Embed Size (px)
Citation preview

BrazilianNeurosurgery Arquivos Brasileiros de Neurocirurgia
EditorEberval Gadelha Figueiredo
ISSN 0103-5355
Number 2 • Volume 36 • Pages 75–142 • June 2017


Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
ISSN 0103-5355
Editor-in-Chief | Editor-Chefe
Eberval Gadelha Figueiredo
Emeritus Editors | Editores Eméritos
Milton ShibataGilberto Machado de Almeida†
Editorial Board | Conselho EditorialChairman | Presidente
José Marcus RottaManoel Jacobsen Teixeira
National Board | Conselho Nacional
Albedi BastosBelém, PA
Arnaldo ArrudaFortaleza, CE
Benedicto Oscar ColliRibeirão Preto, SP
Carlos TellesRio de Janeiro, RJ
Carlos Umberto PereiraAracaju, SE
Eduardo VellutiniSão Paulo, SP
Ernesto CarvalhoPorto, Portugal
Evandro de OliveiraSão Paulo, SP
Fernando Menezes BragaSão Paulo, SP
Francisco Carlos de AndradeSorocaba, SP
Hélio Rubens MachadoRibeirão Preto, SP
Hildo AzevedoRecife, PE
João Cândido AraújoCuritiba, PR
João Paulo FariasLisboa, Portugal
Jorge Luiz KraemerPorto Alegre, RS
José Alberto Gonçalves†
João Pessoa, PBJosé Alberto Landeiro
Rio de Janeiro, RJJosé Carlos Esteves Veiga
São Paulo, SPJosé Carlos Lynch Araújo
Rio de Janeiro, RJJosé Marcus Rotta
São Paulo, SPJosé Perez Rial
São Paulo, SPJose Weber V. de Faria
Uberlândia, MGLuis Alencar Biurrum Borba
Curitiba, PRManoel Jacobsen Teixeira
São Paulo, SPMarco Antonio Zanini
Botucatu, SPMarcos Barbosa
Coimbra, PortugalMarcos Masini
Brasília, DFMário Gilberto Siqueira
São Paulo, SPNelson Pires Ferreira
Porto Alegre, RSÓscar Luis Alves
Porto, PortugalPedro Garcia Lopes
Londrina, PRRicardo Vieira Botelho
São Paulo, SPRoberto Gabarra
Botucatu, SPSebastião Gusmão
Belo Horizonte, MGSérgio Cavalheiro
São Paulo, SPSergio Pinheiro Ottoni
Vitória, ESWaldemar Marques
Lisboa, Portugal
International Board | Conselho Internacional
Albert Sufi anovRussia
André G. MachadoUSA
Antonio de SallesUSA
Beatriz LopesUSA
Clement HamaniUSA
Daniel PrevedelloUSA
Felipe AlbuquerqueUSA
Jorge MuraChile
Kumar KakarlaUSA
Michael LawtonUSA
Nobuo HashimotoJapan
Oliver BozinovSwitzerland
Pablo RubinoArgentina
Paolo CappabiancaItaly
Peter BlackUSA
Peter NakajiUSA
Ricardo HanelUSA
Robert F. SpetzlerUSA
Rungsak SiwanuwatnThailand
Volker SonntagUSA
Yasunori FujimotoJapan

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
ISSN 0103-5355
S ociety Board | Diretoria (2017–2018)
Chairman | PresidenteRonald de Lucena Farias
Vice-Chairman | Vice-PresidenteValdir Delmiro Neves
General Secretary | Secretário-GeralItalo Capraro Suriano
Treasurer | TesoureiraMarise Augusto Fernandes Audi
First Secretary | Primeiro SecretárioMarco Antonio Herculano
Former Chairman | Presidente AnteriorModesto Cerioni Junior
Next Chairman 2019–2020 | Presidente Eleito 2019–2020Luis Alencar Biurrum Borba
Congress Chairman 2018 | Presidente do Congresso 2018Marcelo Paglioli Ferreira
Congress Chairman 2020 | Presidente do Congresso 2020Stenio Abrantes Sarmento
Equity and Controllership | Patrimônio e ControladoriaFrancisco de Assis Ulisses Sampaio Júnior
Educational & Scientifi c | Educacional e Científi co
Neurosurgery Formation | Formação NeurocirúrgicaSérgio Cavalheiro
Continued Education | Educação ContinuadaAlexandre Novicki Francisco
Guidelines and New Technologies | Diretrizes e Novas TecnologiasRicardo Vieira Botelho
Research | PesquisaEberval Gadelha Figueiredo
Public Relationship & Communication | Comunicação e Relacionamento Social
Communication & Marketing | Comunicação e MarketingFernando Campos Gomes Pinto
Social Responsibility | Responsabilidade SocialCarlos Roberto Sampaio de Assis Drummond
Ombudsman | OuvidoriaJair Leopoldo Raso
Professional Protection of Associated Activities | Defesa Profi ssional de Atividades Associativas
Professional Protection | Defesa Profi ssionalAlbert Vincent Berthier Brasil
National Integration | Integração Nacional Mauro Takao Marques Suzuki
Departments | Departamentos Ruy Castro Monteiro da Silva Filho
Technical - SUS | Câmara Técnica - SUSBruno Silva Costa
Statute | Codifi cação Wuilker Knoner Campos
Institutional Relations | Relações Institucionais Aluízio Augusto Arantes Junior
International Relations | Relações InsternacionaisJosé Marcus Rotta
Policies | PolíticasModesto Cerioni Junior
Parliament | ParlamanetoSandoval Inácio Carneiro
Think First Project | Projeto Pense BemFrancisco Ricardo Borges Ribeiro
Advisory Board | Conselho Deliberativo
Chairman | PresidenteLuiz Carlos de Alencastro
Secretary | SecretárioMarcos Masini
Directors | ConselheirosAluízio Augusto Arantes JuniorBenjamim Pessoa ValeGeraldo de Sá Carneiro FilhoJair Leopoldo RasoJânio NogueiraJorge Luiz KraemerJosé Carlos SalemeJosé Fernando Guedes CorreaJosé Marcus RottaLuis Renato Garcez de Oliveira MelloOrival AlvesOsmar José Santos de MoraesRicardo Vieira Botelho

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
Volume 36, Number 2/2017
online www.thieme-connect.com/products
Original Articles | Artigos Originais75 Endoscopic Sural Nerve Removal in Obstetric Brachial Plexopathy Using Basic Endoscopy Instruments:
Technical Note Retirada endoscópica do nervo sural na plexopatia braquial obstétrica utilizando instrumentos básicos de
endoscopia: nota técnicaJosé Augusto Malheiros, Sérgio Augusto Vieira Cançado, João Tiago Alves Belo, Luiz Alberto Otoni Garcia, Marcelo Magaldi de Oliveira, Martjin J. A. Malessy
80 Glioblastoma Multiforme: an Advanced Analysis of 153 Patients and Review of the Literature Glioblastoma Multiforme: uma análise avançada de 153 pacientes e revisão da literatura
Mohammad Sadegh Nikdad, Farshid Farhan, Milad Shafizadeh, Atefeh Sadat Mirmohseni, Mohsen Afarideh, Shabnam Asadi Komeleh, Marzieh Lashkari, Morsaleh Ganji, Alireza Ghajar, Saeed Shafiei, Yalda Shafizadeh, Ali Kazemian, Hooshang Saberi
91 Head Measurements for the Diagnosis of Craniosynostosis As medidas cranianas no diagnóstico das craniossinostoses
José Aloysio CostaVal, Leopoldo Furtado Mandic, Sebastião Nataniel Gusmão
Review Articles | Artigos de Revisão96 Chronic Subdural Hematoma Spontaneous Resolution Resolução espontânea de hematoma subdural crônico
Nícollas Nunes Rabelo, Vitor Hugo Honorato Pereira, George Santos dos Passos, Luciano José Silveira Filho, André Luiz Cicilini, Neiffer Nunes Rabelo, Luiz Antônio Araujo Dias Junior, Carlos Umberto Pereira, Luiz Antônio Araujo Dias
101 Axis Screw Fixation – A Step-by-Step Review of the Surgical Techniques Fixação do áxis com parafusos – uma revisão passo a passo das técnicas cirúrgicas
Andrei F. Joaquim, K. Daniel Riew
108 Revisiting Retrograde Ventriculosinus Shunt as an Alternative for Treating Hydrocephalus in Children Revisitando a derivação ventriculosinusal retrógrada como uma alternativa para tratamento de hidrocefalia
em criançasMatheus Fernandes Oliveira, Manoel Jacobsen Teixeira, Marcelo Lima Oliveira, Edson Bor Seng Shu, Fernando Campos Gomes Pinto
Case Reports | Relatos de Caso117 Compressive Myelopathy Due to Ossifi cation of the Ligamentum Flavum: Case Report and Review of
the Literature Mielopatia compressiva devido à ossifi cação do ligamento fl avo: relato de caso e revisão da literatura
Alisson R. Teles, Frederico A. Criscuoli de Farias, Marcelo R. Roxo, Albert Vincent Berthier Brasil
122 Arachnoid Cyst with a Non-traumatic Acute Subdural Hematoma in an Eleven-year-old Patient Cisto aracnoide associado a hematoma subdural agudo não traumático em um paciente de onze anos de
idadeGabriel Flamarin Cavasana, Rodrigo Mendonça, Fabricio Willian Mantelo Zanini
125 Intramedullary Spinal Capillary Hemangioma: Case Report Hemangioma capilar intramedular: relato de casoLeonardo Welling, Mariana S. Welling, Eberval G. Figueiredo
Thieme Revinter Publicações Ltda

128 Retrograde Endovascular Approach for Treating Unruptured Basilar Apex Aneurysms: Two Case Reports and Review of Literature
Acesso endovascular retrógrado no tratamento de aneurismas não rotos do ápice basilar: relato de dois casos e revisão da literaturaMarcus Alexandre Rotta, Guilherme M. Dias, André Luiz Rezende, Felix H. Pahl, Matheus Fernandes Oliveira, José Marcus Rotta
133 Disc Herniation and Cyst Gas: A Rare Association Causing Radicular Compression Herniação de gás intraespinal: uma associação rara causando compressão radicular
Cherkaoui Mandour, Miloudi Gazzaz, Brahim el Mostarchid
Miscellaneous | Artigo de Atualização136 Orbital Lymphangioma: Case Report and Management Paradigms Linfoma de órbita: relato de caso e paradigmas do manejo clínico
Alex Roman, Larissa Bianchini, Bárbara Battistel, Miguel Franzoi Neto, Daniela Schwingel
Letter to the Editor | Carta ao Editor141 Cervicomedullary Junction Ependymoma Associated with NF2: A Case Report and Literature Review Ependimoma da junção cervicobulbar associado a neurofi bromatose tipo II: relato de caso e revisão de
literaturaOtávio T. da Silva
Erratum | Errata142 Erratum: Chronic Subdural Hematoma Spontaneous Resolution Errata: Resolução espontânea de hematoma subdural crônico
Nícollas Nunes Rabelo, Vitor Hugo Honorato Pereira, George Santos dos Passos, Luciano José Silveira Filho, André Luiz Cicilini, Neiffer Nunes Rabelo, Luiz Antônio Araujo Dias Junior, Carlos Umberto Pereira, Luiz Antônio Araujo Dias
Brazilian Neurosurgery | Arquivos Brasileiros de Neurocirurgia Volume 36, Number 2/2017
Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
Copyright © 2017 by Thieme Revinter Publicações Ltda, Rio de Janeiro, Brazil. Arquivos Brasileiros de Neurocirurgia is published four times a year in March, June, September, and December by Thieme-Revinter Publicações Ltda, Rua do Matoso, 170, Rio de Janeiro, 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.thieme.com/bns.
Arquivos Brasileiros de Neurocirurgia is an official publication of the Brazilian Neurosurgery Society (Sociedade Brasileira de Neurocirurgia) and the Portuguese Language Neurosurgery Societies. It is listed in LILACS and LILACS-Express (Latin-American and Caribbean Center on Health Sciencies Information), and Latindex (Regional Cooperative Online Information System for Scholarly Journals from Latin America, the Caribbean, Spain and Portugal). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0103-5355
The colored content of this issue is available online at www.thieme.com/bns.

