Embed Size (px)
Citation preview

Am. J. Trop. Med. Hyg., 101(1), 2019, pp. 164–179doi:10.4269/ajtmh.18-0534Copyright © 2019 by The American Society of Tropical Medicine and Hygiene
Bridging Efficacy of a Tetravalent Dengue Vaccine from Children/Adolescents to Adultsin Highly Endemic Countries Based on Neutralizing Antibody Response
Peter B. Gilbert,1,2*† Ying Huang,1,2†Michal Juraska,1 Zoe Moodie,1 Youyi Fong,1,2 Alexander Luedtke,1 Yingying Zhuang,2
Jason Shao,1 Lindsay N. Carpp,1 Nicholas Jackson,3 Laurent Chambonneau,4 Alain Bouckenooghe,5 Betzana Zambrano,6
Carina Frago,5 Sophie Pallardy,4 and Fernando Noriega71Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center, Seattle, Washington; 2Department of Biostatistics,
University of Washington, Seattle, Washington; 3Research and Non Clinical Safety, Sanofi Pasteur, Marcy-L’Etoile, France;4Clinical Programs, Sanofi Pasteur, Marcy-L’Etoile, France; 5Clinical Sciences, Sanofi Pasteur, Singapore; 6Clinical Sciences,
Sanofi Pasteur, Montevideo, Uruguay; 7Clinical Sciences, Sanofi Pasteur, Swiftwater, Pennsylvania
Abstract. The CYD-TDV vaccine is licensed in multiple endemic countries based on vaccine efficacy (VE) againstsymptomatic, virologically confirmed dengue demonstrated in two phase 3 trials (CYD14, 2- to 14-year-olds, Asia;CYD15, 9- to 16-year-olds, Latin America). 50%plaque reduction neutralization test (PRNT50) titers at baseline andmonth13 (post-vaccination) were associated with VE and may enable bridging VE to adults. Two phase 2 trials of CYD-TDVmeasured baseline and month 13 PRNT50 titers: CYD22 (9- to 45-year-olds, Vietnam) and CYD47 (18- to 45-year-olds,India). 50% plaque reduction neutralization test distributions were compared between age cohorts, and four versions ofan epidemiological bridging method were used to estimate VE against any serotype (dengue virus [DENV]-Any) andagainst each serotype over 25 months post first vaccination in a hypothetical CYD14 + CYD15 18- to 45-year-old cohort(bridging population 1) and in the actual CYD47 18- to 45-year-old cohort (bridging population 2). Baseline andmonth 13geometricmeanPRNT50 titers to eachserotypewere significantly greater in 18- to45-year-olds than9- to16-year-olds forall comparisons. The four methods estimated VE against DENV-Any at 75.3–86.0% (95% CIs spanning 52.5–100%) forbridging population 1 and 68.4–77.5% (95% CIs spanning 42.3–88.5%) for bridging population 2. The vaccine efficacyagainst serotype 1, 2, 3, and 4 was estimated at 56.9–76.9%, 68.3–85.8%, 91.4–95.0%, and 93.2–100% (bridgingpopulation 1) and 44.5–66.9%, 53.2–69.2%, 79.8–92.0%, and 90.6–95.0% (bridging population 2), respectively; thus,CYD-TDVwould likely confer improved efficacy in adults than 9- to 16-year-olds. Using the samemethods, we predictedVE against hospitalized DENV-Any over 72 months of follow-up, with estimates 59.1–73.5% (95% CIs spanning40.9–92.2%) for bridging population 1 and 50.9–65.9% (95% CIs spanning 38.1–82.1%) for bridging population 2.
INTRODUCTION
The four serotypes of dengue virus (DENV-1, DENV-2,DENV-3, and DENV-4) are transmitted by Aedes mosquitoesand have been estimated to cause nearly 400 million infec-tions (100 million symptomatic) annually.1–3 The spectrum ofdengue disease ranges from mild febrile illness to denguehemorrhagic fever (DHF) and potentially fatal dengue shocksyndrome (DSS). Dengue occurs in more than 100 countriesworldwide, predominantly in tropical and subtropical regions,and up to 4 billion people worldwide are at the risk of in-fection.4 Epidemiological studies have shown that the sero-prevalence of dengue neutralizing antibodies elicited bynatural infection increases with age in endemic regions, in-dicating the ongoing and repeated exposure to DENV in theseregions.5–8 There is clearly a need for wide geographic de-ployment of an effective dengue vaccine in endemic regions,including one indicated for adults.9–13
The only dengue vaccine licensed to date is the recombi-nant live attenuated tetravalent CYD-TDV vaccine (Deng-vaxia®), developed and manufactured by Sanofi Pasteur(Marcy-l’Etoile, France).14 Estimated vaccine efficacy (VE)was56.5% (95% CI: 43.8–66.4%) and 60.8% (52.0–68.0%) toprevent symptomatic virologically confirmed dengue (VCD) ofany serotype in the active phase of two phase 3 trials (CYD14in 2- to 14-year-olds in Asia andCYD15 in 9- to 16-year-olds inLatin America, respectively).15,16 Vaccine efficacy also varied
by serotype, with the lowest VE observed against DENV-2 inboth trials.17 In 9- to 16-year-olds pooled across the two trials(active phase), overall VE was 65.6% and the serotype-specific VEs were 58.4% (DENV-1), 47.0% (DENV-2), 73.6%(DENV-3), and 83.2% (DENV-4). Exploratory analyses inboth trials indicated that VE increased with age and VE washigher in individuals who were dengue seropositive at thebaseline.15,16,18 Vaccination of individuals aged at least 9years is currently approved in several dengue-endemic re-gions, including in more than a dozen countries, with mostcountries up to 45 years and a fewwith other age caps (age 16for Indonesia and age 60 for Paraguay).We previously analyzed data from CYD14 and CYD15 to
determine how VE varied with dengue neutralizing antibodytiters measured by the 50% plaque reduction neutralizationtest (PRNT50), both at the baseline (pre-vaccination) andat 1 month after the final vaccination (month 13).18 We foundthat, in 9- to 16-year-olds pooled across the two trials, bothbaseline and month 13 PRNT50 titers were significantly as-sociated with CYD-TDV VE to prevent VCD of any serotype,with month 13 PRNT50 titers being stronger predictors of VEthan baseline titers. Serotype-specific analyses revealed that,in 9- to 16-year-olds pooled across the two trials, estimatedVE against VCD of a given serotype increased significantlywith homologous titer for DENV-1, DENV-2, and DENV-4.Consistent with previous reports,5–8 we found that baselineseroresponse rates and baseline PRNT50 titers increased withage.18
Given that CYD-TDV had lower VE against VCD through25 months in baseline dengue seronegative individuals, andinitial exploratory analyses suggested that VE against hospi-talization for VCD and against severe VCD over longer term
*Address correspondence to Peter B. Gilbert, Vaccine and InfectiousDisease Division, Fred Hutchinson Cancer Research Center, 1100Fairview Ave. North, Seattle,WA98109. E-mail: [email protected]†These authors contributed equally to this work.
164

follow-up could be negative in this subgroup,19 Sridhar et al.20
conducted additional analyses of VE by baseline serostatus,considering the three endpoints of VCD through 25 months,hospitalized VCD through 72 months, and severe VCDthrough 72 months. Sridhar et al. found that VE against hos-pitalized and severe VCDwaspositive in baseline seropositiveindividuals uniformly over 72 months of follow-up (about 70%risk reduction) and was negative in baseline seronegative in-dividuals, with increased risk by vaccination (about doubledrisk) evident starting at about 2–3 years post first vaccination.As the risk of severe dengue (DHF/DSS) is known to be
higher during secondary infection than during primaryinfection,21–23 it has been hypothesized that CYD-TDV vac-cination of a dengue seronegative individual acts as a primaryinfection, placing she or he at an increased risk of severedengue after natural infection post-vaccination.24 Morover,anti-dengue antibody titers at the time of exposure appear tobe important factors in influencing the risk of severe denguewith a relationship that is not monotonic.25 For example, Saljeand others26 dynamic transmission model supported asso-ciations of antibody titerswith an instantaneous risk of dengueinfection, VCD, hospitalized VCD, and DHF, where dengueseronegative individuals had lower risk than individuals withlow-level titers (until around log2 titer 3). These findings arealso consistent with the hypothesis described previously andfurther discussed by others.27
In April of 2018, the WHO published updated recommen-dations of the Strategic Advisory Group of Experts on Immu-nization (SAGE) on the use of CYD-TDV: “For countriesconsidering vaccination as part of their dengue control pro-gram, a ‘pre-vaccination screening strategy’ would be thepreferred option, in which only dengue-seropositive personsare vaccinated.”28 Although the updated SAGE recommen-dations imply that individual pre-vaccination screening basedon a reliable and rapid test to determine previous dengueexposure would be ideal, no such test has been widely reg-istered for this indication, such that vaccination policies areforged without such a test. In highly endemic settings wheremost vaccinated individuals are seropositive, extrapolationof the vaccine versus placebo risk difference estimates ofSridhar et al.20 suggests that the use of CYD-TDV withoutscreening confers large overall reductions in hospitalized andsevere VCD,20 although at the cost of causing some cases forseronegative individuals.Given that CYD14 andCYD15 focused on a population with
high VCD attack rates, but did not include adults, an importantconsideration is to now develop an evidence-based approachto support the decisions of regulatory agencies aboutwhetherthe indication for the CYD-TDV vaccine may be extended toadults. In general, where a treatment has been licensed in apopulation studied in a phase 3 trial and it is deemed unethicalto conduct a new randomized placebo-controlled phase 3 trialof the treatment in a new population of interest not repre-sented in the phase 3 trial cohort, a surrogate endpoint cansometimes be used for the provisional approval of the treat-ment for the new population. For example, the U.S. Food andDrug Administration’s Accelerated Approval process may beusedwhen all four of the following criteria apply: 1) a treatmentin a population would fill an unmet medical need; 2) there ex-ists a surrogate end point that has not yet been validated buthasbeendemonstrated to be “reasonably likely” to predict thereal clinical benefit; 3) the treatment is shown to have a
beneficial effect on the surrogate endpoint in the new pop-ulation; and 4) a commitment is made to directly study thetreatment’s effect on the true clinical endpoint in the newpopulation in a phase 4 post-approval study (Food and DrugAdministration Safety Innovations Act of 2012). The CYD-TDVvaccine with VCD, hospitalized VCD, and/or severe VCD as theclinical endpoint and thePRNT50 titer as the surrogate endpointcould fit this scenario, given that its use in adults may beexpected to significantly reduce morbidity and mortality inadults. Specifically, for the endpoint VCD over 25 months,month 13 PRNT50 titers were a strong effect modifier of VE inthe CYD14 and CYD15 trials, overall and in baseline seropos-itive and baseline seronegative subgroups,18 with high PRNT50titers associatedwith high VE in all age and baseline serostatussubgroups. In addition, two phase 2 trials of CYD-TDV havebeen conducted to evaluate the PRNT50 titer responses in 18-to 45-year-old adults in highly endemic countries: CYD22 andCYD47. The CYD22 study enrolled healthy individuals in Viet-nam aged 2 to 45 years,29 whereas the CYD47 trial enrolledhealthy adults in India aged 18–45 years.30
If PRNT50 titers were judged to meet the “reasonably likely”criterion noted previously, then comparing vaccine-inducedtiters between 9- to 16-year-olds and 18- to 45-year-oldscould help support the use of the vaccine in adults in terms ofthe reduction in the overall dengue incidence. We first con-ducted a standard bridging analysis that fits an AcceleratedApproval–type paradigm, by comparing PRNT50 titers be-tween18- to 45-year-olds and9- to 16-year-olds basedon theCYD22, CYD47, CYD14, and CYD15 data. Demonstratingnon-inferiority of PRNT50 titers in the older cohort wouldconstitute the typical evidence provided to regulatory agen-cies to justify the bridging clinical efficacy based on a surro-gate end point. In addition, we then estimated VE against VCDover the first 25monthspost first vaccination in 18- to45-year-olds based on an epidemiological method we developed forbridging efficacy based on baseline covariates and interme-diate response end points and accounting for multiple sero-types of the pathogen.31
MATERIALS AND METHODS
CYD14 and CYD15 trials. The trials had the same studydesign and protocol, which randomly assigned healthy chil-dren in 2:1 allocation to vaccine or placebo administeredat months 0, 6, and 12 (further details are given in refs. 15 and16). Active surveillance was used to identify primary endpointcases (VCD) of any of the 4 serotypes (DENV-Any) over25 months since first vaccination. A case–cohort design wasused to measure neutralization responses in CYD14 andCYD15, whereby enrollees in the first 2–4 months of the trialswere randomly assigned to an immunogenicity subset formeasuring the neutralization response at months 0 (baselinebefore first vaccination), 7, 13, and 25.18 Neutralization re-sponseswere alsomeasured atmonth 13 from all subsequentDENV-Any cases. The correlates analyses in Moodie et al.18
were performed in participants who had not previously ex-perienced the DENV-Any endpoint by month 13.CYD22 and CYD47 trials. Sanofi Pasteur conducted the
CYD22 study (ClinicalTrials.gov ID NCT0087552429), a phase2 trial of the CYD-TDV vaccine that enrolled 180 healthy in-dividuals in Vietnam aged 2–45 years. Within four age strata2–5, 6–11, 12–17, and 18–45, participants were randomized
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 165

