Embed Size (px)
Citation preview

This may be the author’s version of a work that was submitted/acceptedfor publication in the following source:
Romeo, Michele, Fitzgerald, Gerard, Toloo, Sam, Rego, Joanna, Aitken,Peter, Tippett, Vivienne, Chu, Kevin, Ting, Joseph, Bosley, Emma, & Ba-niahmadi, Sara(2017)Emergency Health Services (EHS): Demand and service delivery models- Monograph 4: Demand management and policy options.Emergency Health Services (EHS): Demand and Service Delivery Models.Queensland University of Technology, Australia.
This file was downloaded from: https://eprints.qut.edu.au/115052/
c© Consult author(s) regarding copyright matters
This work is covered by copyright. Unless the document is being made available under aCreative Commons Licence, you must assume that re-use is limited to personal use andthat permission from the copyright owner must be obtained for all other uses. If the docu-ment is available under a Creative Commons License (or other specified license) then referto the Licence for details of permitted re-use. It is a condition of access that users recog-nise and abide by the legal requirements associated with these rights. If you believe thatthis work infringes copyright please provide details by email to [email protected]
Notice: Please note that this document may not be the Version of Record(i.e. published version) of the work. Author manuscript versions (as Sub-mitted for peer review or as Accepted for publication after peer review) canbe identified by an absence of publisher branding and/or typeset appear-ance. If there is any doubt, please refer to the published source.

Emergency Health Services:
Demand & Service Delivery Models

Demand Management & Policy Options
2
Suggested citation
Romeo M, FitzGerald G, Toloo S et al. Emergency Health Services (EHS): Demand and Service Delivery Models. Monograph 4: Demand management and policy options. Queensland University of Technology, Brisbane 2017.
ISBN: 978-1-925553-07-9
Copyright
© Copyright 2017. This publication is copyright. Subject to the Copyright Act 1968, no part of this monograph may be reproduced by any means without the written permission of the authors. Cover photograph © Copyright 2011 Denielle Bailey.
Disclaimer:
Opinions and views expressed in this monograph are those of the authors and do not necessarily reflect the opinions and views of the organizations who have funded or provided the project with data and information.
Michele Romeo undertook the literature review update (Chapters 2 & 3) and qualitative study (Chapter 4) in partial fulfilment of her Master of Public Health degree.
Further Information:
Professor Gerry FitzGerald School of Public Health and Social Work, QUT Victoria Park Road Kelvin Grove, QLD 4059 Email: [email protected]

Demand Management & Policy Options
3
Emergency Health Services: Demand & Service Delivery Models
Monograph 4
Demand Management and Policy Options
Principal Authors: Michele Romeo
Gerry FitzGerald Sam Toloo
Joanna Rego Peter Aitken
Vivienne Tippet Kevin Chu Joseph Ting
Emma Bosley Sara Baniahmadi

Demand Management & Policy Options
4
Related publications
The following publications and academic works are the outcomes of the Emergency Health Services study and supplement this monograph:
Previous Monographs
2011 Toloo S, FitzGerald G, Aitken P, Ting J, Tippett V, Chu K. Emergency Health Services (EHS): Demand and Service Delivery Models. Monograph 1: Literature Review and Activity trends. Queensland University of Technology, Brisbane 2011. (ISBN:987-1-921897-11-5).
2012 Toloo S, Rego, FitzGeraldG, Aitken, Ting, J, Quinn, Enraght-MoonyE. Emergency Health Services (EHS): Demand and Service Delivery Models. Monograph 2: Queensland EHS Users’ Profile. Queensland University of Technology. Brisbane 2012. (ISBN: 978-1-921897-52-8).
2013 Ghasem Sam Toloo, Joanna Rego, Gerry FitzGerald, Kirsten Vallmuur, Joseph Ting. Emergency Health Services: Demand & Service Delivery Models- Monograph 3: Patients' Reasons and Perceptions. 12/2013; Publisher: Queensland University of Technology, ISBN: 978-1-921897-93-1
Journal Articles
2016 Toloo GS, Aitken P, Crilly J, FitzGerald G. Agreement between triage category and patient's perception of priority in emergency departments. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 24, Article No.: 126.
2016 FitzGerald G. Uncomfortable truth about emergency care. MJA Insight Issue 8, 7 March 2016. Available: http://www.doctorportal.com.au/mjainsight/2016/8/uncomfortable-truth-about-emergency-care/.
2015 Rego J, FitzGerald G, Toloo S, Vallmuur K. Why do Queenslanders seek care in emergency departments? A population study. Emergency Medicine Australasia 27(6), pp. 516-521.
2015 FitzGerald G, Toloo GS, Aitken P, Keijzers G, Scuffham P. Public use and perceptions of emergency departments: A population survey. Emergency Medicine Australasia 27(4), pp. 336-342.
2014 FitzGerald G, Toloo GS, Romeo M. Emergency healthcare of the future. Emergency Medicine Australasia 26(3), pp. 291-294.
2013 FitzGerald G, Toloo GS. General practice patients in the emergency department. Medical Journal of Australia 198(11): 573-574.
2013 Toloo GS, FitzGerald G, Aitken P, Ting J, McKenzie K, Rego J, et al. Ambulance use is associated with higher self-rated illness seriousness: user attitudes and perceptions. Academic Emergency Medicine 20: 576–583.

Demand Management & Policy Options
5
2013 Tippett V, Toloo S, Eeles D, Ting J, Aitken P, FitzGerald G. Universal access to ambulance does not increase overall demand for ambulance services in Queensland, Australia. Australian Health Review 37: 121-126.
2012 FitzGerald G, Toloo S, Rego J, Ting J, Aitken P, Tippett V. Demand for public hospital emergency department services in Australia: 2000–2001 to 2009–2010. Emergency Medicine Australasia 24: 72–78.
PhD Thesis
2015 Rego J. Growing demand for emergency department services: associated factors and patients’ perspective. School of Public Health and Social Work. Queensland University of Technology. Completion Date: September 2015.
Conference Presentations
2014 Toloo GS, FitzGerald G, Aitken P. Conceptual framework for understanding the demand for emergency health services. [poster presentation]. In International Conference on Emergency Medicine (ICEM) 2014, 11 - 14 June 2014, Hong Kong Convention and Exhibition Centre, Hong Kong.
2013 Rego J, FitzGerald G, Toloo S. Patients’ perceptions of emergency department services: better specialised staff, convenient and available services. [poster presentation]. In: Australasian College for Emergency Medicine (ACEM) 30th Annual Scientific Meeting. 24–29 Nov 2013. Adelaide Convention & Exhibition Centre; Adelaide, Australia.
2013 Toloo S, Aitken P, FitzGerald G. Decision and reasons for calling an ambulance: patients’ perspective [Abstract]. Prehospital and Disaster Medicine 28(S1): s65–s66.
2013 FitzGerald G, Toloo S, Aitken P. The growing demand for emergency healthcare [Abstract]. Prehospital and Disaster Medicine 28(S1): s158.
2012 FitzGerald G, Toloo S, Rego J. Shaping the future demand for ambulance: understanding patient’s reasons and decision making [oral presentation]. In: 2012 Council of Ambulance Authorities (CAA) Conference: Shaping the Future. 3–4 October 2012. Wrest Point Centre, Hobart, Tasmania, Australia.
2011 Toloo S, FitzGerald G, Rego J. Inequality in using emergency health services (EHS): Is it all about money? [oral presentation]. In: The Australian Sociological Association (TASA) 2011 Conference, 29 Nov – 1 Dec 2011. University of Newcastle; Newcastle, Australia.
2011 Rego J, FitzGerald G, Toloo S. Reasons for ED utilisation: patients’ perspective [oral presentation]. Australasian College for Emergency Medicine (ACEM) 28th Annual Scientific Meeting. 20–24 Nov 2011. Sydney Convention & Exhibition Centre; Sydney, Australia.

Demand Management & Policy Options
6
2011 Hou XY, Toloo S, FitzGerald G. Acuity and severity of patients attending 28 Queensland hospitals emergency departments in 2008–09. Australasia Epidemiology Association Annual Conference: Combining Tradition and Innovation, 19–21 September 2011. Burswood Conference Centre, Perth, Australia.
2011 Rego J, FitzGerald G, Toloo S. Where do ED patients come from? [Abstract]. Prehospital & Disaster Medicine 26(S1): s23-s24 (Article No. A67).
2010 Toloo S, FitzGerald G, Rego J, Tippett V, Quinn J. Age and Gender Differences in Ambulance Utilisation in Queensland [oral presentation]. Australasian College for Emergency Medicine (ACEM) 27th Annual Scientific Meeting, 21–25 Nov 2010. National Convention Centre, Canberra, Australia.
2010 Rego J, FitzGerald G, Toloo S. Utilisation of Queensland Emergency Departments by Different Age Groups [oral presentation]. Australasian College for Emergency Medicine (ACEM) 27th Annual Scientific Meeting, 21–25 Nov 2010. National Convention Centre, Canberra, Australia.
2009 Toloo S, Tippett V, FitzGerald G, Chu K, Eeles D, Miller A, Ting J, Ward D. How does Ambulance Service utilisation impact demand for Emergency Departments in Queensland, Australia? [Abstract]. Journal of Emergency Primary Health Care 7(3): Article No.: 990354.
2009 FitzGerald G, Aitken P, McKenzie K, Kozan E, Tippett V, Toloo S, Rego J, Kim JA. Growing demand for emergency health services in Queensland, Australia [Abstract]. Prehospital and Disaster Medicine 24(2): s52.

Demand Management & Policy Options
7
Acronyms
ACEM Australasian College for Emergency Medicine ATS CAA
Australasian Triage Scale Council of Ambulance Authorities
ARC Australian Research Council ED Emergency Department EHS Emergency Health Services EHSQ Emergency Health Services Queensland study ERUMI Emergency Room Utilisation Management Initiative GP General Practitioner HITH Hospital in the Home HiNH Hospital in the Nursing Home NEAT National Emergency Access Target NP Nurse Practitioner QAS Queensland Ambulance Services QH Queensland Health QUT Queensland University of Technology RAP Resource Access Program WIC Walk-in-clinic

Demand Management & Policy Options
8
Acknowledgements
The authors would like to acknowledge the support and contribution of the following without which this monograph and the research project would not have come into existence:
• The Australian Research Council (ARC) that provided funding for the project under the ARC-Linkage grant number LP0882650 in 2007;
• The Queensland Ambulance Service (QAS) and its then Commissioner Mr Jim Higgins and the (then) Department of Community Safety who as partner organisations provided funding for the project and assisted with the provision of ambulance data;
• Queensland Health for ethics approval and the provision of ED data;
• The Council of Ambulance Authorities (CAA) and EMERG Qld (a research group within the Australasian College for Emergency Medicine) for supporting the research project;
• Other members of the EHSQ research team including:
o Professor Erhan Kozan (chief investigator, QUT) o Assoc/Prof Kirsten Vallmuur (chief investigator, QUT) o Mr Russell Bowles (partner investigator, Commissioner QAS) o Mr David Eeles (partner investigator, QAS) o Ms Jamie Quinn (partner investigator, QAS) o Ms Ann Miller (partner investigator, QH) o Dr David Ward (research collaborator, Emergency Physician)
• Queensland University of Technology Human Research Ethics Committee for approving the research project.

Demand Management & Policy Options
9
Contents
Acronyms ................................................................................................................................ 7
Acknowledgements .............................................................................................................. 8
Figures .................................................................................................................................. 10
Executive Summary ............................................................................................................ 11
1. Introduction ................................................................................................................. 13
Background and context ....................................................................................................... 16
Definition of demand ........................................................................................................ 17
Impact of EHS congestion ................................................................................................. 17
Patient outcomes .......................................................................................................... 18
Staff outcomes ............................................................................................................... 18
System wide outcomes ................................................................................................ 18
Understanding demand .................................................................................................... 19
Causes of demand .............................................................................................................. 20
2. Demand management ................................................................................................ 23
Methods .............................................................................................................................. 23
Findings .............................................................................................................................. 24
Managing EHS demand ..................................................................................................... 25
Prevention ...................................................................................................................... 26
Enhanced primary care ................................................................................................. 26
Case management of frequent users ............................................................................ 28
Discharge management ................................................................................................. 30
Enhanced community nursing ...................................................................................... 30
Using technology to avoid admissions ......................................................................... 30
Walk-in or urgent care clinics ....................................................................................... 31
Minor injury units .......................................................................................................... 32
Emergency care practitioners ...................................................................................... 32
Patient centred medical home ...................................................................................... 32
Improved end of life care .............................................................................................. 32
Diversion ........................................................................................................................ 33
Conclusion .......................................................................................................................... 37
3. Policy analysis .............................................................................................................. 39
Introduction ....................................................................................................................... 39
Methods .............................................................................................................................. 39
Findings .............................................................................................................................. 41

Demand Management & Policy Options
10
Why is it important? .......................................................................................................... 41
What are the key issues?................................................................................................... 43
What is the extent of the problem? .................................................................................. 47
What can be done about it? .............................................................................................. 49
4. Discussion ..................................................................................................................... 51
Introduction ....................................................................................................................... 51
Primary and secondary prevention ................................................................................. 53
Treatment on site .............................................................................................................. 56
Diversion ............................................................................................................................ 58
5. Conclusion ..................................................................................................................... 61
References ............................................................................................................................. 63
Appendix ................................................................................................................................ 80
Figures
Figure 1 The Input-Throughput-Output Model of ED Congestion .................................... 19 Figure 2 Integrated Model of Demand for Emergency Health Services ........................... 20

Demand Management & Policy Options
11
Executive Summary
The emergency healthcare system (EHS) is a critical component of Australia’s healthcare system. The EHS has been fundamentally reformed over the last four decades with the development, upgrading and modernisation of both ambulance services and Emergency Departments (EDs) and the emergence of new professions of Paramedic, Emergency Physician and Emergency Nurse.
These changes have unquestioned impact on improving the standards and quality of care and therefore on the outcomes for patients suffering acute illness and injury. However, emergency health services are increasingly congested from the combined impact of growing demand for care and blocked access to inpatient beds and this congestion has proven adverse clinical, organisational and staff impacts.
However, often the public, bureaucratic and political perspective is that this problem somehow reflects at worst gaming of the system and at best inefficiency and so public policy solutions have been underpinned by blaming someone for the problem; either the patient, the Commonwealth/States or the providers. Phrases such as “inappropriate attendance”, GP patients, frequent flyers, unrealistic expectations and provider induced demand have characterised much of the public discourse.
The feasible alternative proposition is that there are more sick people seeking care and exercising largely thoughtful and wise choice of the most appropriate source of that care.
The Emergency Health Services Queensland (EHSQ) study was a program of research funded by an ARC Linkage grant which sought to describe the trends in EHS demand, to identify the factors driving increased demand and to evaluate strategies which may safely reduce the future demand growth.
Our research findings, which largely align with similar studies across Australia and in similar jurisdictions, has demonstrated the demand is growing across all developed nations; it is growing amongst the more urgent categories of patients, across all age groups and a broad range of clinical conditions. There is no evidence of widespread misuse (however so defined) nor is there any evidence that the growth in demand will not continue at the current rate.
On all the evidence we have identified the growing demand represents:
The legitimate and reasonable choice of patients suffering acute illness and injury to seek care at a location they perceive to offer the most appropriate and safest assessment and intervention.
The question underpinning this aspect of the research is ‘can anything be done to moderate the growing demand while still offering safe, appropriate and efficient care?’ The aim of this

Demand Management & Policy Options
12
the final report of this research is to summarise the findings and to place those findings within the context of the public literature, to identify what is known about the application of these findings into public policy and to make recommendations for future research and the future direction of acute health services.
This study involved a detailed review of the literature to identify intervention strategies and a policy evaluation undertaken with the support of stakeholder interviews. The strategies that may moderate the growth in demand may be broadly categorised into three categories:
1. Enhanced prevention 2. Management in situ 3. Diversion to alternative services.
The analysis of policy options has confirmed there is no single or even small group of interventions likely to make a difference. One distinct possible policy alternative is that the current arrangements offer the most efficient and effective means of providing the required care and so ongoing expansion of those services may be most appropriate. However, the alternative is a comprehensive suite of strategies properly coordinated at both policy and operational levels to ensure patients have access to a range of services from which they may choose the most appropriate to their needs after weighing up the social, clinical and financial implications.
Additional research is required to develop and evaluate these strategies including the economic, clinical, professional and social costs and benefits.

Demand Management & Policy Options
13
1. Introduction
This is the fourth and final in a series of monographs reporting the findings of the Emergency Health Services Queensland (EHSQ) study. The aim of EHSQ was to characterise the growing demand for acute healthcare, to identify the factors driving the increased demand and to identify and evaluate strategies which may better meet that increased demand in a safe and more efficient manner.
Monograph 1 addressed the background literature and context. It also outlined conceptual frameworks that form the basis of the more detailed analysis of publicly accessible data and of primary data collected specifically for this project.1 This Monograph examined the publicly available data on demand in Australia which demonstrated the following key observations:
• Per capita demand for ED attendance increased over the last decade at a rate of 2% per annum.
• Per capita demand for ambulance increased over the last decade at a rate of 3.7% per annum.
• A combination of individual, societal and health system factors contribute to the growth in demand.
The aim of Monograph 2 was to identify the characteristics of users and, through comparison with the population, determine those characteristics of the population which appear to contribute to the growth in demand.2 This Monograph examined data obtained from Queensland Department of Health and Queensland Ambulance Service with the following key findings:
• The growth in ED demand is prominent in the more urgent triage categories with an actual decline in less urgent patients.
• An estimated 55% of patients attend hospital EDs outside of normal working hours. There is no evidence that patients presenting out of hours are significantly different to those presenting within working hours; they have similar triage assessments and outcomes.
• In terms of major illness presentations, in 2010-11, patients suffering from injuries and poisoning comprised 28% of the ED workload, followed by conditions related to the respiratory system (8.7%), digestive system (5.5%), infectious and parasitic problems (5.2%), genitourinary system (4.5%) and cardiovascular and circulatory system (4.2%). These categories showed a total growth of +64%, +54%, +54%, +90%, +64% and -32% respectively compared to 200-04.

Demand Management & Policy Options
14
• 25.6% of patients attending EDs are admitted to hospital. 19% of admitted patients and 7% of patients who die in the ED are triage category 4 or 5 on arrival.
• The average age of ED patients is 35.6 years. Demand has grown in all age groups and amongst both men and women. Men have higher utilisation rates for ED in all age groups. The only group where the growth rate in women has exceeded men is in the 20-29 year old age group; this growth is particularly in the injury and poisoning categories.
• Considerable attention has been paid publicly to ED performance criteria. While this research was not intended to assess performance, it is worth noting that 50% of all patients were treated within 33 minutes of arrival.
• Patients from lower socioeconomic areas appear to have higher utilisation rates and the utilisation rate for indigenous people appears to exceed those of European and other backgrounds. The utilisation rates for immigrant people is generally less than that of Australian born however it has not been possible to eliminate the confounding impact of different age and socioeconomic profiles.
• Demand for ambulance service is also increasing at a rate that exceeds population growth. Utilisation rates have increased by an average of 5% per annum in Queensland compared to 3.6% nationally, and the utilisation rate in Queensland is 27% higher than the national average.
• The growth in ambulance utilisation has also been amongst the more urgent categories of dispatch and utilisation rates are higher in rural and regional areas than in the metropolitan area. Whilst the demand for ambulance increases with age, the growth in demand for ambulance service has been more prominent in younger age groups.
The main objectives of Monograph 3 were to: (1) Understand patients’ reasons for using emergency health services in Queensland, including ambulance and ED services; (2) Explore potential relationships between attitudinal and perceptual factors with health service utilisation; and (3) Analyse the potential role of socio-demographic factors in the decisions and reasons for using the emergency health services.3 The monograph examined and reported the findings from a survey of 911 patients who attended eight public hospital EDs in Queensland.
The study demonstrated that patients elected to attend hospital EDs in a considered fashion after weighing up alternatives, and there is no evidence of deliberate or ill-informed misuse. Similarly patients exercised considered and rational judgements in their choice to seek help from the ambulance service. Key findings included:
• Patients attending ED have high levels of social support and self-efficacy that speak to the considered and purposeful nature of the exercise of choice.