Siga-nos: Facebook/ThiemeRevinter
UNICAMPSEMIOLOGIA NEUROLÓGICA
Sem dúvida, o mais completo livro brasileiro do gênero! Mais de 500 páginas, com 258 fotos e ilustrações, distribuídos em
24 capítulos, auxiliam o entendimento de complexos conceitos para uma minuciosa avaliação neurológica. Através de um
arsenal de manobras e testes, que carregam conceitos e elementos singulares, os autores conduzem o leitor aos
diagnósticos topográficos mais precisos. Apresenta capítulos nunca antes abordados, como Semiologia Cefaliátrica,
Refinamentos em Neuro-Oftalmologia, Exame Otoneurológico, Semiologia dos Distúrbios do Sono, Refinamentos em
Exame Neuromuscular, Refinamentos nos Distúrbios do Movimento, dentre outros.
584 Páginas – Papel Couché
Formato 16 x 23 cm
Brochura – Peso 1.240g
Ricamente Ilustrado
ISBN: 978-85-372-0691-1
Ano de Lançamento: 2017
Especialidades: Neurologia
Preço: R$ 198,99
Carlos Roberto Martins Jr.
Marcondes C. França Jr.
Alberto R. M. Martinez
Ingrid Faber
Anamarli Nucci
RE1
72
7
ADQUIRA JÁ EM http://www.thiemerevinter.com.br

ADQUIRA JÁ EM http://www.thiemerevinter.com.br
Siga-nos: Facebook/ThiemeRevinter
Inovação e integração
Esta obra proporciona um texto atualizado aos cursos de Medicina, Fisioterapia e Terapia Ocupacional, aos neurologistas e aos médicos em geral. Utiliza, ainda, as conquistas científico-tecnológicas, em especial a neuroimagem, uma inovação, facilitando o ensino da Neuroanatomia na aplicação clínica. O propósito deste livro é integrar a Neuroanatomia, a Neurologia e as clínicas relacionadas com transtornos do Sistema Nervoso. Os primeiros capítulos enfocam a Neuroanatomia básica da medula ao telencéfalo, com desenhos simplificados, incluindo o circuito e a chave dos sistemas neurotransmissores. Esta maneira de apresentar a exposição do texto facilita a memorização, a compreensão e o aprendizado das vias ascendentes, das vias descendentes e das grandes síndromes neurológicas. As ilustrações do desenhista Gabriel e fotos ajudam a compreensão, despertando grande interesse devido às aplicações clínicas, sem necessitar do uso de atlas.
184 Páginas – Papel Couché
Formato 21 x 28 cm
Brochura
Ricamente Ilustrado em 4 Cores
ISBN: 978-85-372-0637-9
Ano de Lançamento: 2015
Especialidades: Neurologia
Preço: R$ 102,99
Marco Antônio Rocha
Marco Antônio Rocha Júnior
Cristiane Franklin Rocha
RE1
65
8

Endoscopic Sural Nerve Removal in ObstetricBrachial Plexopathy Using Basic EndoscopyInstruments: Technical Note
Retirada endoscópica do nervo sural na plexopatiabraquial obstétrica utilizando instrumentos básicos deendoscopia: nota técnica
José Augusto Malheiros1,2 Sérgio Augusto Vieira Cançado1 João Tiago Alves Belo1
Luiz Alberto Otoni Garcia1 Marcelo Magaldi de Oliveira2 Martjin J. A. Malessy3
1Neurological and Neurosurgery Clinic, Hospital Felício Rocho -Fundação Felice Rosso, Belo Horizonte, MG, Brazil
2Neurosurgery Department, Hospital das Clínicas, UniversidadeFederal de Minas Gerais (HC-UFMG), Belo Horizonte, MG, Brazil
3Department of Neurosurgery, Leids Universitair Medisch Centrum,Leiden, Netherlands
Arq Bras Neurocir 2017;36:75–79.
Address for correspondence José Augusto Malheiros, MD, PhD,Departamento de Neurocirurgia do Hospital das Clínicas daUniversidade Federal de Minas Gerais (HC-UFMG), Av. do Contorno,9530. 2o andar., Belo Horizonte, MG, CEP 30110-934, Brasil(e-mail: [email protected]).
Keywords
► sural nerve► endoscopy► brachial plexus
Abstract Introduction The sural nerve (SN) is commonly used for grafting following resection of aneuroma-in-continuity in neonatal brachial plexus lesions (NBPL). The main drawbacks ofthe current open techniques are large scars and contractures in the late postoperativestage, which may, in severe cases, cause equinovarus contractures.Objective To describe the feasibility and the technical aspects of endoscopic SNharvesting with the use of basic endoscopy instruments and small incisions.Methods Prospective observational study of NBPL subjected to endoscopic nerveharvesting between February of 2012 and February of 2014 in a consecutive series.Patients were operated at the Felício Rocho Hospital (Hospital Felício Rocho) and theClinical Hospital, Federal University of Minas Gerais (Hospital das Clínicas UFMG), BeloHorizonte/MG, in Brazil. The study outcomes assessed were: scar size, presence orabsence of contractures in the calf, bleeding volume (measured by the number ofgauzes used) and number of incisions. Only patients with a follow-up longer than6 months were included.Results Seven patients were selected and twelve endoscopic nerves were endoscopi-cally harvested. The average surgery time was 45 minutes. Nine SNs were harvestedthrough two incisions, and three nerves through three incisions. The estimatedbleeding was less than 5ml and there were no complications or contractures duringthe follow-up period of 6 months to 4 years.
receivedFebruary 28, 2017acceptedMay 2, 2017
DOI https://doi.org/10.1055/s-0037-1603966.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 75

Introduction
The sural nerve (SN) is commonly used for grafting followingresection of a neuroma-in-continuity in neonatal brachialplexus lesions (NBPL).1,2 Generally, the entire length of theSN is used, which involves large incisions or incisions inmultiple steps between the ankle and the popliteal fossa.3–5
The main drawbacks of the current open techniques arelarge scars and contractures in the late postoperative stage,whichmay, in severe cases, cause equinovarus contractures.5,6
Other disadvantages related to this technique are the higherintraoperative blood loss, lack of temperature control andpostoperative pain and wound infections.
Here we describe the feasibility and technical aspects ofSN harvesting with the use of basic endoscopy instrumentsand small incisions.
Methods
This was a prospective observational study of patients withNBPL subjected to endoscopic nerve harvesting betweenFebruary of 2012 and February of 2014 in a consecutiveseries. The patients were operated at two institutions in thestate of Minas Gerais, Brazil. The study outcomes assessed
were: scar size, presence or absence of contractures in thecalf, bleeding volume (measured by the number of gauzesused) and number of incisions. Only patients with a follow-up longer than 6 months were included.
Instruments Used
– Pediatric cystoscope (Karl Storz, Tuttlingen, Germany),thirty-degree lens, 2.7 mm in diameter and 17.5 cm inlength.
– Nasal speculum numbers 2 (5 cm) and 3 (7 cm).
Technique of Endoscopic Sural Nerve Harvesting
1) Placement of an arch on the operating table to positionthe lower limbs for endoscopy and fixation of the lowerlimbs onto the arch with sterile tape (►Fig. 1).
2) Ankle incision and SN repair with silicone tape (►Fig. 2A).3) Preparation of endoscopy instruments: rigid thirty-de-
gree endoscope and two nasal specula (short and long)(►Fig. 2B).
4) Dissection of a tunnel to introduce the nasal speculumthat will be the endoscopic working channel (►Fig. 2C).
5) Introduction of the endoscope and dissection of the suralnerve (►Fig. 2D).
Conclusion Sural nerve harvesting in children with NBPL is feasible and it offers theadvantage of needing only twoor three small incisions using basic endoscopy instruments.
Resumo Introdução O nervo sural é a melhor opção para enxertia nas reconstruções microci-rúrgicas da plexopatia braquial obstétrica. O método clássico aberto com incisãolongitudinal desde o tornozelo até a fossa poplítea ou em incisões em degraus possuemas desvantagens de cicatrizes amplas e contraturas em equinovarus (pé torto).Atualmente, o emprego de endoscópios específicos para a retirada de enxertia denervos e vasos mostra resultados satisfatórios em relação ao encurtamento do tempocirúrgico e à redução no tamanho das incisões, mas tem como inconveniente o altocusto de aquisição e manutenção.Objetivo Discutir a viabilidade e descrever nota técnica da retirada do nervo suralutilizando instrumental básico de endoscopia e pequenas incisões.Métodos Estudo observacional prospectivo em pacientes com plexopatia braquialobstétrica submetidos a retirada do nervo sural por endoscopia no período de fevereirode 2012 a fevereiro de 2014 no Hospital Felicio Rocho e no Hospital das Clinicas UFMG,Belo Horizonte/MG, Brasil.Resultados Sete pacientes foram selecionados e foram retirados doze nervos suraispor endoscopia. O tempo médio da cirurgia foi de 45 minutos. Nove nervos suraisforam retirados por duas incisões, e três nervos foram retirados por três incisões. Osangramento foi inferior a 5ml e não houve complicações no pós-operatório imediato etardio em acompanhamento entre 6 meses e 4 anos. Não foram observadas contra-turas no período observacional.Conclusão O nervo sural pode ser retirado utilizando duas ou três pequenas incisõespor meio de instrumental endoscópico básico em crianças com plexopatia braquialobstétrica.
Palavras-chave
► nervo sural► endoscopia► plexo braquial
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Endoscopic Sural Nerve Dissection Malheiros et al.76

6) Endoscopic SN microdissection, which begins withseparation of the sural nerve from the small saphenousvein (►Fig. 3A and B).
7) Release of the SN and incision of the gastrocnemiusmuscle fascia (►Fig. 3C). Exchange of the short speculumfor a long speculum.
8) Incision at the back of the leg, using the tip of theendoscopic speculum as a reference, and dissection tothe endoscopic working area.
9) Passing of the silicone repair tape from the nerve via theendoscopy tunnel to the incision at the back of the leg.
10) Repositioning of the nasal speculum through the newincision and reintroduction of the endoscope withmicrodissection in the popliteal fossa.
11) Externalization of the SN and suturing by planes. Depend-ingon thedegreeof releaseof theSN fromthefascia, oneortwo incisions can be made (►Fig. 3D and E).
Results
During the period of 2012–2014, seven cases of obstetricplexopathy were selected for endoscopic SN harvesting.
In two patients, only one SN was harvested. In the otherfive patients, both SNs were removed, for a total of 12endoscopically harvested SNs.
Themean harvesting time of each SNwas 45minutes. Themaximum timewas 65minutes, whereas theminimum timewas 35 minutes.
Nine SNs were harvested using only two incisions.Three SNs were harvested through three incisions.The mean incision size was 20 mm, with a minimum sizeof 15 mm and a maximum size of 26 mm.Only one gauze was used during the harvesting of two
SNs. In the case of one patient, only one gauze was used foreach SN.
Discussion
The SN is the best graft source in NBPL reconstructions.1,2,6
The SN is placed between the proximal stumps (cervical root)and distal stumps (trunk divisions) after neuroma’s removal(►Fig. 4). The classical sural harvesting techniques, whichinclude a longitudinal incision from the ankle to the poplitealfossa or incisions in multiple steps (with transverse inci-sions), have the disadvantage of greater blood loss and largescars that may cause contractures and deformities of theequinovarus type.6,7
The endoscopic technique was developed to minimizesurgical trauma, decrease the skin incision size and, there-fore, decrease the likelihood of lower limb deformities.5–7
Endoscopic techniques have been widely used in theharvesting of the saphenous vein and the radial artery forvascular surgeries with the advantages of minimal scars andless postoperative complications, such as hypersensitivity ofthe skin, scars and infections.8,9
Fig. 1 Patient positioning for the endoscopic procedure. The feet arefixed on the arch with adhesive tape or bandaging.
Fig. 2 Initial step of the endoscope procedure. (A) Macroscopic dissection and repair of the sural nerve with silicone tape. (B) Instruments usedfor the endoscopic procedure. (C) Introduction of the short speculum into the ankle incision. (D) Introduction of the endoscope through thetunnel formed by the speculum.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Endoscopic Sural Nerve Dissection Malheiros et al. 77