in 2:1 allocation to receive either the CYD-TDV vaccine or acontrol (placebo or control vaccine), administered at months0, 6, and 12 (the identical schedule as for CYD14 and CYD15).Relevant for our analyses, n = 52 9- to 16-year-olds and n = 3018- to 45-year-olds (vaccine and placebo combined) hadbaseline PRNT50 measurements. In addition, n = 32 9- to16-year-old and n = 18 18- to 45-year-old vaccine recipientsreceived all three doses of the CYD-TDV vaccine and hadmonth 13 PRNT50 measurements. A primary aim of CYD22was to measure dengue neutralizing antibodies at baselineand at 28 days after each CYD-TDV vaccination (including atmonth 13). The study began enrollment in March 2009 andwas completed in December 2014.Another phase 2 trial, CYD47 (ClinicalTrials.gov ID
NCT0155028930), evaluated the immunogenicity and safety ofthe CYD-TDV vaccine in healthy adults aged 18–45 years inIndia.30 Participantswere randomized2:1 to receiveCYD-TDV(n = 128) or placebo (n = 61) at months 0, 6, and 12; n = 187 ofthese had baseline PRNT50 measured and n = 115 CYD-TDVrecipients received all three vaccinations and had month 13PRNT50 measured. A main objective was to measure dengueneutralizing antibodies at the baseline and at 28 days aftereachCYD-TDV vaccination (including atmonth 13). The studybegan enrollment in March 2012 and was completed in Feb-ruary 2014.50% plaque reduction neutralization test assay. In this
study, 50% plaque reduction neutralization test titers weremeasured using an optimized and validated assay as pre-viously described.32 The assaywasconducted in a centralizedSanofi Pasteur facility for all studies. The assay measures theability of antibodies present in serum samples to neutralizethe infectivity to Vero cells of each of the four parental DENVsfrom which the CYD-TDV recombinant vaccine viruses werederived. Titers were expressed as the reciprocal of the highestserumdilution atwhich thenumber of plaques in infectedwellswas ³ 50% lower than that in negative control wells. The lowerlimit of quantitation was 10; values below this were set to 5.Statistical analysis. Non-inferiority of month 13 neutraliz-
ing responses in 18- to 45-year-olds versus 9- to 16-year-olds.For each analyzed cohort and time point (baseline or month13), the geometric mean (GM) PRNT50 was estimated, withCIs calculated as transformed t-distribution CIs of log base10 PRNT50 values. Point and CI estimates about GM ratioscomparing cohorts were calculated similarly. Titers to eachserotype and the average titer were assessed, where a par-ticipant’s average titer was the GM of the four serotype-specific antibody titers.18
Estimating VE in 18- to- 45-year-olds. The full statisticalanalysis plan (SAP) that was prespecified for the bridginganalysis is provided in the supplementary material (“SAP forbridgingVE from theCYD14+CYD159- to 16-year-old cohortto a new setting (18- to 45-year-old adults) via the Gilbert andHuang (2016) bridging method”; April 5, 2017) and describesall of the used methods in detail, including the assumptionsneeded for valid bridging. Here, we summarize the usedmethods, which address two objectives. Objective 1 esti-mated VE against DENV-Any occurring between months0 (first vaccination) and 25 (13 months post last vaccination atmonth 12) in a population of 18- to 45-year-olds; this VE pa-rameter was one minus the ratio (vaccine versus placebo) ofthe cumulative probabilities of VCD occurrence by month 25.Objective 2was the same, except VEagainst VCD is estimated
for each serotype v separately, VE(v) for v = 1, 2, 3, and 4,where VE(v) was one minus the ratio (vaccine versus placebo)of the cumulative probabilities of VCD occurrence by month25 and the first VCD occurrence was of serotype v. Objectives1 and 2 were repeated for additive–difference versions of theVE parameters—referred to as VEd and VEd(v)—which were(vaccine minus placebo) cumulative probabilities. Under anassumption that vaccinationdid not increase the risk of VCD in18- to 45-year-olds, each of these parameters VEd and VEd(v)had an attributable risk interpretation as the probability arandomized participant had VCD by month 25 averted byvaccination.The VE parameters were estimated for two populations of
18- to 45-year-olds. Bridging population 1was 18- to 45-year-olds for the hypothetical scenario, where the entire CYD14 +CYD15 study had included an 18- to 45-year-old cohort underidentical follow-up/ecological conditions and surveillance forVCD as for the 9- to 16-year-olds. Bridging population 2 was18- to 45-year-olds in India (CYD47) for the hypotheticalscenario that the background/unvaccinated risk of VCD overthe first 25months post first vaccination was the same as thatfor CYD14 + CYD15 9- to 16-year-olds.Estimation for bridging population 1 was performed using
theCYD22 study as a “calibration study”because itmeasuredPRNT50 titers for both 9- to 16-year-olds and 18- to 45-year-olds, allowing estimation of age–cohort differences in titerdistributions. Assuming that these age–cohort differences inCYD22 would be the same in CYD14 + CYD15 allowed usingthe PRNT50 titer data from CYD14 + CYD15 9- to 16-year-olds—plus a calibration factor estimated from CYD22—toestimate these titer distributions in the hypothetical CYD14 +CYD15 18- to 45-year-old study. (See the SAP Section 2.2Assumption 2 for details on how the calibration was per-formed.) Estimation for bridging population 2 used the CYD47study titer data. Because CYD47 did not include a 9- to16-year-old cohort, the calibration technique could not beused, such that we defined bridging population 2 as theCYD47 18- to 45-year-old population itself, for which the di-rect estimates of the CYD47 18- to 45-year-old titer distribu-tions could be used.Different versions of the Gilbert and Huang31 transport for-
mula were used for both objectives, each with multiple steps.The first step of every method estimated from CYD14 +CYD15 data how VE varied over vaccinated subgroups de-fined by month 13 PRNT50 titers and/or how VE varied oversubgroups defined by baseline PRNT50 titers, as performedby ref. 18. For this step, we always used the cohort of 9- to16-year-olds in CYD14 + CYD15 pooled, based on the factsthat the CYD14 and CYD15 protocols were the same, thepooling increased precision for estimation of the VE curves,and the PRNT50 titer distributions and estimated vaccine ef-ficacies were similar in CYD14 9- to 14-year-olds and CYD159- to 16-year-olds.18 The first set ofmethods address bridgingobjective 1 to estimate the overall VE, with four variants 1a, 1b,1c, and 1d that differ by being based on (a) month 0 and13 serotype titers, (b) month 0 serotype titers, (c) month 0 and13 average titers, and (d) month 0 average titers. The secondset of methods address bridging objective 2 to estimateserotype-specific VE, with two variants, where method 2auses both month 0 and month 13 serotype titers and method2b only uses month 0 serotype titers. We summarize themethods addressing objective 2 first because the methods
166 GILBERT, HUANG, AND OTHERS