Demand Management & Policy Options
15
• About one third of patients have new conditions while two thirds have chronic illnesses.
• More than half the attendees (53.1%) had consulted a healthcare professional prior to making the decision.
• The decision to seek urgent care at an ED was mostly constructed around the patient’s perception of the urgency and severity of their illness, reinforced by a strong perception that the hospital ED was the correct location for them and that other options were not considered appropriate.
• One-third of the respondents held private hospital insurance but nevertheless attended a public hospital ED.
• The decision to seek ambulance assistance was influenced by a perception that the ambulance provided appropriate access to the ED which was considered most appropriate for their particular condition.
• In 43.8% of cases a health care professional advised use of the ambulance.
The challenges identified from the previous stages of the study require health services to better understand the patient’s needs, and to design and validate services that meet those needs. The final Monograph (this document) aims to bring the outcomes of the research into a cohesive analysis and to present options for public policy derived from the evidence.
In this monograph we first review the background to the current EHS and then offer a critical evaluation of the available evidence on demand management solutions. We then describe the policy options informed with the aid of interviews with a small number of key stakeholders in regard to demand management strategies. Finally, future policy and research directions will be discussed.

Demand Management & Policy Options
16
Background and context Emergency Health Services (EHS) is a relatively new domain of medical endeavour which has been reformed in the last four decades in most developed countries through the modernisation of core services such as the Emergency Departments (ED), ambulance services and patient transfer and retrieval services.4 This reformation has been underpinned professionally by the development of a new medical specialisation of Emergency Medicine, a specialisation in nursing of emergency nursing and the introduction of Paramedics. Each of these has been associated with the development of professional support strategies particularly educational programs.
These reforms have had an undeniable impact on the quality of care for acutely ill and injured people but there is currently considerable public and professional concern with the congestion being experienced in emergency health services. This congestion is known to be associated with significant adverse clinical impacts as well as having adverse organisational consequences and being the cause of staff and patient distress.2
Concerns about the negative impact of crowding have led to research into effective interventions1 however there is currently no common cohesive evidence based guidance for practitioners and policy makers. The research to date has focused on particular aspects of the issue including best practice for delivery of pre-hospital emergency care,5, 6 strategies to reduce attendance,1,7, 8 and the time patients wait.8, 9 However the current public discourse often does not reflect an in-depth understanding of the factors that contribute to this congestion nor of the evidence based strategies required to address it.
Demand for EHS has been growing in excess of population growth for the last decade at least. Ambulance demand on a per capita basis has grown at an average of 3.7% per annum. The current utilisation rate for EDs in Australia is 331 per 1000 persons per annum and this rate has been consistently increasing over the last decade at an average of 1.8% per annum.2 However there is considerable variance across states and territories of Australia in both the growth, and utilisation rates, which requires understanding so as to better map future trends to population and social change.10 The UK,11 New Zealand,12 Canada,13 Japan14 and the USA15 report increased ED attendances with current growth rates ranging from 3%–6% annually.16 The factors influencing this growth in demand are complex. The increase in the number of emergency attendances across Australia is not unique.

Demand Management & Policy Options
17
Definition of demand
To date there is no universally agreed upon definition or measurement of EHS demand.1 In prehospital care this is complicated by the variability in measures of incidents, responses and patients treated and transported.1 For example a single incident (e.g. a car crash) may be associated with multiple or no patients and may attract zero or multiple responses dependent on the nature of the event. Similarly, ED attendance numbers (which is where ambulance takes most of its patients) may be complicated by inter-hospital transfers, recalled patients, those who do not wait for treatment and those who may be deceased on arrival.
Much of the public reporting and the literature uses raw activity counts to represent patient load. While such figures may be useful in helping resource allocation decisions within institutions, they tell little of the population perspectives. Utilisation rates (patients per 1000 population or equivalence) represent a more meaningful population descriptor as it removes the impact of changes in population size but also allows comparative analysis of utilisation between various population classes.
However the principal issue of public and professional concern is congestion of EHS. This is reflected in terms such as waiting time, boarding of patients in the ED, Access Block and ramping of ambulance patients. Congestion, is also often described as crowding and other times overcrowding in the literature. We use the term congestion for convenience and consistency. There is little agreement whether ‘access block’ – the term used to describe the practice of keeping a patient who remains for a prolonged period in the ED while they wait for an inpatient bed – is a cause,17 a consequence 18 or a measure of demand.18, 19
Cowan and Trzeciak defined congestion as “an extreme volume of patients in ED treatment areas, forcing the ED to operate beyond its capacity”.20, 1 Previous work by QUT considers definitions such as this are easier to operationalise and investigate, providing a useful criteria by which to measure the extent of the problem.1
Researchers such as Hwang and Concato21 as well as Morris and colleagues22 conclude that the lack of clarity also makes drawing conclusions about effective interventions more difficult, as studies do not compare like with like.
Impact of EHS congestion
The negative consequences of EHS demand growth and associated overcrowding are recurrent themes in the literature. Congested EHS has clinical, organisational and social impacts, characterised by long waiting items in ED, delayed ambulance

Demand Management & Policy Options
18
response times, hospital bypass and thus patient and staff dissatisfaction and system wide inefficiencies.1
Patient outcomes
Patient satisfaction is impaired as waiting time increases8 as well as undermining patient privacy and confidentiality and dignity.23 Delays in treatment due to congestion can not only cause prolonged pain and anxiety,22, 24, 1, 2 but may also lead to a considerable number of patients leaving the hospital without seeing a doctor, or leaving before the treatment is completed.25, 1, 26 Additionally, there is considerable evidence that congestion is associated with in-hospital mortality.27
Staff outcomes
The literature also highlights that working in a ED is stressful and potentially more dangerous than other sites in the health care systems.1 Workplace stress related to demand, workload pressures and insufficient resources have been shown to be associated with ED physicians reducing their working hours1 as well as staff burnout and high turnover.1, 2, 28, 29 This leads to greater use of less experienced staff, reported in previous QUT research which creates a situation where junior doctors are assigned to fast tract patients to reduce the pressure in the ED. This reduces the time that junior staff may otherwise spend on specialised training.1
System wide outcomes
Problems associated with ED demand are not just restricted to the individual ED involved. Ambulance diversion, bypass and ramping are immediate effects of ED congestion. Providing a solution for one ED is adding to the burden of others.15, 1, 30
There are very few studies which demonstrate the actual costs to the EHS as a direct result of congestion.1 However, it can be considered that extended length of stay increases EHS cost and where relevant revenue because of the reduced turnover of patients. Furthermore, the costs may be higher when the number of patients who leave without being seen is taken into consideration.1
A congested EHS effects an entire hospital and health system; challenging infection control31 and the ability to respond to major incidents20 as well as contributing to considerable public dissatisfaction with health system responsiveness and cost.22, 1

Demand Management & Policy Options
19
Understanding demand
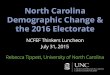
Asplin32 perhaps best described the underpinning rationale by considering the EHS as a closed system which becomes congested if more goes in than comes out (Figure 1). Alternatively EHS is congested because of push factors (increased demand), blockages (Access block) and pull factors (increased scope of care).
Figure 1 The Input-Throughput-Output Model of ED Congestion [Reprinted from Asplin et al,32
with permission from Elsevier]
Reductions in inpatient beds particularly in the public sector despite growth in admissions has resulted in widespread difficulty in accessing ongoing care for patients (Access Block) leading to ‘boarding’ of patients and consequentially ramping of ambulance patients and hospital bypass. At the same time increasing professionalization of EHS has provided capacity for more extensive clinical intervention. Patients stay longer within the ED as it is often the most appropriate place within hospitals to provide ongoing highly professional care and EDs in particular can offer a much larger range of clinical interventions than in the past.
While there is extensive reporting of strategies to improve patient flow within the EHS and thus reduce congestion,4 there is less attention to strategies that manage the input. These flow strategies may be internal to the EHS or take a whole of hospital perspective. Indeed in Australia the introduction of the NEAT was aimed directly at improving the flow of patients within the system. While recognising the multifactorial nature of EHS congestion, the focus of our study is on the demand (input) for EHS.

Demand Management & Policy Options
20
Causes of demand
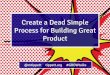
Our previous research and publications argue that there is no single explanation for the growth in demand but rather a range of factors that impact differently as cultures, social groups, health systems and individuals differ. The diagram (Figure 2) demonstrates the complex interconnectivity of socio demographic and perceptual factors affecting demand.4
Figure 2 Integrated Model of Demand for Emergency Health Services.3
This Figure creates a fundamental logic of EHS demand.
The level of acute illness and injury, which is determined by socio-demographic factors, is converted into perceived acuity by the combined influence of individual personal factors (self-efficacy, health status and health perception) and social/community factors (social and network support and health beliefs and preferences) into a decision to seek care which is determined by cues to action and perceptions of costs and benefits.
The literature has demonstrated that the flow of patients into the EHS is the largest influence on congestion (demand). This is influenced by both the volume and nature of demand.1 Conceptually, this need not cause congestion if the service has capacity and capability to deal with the flow into the EHS. However, problems arise when this pressure caused by the backups which occur when the EHS cannot cope with the demand.4

Demand Management & Policy Options
21
Reasons proposed to explain the trend towards an increasing number of patients using the EHS include4:
• Socio-economic factors such as social deprivation and poverty33,34,
loneliness,16 parental expertise (children who have a grandmother involved in their care are less likely to attend)35 and parental convenience.36
• Health system factors such as lack of access to a regular general practitioner,37 using the ED as a source of regular medical care,38 access on holidays,39 organisational and service delivery problems in primary care and convenience and accessibility including distance from emergency department.40 Research often reports that the lack of alternative sources of care in the community,41,42 closure of community based primary healthcare,43,
15 poor links between hospital and out of hospital services,44, 42 and the lack of community access to diagnostic services44 also contribute to the growth in demand. Higher levels of continuity of care are associated with lower ED use.45, 42 Equally the changing role of emergency medicine1 has attracted higher interest, expectations and confidence in the ED compared to primary care services.46, 47
• Health literacy and the ability to read and understand health related material appear to contribute to awareness of symptoms and the choice of health services.48
• Environmental risk factors including traffic pollution may contribute to the burden of ED visits for paediatric asthma.49 Thunderstorms may increase in asthma exacerbations50 and warm weather is associated with higher incidence of ED visits for paediatric asthma51 and heat-related diseases.52
• Demographic factors associated with demand include gender and age. Males are more common users of EDs.1 In terms of age, there are three peaks in utilisation rates: infants, young adults, and the elderly.16, 1 The elderly have the highest utilisation rates hence population ageing explains a proportion of the demand growth.53, 54
• Lifestyle factors such as diet, exercise, drug taking and risk taking behaviours are associated with increased utilisation.55
• Attitudes, perceptions and individual self-efficacy also contribute to demand including patient’s perception of illness severity.56-60

Demand Management & Policy Options
22
• Clinical drivers of demand include the increased number of high acuity patients (ATS category 1-3),61 increased rates of injury and poisoning,62 and higher prevalence of patients with chronic conditions.63, 45, 64, 41 ED utilisation is known to be higher amongst psychiatric patients, alcoholics and other drug misusers.65, 41, 66
There are known variations in use by time of day and day of the week. Throughout the literature temporal and demographic variations of emergency department attendances at single sites are described, but few have done so across generalisable samples.8, 67, 68 More patients present on weekends than midweek and in summer and late winter. 17 Presentation rates rise to a peak by around 10 am and continue at a relatively fixed rate until 8pm then decline to a lowest rate at 5am.2 Patients sustaining minor injuries are likely to present in the late morning and early afternoon.69, 8
The way in which the factors influencing demand contribute to the observable patterns of demand are unclear and require more detailed evaluation.

Demand Management & Policy Options
23
2. Demand management
Managing demand for emergency healthcare is problematic. The particular nature of acute health crises prevents normal strategies used in demand management such as queuing, and the prevailing public expectations of universal access prevent using price or service refusal to restrain demand.
While each of these is used to some extent to even out the peaks and troughs in demand, the public tolerance for waiting times and the clinical risks associated, lead to public and professional dissatisfaction. Similarly the variation in demand on an hourly and daily basis is such that matching demand against the availability of resources is not easily predictable except at the macro (population) level.
The question is how demand could be better managed or alternative services provided that may reduce the net demand on the EHS and yet ensure patient safety and satisfaction and thus public and political acceptance. The principal aim of this final element of the EHSQ study was to explore what is known of the interventions that have been shown to modify EHS demand. The specific objectives included:
1. To identify interventions that have been demonstrated to reduce attendances;
2. To assess the effectiveness of those interventions;
3. To identify the policy implications and areas requiring further research.
Methods
This is a descriptive literature review of both peer reviewed and publicly accessible “grey” documents that address the principal objectives. To be included in the review a study must report an outcome measure that impacts on attendance at the EHS. Whilst RCT studies are most favourable, they are often impossible and sometimes, an inappropriate technique. The literature review broadened its scope to include all study designs with appropriate outcome measures have been reviewed including RCTs, quasi-experimental, cohort, cross-sectional, and qualitative studies.
We utilised a comprehensive, systemised frame-work to utilise the most relevant quantitative and qualitative literature. Since the initial literature review for the EHSQ study had been conducted covering the years up to 2010,1 this study was undertaken to update the literature by searching for studies published after January 2011 up to the end of March 2014 (this update was undertaken as a Master’s project by Michele Romeo).

Demand Management & Policy Options
24
The following databases were searched: PubMed, Science Direct, ProQuest, EMBASE, Medline, and The Cochrane Database of Systematic Reviews. Google Scholar also supplemented these searches. The following terms were used to search and identify relevant articles:
• Emergency Health Service(s), ambulance, emergency department, demand, utilisation; demand management, afterhours, fast-track, helpline, telephone advice, queuing, client expectation, house calls, prehospital transport, non-urgent, co-located GP, primary care, co-payment, acute care, diversion, outpatients, clinical coordination.
• Strategies, solutions, policies, interventions, methods, practices, models.
Studies were excluded if they (or at least an abstract) were not published in English, the full text was unavailable, they were editorials or commentaries, did not identify or implement an intervention to address the outcome measure, namely emergency attendance.
Findings
A total of 2771 eligible titles were identified initially. Following the removal of duplicates (726), the titles of the remaining 2045 articles were screened identifying 347 potentially relevant articles. After reviewing the abstracts of these 347 studies, 179 articles were determined eligible for full review as they appeared relevant and significant. Studies were removed following detailed evaluation if they failed to address the study objectives or were not significant in contributing new information or their findings lacked impact. A final list of 13 eligible studies was included in the final review.70-82
The final articles are detailed in the Appendix Table including the titles and principal findings. The findings were then analysed for consistent themes and these themes have formed the basis of the following discussion. In addition to the 13 studies, many other studies from the literature review have been incorporated into this document to provide a cohesive and comprehensive insight into demand management programs and the background context.
The evidence to inform public policy initiatives that may act to reduce the level of ED demand was limited. The literature demonstrates confusion in terminology with the terms non urgent; inappropriate and primary care used and expressed in varying ways.83

Demand Management & Policy Options
25
It has long been identified that prevalence of chronic conditions or negative relationship with primary care services as well as socio-economic status, ethnicity, age, social deprivation, homelessness and health insurance status is a contributing factor to higher ED utilisation rates. 5, 8, 1 In addition, many reasons are cited in the literature for people attending EDs with the focus on the appropriateness of patient choice, particularly to their use alternative primary care services particularly patient’s lack of awareness of other facilities (including GP services); perceived seriousness or urgency of care; distance from the ED and primary care facilities; perception that better/ more efficient treatment provided in the ED and the convenience of 24/7 access, unreliable access and availability to GP out of hours.84-91, 58, 16, 92, 93
It must be remembered that the majority manage to seek their care in what the carers consider the most appropriate location, despite a lack of guidance or uniformity,4, 1 and that post-hoc assessments of appropriateness are meaningless to the patients seeking medical attention.94 However, from a patient perspective, they are seeking care at what they consider the most appropriate resource and in the timeliest manner. 1, 3
Agarwal et al95 found four themes that influenced the decision to use the ED: (1) anxiety about their health and the reassurance arising from familiarity with knowledge of the emergency service; (2) issues surrounding access to general practice (3) perceptions of the efficacy of the service and (4) lack of alternative approaches to care.95 These considerations of the factors that contribute to patient demand and the way in which they interact has been the subject of previous analysis and has informed the conceptual basis of this monograph.
Managing EHS demand
Our review has identified a range of initiatives that have been described as addressing demand growth. Few have high levels of research rigour, mostly they are descriptive in nature although some do address or evaluate the impact. In addition, the strategies identified may be categorised into universal strategies (those that apply to any users of EDs) and specific strategies (those that focus on specific groups of users such as so-called frequent users).
A thematic analysis has identified a range of issues and associated strategies which are described in detail below. These categories are not discreet but rather overlap and complement each other. They are presented separately merely to capture and present them. Because of this diversity, it is difficult to simply categorise the strategies. We have chosen a broad categorisation which is emerging from our research; namely

Demand Management & Policy Options
26
enhanced prevention, management on site and diversion to alternative services. Even still there is inevitable overlap between these categories.
Prevention
Prevention strategies include primary, secondary and tertiary prevention. The breadth of primary prevention involving health promotion and injury/illness prevention is beyond the scope of this review. It is also beyond the capacity generally of the EHS to influence except in a broad way as a contributor to public awareness and public health interventions.
However studies have demonstrated reducing demand for emergency care can be achieved through improved injury and disease prevention.22 Older patients, as the group with the highest utilisation rate for emergency care has received the most focus.96, 97 Secondary prevention strategies enhancing primary care management of patients with chronic disease condition and who may be frequent attenders through active case management, is challenging and the provision of these services are significantly resource intensive with the benefits unclear.98 Tertiary prevention encompasses emergency health care generally but include in this context, alternative treatment option.
Enhanced primary care
There is growing concern regarding the volume of patients turning to EDs for non-urgent or primary care.159, 94, 160 They are seen by many as a source of problems for EDs, causing prolonged waiting times, inefficient care, staff stress and preventable costs.161, 46, 83
Little consensus exists as to how to define and measure non-urgent visits or the more problematic descriptor of “GP patients”. It is difficult enough to define a GP (considering the diversity of GP practice scope) much less to categorise patients with undifferentiated illness into a category based on where they should receive care.
There is little research which describes specific populations who utilise EDs for non-emergent visits, or even why they are doing so. Further, there is very little examination of individual decision making to present to the ED and what factors may influence this.
One study in the US suggested that people with insurance had fewer non-emergent visits.162 Studies have further exhibited higher rates of such visits among the elderly, patients with mental health concerns, among the lower socio economic populations, in paediatric patients and those without a GP.163 For some, the ED is seen as a place that is most appropriate for critical or emergency medical concerns. For others, the

