Embed Size (px)
Citation preview

BURN INJURIES
Margaret Tandoh,MD
Assistant Professor of Surgery
University of Vermont
OBJECTIVES
• TYPES OF BURNS
• HOW DEEP IS IT
• HOW MUCH IS BURNED
• HOW DO YOU CARE FOR THE BURN
SCOPE OF THE PROBLEM
• Burn injuries receiving medical treatment: ~450,000
• Hospitalizations: 45,000 (10%)-- ~25,000 at burn centers
• Fire/Burn deaths/year: 3,500– 3,000 residential, 500 other(MVC, aircraft, etc)
• 75% of deaths at scene or initial transport
SCOPE OF THE PROBLEM
• GENDER: 70% males, 30% females
• ETHNICITY: 60% Caucasian, 19% African-American, 15% Hispanic, 6% Other
CAUSES:
– Flame 44% – Scald 33% – Contact 9% – Electrical 4% – Chemical 3% – Other 7%
SCOPE OF THE PROBLEM
• In severe burns:
– 37% flame
– 24% scalds
– Structural fires: 50% of death due to CO, not burns
ANATOMY
• Largest organ
• Protective barrier
• Regulates temperature
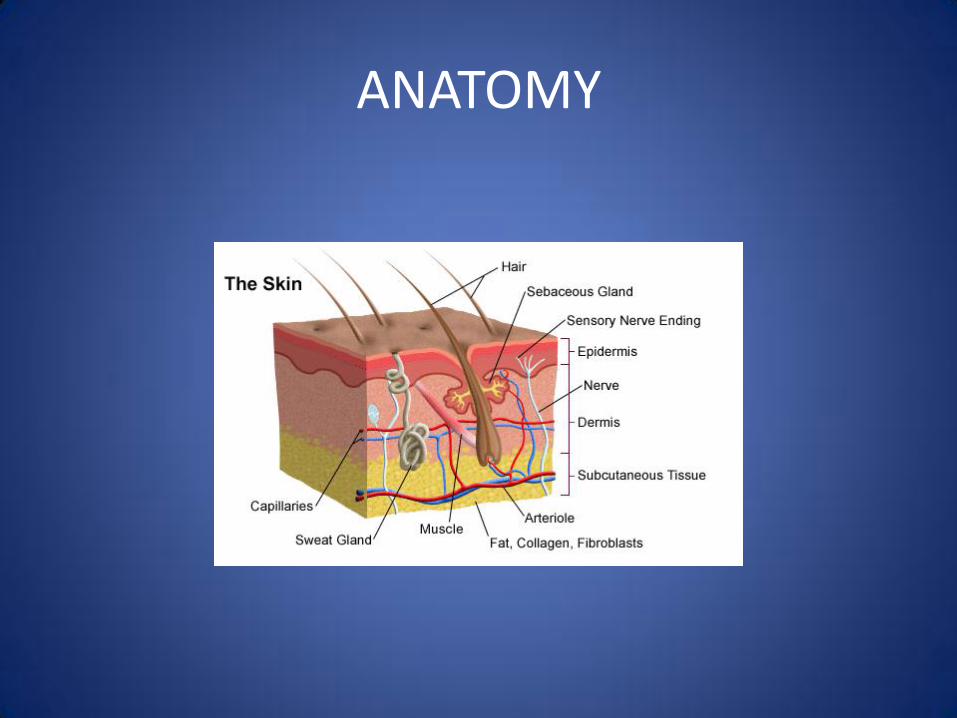
ANATOMY
TYPES/CLASSES OF BURNS
– THERMAL
• FLAME
• SCALD
• FLASH
• CONTACT
TYPES/CLASSES OF BURNS
– NON-THERMAL
• CHEMICAL
• ELECTRICAL
• RADIATION
• COLD
PAHOPHYSIOLOGY OF THE BURN WOUND
• Burn injury-coagulation necrosis-increased capillary permeability-fluid moves from intravascular space toward burn
• Ebb phase
– Initial decrease in CO, metabolic rate
• Flow phase(after resuscitation)
– Increase CO, resting energy expenditure
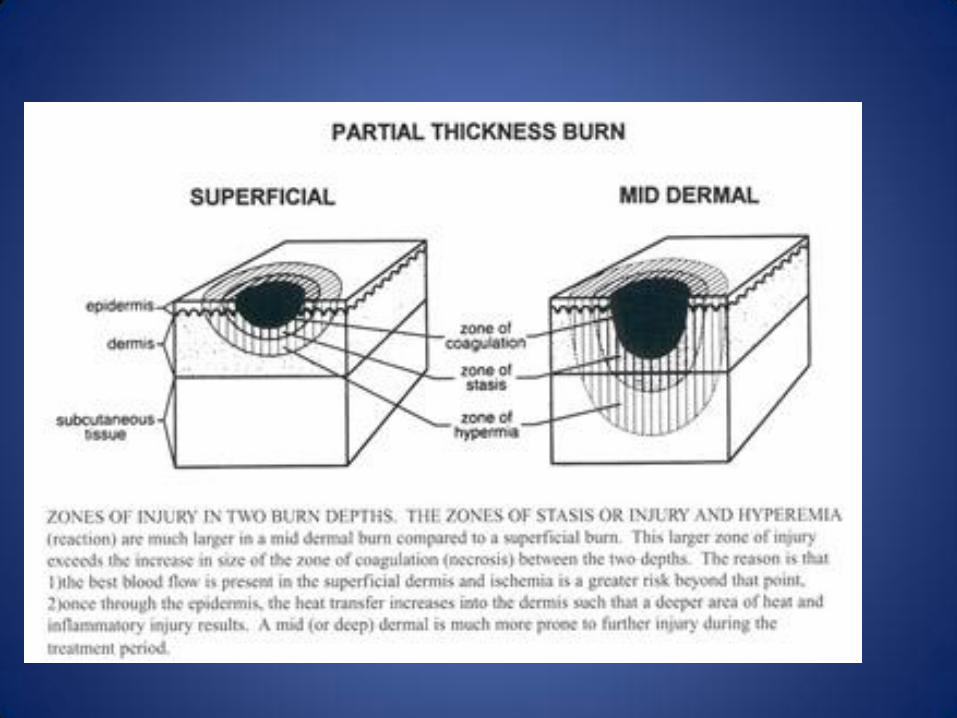
PATHOPHYSIOLOGY cont’d
• 3 zones of tissue injury:
– Coagulation: dead or dying cells, most intimate contact with heat source
– Stasis: vasoconstriction and ischemia, may convert to coagulation
– Hyperemia: vasodilation, viable cells
SCALDS
• Most common cause of burns
• Water at 140F causes full-thickness burns in 3secs, at 156F in 1sec.