for addressing objective 1 use results from the objective 2analyses.Method 2a: Serotype-specific VE objective based on
month 0 and 13 serotype titers. Based on the CYD14 +CYD15 9- to 16-year-old cohort, step 1 estimated each of thefour serotype-specific VE curves VE14.15.9–16(t = 25, vjSv = s)for DENV-v through 25 months as functions of month 13homologous serotype v titers Sv using the Juraska et al.method33 as implemented in Moodie et al.18 (SupplementalFigure 1); these VE curves express how VE varied over vac-cinated subgroups defined by month 13 neutralization titers,using the VE curve effect modification framework.34–36 Step 2estimated each of the four serotype-specific VE curvesVE14.15.9–16(t = 13, vjXv = s) for DENV-v through 13 months asfunctions of baseline homologous titers Xv using the Huanget al.37 logistic regression method as also implemented in ref.18 (Supplemental Figure 2). Step 3 estimated VEd(v) in the 18-to 45-year-old cohort by combining two averages. The firstaveraged the estimate of VE14.15.9–16(t = 25, vjSv = s) over theestimated distribution of Sv in the 18- to 45-year-old cohort,with weighting by 1) a specified ratio of the VE curveVE18–45(t = 25, vjSv = s) in the 18- to 45-year-old cohortcompared with VE14.15.9–16(t = 25, vjSv = s) and 2) an estimateof the background/unvaccinated DENV-v risk from month 13to 25 conditional on Sv in the 18- to 45-year-old cohort. Thesecond averaged the estimate of VE14.15.9–16(t = 13, vjXv = s)over the estimated distribution of Xv in the 18- to 45-year-oldcohort, with weighting by 1) a specified ratio of the true curveVE18–45(t = 13, vjXv = s) in the 18- to 45-year-old cohortcompared with VE14.15.9–16(t = 13, vjXv = s) and 2) an estimateof the background/unvaccinated DENV-v risk frommonth 0 to13 conditional on Xv in the 18- to 45-year-old cohort. Thisformula was published as equations (8)–(11) in Gilbert andHuang31 and is listed in the April 5, 2017, SAP as equations (8)and (13)–(15) (with τ = 13 and t = 25). Last, VE(v) was estimatedby plugging the estimate of VEd(v) into equation (16) in theApril 5, 2017, SAP.Method 2b: Serotype-specific VE objective based onmonth
0 serotype titers. This approach was based on baseline titersXv, not accounting formonth 13 titers Sv. Step 1was the sameas step 2mentioned previously, except for DENV-v end pointsfrom month 0 to 25. Step 2 was the same as the second av-erage computed in step 3 mentioned previously, except forDENV-v end points from month 0 to 25; specifically, it aver-aged the estimate of VE14.15.9–16(t = 25, vjXv = s) over theestimated distribution of Xv in the 18- to 45-year-old cohort,with weighting by 1) a specified ratio of the true curveVE18–45(t = 25, vjXv = s) in the 18- to 45-year-old comparedwith VE14.15.9–16(t = 25, vjXv = s) and 2) an estimate of thebackground/unvaccinated DENV-v risk from month 0 to 25conditional onXv in the 18- to 45-year-old cohort. This formulawas published as equation (11) in Gilbert and Huang31 and islisted in the April 5, 2017, SAP as equations (15) and (16) (withτ = 25).Method 1a: Overall VE objective based on month 0 and 13
serotype titers. The estimate of VEd against DENV-Any wasthe sum of the estimates of VEd(v) for v = 1, 2, 3, and 4obtained from analysis 2a. Then, VE was estimated byplugging the estimate of VEd into equation (16) of the April 5,2017, SAP.Method 1b: Overall VE objective based on month 0 sero-
type titers. Similarly, the estimate of VEd against DENV-Any
was the sum of the estimates of VEd(v) for v = 1, 2, 3, and 4obtained from analysis 2b, and then, VEwas estimated usingequation (16) of the April 5, 2017, SAP.Method 1c: Overall VE objective based on month 0 and 13
average titers. This approach was identical to method 2a,except the DENV-v end point was replaced with DENV-Anyand homologous serotype v titers Sv and Xv were replacedwith average titers Savg and Xavg, respectively.Method 1d: Overall VE objective based on month 0 average
titers.Similarly, this approachwas identical tomethod2b,withDENV-v replaced with DENV-Any and the homologous sero-type v titer Xv was replaced with the average titer Xavg.The month 0 and 13 methods made use of baseline and
month 13 titers, whereas the month 0 methods used baselinetiters only. An advantage of the former methods is that month13 titers were shown to bemore predictive of VE than baselinetiters (Figure 4 of ref. 18). By contrast, it is logistically simplerto base bridging on baseline titers because future phase 1bridging studies would not require 13 months of follow-up formeasuring postvaccination titers. Moreover, by not requiringestimation of VE curves VE14.15.9–16(t = 25, vjSv = s) thatcondition on month 13 titers if assigned vaccine, Sv, thesemethods avoid making assumptions to accommodate themissing month 13 responses of placebo recipients. However,the challenge posed to the month 0 methods is that, becauseof a lack of available samples, baseline titers could only bemeasured in 13.4% of VCD cases in CYD14 and CYD15,limiting precision.We included both approaches to assess theconsistency of results obtained with methods that make dif-ferent assumptions, where consistent results may strengthenthe evidence base for bridging.Key assumptions of the bridging methods. We summarize
and briefly discuss the three key assumptions for themethods(Supplemental Table 1, complete details in the April 5, 2017,SAP Section 2). For methods 1a and 2a, assumption 1 spec-ified that the VE(v) curve by themonth 13 serotype v titer is thesame in the 18- to 45-year-old and9–16-year-old cohorts, andsimilarly for the VE(v) curve by the baseline serotype v titer.This posited that the homologous serotype v titer was the keypredictor of VE(v) and that conditional on its value, VE againstDENV-v was the same in the two age cohorts. Assumption 2was only needed for bridging to population 1. It posited thatthe cumulative distribution functions (cdfs) of each titer vari-able (Sv and Xv for v = 1, 2, 3, and 4) for the two CYD22 agecohorts (18–45 versus 9–16 years) were linked by a mixedbinary and continuous location shift model, that the odds ratioof positive response (i.e., titer > 10) for the two CYD14 +CYD15 age cohorts was the same as that for the two CYD22age cohorts, and that the location-shift model in positive re-sponders was the same for CYD14 + CYD15 and CYD22.Assumption 2 was used to obtain estimates of the distribu-tions of Sv and Xv for CYD14 + CYD15 18- to 45-year-olds,using Hodges–Lehmann estimators of the shift parametersbased on the CYD22 data (for each v = 1, 2, 3, and 4). As-sumption3posited that after accounting forSv, the agecohortdid not affect the background/unvaccinated dengue-v riskfrommonth 13 to 25, and that after accounting for Xv, the agecohort did not affect the background/unvaccinated dengue-vrisk from month 0 to 13 and from month 0 to 25. For the ob-jective 1 methods based on average titers, the parallel as-sumptions were made for DENV-Any and average titers. Themonth 0 and 13 method 1c made the same assumptions,
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 167

except in terms of the average titer instead of serotype-specifictiters. Moreover, the month 0 methods (1b and 2b) made thesame assumptions, except only for baseline titers and fordengue VCD follow-up from month 0 to 25 instead of frommonth 0 to 13 (see Supplemental Table 1).Assumption 1 could be violated if there was another
immune response marker with a different distribution inCYD14 + CYD15 9- to 16-year-olds and 18- to 45-year-oldsthat modified VE(v) after accounting for the homologous se-rotype PRNT50 titer. For assumption 2, the location-shiftmodel in CYD22 could be directly checked from the observeddata, and the bridging of this model to CYD14 + CYD15 isreasonable if we expect the age cohort to have a similar effecton titers in Vietnam and in the other CYD14 + CYD15 coun-tries. Assumption 3 posited that the age cohort adds no moreinformation about the dengue risk of unvaccinated personsafter accounting for neutralizing antibody titers, and so es-sentially is about the sufficiency of this marker for capturingthe risk. There seems to be limited epidemiological dataavailable for verifying this assumption. It is reasonable under apremise/model that the degree of prior dengue exposure andinfection is the fundamental underlying dengue risk factor in9- to 45-year-olds and the neutralization titer is a better proxyfor that factor than age. Some support for this premise derivesfrom the four multivariable logistic regression models ofDENV-v risk for CYD14 and CYD15 9- to 16-year-old placeborecipients conditional on both serotype v titer and age (9–11versus 12–16 years) for each v = 1, 2, 3, and 4, which showedstrong inverse associations of serotype v titers with DENV-vrisk and no evidence of age associations.18
CIs about VE in the 18- to 45-year-old cohorts. Bootstrappercentile 95% CIs were computed about the VE parametersthat accounted for themultiple sources of sampling variability,namely, the estimated VE curves from CYD14 + CYD15 9- to16-year-olds; the estimated distributions of Sv, Xv, Savg, andXavg in the 18- to 45-year-old cohorts (which accounted for
sampling variability in theCYD22calibration study for bridgingpopulation 1 and for the sampling variability in CYD47 forbridging population 2); and the estimated background denguerisks as a function of month 0 titers in CYD14 + CYD15 9- to16-year-olds. In addition, bootstrap percentile 95%estimateduncertainty intervals (EUIs) were computed about the VE pa-rameters that accounted for uncertainty both due to samplingvariability and to possible violations of assumptions 1 and 3(see the April 5, 2017, SAP).Sensitivity analysis to possible violations of assumptions 1
and 3. Two sensitivity analyses were conducted for all of themethods, which we describe for method 2a; parallel ap-proaches were used for the other five methods. The firstsensitivity analysis specified the ratio of the Denv-v VE curvesin the two age cohorts, VE18–45(t = 25, vjSv = s)/VE14.15.9–16(t =25, vjSv = s), to be a fixed constant f that varied between0.8 and 1.2, and studied how the results varied with f. In thesecond sensitivity analysis,fwas again varied from0.8 to 1.2,and a second sensitivity parameter ρ, defined as the ratio ofthe background/unvaccinated incidence of DENV-v frommonth 0 tomonth 13 and frommonth 0 to 25 conditional on Xvin the two age cohorts (18–45/9–16 years), was set equal to0.8. This allowed the background DENV-v risk to be lower inthe older age cohort, where ρ above 1 was not consideredbecause it is thought to be unlikely based on the epidemio-logical literature.
RESULTS
Non-inferiority of month 13 neutralizing responsesin 18- to 45-year-olds versus 9–16-year-olds. We firstassessed whether month 13 neutralizing responses in 18- to45-year-olds were non-inferior to those in 9- to 16-year-olds,by comparing month 13 PRNT50 titers 1) between the twoage cohorts within CYD22 (CYD22 18- to 45-year-olds ver-sus CYD22 9–16-year-olds) and 2) between the two age
TABLE 1Comparison of month 13 neutralizing antibody titers (50% plaque reduction neutralization test) in CYD-TDV vaccine recipients receiving all threevaccinations between age cohorts (18–45 vs. 9–16 years) in the CYD22, CYD47, and CYD14 + CYD15 studies
Study CYD22 CYD47 CYD14 + CYD15
Age (years) 18–45 9–16 18–45 9–16Sample size 18 32 115 1870Average titer Response rate (95% CI) 100.0% (82.4, 100.0) 100.0% (89.3, 100.0) 100.0% (96.8, 100.0) 99.8% (99.5, 99.9)
GM (95% CI) 549.6 (392.6, 769.3) 204.5 (125.6, 333.0) 480.5 (387.8, 595.3) 374.8 (352.5, 398.5)GM ratio (95% CI) 2.69 (1.49, 4.84) Ref 1.28 (1.03, 1.60) Ref
1.47 (1.04, 2.07) – – RefDENV-1 Response rate (95% CI) 100.0% (82.4, 100.0) 96.9% (84.3, 99.4) 97.4% (92.6, 99.1) 94.8% (93.7, 95.7)
GM (95% CI) 695.5 (335.3, 1,442.7) 176.7 (87.3, 357.7) 461.2 (340.2, 625.3) 352.0 (321.1, 385.8)GM ratio (95% CI) 3.94 (1.43, 10.85) Ref 1.31 (0.95, 1.80) Ref
1.98 (0.95, 4.13) – – RefDENV-2 Response rate (95% CI) 100.0% (82.4, 100.0) 100.0% (89.3, 100.0) 97.4% (92.6, 99.1) 98.6% (97.9, 99.0)
GM (95% CI) 825.2 (492.5, 1,382.6) 350.6 (187.1, 656.9) 484.5 (370.3, 633.9) 565.3 (527.2, 606.1)GM ratio (95% CI) 2.35 (1.05, 5.29) Ref 0.86 (0.65, 1.13) Ref
1.46 (0.87, 2.46) – – RefDENV-3 Response rate (95% CI) 100.0% (82.4, 100.0) 96.9% (84.3, 99.4) 99.1% (95.2, 99.8) 97.9% (97.2, 98.5)
GM (95% CI) 423.8 (286.3, 627.4) 157.1 (94.9, 260.1) 709.0 (551.9, 911.0) 431.6 (400.4, 465.2)GM ratio (95% CI) 2.70 (1.43, 5.10) Ref 1.64 (1.26, 2.13) Ref
0.98 (0.66, 1.47) – – RefDENV-4 Response rate (95% CI) 100.0% (82.4, 100.0) 96.9% (84.3, 99.4) 100.0% (96.8, 100.0) 97.8% (97.0, 98.3)
GM (95% CI) 375.0 (250.7, 561.0) 179.7 (106.8, 302.4) 336.3 (271.4, 416.8) 229.8 (216.9, 243.5)GM ratio (95% CI) 2.09 (1.08, 4.02) Ref 1.46 (1.17, 1.83) Ref
1.63 (1.09, 2.45) – – RefDENV = dengue virus; GM = geometric mean; Ref = reference group in the denominator.
168 GILBERT, HUANG, AND OTHERS
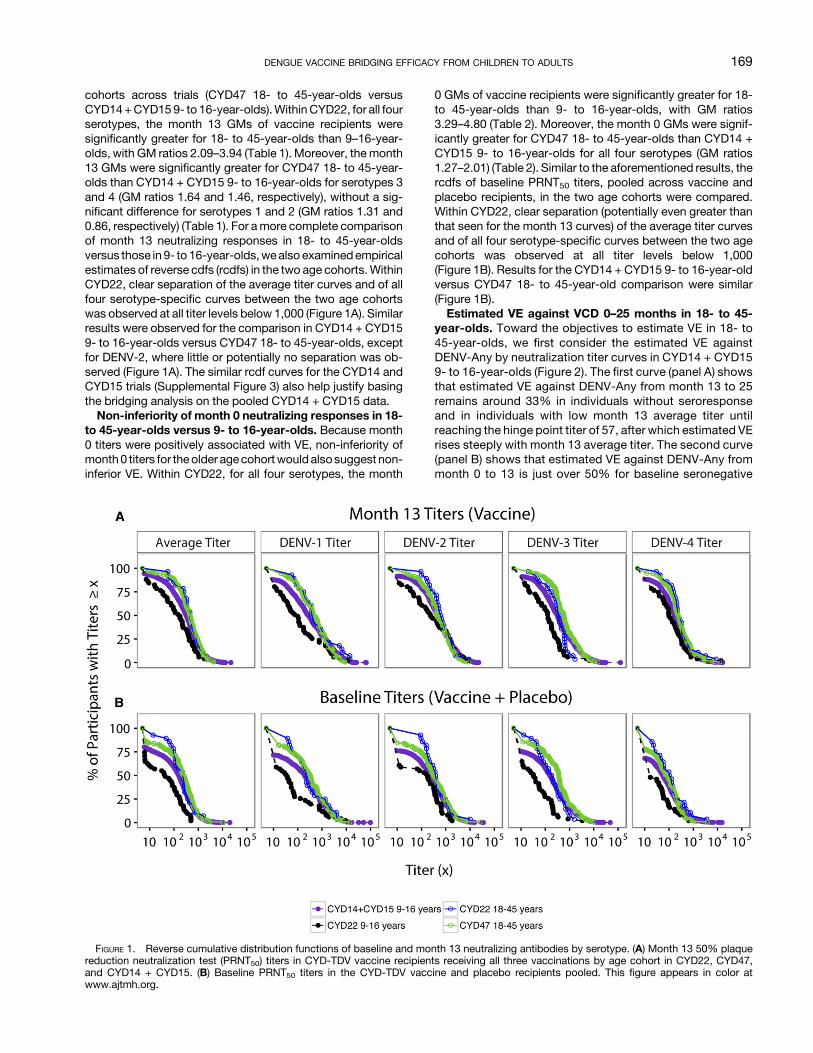
cohorts across trials (CYD47 18- to 45-year-olds versusCYD14+CYD159- to 16-year-olds).WithinCYD22, for all fourserotypes, the month 13 GMs of vaccine recipients weresignificantly greater for 18- to 45-year-olds than 9–16-year-olds, with GM ratios 2.09–3.94 (Table 1). Moreover, themonth13 GMs were significantly greater for CYD47 18- to 45-year-olds than CYD14 + CYD15 9- to 16-year-olds for serotypes 3and 4 (GM ratios 1.64 and 1.46, respectively), without a sig-nificant difference for serotypes 1 and 2 (GM ratios 1.31 and0.86, respectively) (Table 1). For amore complete comparisonof month 13 neutralizing responses in 18- to 45-year-oldsversus those in 9- to 16-year-olds,wealso examinedempiricalestimates of reverse cdfs (rcdfs) in the two age cohorts.WithinCYD22, clear separation of the average titer curves and of allfour serotype-specific curves between the two age cohortswas observed at all titer levels below 1,000 (Figure 1A). Similarresults were observed for the comparison in CYD14 + CYD159- to 16-year-olds versus CYD47 18- to 45-year-olds, exceptfor DENV-2, where little or potentially no separation was ob-served (Figure 1A). The similar rcdf curves for the CYD14 andCYD15 trials (Supplemental Figure 3) also help justify basingthe bridging analysis on the pooled CYD14 + CYD15 data.Non-inferiority of month 0 neutralizing responses in 18-
to 45-year-olds versus 9- to 16-year-olds. Because month0 titers were positively associated with VE, non-inferiority ofmonth0 titers for theolder agecohortwould also suggest non-inferior VE. Within CYD22, for all four serotypes, the month
0 GMs of vaccine recipients were significantly greater for 18-to 45-year-olds than 9- to 16-year-olds, with GM ratios3.29–4.80 (Table 2). Moreover, the month 0 GMs were signif-icantly greater for CYD47 18- to 45-year-olds than CYD14 +CYD15 9- to 16-year-olds for all four serotypes (GM ratios1.27–2.01) (Table 2). Similar to the aforementioned results, thercdfs of baseline PRNT50 titers, pooled across vaccine andplacebo recipients, in the two age cohorts were compared.Within CYD22, clear separation (potentially even greater thanthat seen for the month 13 curves) of the average titer curvesand of all four serotype-specific curves between the two agecohorts was observed at all titer levels below 1,000(Figure 1B). Results for the CYD14 + CYD15 9- to 16-year-oldversus CYD47 18- to 45-year-old comparison were similar(Figure 1B).Estimated VE against VCD 0–25 months in 18- to 45-
year-olds. Toward the objectives to estimate VE in 18- to45-year-olds, we first consider the estimated VE againstDENV-Any by neutralization titer curves in CYD14 + CYD159- to 16-year-olds (Figure 2). The first curve (panel A) showsthat estimated VE against DENV-Any from month 13 to 25remains around 33% in individuals without seroresponseand in individuals with low month 13 average titer untilreaching the hinge point titer of 57, after which estimated VErises steeply with month 13 average titer. The second curve(panel B) shows that estimated VE against DENV-Any frommonth 0 to 13 is just over 50% for baseline seronegative
FIGURE 1. Reverse cumulative distribution functions of baseline and month 13 neutralizing antibodies by serotype. (A) Month 13 50% plaquereduction neutralization test (PRNT50) titers in CYD-TDV vaccine recipients receiving all three vaccinations by age cohort in CYD22, CYD47,and CYD14 + CYD15. (B) Baseline PRNT50 titers in the CYD-TDV vaccine and placebo recipients pooled. This figure appears in color atwww.ajtmh.org.
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 169