Demand Management & Policy Options
27
ED provides access to medical care out of hours with self-perceived severity of complaints, ease of access to emergency care and ready primary care provider availability have also been described as the most influential factors in the research.72,
74, 46, 83
The decision to attend an ED is likely a complex one. Presentation to the ED may occur due to a complex interplay of personal, practical and emotional factors, in addition to the physical concerns. Regardless of the medical urgency of a patient’s condition, if the patients and/or caregiver perceive the complaints serious enough to warrant medical evaluation the same day they will continue to utilise the ED2 and on all objective assessments they get it mostly right.164, 3
To reduce the burden on the ED, various initiatives involved providing primary care within (or attached to) the ED. These measures have included providing primary care services within ED,161, 1 encouraging regular primary care provision,161, 1and making the GP as the ED gatekeeper.161 Other initiatives aimed at improving primary care access including the use of telephone triage,1 public education,87-89 and co-payments.165 However, the effectiveness of such initiatives on reducing the demand for ED care in long-term is unknown.
Within the broader literature many studies have compared GP and usual medical care in EDs. However there is limited studies looking at the effect of this type of intervention and its impact on ED demand. From the research, a single contact with a GP working in an ED does not appear to have long-lasting effect on health service use and in particular subsequent ED attendance.8, 166, 1 However, brief focused interventions have been shown to have lasting effects in other settings.8, 166, 1 People will continue to attend the ED for healthcare which service providers define as more appropriate for primary care. There is strong argument that a more appropriate action is for the system to adjust to this requirement rather than attempting to adjust patient behaviour to fit the system.8, 166, 1
It is recognised that improved access to primary care could reduce the number of ED attendances and continuity of primary care may enhance chronic disease management and thus decrease the number of ED attendances for acute exacerbations. General practice models can range from solo practitioners with no integrated health team support to practices operating with onsite diagnostic services and multi-disciplinary health teams. A comparative study to evaluate the effect of mortality in frail older people undertaken in Canada demonstrated the benefit of integrated care practice.76 Researchers found that for the intervention group (with integrated care) there was a reduction in hospital admission and total hospital days as well as a 20% reduction in ED visits.76

Demand Management & Policy Options
28
The introduction of new services for out-of-hours GP care is a key development in primary care. However very little research has been published on the effects of this change on ED utilisation. This is surprising given that recent patient surveys have found mixed results in relation to their preference for out-of-hours care. 167
There is little evidence that co-location of GP services with the ED reduces ED demand. Theoretically the co-located out-of-hours primary care centre with the ED is an opportunity to remove the responsibility of choice from the patient to the health care providers.160 Anecdotal evidence suggests that co-located GP clinic simply transfers demand from the community to the co-located clinic and does not impact on ED demand.168 A research team of emergency physicians concluded as a result of a study into the variety of methods for calculating GP type patients presenting to the ED, that GP practice clinics collocated with hospital emergency departments are not an effective use of resources.160
Case management of frequent users
Patients who use the ED on multiple occasions have been coined the term ‘frequent users’, and numerous studies focussed on this group.10, 99, 100 This population has received different descriptive names: frequent users, frequent flyers, heavy users, repeaters, recidivists or frequent attendees.10 The risk factors or potential predictors of high use ED utilisation have been found consistent across developed countries. Frequent users represent a relatively small group of patients accounting with a disproportionally high number of visits to hospital EDs.63, 88, 101-108 Older patients is the group are consistently reported as the most frequent presenters to EDs followed by complex chronic conditions, mental health and people from lower socioeconomic groups. These small groups of patients have been the focus of interest and concern in emergency medicine and health policy for the last 40 years.109, 110
Frequent use by specific patient subgroups of hospital EDs has been reported in many countries and health systems.63, 101, 103, 111-125 The definition of what constitutes a frequent user varies worldwide and within studies, ranging from three contacts over a six month period to more than ten visits over the same period.126, 127
Reasons why some patients repeatedly use EDs vary.103 Some studies point to the lack of a primary care physician,128, 129 while some other reports show that the majority of frequent users have a primary care provider.130-133 Other possible reasons include unmet medical and non-medical needs134 or the appeal of complementary care and treatment at the ED.135 Understanding better the characteristics of these patients may help reduce their attendance.

Demand Management & Policy Options
29
The literature has focused on the following 3 reasons for frequent attendance at the EHS: 136, 137
1. Appropriateness: EDs are not designed to provide longitudinal patient care over repeated visits 138 139, as it is often considered that these frequent users are not in need of hospital care and are illegitimate users of ED resources.140 141 In turn, this influences the quality of care they receive.142 However, frequent users are often seriously ill patients in whom rapid and frequent health crises may characterise the severity of their illness. They are also more likely to be unwell and report chronic medical conditions 146,147, 132 with a higher rate of mortality148, 149 and consume more health resources. 132, 135
2. Cost. Frequent users of the ED generate high health care costs and suggest that appropriateness of care, rather than access and/or attachment to a healthcare provider may be an issue for users as well as that very few settings outside the ED can provide the level and rapid access of care. 103, 143, 133
3. Vulnerability. Frequent users (compared with non-users or infrequent users) of EDs have been recognised to be of more vulnerable and of greater disadvantage (ie: more likely to be of low socioeconomic status130,132 isolated, and living alone144,145).
A systematic review identified 11 studies assessing the effectiveness of interventions targeting adult frequent users of hospital EDs.103 Eight of these interventions involved better case management. Almost all studies observed a reduction in the number of ED visits. Researchers purported that case management could reduce ED costs by at least as much as the cost of the case management team. 150,151,152, Only one study reported an increase in ED use after the introduction of case management. 122
However the researchers of this study argued that this increase may be considered a sign of better integration and service quality and that case management may reduce cost as well as improve social (and some clinical outcomes).
An historical cohort study of pilot RAP (Resource Access Program) records and administrative data for patients enrolled in the program over 15 months suggested that an EMS based case management and referral program is an effective means of decreasing EMS transports by frequent users.153 Whilst it had only a limited impact on use of hospital services the researchers recommended that the case management program such as RAP could be integrated with existing models of intervention resulting in additional benefits.

Demand Management & Policy Options
30
Discharge management
Initiatives in the ED may contribute to a reduction in re-attendance. As well as its effects on delayed discharged care the role of social support can have an effect on ED demand.80 Studies have examined the introduction of social workers to EDs to facilitate safe discharge home either directly from the ED or following admission.154,
155 The use of the social worker in this intervention has been seen as positive from both patient and clinicians with reduced return visits.155
Representation to the ED shortly after hospital discharge may reflect poor in-hospital care or poor follow-up and planning during hospitalisation.125 A telephone call to a recently discharged patient to provide answers to patients’ questions about medical conditions or medications and improve patient well-being, satisfaction and clinical outcomes. A before and after study was conducted to evaluate the effects of post discharge telephone calls on the rate of ED visits within three days following hospitalisation in paediatric patients.80 It found that post-discharge telephone calls by NPs involved in the patients’ hospital care reduced the rate of ED visits within three days following hospitalisation.80
Enhanced community nursing
Nurse practitioners (NP) in the emergency setting have been widely used in Australia and internationally for the past 30 years.156 It is well documented in the literature that patients are satisfied with the care they are administered and they have been shown to be as safe as junior doctors.156 What is not well documented is the impact of nurse practitioner in home care on ED use.
In Canada researchers investigated whether the management of home patients by nurse practitioners who conduct appropriate assessments and treatments in the home led to a reduction in unnecessary ED visits.77 This pilot study examined changes in ED use when nurse practitioners manage homebound older patients in their homes. They collected prospective comparative information from records of patients who received at least one home visit by a nurse practitioner (intervention group) and patients who did not receive a NP intervention (control group). The researchers found more ED visits were documented in the control group than the intervention group.77
Using technology to avoid admissions
Controlling costs whilst maintaining and/ or increasing access to care, ensuring patient safety and improving quality is challenging and has intensified with the changes in demography. With chronic disease on the rise, new delivery models and technology may help minimise the cost and the increasing burdens on those affected,

Demand Management & Policy Options
31
their carers and the health system.157, 158 Technology and disease management programs for chronic conditions has a key role to alleviate this burden, and to improve the health of patients and reducing cost outcomes.
Tele-monitoring of chronic patients is one of the programs aimed at improving the quality of life of patients and their families as well as reducing health care costs. A study to determine if tele-monitoring does impact on ED use visits for home health patients receiving skilled nursing services was undertaken by Wood and Snow.79 The researchers found the patients in the tele-monitoring group had a significantly lower rate of ED visits.79
Walk-in or urgent care clinics
One specific primary care intervention has involved the introduction of ‘Walk In’ or ‘Urgent care’ centres. A few articles have been written assessing the impact of Walk in Centres (WICs). In 2009, GP walk in centres were established in the UK as a way of decreasing unnecessary attendance at the ED, by promoting GP accessibility.70
However, this did not seem to reduce demand for ED care.70, 71 Another alternative proposed source of care for unscheduled patients are Nurse-led walk in centres.70
Arain et al. undertook a survey of patients visiting a Sheffield GP WIC over 3 weeks in September-October 2011.70 A short post visit questionnaire was also sent to those who agreed to participate so as to determine if the patient had used another NHS service for the same problem. A total of 529 patients responded to the survey (51% response rate) with 64 of these patients reported they were diverted from going to ED in the survey period as a result of the establishment of the GP WIC. The introduction of a WIC was shown to reduce GP type daytime attendances at an adult ED although the after-hours attendances (when the WIC was closed) did not change.70 The reduction in patient load at the ED indicated in this study is that of GP-type attendances only and not total ED attendances and this reduction may have been the result of opening of the GP WIC.
At the same time as the above survey, Arain et al70 conducted a mixed method evaluation consisting of cross sectional survey, review of ED administrative data and qualitative surveys of two WICs in the UK to understand more about community needs and satisfaction with WICs. Based on the sample of 1030 patients 93% of patient were fairly/ highly satisfied with the service of Centre A and 86% at Centre B. The researchers found that the difference in satisfaction between the two centres was due to the longer reported waiting times to be seen in Centre B. There was no difference in satisfaction between first time users and repeat users. Most patients reported the reason for attending the WIC was because they were unable to access a

Demand Management & Policy Options
32
GP without an appointment (50%) or because their regular GP clinic was closed (9%).70
Minor injury units
As part of a service reconfiguration, Minor Injury Units (MIU) were established in some countries, e.g. USA, Canada and UK, in a variety of settings, mainly co-located within a Primary Health Clinic or nearby an ED, but these have not been extensively studied.166 Rudge et al169 explored whether the proximity to a MIU affects the extent to which a patient use an ED and found that this was significant and attendance was greater in populations who lived further away from them, suggesting that MIUs may reduce ED demand.
Emergency care practitioners
Emergency care practitioner has been adopted to cover clinicians working in emergency care who have skills that apply across traditional boundaries. Lately it has applied to ambulance paramedics with extra skills and training to increase the diagnostic and clinical management abilities,1 but it has also been applied to nurses who have expanded their skills in pre-hospital care and other professional groups working in EDs. We have been unable to locate any studies that have evaluated the outcomes of this as an intervention.
Patient centred medical home
As patient centred medical home models and related innovations emerge as a key vehicle to improve the quality of health care and control costs have shown improvements in provider experience,170 patient experience,171, 172 processes of care,173-175 practice level composite measures of quality of preventative care utilisation176 as well as reduced emergency visits.177 This is a particular policy focus of the Australian Medical Association and has been financially supported by the Australian Government through specific pilot scheme.
A US based study found that this model of care reduced ED utilisation by 5-8% among chronically ill patients but not for non-chronically ill.177 By improving coordination of care and reducing the likelihood of complications by reducing delays in treatment, the study suggests the conceptual models of patient centre medical home that this may lead to fewer ED presentations.178
Improved end of life care
One of the more difficult situations encountered is the transfer of patients, sometimes from high level residential aged care facilities for terminal care. Not only is this

Demand Management & Policy Options
33
inefficient but it is often inappropriate on both humanitarian and clinician grounds. Factors that influence this is poor end-of-life care planning and the reliance often on junior nursing staff at aged care facilitates. We have been unable to locate any evaluation studies of the impact of interventions aimed at improving end of life care and the impact of such strategies on EHS demand.
Diversion
Diversion describes the notion that patients who seek acute health care could be diverted to an alternative source of care. Ambulance services in Australia have taken such steps to combat rising demand.179, 180 The introduction of referral services has been documented to reduce the rate of transportations, however, over time did not slow the steady increase. Further while referral services divert and increasing number of emergency calls the rate continues to accelerate.53
When a person telephones the emergency access number they have traditionally received an ambulance response and over recent years this has invariably been a paramedic response. In most states, ambulance services use a priority dispatch system to determine which calls require a fast response because of life threatening conditions, and which cases may not require lights and sirens. A systematic review of ambulance dispatch and prioritisation systems in the UK8 found conflicting results finding that the accuracy was limited with poor evidence for their safety and clinical effectiveness.
Paramedic treating and not transporting
The perceived tradition of ambulance services has been to offer immediate care, stabilisation and transfer the patient to a source of safe ongoing care. However it is recognised that about 20% of patients are not transported.2 Either they decline further treatment or there are no clinical grounds for further treatment. This later may be determined by agreement with the patient but is heavily reliant on the professional judgement and advice of the paramedic. A small proportion of patients (2.4%) refuse treatment and/or transport against the paramedic’s advice.2 The value of professional advice of the paramedic has been improved with upgraded training and education (to university level) and through the introduction of experienced supervisors in the field.
The reliance on paramedics’ clinical judgement does pose a risk as the paramedics lack the ability generally to be able to support that judgement with appropriate investigation and to rely on higher level clinical judgements that would be available in an ED for example. However the risk remains for all clinicians that judgement made in good faith may occasionally be incorrect. Mechanisms aimed at reducing risk

Demand Management & Policy Options
34
may include seeking advice and support from more experienced clinicians or those with higher levels of education and training. They may also be reduced by implementing arrangements which provide technological support and ongoing monitoring. Finally they may also rely on follow up with patients to ensure their condition has improved. Most ambulance service lack the capacity in the light of often overwhelming demands for service to provide such follow up.
We have not been able to locate reliable high quality studies that have explored the effectiveness or cost effectiveness of such strategies. Anecdotal responses from paramedics suggest such efforts often take considerably longer and are more resource intensive than simply transporting the patient. However once the patient is transported then they often enter a continuum of care which is difficult to extract them from. Studies investigating the alternatives for emergency cases that are neither life threatening or serious concludes that the evidence that supports the alternative approaches should to be developed.181, 182
Telephone triage and advice centres
Telephone triage and advice centres have been established in Australia183, 184 and elsewhere185 with the aim of advising patients about available health care options and diverting potential non-urgent users away from EDs. In Australia, the national Health Direct and the Queensland based 13 HEALTH telephone advisory service are run by trained nurses, while the UK’s NHS 111 is run by non-clinical advisers supported by healthcare professionals. We did not find any studies on the effectiveness of the Australian services in reducing ED demand. However, a pilot study in four sites in UK found that in its first year of operation, the NHS 111 intervention did not shift patients to urgent centres rather than ED care. The researchers further concluded that there was “potential that this type of intervention increases overall demand for urgent care.”78
Patient education
Patient and public education has been tried in many areas of health and medicine to change or improve health behaviour. These may include phoning for advice before going to the ED, publication of waiting time information, and TV and roadside advertisements. Education of patients as to what types of conditions are appropriate for ED is widely advocated and government campaigns are run regularly.1, 2 Public education programs have had some success in reducing attendances at the ED, although their long-term sustainability is not documented.1, 2
A before and after intervention study was undertaken in a regional hospital system in the United States.82 A 20-page booklet was given to parents of children aged 10

Demand Management & Policy Options
35
years and younger with the instruction that it contained could help provide non-emergency care for their children at home and make better decisions about when emergency services may be needed. The researchers concluded that the education intervention allowed parents to more effectively utilise the level of care appropriate for their child’s medical needs and that the intervention substantially and significantly reduced paediatric use of the ED.82
A comparative study was conducted in the ED of a large adult tertiary-referral teaching hospital in Queensland, Australia.73 The study used administrative data measuring three outcomes post campaign period, i.e. arrival mode (measuring ambulance usage), triage category (measuring clinical urgency) and departure status (admitted vs non-admitted) and compared with those 3 months pre- campaign period. The researchers found that the campaign had no significant impact on the arrival mode of the patients. However, after the campaign, while the number of patients with higher illness urgency decreased, the odds of patients being admitted increased.73
Providing ED waiting time information to the public has been proposed and implemented in some jurisdictions in Canada.186 As hospitals must now report time spent waiting to be seen, hospitals have begun to advertise ED waiting times on the Internet sites, billboards, smartphone applications, Twitter and text messaging publishing waiting time information of different providers so patients can make informed choices on which provider to use has been suggested as a mechanism to reduce lengthy ED wait times.186, 187 Commentary on the publication of posted wait times is that posted wait times are shorter than actual wait times and that while most hospitals have made their wait time calculation methods available, most consumers do not read the fine print.186, 187 A before and after study was undertaken to test whether or not individual patients used published wait time to decide which hospital to visit.186 The researchers found that the rates of wait times exceeding 4 hours decreased after publication of wait time information even though the average wait time experienced a slight increase. The study also found that after controlling for other factors, the site with shorter wait time had a higher likelihood of being selected after the publication of waiting time information, but there was no relationship before the intervention. Also, those opposing posting ED wait times raise concerns that patients with time critical conditions may inappropriately chose their ED based on the posted wait time and not on medical as they may be unable to take the urgency and complexity of their condition.186

Demand Management & Policy Options
36
Co-payment and financial incentives (or disincentives)
Previous research involving a survey found that patients were more willing to pay for same day care than if they made an appointment.188 It is recognised in the USA that there are significant variations in how people use EDs and this is associated with their financial capacity; those with responsibility for partial or full payment were associated with fewer non urgent attendances in an ED.189
Co-payment systems have demonstrated their ability to reduce ED demand. The greatest impact is on non-urgent attendances at ED departments. However there is also evidence that is reduces attendances in urgent cases.190, 191 As such the safety of such systems should be questioned.190
A cross sectional comparison of utilisation rates of ED between employees with a sponsored Emergency Room Utilisation Management Initiative (ERUMI) and others in the region without a ERUMI was undertaken in the United States.192 The ERUIM is a combination of increase patient co-payments for ED visits with educational outreach aimed at reducing inappropriate ED use and encouraging use of retail health clinics for acute but not life threatening health conditions.192 The study compared patients over a 6 month period -before the plan (baseline) and compared this over a 6 month period whilst on the plan fining ED utilisation for conditions that could be treated appropriately elsewhere (ie: the encouraged retail health clinics, walk-in clinics and urgent care centres) decreased by 10.39 visits per 1000 members in the intervention group versus 6.29 visits in the comparison group.192
Requiring pre-authorisation for reimbursement of ED care is now common in the USA.189 Co-payment systems are often associated with systems of pre-authorisation for attending the ED.189
Private Hospital EDs
Our research has also sought to explore the role of the private hospital sector. While 47% of the population are privately insured in Australia, only 6% use private hospital EDs for their emergency healthcare. This choice by patients is influenced by perceptions of cost, balanced against waiting times. It is also influenced by a lack of awareness of private hospital ED capability and by the advice of paramedics and other health professionals. Enhanced awareness of the scope of private hospital EDs by both the public and professionals along with changes to financial arrangement and insurance policies may alter these choices.4, 193

Demand Management & Policy Options
37
Conclusion
The aim of this section was to review potential solutions to the observed growth in ED demand by identifying interventions for health practitioners and policy makers to help focus future policy, practice and research. Demand for emergency care is growing by around 2% per capita each year1 among the more urgent categories, across both genders and all age groups. There has been a tendency to blame the patient, labelling them as ‘inappropriate users’.1 However, our research has demonstrated that the decisions that patients make to access an ED is usually a well-considered decision which is often supported by advice from family, bystanders or health professionals.4, 194, 195
Much of the current literature is based on either single descriptive case studies or expert opinion, and therefore does not provide a robust basis for policy and practice. The methodological rigour of the evaluation is limited for the majority of the studies making what practitioners and policy makers should do challenging.
There is no consistent evidence of the effects of improved primary care access on the demand for ED care. Nurse led telephone advisory services, public awareness programs on appropriate use and extended primary care have not definitively been shown to reduce ED demand,194 with the safety of these primary care ‘gatekeeping’ measures unknown.98 The argument that if GP services were open for longer, or were more generally accessible, this would alleviate the demand for ED services may require changes to primary care or the creation of acute care centres such as walk-in clinics and minor injury units or greater reliance on community based mobile services to care to patients in their own home. Yet there may be some challenges with this policy approach as analysis of ED attendance rates, increasing deprivation, increased patient age, smaller practice list and lower reported satisfaction with practice telephone access have all been found to be associated with higher use of ED.40
There is remarkably little evidence of the effect of telephone triage and advice services, given that their primary objective has been to improve and simplify access to urgent care.196, 197
It is probably unrealistic to think that any one, or series of coordinated measures designing to increase efficiency may be an effective strategy to reduce hospitalisation and ED visits for patients. Follow up of patients may reveal inadequacies in their care that may require simple advice, referral to a GP or a home visit. Providing patients with reassurance, advice of medical alternatives an effective way of providing health information, managing remaining symptoms, recognising complications and may reduce unnecessary patient ED visits.1, 77

Demand Management & Policy Options
38
On balance, this review of the literature has identified the following concepts as requiring additional research focus:
• Co-payment systems may reduce attendances but may equally reduce attendance by those requiring emergency care;
• Patient education is unproven in most areas except chronic conditions. Telephoning for advice before going to the ED may reduce attendances;
• Publication of waiting time information leads to patients selecting the site with shorter wait time and reduces the rates of lengthy wait time;
• Primary integrated interdisciplinary practices may reduce ED demand;
• The role of paramedics and the impact on ED demand needs evaluation.
Whatever the solutions, an array of strategies aimed at moderating the growth in demand may assist provided they include illness reduction, community care, and diversion to alternative services.4 This framework used in the analysis of the literature is also used to evaluate potential policy solutions in the following Chapter.