• Cup of coffee, 180F
• Grease clings to skin
• Thicker soups and sauces remain in contact longer
FLAME
• Most common in severe burns
• 67% in Caucasian population
• 66% involve a flammable liquid
• 63%, gasoline is liquid of choice
• 26% association with EtOH
CONTACT
• Can be 4th degree
• Unconscious patients resting on hot surface
• Toddlers falling on to wood stoves
• Industrial accidents: contact and crush
ELECTRICAL INJURIES
~ 20, 000 ED visits/yr
~ 500-1000 deaths/yr
> 50% of deaths occur at workplace
• 2-3% of burns in children
ELECTRICAL BURNS
• 3-5% of all admitted burns
• Visible burned areas represent only a small portion of destroyed tissue
• Electrical currentheat tissue with lowest resistance(nerves, vessels muscles)
• Low-voltage: similar to thermal burns, only local damage, 110-220 V
• High-voltage:1000 V or more, CPR, full trauma evaluation, EKG monitoring
• Multiple complications: cataracts(up to 30%), neurologic
CHEMICAL BURNS
• Most are from household cleaners
• Industrial exposures
• Injury caused by protein destruction
• Speed is essential in management
• Copious lavage with water
• Alkalis: lime, KOH, bleach, cement(calcium oxide), NaOHusually deep