individuals and rises gradually with baseline average titer.The third curve (panel C) shows a similar pattern for esti-mated VE against DENV-Any frommonth 0 to 25 by baselineaverage titer as that shown in panel B. These estimatedcurves are key elements of the bridging formula, where thecurves in (A) and (B) were used bymethod 1c and the curve in(C) was used by method 1d.We next used all four methods, 1a–1d, to estimate VE
againstDENV-Any for bridging populations 1 and2 (objective1). For population 1, estimated VE was greater than 75% forall of the methods, with the widest 95% CI extending from52.5% to 100.0% (Table 3). For population 2, estimatedVE was greater than 68% for all of the methods, with thewidest 95% CI extending from 42.3% to 88.5% (Table 3). Allof the VE estimates were greater than the observed estimatein CYD14 + CYD15 9- to 16-year-olds (65.6%, 95% CI:60.6–69.9%). This is explained by the monotone increasingVE curves in CYD14 + CYD15 9- to 16-year-olds (Figure 2,Supplemental Figures 1 and 2) combined with the fact thatbaseline and month 13 titers are consistently higher in 18- to45-year-olds than 9- to 16-year-olds (Tables 1 and2, Figure 1based on Vietnam data and India data versus the 10 endemiccountries in CYD14 and CYD15).Figure 3 shows the parallel results of Table 3 for estimating
the serotype-specific parameters VE(v) by methods 2a and 2bfor bridging populations 1 and 2, for each v = 1, 2, 3, and 4(objective 2). For both populations, the estimates for sero-types 3 and 4 were high (79.8–100.0%)—higher than thecorresponding estimates observed for CYD14 + CYD15 9- to16-year-olds of 73.6% (95% CI: 64.4, 80.4%) and 83.2%(95% CI: 76.2, 88.2%). For serotype 1, the estimates of VEwere 56.9% and 76.9% by methods 2a and 2b for population1, respectively, comparable with or higher than the CYD14 +CYD15 9- to 16-year-old estimate of 58.4% (95% CI: 47.7,66.9%), whereas for population 2, methods 2a and 2b gavedifferent VE estimates of 44.5% and 66.9%, respectively.
Whereas the 44.5% estimate might be surprising, given it isless than the estimate observed in CYD14 + CYD15 9- to16-year-olds (58.4%), it is larger than the estimate of 39.6% inCYD14 +CYD15 9- to 16-year-olds if method 2a were appliedto CYD14 + CYD15 9- to 16-year-olds; it may be explained bythe random difference in the estimated unvaccinated denguerisk and the estimated VE frommonth 0 to month 13 and frommonth 0 to month 25 between the sub-cohort with the base-line titer measured and the full cohort: the former was used inmethod 2a. For both populations, the estimates for serotype 2were all higher than the estimate from CYD14 + CYD15 9- to16-year-olds of 47.0% (95% CI: 31.3, 59.2%), although withwide CIs. In methods-validation analyses that applied VEcurves to estimate the overall VE for CYD14 + CYD15 9- to16-year-olds, we found that application of the month 13 VEcurves (used in methods 1a, 1c, and 2a) tended to yield esti-mates of overall VE that were smaller than the direct empiricalestimates, whereas application of the month 0 VE curves(used in methods 1b, 1d, and 2b) tended to yield similar esti-mates, suggesting that the bridging estimates 56.9% and44.5% may be conservative lower bounds.The CIs in Figure 3 show reasonable precision about the
beneficial efficacy in 18- to 45-year-olds against serotypes 3and 4 (lower 95% confidence limits [LCLs] varying between49.5% and 75.3% depending on the bridging method), andreasonable but less precision about the beneficial efficacyagainst serotype 1 (LCLs from 26.7% to 39.3%). By contrast,for serotype 2, there is lower precision, with all LCLs well be-low 0%. The CIs support a conclusion that there is fairly highconfidence that the CYD-TDV vaccine would protect wellagainst serotypes 3 and 4 in both bridging populations, and atleastmoderatelywell against serotype 1,whereas for serotype2, much uncertainty remains as to the protection level.Supplemental Table 2 and Figure 4 show the parallel results
asTable 3 andFigure 3, for the additive–differenceparametersVEd and VEd(v), respectively. The results in Supplemental
TABLE 2Comparison of month 0 neutralizing antibody titers (50% plaque reduction neutralization test) in the CYD-TDV vaccine and placebo recipients(pooled) between age cohorts (18–45 vs. 9–16 years) in the CYD22, CYD47, and CYD14 + CYD15 studies
Study CYD22 CYD47 CYD14 + CYD15
Age (years) 18–45 9–16 18–45 9–16Sample size 30 52 187 2,728Average titer Response rate (95% CI) 93.3% (78.7, 98.2) 75.0% (61.8, 84.8) 87.2% (81.6, 91.2) 80.1% (78.5, 81.5)
GM (95% CI) 156.2 (93.2, 262.0) 39.0 (23.7, 64.1) 152.3 (117.8, 196.9) 94.1 (87.6, 101.1)GM ratio (95% CI) 4.00 (1.96, 8.20) Ref 1.62 (1.24, 2.11) Ref
1.66 (0.99, 2.80) – – RefDENV-1 Response rate (95% CI) 90.0% (74.4, 96.5) 61.5% (48.0, 73.5) 82.4% (76.3, 87.1) 71.5% (69.8, 73.2)
GM (95% CI) 215.5 (107.1, 433.6) 44.9 (24.0, 83.9) 199.2 (146.4, 271.1) 116.1 (106.3, 126.9)GM ratio (95% CI) 4.80 (1.88, 12.29) Ref 1.72 (1.24, 2.36) Ref
1.86 (0.92, 3.76) – – RefDENV-2 Response rate (95% CI) 93.3% (78.7, 98.2) 63.5% (49.9, 75.2) 84.5% (78.6, 89.0) 76.0% (74.3, 77.5)
GM (95% CI) 290.3 (163.6, 515.0) 70.6 (37.3, 133.8) 215.8 (160.8, 289.8) 137.6 (126.6, 149.5)GM ratio (95% CI) 4.11 (1.74, 9.69) Ref 1.57 (1.15, 2.13) Ref
2.11 (1.18, 3.77) – – RefDENV-3 Response rate (95% CI) 93.3% (78.7, 98.2) 65.4% (51.8, 76.8) 85.6% (79.8, 89.9) 75.0% (73.4, 76.6)
GM (95% CI) 132.2 (76.7, 227.7) 33.4 (20.4, 54.8) 217.7 (163.5, 289.9) 108.3 (99.8, 117.6)GM ratio (95% CI) 3.95 (1.89, 8.26) Ref 2.01 (1.49, 2.71) Ref
1.22 (0.70, 2.12) – – RefDENV-4 Response rate (95% CI) 83.3% (66.4, 92.7) 50.0% (36.9, 63.1) 78.1% (71.6, 83.4) 68.0% (66.3, 69.8)
GM (95% CI) 72.1 (38.4, 135.3) 21.9 (13.9, 34.6) 57.5 (45.6, 72.5) 45.3 (42.3, 48.5)GM ratio (95% CI) 3.29 (1.51, 7.18) Ref 1.27 (1.00, 1.62) Ref
1.59 (0.84, 3.00) – – RefDENV = dengue virus; GM = geometric mean; Ref = reference group in the denominator.
170 GILBERT, HUANG, AND OTHERS
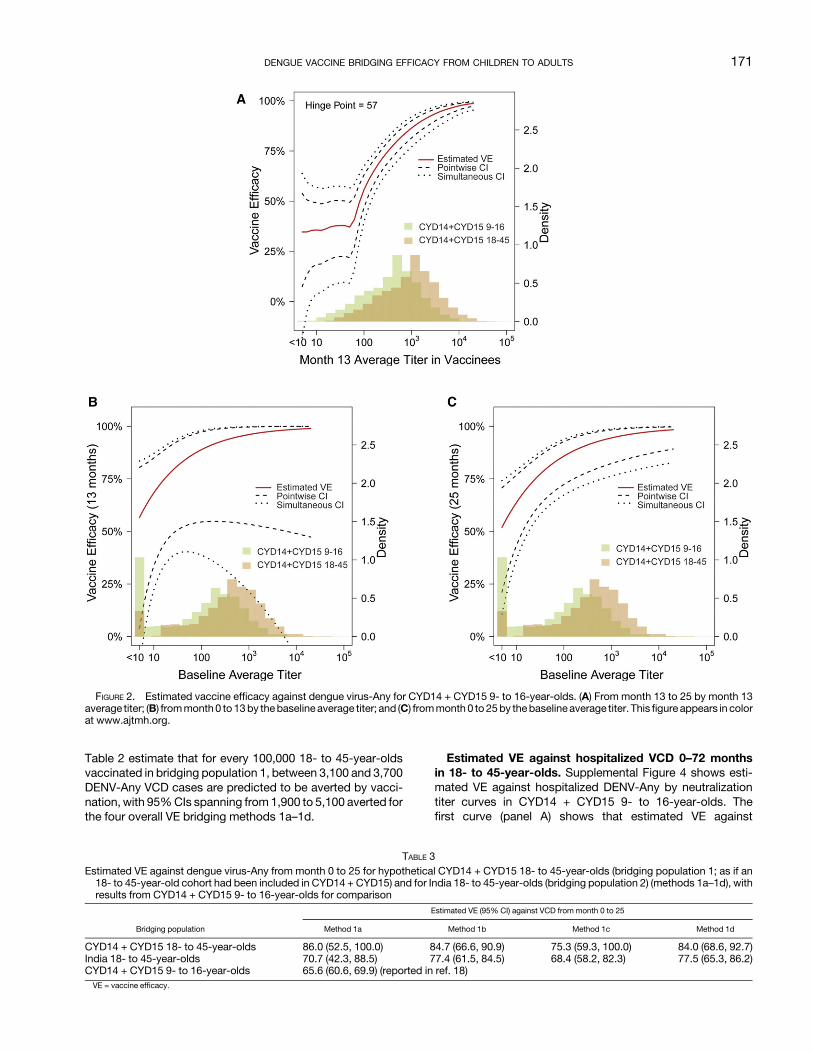
Table 2 estimate that for every 100,000 18- to 45-year-oldsvaccinated in bridging population 1, between 3,100 and 3,700DENV-Any VCD cases are predicted to be averted by vacci-nation, with 95%CIs spanning from 1,900 to 5,100 averted forthe four overall VE bridging methods 1a–1d.
Estimated VE against hospitalized VCD 0–72 monthsin 18- to 45-year-olds. Supplemental Figure 4 shows esti-mated VE against hospitalized DENV-Any by neutralizationtiter curves in CYD14 + CYD15 9- to 16-year-olds. Thefirst curve (panel A) shows that estimated VE against
FIGURE 2. Estimated vaccine efficacy against dengue virus-Any for CYD14 + CYD15 9- to 16-year-olds. (A) From month 13 to 25 by month 13average titer; (B) frommonth0 to13by thebaselineaverage titer; and (C) frommonth0 to 25by thebaselineaverage titer. This figure appears in colorat www.ajtmh.org.
TABLE 3Estimated VE against dengue virus-Any from month 0 to 25 for hypothetical CYD14 + CYD15 18- to 45-year-olds (bridging population 1; as if an18- to 45-year-old cohort had been included in CYD14 + CYD15) and for India 18- to 45-year-olds (bridging population 2) (methods 1a–1d), withresults from CYD14 + CYD15 9- to 16-year-olds for comparison
Bridging population
Estimated VE (95% CI) against VCD from month 0 to 25
Method 1a Method 1b Method 1c Method 1d
CYD14 + CYD15 18- to 45-year-olds 86.0 (52.5, 100.0) 84.7 (66.6, 90.9) 75.3 (59.3, 100.0) 84.0 (68.6, 92.7)India 18- to 45-year-olds 70.7 (42.3, 88.5) 77.4 (61.5, 84.5) 68.4 (58.2, 82.3) 77.5 (65.3, 86.2)CYD14 + CYD15 9- to 16-year-olds 65.6 (60.6, 69.9) (reported in ref. 18)VE = vaccine efficacy.
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 171