Demand Management & Policy Options
39
3. Policy analysis
Introduction
The previous section presented the results of our literature review on programs and initiatives that aimed at reducing demand for EHS. In this chapter we present the results of the final phase of the research project which involved initial face validation of the demand management policies and initiatives utilising a small expert reference group.
The aim of this aspect of the research was to test the clinical and policy relevance of proposed interventions from the perspective of the leading clinicians, policy makers and researchers, and thus guide the future policy by identifying and evaluating interventions to better manage the EHS demand. The study is based on a conceptual logic that was identified through the literature review (previous chapter).
Accordingly, strategies aimed at moderating the growth in demand may be broadly categorised as:
1. Those aimed at improved primary and secondary prevention particularly better management of chronic disease. Primary prevention involves not only promotion of healthier lifestyles, risk reduction, surveillance and early detection but perhaps more effectively secondary prevention through reengineering of primary healthcare to ensure more integrated and accessible care.
2. Those aimed at diversion of patients to more cost effective services including private hospital EDs, pre booked services such as outpatient clinics, integrated primary care services that manage minor emergencies, and community based/mobile services and community based mobile services.
3. Those directed towards sustaining patients in their own home when they fall ill involving greater reliance on family supported by home monitoring and home based interventions such as hospital in the home (HITH), hospital in the nursing home (HiNH), and e-health/tele-health.
Methods
This was a small qualitative pilot study performed using semi-structured open-ended interviews intended to complement the findings from the literature. A total of six participants were involved in the study. Participants were a purposive sample

Demand Management & Policy Options
40
including EHS medical directors, EHS researchers and EHS executives. Purposive sampling was used to maximise diversity and to provide the broadest representation.
An interview protocol was developed based on the literature and refined through consultation with senior researchers in the field. The interview initially asked about the participant’s general knowledge of the issues and their experience. They were then provided with a description of the research, the findings from the literature and a suggested conceptual framework and definitions.
The interviews comprised of seven core questions:
1. Why is EHS demand management important?
2. What do you think are the two or three main issues of EHS demand management and why?
3. How big is the problem and how do you quantify it?
4. What strategies (interventions) do think are useful to mitigate EHS demand management and why?
5. If you have tried these strategies what was the impact on demand, staff and the organisation?
6. Literature has identified three main approaches including prevention, enhanced primary care and diversion. Do the strategies you have tried apply to one of these categories? If yes why, if not, can you think of another suitable category?
7. Is there anything else you can contribute to this topic and investigation?
Nine stakeholders were invited by email on 1 September 2015 to participate in this study. Follow-up telephone contacts were made and suitable dates for interview found with those willing to participate. Three stakeholders declined the invitation because of their workload. Interviews were held between 4 and 15 September 2015 by the first principal author. An initial (training) interview was conducted to improve consistency of interviewing style. Three interviews were conducted by telephone and three conducted in person. The method of interview was determined by practical considerations and convenience. Only the participant and the researcher were present during the interview. Interviews were audio recorded and field notes taken by the interviewer. Interviews on average lasted 30 minutes. Interviews were transcribed by an independent professional transcription service. The researcher reviewed the transcripts to ensure comprehensiveness and quality of the responses. All transcripts were reviewed and coded by the researcher. Some codes were anticipated, others

Demand Management & Policy Options
41
were generated after multiple readings using a list of broad themes derived from the main categories of the interview schedule.
Data analysis was performed according to thematic and content analysis techniques. Data analysis was conducted iteratively as the data was collected. To ensure confidentiality during analysis, interviews were assigned and identified by a code prior to interview data being transcribed and analysed. Conventional content and thematic analysis was undertaken with interim analysis of early interviews to ensure there was no necessity to adjust interview schedule to include unanticipated themes as prompts for subsequent interviews. Cross cutting themes and recurrent patterns were identified and examined for analytical correctness.
This phase of the research received ethical approval from the QUT Human Research Ethics Committee on Monday 31 August 2015 (approval number 1500000670).
Findings
The themes that were identified from the interviews are presented within the concepts of importance, key issues, extent of problem and what can be done to manage EHS demand.
Why is it important?
Overall respondents were of the view that there are a number of challenges facing the Australian healthcare system that tests its ability to deliver effective, efficient, and responsive services to the population. These challenges are well documented throughout the literature and include the increase in demand for services, ever increasing costs, availability of workforce, and intensifying community expectations.
‘…increasingly aware of the demand that’s being placed upon our health care systems in Australia, particularly at the end of the spectrum which is based in emergency and given a whole range of things including growing population base, shifting patterns of disease, increasing patient expectations of health care quality, increasing technology and the digital economy.’
‘… we’re obviously getting more and more people through the door, as I’ve just explained to you. There’s an array of reasons for that. One, we’ve got that growing aging population. I think we’re seeing out nearly 2% population growth in Queensland a year. However our attendances into emergency department and in fact attendances into GP are growing at 4% and 3% respectively. There is a differential

Demand Management & Policy Options
42
there between population growth and growth in ED presentations. What that equates to I’m not really sure.’
The respondents indicated that increased patient volumes and congestion are challenging the safe delivery of EHS services.
‘…essentially the front door gets busier and busier, the expectations of what we will do within the department are more.’
with another acknowledging that
‘…there is only so much finite work a human resource population can deliver with regards to emergency medicine care.’
Public health services are showing clear signs of tension and the increasing pressure is unsustainable.
‘…demands on our healthcare systems [particularly] in emergency are increasing and it’s becoming increasingly so a pressure point for the health care system.’
The ageing of the population, coinciding with rising wealth and biomedical technologies is tending to change both the underlying demand and the expectations of the community. This is placing the Australian health care system under increasing strain.
Respondents identified that there are many repercussions for staff in a health system under this kind of strain. The workforce often struggles to maintain morale; they have high workloads; they often feel that they have limited or no control over their working conditions, and they lack the ability to make decisions.
‘…well, when workers and systems that are overworked, especially chronically overworked, well they’re going to burn out and slow down and start making more errors and recruitment and retention become problems.’
‘..this is a big issue for the community given we have got an ageing population. We hear about it but it’s actually starting the really ring true. The elderly in the community require higher rates of intervention from the health system.’
The increasing demand for emergency health services represents a crisis that may affect the quality, patient safety and access of health care. EHS congestion causes delays in diagnosis, delays in treatment, decreased quality of care and poor patient outcomes.41

Demand Management & Policy Options
43
‘…my concern, and I’m sure my colleagues concern, is that when the system or the individual becomes overwhelmed with demand, that’s when care starts to become compromised. My ultimate concerns is that if we do not have demand management, then we’re going to see pockets or wider spread areas where providers are overwhelmed and as a result patients will suffer because their treatment is not delivered in the appropriate timeframe, so safety and quality of care can be compromised out of delays. Furthermore, safety and quality can be compromised if providers start rushing and taking shortcuts and omitting detail or overlooking injury or illness. ‘
What are the key issues?
The respondents identified a range of issues that speak to the reason why patients seek acute health care within the professional EHS.
Safety Net: The EHS has always been available to help if all else fails in the health system. In the ED, services are provided to everyone regardless of their ability to pay, 24 hours a day, 7 days a week and as such the EHS serves as the as the health/social safety net.
‘… there tends to be this idea that ED is the place, which effectively formed almost a safety net for the community.’
‘… people turn up at the ED and we tend to be seen as a bit of a safety net.
EHS is often a reliable point of access to the health care system for many; particularly vulnerable and disenfranchised people:
‘... seems as if at times when [alternatives] do fail, and not infrequently, and for all sorts of different reasons…. that we seem to be all things to all people and when the wheels fall off we tend to be the ones who end up seeing the patients.’
Convenience: The choice to utilise the EHS may be attributable to the convenience and ease of access to emergency services, relative to primary care services, close to their home.
‘… is just the whole sociological concept of convenience. Unfortunately emergency departments are too efficient and too effective as one-stop-shops. You can see the doctor, you can get your blood tests done, you can get your x-rays done, you get the results almost instantaneously, you get your interventions, your consultations- you get everything done. For people who think they are time poor; the hospital is closer. It’s just far more convenient to stop into the emergency department.’

Demand Management & Policy Options
44
‘… there are no deterrents to stop people from turning up and there is not perceivable incentive or value to go to an alternative source.’
Several factors lead patients to choose the EHS instead of primary and specialized health services; these included preference to receive care of the same day, access to ancillary, laboratory and radiological services as well as the belief that EHS services are able to solve complex types of health problems.
‘…there is a perception that the health system is free and free for everyone 24 hours a day, seven days a week. That needs to be, it’s free for you, if you need it, but if you don’t need it… bugger off and go away and stop utilizing valuable-- the health service has never been seen as a restricted capacity system. But it is a restricted capacity system.’
‘… again from data and analysis, that patients in triage category 4 and 5 are not patients that ordinarily need to be seen by emergency care teams. It’s not that they can’t its more of a question of the fact that they have conditions, or ailments, or illnesses that are readily treatable manageable by other health care workers in the health care system.’
It was recognized that it may be medically unsafe to create barriers to EHS care for patients who need care.
‘…we don’t care about them because they are so easy to sort out, we can just discharge them and send them home… our focus has been on the sick patients who should be in the emergency department who we cannot get out when we have finished with them…’
It seems more appropriate to identify what needs this subset of patients has and to tailor the delivery of resources to meet those needs. Efforts to steer patients away from the EHS triage desk may do more harm than good if patients cannot get care elsewhere. Financial disincentives may deter patients from using the EHS for serious or even life threatening conditions. Seemingly minor symptoms may be the indicator of a more serious or even life threatening problem.
‘…there’s this huge anxiety that that public message will discourage people who should be at the emergency department from turning up. We are so risk averse around that particular message that no-one’s prepared to push the ‘don’t come to the emergency department’ story because they’re worried. The public health campaign’s about ‘have you got chest pain, you need to come to the hospital’, ‘have you got a stroke, you need to come to the…’ it’s all time critical. That completely overwhelms every other driver around public message.’

Demand Management & Policy Options
45
Perceived quality of care: There was a view that people have reset their expectations and standards for when they seek medical care.
‘…in simple terms people go to a doctor for all sorts of ….reasons that they don’t need to be there for. I think that’s one large complex cultural social phenomenon that we need to address in some way, in that we see people by the thousands who turn up at our EDs who’ve had a cough for 24 hours, or who’ve had a fever for 24 hours or who’ve had a sore ankle since yesterday or whatever it may be.’
‘...there are a large proportion of patients that come into our emergency departments who truly need emergency department care; the elderly, those with chronic conditions and multiple comorbidities and the critically unwell. A large proportion of what we see [in the ED] needs to be seen and we can’t take away from that and a variety of reasons and we can’t down play that. There is however a segment of our population who attend the emergency medicine care who for a variety of reasons aren’t as sick as they think they are.’
‘…that business of looking after yourself and having self-interventions, it seems to have just disappeared from the community. That’s one thing that I think is an area of activity for us….resetting peoples expectation about health and needing medical assistance.’
The concept that primary health care is struggling in a health system that continues to emphasise the importance of technology-oriented specialty care was also raised.
’….there is a long term problem in the health system in Australia around devaluing primary care… the role of the general practitioner as the medical home has just been continuously devalued.’
‘… this has been driven by the medical profession..[that] there’s been a hospital centric model of care for some time, so when people who get referred up to the hospital for a specialist consultation then continuously get brought back to the hospital to have their care year, after year, after year… they begin to see the hospital as their medical home rather than the GP as their medical home.
Measuring and monitoring the performance and quality of EHS services is believed to have created more demand itself.
‘… broadly speaking, in a system which shouts from the rooftops how much better EDs are performing and, it’s a badge of honour for a Health Minister or a Director-General to say “wow, look how awesome our EDs are, we’re going to see 80% of you in four hours” and it’s all part of the election commitments and the hype and everything.

Demand Management & Policy Options
46
People hear that think “wow, I can go there and get all of that in under four hours 80% of the time. Why would I do anything else, and it’s free”…’
‘… when it comes to emergency health service demand one reality is that it doesn’t matter how many patients come to our emergency departments everyday, ultimately they’re all being seen. So while clinicians and communities are frustrated that the waiting rooms are full and that the times in the ED are long, another observer would say everyone who came yesterday was seen yesterday, so what’s the problem? ‘
Limited Health System Literacy: Another challenge is at what capacity people have to obtain, process and understand basic health information and what services they need to obtain the best medical attention.
‘…I think probably it’s a combination of health literacy and of system literacy. People have to understand enough about their condition and have enough or a sense about that in the context of knowing how to navigate a system. I just don’t think half the time the medical or the health professions really have a good understanding of what it is that each other do and what role they play in the system, so then how can a patient possibly be expected to? I think that people don’t really have an understanding; they just think I’ll go to the ED. They don’t realize they can get this somewhere else, they don’t realize in fact they need physiotherapist for that not an emergency department, or whatever it is. I think health literacy and a sense of system literacy and a sense of amenities you need to come to an ED. It’s a sort of literacy and education in a way.’
Availability of Alternatives: The EHS plays multiple functions for the population: 24 hour access to comprehensive services within the hospital (including subspecialty care) at no cost. The EHS also functions as an alternative source for primary medical care, particularly out of hours.
‘… until we can offer alternate models of care to manage this demand, what we’re stuck with is ambulances and private cars and walk-ins just arriving at our department at their own discretion.’
‘…we need to look at it from an emergency perspective and where GPs might have a role to play. I am not convinced the community – we’ve talked about EDs being able to provide a whole service for a patient, you go there, yes, you may have to wait two three of four hours to been seen … but where I live, I try to get into a GP and I have to wait 24-48 hours.’
Attempts at establishing alternative care settings for (urgent) non-severe care - typically GP extended hours with on-site X ray and laboratory testing have had limited success in reducing presentation to EDs.

Demand Management & Policy Options
47
‘….I still don’t think there’s anywhere, despite all of the hype about medical centres and the multidisciplinary nature of them and the way in which they say they provide radiology and pathology …who have extended hours.
‘…..the idea that if you have an acute problem, which are you going to choose – 24 hour GP clinic which may or not be well resources, with a doctor you do not know or a very well-resourced emergency department…
Reasons for this included the geographical disparity of these types of alternatives.
[These medical centres are still] ‘a minority in any given geographical region of an urban area [and] there might be only one of those relative to a much larger population. So yes, whilst of course they’re a good idea, I’d never say they’re not a good idea… but then it tends to be isolated examples of a good clinic with all of those services and the ability to do all that stuff.’
Respondents stressed the importance that primary health care is the appropriate setting for continuous care. And recognised that the relationship between a physician and patient has long been thought to have a positive effect on health care use and outcomes. They recognised that much of the research recognised that patients with higher continuity are more satisfied with their care, are more likely to take the correct medications and are more likely to have better health literacy and have problems identified early by their doctor as well as the decreased likelihood of ED presentation.
What is the extent of the problem?
Overall complexity of patients presenting to EDs has increased: The population is aging and this is associated with increased prevalence of chronic diseases, which often require ED care. In addition, medical technology and better pharmaceuticals enable people with chronic diseases to survive longer.
‘… the problem is that now, this emergency department everyday will be full of 95 year olds who’ve got diabetes, heart disease, lung disease, cancer, all that sort of stuff. Therefore the resources we invest in them to keep them well- and it’s not just an additive, it exponentially increases-we’re spending thousands times more than we ever used to in keeping people alive these days, and people wonder why we can’t afford to look after them.’
Impaired Access: The increasing demand and ambulance utilisation ‘... creates a range of tensions for us’.

Demand Management & Policy Options
48
‘…during period of peak hospital demand, when ambulances remained queued outside public hospital EDs, the ability of the ambulance to service their own demands within acceptable timeframes is severely compromised’
‘…we’re seeing extended or prolonged ramping periods… having patients waiting in the back of ambulances for three, four, five hours is not good from both a clinical perspective and a public perception.
Reduction in Quality of Care: Congestion is evidenced by the reduction in quality of care. Examples such as the delays to transfer a patient into an inpatient bed; delay in initial care; delay in offload of patients into ED from Ambulances; to use of hallways as treatment area. Increased demand on the ED can have adverse impact on the ability to deliver quality and timely care; particularly the adequacy and efficiency of patient assessments which may contribute to adverse patient outcomes.
‘…the patients maybe are suffering longer than they have to. Philosophically pain and suffering don’t necessarily cause harm.. they can cause emotional scarring which is not to be trivialized however the longer people wait with illness or injury the more likely it is that the illness and injury becomes associated with complications that could have been avoided if they were seen earlier.’
System Capacity -the EDs cannot do it alone: As with any system- when the balance between demand and capacity is correct: performance is optimum. However, when demand becomes too great, trade-offs between competing goals become necessary – it is at this point performance is diminished.
‘… look, I just think that we’re at that tipping point now where honestly, the way in which EDs have been built, the way in which they’ve been staffed and they resourced on top of actual staff, in the context that they’re as physically only as big as they can be, and the hospitals aren’t often using all of their built bed capacity because of issues with either funding or available bed spaces, or in fact being able to staff them if they are funded because of workforce issues, that really is sort of probably at the tipping point now, isn’t it … where things just keep getting busier.’
While proper capacity planning is vital, it is however, often poorly done and that it carries risks for both patients and staff and the system.
‘…the growth in demand continuously climbs , and climbs…. and climbs and so we are exhausting strategies and ideas and innovations around redesigning the way we do things to become more efficient and there’s going to become a time where our ability to continually remodel and redesign is going to run out of steam.’

