Embed Size (px)
Citation preview

Breaking Bad: A User’s Guide to Quality Improvement
Julie-Clare Becher
Consultant Neonatologist and Honorary Senior Lecturer
Royal Infirmary of Edinburgh


Clinical Research vs Quality Improvement
Research and RCTs QI and Statistical Process Control
• Creation of new knowledge
• One tightly controlled comparison with current practice
• Fixed hypothesis
• ‘Just in case’ data
• Slow, cumbersome and expensive
• Harder to repeat
• Implementation of knowledge
• Flexible hypothesis
• ‘Just enough’ data
• Sequential small tests of change
• Real time and immediate information
• Easily repeatable

Florence Nightingale
Ignaz Semmelweiss
Early Pioneers of Healthcare QI

Marginal Gains Theory: “If you broke down everything you could think of that goes into riding a bike, and then improved it by one percent, you will get a significant increase when you put them all together” Dave Brailsford Performance Director of the GB Cycling Team
Hudson plane crash 2009: A miracle? ‘That’s what we’re trained to do’ Sullenberger, Pilot

Neonatal benchmarking networks: • North America: VON, CNN-EPIC, CPQCC, iNeo, NICHD,
Pediatrix
• Australia: ANZNN
• UK: NNAP
?CQC
NICORE Neonatal SPSP MBRRACE
‘The habit for evidence-based thinking The habit for change The habit for systems thinking The habit for collaborative learning’
“We can only be sure to improve what we can actually measure” Lord Darzi, High Quality Care for All, 2008

If all variation were bad, solutions would be easy. The difficulty is in reducing the bad variation, which reflects the limits of professional knowledge and failures in its application, while preserving the good variation that makes care patient centred. Mulley 2010
Horbar et al. Pediatrics 2012 MBRRACE Jun 2015
Mortality and Morbidity in VLBW, VON 2000-2009
Reducing Unwanted Variation in Practice

The Scottish Patient Safety Programme
• Overall Aim: to reduce hospital mortality by 15%
• ‘one of the most ambitious patient safety initiatives in the world – national in scale, bold in aims, and disciplined in science. It harnesses the energies and wisdom of Scotland’s healthcare leaders – all aligned toward a common vision, making Scotland the safest nation on earth from the viewpoint of healthcare’ Don Berwick DoH England
Key Highlights since 2008
• Reduction in mortality by 16% (10,500 lives)
• Reduction in surgical mortality by 25%
• 80% reduction C Diff and MRSA
• Surgical pause, VTE and Sepsis 6 (70-95%)

Key objectives of the initial Neonatal SPSP
By December 2015 to achieve a 30% reduction in ‘avoidable harm’ in Scottish Neonatal Services by seeking to reduce:
• harm from mechanical ventilation
• harm from invasive lines
• high risk medicines
• NEC
• harm from transitions of care
• undetected deterioration

NeoSPSP: Challenges of the first phase
• Too ambitious- 47 different measures
• Too little capacity in the workforce, no ‘Champions’
• Definitions did not match other national targets
• Burden of data collection precluded QI
• Suboptimal engagement
• National Survey of the Neonatal Community: ▫ Momentum for ongoing QI and PS work
▫ Sharing of challenges and of improvement strategies
▫ Commitment to shape the next steps of the programme Feb 2015. Becher JC, Jackson A and Staines J


‘Next Steps’ of the NeoSPSP 2016-
• Clinicians leading in format and design
• Branding focus on QI and not only PS
• Staged and flexible approach – centre-relevant aims ▫ Building a QI and safety culture in every unit- standards
▫ Improving specific outcomes using national guidance
• Benchmarkable and transparency at a national level
• Congruence with other data organisations
• Streamlined solution for national data collection/analysis
• National learning for both QI and adverse events


The Model for Improvement
What change can we make that will result in improvement?
Plan
How will we know that a change is an improvement?
Measurement: outcome, process and balancing
What are we trying to accomplish?
Outcome
Langley, Nolan et al 1996

The Lothian story: The Newborn Care Collaborative
▫ Established November 2013
▫ Provides oversight of all improvement work- >50 projects
▫ Strategic vision for improvement
▫ Avoid duplication of effort and time and provide project support
▫ Led by multidisciplinary committee
QI team
Patient safety including HAI
Audit
Guidelines
Pharmacy
Postnatal and Labour ward representatives
Parents
▫ Aims to listen to every voice


Implementing change: Understanding people factors
‘’There are only
two things I hate:
Change, and the way things are..’’
Not enough
time Too much change
Loss of power
Top down approach
Who’s sharing
this with me?
What’s in it for me?
I don’t like your
style
No one told me
Is this solution the right
one?
Not all change is for better
20% → effective change
Diffusion of Innovation Theory
THERE ARE ONLY TWO THINGS I HATE….
CHANGE AND THE WAY THINGS ARE