hospitalized DENV-Any from month 13 to 72 is near zero inindividuals without month 13 seroresponse and individualswith low month 13 average titer until reaching the hinge pointtiter of 31, after which estimated VE rises steeply with month13average titer (estimatedVE is 0%for vaccine recipientswithno month 13 seroresponse and reaches about 60% and 90%at titers 100 and 1,000, respectively). The second curve (panelB) shows a similar monotone pattern for estimated VE againstDENV-Any from month 0 to 72 by baseline average titer, butless steep. These estimated curves are key elements of thebridging formula, where the curve in (A) was used by method1cand thecurve in (B)wasusedbymethod1d.Vaccineefficacycurves for hospitalized DENV-Any by serotype were not com-puted because of limited serotype-specific end point counts.Table 4 shows the results of methods 1c and 1d applied to thetwo bridging populations. For bridging population 1, estimatedVE is 59.1% (95% CI: 40.9–92.2%) and 73.5% (95% CI:44.7–89.0%) by method 1c and 1d, respectively. For bridgingpopulation 2, estimatedVE is 50.9% (95%CI: 38.1–70.1%) and65.9% (95%CI: 39.2–82.1%), respectively. Theseestimates foradults are comparable or slightly less than the estimates fromSridhar et al.20 forCYD14+CYD15+CYD239- to16-year-olds:estimated VE = 66% (95% CI: 27–84%) (Table 4).
Supplemental Table 3 shows the results for VEd for thehospitalized DENV-Any VCD endpoint from 0 to 72 months.The results estimate that for every 100,00018- to 45-year-oldsvaccinated in bridging population 1, between 1,000 and 1,200hospitalized DENV-Any VCD cases are predicted to be aver-ted by vaccination, with 95% CIs spanning from 600 to 1,900averted for the two overall VE bridging methods 1c and 1d.Sensitivity analysis for estimated VE against VCD
0–25 months in 18- to 45-year-olds. Figure 5 shows theestimates of VE against DENV-Any for bridging population 1 inthe first sensitivity analysis, which varied the sensitivity pa-rameter f from 0.8 to 1.2 and fixed the sensitivity parameter ρto value 1.0. For f above one, the VE estimates were greaterthan the original estimates at f = 1, and we focus on theestimates for f < 1, as there is particular interest in un-derstanding VE if the original assumptions were incorrect ingiving optimistically high VE.At the boundary pointf=0.8, theestimates of VE across methods 1a–1d were 65.6%, 67.8%,56.8%, and 67.2%, decreases of 23.7%, 20.0%, 24.6%,and 20.0%, respectively, compared with the original esti-mates at f = 1. These results show that if assumption 1 isviolated such that theVEcurvebymonth 13 titers is 20% lowerin 18- to 45-year-olds than 9- to 16-year-olds, then VE in
FIGURE 3. Estimated vaccine efficacy against dengue virus-v for each serotype v = 1, 2, 3, and 4 from month 0 to 25. Estimates are shown forCYD14+CYD159- to16-year-olds (top rowpanel, for reference); for hypotheticalCYD14+CYD1518- to45-year-olds (bridgingpopulation1) undermethod 2a (second row panel); for India 18- to 45-year-olds (bridging population 2) under method 2a (third row panel), and repeating the latter twoanalyses under method 2b (fourth and fifth row panels).
172 GILBERT, HUANG, AND OTHERS

CYD14 + CYD15 18- to 45-year-olds is predicted to be aboutthe same as that observed in CYD14 + CYD15 9- to 16-year-olds (VE = 65.6%). Supplemental Figure 5 shows the esti-mates of VE against DENV-Any for bridging population 1 in thesecond sensitivity analysis (with ρ = 0.8): the results at themost conservative point inf (f=0.8,ρ=0.8)were the sameasthose at (f = 0.8, ρ = 1.0).These results show that this par-ticular violation of assumption 3 does not affect the results.
Supplemental Figures 6 and 7 show the parallel results forbridging population 2, where at (f = 0.8, ρ = 1.0), the VE es-timates are 53.3%, 61.9%, 51.3%, and 62.0% and at (f = 0.8,ρ = 0.8), are 53.4%, 61.9%, 51.5%, and 62.0% under the fourmethods, respectively. Thus, estimated VE in India 18- to 45-year-olds ranges from 51.3% to 62%, depending on themethod and bounds of the sensitivity analysis, which isslightly less than the estimated VE observed in CYD14 +
FIGURE 4. Estimated additive–difference vaccine efficacy against dengue virus-v frommonth 0 to 25. Estimates are shown for CYD14 + CYD159- to 16-year-olds (top row panel, for reference); for hypothetical CYD14 + CYD15 18- to 45-year-olds (bridging population 1) under method 2a(second row panel); for India 18- to 45-year-olds (bridging population 2) under method 2a (third row panel), and repeating the latter two analysesunder method 2b (fourth and fifth row panels).
TABLE 4Estimated VE against hospitalized dengue virus-Any frommonth 0 to 72 for hypothetical CYD14 + CYD15 18–45-year-olds (bridging population 1;as if an 18- to 45-year-old cohort had been included inCYD14+CYD15) and for India 18- to 45-year-olds (bridging population 2) (methods 1c and1d), with results from CYD14 + CYD15 9- to 16-year-olds for comparison
Bridging population
Estimated VE (95% CI) against hospitalized VCD from month 0 to 72
Method 1c Method 1d
CYD14 + CYD15 18- to 45-year-olds 59.1% (40.9%, 92.2%) 73.5% (44.7%, 89.0%)India 18- to 45-year-olds 50.9% (38.1%, 70.1%) 65.9% (39.2%, 82.1%)CYD14 + CYD15 + CYD57 9- to 16-year-olds 66 (27, 84)*TMLE = targeted maximum likelihood estimation; VE = vaccine efficacy.* Estimates fromSridhar et al.20 The log cumulative relative risk (vaccine/placebo) for all CYD14+CYD15+CYD57 9- to 16-year-oldswas estimated as theweighted average of the log cumulative
relative riskestimates for baseline seropositive andseronegativeparticipants reported inFigure1ofSridhar et al.20 (the “TMLE,month0onward”entries). CYD57contributed less than5%of the totalsample size. The weights include inverse variance estimates of the log cumulative relative risks reported in Figure 1 (1/0.164 and 1/0.136 for seropositive and seronegative participants) and thereportedestimates (bySuperlearner) of the fractionsof participantswhoarebaseline seropositiveandseronegative (76.0%and24.0%).CumulativeVE isestimatedas100%multipliedbyoneminusthe exponentiated log cumulative relative risk estimate with 95% CI computed by transforming symmetric Wald confidence limits for the log cumulative relative risk.
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 173