Demand Management & Policy Options
49
Efficiency – poison chalice: Respondents identified that the impact of the introduction of the National Emergency access Target has had an unexpected effect on emergency crowding.
‘… The better we perform in our emergency departments the more demand we generate and the more demand we allow to flow in. We used to almost- I’ll use a medical word- tamponade- our growth in ED activity because we were so over choked and so overwhelmed, so access blocked and so hopelessly dysfunctional that we simply couldn’t get dramatic growth in activity because we simply couldn’t see it. That was a natural diversionary tactic that people stopped going to the emergency department because they didn’t think they’d get seen. But we’ve become better as we’ve created our own problems.’
What can be done about it?
The respondents recognized that there is no easy answer for ED congestion- there is no simple fix and that congestion will remain until the dangers of diminished inpatient capacity are fully recognized.
‘… we’re at that point now where the demand is such in the context of a relatively fixed bed stock within the hospitals that we’re just about at the point where in fact something going to have to give because we just can’t keep doing more, and more and more with the same, same, same all the time. There’s only so much efficiency you can actually extract out of the system.
Demand at the ED must be treated as a whole of system capacity issue – not just an ED problem.
‘…it needs system solutions that tackle all of them simultaneously. Something that focuses just on one or another in isolation, I think is a waste of time.’
It is essential that there is system –wide recognition that ED demand is just one pressure point along a variety of points along the health care continuum.
‘… I think the bulk of the improvements that we’ve seen in terms of waiting times, performance in the ED, we’ve kind of done it. There are other things, there’s no doubt. The big challenge for use now is how do we improve the flow through the whole system, not just through the emergency department.’
Several possible policy responses were suggested including hospital load -sharing, re-opening inpatient beds, augmenting emergency department resources and or productivity, delaying elective surgery and improving discharge processes,

Demand Management & Policy Options
50
instituting patient cost sharing and refusing emergency department services to patients with non-emergency conditions.
‘… we either build more beds, more hospitals or we start investing in some of that release capacity type initiatives: different model of care, different avoidance models. That’s where we need to be. Our current economic environment, fiscal environment for the state government isn’t one that we can go and build more…’
However these measures focus on the most immediate problems and specific policy solutions are needed to address all the causes of ED congestion.
‘… maybe we need to change the system to look at some of those things and do some more surgery on weekends. Maybe we need to be doing more day surgery during the winter months rather than overnight surgery, which doesn’t have that same demand for beds.’
Increased access to alternative primary care services was considered to offer continuity of care for both acute and chronic health care needs.
‘… I’m aware that there are all sorts of mechanisms and models of care in place and they’re piloting various initiatives to either see and treat people in the community, to pick people up and triage them to a more appropriate place, like a GP surgery’
Timely referral of patients to appointments at primary care facilities along with the enhancement of the capacity of the primary care system to accommodate additional patients may be of value. As one respondent said…
‘we need to find out how can we meet the needs and meet the demand using alternative models of care….I think we need to invest in models of care, not just activity.’

Demand Management & Policy Options
51
4. Discussion
Introduction
The modernisation and transformation of emergency health services over the last 40 years has had unquestioned impact on improving the quality and standards of clinical care for patients suffering acute illness and injury. However, these changes have been associated with the relative concentration of acute health care to the EHS from within the community and within the hospitals. This along with the relative reduction in inpatient capacity resulting in Access Block has led to increasing system wide congestion which has well documented clinical, organisational and social impact. Emergency health services congestion has been described as the most serious problem and most avoidable cause of harm facing our hospital system.4, 1-3 Reducing EHS congestion is important for patient’s safety and is under constant public and government scrutiny.198-202, 1-3, 203
However despite the well-known dimensions of the problem and increasing understanding of its elements, the public policy solutions have lacked a rigorous evidence base and have therefore had little or unsustainable impact. Interventions such as the co-location of GP clinics, Super GP clinics, telephone advisory services and public awareness program directed towards “appropriate” use have been shown at best to have minimal impact and in some studies have been associated with increased activity. Strategies have also been designed and implemented that aim to increase the rate of flow of patients through the ED including ‘fast tracking’ advanced triage and the establishment of short stay wards and medical assessment units.
Additionally changes to models of care and expanded scope of care including Nurse Practitioners and Emergency Care Practitioners have been trialled to reduce dependence of medical practitioners and thus increase flow. Another option to reduce demand and pressure on the EDs is to expand the role of nurses and/or introduce nurse practitioners and physician assistants within an ED. 47-55
Our research has focused on the demand for emergency healthcare. This is not to devalue the impact of Access Block or EHS processes but rather to recognise that demand has a ‘whole of community’ dimension to it and therefore requires a whole of system approach. We have previously detailed not only our findings but those of others in the way of comprehensive reviews of the literature and evidence. What we know is that the growth in demand occurs across most jurisdictions, all age groups and within the more urgent categories. We also know that patients in choosing to

Demand Management & Policy Options
52
seek emergency healthcare do so following a reasoned and largely rational exercise of choice based on available information and careful consideration of the relative value of available options. This is not to say there are not poor choices made or at times deliberate manipulative behaviour by some people. It is also not to say that some people’s behaviours or risk choices do not contribute to the presence of their health crisis. However the overwhelming majority of patients are genuinely ill and are seeking urgent medical advice and care. Our response as a healthcare system should be to understand the needs of those patients and to identify and make available options that meet those needs in an appropriate and timely manner.
In order to better respond to the perceived demand, the whole healthcare system must be considered. The inflow of patients determines the workload of the EHS which in-turn impacts on providing quality and timely care.4, 201 Congestion of inpatient units causes blocked access for emergency patients. Equally, difficulties in accessing community services including residential aged care may block inpatient beds with flow-on impacts to the EHS.
No single measure has been shown to independently reduce demand significantly. There is evidence that the availability of alternative service options (particularly high quality and accessible primary care) is associated with lower utilisation rates of specialist EHS. However there is clear evidence that the (so called) GP workload in the EHS is a relatively small proportion of caseload and an even smaller proportion of the workload. The proportion of current EHS patient load that could be managed in alternative venues depends on the nature and capability of these services and their accessibility in terms of timeliness and affordability.
Various jurisdictions have tried to identify alternative options including Urgent Care centres, Minor Injuries Clinics etc. To date, the most common approach in Australia has been to expand existing services. It may well be that the most efficient means of meeting this aspect of acute healthcare demand is served by expanding existing services rather than creating new services. In that case, the services are provided at ‘marginal cost’ from within an infrastructure that exists principally for other purposes rather than creating an entire new service infrastructure. However other social, professional and economic impacts may need to be considered and a genuine economic analysis is required of the alternative solutions.
What is likely to be most efficient (if interim) solution which may have an impact on demand while meeting patient needs, is a comprehensive suite of strategies based on coordinated access to the range of services available. Development of a comprehensive whole of community and evidence based approach would logically include strategies aimed at enhanced primary and secondary prevention, patient

Demand Management & Policy Options
53
management on site and diversion to alternative (but appropriate) services.
Primary and secondary prevention
Prevention of acute health care includes primary, secondary prevention and tertiary strategies.
Primary prevention seeks to prevent the onset of specific diseases by reducing risk of exposure, altering behaviours or enhancing resistance. There are extensive efforts underway aimed at enhanced primary prevention, ranging from health promotion (e.g. anti-smoking campaigns) through to early detection of risk factors and disease. The EHS has little direct responsibility for such programs apart from the involvement of clinicians in support of primary prevention programs by highlighting the consequences of the failure of prevention (“we see the results”) and through using the opportunity posed by a health crisis to highlight preventive strategies; the so called “teachable moment.”
Secondary prevention involves preventing the complications (including acute health crises) for those with established disease. This is generally the responsibility of primary and community based care and revolves around improved management of chronic disease. Again the EHS has little direct responsibility in this element except in a supportive role as part of the medical team. EHS can also ensure effective communication about health crises is passed back to those managing the disease long term and using the opportunity posed to encourage more attention to risk and complication management.
The patient-centred medical home is becoming a central theme of health reform efforts related to enhanced primary care.205-208 Patient centred medical home models and related innovations emerge as a key vehicle to improve the continuity and quality of health care and to control costs while improving provider and patient experience, processes of care, practice level measures of quality of preventative care utilisation as well as reduced emergency visits.209
Tertiary prevention describes processes that seek to provide alternative management for patients who experience an acute care crisis or to dissuade them from attending the EHS. These include public awareness campaigns, financial disincentives, enhanced primary care, telephone advisory services and improved end of life care.
Additionally there are other strategies that have been used to directly discourage patients from attending EHS. These include financial co-payments, public awareness programs, telephone advisory services and maximising access to alternative systems of care.

Demand Management & Policy Options
54
Financial disincentives are commonly used as a means of restraining demand in health services and even in systems with universal access. The evidence suggests that financial disincentives are not generally effective in acute healthcare because people see the need to access care or not in acute health crises is not a choice; therefore the price to be paid is not rated highly. This does not mean it is not a factor which may influence the location of care. Our research does show it is a factor in the choice between public and private hospital EDs.
However even if it is an influence, it is not one which is generally considered appropriate as it does not discriminate and so will deter people in need of care as much as it may deter those who could seek care elsewhere.
Many jurisdictions have used public awareness programs to encourage (or discourage) demand. The underpinning philosophy of these programs is aimed at improving health literacy and thus leading to ‘improved choices’ being made by patients. Governments in Australia have often reverted to these and they are often based on the assumption that much of ED demand is inappropriate and people should be told to “stop it.”
As indicated above, the evidence is contrary. Most demand is entirely appropriate when considered from the patient perspectives. Additionally such “appropriate use” campaigns are contradicted by other public awareness programs aimed at alerting patients to the risks, raising awareness of ‘early warning signs’ and encouraging early intervention. Improvement of ‘health literacy and awareness’ are more likely to raise awareness of risk and therefore lead to increased demand. This understanding is reinforced by the evidence which points to nil or perverse impact on demand arising from such programs.
These programs may heighten demand from a better informed public. Discerning patients may become increasingly aware and cautious, partly due to success of public health campaigns designed to increase awareness and partly due to better access to information such as the internet.
‘…try to educate the public about the use of emergency departments – that EDs are for emergencies. But recognized that …people don’t really know what an emergency is. If we’re sick, or injured, or hurting, then to us that’s an emergency and we want to go somewhere.’
Another unintended consequence of public awareness campaigns is that they may run the risk of deterring seriously ill patients from accessing or using the EHS appropriately.

Demand Management & Policy Options
55
Public awareness programs may be valuable if they help guide people to alternative services that may meet their needs. As part of a comprehensive approach, they may also help create a supportive social environment for other interventions that may have more direct impact.
Demand may be constrained if patients do have more access to appropriate primary care for acute health crises. In addition to improved chronic disease management, patients who are able to access primary care for minor illnesses and injuries are less likely to seek that care within the specialised EHS. There is no consistent evidence in the literature of the effects of improved primary care access on the demand for ED care.204-207 Primary care ‘gate keeping’ may reduce ED attendance but its safety is unknown.204-207 It is often argued that if GP services were open for longer, or were more generally accessible, this would alleviate the demand for ED services.71, 208-217 However, analysis of ED attendance rates, increasing social deprivation, increased patient age, smaller practice list and lower reported satisfaction with practice telephone access have been associated with higher use of the ED.7
Access to alternative safe and appropriate care is a critical component in managing demand for EHS. Ensuring a patient has access to a provider through open scheduling, extended hours and new options such as e-visits and communication via email can decrease utilization of EHS.178, 218-220 Having a regular primary health practitioner has long been thought to be an important component of maintaining a patient’s health and that access to regular care enhances the chance that the patient will turn to their doctor for medical need first versus going directly to the emergency department is more likely.212
However primary care needs not only to be accessible in a timely manner but also appropriate to need. Primary care needs to be able to handle acute health crises. They need appropriate training but also access to investigation facilities and procedural equipment. The ‘one stop shop’ remains important to patients who don’t want to have to travel to a variety of locations. Not all primary care is therefore suitable. Identifying those with capacity and capability and providing that information to patients may assist with their choices.
The use of co-located out-of-hours primary care centres with the ED is theoretically an opportunity to remove the responsibility of choice from the patient to the health care providers.221-226 However there is little evidence that such co-location reduces ED demand.221, 222, 224, 226 Indeed the experience suggests that they draw more patients for the community primary care services than they do from the EHS.
The provision of telephone advisory services to guide patients and people in need of

Demand Management & Policy Options
56
advice to choose or refer to appropriate healthcare service is sensible considering the extent of confusion and concerns the general public may experience at the time they need healthcare urgently around which service to access. 78, 80, 197, 227-230
While diversion of non-serious emergency calls to an advice line has the potential to reduce the number of ambulance responses and therefore affect the number of emergency department attendances,231-234 there is little evidence that such services actually reduce demand. Indeed much anecdotal commentary that they lead to increased demand.
Finally a small number of patients present for end of life care either from the community or from residential facilities. The reasons are complex ranging from failed policy to inexperienced staff. Using the EHS for predicted end of life care is not only ineffective and inefficient but more importantly inappropriate on ethical and humanitarian grounds. Therefore improved end of life care is important on a number of grounds but least of which is to help reduce EHS demand.
Treatment on site
The second option is to provide patients with their urgent medical advice and treatment on location; either at their home or in an alternate public space. These may be broadly described as “hospital avoidance programs”. A number of interventions have been trialled which aim to provide medical care on location without the need for EHS involvement.
Paramedic services may be able to treat and not transport more patients and thus avoid the need for transportation and ED attendance. While 20% of patients seen by paramedics are not transported (Monograph 2), this proportion may be able to be increased although the risk remains for all clinicians that judgement made in good faith may occasionally be incorrect. Increasing the capacity of paramedics to provide definitive care and not transport has the potential to reduce ED demand but at the same time increases the workload of ambulance services. This may simply shift the workload burden to a health service experiencing even greater increases in workload than the ED.
Mechanisms aimed at reducing the risk associated with ‘treat and not transport’ may include seeking advice and support from more experienced clinicians or those with higher levels of education and training. They may also be reduced by implementing arrangements which provide technological support and ongoing monitoring. Finally they may also rely on follow up with patients to ensure their condition has improved. Most ambulance service lack the capacity in the light of often overwhelming demands

Demand Management & Policy Options
57
for service to provide such follow up.
We have not been able to locate reliable high quality studies that have explored the effectiveness or cost effectiveness of such strategies. Anecdotal responses from paramedics suggest such efforts often take considerably longer and are more resource intensive than simply transporting the patient. However once the patient is transported then they often enter a continuum of care which is difficult to extract them from. Studies investigating the alternatives for emergency cases that are neither life threatening or serious concludes that the evidence that supports the alternative approaches should to be developed.135, 136
Previous QUT research found that the majority of ambulance calls did not warrant an emergency ambulance response.189, 192 However it is recognised that many people lack the knowledge or ability to assess the seriousness of the call and those communication difficulties may impede the ability to assess this. However it may be more appropriate to modify the response from the ambulance service in order to increase the appropriateness of care.
Instead of taking patients to hospital, an alternative is to ‘take the hospital to the home’; providing home- based treatment for acutely ill patients who would otherwise be in hospital.196-204 Other strategies that may assist with safely maintaining people in their home without the need for EHS involvement include formal Hospital In The Home programs which seek to provide advanced clinical care at home. These programs are difficult to access at the time of an acute health crisis and may well be a high cost alternative. However EHS may complement these programs; assisting with procedural support (e.g. replacing the drip) or by consulting with HITH coordinators and ensuring active follow up.
Similar schemes have been trialled with nursing homes which confront ongoing difficulties with maintenance of clinical advice. Hospital in the Nursing Home programs have been trialled to provide advanced clinical care to patients as an alternative to active involvement directly in the EHS.
Mobile GP services provide an alternative to EHS demand. Such services confront their own operational difficulties including securing an appropriately skilled workforce, security and integration with community and primary care services. However as part of a cohesive and integrated system they may well be able to avert some patents from the EHS.
Finally technology may be used to support home care. Technology may enable extended monitoring capability and access to centralized information (e.g. electronic health records or advanced care directives) to support decision making and patient

Demand Management & Policy Options
58
safety. It may also support telemedicine that may assist ongoing home care and communication technology generally may assist with follow up and patient support.
Diversion
Patients who enter the EHS may be diverted around components of the system in order to spread the burden, provide direct access to definitive sources of care or to access alternative sources of care.
EHS congestion may be reduced by ensuring a more even spread of the workload. This is often achieved by “queuing” but this has clinical and social consequences. It is often achieved at a local level by the ‘sharing of the load’ or controlling the destination of the patient.235-237
However there is considerable resistance to system wide management. Ambulance services object reasonably to resources being moved from their base area of operations which leads to degraded coverage for the community and prolonged travel times. Patients object to being taken away from the “usual” sources of care and away from family and social supports. There is also a clinical risk and inefficiencies to be derived from moving patients away from their ‘normal location of care’ which may be more familiar with their needs.
A special case involves the access to private hospital EDs. While 47% of Australians are privately insured, 6% attend private hospital EDs.238 Our research has demonstrated that patients exercise a judgement based on weighing up the perceptions of cost against the perceptions of waiting time however some patients are influenced by others or by lack of awareness of the calibre and scope of private EDs. However there are other influences including advice from paramedics and family that may also influence this inconsistency. Strategies which address the cost and waiting time perceptions may well result in greater use of private hospital EDs where appropriate and available.
The other alternative is direct access to definitive care. One of the principal reasons for the development of EDs within hospitals was the fact that patients referred into hospital with an acute health crisis were often lost in the system and not evaluated, resuscitated and acutely managed. EDs were seen as a ‘single front door’ through which all patients entered thus allowing for their (relatively) immediate evaluation, investigation and stabilization. This single entry also allowed for system wide management, ensuring patients were appropriately assigned and ongoing care ensured. The resultant instigation of the treatment process has the aim of reducing adverse clinical outcomes and to reduce hospital length of stay and thus improve

Demand Management & Policy Options
59
system efficiency.
However modern technology and the upgraded capability of paramedics’ means that it is now possible to directly access appropriate definitive care locations for some patients. Initiatives are underway to directly access Catheter Laboratories for patients with myocardial infarction, stroke centres, and spinal injuries units and so on; bypassing the ED.
There is also the potential for paramedics acting either under direct advice or on protocol to distribute patients to sources of appropriate care within the community ensuring definitive access for complex paediatric cases or maternity or palliative care.
Clearly patients undergoing institutional transfer should be able to directly access ongoing care at level where appropriate; e.g. ICU-ICU transfer. Such strategies do have an impact on ambulance services as they may often be associated with prolonged handover times, however these considerations need to be taken into account in resourcing decisions. Put simply, it may be cheaper and better for the system for the ambulance paramedics to take an extra 30 minutes taking the patient to definitive care than to incur those costs elsewhere through double handling and placing the patient at clinical risk of multiple handovers.
The final option is directing patients to alternate community based options. Such strategies may range from arranging access to appropriate existing services through to designing specific purpose alternate services. Improved coordination of access holds promise for moderating demand growth. Research has shown that patients are often unaware of alternative options or are unclear about their appropriateness. The NHS 111 is an experiment in directing patients to alternate services in a unitary system although evidence to date does not demonstrate significant improvement in demand for EHS arising from this strategy.
The alternate is purpose designed services that are intended to deal with lesser severity patients; variously titled but essentially urgent care centres. These centres hold promise for meeting the one stop shop and accessibility requirements of patients but well may not demonstrate economic advantage over treating those patients at marginal cost within existing EDs.
There is also an emerging interest in standalone “urgent care centres” both in the UK and in Australia. Although there is value intuitively in such a concept, to deal with these less acute health crises, there remains concerns with the risk of misallocation of severely ill people to a location which lacks the extensive professional support available in a hospital. There is also no clear evidence that such centres are cost-effective. The less acute patients are treated at marginal costs within current EDs and

Demand Management & Policy Options
60
the creation of a whole new centre means that the infrastructural costs must be fully recovered.
System coordination
While there is no evidence of any single or simple solution, there is the potential for significant improvements in the coordination of care provision at both policy and operational levels. Most of the solutions to ED congestion lie outside the ED. Many attempts to improve coordination of acute care through centralisation of ambulance coordination and the development of clinical coordination services for inter-hospital transfer and retrieval have resulted in more effective care of severely ill people. There is the potential for such principles to also be applied to the less urgent patients. Rather than determining why they may not be appropriate for certain services, perhaps we could refocus on finding the right service for the patient which meets their needs in terms of timeliness, scope and quality of care.
We believe there is value in improved coordination and integration of care which link the various providers, public and private, into a system which is coordinated around the patient needs. This more ‘patient centric’ approach is most likely to deliver the safest but also the most cost-effective care.
Also there is value to be gained form a system which monitors and evaluates system wide performance. The introduction of NEAT was an attempt to forge improved performance through the application of a process measure and target. The weakness of NEAT is that it is unidimensional. Process can always be traded off against quality or cost. What is needed is a balanced score card of measures at a system level which bring together clinical indicators of performance with process measures and cost measures. Applied to the system as a whole, this approach is more likely to generate reform which is sustainable.