• Acids:protein breakdown by hydrolysishard escharnot as deep as alkalis
ASSESSMENT OF THE BURN WOUND
• Outcome dependent on depth and extent of injury
• Extent of injury
– Rule of nines
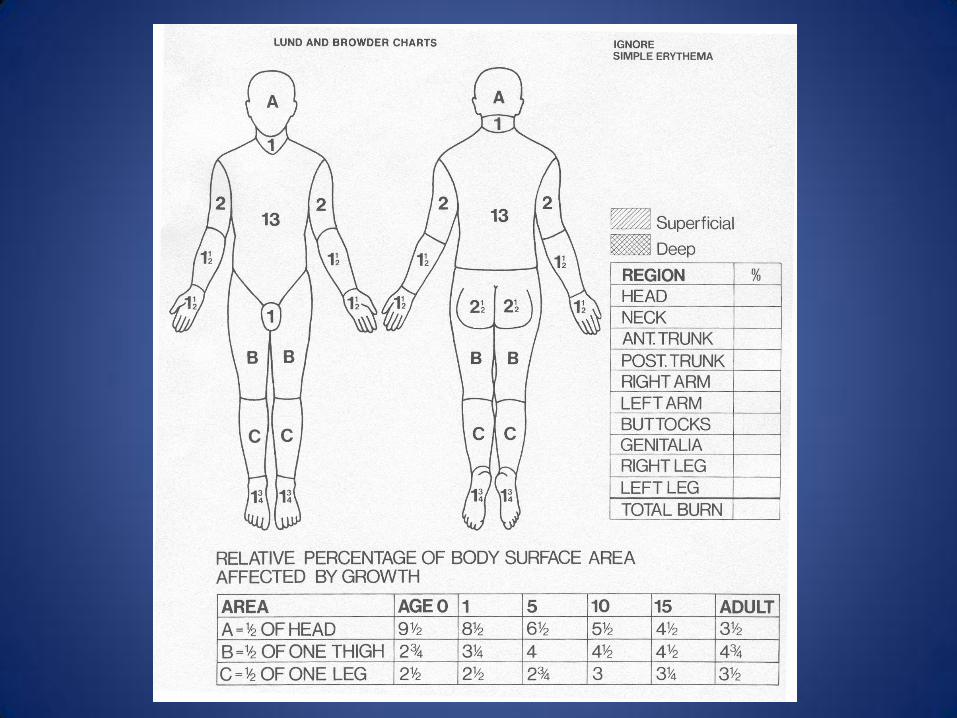
– Lund Browder chart
– Palm size(of patient) including digits
DEPTH OF BURN
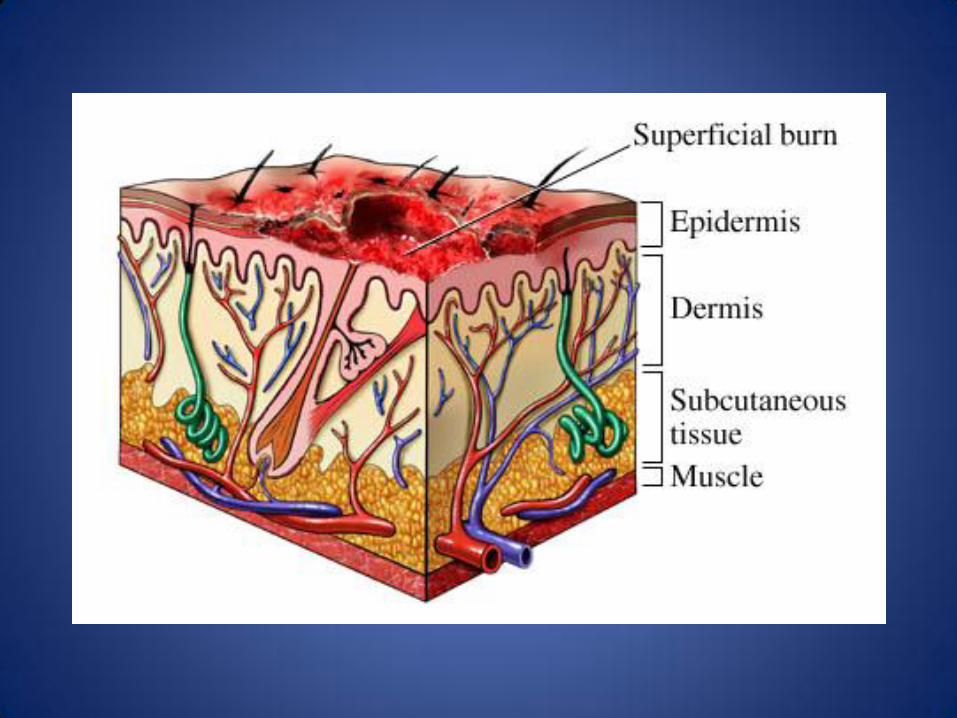
• 1st degree
– Epidermis only, painful, dry, heals in ~ 7days, no scars
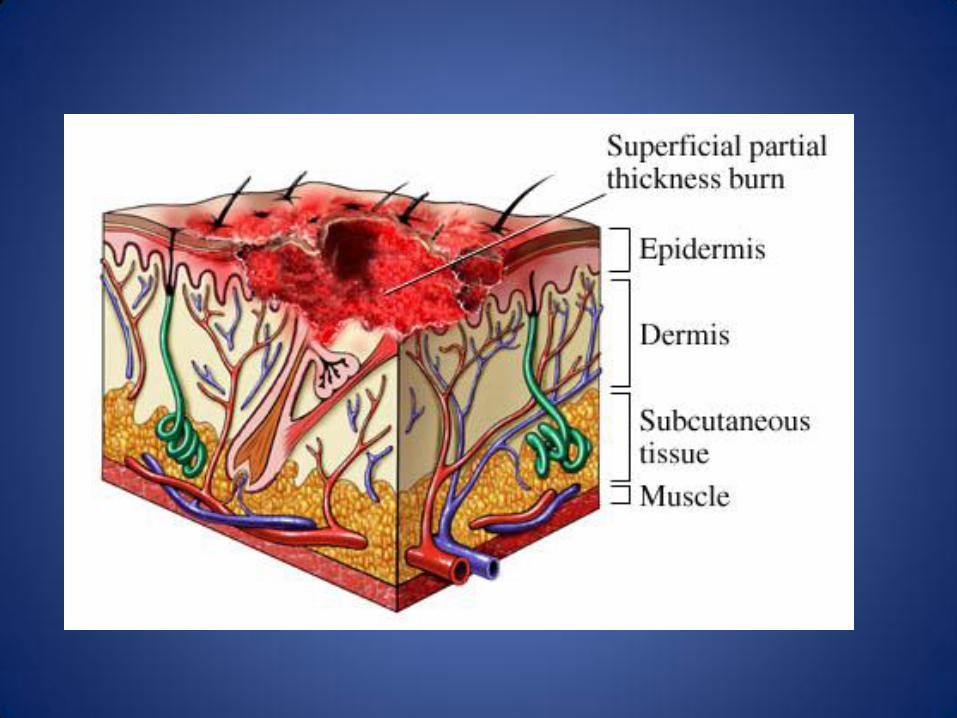
• 2nd degree
– Superficial: various portions of superficial dermis, painful, moist(dermal vessels present), blisters, minimal scarring, heals in ~ 14 days
DEPTH OF BURN
• 2nd degree – Deep: usually insensate, no blisters, treat like 3rd
degree
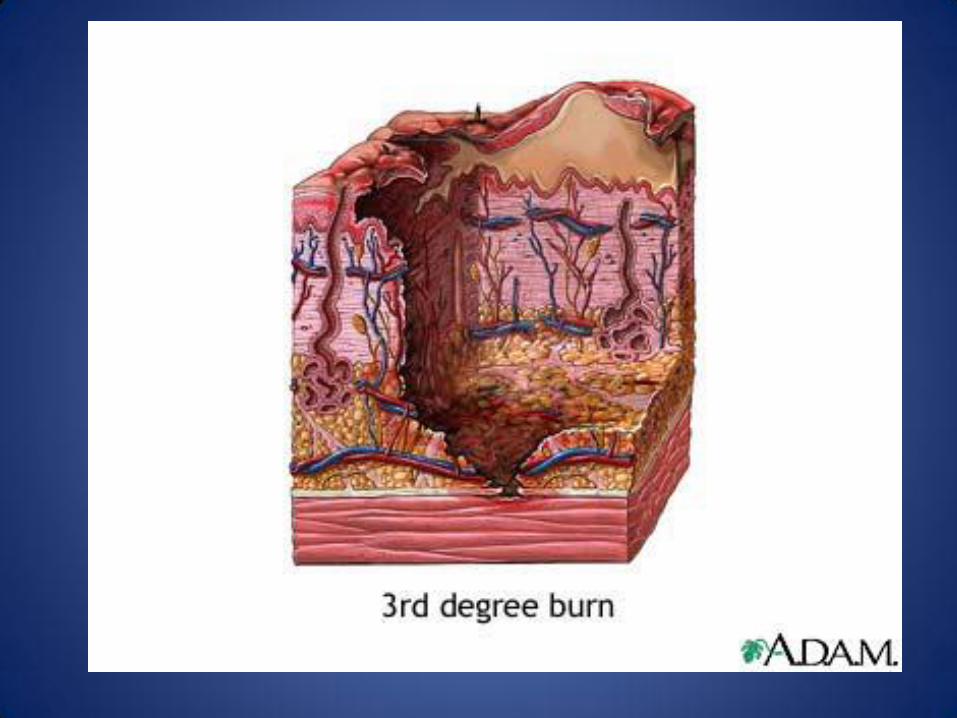
• 3rd degree – Full-thickness necrosis, painless, dry, can be any
color, will scar, needs excision
• 4th degree – Underlying structures(muscle, bone) involved
FOURTH DEGREE
• Extends into muscle, bone, etc
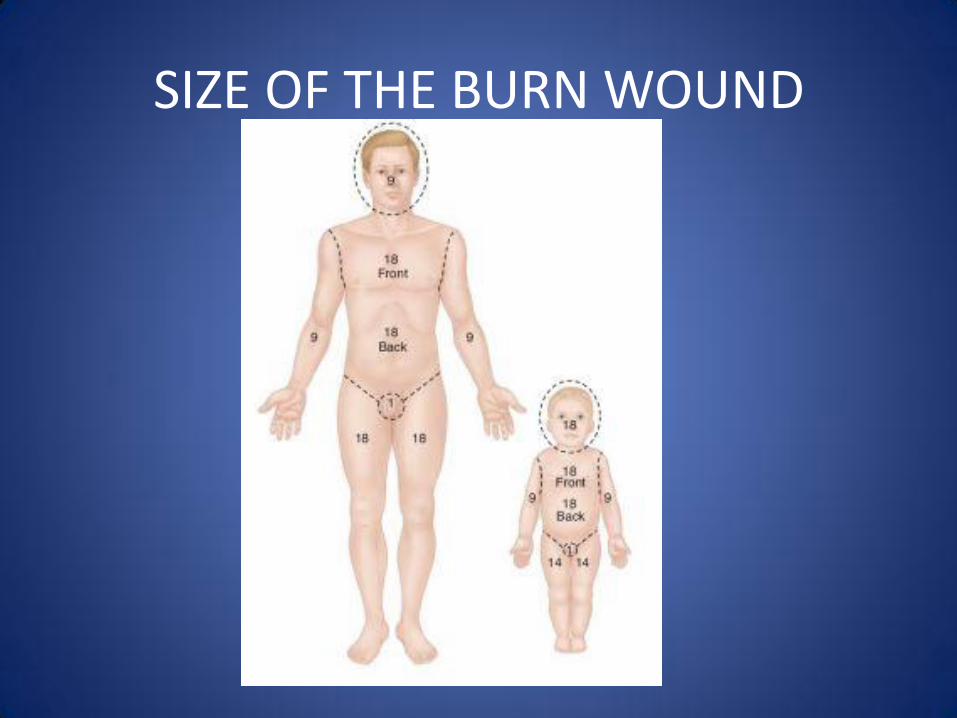
SIZE OF THE BURN WOUND

INITIAL MANAGEMENT
• Airway
• Breathing
• Circulation
• Disability
• Exposure/environment
INITIAL MANAGEMENT
• Cover with clean dry sheet