CYD159- to 16-year-olds. Vaccine efficacy is projected to beless in 18- to 45-year-olds in India than in CYD14 + CYD15,given the higher estimated titers in hypothetical CYD14 +CYD15 18- to 45-year-olds than for CYD47 18- to 45-year-olds (Supplemental Figure 8). The sensitivity analyses for theserotype-specific VE parameters show a similar amount ofsensitivity of the results to violations of assumptions 1 and 3(results not shown).Sensitivity analysis for estimated VE against hospital-
izedVCD0–72months in 18- to 45-year-olds.SupplementalFigures 4 and 5 list ignorance intervals and 95% EUIs for VEand VEd against hospitalized dengue over 0–72 months ineach bridging population for f varying from 0.8 to 1.2 and ρ =0.8 (results are almost identical for ρ = 1.0). Based on the 95%EUIs, the vaccine effect is consistently estimated to be ben-eficial, for example, 95%EUIs31.2–100%and28.9–88.2%forbridging populations 1 and 2 using method 1c, respectively.
DISCUSSION
Neutralizing antibody titers measured by PRNT50 at base-lineandatmonth13 (1monthpost dose3) havebeenshown tobe strongly associatedwithCYD-TDVVE to prevent VCD from
month 13 to 25 in the CYD14 and CYD15 phase 3 trials, withVE increasing with titers, and consistent result that high titersare associated with high VE across both trials, both baselineserostatus subgroups, all age groups, and for all four dengueserotypes. Although therewas somevariation in the estimatedVE curves between the two efficacy trials in the lower titerrange, indicating that other factors may influence VE, espe-cially at lower titers post third vaccination, the VE curves weresimilar when focusing on the 9- to 16-year-old cohort. Thesestatistical results, together with the assumption that neutral-izing antibodies are a mechanism of protection for the CYD-TDV vaccine, provide a ground for extrapolating VE to 18- to45-year-old adults from theCYD14- andCYD15-combined 9-to 16-year-old cohort based on baseline and month 13PRNT50 titers, in the absence of direct efficacy data in 18- to45-year-old adults. To enable bridging analyses, phase 2studies were conducted in Vietnam (CYD22) and India(CYD47) that measured baseline and month 13 PRNT50 titersin CYD-TDV vaccine recipients in 18- to 45-year-olds.In the Vietnam study that compared PRNT50 titers in 18- to
45-year-olds versus 9- to 16-year-olds, baseline and month13 titerswere consistently higher in theolder agegroupacrossthe serotypes (GM ratio of vaccine recipient month 0 and 13
FIGURE 5. First sensitivity analysis showing estimated vaccine efficacy (VE) against dengue virus-Any for hypothetical CYD14 + CYD15 18- to45-year-olds. Estimated VE against DENV-Any was calculated from month 0 to 25 with 95% CIs for the sensitivity parameter f varying between0.8 and 1.2 and sensitivity parameter ρ = 1.0 for hypothetical CYD14 + CYD15 18- to 45-year-olds (bridging population 1). The union of thepoint estimates is the estimated ignorance interval, and the union of the 95%CIs is the EUI. The analysis is performedusing eachmethod 1a, 1b, 1c,and 1d.
174 GILBERT, HUANG, AND OTHERS

average titers of 4.00 and 2.69, respectively). To a lesser de-gree, in the India study, titers in 18- to 45-year-olds wereconsistently higher than those in 9- to 16-year-olds combiningacross CYD14 and CYD15 (GM ratio of vaccine recipientmonth 0 and 13 average titers of 1.62 and 1.28, respectively),as well as being consistently higher than each of the 10countries included in CYD14 and CYD15. These results implythat if PRNT50 titers are a reliable correlate of VE that operatessimilarly in the two age cohorts, then VE in the adult cohort isexpected to be at least as high as that in the younger cohort,for VCD of each serotype and for VCD of any of the four se-rotypes (DENV-Any). The result of higher titers in the older agecohort may be generalized to other highly endemic settings,given that the cumulative amount of dengue exposure in-creases with age and this cumulative exposure increasesPRNT50 titers.16,18,38,39 Therefore, it is reasonable to expectthat in any given highly endemic setting, VE of CYD-TDVwould be equal to or greater in 18- to 45-year-olds than in9- to 16-year-olds. Although differences in prior exposure todengue and in the distribution of circulating serotypesacross highly endemic settings would impact the absolutelevel of VE across the settings, the fact that titers wouldgenerally be higher in the older population within any suchsetting implies that VE would also be expected to be at leastas high in the older than younger population within eachsetting.Our formal estimation and inference of VE against
DENV-Any from 0 to 25 months in a hypothetical cohort of18- to 45-year-olds (had it been included in CYD14 andCYD15—bridging population 1) support this conclusion, withVE estimates against DENV-Any across the four statisticalmethods of 75.3–86.0%, compared with the 65.6% estimatein CYD14 + CYD15 9- to 16-year-olds. These VE estimatesdecrease to 56.8–67.8% under a sensitivity analysis that al-lows the VE by titer curves to be lower in the older age cohortthan the younger age cohort.For making inference for a hypothetical cohort of 18- to
45-year-olds in India that would have the same background/unvaccinated dengue incidence as the CYD14 + CYD15 9- to16-year-old study, our methods yielded estimates of VEagainst DENV-Any from 0 to 25months of 68.4–77.5%, whichdecrease to 51.3–62.0% under the sensitivity analysis allow-ing departures from assumptions. Because there was not aninternal 9- to 16-year-old comparison group within CYD47,and India was not included in CYD14 or CYD15, it is moredifficult to interpret these VE estimates relative to a 9- to16-year-old cohort in India. The bridging results for Indiashould be interpreted as “what if” results in a hypotheticalscenario that an18- to 45-year-old cohort in India experiencedthe same incidence of symptomatic VCD incidence in theabsence of vaccination as the CYD14- and CYD15-combined9- to 16-year-old cohort. By contrast, the first set of bridgingresults is less hypothetical because of the internal age cohortcomparison within CYD22 and because the bridging is fromthe CYD14 + CYD15 efficacy trial to a hypothetical older agecohort in the same CYD14 + CYD15 context (same geogra-phies and time periods of exposure to dengue). In general, thebridging estimation methodology may also be applied to anyassumed/what if scenario about background/unvaccinatedDENV-Any VCD risk and/or serotype frequencies in a newpopulation, where these scenarios may be informed by epi-demiological data in the new population.
For estimating serotype-specific VE in CYD14 + CYD15 18-to 45-year-olds, estimated VE is higher than that in CYD14 +CYD15 9- to 16-year-olds for all four serotypes. The result forDENV-2 is of particular interest, given that VE was lowestagainst this serotype in CYD14 and CYD15 (as well as in theearlier efficacy trial CYD2340), despite DENV-2 titers being ashigh or higher than titers to the other three serotypes, and theestimatedDENV-2VEcurve by themonth 13DENV-2 titer wasthe steepest of the four curves for each of these three trials.Presumably, the higher levels of antibody compensate for thequality differences across serotypes in the antibody response,with high DENV-2 titers protecting against DENV-2; someheterotypic cross-response from any recent DENV exposuremight also account for this. For estimating serotype-specificVE in CYD47 18- to 45-year-olds, estimated VE is higher thanthat in CYD14 + CYD15 9- to 16-year-olds for the four sero-types yet by onemethodwas less for serotype 1. Although thislatter result is surprising, given that titerswerehigher inCYD4718- to 45-year-olds than in CYD14 + CYD15 9- to 16-year-olds, it can be explained as an anomaly because the bridgingmethod used data from the relatively small sub-cohort withbaseline titersmeasured, and sampling variability led to a too-low estimate.We also applied methods 1c and 1d used for bridging to VE
againstDENV-Anyover 0–25months for 18- to45-year-olds inan identical way for bridging to VE against hospitalized DENV-Any over 0–72 months for 18- to 45 year-olds, with VE esti-mates 59.1–73.5% for bridging population 1 andVE estimates50.9–65.9% for bridging population 2, which are comparablewith or slightly less than the 64% estimate in CYD14 +CYD15 + CYD57 9- to 16-year-olds from Sridhar et al.20
Method 1c requires an estimate of how VE against hospital-ized DENV-Any through month 13 varies with baseline aver-age titer. Of all participants who experienced the hospitalizedDENV-Any endpoint by month 13, there were only 4 partici-pants in the placebo group and 0 participants in the vaccinegroup for whom baseline average titer was measured. Thus,we modeled this VE curve by a logistic regression model withtwo independent variables (treatment assignment and base-line average titer), without an interaction term. This modelingchoice is conservative, tending to result in lower estimated VEin adults. We discuss in the following paragraphs further waysinwhich themethodswere implemented in amanner that aimsfor conservative lower bounds; thus, the overall conclusion isthat the multiplicative VE in preventing hospitalized dengueover 6 years of follow-up is expected to be as high in adults aschildren.Extrapolation of efficacy results to a newpopulationwithout
directlymeasuring efficacy in the newpopulation is generally adifficult task, given the inherent inability to empirically checkthe results, at least until results are available from phase 4post-licensure trials. A limitation of the bridging estimationmethods that use both month 0 andmonth 13 titers is that thekey assumption 1 would fail if there exists another immuneresponse to vaccination besides the month 13 neutralizationtitermeasuredbyPRNT50,whichmodifiesVEafter accountingfor month 13 PRNT50, and which has a different distribution in18- to 45-year-olds than 9–16-year-olds. This could occur, forexample, if the CD4 and/or CD8 T-cell response is also im-portant for VE and increases with age (albeit antibody alonehas been validated as a correlate of protection for Japaneseencephalitis virus vaccine and yellow fever vaccine),41 and
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 175