There is now the option of harvesting the SN endoscopi-cally, with only one incision, using the same endoscopicinstruments as in vascular surgery.5
This system, namely Guidant VasoView Uniport Plus(Guidant Corp., Indianapolis, IN, USA) optimizes SNharvesting,requiring only one 12–13 mm incision and a mean operativetime of 20 minutes.5,6 The greatest drawback of this device is
the high cost of purchase and maintenance, which makes itimpractical in large Brazilian hospital centers. In this context,this study contributes to the literature by describing an endo-scopic technique using ordinary and low-cost instruments. Toourknowledge, thiswas thefirst Brazilian article todescribe anendoscopic technique of SN harvesting in infants.
The advantages of the endoscopic technique described inthe literature in relation to the classical technique were alsoobserved in this study. In infants, this has an effect that shouldbe considered because it reduces harm to the child by decreas-ing the heat loss caused by larger incisions; it involves lessblood loss; itoffersbettercosmetic results and it also involvesalower likelihood of equinovarus contractures.6,7
In thefirstcases,wehadtriedtouseazero-degreeendoscope,but it was much more cumbersome than using a thirty-degreeendoscope. Therefore, a thirty-degree cystoscopic lenswas usedfor theprocedure, but anyshort and thinendoscope canbeused.Blood losswasminimalandestimatedat less than5ml (less thanone gauze); therewas no change in body temperature, and all ofthe patients were discharged after less than 48 hours of hospi-talization. Long-term monitoring of patients showed no con-tractures or deformities of the lower limbs, and long-termscarring was almost unnoticeable (►Fig. 3G).
The greatest drawback of the technique described in thisstudy and of the endoscopic technique using this particulardevice was the longer duration of the surgery (45 minutesversus 20 minutes) and the number of incisions (2 or 3 versus
Fig. 3 Endoscopic steps for dissection of the sural nerve. (A and B) Initial dissection of the sural nerve from the small saphenous vein. (C) Incisionof the gastrocnemius muscle fascia. D and E – Sural nerve externalization using three (D) or two incisions (E). (F) Final appearance after suture.(G) Healing four years after the procedure (asterisk ¼ sural nerve; v ¼ small saphenous vein).
Fig. 4 Intraoperative photo of brachial plexus reconstruction using asural nerve graft after removal of the neuroma. In this case, there wasa neuroma in the upper trunk that was resected. Several sural nervefascicles were made that were grafted (�sural nerve as a graft betweenthe C5 root and anterior division (AD); �sural nerve being prepared forgrafting between C5 and posterior division).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Endoscopic Sural Nerve Dissection Malheiros et al.78

one incision).5,6 These differences, however, did not alter themain benefits of the endoscopic technique in regard to theamount of bleeding and final aesthetic results in the short andlong term.
Special Thanks
Special thanks to the neurosurgery team from Leiden,Netherlands, where the first author of this article performedtraining as an observer and was able to adapt such anendoscopic technique in Brazil.
Conclusion
Sural nerve harvesting in childrenwith NBPL is feasible and itoffers the advantage of needing only two or three smallincisions made with basic endoscopy instruments.
References1 van Vliet AC, TannemaatMR, vanDuinen SG, Verhaagen J, Malessy
MJ, De Winter F. Human Neuroma-in-Continuity Contains Focal
Deficits in Myelination. J Neuropathol Exp Neurol 2015;74(09):901–911
2 Malessy MJ, Pondaag W. Obstetric brachial plexus injuries. Neu-rosurg Clin N Am 2009;20(01):1–14, v
3 Lapid O,Ho ES, Goia C, ClarkeHM. Evaluation of the sensory deficitafter sural nerve harvesting in pediatric patients. Plast ReconstrSurg 2007;119(02):670–674
4 Ramakrishnan PK, Henry BM, Vikse J, et al. Anatomical variationsof the formation and course of the sural nerve: A systematicreview and meta-analysis. Ann Anat 2015;202:36–44
5 Park SB, Cheshier S, Michaels D, Murovic JA, Kim DH. Endoscopicharvesting of the sural nerve graft: technical note. Neurosurgery2006;58(1, Suppl)E180, discussion E180
6 Spinks TJ, Adelson PD. Pediatric sural nerve harvest: a fully endo-scopic technique. Neurosurgery 2009;64(05, Suppl 2):360–363,discussion 363–364
7 Strauch B, Goldberg N, Herman CK. Sural nerve harvest: anatomyand technique. J Reconstr Microsurg 2005;21(02):133–136
8 Vitali RM, Reddy RC, Molinaro PJ, Sabado MF, Jacobowitz IJ. Hemo-dynamic effects of carbon dioxide insufflation during endoscopicvein harvesting. Ann Thorac Surg 2000;70(03):1098–1099
9 Navia JL, Brozzi N, Chiu J, et al. Endoscopic versus open radialartery harvesting for coronary artery bypass grafting. J CardiovascSurg (Torino) 2012;53(02):257–263
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Endoscopic Sural Nerve Dissection Malheiros et al. 79

Glioblastoma Multiforme: an Advanced Analysisof 153 Patients and Review of the Literature
Glioblastoma Multiforme: uma análise avançada de 153pacientes e revisão da literatura
Mohammad Sadegh Nikdad1,2 Farshid Farhan3 Milad Shafizadeh1,2 Atefeh Sadat Mirmohseni1,2
Mohsen Afarideh1,2 Shabnam Asadi Komeleh1,2 Marzieh Lashkari3 Morsaleh Ganji1,2
Alireza Ghajar1,2 Saeed Shafiei1,2 Yalda Shafizadeh4 Ali Kazemian3 Hooshang Saberi1,2
1Neurosurgery Research Center, Tehran University of MedicalSciences, Tehran, Iran
2Department of Neurosurgery, Tehran University of Medical Sciences,Tehran, Iran
3Department of Radiation Oncology, Cancer Institute, TehranUniversity of Medical Sciences, Tehran, Iran
4Department of Pathology and Laboratory Medicine, EmoryUniversity School of Medicine, Atlanta, GA, USA
Arq Bras Neurocir 2017;36:80–90.
Address for correspondence Farshid Farhan, MD, Department ofRadiation Oncology, Cancer Institute, Tehran University of MedicalSciences, P.O. Box: 14155-6447, Tehran, Iran(e-mail: [email protected]).
Keywords
► glioblastomamultiforme
► survival► local recurrence
Abstract Objective Glioblastoma multiforme (GBM) is an aggressive primary tumor withfrequent recurrences that leaves patients with a short survival time and a low qualityof life. The aim of this study was to review the prognostic factors in patients withglioblastoma multiforme.Material and Methods The focus of this retrospective study was a group of 153patients with supratentorial GBM tumors, who were admitted to a tertiary-care referralacademic center from 2005 to 2013. The factors associated with survival and localrecurrence were assessed using the hazard ratio (HR) function of Cox proportionalhazards regression and neural network analysis.Results Outof the153patients, 99 (64.7%)weremale. Theaverageageof thepatientswas55.69 � 15.10 years. The median overall survival (OS) and progression-free survival (PFS)rateswere 14.0 and7.10months respectively. In themultivariate analysis, age (HR ¼ 2.939,p < 0.001), operative method (HR ¼ 7.416, p < 0.001), temozolomide (TMZ, HR¼ 11.723, p < 0.001), lomustine (CCNU, HR ¼ 8.139, p < 0.001), occipital lobe involve-ment (HR ¼ 3.088, p < 0.001) and Karnofsky Performance Status (KPS, HR ¼ 4.831,p < 0.001) scores were shown to be significantly associated with a higher OS rate.Furthermore, higher KPS (HR ¼ 7.292, p < 0.001) readings, the operative method (HR¼ 0.493, p ¼ 0.005), the use of CCNU (HR ¼ 2.047, p ¼ 0.003) and resection versuschemotherapy (HR ¼ 0.171, p < 0.001) were the significant factors associated with thelocal recurrence of the tumor.Conclusion Our findings suggest that the use of CCNU and TMZ, the operativemethod and higher KPS readings are associated with both higher survival and lowerlocal recurrence rates.
receivedDecember 30, 2016acceptedMarch 16, 2017published onlineMay 22, 2017
DOI https://doi.org/10.1055/s-0037-1603199.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original Article | Artigo Original80

Introduction
With an annual incidence rate of 3 to 4 cases per 100,000persons1, glioblastoma multiforme (GBM) is by far the mostcommonmalignant primary tumor of the brain in adults. Theoverall incidence of primary malignant brain tumors isreported to be around 2.74 per 100,000 persons in Iran.2
Patientswith GBMhave a short survival term, and frequentlypresent with tumor recurrence; therefore, an effective man-agement of these patients is crucial. The longest reportedsurvival terms, despite aggressive therapy, are lower thantwo years.3–9 Aggressive therapies, including surgery, che-motherapy and radiation are not only costly, but bear addi-tional complications.10–12Nearly all patients with GBM havea poor quality of life, and health related quality of life(HRQoL) is defined as a multidimensional concept coveringphysical, psychological, and social domains, as well as symp-toms induced by the disease and its treatment.13 Treating thetumor is intensive and time-consuming, and treatmentcomplications, as well as tumor recurrences, are common.Effective treatment will improve the patients’ performancestatus14, neurocognitive function15, overall quality of life16
and overall survival.4,17–19 In addition, the effective treat-ment will also improve the psychological health of thepatients. Achieving high quality of life in patients withGBM requires the cooperation of various specialists, andcertain loss of quality of life is intrinsic to cancer patients.However, one should identify and target the factors that will
help the radiotherapists, oncologists, and neurosurgeonsimprove the overall survival of the patients without therecurrence of the tumor.
Our study assesses the factors that are associated withprolonged survival, improved quality of life and reducedtumor recurrence in patients with GBM.
Material and Methods
Patient SelectionA total of 153 patients with supratentorial GBM tumors wereadmitted to a referral tertiary academic center between 2005and 2013 at a hospital in Tehran, Iran. In all cases, the GBMpatientswere diagnosedwith the pathology, as confirmed bytwo senior neuropathologists, and the grading criteria wasbased on the classification system of the World HealthOrganization (WHO).20,21 Patients at any age with a tissue-proven diagnosis of supratentorial GBM (WHO Grade IV)were included in the study. Patients who had serious con-comitant malignant or chronic diseases, and patients withinfratentorial gliomas and prior lower grade gliomas wereexcluded from the analysis to create a more uniform patientpopulation.
Apart from the research’s objectives, all patients receivedvarious management procedures depending on their pre-operative assessment and on necessity indicators. Addition-ally, all patients were followed-up after undergoing thetreatment.
Palavras-chave
► glioblastomamultiforme
► sobrevida► recorrência local
Resumo Objetivo Glioblastoma multiforme (GBM) é um tumor primário agressivo comrecorrências frequentes que deixam pacientes com uma curta sobrevida e baixaqualidade de vida. O objetivo deste estudo é rever fatores de prognóstico em pacientescom glioblastoma multiforme.Material e Métodos O foco deste estudo retrospectivo foi um grupo de 153 pacientescom tumores GBM supratentoriais, os quais deram entrada em um centro acadêmicode atendimento de referência de 2005 a 2013. Fatores associados com a sobrevivênciae a recorrência local foram avaliados usando a razão de risco (RR) da regressão de riscoproporcional de Cox e análise de redes neurais.Resultados Dos 153 pacientes, 99 (64,7%) eram homens. A média de idade foi de55,69 � 15,10 anos. A sobrevida geral (SG) mediana e a sobrevida de livre progressão(SLP) foram 14,0 e 7,10 meses, respectivamente. Na análise multivariada, idade(RR ¼ 2,939, p < 0,001), método operatório (RR ¼ 7,416, p < 0,001), temozolomida(TMZ, RR ¼ 11,723, p < 0,001), lomustina (CCNU, RR ¼ 8,139, p < 0,001), envolvi-mento do lobo occipital (RR ¼ 3,088, p < 0,001) e Índice de Desempenho deKarnofsky (IDK, RR ¼ 4,831, p < 0,001) foram identificados como significativamenteassociados a uma SG maior. Além disso, leituras maiores de IDK (RR ¼ 7,292,p < 0,001), o método operatório (RR ¼ 0,493, p ¼ 0,005), o uso de CCNU (RR¼ 2,047, p ¼ 0,003) e ressecção versus quimioterapia (RR ¼ 0,171, p < 0,001) foramfatores significativos associados à recorrência local de tumor.Conclusão Nossos resultados sugerem que o uso de CCNU e TMZ, o métodooperatório e leituras maiores de IDK estão associados tanto à maior sobrevida quantoà menor recorrência local.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al. 81