Demand Management & Policy Options
61
5. Conclusion
The management of Emergency Health Services (EHS) has traditionally focused on supply rather than management of demand. Managing demand for EHS is a complicated and multi-faceted issue compounded by political, social, economic, scientific, ethical and ideological concerns.1 Emergency healthcare has been transformed over the past four decades in many countries throughout the world.
However, despite this rapid development, and associated investments in service standards, there is a high level of concern with the performance of emergency health services relating principally to system wide congestion.4, 239 The factors driving this problem are complex but relate largely to the combined impact of growing demand, expanded scope of care and blocked access to inpatient beds.1
The public health system has to balance its use of resources in such a way that optimum services are provided, maximum expectations are met and minimum sensitivities are provoked.1, 4, 239 In response to increasing demand, the concept of demand management in health care systems has attracted the attention of policy makers, researchers and other stakeholders. Previous QUT research has identified the growth in demand for emergency health services and analysed and evaluated the factors that appear to contribute to this growing demand.1-3, 10, 167, 240, 241 The consistent finding is that demand is growing, influenced by the wider health care system and that many solutions need to be system wide.1-4 However the literature does not paint a consistent picture as to the cause, consequence and remedial actions required.4
While ED congestion is an international issue, not all solutions are equally applicable in all countries.1, 4 Much of the current literature is based on either single descriptive case studies or expert opinion and therefore does not provide a robust basis for policy and practice.
On the basis of the literature and the commentary by the respondents, agencies across the continuum of urgent and unscheduled care need to prioritise working together to develop a coordinated whole of system approach including innovative models for out of hospital patient centred care.
There is no reliable evidence from the literature or from the collective experience of those involved in emergency care of any simple solutions that can be shown to reduce demand. Those interventions that have been trialled particularly nurse telephone advisory services and co-located primary care centres have not been shown to reduce ED demand; often the contrary. The only consistent observations from the research

Demand Management & Policy Options
62
are that access to primary care is associated with less dependence on the ED.
This study sought to collect and collate the evidence from the literature and to contribute new knowledge to that literature by identifying the factors that influence the growing demand for acute healthcare. This final Monograph has reported the final analysis of what is known form the literature about the strategies that have been trialled to reduce demand and added to that by the views not only of our research group but through interviews with leading figures involved in emergency care delivery.
There are significant limits to this research. The study is necessarily small and constrained to the particular environment of Australia and Queensland in particular. The number of participants in all aspects of this research was limited by the resources available. Those informing this research both those involved in its conduct and those consulted came from a single geographical location raising the risk that context and group thinking may have limited the range of themes identified. Their views are thus flavoured by the policy and operational environment. However the literature is international and the views expressed locally largely coincide with the themes identified from the literature.
Secondly the analysis of policy options is necessarily restricted to high order “first cut” analysis. Further more detailed analysis is required including the development of detailed business cases around individual or collective strategies. Additionally further research is required to develop, test and evaluate these strategies including economic evaluation.
Clearly no single strategy will resolve the challenge. Rather multiple strategies must be trialled and evaluated so that identification of the most effective may evidence policy direction. There is a need to develop a future strategy which is reflective of the evidence currently available and to design strategies that reflect the patient voice, which has been largely absent in previously public policy approaches.

Demand Management & Policy Options
63
References
1. Toloo S, FitzGerald G, Aitken P, Ting J, Tippett V, Chu K. Emergency Health Services: Demand and service delivery models. Monograph 1: Literature review and activity trends. Brisbane: Queensland University of Technology; 2011.
2. Toloo S, Rego J, FitzGerald G, Aitken P, Ting J, Quinn J, et al. Emergency Health Services: Demand and service delivery models. Monograph 2: Queensland EHS users' profile. Research Monograph. Brisbane: Queensland University of Technology, 2012 978-1-921897-52-8.
3. Toloo S, Rego J, FitzGerald G, Vallmuur K, Ting J. Emergency Health Services: Demand and service delivery models. Monograph 3: Patients' reasons and perceptions. Research Monograph. Brisbane: Queensland University of Technology, 2013 978-1-921897-93-1.
4. FitzGerald G, Toloo GS, Romeo M. Emergency healthcare of the future. EMA. 2014;26(3):291-4.
5. Clark MJ, Purdie J, FitzGerald GJ, Bischoff NG, O'Rourke PK. Predictors of demand for emergency prehospital care: An Australian study. Prehosp Disaster Med. 1999;14(3):167-73.
6. Snooks H, Evans A, Wells B, Peconi J, Thomas M. What are the highest priorities for research in emergency prehospital care? Emerg Med J. 2009;26:549-50.
7. Agarwal S, Banerjee J, Baker R, Conroy S, Hsu R, Rashid A, et al. Potentially avoidable emergency department attendance: Interview study of patients’ reasons for attendance. Emerg Med J. 2011.
8. Cooke MW, Fisher F, Dale J, McLeod E, Szczepura A, Waley P, et al. Reducing attendances and waits in emergency department: A systematic review of present innovations. Report to the National Coordinating Centre for NHS Service Delivery and Organisation. Warwick Medical School: University of Warwick; 2004.
9. Locker T, Mason S, Wardrope J, Walters S. Targets and moving goal posts: Changes in waiting times in a UK emergency department. Emerg Med J. 2005;22(10):710-4.
10. FitzGerald G, Toloo S, Rego J, Ting J, Aitken P, Tippett V. Demand for public hospital emergency department services in Australia: 2000-2001 to 2009-2010.EMA . 2012;24(1):72-8.
11. Department of Health. Attendances at A&E departments, England, 1987-88 to 2007-08 London: Department of Health, England; Multi-Year [updated 22/2/2011 - 15/4/2011]. Available from: http://www.dh.gov.uk/en/Publicationsandstatistics/Statistics/Performancedataandstatistics/AccidentandEmergency/DH_077485.
12. Richardson SK. Increasing patient numbers: The implications for New Zealand emergency departments. Emerg Nurse. 1999;7(3):158-63.

Demand Management & Policy Options
64
13. Bond K, Ospina MB, Blitz S, Afilalo M, Campbell SG, Bullard M, et al. Frequency, determinants and impact of overcrowding in emergency departments in Canada: A national survey.. 2007;10(4):32-40.
14. Ezaki T, Hashizume M. Emergency medicine in japan. A look at a current university hospital and the problems faced. EMA. 2007;19(4):296-9.
15. Hoot NR, Aronsky D. Systematic review of emergency department crowding: Causes, effects, and solutions. Ann Emerg Med. 2008;52(2):126-36.
16. Lowthian JA, Curtis AJ, Cameron PA, Stoelwinder JU, Cooke MW, McNeil JJ. Systematic review of trends in emergency department attendances: An Australian perspective. Emerg Med J. 2011;28(5):373-7.
17. Richardson DB, Mountain D. Myths versus facts in emergency department overcrowding and hospital access block. MJA. 2009;190(7):369-74.
18. McCarthy ML, Zeger SL, Ding R, Levin SR, Desmond JS, Lee J, et al. Crowding delays treatment and lengthens emergency department length of stay, even among high-acuity patients. Ann Emerg Med. 2009;54:492-503.
19. Schull MJ, Slaughter PM, Redelmeier DA. Urban emergency departments overcrowding: Defining the problem and eliminating misconceptions. CJEM. 2002;4(2):76-83.
20. Cowan RM, Trzeciak S. Clinical review: Emergency department overcrowding and the potential impact on the critically ill. Crit Care. 2005;9(3):291-5.
21. Hwang U, Concato J. Care in the emergency department: How crowded is overcrowded? Acad Emerg Med. 2004;11(10).
22. Morris ZS, Boyle A, Beniuk K, Robinson S. Emergency department crowding: Towards an agenda for evidence-based intervention. Emerg Med J. 2012;29(6):460-6.
23. Olsen JC, Cutcliffe B, O'Brien BC. Emergency department design and patient perceptions of privacy and confidentiality. Emerg Med.J 2008;35(3):317-20.
24. Pines J, Iyer S, Disbot M, Hollander J, Shofer F, Datner E. The effect of emergency departments crowding on patients satisfaction for admitted patients. Acad Emerg Med. 2008;15:825-31.
25. Kennedy D, Ardagh M. Frequent attenders at Christchurch hospital's emergency department: A 4-year study of attendance patterns. NZ Med J 2004;117(1193):U871.
26. Bernstein SL, Aronsky D, Duseja R, Epstein S, Handel D, Hwang U, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16(1):1-10.
27. Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. MJA. 2006;184(5 (Print)):213-6.
28. Fatovich DM, Hirsch RL. Entry overload, emergency department overcrowding, and ambulance bypass. Emerg Med J. 2003;20(5):406-9.

Demand Management & Policy Options
65
29. Walley P. Designing the accident and emergency system: Lessons from manufacturing. Emerg Med J. 2003;20(2):126-30.
30. Vilke GM, Brown L, Skogland P, Simmons C, Guss DA. Approach to decreasing emergency department ambulance diversion hours. Emerg Med J. 2004;26(2):189-92.
31. Gilligan P, Winder S, Singh I, Gupta V, Kelly PO, Hegarty D. The boarders in the emergency department (bed) study. Emerg Med J. 2008;25(5):265-9.
32. Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA, Jr. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173-80.
33. Cheung PT, Wiler JL, Lowe RA, Ginde AA. National study of barriers to timely primary care and emergency department utilization among medicaid beneficiaries. Ann Emerg Med. 2012;60(1):4-10 e2.
34. Jiang Y, Novais AP, Viner-Brown S, Fine M. Non-emergent hospital emergency department use and neighborhood poverty in rhode island, 2008–2012. Rhode Island Medical Journal 2014;July 2014:47-51.
35. Fergusson E, Li J, Taylor B. Grandmothers' role in preventing unnecessary accident and emergency attendances: Cohort study. BMJ. 1998;317(7174):1685.
36. Land L, Meredith N. An evaluation of the reasons why patients attend a hospital emergency department. Int Emerg Nurs. 2013;21(1):35-41.
37. Villani J, Mortensen K. Nonemergent emergency department use among patients with a usual source of care. J Am Board Fam Med. 2013;26(6):680-91.
38. McCusker J, Vadeboncoeur A, Levesque JF, Ciampi A, Belzile E. Increases in emergency department occupancy are associated with adverse 30-day outcomes. Acad Emerg Med. 2014;21(10):1092-100.
39. McHale P, Wood S, Hughes K, Bellis MA, Demnitz U, Wyke S. Who uses emergency departments inappropriately and when -A national cross-sectional study using a monitoring data system. BMC Med. 2013;11:258.
40. Baker R, Bankart MJ, Rashid A, Banerjee J, Conroy S, Habiba M, et al. Characteristics of general practices associated with emergency-department attendance rates: A cross-sectional study. BMJ Qual Saf. 2011;20(11):953-8.
41. Derlet RW, Richards JR. Overcrowding in the nation's emergency departments: Complex causes and disturbing effects. Ann. Emerg.Med. 2000;35(1):63-8.
42. Grumbach K, Keane D, Bindman A. Primary care and public emergency department overcrowding. Am J Public Health. 1993;83(3):372-8.
43. Green J, Dale J. Primary care in accident and emergency and general practice: A comparison. Soc Sci Med. 1992;35(8):987-95.
44. Brailsford SC, Lattimer VA, Tarnaras P, Turnbull JC. Emergency and on-demand health care: Modelling a large complex system. JORS. 2004;55(1):34-42.

Demand Management & Policy Options
66
45. Carret MLV, Fassa AG, Kawachi I. Demand for emergency health service: Factors associated with inappropriate use. BMC Health Serv. Res . 2007;7:131.
46. Penson R, Coleman P, Mason S, Nicholl J. Why do patients with minor or moderate conditions that could be managed in other settings attend the emergency department? Emerg Med J. 2012;29(6):487-91.
47. Salisbury C, Coulter A. Urgent care and the patient. Emerg Med J. 2010;27(3):181-2.
48. Schumacher JR, Hall AG, Davis TC, Arnold CL, Bennett RD, Wolf MS, et al. Potentially preventable use of emergency services: The role of low health literacy. Med Care. 2013;51(8):654-8.
49. Strickland MJ, Darrow L, Klein M, Flanders D, Sarnat J. Short-term associations between ambient air pollutants and pediatric asthma emergency department visits. Am J Respir Crit Care Med. 2010;182:307-16.
50. Elliot AJ, Hughes HE, Hughes TC, Locker TE, Brown R, Sarran C, et al. The impact of thunderstorm asthma on emergency department attendances across London during July 2013. Emerg Med J. 2014;31(8):675-8.
51. Xu Z, Huang C, Hu W, Turner LR, Su H, Tong S. Extreme temperatures and emergency department admissions for childhood asthma in Brisbane, Australia. J Occup Environ Med. 2013;70(10):730-5.
52. Toloo GS, Yu W, Aitken P, FitzGerald G, Tong S. The impact of heatwaves on emergency department visits in Brisbane, Australia: A time series study. Crit Care. 2014;18(2):R69.
53. Lowthian JA, Cameron PA, Stoelwinder JU, Curtis A, Currell A, Cooke MW, et al. Increasing utilisation of emergency ambulances. Aust Health Rev. 2011;35(1):63-9.
54. Lowthian JA, Jolley DJ, Curtis AJ, Currell A, Cameron PA, Stoelwinder JU, et al. The challenges of population ageing: Accelerating demand for emergency ambulance services by older patients, 1995-2015. MJA. 2011;194(11):574-8.
55. Johar M, Jones G, Savage E. The effect of lifestyle choices on emergency department use in Australia. Health Policy. 2013;110(2-3):280-90.
56. Gill JM, and A. W. Riley. Nonurgent use of hospital emergency departments: Urgency from the patient’s perspective. J Fam Prac 1996;42(5).
57. Koziol-Mclain J, D. W. Price, B. Weiss, A. A. Quinn, and B. Honigman. Seeking care for nonurgent medical conditions in the emergency department: Through the eyes of the patient. JEN 2000;26:554-63.
58. Limbourn S, Celenza A. Patient perceptions of caring and association with emergency department activity and access block. EMA. 2011;23(2):169-80.
59. Padela AI, Schneider SM, He H, Ali Z, Richardson TM. Patient choice of provider type in the emergency department: Perceptions and factors relating to accommodation of requests for care providers. Emerg Med J. 2010;27(6):465-9.

Demand Management & Policy Options
67
60. Siminski P, Cragg S, Middleton R, Masso M, Lago L, Green J, et al. Primary care patients views on why they present to the emergency departments: Innapropriate attendances or inappropriate policy. Aust J Prim Health 2005;11:87-95.
61. Dent AW, Phillips GA, Chenhall AJ, McGregor LR. The heaviest repeat users of an inner city emergency department are not general practice patients. Emerg Med J. 2003;15:322–9.
62. Kreisfeld R, Harrison JE. Hospital separations due to injury and poisoning 2005–06. Canberra: Australian Institute of Health and Welfare, Cat. no. INJCAT 131, 2010.
63. Billings J, Raven MC. Dispelling an urban legend: Frequent emergency department users have substantial burden of disease. Health Affairs. 2013;32(12):2099-108.
64. Derlet RW. Overcrowding in emergency departments: Increased demand and decreased capacity. Ann Emerg Med. 2002;39(4):430-2.
65. Barnett NP, Apodaca TR, Magill M, Colby SM, Gwaltney C, Rohsenow DJ, et al. Moderators and mediators of two brief interventions for alcohol in the emergency department. Addiction. 2010;105(3):452-65.
66. Vardy J, Mansbridge C, Ireland A. Are emergency department staffs' perceptions about the inappropriate use of ambulances, alcohol intoxication, verbal abuse and violence accurate? Emerg Med J. 2009;26(3):164-8.
67. Hossain MM, Laditka JN. The influence of rurality on the volume of non-urgent emergency department visits. Spatial and Spatio-temporal Epidemiology. 2011;2(4):311-9.
68. Setzler HH. Developing an accurate forecasting model for temporal and spatial ambulance demand via artificial neural networks: A comparative study of existing forecasting techniques vs. an artificial neural network [Ph.D.]: The University of North Carolina; 2007.
69. Airey C, Franks A. Major trauma workload within an English health region. Injury. 1995;26(1):25-31.
70. Arain M, Campbell MJ, Nicholl JP. Impact of a GP-led walk-in centre on NHS emergency departments. Emerg Med J. 2015;32(4):295-300.
71. Arain M, Nicholl J, Campbell M. Patients' experience and satisfaction with gp led walk-in centres in the UK; A cross sectional study. BMC Health Serv Res. 2013;13:142.
72. Block L, Ma S, Emerson M, Langley A, Torre Dde L, Noronha G. Does access to comprehensive outpatient care alter patterns of emergency department utilization among uninsured patients in East Baltimore? J Prim Care Community Health. 2013;4(2):143-7.
73. Hou XY, Zhao J, Chu K. Impact of a government triple zero awareness campaign on emergency department patient characteristics. EMA. 2012;24(4):393-400.

Demand Management & Policy Options
68
74. Mian O, Pong R. Does better access to fps decrease the likelihood of emergency department use? Results from the primary care access survey. Can Fam Physician. 2012;58(11):e658-66.
75. Raven MC, Kotchko SM, Gould DA. Can targeted messaging encourage PCP contact before ED visits? Am J Manag Care. 2013;19(1):41-5.
76. Rosenberg T. Acute hospital use, nursing home placement, and mortality in a frail community-dwelling cohort managed with primary integrated interdisciplinary elder care at home. J Am Geriatr Soc. 2012;60(7):1340-6.
77. Tung TK, Kaufmann JA, Tanner E. The effect of nurse practitioner practice in home care on emergency department visits for homebound older adult patients: An exploratory pilot study. Home Healthc Nurse. 2012;30(6):366-72.
78. Turner J, O'Cathain A, Knowles E, Nicholl J. Impact of the urgent care telephone service NHS 111 pilot sites: A controlled before and after study. BMJ Open. 2013;3(11):e003451.
79. Woods LW, Snow SW. The impact of telehealth monitoring on acute care hospitalization rates and emergency department visit rates for patients using home health skilled nursing care. Home Healthc Nurse. 2013;31(1):39-45.
80. Yang C, Chen CM. Effects of post-discharge telephone calls on the rate of emergency department visits in paediatric patients. J Paediatr Child Health. 2012;48(10):931-5.
81. Yip A, McLeod S, McRae A, Xie B. Influence of publicly available online wait time data on emergency department choice in patients with noncritical complaints. CJEM. 2012;14(4):233-42.
82. Yoffe SJ, Moore RW, Gibson JO, Dadfar NM, McKay RL, McClellan DA, et al. A reduction in emergency department use by children from a parent educational intervention. Family Medicine-Kansas City. 2011;43(2):106.
83. Rocovich C, Patel T. Emergency department visits: Why adults choose the emergency room over a primary care physician visit during regular office hours? World J Emerg Med. 2012;3(2):91-7.
84. Arendts G, Howard K, Rose JM. Allocation decisions and patient preferences in emergency medicine. Emerg Med J. 2011;28(12):1051-4.
85. Benahmed N, Laokri S, Zhang WH, Verhaeghe N, Trybou J, Cohen L, et al. Determinants of non-urgent use of the emergency department for pediatric patients in 12 hospitals in Belgium. Eur J Pediatr. 2012;171(12):1829-37.
86. Blau G, Hochner A, Portwood J. What variables affect public perceptions for ems meeting general community needs? J Allied Health. 2012;41(2):e39-43.
87. Browne AJ, Smye VL, Rodney P, Tang SY, Mussell B, O'Neil J. Access to primary care from the perspective of aboriginal patients at an urban emergency department. Qual Health Res. 2011;21(3):333-48.