there is no validated T-cell correlate of protection, which isbeing evaluated in an ongoing ancillary study of CYD14.For example, even though the CYD-TDV chimeric vaccinecontains yellow fever virus nonstructural (NS) proteins ratherthan DENV NS proteins, CYD-TDV vaccination appears toresult in higher DENV-2/-3 NS3–specific CD8+ T-cell re-sponses in adults than adolescents at multiple time pointspostvaccination.42 This selective boosting of CD8+ T-cell re-sponses (i.e., from prior DENV infection) in vaccinated adultscompared with adolescents could contribute to increasedVE in adults because both serotype-specific and cross-serotype–reactive CD8+ T-cell responses against DENV NSproteins (including NS3) can contribute to protection fromPCR-confirmedDENV infection, at least in a transgenicmousemodel.43 We note that CD4+/CD8+ T-cell responses specificto DENV structural proteins, which can contribute to naturalprotection,44,45 are also elicited inCYD-TDVvaccinees.24,42,46
Although it is not known whether these responses differ sig-nificantly between 18- to 45-year-old versus 9- to 16-year-oldCYD-TDV vaccinees, which would impact the validity of as-sumption 1, CD4+ T-cell responses to staphylococcal en-terotoxin B have been shown to generally increase with ageuntil adulthood.47 This finding raises the possibility that similarDENV-specific CD4+ T-cell response boosting could occur inadult CYD-TDV vaccinees.Assumption 1would also be invalidated if baseline PRNT50
titer modifies VE after accounting for month 13 PRNT50 titer,given that baseline titers tend to be higher in 18- to 45-year-olds than 9- to 16-year-olds. Had baseline titers been mea-sured from most VCD cases in CYD14 and CYD15, then itwould have been possible to base the bridging analysis onthe bivariate VE surface that expresses how VE varies jointlyover subgroups defined by both baseline and month 13 ti-ters; the fact that baseline titers were only available from13.4% of VCD cases precluded this analysis. Given thislimitation, the sensitivity analysis is important, which showedhow the estimate of VE changes if assumption 1 is allowed tohave up to a 20% violation, and quantifies uncertainty via anEUI that accounts for uncertainty both due to sampling var-iability and due to possible violations of assumption 1 up to20%. Moreover, if there is an unmeasured immune responsethat modifies VE after accounting for the month 13 PRNT50titer that tends to be higher in 18- to 45-year-olds than9–16-year-olds, then not accounting for this immune re-sponse in the analysis would likely lead to biased estimatesof VE in the new population that are too low; this would occurif VE does not decrease with increasing levels of the un-measured immune response after fixing the month 13PRNT50 titer. Under the premise that the relevant immuneresponses do not decrease as age increases from 9–16 to18–45 years, this implies that the estimated VEs may beinterpreted as conservative lower bounds; moreover, theestimates under the sensitivity analysis may be interpretedas more conservative lower bounds.For the bridging methods that only use month 0 titers (not
month 13 titers), the same arguments apply swapping theroles of month 13 and baseline titers. Given that month 13titers were a stronger modifier of VE than baseline titers inCYD14andCYD15and are higher in 18- to 45-year-olds than9–16-year-olds, it seems likely that VEdependson themonth13 titer after accounting for the baseline titer, thus biasingthe VE estimates. However, similar arguments as mentioned
previously support that the direction of bias would render theobtained estimates of VE as conservative lower bounds.The challenges in assuring that assumptions are true for
bridging estimation led us to apply several versions of thebridgingmethods, that either usebothmonth0and13 titers, onlymonth0 titers, and that arebasedonserotype-specificVEcurvesor on average titer DENV-Any VE curves. The fairly consistentresults obtained across the methods provide some support forthe reliability of the results. The main advantage of the methodsusingbothmonth0 and13 titers is thatmonth 13 titersmodify VEmore strongly than baseline titers, such that not includingmonth13 titers likely excludes an effect modifier. By contrast, it is lo-gistically simpler to base bridging on month 0 baseline titersbecause future phase 1 bridging studies would not require13months of follow-up formeasuring postvaccination titers, andmoreover, themethodsbasedonbaseline titers donotmake anyassumptions about counterfactual causal parameters whoseestimation is made more complicated by missing data.We next discuss some additional limitations of this work. It
would be of considerable interest to apply our method to es-timate VE against symptomatic VCD in 18- to 45-year-oldsover a longer period of follow-up than 25 months, such asout to 72 months. This question is important given the con-cern of waning VE. However, we restricted our analysis ofthe symptomatic VCD end point to the protocol-specified25-month follow-up period because analysis of symptomaticVCD through 72 months is hindered by the gap (median27.1months) between the 25-month active surveillancephaseof follow-up for symptomatic VCD and the resumption of ac-tive surveillance. The intermediate passive surveillance phasetended to only capture highly symptomatic cases, and it isdifficult to conduct valid and interpretable analyses with mul-tiple case-ascertainment systems in the same study. Given thislimitation, we acknowledge that the analysis in this study doesnot directly support the extrapolation of VE against the symp-tomatic VCD end point for time frames longer than 25 months.It is also of considerable interest to apply our method
to estimate VE against hospitalized or severe VCD in 18- to45-year-olds over the entire follow-up period of 72months. Forthese dengue endpoints, the surveillance system was consis-tent during the 72-month follow-up period. However, precisionof estimates would be relatively low because of the relativelysmall number of hospitalized or severe VCD end points thansymptomatic VCD endpoints (in CYD14 and CYD15 9- to 16-year-olds pooled, there were an estimated 886 total symp-tomatic VCD end points over 25 months compared with 242hospitalized and 62 severe VCD end points over 72 months).Althoughwewereable to estimateVEagainst hospitalizedVCDof any serotype through 72 months, given the 242 endpoints,this number was too small to produce reliable estimates byserotype, and the total number of severe VCD end points wastoo small to venture any estimates of VE against severe VCD.Moreover, whereas it would also be of interest to bridge
VE for baseline seronegative and baseline seropositive sub-groups separately, because baseline serostatus was onlymeasurable in 13.4% of symptomatic VCD cases we de-termined that the resulting precision would be too low towarrant these analyses. However, because most 18- to45-year-olds in endemic regions are seropositive (93.3% inCYD22 and 84% in CYD47), the bridging estimates of multi-plicative VE reported here may be interpreted as reasonablyon target or lower bounds for multiplicative VE in seropositive
176 GILBERT, HUANG, AND OTHERS

18- to 45-year-olds. Because our bridging analyses werebased on VE curves including all CYD14 + CYD15 9- to16-year-olds and the estimated VE curves were higher forbaseline seropositive participants than baseline seronegativeparticipants, the multiplicative VE estimates in 18- to 45-year-olds are probably lower bounds. Another limitation of theanalyses is that estimation of the VE curves is challenging,given the missing counterfactual immune responses ifassigned vaccine in placebo recipients, and to tackle thischallenge, our analyses relied on parametric hinge linear lo-gistic models. These parametric assumptions cause the CIsabout the VE curves to be narrower than if these assumptionswere avoided, especially in the tails, where there are smallnumbers of participants with marker measurements. As aconsequence, our reported confidence and uncertainty in-tervals about VE parameters do not account for uncertainty inwhether these parametric assumptions hold, and, thus, arelikely too narrow in a sense. In addition, although ourmethodsfor calculating CIs and EUIs account for the finite-samplingvariability of the CYD22 and CYD47 trials, the limited samplesizes of these trials that provided critical data for immuno-bridging constitutes another limitation.Although our focus has been on bridging estimation of mul-
tiplicative and additive–difference VE for populations aged18–45 years as a group, we observe that within this age range,based on our modeling approach, we expect multiplicative VEto increase moving from 18-year-olds to 45-year-olds, andadditive-difference VE may potentially decrease moving from18-year-olds to 45-year-olds. The former statement is sup-ported by two findings, the first being that baseline seroposi-tivity frequency increases with age in CYD22 and CYD47 (e.g.,in CYD47 an estimated 69%, 73%, 77%, and 63% of 18-year-olds are seropositive for serotypes 1, 2, 3, and 4, respectively,compared with 94%, 95%, 94%, and 93% of 45-year-olds),and themeanbaseline serotype titer increaseswith age (e.g., inCYD47, the estimated mean titer is 126, 138, 120, and 32 forserotypes 1, 2, 3, and 4 for 18-year-olds comparedwith 389, 417,513, and 132 for 45-year-olds). The second finding is that theestimated VE curves from CYD14 + CYD15 9- to 16-year-oldsincreasewithbaselineandmonth13titers (Figure2,SupplementalFigures 1 and 2). Together, these two findings and our modelingapproach imply higher predicted VE for higher ages within 18–45years. The latter statementonadditive–differenceVE is supportedby the finding that baseline andmonth 13 neutralization titers areinverse correlates of VCD risk in both the vaccine and placebogroups,18 such that the VCD risks in both groups are expected todecrease closer to zero as age increases from 18 to 45 years.An important question is whether the increased risk for hospi-
talized and severe VCD seen in vaccinated seronegative (versusplacebo seronegative) children and adolescents20 would also beseen in adults, as such a scenario could limit the public healthimpact ofCYD-TDVvaccination of adults in endemic areaswhereseropositivity rates of adults are insufficiently high (we recentlyfound that seroposivity rates of 18- to 45-year-olds in endemicareas range from48.7% [Singapore] to 94.5% [Vietnam]48). Giventheextensiveevolutionof thehuman immunesystemfrominfancythrough old age (reviewed in ref. 49) and the fact that the contri-butions of age to infection outcomes and disease severity remainpoorly quantified, this remains an open question. In the context ofthepreviouslydiscussedhypothesis thatvaccinationofabaselineseronegative individual actsasaprimary infection, thisquestioncould be examined by comparing the risk of developing severe
disease in secondary infection in adults versus children. Un-fortunately, few such analyses have been performed.However,there is hospital and seroepidemiological evidence to supportthat children have much higher risk of developing DHF/DSS insecondary infection than adults, in addition tomuch higher riskof dying from DHF/DSS in secondary infection than adults.50
Whereas it is unknown whether this finding holds true in othergeographic regions, with different circulating viral variants, theavailable evidence suggests that we would not expect the in-creased risk for hospitalized and severe VCD of vaccinatedseropositive (compared with seronegative) adults to be as highas that for their corresponding child/adolescent counterparts.Another modeling consideration of interest is whether wide-spread vaccination with CYD-TDV could lead over time to adelay in the age at which natural DENV-Any seropositivity oc-curs, which could theoretically increase the proportion of 18- to45-year-olds who are dengue seronegative.In the future, the epidemiological bridging methods applied
here to dengue vaccination may be useful for other vaccines,especially vaccines against antigenically heterogeneouspathogens such as influenza, HIV, and malaria.
Received June 27, 2018. Accepted for publication March 30, 2019.
Published online May 20, 2019.
Note: Supplemental tables and figures appear at www.ajtmh.org.
Acknowledgments: We thank all participants in the CYD14, CYD15,CYD22, and CYD47 trials, and administrative and clinical researchstaff who helped ensure successful completion of the trials.
Financial support: This work was supported by Sanofi Pasteur(www.sanofipasteur.us) through a contract to P. B. G. and by theNational Institute of Allergy and Infectious Diseases (NIAID), NationalInstitutes of Health (NIH), Department of Health and Human Ser-vices, under award number R37AI054165 to P. B. G.
Disclosures: N. J., L. C., A. B., B. Z., C. F., S. P., and F. N. are em-ployeesof SanofiPasteur. B. Z., F.N., L.C., A. B., andC. F. ownstocksin Sanofi Pasteur, and N. J. has long-term incentives for SanofiPasteur. P. B. G., Y. H., M. J., Z. M., Y. F., A. L., Y. Z., J. S., and L. N. C.received a contract from Sanofi Pasteur to conduct the statisticalanalysis work. P. B. G., M. J., and Y. F. received support for travel tomeetings fromSanofiPasteur, andP.B.G. servedasanunpaidconsultantto Sanofi Pasteur at Advisory meetings in June and November of 2017.
Authors’ addresses: Peter B. Gilbert, Ying Huang, and Youyi Fong,Vaccine and Infectious Disease Division, Fred Hutchinson CancerResearch Center, University of Washington, Seattle, WA, E-mails:[email protected], [email protected], and [email protected] Juraska, Zoe Moodie, Alexander Luedtke, Jason Shao, andLindsay N. Carpp, Vaccine and Infectious Disease Division, FredHutchinson Cancer Research Center, Seattle, WA, E-mails: [email protected], [email protected], [email protected], [email protected], and [email protected]. Yingying Zhuang, University of Wash-ington, Seattle, WA, E-mail: [email protected]. Nicholas Jackson,Laurent Chambonneau, Sophie Pallardy, Sanofi Pasteur, Marcy-L’Etoile, France, E-mails: [email protected], [email protected], and [email protected]. AlainBouckenooghe and Carina Frago, Sanofi Pasteur, Singapore, E-mails:[email protected]@sanofi.com.BetzanaZambrano, Sanofi Pasteur, Montevideo, Uruguay, E-mail: [email protected]. Fernando Noriega, Sanofi Pasteur, Swiftwater,PA, E-mail: [email protected].
REFERENCES
1. Murray NE, Quam MB, Wilder-Smith A, 2013. Epidemiology ofdengue: past, present and future prospects. Clin Epidemiol5: 299–309.
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 177