Recorded VariablesThe clinical, operative, and hospital course records of thepatients who met the inclusion and exclusion criteria wereretrospectively reviewed. The information was collectedfromneurosurgery and radiotherapy clinical notes, includingthe patients’ demographics, presenting symptoms, neuro-logical function and neurologic signs, as well as the neuro-imaging perioperative course and the adjuvant therapy. TheKarnofsky Performance Status (KPS) scale was used to speci-fy the patients’ preoperative functional status.22 The KPSscores were collected during a physical examination byoncologists who were blind to the outcomes of the patientsat the clinical visit, and prior to surgery. Preoperative sensorydeficit was defined as decreased sensation to any stimulant.Motor deficit was defined as decreased force, as identified bya clinician during a physical examination. Language deficitwas defined as any combination of receptive or expressiveaphasia. Finally, cognitive deficits were defined as confusionor memory loss. The magnetic resonance imaging (MRI)characteristics were recorded, including the specific lobelocation and eloquent brain involvement. This assessmentwas based on radiographic, not clinical, criteria. Unfortu-nately, the sizes of the lesions were not registered in therecords. The geometric estimation of the volume of theresected tumor was based on the comparison of the en-hanced tumor margin in the gadolinium-enhanced T1-weighted sequences of pre-op MRIs with those of post-opMRIs obtained less than 48 hours after tumor resection. Theresections were then defined as either gross total resections(GTRs; > 99% resection) or subtotal resections (STR; 90–99%resection) by an independent neuroradiologist who wasblind to the outcomes of the patients. The patients whounderwent biopsies were not classified as having undergonea resection. The date of death was recorded for any patientwhose record was available in the hospital records. Timeuntil death was defined as the time from the initial glioblas-toma diagnosis (with the pathology) until death. Patientswhose deathswere unconfirmedwere classified as lost to thefollow-up at the time of the last clinic visit. The concepts ofstable disease, local recurrence and progression were de-fined according to the Response Assessment in Neuro-oncol-ogy (RANO) criteria. Briefly, the RANO criteria are based onthe evaluation of the product of the maximal cross-sectionaldiameters of an enhancing lesion in the post-gadoliniumenhanced T1-weighted MRI and/or T2-weighted /flair se-quences before and 4 weeks after surgery. Depending onmeeting a complex criteria comprised of the following, (i)postoperative radiographic assessment of tumor size basedon the extent of the preoperative involvement (that is,disappearance, reduction or progression of all measurableand non-measurable lesions on gadolinium-enhanced T1-weighted images in addition to stable, regressing, or pro-gressing tumor size in the T2-weighted/flair images), (ii)clinical status (stable, improved, or deteriorated condition),(iii) the use of corticosteroids (that is, none, stable/decreasedor increased [conditional] dosage ofmedication), and (iv) thepresence of new lesions (that is, none or present); thepatients with glioblastoma were divided into 4 categories:
“complete response,” “partial response,” “stable disease” or“progressive disease.” For the present manuscript, thegroups of patients with “complete response” and “partialresponse” on the RANO criteria were designated as having a“stable disease”, and the group of patients with “stablediseases” and “progressive diseases” on the RANO criteriawere defined as having “local recurrence.”
Perioperative TreatmentAll patients had been visited by neurosurgeons and radiationoncologists before surgery. The general aim of the neurosur-geons was to achieve GTR of the tumor when possible.Subtotal resection was achieved primarily when the tumorinvolved eloquent brain as confirmed by intraoperativemapping and/or monitoring, and surgical navigation (com-puted tomography [CT] and/or MRI wand) was used in allcases. Implant therapy was not performed in any of thepatients. Radiation oncologists treated all the patients with60 Gy 2-dimensional or 3-dimensional radiotherapy in 30fractions. The patients were prescribed 6 sessions of adju-vant chemotherapy with 150 mg/m2 over 5/28 days in 6cycles of the first-line agent temozolomide (TMZ) in additionto the concurrent chemotherapy with 75 mg/m2/day TMZ 1hour prior to radiotherapy. A total of 6 cycles of 110mg/m2
lomustine (CCNU) adjuvant chemotherapywas performed asthe second-line agent because of inaccessibility to TMZ dueto the cost of it and the lack of insurance coverage. Althoughprocarbazine, CCNU and vincristine (PCV) remain the salvagechemotherapy regimen in patients with high-grade glio-mas,23 the alternative agent CCNU was used as an adjuvantchemotherapy regimen in this group of patients because ofthe lower complication rates, better tolerability and compa-rable survival rate to the use of PCV in our country.24
In this study, many patients were denied surgery orchemotherapy options, or both, because of the inability ofthe patients or their families to pay for the treatments.Therefore, apart from the study’s objectives, some patientswere treated depending on their preoperative assessmentand based on necessity indicators depending on standardtreatment options,25,26 and some patients received incom-plete treatments perforce. The decision involved input from asurgeon, a radiation oncologist and the patients themselves.Recurrent tumors were usually discovered on follow-upvisits via postoperative MRI performed at 3-month intervalsfollowing surgery, or at the time that any symptomsdeveloped.
Statistical AnalysisAll analyses were performed using the Statistical Package forthe Social Sciences (SPSS, IBM Corp. Armonk, NY, US) soft-ware, version 20. Summary data was presented as mean �standard deviation (SD) for parametric data, and nonpara-metric data, as median (interquartile range [IQR]). For theintergroup comparison, the Student’s t-test was used forparametric data, and the Mann-Whitney U-test was usedfor nonparametric data. The percentages were comparedusing the chi-square test or Fisher’s exact test where appro-priate. Survival as a function of time was plotted using the
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al.82

Kaplan-Meier method. Moreover, log-rank analysis was usedto compare the Kaplan-Meier plots. The factors associatedwith overall survival were assessed using the Cox propor-tional hazard regression models for multivariate associa-tions. For this purpose, all variables associated with survivalin the univariate analysis (p < 0.10) were included.
The factors predicting the outcomes of survival and localrecurrence were separately analyzed using the neural net-work analysis. For this purpose, two models for neuralnetwork analyses were developed to firstly predict thesurvival and secondly to predict local recurrence usingselected baseline characteristics of the patients.
The analysis of a neural network uses a learning algorithmto define the nonlinear mathematical transfer functions tomodify the synaptic weights of a network’s processing unitsin an orderly fashion to obtain the desired outcome predic-tion (training datasets). Both theweights and the value of theactivation functions can be adjusted during the training of anartificial neural network. However, this is impractical, as itwould be simpler to only adjust for a single parameter. Tosurpass this problem, the bias neuron is generated. The biasneurons in layer 1 are connected to all the neurons in thefollowing layer, but with none of the neurons present in theprevious layer. The hidden layer contains unobservablenetwork nodes (units). Each hidden unit is a function oftheweighted sum of the inputs. It is similar to the correlationcoefficient in the linear regression model. In all subsequentanalyses, values of p < 0.05 were considered statisticallysignificant.
Results
Preoperative, Perioperative and PostoperativeCharacteristics of the PatientsAmong the 155 patients diagnosed with supratentorial pri-mary GBM, 153met the eligibility criteria andwere includedin the analysis. The pre-, peri- and postoperative charac-teristics of these 153 patients (99 men, 64.7% of the totalstudy population) are summarized in ►Table 1. The mean� SD age of the patients was 55.69 � 15.10 years at the timeof the diagnosis. In total, 40 patients (26.1%) were youngerthan 45 years, 88 patients (57.5%) were between 45 and 70years old, and 25 patients (16.3%) were older than 70 years ofage. Themedian preoperative KPSwas 60 (IQR: 50–80, range:20–100). A total of 52 patients did not express any neurologicsymptoms at their consultations. Among 101 patients withneurologic signifiers, the major symptoms presented aredescribed in declining order: seizures in 36 patients(23.5%); motor deficits in 21 patients (13.7%); sensory andlanguage deficits in 15 patients (9.8%); visual deficits in 9patients (5.9%); and cognitive deficits (memory loss/confu-sion) in 5 patients (3.3%). The median duration of thesymptoms was 2 months prior to the diagnosis of thepathology. A total of 81 tumors (52.9%) were found in theright hemispheres, with the remainder involving the lefthemispheres. Ninety-four tumors (61.4%) involved only 1brain lobe, while all other tumors involved 2 brain lobes.Twenty-nine tumors (19.0%) involved the frontal lobe, 37
tumors (24.2%), the parietal lobe, 18 tumors (11.8%), thetemporal lobe, 8 tumors (5.2%), the occipital lobe, 24 tumors(15.7%), the temporoparietal lobe, 16 tumors (10.5%), theparieto-occipital lobe and 21 tumors (13.7%) involved otherareas. A total of 60 patients (39.2%) underwent biopsy, 91patients (59.5%) underwent near total resection (NTR) orSTR, and only 2 patients (1.3%) underwent GTR. There wereno cases of perioperative mortality. Radiotherapy was per-formed in all patients (100%) with a median dose of 60 Gy in30 fractions. A total of 100 patients (94.8%) underwent 2-dimensional radiotherapy, whereas 8 patients (5.2%) under-went 3-dimensional radiotherapy. Of the 153 patients, 78(51%) underwent only radiotherapy, 57 (37.3%) underwentadjuvant chemotherapy, and 18 (11.8%) underwent concur-rent þ adjuvant chemotherapy. Concurrent þ adjuvant che-motherapy was performed using TMZ. Among the 75patients who underwent chemotherapy, TMZ was adminis-tered to 39 (25.5%), and CCNU was administered to 36(23.5%). At the last follow-up, 136 (88.9%) patients haddied, 10 patients (6.5%) were alive, and 7 patients (4.6%)did notmake appointments, and had an unknown status. Themedian follow-up time for the surviving patients was 14months (IQR: 10–20 months). The median overall survivalrate of the patients was 14 months (IQR: 9–17 months). Themedian survival rates at 3, 6, 9, 12, 18, 24 and finally, 32months of the patients in this studywere 98.0%, 85.6%, 70.5%,55.5%, 22.8%, 15.6% and 5.8% respectively. The patients weredivided into certain categories tomatch case and controls forbetter analysis (►Table 2).
Factors Independently Associated with Survival
Univariate AnalysisWe investigated the factors associated with the overallsurvival and progression-free survival using the Kaplan-Meier analysis. We found that age (p ¼ 0.005), confusionand/or memory loss (p < 0.001), CCNU (p < 0.001), TMZ(p < 0.001), KPS (p < 0.001), operative method (p < 0.001),TMZversusCCNU (p ¼ 0.007), 2Dversus3D radiationprotocol(p < 0.001), frontal lobe involvement (p ¼ 0.009) and localrecurrence (p < 0.001)hadvarious degrees of impacts onboththe overall survival and progression-free survival rates of ourpatients with glioblastoma multiforme (►Table 3).
Multivariate AnalysisAll variables associated with survival in the univariate analy-sis (p < 0.10) and clinically important variables were includ-ed in themultivariate proportional hazards regression model.We found that age (hazard ratio [HR] [95% CI (confidenceinterval)], 2.939 [1.73–4.99], p < 0.001), operative method(HR [95% CI], 7.416 [3.81–14.42], p < 0.001), TMZ (HR [95%CI], 11.723 [5.46–25.13], p < 0.001), CCNU (HR [95% CI],8.139 [4.04–16.38], p < 0.001), occipital lobe involvement(HR [95% CI], 3.088 [1.81–5.25], p < 0.001) and KPS (HR [95%CI], 4.831 [3.00–7.77], p < 0.001) had various degrees ofimpact on both the overall survival and progression-freesurvival rates of our patients with glioblastoma multiforme(►Table 4).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al. 83

