and heterogeneous bone for sinus augmentation in sheep. Part I: histological findings. Clin Oral Implants Res 13, 396-404 (2002). 149. Ohura, K. et al. Resorption of, and bone formation from, new beta-tricalcium phosphate-monocalcium phosphate cements: an in vivo study. J Biomed Mater Res 30, 193-200 (1996). 150. Lugowski, S. J., Smith, D.C., Bonek, H., Lugowski, J., Peters, W., J. Semple. . Analysis of silicon in human tissues with special reference to silicone breast implants. . J Trace Elem Med Biol 14 31-42 (2000). 151. Ishikawa, K., Takagi, S., Chow, L.C., Ishikawa, Y. Properties and mechanisms of fast-setting calcium phosphate cements. Journal of Materials Science: Materials in Medicine 6, 528-533 (1995). 152. Gautier, H., Daculsi, G., Merle, C. . Association of vancomycin and calcium phosphate by dynamic compaction in vitro: characterization and microbiological activity. Biomaterials 22, 2481-2487 (2001). 153. Lee, J. E. et al. Effects of the controlled-released TGF-beta 1 from chitosan microspheres on chondrocytes cultured in a collagen/chitosan/glycosaminoglycan scaffold. Biomaterials 25, 4163-73 (2004). 154. El-Ghannam, A. Bone reconstruction: from bioceramics to tissue engineering. Expert Rev Med Devices 2, 87-101 (2005). 155. Queiroz, A. C., Santos, J. D. & Monteiro, F. J. Development of a system to adsorb drugs onto calcium phosphate materials. J Mater Sci Mater Med 16, 641-6 (2005). 156. Grover, L. M., Gbureck, U., Wright, A. J., Tremayne, M. & Barralet, J. E. Biologically mediated resorption of brushite cement in vitro. Biomaterials 27, 2178-85 (2006). 157. Ruhe, P. Q., Boerman, O. C., Russel, F. G. M., Spauwen, P. H. M., Mikos, A. G., Jansen, J. A. Controlled release of rhBMP-2 loaded poly(DL-Lactic-Co-Glycolicacid)/Calcium phosphate cement composites in vivo. Journal of Controlled Release 106, 162-171 (2005). 158. Kikuchi, L., Park, J. Y., Victor, C. & Davies, J. E. Platelet interactions with calcium-phosphate-coated surfaces. Biomaterials 26, 5285-95 (2005). 159. Geisow, M. J. & Evans, W. H. pH in the endosome. Measurements during pinocytosis and receptor-mediated endocytosis. Exp Cell Res 150, 36-46 (1984). 160. Geisow, M. J. Fluorescein conjugates as indicators of subcellular pH. A critical evaluation. Exp Cell Res 150, 29-35 (1984). 161. Holy, C. E., S. M. Dang, J. E. Davies, M. S. Shoichet. In vitro degradation of a novel poly(lactide-co-glycolide) 75/25 foam Biomaterials 20, 1177-1185 (1999 ).

93162. Lees, R. L., Sabharwal, V. K. & Heersche, J. N. Resorptive state and cell size influence intracellular pH regulation in rabbit osteoclasts cultured on collagen-hydroxyapatite films. Bone 28, 187-94 (2001). 163. Lader, C. S., Scopes, J., Horton, M. A. & Flanagan, A. M. Generation of human osteoclasts in stromal cell-free and stromal cell-rich cultures: differences in osteoclast CD11c/CD18 integrin expression. Br J Haematol 112, 430-7 (2001). 164. Ramnaraine, M. L. et al. Osteoclasts direct bystander killing of bone cancer. Cancer Res 66, 10929-35 (2006). 165. Lutgens, E. et al. Disruption of the cathepsin K gene reduces atherosclerosis progression and induces plaque fibrosis but accelerates macrophage foam cell formation. Circulation 113, 98-107 (2006). 166. Al-Saffar, N. & Revell, P. A. Frustrated wound healing: The immunopathogenesis of bone resorption (Toronto, Canada, In: Davies, J.E. (ed) Bone Engineering, 2000). 167. Mendes, V. C., Moineddin, R. & Davies, J. E. The effect of discrete calcium phosphate nanocrystals on bone-bonding to titanium surfaces. Biomaterials 28, 4748-55 (2007). 168. Rahman, N., Bano, Z. & Azmi, S. N. Kinetic spectrophotometric analysis of pantoprazole in commercial dosage forms. Anal Sci 22, 983-8 (2006). 169. Wahbi, A. A., Abdel-Razak, O., Gazy, A. A., Mahgoub, H. & Moneeb, M. S. Spectrophotometric determination of omeprazole, lansoprazole and pantoprazole in pharmaceutical formulations. J Pharm Biomed Anal 30, 1133-42 (2002). 170. Karljikovic-Rajic, K., Novovic, D., Marinkovic, V. & Agbaba, D. First-order UV-derivative spectrophotometry in the analysis of omeprazole and pantoprazole sodium salt and corresponding impurities. J Pharm Biomed Anal 32, 1019-27 (2003). 171. Lagerstrom, P., Persson, B. Determination of Omeprazole and metabolites in plasma and urine by liquid chromatography. Journal of Chromatography 309, 347-356 (1984).

947. APPENDICES
7.A In vivo implantation
7.A.1 Pilot study
BAF Control PANT OMP
Figure 7.1 µCT scans of calcium phosphate cements, OMP-, PANT-, and BAF-cements. Top row =1 week samples. Bottom row = 3 week samples.
PANT OMP BAF Control

95
Figure 7.2 Threshold-based volumetric measurements of calcium phosphate cements.

96
7.A.2 MP x BioOssTM x BioGranTM x AllogenixTM
Figure 7.3 SEM images of BioOssTM
Figure 7.4 Histological section of BioOssTM at 16 weeks post-operative. Increased volumes of
the particulate material surrounded by a thin layer of bone are found (FW=5446µm).

97
Figure 7.5 SEM images of BioGranTM
Figure
the parti
7.6 Histological section of BioGranTM at 16 weeks post-operative. Increased volumes of
culate material surrounded by a thin layer of bone are found (FW=5446µm).

98
Figure 7.7 SEM images of AllogenixTM
Figure 7.8 H
the putty ma
istological section of AllogenixTM at 16 weeks post-operative. Increased volumes of
terial surrounded by bone are found (FW=5446µm).