Parent representatives
on NCC
Antenatal preparedness
Ready, Coming or Not
Early information
Senior communication
Empowering parents
Our Journey Together
Real-time Feedback Getting Better Together
Building relationships
Baby diaries
Parent information Babylink
Discharge survey
The essential other elements of your team….. ‘Engage, empower, and hear patients and carers throughout the entire system, and at all times’ Don Berwick 2013


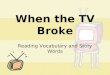
Getting Better Together Tree

Parent representatives
on NCC
Antenatal preparedness
Ready, Coming or Not
Early information
Senior communication
Empowering parents
Our Journey Together
Real-time Feedback Getting Better Together
Building relationships
Baby diaries
Parent information Babylink
Discharge survey
The essential other elements of your team….. ‘Engage, empower, and hear patients and carers throughout the entire system, and at all times’ Don Berwick 2013

Specific projects and activities High level factors
needed to influence the goal
Goal
Reduce NEC
Optimise obstetric care
Increase number of women receiving antenatal steroids
Delayed cord clamping 60 seconds for all preterm infants
Improve likelihood of breast milk feeding
Improve early and sustained maternal breast milk provision
Use donor breast milk in preference to formula
Minimise antibiotics
Reduce sepsis
Reduce empirical antibiotics
Driver diagram: Reducing NEC in infants <1501g (Neonatal SPSP target)

What change can we make that will result in improvement?
Plan
How will we know that a change is an improvement?
Measurement
What are we trying to accomplish?
Early provision of MBM
Reducing NEC and late onset sepsis in infants <1501g
(Neonatal SPSP target)
Outcome
• Babies <1501g or <30 weeks should receive their own mother’s breast milk:
• 90% within 24 h
• 100% within 72h
Measurement
• Number of mothers given support to express within 6 hours
• Measurement of early MBM on a monthly basis
• (Measurement of NEC)
Plan
• Education of all staff
• Information for parents
• Facilitation of expression and of MBM provision
• Guidelines and standards

UNICEF training days
National Conference
Infant Feeding Advisors
Feedback to staff
Early expression packs
Working Group
Improvement maternal information- Milk Diaries, BF App
Guideline-led enteral feeding
Skin to Skin initiative
Standard: Expression <6h
Standard: Expression <1h
2013
2015
Colostrum for mouthcare
2014

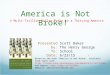
Improving MBM in <1501g infants: <24h
30
40
50
60
70
80
90
100
Au
g-1
3
Sep
-13
Oct-
13
No
v-1
3
De
c-1
3
Jan
-14
Fe
b-1
4
Ma
r-14
Ap
r-14
Ma
y-1
4
Ju
n-1
4
Ju
l-14
Au
g-1
4
Sep
-14
Oct-
14
No
v-1
4
De
c-1
4
Jan
-15
Fe
b-1
5
Ma
r-15
Ap
r-15
Ma
y-1
5
% receiving MBM <24h
Target
6 month mean

Improving MBM in <1501g infants: <72h
30
40
50
60
70
80
90
100
Au
g-1
3
Sep
-13
Oct-
13
No
v-1
3
De
c-1
3
Ja
n-1
4
Feb
-14
Mar-
14
Ap
r-14
May-1
4
Ju
n-1
4
Ju
l-1
4
Au
g-1
4
Sep
-14
Oct-
14
No
v-1
4
De
c-1
4
Ja
n-1
5
Feb
-15
Mar-
15
Ap
r-15
May-1
5
Target
% receiving MBM <72h
6mo mean

Specific projects and activities High level factors
needed to influence the goal
Goal
Reduce NEC
Optimise obstetric care
Increase number of women receiving antenatal steroids
Delayed cord clamping 60 seconds for all preterm infants
Improve likelihood of breast milk feeding
Improve early and sustained maternal breast milk provision
Use donor breast milk in preference to formula
Minimise antibiotics
Reduce sepsis
Reduce empirical antibiotics
Driver diagram: Reducing NEC and late onset sepsis in infants <1501g (Neonatal SPSP target)

Minimising prolonged exposure to admission antibiotics in babies with negative cultures
Baseline data collection
Mandatory automatic stop orders for all
Single CRP measurement
Introduction of 48h automatic stop orders

Duration of admission antibiotics in babies with
negative cultures
1 2 3 4
Intervention: Baseline 48hr
Autostop
Single
CRP
CRP and
Mandatory
Autostop
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
≥5d (treatment course)
>48h <5d (avoidable doses)
≤48h of antibiotics (empirical course)

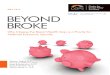
% NEC in inborn infants <1501g : RIE Edinburgh 2012-2014
0
1
2
3
4
5
6
7
8
9
10
2012 2013 2014
RIE, Edinburgh
VON mean

Final thoughts
• QI is here to stay and stands shoulder to shoulder with neonatal research ▫ ‘where is the RCT?’ is important but so is ‘what is everyone
learning?’
• QI is a journey without an end ▫ During which we learn that being good enough, isn’t good enough
• Delivering change is dependant on giving power to the people ▫ Clinicians leading in their own national QI projects ▫ Bottom up approach for engagement of frontline staff ▫ Parent partnerships in deciding what is best for their baby