Neural Network AnalysisThe variables with the greatest impact on the survival rate ofthe included patients were considered for the neural net-work analysis (input variables for the outcome of survival:age, occipital lobe involvement, KPS, operative method andthe use of CCNU and TMZ). We found the importance of thevariables to predict survival in the following declining order:KPS ¼ 30.6%, operative method ¼ 20.4%, TMZ ¼ 17.0%,CCNU ¼ 15.0%, age ¼ 13.5%, and occipital lobe involvement¼ 3.6% (►Fig. 1). In this model, four hidden layers and onebias neuron were germane to the calculation.
Factors Independently Associated with LocalRecurrence
Univariate AnalysisOut of the 153 patients, 115 (75.2%) had one local recurrence.We analyzed the factors associated with local recurrenceusing the Kaplan-Meier analysis that defined time asprogression-free survival, and status as occurrence oflocal recurrence. We found that CCNU (p < 0.001), TMZ(p ¼ 0.003), chemotherapy versus resection (p < 0.001), op-erative method (p ¼ 0.016) and KPS (p < 0.001) were eachassociated with local recurrence.
Multivariate AnalysisWeidentifiedthefactorsassociatedwith local recurrenceusingthe Cox regression model analysis that defined time as pro-gression-free survival and status as occurrence of local recur-rence. All variables associated with survival in the univariateanalysis (p < 0.10), aswellas theclinically important variables,
Table 1 pre-, peri- and postoperative characteristics of thepatients
Study population! N ¼ 153
Characteristics N (percent)
Age (mean � SD) 55.69 � 15.10
Male 99 (64.7%)
Preoperative factors
KPS > 60 48 (31.4%)
KPS ¼ 60 62 (40.5%)
40 < KPS < 60 35 (22.9%)
KPS < 40 8 (5.2%)
Neurologic sign 101 (66.0%)
Confusion/memory loss 5 (3.3%)
Language deficit 15 (9.8%)
Motor deficit 21 (13.7%)
Sensory deficit 15 (9.8%)
Seizure 36 (23.5%)
Visual deficit 9 (5.9%)
Mass location
Right hemisphere 81 (52.9%)
Frontal lobe 29 (19.0%)
Parietal lobe 37 (24.2%)
Temporal lobe 18 (11.8%)
Occipital lobe 8 (5.2%)
Temporoparietal lobes 24 (15.6%)
Others 37 (24.2%)
Perioperative factors
Operative method
Biopsy 60 (39.2%)
Total and near totalresection
93 (60.8%)
Chemoradiation plan
Radiotherapy 78 (51.0%)
Radiotherapy þ adjuvantchemotherapy
57 (37.2%)
Radiotherapy þ concurrentchemotherapy þ adjuvantchemotherapy
18 (11.8%)
Chemotherapy drugs
TMZ 39 (25.5%)
CCNU 36 (23.5%)
Radiation method
2D 145 (94.8%)
3D 8 (5.2%)
Postoperative factors
Died at last follow-up, n 136 (88.9%)
Table 1 (Continued)
Study population! N ¼ 153
Characteristics N (percent)
Follow-up months (range) 49 (3–49)
Median survival (months) 14.0
Mean survival (months) 15.34 � 9.63
3-month survival rate 98.0%
6-month survival rate 85.6%
9-month survival rate 70.5%
12-month survival rate 55.5%
18-month survival rate 22.8%
24-month survival rate 15.6%
32-month survival rate 5.8%
Recurrence
Tumor recurrence, n 115 (75.2%)
progression-free survival(median)
7.1
Abbreviations: 2D, two-dimensional; 3D, three-dimensional; CCNU,lomustine; KPS, Karnofsky Performance Status; TMZ, temozolomide.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al.84

were included in themultivariate proportional hazards regres-sionmodel. We found that the operative method (HR [95% CI],0.493 [0.30–0.80], p ¼ 0.005), CCNU (HR [95% CI], 2.047 [1.27–3.29], p ¼ 0.003), resection versus chemotherapy (HR [95% CI],0.171 [0.08–0.33],p < 0.001) andKPS (HR [95%CI], 7.29 [4.77–11.12],p < 0.001)assignificant risk factors for local recurrence(►Table 4). Interestingly, TMZ (HR [95% CI], 1.394 [0.75–2.58],p ¼ 0.292) was not a significant predictor of local recurrence.
Neural Network AnalysisSignificant variables from the multivariate model of localrecurrence were included as input variables in the neuralnetwork analysis (input variables: KPS, operative method andthe use of CCNU and TMZ). Subsequently, we found theimportance of the variables to predict local recurrence inthe following decreasing order: KPS ¼ 41.5%, operative meth-od ¼ 21.8%, TMZ ¼ 21.5%, and CCNU ¼ 15.2% (►Fig. 2). Inthis model, four hidden layers and one bias neuron weregenerated.
Discussion
The Karnofsky Performance Status (KPS) scale was the mostimportant factor associated with decreasing survival in thisstudy (►Fig. 3). We categorized the patients in four groupsfor KPS. The first group was composed of patients withKPS > 60. The second group comprised patients with KPS¼ 60. The third group included patientswith 40 � KPS < 60.The fourth group featured patients with KPS < 40. It isinteresting that survival decreased equiponderant with thedecreasing KPS scores. Among all four groups, there is astatistically significant correlation (p ¼ 0.000) between theKPS scores and decreased survival. Many studies have veri-fied that a lower KPS score has a correlation with decreasingsurvival in GBM patients.27–31 Abdullah Kalil et al conducteda study on factors associated with increased survival aftersurgical resection on GBM patients of more than 80 years ofage in which they found a statistically significant correlationbetween the KPS and overall survival.30 In another study,Chaichana et al considered preoperative factors associatedwith decreased survival for older patients who underwentresection of a GBM, and found that one of the preoperativefactors that was independently associated with decreasedsurvival was a KPS score of less than 80.31 Chaichana et al, inanother study, evaluated functional outcomes over time forpatients with glioblastoma, and found that a preoperativeKPS score of � 90 is associated with a prolonged functionaloutcome. Their findings may help guide treatment strategiesaimed at improving the quality of life of patients withglioblastoma.32 The KPS was not statistically important incorrelations with local recurrence in this study. Therefore, itseems that the KPS has a greater impact on quantity of lifethan on quality of life.
Age was another important factor associated with de-creased survival in our study. We assessed the age effect onsurvival in two different ways. Initially, we found that thecut-off point for age in this study was 70 years. Patients withmore than 70 years of age had significantly lower survival
Table 2 Case control matching
Categorization of the patients
Study population ! N ¼ 153
Groups: N (percent)
Age groups (two categories)
• Age � 70 28 (18.3%)
• Age < 70 125 (81.7%)
Age groups (three categories)
• Age � 70 28 (18.3%)
• 70 > Age � 45 87 (56.9%)
• Age < 45 38 (24.8%)
Survival
• More than 14 months 77 (50.3%)
• Less than 14 months 76 (49.7%)
TMZ versus without TMZ
• Radiotherapy þ resection þ TMZ 28 (18.3%)
• Radiotherapy þ resection 42 (27.5%)
TMZ
• Using TMZ 39 (25.5%)
• Not using TMZ 114 (74.5%)
CCNU versus without CCNU
• Radiotherapy þ resection þ CCNU 21 (13.7%)
• Radiotherapy þ resection 42 (27.5%)
CCNU
• Using CCNU 36(23.5%)
• Not using CCNU 117(76.5%)
TMZ versus CCNU
• Radiotherapy þ resection þ TMZ 28 (18.3%)
• Radiotherapy þ resection þ CCNU 21 (13.7%)
Adjuvant versus concurrent chemotherapy
• Radiotherapy þ resection þ adjuvant 33 (21.6%)
• Radiotherapyþresectionþ concurrentþadjuvant
16 (10.5%)
Resection versus chemotherapy
• Radiotherapy þ resection 42 (27.5%)
• Radiotherapy þ biopsy þchemotherapy
26 (17.0%)
Resection versus without resection
• Radiotherapy þ chemotherapy þresection
49 (32.0%)
• Radiotherapy þ chemotherapy þbiopsy
26 (17.0%)
Resection
• Radiotherapy þ resection 42 (27.5%)
• Radiotherapy þ biopsy 34 (22.2%)
Abbreviations: CCNU, lomustine; TMZ, temozolomide.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al. 85

rates. Since the presence of other comorbidities in old age ismore common, we assessed the correlation between agegroups (age� 45, 45 < age� 70, age > 70) and survival. Wefound that there is a correlation between age and survival.Age and preoperative neurological function are the twofactors most consistently associated with survival in severalstudies;1,31–33 however, we could not find any correlationbetween age and local recurrence.
Chemotherapy, in the present study, was shown to de-crease local recurrence and improve survival. Chemotherapyplans (radiotherapy alone versus radiotherapy þ adjuvantchemotherapy versus radiotherapy þ concurrent chemo-therapy) cause a demonstrable statistically significant de-crease in local recurrence (p < 0.001). Also, patients whoreceived CCNUand TMZhad significant lower local recurrencerates andhigher overall survival rates versuspatients towhomCCNU or TMZ was not administered (►Fig. 3A and B).We compare two groups of patients: those who underwentradiotherapy þ chemotherapy þ biopsy versus the groupof patients who underwent radiotherapy þ resection. The
interesting and important thing here is that chemotherapywas significantly more effective than resection in decreasingthe local recurrence rate. Moreover, chemotherapy was effec-tive on prolonging the overall survival. However, when wecompared the efficacyof the TMZversus the CCNU, for thefirsttime, we found that patients who used TMZ had a higheroverall survival than patients who used CCNU (p ¼ 0.007).Johnson et al assessed the glioblastoma survival in the UnitedStates before and during the TMZ era.34 They found thatamongst patients treated with surgery and a radiation-con-taining regimen, the median survival rate was of 12.0 monthsduring theperiodwithoutTMZagainst14.2months in theTMZera. The survival of patients with newly diagnosed glioblasto-mas improved from one period to the other, likely due to theuse of TMZ. In a recent experimental study, Harvey et alassessed the anticancer properties of CCNU in glioblastomacell lines, and found that the combination of docosahexaenoicacid (DHA) and CCNU strongly induced Uppsala 87 malignantglioma (U87-MG0 apoptosis and necrosis as indicated by flowcytometric analysis.35 They suggested a potential role for a
Table 3 Univariate analysis of the pre- peri- and postoperative characteristics of the patients using the Kaplan-Meier analysis
Group: A B C D
Time:Status:
Overall survivalRecurrence: No
Overall survivalRecurrence: Yes
Overall survivalDead
Progression-free survivalRecurrence: Yes
Age groups (two categories) No# (p ¼ 0.532) Yes� (p ¼ 0.027) Yes (p ¼ 0.009) No (p ¼ 0.738)
Age groups (three categories) No (p ¼ 0.066) No (p ¼ 0.060) Yes (p ¼ 0.005) No (p ¼ 0.731)
Motor deficit No (p ¼ 0.300) No (p ¼ 0.910) No (p ¼ 0.584) No (p ¼ 0.052)
Confusion and/or memory loss Yes (p < 0.001) No (p ¼ 0.222) No (p ¼ 0.307) No (p ¼ 0.855)
Seizure No (p ¼ 0.414) No (p ¼ 0.403) No (p ¼ 0.135) No (p ¼ 0.089)
CCNU No (p ¼ 0.114) No (p ¼ 0.108) No (p ¼ 0.144) Yes (p < 0.001)
TMZ No (p ¼ 0.450) Yes (p < 0.001) Yes (P <0.001) Yes (p ¼ 0.003)
Resection versus biopsy No (p ¼ 0.085) Yes (p < 0.001) Yes (p < 0.001) Yes (p < 0.001)
Resection versus chemotherapy No (p ¼ 0.827) No (p ¼ 0.211) No (p ¼ 0.171) Yes (p < 0.001)
Resection versus without resection No (p ¼ 0.306) Yes (p < 0.001) Yes (p < 0.001) Yes (p ¼ 0.030)
TMZ versus CCNU No (p ¼ 0.249) Yes (p ¼ 0.007) No (p ¼ 0.315) No (p ¼ 0.935)
CCNU versus without CCNU No (p ¼ 0.237) Yes (p < 0.001) Yes (p < 0.001) Yes (p ¼ 0.001)
TMZ versus without TMZ No (p ¼ 0.339) Yes (p < 0.001) Yes (p < 0.001) Yes (p ¼ 0.003)
Occipital lobe No (p ¼ 0.053) No (p ¼ 0.067) No (p ¼ 0.685) No (p ¼ 0.468)
Frontal lobe No (p ¼ 0.051) Yes (p ¼ 0.009) Yes (p ¼ 0.034) No (p ¼ 0.912)
Operative method No (p ¼ 0.056) Yes (p < 0.001) Yes (p < 0.001) Yes (p ¼ 0.016)
KPS Yes (p < 0.001) Yes (p < 0.001) Yes (p < 0.001) Yes (p < 0.001)
2D versus 3D radiation Yes (p < 0.001) Yes (p ¼ 0.004) No (p ¼ 0.547) �Chemotherapy plan No (p ¼ 0.090) Yes (p < 0.001) Yes (p < 0.001) Yes (p < 0.001)
Recurrence � � Yes (p < 0.001) �Abbreviations: 2D, two-dimensional; 3D, three-dimensional; CCNU, lomustine; KPS, Karnofsky Performance Status; TMZ, temozolomide.Notes: A: Time defined as overall survival and status defined as no tumor recurrence.B: Time defined as overall survival and status defined as tumor recurrence.C: Time defined as overall survival and status defined as death.D: Time defined as progression-free survival and status defined as tumor recurrence.�Yes means there is a significant correlation between an obvious factor and survival or recurrence.#No means there is not a significant correlation between an obvious factor and survival or recurrence.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al.86