2. World Health Organization, 2012. World Health Organization(WHO) Global Strategy for Dengue Prevention and Control,2012–2020. Geneva, Switzerland: WHO Press.
3. Bhatt S et al., 2013. The global distribution and burden of dengue.Nature 496: 504–507.
4. BradyOJ,GethingPW,BhattS,MessinaJP,Brownstein JS,HoenAG,MoyesCL, FarlowAW,Scott TW,HaySI, 2012.Refining theglobal spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis 6: e1760.
5. Thai KT, Binh TQ, Giao PT, Phuong HL, Hung le Q, Van Nam N,Nga TT, Groen J, Nagelkerke N, de Vries PJ, 2005. Seropre-valenceof dengueantibodies, annual incidenceand risk factorsamong children in southern Vietnam. Trop Med Int Health10: 379–386.
6. Low SL, Lam S, Wong WY, Teo D, Ng LC, Tan LK, 2015. Dengueseroprevalence of healthy adults in Singapore: serosurveyamong blood donors, 2009. Am J Trop Med Hyg 93: 40–45.
7. Chew CH et al., 2016. Rural-urban comparisons of dengueseroprevalence in Malaysia. BMC Public Health 16: 824.
8. Rodriguez-Barraquer I, Buathong R, Iamsirithaworn S, Nisalak A,Lessler J, Jarman RG, Gibbons RV, Cummings DA, 2014.Revisiting Rayong: shifting seroprofiles of dengue in Thailandand their implications for transmission and control. Am J Epi-demiol 179: 353–360.
9. Carabali M, Hernandez LM, Arauz MJ, Villar LA, Ridde V, 2015.Why are people with dengue dying? A scoping review of de-terminants for dengue mortality. BMC Infect Dis 15: 301.
10. Sam SS, Omar SF, Teoh BT, Abd-Jamil J, AbuBakar S, 2013.Review of dengue hemorrhagic fever fatal cases seen amongadults: a retrospective study. PLoS Negl Trop Dis 7: e2194.
11. Moraes GH, de Fatima Duarte E, Duarte EC, 2013. Determinantsof mortality from severe dengue in Brazil: a population-basedcase-control study. Am J Trop Med Hyg 88: 670–676.
12. Egger JR, Coleman PG, 2007. Age and clinical dengue illness.Emerg Infect Dis 13: 924–925.
13. Thai KT, Nishiura H, Hoang PL, Tran NT, Phan GT, Le HQ, TranBQ, Nguyen NV, de Vries PJ, 2011. Age-specificity of clinicaldengue during primary and secondary infections. PLoS NeglTrop Dis 5: e1180.
14. Guy B, Lang J, Saville M, Jackson N, 2016. Vaccination againstdengue: challenges and current developments. Annu Rev Med67: 387–404.
15. Villar L et al., 2015. Efficacy of a tetravalent dengue vaccine inchildren in Latin America. N Engl J Med 372: 113–123.
16. Capeding MR et al., 2014. Clinical efficacy and safety of a noveltetravalent dengue vaccine in healthy children in Asia: a phase3, randomised, observer-masked, placebo-controlled trial.Lancet 384: 1358–1365.
17. Juraska M et al., 2018. Viral genetic diversity and protective effi-cacy of a tetravalent dengue vaccine in two phase 3 trials. ProcNatl Acad Sci USA 115: E8378–E8387.
18. Moodie Z et al., 2018. Neutralizing antibody correlates analysis oftetravalent dengue vaccine efficacy trials in Asia and LatinAmerica. J Infect Dis 217: 742–753.
19. Hadinegoro SR et al., 2015. Efficacy and long-term safety of adengue vaccine in regions of endemic disease. N Engl J Med373: 1195–1206.
20. Sridhar S et al., 2018. Effect of dengue serostatus on denguevaccine safety and efficacy. N Engl J Med 379: 327–340.
21. Mizumoto K, Ejima K, Yamamoto T, Nishiura H, 2014. On the riskof severe dengue during secondary infection: a systematic re-view coupled with mathematical modeling. J Vector Borne Dis51: 153–164.
22. Pancharoen C, Mekmullica J, Thisyakorn U, 2001. Primary den-gue infection: what are the clinical distinctions from second-ary infection? Southeast Asian J Trop Med Public Health32: 476–480.
23. Endy TP, Yoon IK, Mammen MP, 2010. Prospective cohortstudies of dengue viral transmission and severity of disease.Curr Top Microbiol Immunol 338: 1–13.
24. Guy B, Jackson N, 2016. Dengue vaccine: hypotheses to un-derstand CYD-TDV-induced protection. Nat Rev Microbiol14: 45–54.
25. Katzelnick LC, Gresh L, Halloran ME, Mercado JC, Kuan G,Gordon A, Balmaseda A, Harris E, 2017. Antibody-dependent
enhancement of severe dengue disease in humans. Science358: 929–932.
26. Salje H et al., 2018. Reconstruction of antibody dynamics andinfection histories to evaluate dengue risk.Nature 557: 719–723.
27. Ferguson NM, Rodriguez-Barraquer I, Dorigatti I, Mier-Y-Teran-Romero L, Laydon DJ, Cummings DA, 2016. Benefits and risksof the Sanofi-Pasteur dengue vaccine: modeling optimal de-ployment. Science 353: 1033–1036.
28. World Health Organization, 2018. Revised SAGE Recom-mendation on Use of Dengue Vaccine. Available at: http://www.who.int/immunization/diseases/dengue/revised_SAGE_recommendations_dengue_vaccines_apr2018/en/. AccessedApril 19, 2018.
29. Tran N, Luong C, Vu T, Forrat R, Lang J, Vu Q, Bouckenooghe A,Wartel T, 2012. Safety and immunogenicity of recombinant, liveattenuated tetravalent dengue vaccine (CYD-TDV) in healthyVietnamese adults and children. J Vaccines Vaccin 3: 162.
30. Dubey AP, Agarkhedkar S, Chhatwal J, Narayan A, Ganguly S,Wartel TA, Bouckenooghe A, Menezes J, 2016. Immunoge-nicity and safety of a tetravalent dengue vaccine in healthyadults in India: a randomized, observer-blind, placebo-controlledphase II trial. Hum Vaccin Immunother 12: 512–518.
31. Gilbert PB, Huang Y, 2016. Predicting overall vaccine efficacy ina new setting by re-calibrating baseline covariate and in-termediate response endpoint effect modifiers of type-specificvaccine efficacy. Epidemiol Methods 5: 93–112.
32. Timiryasova TM, Bonaparte MI, Luo P, Zedar R, Hu BT, HildrethSW, 2013. Optimization and validation of a plaque reductionneutralization test for the detection of neutralizing antibodies tofour serotypes of dengue virus used in support of denguevaccine development. Am J Trop Med Hyg 88: 962–970.
33. Juraska M, Huang Y, Gilbert PB, 2018. Inference on treatmenteffect modification by biomarker response in a three-phasesampling design. Biostatistics. Available at: https://doi.org/10.1093/biostatistics/kxy074 [Epub ahead of print].
34. PlotkinSA,Gilbert PB, 2012.Nomenclature for immunecorrelatesof protection after vaccination. Clin Infect Dis 54: 1615–1617.
35. Qin L, Gilbert PB, Corey L, McElrath MJ, Self SG, 2007. Aframework for assessing immunological correlates of pro-tection in vaccine trials. J Infect Dis 196: 1304–1312.
36. Gilbert PB, Gabriel EE, Miao X, Li X, Su SC, Parrino J, Chan IS,2014. Fold rise in antibody titers by measured by glycoprotein-based enzyme-linked immunosorbent assay is an excellentcorrelate of protection for a herpes zoster vaccine, demon-strated via the vaccine efficacy curve. J Infect Dis 210:1573–1581.
37. Huang Y, Gilbert PB, Janes H, 2012. Assessing treatment-selection markers using a potential outcomes framework.Biometrics 68: 687–696.
38. Clapham HE et al., 2016. Dengue virus (DENV) neutralizing anti-body kinetics in children after symptomatic primary and post-primary DENV infection. J Infect Dis 213: 1428–1435.
39. Katzelnick LC,MontoyaM,Gresh L, BalmasedaA, Harris E, 2016.Neutralizing antibody titers against dengue virus correlate withprotection from symptomatic infection in a longitudinal cohort.Proc Natl Acad Sci USA 113: 728–733.
40. Sabchareon A et al., 2012. Protective efficacy of the recombi-nant, live-attenuated, CYD tetravalent dengue vaccine in Thaischoolchildren: a randomised, controlled phase 2b trial.Lancet 380: 1559–1567.
41. PlotkinSA,2010.Correlatesof protection inducedbyvaccination.Clin Vaccine Immunol 17: 1055–1065.
42. Harenberg A et al., 2013. Persistence of Th1/Tc1 responses oneyear after tetravalent dengue vaccination in adults and ado-lescents in Singapore. Hum Vaccin Immunother 9: 2317–2325.
43. Elong Ngono A, Chen HW, TangWW, Joo Y, King K, Weiskopf D,Sidney J, Sette A, Shresta S, 2016. Protective role of cross-reactive CD8 T cells against dengue virus infection. EBio-Medicine 13: 284–293.
44. Weiskopf D, Bangs DJ, Sidney J, Kolla RV, De Silva AD, de SilvaAM, Crotty S, Peters B, Sette A, 2015. Dengue virus infectionelicits highly polarized CX3CR1+ cytotoxic CD4+ T cells as-sociatedwithprotective immunity.ProcNatlAcadSciUSA112:E4256–E4263.
178 GILBERT, HUANG, AND OTHERS

45. Mathew A, Townsley E, Ennis FA, 2014. Elucidating the role ofT cells in protection against and pathogenesis of dengue virusinfections. Future Microbiol 9: 411–425.
46. DayanGH,Galan-HerreraJF,ForratR,ZambranoB,BouckenoogheA, Harenberg A, Guy B, Lang J, 2014. Assessment of bivalentand tetravalent dengue vaccine formulations in flavivirus-naive adults in Mexico. Hum Vaccin Immunother 10:2853–2863.
47. Hanna-Wakim R, Yasukawa LL, Sung P, Fang M, Sullivan B, RinkiM,DeHovitzR,ArvinAM,GansHA,2009.Age-related increase inthe frequencyofCD4(+) T cells thatproduce interferon-gamma in
response to staphylococcal enterotoxin B during childhood.J Infect Dis 200: 1921–1927.
48. L’AzouMet al., 2018.Dengue seroprevalence: data from the clinicaldevelopment of a tetravalent dengue vaccine in 14 countries(2005–2014). Trans R Soc Trop Med Hyg 112: 158–168.
49. Simon AK, Hollander GA, McMichael A, 2015. Evolution of theimmune system in humans from infancy to old age. Proc BiolSci 282: 20143085.
50. GuzmanMG,Kouri G, Bravo J, Valdes L, VazquezS, HalsteadSB,2002. Effect of age on outcome of secondary dengue 2 infec-tions. Int J Infect Dis 6: 118–124.
DENGUE VACCINE BRIDGING EFFICACY FROM CHILDREN TO ADULTS 179













![Dengue Fever/Severe Dengue Fever/Chikungunya Fever · Dengue fever and severe dengue (dengue hemorrhagic fever [DHF] and dengue shock syndrome [DSS]) are caused by any of four closely](https://img.pdfslide.us/doc/110x75/5e87bf3e7a86e85d3b149cd7/dengue-feversevere-dengue-feverchikungunya-dengue-fever-and-severe-dengue-dengue.jpg)





![WHO/BS/11.2159 ENGLISH ONLY EXPERT COMMITTEE ON …€¦ · 9 candidate tetravalent dengue virus vaccines (live) [66]. They should be read in 10 conjunction with other WHO guidelines](https://img.pdfslide.us/doc/110x75/606036d9a271d17c24240a4b/whobs112159-english-only-expert-committee-on-9-candidate-tetravalent-dengue-virus.jpg)