• Irrigate copiously chemical burns)
• No antibiotics
• No ice
• Leave blisters
• Tetanus prophylaxis
INITIAL TREATMENT
• Stop burning process
• Primary and secondary survey
• Resuscitation: Parkland(4ml/kg/% TBSA) and Brooke(1.5ml/kg/%TBSA + 0.5/kg/%TBSA)
• Escharotomies: edema impedes venous outflow and then arterial inflow. Look for numbness and tingling in limbs, increased pain in digits
• Tetanus
WOUND CARE
• Early excision and grafting deep 2nd and 3rd degree wounds
• Full-thickness skin grafts:decreased contracture, but limited and can only be used once. Not commonly used in burn wounds.
• Split-thickness skin grafts: commonly used
FROSTBITE
• 1805: first modern report published
• 1814: Dominique Larrey(Surgeon General of Napoleon’s forces) described frostbite in the forces during the campaign in1812-1813
• His treatment held for over 150 years!
• Friction massage with snow or ice, rather than thawing rapidly
PATHOPHYSIOLOGY
• Direct cellular damage and death
– Caused by extracellular ice crystals
– Rapid coolingintracellular ice crystals, more severe cell damage
Progressive tissue ischemia
Wet/moist skin more susceptible
Alcohol use very common
CLASSIFICATION
• Based on acute physical findings and imaging after rewarming:
• Frostnip: no ice crystals, no tissue loss, not frostbite, but may precede it
• 1st degree: numbness, erythema, mild edema
• 2nd degree: clear or milky blister, erythema, edema
• 3rd degree: hemorrhagic blisters
• 4th degree: extends into muscle or bone
SIGNS AND SYMPTOMS
• 90% is acral
• Ears, nose, cheek, penis also involved
• Numbness prior to rewarming, then severe pain, usually throbbing
• Tingling can occur
• Initial appearance can be deceptive
TREATMENT
• Rapid rewarming
• Temperature should be 40-42C for 15 – 30 mins or until complete
• Tetanus
• Drain clear blisters, leave bloody blisters
• NSAIDS
REMINDERS/PRACTICALS
• Smoke alarms save lives
• Set water temperature to 125F
• Avoid ice to burns
• Dry socks in the winter
• Take oxygen off when smoking
• Smother oil fire, no water

REFERENCES
• Some pictures from Google Images
• Total Burn Care, 3rd edition
• McIntosh, S et al. Wilderness Medical Society Practice Guidelines for the Prevention and Treatment of Frostbite, Wilderness & Environmental Medicine. 22, 156-166(2011)
• ABA Fact Sheet 2011




