combination therapy of CCNU and DHA for the treatment ofglioblastomas. Other studies recommended using CCNU forrecurrent GBMs.36–38
Among our patients, we found that if local recurrence didnot occur, the patients experienced a higher overall survivaltime. This suggests the necessity of effective treatments toprevent local recurrence, leading to increasing survival rates.
The role of resection in prolonging survival in our patientsappeared in the univariate and multivariate analyses(►Fig. 3C). The operative method had a statistically impor-tant role in increasing survival and decreasing local recur-rence. Additionally, we compared patients in two groups:radiotherapy þ resection versus radiotherapy þ biopsy.
Table 4 Multivariate analysis of the factors associated with overall survival and local recurrence using the Cox regression models
Group: A B C
Time:Status:
Overall survivalRecurrence
Overall survivalDeath
Progression-free survivalRecurrence
Hazard Ratio (94% CI)p-value
Hazard Ratio (95% CI)p-value
Hazard Ratio (95% CI)p-value
Age groups (two categories) 2.939 (1.73–4.99)p < 0.001
3.081 (1.89–5.01)p < 0.001
�
TMZ 11.723 (5.46–25.13)p < 0.001
4.906 (2.51–9.56)p < 0.001
1.394 (0.75–2.58)p ¼ 0.292
CCNU 8.139 (4.04–16.38)p < 0.001
4.155 (2.19–7.86)p < 0.001
2.047 (1.27–3.29)p ¼ 0.003
Operative method 7.416 (3.81–14.42)p < 0.001
3.880 (2.00–7.50)p < 0.001
0.493 (0.30–0.80)p ¼ 0.005
KPS 4.831 (3.00–7.77)p < 0.001
6.078 (3.85–9.57)p < 0.001
7.292 (4.77–11.12)p < 0.001
Occipital lobe 3.088 (1.81–5.25)p < 0.001
1.599 (0.95–2.69)p ¼ 0.077
�
Resection versus chemotherapy � � 0.171 (0.08–0.33)p < 0.001
Abbreviations: 95% CI, 95% conficence interval; CCNU, lomustine; KPS, Karnofsky Performance Status; TMZ, temozolomide.Notes: A: Time defined as overall survival and status defined as tumor recurrence.B: Time defined as overall survival and status defined as death.C: Time defined as progression-free survival and status defined as tumor recurrence.
Fig. 1 Result of neural network analysis for predicting survival. Theinput variables are those that had an impact on survival on themultivariate analysis from Cox regression model analysis. Wefound the importance of the variables to predict survival as follows:KPS ¼ 30.6%, operative method ¼ 20.4%, TMZ ¼ 17.0%,CCNU ¼ 15.0%, age ¼ 13.5%, and occipital lobe involvement ¼ 3.6%.In this model, four hidden layers were included in the calculation.
Fig. 2 Result of neural network analysis for predicting localrecurrence. The input variables are those that had an impact onlocal recurrence on the multivariate analysis. We found theimportance of the variables to predict local recurrence as follows:KPS ¼ 41.5%, operative method ¼ 21.8%, TMZ ¼ 21.5%, andCCNU ¼ 15.2%. In this model, four hidden layers were includedin the calculation.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al. 87

Patients who underwent radiotherapy þ resection hadhigher survival and lower recurrence rates than the biopsygroup. This observation clearly defined the important role ofresection in prolonging survival among patients with poorprognoses, especially thosewith advanced ages. Chaichana etal assessed the factors associated with survival for 100patients with glioblastomas with KPS scores � 60.39 Theyfound that the factors associated with improved survivalwere age < 65 years, tumor size > 2 cm, radical tumorresection, and TMZ. Chaichana et al, in another study,assessed the effect of multiple resections on prolongingsurvival in 578 patients with GBM.19 In their study 354,168, 41, and 15 patients underwent 1, 2, 3, or 4 resectionsrespectively. The median survival rate for patients whounderwent 1, 2, 3, and 4 resections was of 6.8, 15.5, 22.4,and 26.6 months respectively, and that was statisticallysignificant. Finally, they concluded that patients with recur-
rent glioblastomas can have improved survival rates withrepeated resections.
Poor neurologic status before surgery was another factorassociated with decreased survival and increasing localrecurrence in our series. We found that confusion and/ormemory loss will decrease survival, while motor deficit willprobably increase local recurrence. In a different study,various neurologic signs have shown to decrease survivaland increase local recurrence rates.31,40–42 We designed aneural network analysis to predict the factors associatedwith decreasing survival, which we also found in the multi-variate analysis, and the factors associated with local recur-rence. The KPS was the most important factor to predictsurvival and local recurrence. We found the importance ofeach factor in predicting survival and local recurrence;however, future studies with larger sample sizes arerecommended.
Fig. 3 (A) Kaplan-Meier curve suggesting the TMZ effect on overall survival (p < 0.001). (B) Kaplan-Meier curves suggesting the CCNU effect onoverall survival (p < 0.001). (C) Kaplan-Meier curves suggesting the resection effect on overall survival (p < 0.001). (D) Kaplan-Meier curves forthe overall survival of four groups of patients. The first group of patients had a KPS score > 60, the second group had a KPS score ¼ 60, the thirdgroup had scores 40 � KPS < 60, and the last group had a KPS score < 40. There was a statistically significant difference (p < 0.001) among thefour groups.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al.88

Strengths and LimitationsWe believe that this study provides several useful insights toidentify the factors associated with survival and local recur-rence in patients with GBM. Firstly, the importance ofquantity and quality of life in GBM is equal, and maybequality of life is preferred, because of the overall short-termsurvival of the patients. There are many important factorsassociated with survival and local recurrence. The factorsthat are reversible are most important because they are themost effective at changing the fate of the patients.
This study confirms the associations of age, confusionand/or memory loss, CCNU, TMZ, KPS, operative method,TMZ versus CCNU, 2D versus 3D radiation and frontal lobeinvolvement in survival. It also confirms the association ofCCNU, TMZ, chemotherapy versus resection, operativemeth-od and KPS with local recurrence. This study also confirmedthat CCNU, TMZ, operative method and KPS are the factorsassociated with both survival and local recurrence.
Secondly, studies applying preoperative risk factors in amanner that provides useful prognostic information have yetto be established, both for survival and local recurrence.Lastly, this study provides a potentially useful guide thatmayprognosticate which GBM patients may benefit from che-motherapy as opposed to radiotherapy and resection. Thismeans that the aggressive treatment is accompanied byhigher survival and lower local recurrence rates.
This study, however, has some limitations. Firstly, thesample size is not large. A significantly larger sample sizewith exact sub-groups will allow a better analysis, especiallyfor achieving neural network analysis. Secondly, we couldnot procure some necessary data from the records, perhapsmost importantly the size of each tumor. Other MRI wasmissed in this study. Thirdly, some patients did not receivethe full treatment, such as undergoing surgery and/or che-motherapy, because the treatments were cost-prohibitive.This study also does not account for the potential implicationof molecular markers and genotypes, which may be associ-ated with survival. Recent studies on GBM patients definedthat O6-methylguanine–DNA methyltransferase (MGMT)promoter methylation leads to prolonged survival afterTMZ and radiation therapy compared with patients withoutthis molecular marker.43 Additionally, Sanson et al indicatedthat isocitrate dehydrogenase 1 (IDH1) codon 132 mutationis closely linked to the genomic profile of the tumor, andconstitutes an important prognostic marker in grade 2 to 4gliomas.44 These molecular markers, and perhaps othermarkers associated with survival, were not analyzed in thisstudy. Additionally, this study was unable to evaluate theother prognostic factors associated with survival, such asmarital status45 and presence of a caregiver,46 which havebeen found in other studies, because these were not consis-tently recorded in our patient records. Finally, this study isnaturally limited because of its retrospective design, and, as aresult, it is not appropriate to infer direct causal relations-hips. Furthermore, we performed multivariate and neuralnetwork analyses, and controlled for potential confoundingvariables. Given these statistical controls and a relativelyprecise outcome measure, we believe that our findings offer
useful insights for the treatment of patients with primaryGBM. Prospective studies with huge sample sizes are neededto provide better data to guide clinical decision making.
Conclusion
Almost all of the patients with GBM will benefit fromaggressive therapy, including radiotherapy, chemotherapyand resection. We cannot guarantee the patients’ survival orguarantee non-recurrence, but it is certain that patientswithGBM should be managed with an effective therapy to reachtwo goals: higher survival and zero recurrence rates. Thesetwo goalswill guarantee better quality and quantity of life forthese patients. In this study CCNU, TMZ, operative methodand KPS appear as factors associated with both increasingsurvival and decreasing local recurrence rates. A prospectivestudy with a global partnership and a larger sample size isrecommended for the future.
AcknowledgmentThe authors would like to extend a special thanks toPeriasamy Selvaraj, PhD, Professor of Immunology atEmory University School of Medicine, USA, for his advicesand recommendations.
References1 DeAngelis LM. Brain tumors. N Engl J Med 2001;344(02):114–1232 Jazayeri SB, Rahimi-Movaghar V, Shokraneh F, Saadat S, Ramezani
R. Epidemiology of primary CNS tumors in Iran: a systematicreview. Asian Pac J Cancer Prev 2013;14(06):3979–3985
3 Mazaris P, Hong X, Altshuler D, et al. Key determinants of short-term and long-term glioblastoma survival: a 14-year retrospec-tive study of patients from the Hermelin Brain Tumor Center atHenry Ford Hospital. Clin Neurol Neurosurg 2014;120:103–112
4 McGirt MJ, Than KD,Weingart JD, et al. Gliadel (BCNU) wafer plusconcomitant temozolomide therapy after primary resection ofglioblastoma multiforme. J Neurosurg 2009;110(03):583–588
5 Ening G, Huynh MT, Schmieder K, Brenke C. Repeat-surgery atGlioblastoma recurrence, when and why to operate? Clin NeurolNeurosurg 2015;136:89–94
6 Gan HK, Rosenthal MA, Cher L, et al. Management of glioblastomain Victoria, Australia (2006-2008). J Clin Neurosci 2015;22(09):1462–1466
7 Malmström A, Grønberg BH, Marosi C, et al; Nordic Clinical BrainTumour Study Group (NCBTSG). Temozolomide versus standard6-week radiotherapy versus hypofractionated radiotherapy inpatients older than 60 years with glioblastoma: the Nordicrandomised, phase 3 trial. Lancet Oncol 2012;13(09):916–926
8 Stupp R, Hegi ME, Mason WP, et al; European Organisation forResearch and Treatment of Cancer Brain Tumour and RadiationOncology Groups; National Cancer Institute of Canada ClinicalTrials Group. Effects of radiotherapy with concomitant and ad-juvant temozolomide versus radiotherapy alone on survival inglioblastoma in a randomised phase III study: 5-year analysis ofthe EORTC-NCIC trial. Lancet Oncol 2009;10(05):459–466
9 Chaichana KL, Jusue-Torres I, Navarro-Ramirez R, et al. Establish-ing percent resection and residual volume thresholds affectingsurvival and recurrence for patients with newly diagnosed in-tracranial glioblastoma. Neuro-oncol 2014;16(01):113–122
10 Vives KP, Piepmeier JM. Complications and expected outcome ofglioma surgery. J Neurooncol 1999;42(03):289–302
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al. 89