Demand Management & Policy Options
69
88. Chambers C, Chiu S, Katic M, Kiss A, Redelmeier DA, Levinson W, et al. High utilizers of emergency health services in a population-based cohort of homeless adults. AM J Public Health. 2013;103(S2):S302-10.
89. Cheung PT, Wiler JL, Ginde AA. Changes in barriers to primary care and emergency department utilization. Arch Intern Med. 2011;171(15):1397-9.
90. Fieldston ES, Alpern ER, Nadel FM, Shea JA, Alessandrini EA. A qualitative assessment of reasons for nonurgent visits to the emergency department: Parent and health professional opinions. Pediatr Emerg Care. 2012;28(3):220-5.
91. Higginson I, Whyatt J, Silvester K. Demand and capacity planning in the emergency department: How to do it. Emerg Med J. 2011;28(2):128-35.
92. Morgans A, Burgess S. Judging a patient's decision to seek emergency healthcare: Clues for managing increasing patient demand. Aust Health Rev. 2012;36(1):110-4.
93. Rasch EK, Gulley SP, Chan L. Use of emergency departments among working age adults with disabilities: A problem of access and service needs. Health Serv Res. 2013;48(4):1334-58.
94. FitzGerald GJ, Toloo G. General practice patients in the emergency department. MJA 2013;198(11):573-4.
95. Agarwal S, Banerjee J, Baker R, Conroy S, Hsu R, Rashid A, et al. Potentially avoidable emergency department attendance: Interview study of patients' reasons for attendance. Emerg Med J. 2012;29(12):e3.
96. Lowthian J. Population changes do not explain rising demand for emergency care by the elderly. EMA. 2013;25:12.
97. Lowthian J, Curtis A, Stoelwinder J, McNeil J, Cameron P. Emergency demand and repeat attendances by older patients. Intern Med J. 2013;43(5):554-60.
98. Cooke M, Fisher J, Dale J, McLeod E, Szczepura A, Walley P, et al. Reducing attendances and waits in emergency departments: A systematic review of present innovations. 2004.
99. Bodenmann P, Velonaki VS, Ruggeri O, Hugli O, Burnand B, Wasserfallen JB, et al. Case management for frequent users of the emergency department: Study protocol of a randomised controlled trial. BMC Health Serv Res. 2014;14(1):264.
100. Brennan JJ, Chan TC, Hsia RY, Wilson MP, Castillo EM. Emergency department utilization among frequent users with psychiatric visits. Acad Emerg Med. 2014;21(9):1015-22.
101. Abbott J, Wright J, Madrid S. 'Frequent flyers' characteristics of emergency department patients with 6 or more visits in a single year. Ann Emerg Med. 2011;58(4):S297.
102. Adams JG. Emergency department overuse perceptions and solutions. JAMA. 2013;309(11):1173-4.

Demand Management & Policy Options
70
103. Althaus F, Paroz S, Hugli O, Ghali WA, Daeppen JB, Peytremann-Bridevaux I, et al. Effectiveness of interventions targeting frequent users of emergency departments: A systematic review. Ann Emerg Med. 2011;58(1):41-52 e42.
104. Castillo EM, Vilke GM, Killeen JP, Brennan JJ, Chan CT. Visit urgency between frequent emergency department users in a large metropolitan region network. Acad Emerg Med 2012;19:S96.
105. Crane S, Collins L, Hall J, Rochester D, Patch S. Reducing utilization by uninsured frequent users of the emergency department: Combining case management and drop-in group medical appointments. J Am Board Fam Med. 2012;25(2):184-91.
106. Hardie TL, Polek C, Wheeler E, McCamant K, Dixson M, Gailey R, et al. Characterising emergency department high-frequency users in a rural hospital. Emerg Med J. 2013.
107. Markham D, Graudins A. Characteristics of frequent emergency department presenters to an Australian emergency medicine network. BMC Emerg Med. 2011;11:21.
108. McCusker J, Tousignant P, Da Silva RB, Ciampi A, Lévesque J-F, Vadeboncoeur A, et al. Factors predicting patient use of the emergency department: A retrospective cohort study. Canadian Medical Association Journal. 2012;184(6):E307-E16.
109. Andren KG, Rosenqvist U. Heavy users of an emergency department: Psycho-social and medical characteristics, other health care contacts and the effect of a hospital social worker intervention. Soc Sci Med. 1985;21(7):761-70.
110. Ullman R, Block J, Stratmann W. An emergency room's patients: Their characteristics and utilization of hospital services. Med care. 1975;13(12):1011-20.
111. Alrajab S, Smith TR, Owens M, Areno JP, Caldito G. A home telemonitoring program reduced exacerbation and healthcare utilization rates in copd patients with frequent exacerbations. Telemed J E Health. 2012;18(10):772-6.
112. Brown EM, Goel V. Factors related to emergency department use: Results from the ontario health survey 1990. Ann Emerg Med. 1994;24(6):1083-91.
113. Byrne M, Murphy AW, Plunkett PK, McGee HM, Murray A, Bury G. Frequent attenders to an emergency department: A study of primary health care use, medical profile, and psychosocial characteristics. Ann Emerg Med. 2003;41(3):309-18.
114. Calderon-Larranaga A, Carney L, Soljak M, Bottle A, Partridge M, Bell D, et al. Association of population and primary healthcare factors with hospital admission rates for chronic obstructive pulmonary disease in England: National cross-sectional study. Thorax. 2011;66(3):191-6.
115. Castillo EM, Chan TC, Brennan JJ, Killeen JP, Vilke GM. Multiple hospital emergency department visits among 'frequent flyer' patients with a pain associated-discharge diagnosis. Acad Emerg Med. 2012;19:S321.

Demand Management & Policy Options
71
116. Chukmaitov AS, Tang A, Carretta HJ, Menachemi N, Brooks RG. Characteristics of all, occasional, and frequent emergency department visits due to ambulatory care-sensitive conditions in florida. J Ambul Care Manage. 2012;35(2):149-58.
117. Hansagi H, Olsson M, Sjoberg S, Tomson Y, Goransson S. Frequent use of the hospital emergency department is indicative of high use of other health care services. Ann Emerg Med. 2001;37(6):561-7.
118. Hockey DJ, Fluxman J, Watson M, Klaber R. Understanding the service use patterns of emergency department frequent attenders: Could paediatric outreach be a solution? Arch Dis Child. 2014;99(1):90-1.
119. Huang J-A, Tsai W-C, Chen Y-C, Hu W-H, Yang D-Y. Factors associated with frequent use of emergency services in a medical center. Journal-Formosan Medical Association. 2003;102(4):222-8.
120. Knowlton A, Weir BW, Hughes BS, Southerland RJH, Schultz CW, Sarpatwari R, et al. Patient demographic and health factors associated with frequent use of emergency medical services in a midsized city. Accad Emerg Med. 2013;20(11):1101-11.
121. Lang T, Davido A, Diakité B, Agay E, Viel JF, Flicoteaux B. Using the hospital emergency department as a regular source of care. European Journal of Epidemiology. 1997;13(2):223-8.
122. Phillips GA, Brophy DS, Weiland TJ, Chenhall AJ, Dent AW. The effect of multidisciplinary case management on selected outcomes for frequent attenders at an emergency department. MJA. 2006;184(12):602-6.
123. Salazar A, Bard??s I, Juan A, Olona N, Sabido M, Corbella X. High mortality rates from medical problems of frequent emergency department users at a university hospital tertiary care centre. European Journal of Emergency Medicine. 2005;12(1):2-5.
124. Scott J, Strickland AP, Warner K, Dawson P. Frequent callers to and users of emergency medical systems: A systematic review. Emerg Med J. 2013.
125. Wajnberg A, Hwang U, Torres L, Yang S. Characteristics of frequent geriatric users of an urban emergency department. J Emerg Med. 2012;43(2):376-81.
126. Skinner J, Carter L, Haxton C. Case management of patients who frequently present to a scottish emergency department. Emerg Med J. 2009;26(2):103-5.
127. Wetta-Hall R. Impact of a collaborative community case management program on a low-income uninsured population in Sedgwick county, Ks. Appl Nurs Res. 2007;20(4):188-94.
128. Jacoby LE, Jones SL. Factors associated with ed use by “repeater” and “Non Repeater” patients. J Emerg Nurs. 1982;8(5):243-7.
129. Ovens HJ, Chan BT. Heavy users of emergency services: A population-based review. CMAJ. 2001;165(8):1049-50.

Demand Management & Policy Options
72
130. Benjamin TBC, Ovens HJ. Frequent users of emergency departments. Do they also use family physicians' services? Canadian Family Physician. 2002;48(10):1654-60.
131. Blank FS, Li H, Henneman PL, Smithline HA, Santoro JS, Provost D, et al. A descriptive study of heavy emergency department users at an academic emergency department reveals heavy ed users have better access to care than average users. J Emerg Nurs. 2005;31(2):139-44.
132. Hunt KA, Weber EJ, Showstack JA, Colby DC, Callaham ML. Characteristics of frequent users of emergency departments. Ann Emerg Med. 2006;48(1):1-8.
133. Sandoval E, Smith S, Walter J, Schuman SA, Olson MP, Striefler R, et al. A comparison of frequent and infrequent visitors to an urban emergency department. J Emerg Med. 2010;38(2):115-21.
134. Malone RE. Heavy users of emergency services: Social construction of a policy problem. Soc Sci Med. 1995;40(4):469-77.
135. Sun BC, Burstin HR, Brennan TA. Predictors and outcomes of frequent emergency department users. Acad Emerg Med. 2003;10(4):320-8.
136. LaCalle E, Rabin E. Frequent users of emergency departments: The myths, the data, and the policy implications. Ann Emerg Med. 2010;56(1):42-8.
137. LaCalle EJ, Rabin EJ, Genes NG. High-frequency users of emergency department care. J Emerg Med. 2013;44(6):1167-73.
138. Malone RE. Whither the Almshouse? Overutilization and the role of the emergency department. J Health Polit Policy Law. 1998;23(5):795-832.
139. Schaulis MD, Snoey ER. Three years, a thousand visits: A case study of the ultimate frequent flyer. Ann Emerg Med. 2001;38(1):87-9.
140. Arroliga A, Griswold S. "Frequent fliers" do not receive a free trip in the emergency department. Chest. 2005;128(6):4051-2.
141. Malone RE. Almost ‘like family’: Emergency nurses and ‘frequent flyers’. Journal of Emergency Nursing. 1996;22(3):176-83.
142. Pope D, Fernandes CM, Bouthillette F, Etherington J. Frequent users of the emergency department: A program to improve care and reduce visits. CMAJ. 2000;162(7):1017-20.
143. Cook LJ, Knight S, Junkins EP, Jr., Mann NC, Dean JM, Olson LM. Repeat patients to the emergency department in a statewide database. Acad Emerg Med. 2004;11(3):256-63.
144. Dick T. Frequent flyer: Loneliness is an emergency, when it's yours. Emerg Med Serv. 2004;33(12):68.
145. Lucas RH, Sanford SM. An analysis of frequent users of emergency care at an urban university hospital. Ann Emerg Med. 1998;32(5):563-8.
146. Andrén KG, Rosenqvist U. Heavy users of an emergency department—a two year follow-up study. Soc Sci Med. 1987;25(7):825-31.

Demand Management & Policy Options
73
147. Brice M. Care plans for patients with frequent ed visits for such chief complaints as back pain, migraine, and abdominal pain. J Emerg Nurs. 2004;30(2):150-3.
148. Gunnarsdottir OS, Rafnsson V. Mortality of the users of a hospital emergency department. Emerg Med J. 2006;23(4):269-73.
149. Hansagi H, Allebeck P, Edhag O, Magnusson G. Frequency of emergency department attendances as a predictor of mortality: Nine-year follow-up of a population-based cohort. Journal of Public Health. 1990;12(1):39-44.
150. Okin RL, Boccellari A, Azocar F, Shumway M, O'Brien K, Gelb A, et al. The effects of clinical case management on hospital service use among ED frequent users. Am J Emerg Med. 2000;18(5):603-8.
151. Shumway M, Boccellari A, O'Brien K, Okin RL. Cost-effectiveness of clinical case management for ed frequent users: Results of a randomized trial. Am J Emerg Med. 2008;26(2):155-64.
152. Wassmer RW, Winward L, Derlet R. Does counselling reduce frequent emergency department use? Available at SSRN 1093870. 2008.
153. Tadros AS, Castillo EM, Chan TC, Jensen AM, Patel E, Watts K, et al. Effects of an emergency medical services-based resource access program on frequent users of health services. Prehosp Emerg Care. 2012;16(4):541-7.
154. Aminzadeh F, Dalziel WB. Older adults in the emergency department: A systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39(3):238-47.
155. Bristow D, C H. Emergency department case management: The dyad team of nurse case managemenr and social worker improve discharge planning and patient satisfaction. Professional Case Management. 2002;7(6):243-51.
156. O'Connell J, Gardner G, Coyer F. Profiling emergency nurse practitioner service: An interpretive study. Adv Emerg Nurs J. 2014;36(3):279-90.
157. Reddy KS. Global burden of disease study 2015 provides GPs for global health 2030. The Lancet. 2016;388(10053):1448-9.
158. World Health Organisation. The world health report 2002: Reducing risks, promoting healthy life. Geneva: WHO, 2002.
159. Durand AC, Gentile S, Devictor B, Palazzolo S, Vignally P, Gerbeaux P, et al. ED patients: How non-urgent are they? Systematic review of the emergency medicine literature. Am J Emerg Med. 2011;29(3):333-45.
160. Nagree Y, Camarda VJ, Fatovich DM, Cameron PA, Dey I, Gosbell AD, et al. Quantifying the proportion of general practice and low-acuity patients in the emergency department. MJA. 2013;198(11):612-5.

Demand Management & Policy Options
74
161. Harris MJ, Patel B, Bowen S. Primary care access and its relationship with emergency department utilisation: An observational, cross-sectional, ecological study. Br J Gen Pract. 2011;61(593):e787-93.
162. Haltiwanger KA, Pines JM, Williamson AL, Ross PA, Yost MM, Alladin KP, et al. The pediatric emergency department: A substitute for primary care? Ann Emerg Med. 2003;42(4):S53-S.
163. Afilalo M, Guttman A, Colacone A, Dankoff J, Tselios C, Beaudet M, et al. Emergency department use and misuse. Emerge Med. 1995;13(2):259-64.
164. FitzGerald GJ, Toloo GS, Aitken P, Keijzers G, Scuffham P. Public use and perceptions of emergency departments: A population survey. EMA. 2015;24(4): 336-42
165. Selby JV, Fireman BH, Swain BE. Effect of a co-payment on use of the emergency department in a health maintenance organization. N Engl J Med. 2010;334(10):635-41.
166. Fry MM. A systematic review of the impact of afterhours care models on emergency departments, ambulance and general practice services. AENJ 2011;14(4):217-25.
167. Rego J, FitzGerald G, Toloo S. Patients’ perceptions of emergency department services: Better specialised staff, convenient and available services. ACEM 30th Annual Scientific Meeting, 24-29 November 2013; Adelaide Convention Centre, Adelaide, Australia 2013.
168. Richardson DB. Primary care services and emergency medicine. MJA. 2010;192(8):429-30.
169. Rudge GM, Mohammed MA, Fillingham SC, Girling A, Sidhu K, Stevens AJ. The combined influence of distance and neighbourhood deprivation on emergency department attendance in a large English population: A retrospective database study. PLoS One. 2013;8(7):e67943.
170. Reid RJ, Coleman K, Johnson EA, Fishman PA, Hsu C, Soman MP, et al. The group health medical home at year two: Cost savings, higher patient satisfaction, and less burnout for providers. Health Affairs . 2010;29(5):835-43.
171. Solberg LI, Asche SE, Fontaine P, Flottemesch TJ, Anderson LH. Trends in quality during medical home transformation. Ann Fam Med. 2011;9(6):515-21.
172. Soman M, Larson EB. Patient-centered medical home demonstration: A prospective, quasi-experimental, before and after evaluation. Am J Manag Care. 2009;15(9):e71-e87.
173. Domino ME, Humble C, Lawrence WW, Jr., Wegner S. Enhancing the medical homes model for children with asthma. Med Care. 2009;47(11):1113-20.
174. Paul P, Heng BH, Seow E, Molina J, Tay SY. Predictors of frequent attenders of emergency department at an acute general hospital in Singapore. Emerg Med J. 2010;27(11):843-8.
175. Zuckerman B, Parker S, Kaplan-Sanoff M, Augustyn M, Barth MC. Healthy steps: A case study of innovation in pediatric practice. Pediatrics. 2004;114(3):820-6.

Demand Management & Policy Options
75
176. Paustian ML, Alexander JA, El Reda DK, Wise CG, Green LA, Fetters MD. Partial and incremental pcmh practice transformation: Implications for quality and costs. Health Serv Res. 2014;49(1):52-74.
177. David G, Gunnarsson C, Saynisch PA, Chawla R, Nigam S. Do patient-centered medical homes reduce emergency department visits? Health Serv Res. 2015;50(2):418-39.
178. Hearld LR, Alexander JA. Patient-centered care and emergency department utilization: A path analysis of the mediating effects of care coordination and delays in care. Med Care Res Rev. 2012;69(5):560-80.
179. Council of Ambulance Autorities. 2011-12 annual report. CAA, 2012.
180. Mason S, Snooks H. Alternative services to deliver urgent care in the community. Emerg Med J. 2010;27(3):183-5.
181. Snooks H. Nhs emergency response to 999 calls: Alternatives for cases that are neither life threatening nor serious. BMJ. 2002;325(7359):330-3.
182. Snooks HA, Kingston MR, Anthony RE, Russell IT. New models of emergency prehospital care that avoid unnecessary conveyance to emergency department: Translation of research evidence into practice? The Scientific World Journal. 2013:182102.
183. Australian Government. Healthdirect [9/9/2016]. Available from: http://www.healthdirect.gov.au/healthdirect.
184. Queensland Government. 13 health 2010 [9/9/2016]. Available from: https://www.health.qld.gov.au/13health/.
185. NHS. NHS 111 service 2015 [updated 23/4/2015 - 9/9/2016]. Available from: http://www.nhs.uk/NHSEngland/AboutNHSservices/Emergencyandurgentcareservices/Pages/NHS-111.aspx.
186. Xie B, Youash S. The effects of publishing emergency department wait time on patient utilization patterns in a community with two emergency department sites: A retrospective, quasi-experiment design. Int J Emerg Med. 2011;4(1):29.
187. Jouriles N, Simon EL, Griffin P, Williams CJ, Haller NA. Posted emergency department wait times are not always accurate. Acad Emerg Med. 2013;20(4):421-3.
188. Ahmed A, Fincham JE. Physician office vs retail clinic: Patient preferences in care seeking for minor illnesses. Ann Fam Med. 2010;8(2):117-23.
189. Wharam JF, Landon BE, Zhang F, Soumerai SB, Ross-Degnan D. High-deductible insurance: Two-year emergency department and hospital use. Am J Manag Care. 2011;17(10):e410-8.
190. Kindermann DR, Mutter RL, Cartright-Smith L, Rosenbaum S, Pines JM. Admit or transfer? The role of insurance in high-transfer-rate medical conditions in the emergency department. Ann Emerg Med. 2013.