11 Litofsky NS, Farace E, Anderson F Jr, Meyers CA, HuangW, Laws ERJr; Glioma Outcomes Project Investigators. Depression in patientswith high-grade glioma: results of the Glioma Outcomes Project.Neurosurgery 2004;54(02):358–366, discussion 366–367
12 EningG, Osterheld F, Capper D, Schmieder K, Brenke C. Risk factorsfor glioblastoma therapy associated complications. Clin NeurolNeurosurg 2015;134:55–59
13 Aaronson NK. Quality of life: what is it? How should it bemeasured?. Oncology (Williston Park) 1988;2(05):69–76, 64
14 Gállego Pérez-Larraya J, Ducray F, ChinotO, et al. Temozolomide inelderly patients with newly diagnosed glioblastoma and poorperformance status: an ANOCEF phase II trial. J Clin Oncol 2011;29(22):3050–3055
15 Henriksson R, Asklund T, Poulsen HS. Impact of therapyon qualityof life, neurocognitive function and their correlates in glioblas-toma multiforme: a review. J Neurooncol 2011;104(03):639–646
16 Nieder C, Astner ST, Mehta MP, Grosu AL, Molls M. Improvement,clinical course, and quality of life after palliative radiotherapy forrecurrent glioblastoma. Am J Clin Oncol 2008;31(03):300–305
17 McGirt MJ, Chaichana KL, Attenello FJ, et al. Extent of surgicalresection is independently associated with survival in patientswith hemispheric infiltrating low-grade gliomas. Neurosurgery2008;63(04):700–707, author reply 707–708
18 Chaichana KL, Zaidi H, Pendleton C, et al. The efficacy of carmus-tine wafers for older patients with glioblastoma multiforme:prolonging survival. Neurol Res 2011;33(07):759–764
19 Chaichana KL, Zadnik P, Weingart JD, et al. Multiple resections forpatients with glioblastoma: prolonging survival. J Neurosurg2013;118(04):812–820
20 Kleihues P, Louis DN, Scheithauer BW, et al. The WHO classifica-tion of tumors of the nervous system. J Neuropathol Exp Neurol2002;61(03):215–225, discussion 226–229
21 Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHO classifica-tion of tumours of the central nervous system. Acta Neuropathol2007;114(02):97–109
22 Dutta D, Vanere P, Gupta T, Munshi A, Jalali R. Factors influencingactivities of daily living using FIM-FAM scoring system beforestarting adjuvant treatment in patientswith brain tumors: resultsfrom a prospective study. J Neurooncol 2009;94(01):103–110
23 Cairncross G, Macdonald D, Ludwin S, et al; National CancerInstitute of Canada Clinical Trials Group. Chemotherapy foranaplastic oligodendroglioma. J Clin Oncol 1994;12(10):2013–2021
24 Hashemi EL, Haddad P, Kazemian A. Effects of monotherapyversus combination therapy on overall and disease-free survivalin high-grade astrocytoma. Tehran Univ Med J 2007;65(07):32–36(TUMJ)
25 Stupp R, Tonn JC, Brada M, Pentheroudakis G; ESMO GuidelinesWorking Group. High-grade malignant glioma: ESMO ClinicalPractice Guidelines for diagnosis, treatment and follow-up. AnnOncol 2010;21(Suppl 5):v190–v193
26 Mason WP, Maestro RD, Eisenstat D, et al; Canadian GBM Re-commendations Committee. Canadian recommendations for thetreatment of glioblastoma multiforme. Curr Oncol 2007;14(03):110–117
27 Polin RS, Marko NF, Ammerman MD, et al. Functional outcomesand survival in patients with high-grade gliomas in dominant andnondominant hemispheres. J Neurosurg 2005;102(02):276–283
28 LacroixM, Abi-Said D, Fourney DR, et al. Amultivariate analysis of416 patients with glioblastoma multiforme: prognosis, extent ofresection, and survival. J Neurosurg 2001;95(02):190–198
29 Stark AM, Nabavi A, Mehdorn HM, Blömer U. Glioblastomamulti-forme-report of 267 cases treated at a single institution. SurgNeurol 2005;63(02):162–169, discussion 169
30 Abdullah KG, Ramayya A, Thawani JP, et al. Factors associatedwithincreased survival after surgical resection of glioblastoma inoctogenarians. PLoS One 2015;10(05):e0127202
31 Chaichana KL, Chaichana KK, Olivi A, et al. Surgical outcomes forolder patients with glioblastoma multiforme: preoperative fac-tors associated with decreased survival. Clinical article.J Neurosurg 2011;114(03):587–594
32 Chaichana KL, Halthore AN, Parker SL, et al. Factors involved inmaintaining prolonged functional independence following su-pratentorial glioblastoma resection. Clinical article. J Neurosurg2011;114(03):604–612
33 Buckner JC. “Factors influencing survival in high-grade gliomas. ”Seminars in oncology. Vol. 30. WB Saunders; 2003
34 Johnson DR, O’Neill BP. Glioblastoma survival in the United Statesbefore and during the temozolomide era. J Neurooncol 2012;107(02):359–364
35 Harvey KA, Xu Z, Saaddatzadeh MR, et al. Enhanced anticancerproperties of lomustine in conjunction with docosahexaenoicacid in glioblastoma cell lines. J Neurosurg 2015;122(03):547–556
36 TaalW, et al. O10.05 final analysis of the belob trial (a randomizedphase ii study on bevacizumab versus bevacizumab plus lomus-tine versus lomustine single agent in recurrent glioblastoma) andfirst radiology review results. Neuro-oncol 2014;16(Suppl 2):ii24
37 BrandesAA, et al. “Aphase II studyof galunisertibmonotherapyorgalunisertib plus lomustine compared to lomustinemonotherapyin recurrent glioblastoma. ”ASCOAnnualMeeting Proceedings. Vol.33. No. 15_suppl. 2015
38 Wick W, Puduvalli VK, Chamberlain MC, et al. Phase III study ofenzastaurincomparedwith lomustine in the treatmentof recurrentintracranial glioblastoma. J Clin Oncol 2010;28(07):1168–1174
39 Chaichana KL, Martinez-Gutierrez JC, De la Garza-Ramos R, et al.Factors associated with survival for patients with glioblastomawith poor pre-operative functional status. J Clin Neurosci 2013;20(06):818–823
40 Krex D, Klink B, Hartmann C, et al; German Glioma Network.Long-term survival with glioblastoma multiforme. Brain 2007;130(Pt 10):2596–2606
41 Lamborn KR, Chang SM, Prados MD. Prognostic factors for survi-val of patients with glioblastoma: recursive partitioning analysis.Neuro-oncol 2004;6(03):227–235
42 Laws ER, Parney IF, Huang W, et al; Glioma Outcomes Investiga-tors. Survival following surgery and prognostic factors for re-cently diagnosed malignant glioma: data from the GliomaOutcomes Project. J Neurosurg 2003;99(03):467–473
43 Hegi ME, Diserens AC, Gorlia T, et al. MGMT gene silencing andbenefit from temozolomide in glioblastoma. N Engl J Med 2005;352(10):997–1003
44 SansonM,Marie Y, Paris S, et al. Isocitrate dehydrogenase 1 codon132 mutation is an important prognostic biomarker in gliomas.J Clin Oncol 2009;27(25):4150–4154
45 Wrensch M, Rice T, Miike R, et al. Diagnostic, treatment, anddemographic factors influencing survival in a population-basedstudy of adult glioma patients in the San Francisco Bay Area.Neuro-oncol 2006;8(01):12–26
46 Chang SM, Barker FG II. Marital status, treatment, and survival inpatientswith glioblastomamultiforme: a population based study.Cancer 2005;104(09):1975–1984
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Glioblastoma Multiforme and Relative Risk Factors Nikdad et al.90

Head Measurements for the Diagnosis ofCraniosynostosis
As medidas cranianas no diagnóstico dascraniossinostoses
José Aloysio CostaVal1,2 Leopoldo Furtado Mandic1 Sebastião Nataniel Gusmão2
1Department of Pediatric Neurosurgery, Biocor Instituto, Nova Lima,MG, Brazil
2School of Medicine, Universidade Federal de Minas Gerais (UFMG),Belo Horizonte, MG, Brazil
Arq Bras Neurocir 2017;36:91–95.
Address for correspondence José Aloysio CostaVal, MD, PediatricNeurosurgery, Biocor Instituto, Av. Alameda da Serra, 322/408. NovaLima. MG. 34000000. Brazil (e-mail: [email protected]).
Keywords
► child care► diagnostic
recommendations► craniosynostosis and
head circumference
Abstract Objective Craniosynostosis is a group of growth disturbances of the skull, which canresult in serious consequences for the children who suffer from it. Early diagnosisprovides treatment at the correct time. Most of the time, the pediatrician uses the headcircumference (HC) as a parameter for the diagnosis, but the HC does not appear to bechanged in this disease, leading to incorrect interpretations. The anteroposteriordistance (APD) and biauricular distance (BAD) appear to be more accurate. The aim ofthis study is to analyze the value of the HC and the ratio between the measurements ofthe APD and the BAD for this diagnosis.Methods We analyzed the data from 129 children who had already undergone anoperation for craniosynostosis at an institution in Southeastern Brazil. These data werecompared with the normal standards of the population and statistically analyzed toestablish their alterations.Results The HC did not change significantly in cases of craniosynostosis, neither whenit was considered as a single disease, nor when considering the different subtypes. TheAPD/BAD ratio changed significantly in the group.Conclusion The HC does not appear to be useful in the diagnosis of craniosynostosisas an individual parameter. The APD/BAD ratio appears to help in the diagnosis.
Palavras-chave
► cuidado infantil► recomendações de
diagnóstico► craniossinostoses e
perímetro cefálico
Resumo Objetivo Craniossinostoses são alterações do crescimento do crânio que podemresultar graves consequências para a criança. O diagnóstico precoce propicia otratamento correto. O perímetro cefálico (PC) é habitualmente usado como parâmetropara o diagnóstico. Porém, como na maioria das vezes há alteração na forma e não noperímetro, sua utilização isolada pode levar a detecção tardia. As medidas do diâmetroântero posterior (DAB) e bi auricular (DBA) parecem ser mais precisas. O objetivo dotrabalho é analisar o valor do PC no diagnóstico, bem como o da razão entre as medidasDAP/ DBA.
receivedDecember 12, 2016acceptedFebruary 23, 2017published onlineApril 20, 2017
DOI https://doi.org/10.1055/s-0037-1602692.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 91