Demand Management & Policy Options
76
191. Simonet D. Cost reduction strategies for emergency services: Insurance role, practice changes and patients accountability. Health Care Analysis. 2008.
192. DeVries A, Li CH, Oza M. Strategies to reduce non-urgent emergency department use: Experience of a northern Virginia employer group. Medical care. 2013;51(3):224-30.
193. He J, Toloo GS, Hou XY, FitzGerald G. Qualitative study of patients' choice between public and private hospital emergency departments. EMA. 2016.
194. FitzGerald G. Uncomfortable truth about emergency care. MJA Insight. 7 March 2016.
195. Rego J, FitzGerald G, Toloo S, Vallmuur K. Why do Queenslanders seek care in emergency departments? A population study. EMA. 2015;27(6):516-21.
196. Turner J, Coster J, Chambers D, Phung V-H, Knowles E, Bradbury D, et al. What evidence is there on the effectiveness of different models of delivering urgent care? A rapid review. 2015.
197. Blank L, Coster J, O'Cathain A, Knowles E, Tosh J, Turner J, et al. The appropriateness of, and compliance with, telephone triage decisions: A systematic review and narrative synthesis. J Adv Nurse. 2012;68(12):2610-21.
198. Cameron PA. Hospital overcrowding: A threat to patient safety? MJA. 2006;184(5):203-4.
199. Jarousse LA. ED throughput: A key to patient safety. H&HN: Hospitals & Health Networks. 2011;85(8):33-9.
200. Lowthian JA, Cameron PA. Emergency demand access block and patient safety: A call for national leadership. Emerg Med Australas. 2009;21(6):435-9.
201. Media A. Ed boarding creates patient safety issues, increases risk of mortality. Josp Case Manag. 2013;21(3):29-31.
202. Oredsson S. Triage and patient safety in emergency departments. BMJ (Online). 2012;344(7840).
203. Wei E, Sharp B, Santen S, Hopson L, Somand D, Bassin B. Interdisciplinary comparison of attitudes towards patient safety, communication, and teamwork in the emergency department. Ann Emerg Med. 2012;60(4):S51.
204. Cunningham P, Sammut J. Inadequate acute hospital beds and the limits of primary care and prevention. EMA. 2012;24(5):566-72.
205. Einarsdottir K, Preen DB, Emery JD, Holman CD. Regular primary care plays a significant role in secondary prevention of ischemic heart disease in a Western Australian cohort. J Gen Intern Med. 2011;26(10):1092-7.
206. Marrelli T. "Take aways" for moving toward prevention: Home care can play an important role! Home Healthc Nurse. 2010;28(8):453-5.

Demand Management & Policy Options
77
207. Patterson J, Scherger JE, Smith AM. Primary care and prevention. In: Suls JM, Davidson KW, Kaplan RM, editors. Handbook of health psychology and behavioral medicine. New York, NY US: Guilford Press; 2010. p. 340-53.
208. Boeke AJ, van Randwijck-Jacobze ME, de Lange-Klerk EM, Grol SM, Kramer MH, van der Horst HE. Effectiveness of GPs in accident and emergency departments. Br J Gen Pract. 2010;60(579):e378-84.
209. Egbunike JN, Shaw C, Porter A, Button LA, Kinnersley P, Hood K, et al. Streamline triage and manage user expectations: Lessons from a qualitative study of GP out-of-hours services. Br J Gen Pract. 2010;60(572):e83-97.
210. Huibers L, Thijssen W, Koetsenruijter J, Giesen P, Grol R, Wensing M. GP cooperative and emergency department: An exploration of patient flows. J Eval Clin Pract. 2013;19(2):243-9.
211. Iacobucci G. Longer GP opening hours would require pound2bn shift of funding into primary care, says GP leader. BMJ. 2013;347:f6131.
212. Jones D. How GPs can help reduce inappropriate attendance. Emerg Nurs. 2011;19(4):20-3.
213. O'Dowd A. Improving access to GPs will help reduce pressure on emergency departments, says NHS. BMJ. 2013;347:f7642.
214. O'Kelly FD, Teljeur C, Carter I, Plunkett PK. Impact of a GP cooperative on lower acuity emergency department attendances. Emerg Med J. 2010;27(10):770-3.
215. Sharma A, Inder B. Impact of co-located general practitioner (GP) clinics and patient choice on duration of wait in the emergency department. Emerg Med J. 2011;28(8):658-61.
216. Smits M, Huibers L, Oude Bos A, Giesen P. Patient satisfaction with out-of-hours GP cooperatives: A longitudinal study. Scand J Prim Health Care. 2012;30(4):206-13.
217. Voyce CE. GPs in accident and emergency. Forget quantity, think quality. BMJ. 2010;341:c4023.
218. Carrier E, Yee T, Holzwart RA. Care coordination between emergency and primary care physicians. United States: National Institute for Health Care Reform, February 2011.
219. Media. A. Study: Ed-based care coordination interventions need to fit unique needs ofED settings, providers. ED Manag. 2012;24(7):73-7.
220. Murphy SM, Neven D. Cost-effective: Emergency department care coordination with a regional hospital information system. Emerg Med J. 2014.
221. Altmeyer-Ennis S, Littler J. The effective management of out of hours treatment in primary care using telephone clinical assessment software (Tele Assess). Journal of the Royal Army Medical Corps. 2010;156(3):212-3.
222. Benger JR. Bring back local GPs for urgent and out of hours care. BMJ. 2013;346:f986.

Demand Management & Policy Options
78
223. Carlisle R, Groom LM, Avery AJ, Boot D, Earwicker S. Relation of out of hours activity by general practice and accident and emergency services with deprivation in Nottingham: Longitudinal survey. BMJ. 1998;316(7130):520-3.
224. O'Dowd A. Gps' out of hours arrangements are not to blame for pressure on emergency departments, MPs hear. BMJ. 2013;346:f3363.
225. Salisbury C, Trivella M, Bruster S. Demand for and supply of out of hours care from general practitioners in England and sSotland: Observational study based on routinely collected data. BMJ. 2000;320(7235):618-21.
226. Spence D. Out of hours care: A call for continuity. BMJ. 2012;344:e279.
227. Garro AC, Fearon D, Koinis-Mitchell D, McQuaid EL. Does pre-hospital telephone communication with a clinician result in more appropriate medication administration by parents during childhood asthma exacerbations? J Asthma. 2009;46(9):916-20.
228. Hallam L. Organisation of telephone services and patients' access to doctors by telephone in general practice. BMJ (Clinical Research Ed). 1991;302(6777):629-32.
229. Swage T, Longman H. Hanging on the telephone. Health Serv J. 2013;123(6364):24-5.
230. Temte JL. Telephone triage of patients with influenza. Am Fam Physician. 2009;79(11):943-5.
231. Tippett V, Toloo S, Eeles D, Ting J, Aitken P, FitzGerald G. Universal access to ambulance does not increase overall demand for ambulance services in Queensland, Australia. Aust Health Rev. 2013;37:121-6.
232. Toloo GS, FitzGerald GJ, Aitken PJ, Ting JY, McKenzie K, Rego J, et al. Ambulance use is associated with higher self-rated illness seriousness: User attitudes and perceptions. Academic Emergency Medicine. 2013;20:576–83.
233. Toloo S, Aitken P, FitzGerald G. Decision and reasons for calling an ambulance: Patients’ perspective [oral presentation]. 18th World Congress on Disaster and Emergency Medicine (WCDEM), 28-31 May 2013; Manchester, UK: Prehospital and Disaster Medicine; 2013. p. s65-6.
234. Toloo S, Tippett V, FitzGerald G, Chu K, Eeles D, Miller A, et al. How does ambulance service utilisation impact demand for emergency departments in queensland, australia? Australian Council of Ambulance Professionals (ACAP); 15-17/10/2009; Auckland, New Zealand: Journal of Emergency Primary Health Care; 2009. Article No.: 990354.
235. Intas G, Stergiannis P, Chalari E, Tsoumakas K, Fildissis G. The impact of ED boarding time, severity of illness, and discharge destination on outcomes of critically ill ED patients. Adv Emerg Nurs J. 2012;34(2):164-9.
236. Kyle E, Aitken P, Elcock M, Barneveld M. Use of telehealth for patients referred to a retrieval service: Timing, destination, mode of transport, escort level and patient care. J Telemed Telecare. 2012;18(3):147-50.

Demand Management & Policy Options
79
237. Vandeventer S, Studnek JR, Garrett JS, Ward SR, Staley K, Blackwell T. The association between ambulance hospital turnaround times and patient acuity, destination hospital, and time of day. Prehosp Emerg Care. 2011;15(3):366-70.
238. FitzGerald G, Toloo G, He J, Doig G, Rosengren D, Rothwell S, Sultana R, et al. Private hospital emergency departments in Australia: challenges and opportunities. EMA. 2013;25(3):233-40.
239. FitzGerald G, Aitken P, McKenzie KA, Kozan E, Tippett V, Toloo S, et al. Growing demand for emergency health services in Queensland, Australia [Abstract]. Prehosp Disaster Med. 2009;24(2):s52.
240. FitzGerald G, Toloo GS, Aitken P, Keijzers G, Scuffham P. Public use and perceptions of emergency departments: A population survey. EMA. 2015;27(4):336-42.
241. Wylie K, Crilly J, Toloo GS, FitzGerald G, Burke J, Williams G, et al. Review article: Emergency department models of care in the context of care quality and cost: A systematic review. EMA. 2015;27(2):95-101.

Demand Management & Policy Options
80
Appendix Abstracts and key findings of the major studies included in Literature Review
Theme Study Title Country Target Group
Study Design Findings Implication
Enhanced Primary Care
Arain (2014).70 Impact of a GP-led walk-in centre on NHS emergency departments. Emergency Medicine Journal.
UK Frequent Users
Before and after evaluation consisting of a cross sectional survey, ED routine data analysis and qualitative interviews.
This study found that 18% of patients using GP led urgent care centre reported tha they would have used ED if the urgent care centre was not open The GP led urgent care centre produced small changes to attendances at local EDs during daytime working hours (64 patients over 3 weeks), fewer would have been estimated from the patients reported intentions. Evidence of opening of the GP WIC in Sheffield has resulted in a reduction of 8% in adult ED GP type daytime attendances. There was also a 14% reduction in attendances at the children's ED, but because of bigger variability in the counts of monthly attendances, this reduction was not statistically significant. Only small 4% reduction in attendances at the MIU was found. The researcher data suggest that self-reported intentions in survey questionnaires are unreliable and can greatly exaggerate the impact on EDs.
Walk in centers work to increase health care accessibility and a large majority of patients are satisfied with the service. Most follow the advice they are given and their problems are resolved, though many subsequently use other NGS services to their impact on the local health economy remains questionable.
Enhanced Primary Care
Arain (2013).71 Patients' experience and satisfaction with GP led walk-in centres in the UK; a cross sectional study. BMC Health Services Research
UK General Population
A survey was conducted in two GP led walk-in centres in the North of England over three weeks during September and October 2011. A self-reported, validated questionnaire was used to survey patients presenting at these centres. A short post visit questionnaire was also sent to those who agreed. Ethical approval for the study was obtained from an NHS ethical review committee.
Found that a high proportion of the patients attending the two centres were very satisfied with the overall services Longer time to be seen at one centre particularly during evenings and weekends, was of concern: this also affected patients' satisfaction with the service. Most patients had very high compliance with the treatment advice given at the centre and a large proportion of patients reported that their problem was fully resolved after visiting the centre It was also observed that a high proportion of patients visit their GPs soon after visiting the walk in centre which suggest there is a risk of potentially duplicating the existing services.
Walk in centres work to increase health care accessibility and a large majority of patients are satisfied with the service Most follow the advice they are given and their problems are resolved, though many subsequently use other NGS services to their impact on the local health economy remains questionable
Enhanced Primary Care
Block (2013).72 Does access to comprehensive outpatient care alter patterns of emergency department utilization among uninsured patients in East Baltimore? Journal of Primary Care & Community Health.
USA
Outpatients Retrospective cohort study to determine whether access to comprehensive outpatient primary and speciality care coordination reduced ED utilisation among patients.
Patients who accessed comprehensive outpatient primary and speciality care had fewer ED visits with none leading to admission The evaluation found that although rates of ED utilisation did not change, patients accessing outpatient primary and specialty care had somewhat decreased rate of ED visits resulting inpatient admissions relative to comparison group of patients who did not receive the intervention.
As ED utilisation is seen as driving the rising cost of health care, improving access to outpatient services may promote continuity of care while decreasing reliance and demand on the ED.
Diversion Hou (2012).73 Impact of a government triple zero awareness campaign on emergency department patient characteristics. Emergency Medicine Australasia.
Australia General Population
Before and after to determine whether the characteristics of patient attending an ED at a teaching hospital in Brisbane changed significantly following the QAS Triple Zero Community Awareness Campaign
ED visits in a tertiary-referral teaching hospital indicates ambulance use, clinical urgency and illness severity were positively associated with each other. However, the Triple Zero Awareness Campaign had different impacts on the three outcome measures. The arrival mode of the ED patients was not significantly influenced by the campaign. The clinical urgency of the ED patients decreased, whereas the illness severity of the ED patients increased after the campaign.
Further investigation including incorporation of attitude change of individual patients in ambulance use as an outcome may help fully explore the impact of the campaign. Findings from this study might facilitate future policy developments in providing emergency health services in Queensland, Australia.
Enhanced Primary Care
Mian (2012).74 Does better access to FPs decrease the likelihood of emergency department use? Results from the Primary Care Access Survey. Canadian Family Physician Medecin De Famille Canadien.
Canada Non urgent care users
Population based telephone survey to determine an association with better access to FP decreased likelihood of ED visits.
A decreased likelihood of ED use is associated with having a regular FP among those with chronic diseases and with having access to FPs for immediate care among the general population.
The findings of this study will shed light on the complex relationships between access to FPs and use of ED use and help establish stretches to enhance primary care access to reduce unnecessary ED visits.

Demand Management & Policy Options
81
Theme Study Title Country Target Group Study Design Findings Implication
Enhanced Primary Care
Raven (2013).75 Can targeted messaging encourage PCP contact before ED visits? American J of Managed Care
USA Frequent Users
Interview and Phone Survey Overall wait times and PCP availability were the main barriers patients cited that indeed their acceptance of the PCP as a first choice for medical attention. Participants chose to see their PCC for preventative care and maintenance issues. In general participants reported specific reasons including prolonged or acute systems that, while potentially manageable in an ambulatory setting let them to choose ED instead. Participants reported resistance to use services such as walk in clinics instead of EDs because many remain unfamiliar with them.
Targeted messaging holds the potential to increase utilization of PCP resources prior to and ED visit. Promising messages should be tested further to determine their impact on real-world behaviours in order to optimise their use for both patients and capitated plans.
Enhanced Primary Care
Rosenberg (2012).76 Acute hospital use, nursing home placement, and mortality in a frail community-dwelling cohort managed with Primary Integrated Interdisciplinary Elder Care at Home. J of the American Geriatrics Society
Canada Aged Observational Before and After to evaluate the effect of integrated care of older people at home on acute hospital use and mortality in the frail –aged population.
Research found that primary care provided by a physician; nurse and physiotherapist in participants home may reduce acute hospital admissions and facilitate home deaths. This research demonstrated that this model of care may also reduce some of the costs in the acute hospital care system and that for active patients there can be a significant reduction in acute hospital admissions and hospital days as well as smaller reduction in ED use.
By going to individuals homes it improves access to care for people who may have difficulty in getting to a physician’s office. An integrated team combines different skills to provide a large spectrum of services than provided in routine medical care The model may be attractive for older people and their caregivers, providers and the health care system.
Enhanced Primary Care
Tung (2012).77 The effect of nurse practitioner practice in home care on emergency department visits for homebound older adult patients: an exploratory pilot study. Home Healthc Nurse
Canada Aged Prospective descriptive design used to gather data from charts and electronic record of adults aged 65 + or homebound patients who receive at least one NP home visit (n=30) after they were recruited, consented and entered the study from one home care program in a town in Canada
More ED visits were documented in the control group than in the intervention group at 2 and 4 weeks, but not at 8 weeks. Six subjects dropped out in the intervention group and 1 in the control group during the study due to death. The number of ED visits was reduced at 2 and 4 weeks in the intervention group, but there was no significant difference in the death rates between the 2 groups.
The study provides support for further studies of NPs in home care in Canada.
Prevention Turner (2013).78 Impact of the urgent care telephone service NHS 111 pilot sites: a controlled before and after study. BMJ Open
UK Frequent Users
Controlled before and after study using routine data to measure the impact of the urgent care NHS 111 on the emergency and urgent care system
There was no change overall in emergency ambulance calls, ED attendances or urgent care use. Calls to NHS direct reduced by and emergency ambulance incidents increased. Overall emergency and urgent care system activity increased in each site and remained when assuming that NHS 111 would eventually take all NHS direct and GP out of hours calls.
This service was established to focus of directing people to the right place rather than reassurance and self-care advice. With the abolishment of the NHS direct service (which predominantly provided reassurance and self-care advice) the call volumes may increase substantially, the characteristics of the population accessing and utilizing the service may impact on the management of immediate access to clinical advice. The invention of this new service may be creating a supplier induced demand and therefore increasing overall demand for emergency and urgent care. As the NHS11 service increases its profile demand for service could change either by generating new demand or by people using it as an alternative to in-hours primary care (or combination of both).
Prevention Woods (2013).79 The impact of telehealth monitoring on acute care hospitalization rates and emergency department visit rates for patients using home health skilled nursing care. Home Healthc Nurse
USA Home Care patients
Retrospective review of medical records comparing acute care hospitalisation and ED visits
Although the literature generally supports tele monitoring there were significant variances were noted in the number of participants and the diagnosis of patients.
Tele monitoring may be of use to others wishing to engage in targeted strategies to improve the quality of care for patients and reduce healthcare costs associated with acute hospitalisations and emergent care.
Prevention Yang (2012).80 Effects of post-discharge telephone calls on the rate of emergency department visits in paediatric patients. Journal Paediatrics and Child Health.
Australia Paediatric outpatients
Prospective study evaluating the effect of post discharge phone calls by NPs on the rate of ED visits within 3 days following hospitalisations.
Researchers found post discharge telephone calls by NPs reduced the rate of ED visits within 3 days following hospitalisation in paediatric patients. Telephone follow-up in an effective way of providing health information, managing remaining symptoms, advising patients of medical alternatives and giving reassurance
Telephone follow-up is an effective way of providing health information, managing remaining symptoms, recognizing complications, admission patients of medical alternatives and giving reassurance an may reduce unnecessary patient ED Visits.

Demand Management & Policy Options
82
Theme Study Title Country Target Group Study Design Findings Implication
Community awareness
Yip (2012).81 Influence of publicly available online wait time data on emergency department choice in patients with noncritical complaints. CJEM
Canada Noncritical ED patients
Prospective study investigating patients’ awareness of online available ED wait time data and their stated willingness to use this information when choosing an ED
There was low awareness of the availability of wait time data published online in the study location. This was not surprising as there was no advertising or start up campaign to educate the public. Results indicate with efforts such as promotion and advertising, simply publishing ED wait times online results in very low public awareness. Nearly 1/2 of the participants indicated a willingness to use online wait time data when selecting an ED which suggests that increasing public awareness may be beneficial to the uptake and utility of such information. Younger patients were more likely to indicate a willingness to use we based ED wait time information.
The implementation of an awareness campaign and re-evaluation of ED use and patient satisfaction following this. Web based dissemination of wait time information may now reach the largest group of ED users (the aged). Supplementation with different media may increase public awareness of the use of wait time information by those who are most likely to see emergency health care. The publication of ED wait time data along with the publication for alternative health care providers such as walk in clinics, or urgent care centres targeted at patients with conditions suitable for such providers may divert a proportion of patients with conditions that could be managed elsewhere. However too many patients responding to published wait information and selecting ED with shorter wait time may actually lead to over crowing or lengthen wait times for that site. Published wait times may influence patient expectations and if the expectation is not met, may negatively influence patient satisfaction.
Home care Yoffe (2011).82 A reduction in emergency department use by children from a parent educational intervention. Family Medicine-Kansas City
USA Paediatric “realistic evaluation" (aka before and after). Parents of all children aged 10 and under were provided with an information booklet which contained information about providing non-emergency care for their children at home and make better decisions about when emergency services may be needed for their children. Parents were then surveyed to determine whether they through the information provided was clear and understandable and whether they through the information would help them care for their child at home and make better decisions about when their children needed to be seen in the ED.
Long-term changes were observed only among the intervention group. There was a substantial and statistically significant reduction in ED use for non-urgent care of children. There was also a proportional reduction in ED charges for this group.
Study suggests that educational intervention allows parents to more effectively utilise the level of care appropriate for their child’s medical needs. An educational intervention among parents can substantially reduce non-urgent ED visits for their children