Introduction
Craniosynostosis is a well-known group of changes to theshape of the skull, secondary to the early fusion of thesutures. Those changes may cause restrictions in the devel-opment of some regions of the head, which are compensatedfor by abnormal growth in other areas.
The diagnosis of craniosynostosis is essentially clinical,based on the shape of the skull. Anthropometric data shouldbe measured routinely by pediatricians during consulta-tions to help the diagnosis. But, in the daily practice, it iscommon to use only the head circumference (HC) as aparameter, suggesting that, in the presence of a craniosyn-ostosis, these data would be reduced because the skull doesnot grow satisfactorily. However, in most cases there iscompensation in skull growth, resulting in a dysmorphicperimeter, but a normal HC. The measurement of theanteroposterior distance (APD) and the biauricular distance(BAD) could be more accurate, reflecting the changes in theshape of the head.
The aim of this work is to demonstrate the hole of thosemeasurements in the diagnosis of the disease.
Methods
We analyzed the data from 129 childrenwho had undergonesurgical treatment for craniosynostosis at the Biocor Insti-tuto, which were stored in the database of the surgical team.The data collected were age in months, sex, and anthropo-metric variables (HC, APD, and BAD) measured in centi-meters by the traditional semiological technique.1 Thechildren were classified into craniosynostosis subtypes, de-pending on the clinical presentation. The subtypes consid-ered were trigonocephaly (closure of the metopic suture),scaphocephaly (closure of the sagittal suture), brachycephaly(closure of the coronal sutures bilaterally), plagiocephaly(closure of the coronal or lambdoid sutures unilaterally),oxycephaly (potential closure of all sutures) or mixed (clo-sure of more than one suture).
The data were subjected to analysis using the StatisticalPackage for the Social Sciences (SPSS, IBM Corp., Armonk,NY, US) software. A comparison of the percentage ofpatients was performed with a frequency table and thechi-square test.2
The HC was regarded as decreased, normal or enlargedfollowing the World Health Organization (WHO) criteria(http://www.who.int/childgrowth/standards/hc_for_age).
The APD/BAD ratio was considered normal or abnormalbased on a theoretical assumption that the ratio of themeasurements would be equal to 1.
Results
Most of the children were male. The mean age was10.5 months, with a median of 7 months.
Trigonocephalywas themost frequent subtype (49 cases),followed by scaphocephaly (31 cases), plagiocephaly(25 cases), brachycephaly (12 cases), oxycephaly (10 cases)and mixed (2 cases) (►Fig. 1).
The statistical analyses showed that there was a signifi-cant predominance of patients with a normal HC (►Fig. 2).Children with decreased or increased values of HC had thesame statistical expression (►Table 1).
The HC in the subtypes of craniosynostosis was alsoanalyzed according to the parameters of normal and abnor-mal (►Table 2). Although there were numerical differencesin the expression of normal or altered HC in the differentsubtypes, the number of children with decreased or in-creased values of HCwas not significantly different (►Fig. 3).
Data showed that the frequency of patients with anabnormal APD/BAD ratio increased (►Table 3).
Discussion
Craniosynostosis is a group of changes to the shape andgrowth of the skull, secondary to the early partial or totalfusion of one or more sutures of the calvaria and skullbase.3–5 Generally, changes in the function of the suturescause restrictions in the development of some regions of theskull, which are compensated for by abnormal growth inother areas.6 According to the involvement of the sutures,several specific subtypes may develop.7
The etiology is still debated. Teratogenesis and environ-mental factors are known, but genetic involvement appearsto be the most prevalent cause.6,8–10 As a consequence, thedisease has a precocious presentation.
Craniosynostosis can result in serious consequences forthe child. Changes in the shape of the skull can lead toaesthetic impairments with a variable intensity. Rejectionof their appearance, social dumping and lack of emotionalcommitment are known secondary phenomena of thesealterations.11,12
Dysmorphisms may affect the cranial orbits, the base ofthe skull and the face, and lead to functional impairment.13
Métodos Foram analisadas dados de 139 crianças já operadas no Biocor Instituto, emMinas Gerais. Os dados foram comparados com os parâmetros normais já conhecidosda população.Resultados O PC não se alterou de maneira significativa nas craniossinostoses, sejacomo um grupo único ou nos subtipos. A razão das medidas DAP/ DBA alterou-se.Conclusão O PC isolado parece não ser útil para o diagnóstico das craniossinostoses.A razão das medidas DAP/ DBA parecendo ter utilidade.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Head Measurements for the Diagnosis of Craniosynostosis CostaVal et al.92

Hypo- or hypertelorism, airway involvement and localizedbrain compression, especially in the posterior region, mayfollow these manifestations.14–16
Theremight also be restrictions to the growth of the skull.During the first year of life, such growth occurs significantly,following the exponential increase in the size of the brain.The restriction of this growth by the inefficient action of thesutures can lead to decreased cranial volume, with conse-quent chronic intracranial hypertension and injury, in vary-ing degrees, to the infant brain.7,17,18
Surgical treatment is indicated for a significant portion ofchildren with craniosynostosis to avoid the aforementionedconsequences. The treatment should be performed early,even in the first months of life, to promote better cosmeticand functional results, and to prevent compression of thebrain.6,19–22 In addition, the procedure is more aggressive,has more morbidity, and sometimes is less effective whenperformed later.22,23 However, for an early treatment, aneven earlier diagnosis is necessary.
The diagnosis of craniosynostosis is essentially clinical,based on the shape of the skull. Pediatricians see the childrenin consultations in the first months, and have the opportu-nity to make an early diagnosis of the disease. Anthropomet-ric data such as the HC, the APD and the BAD should be
Fig. 2 Distribution by head circumference (HC).
Table 1 Statistical frequency of cases by head circumference
Head circumference Total p-value
Decreased Normal Enlarged
23(17.8%)
80(62.0%)
26(20.2%)
129(100%)
< 0.001
Note: Chi-square test.
Table 2 Distribution by subtypes and head circumference
Craniosynostosis Head circumference Total
Altered Normal
Trigonocephaly 15 (30.6%) 34 (69.4%) 49 (100)
Scaphocephaly 18 (58.1%) 13 (41.9%) 31 (100)
Plagiocephaly 6 (24.0%) 19 (76.0%) 25 (100)
Brachycephaly 6 (50.0%) 6 (50.0%) 12 (100)
Oxycephaly 3 (30.0%) 7 (70.0%) 10 (100)
Mixed 1 (50.0%) 1 (50.0%) 2 (100)
p-value 0.086 � �Note: Chi-squared test.
Fig. 1 Distribution of the subtypes of craniosynostosis.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Head Measurements for the Diagnosis of Craniosynostosis CostaVal et al. 93

measured routinely to help the diagnosis. However, in thedaily practice, pediatricians commonly use the HC as aparameter, believing that in the presence of a craniosynos-tosis, these datawould be reduced because the skull does notgrow satisfactorily. However, in most cases there is compen-sation in the skull growth toward the closed suture, resultingin a dysmorphic perimeter, but a normal HC.24 This mea-surement also does not represent the intracranialvolume.21,25,26
The cranial dysmorphism resulting from asymmetricgrowth could indeed be confirmed by a change in theAPD/BAD ratio.17,27 Those measurements, not universally usedby the pediatricians, could be more precise for the diagnosis.
The analysis of the data showed that the gender of thechildren reflected the traditional knowledge, with cranio-synostosis being more prevalent in boys. The age of thesample revealed the timing of the treatment, when thedisease has become well manifested.
The incidence of the subtypes of craniosynostosis drawsattention. Classically, scaphocephaly is the most frequentsubtype. However, in our sample, trigonocephaly had thehighest number of cases. This phenomenon has been previ-ously observed in several services throughout theworld, andhas been considered a confirmed fact for some authors.28
The analysis of the data seems to show that there aredistinct behaviors between them and the craniosynostosis.While the HC does not change, the APD and the BAD arealtered in this disease.
The data related to the HC were analyzed consideringcraniosynostosis as a single disease, and considering each
subtype separately. The HC is normal in themajority of cases,which is in contrast with the classical belief about cranio-synostosis. There was a significant similarity in the numberof childrenwith increased and decreased HCs. This finding isalso in contrast with the perception that the HC is decreasedin craniosynostosis.
When analyzing the subtypes, we noted a predominanceof HC changes in cases of scaphocephaly and brachycephaly,but such changes were not significant. Therefore, a normalHC is prevalent in all subtypes of craniosynostosis that werestudied.
With the APD and the BAD, the perception is the opposite,as these measurements appear to be altered in craniosynos-tosis. The number of patients with increased or decreasedAPD/BAD ratio changed in the majority of cases. The statisti-cal analysis of the data showed that these values weresignificant. Thus, the APD/DBP ratio was altered incraniosynostosis.
Conclusions
The analysis of the data suggests that in craniosynosto-sis, considered as a single disease, there is no signi-ficant change in the HC. The measurement does notchange significantly, even when considering the subtypesindividually.
Thus, this measurement should not be considered inisolation for the diagnosis of this disease.
Additionally, our study suggests that the APD/BAD ratio isaltered in craniosynostosis. Therefore, the analysis of thisratio appears to be useful as a parameter for the diagnosis ofthis illness.
Funding SourceNo external funding was secured for this study.
Financial DisclosureAll authors have no financial relationships relevant to thisarticle to disclose.
Fig. 3 Distribution by anteroposterior distance (APD)/biauricular distance (BAD) ratio.
Table 3 Comparison of the percentage of patients with normalAPD/BAD ratios
Ratio APD/BAD Total
Normal Altered
22 (17.0%) 107 (83.0%) 129 (100%)
p-value 0.196 � �Abbreviations: APD, anteroposterior distance; BAD, biauricular dis-tance. Note: Chi-squared test.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Head Measurements for the Diagnosis of Craniosynostosis CostaVal et al.94

Conflict of InterestAll authors have no conflicts of interest to disclose.Institutional reviewboard (IRB)/ethics committee and thehuman subjects assurance: COEP UFMG - &CAAE:10306913.8.0000.5149
References1 Marcondes E. Normas para caracterização dos perímetros cefálico
e torácico. Pediat (São Paulo) 1983;5:249–2752 Triloa MF. Elementary Statistics: High School Edition. 9 ed:
Addison-Wesley Educational Publishers, Incorporated; 20053 Delashaw JB, Persing JA, BroaddusWC, Jane JA. Cranial vault growth
in craniosynostosis. J Neurosurg 1989;70(02):159–1654 Foltz EL, Loeser JD. Craniosynostosis. J Neurosurg 1975;43(01):
48–575 Goodrich JT. Skull base growth in craniosynostosis. Childs Nerv
Syst 2005;21(10):871–8796 Lajeunie E, Barcik U, Thorne JA, El Ghouzzi V, Bourgeois M, Renier
D. Craniosynostosis and fetal exposure to sodium valproate.J Neurosurg 2001;95(05):778–782
7 Persing PPSJA. Craniosynostosis. In: Andelson LAIPD, editor.Principals and Practice of Pediatric Neurosurgery. 1. New York:Thieme Medical Publishers Inc.; 1999. p. 219–42.
8 Johnson D, Wilkie AO. Craniosynostosis. Eur J Hum Genet 2011;19(04):369–376
9 Merritt L. Recognizing craniosynostosis. Neonatal Netw 2009;28(06):369–376
10 Wilkie AO, Byren JC, Hurst JA, et al. Prevalence and complicationsof single-gene and chromosomal disorders in craniosynostosis.Pediatrics 2010;126(02):e391–e400
11 Dake JA, Price JH, Telljohann SK. The nature and extent of bullyingat school. J Sch Health 2003;73(05):173–180
12 Ozgur BM, Aryan HE, Ibrahim D, et al. Emotional and psycholo-gical impact of delayed craniosynostosis repair. Childs Nerv Syst2006;22(12):1619–1623
13 Stavrou P, Sgouros S, Willshaw HE, Goldin JH, Hockley AD, WakeMJ. Visual failure caused by raised intracranial pressure incraniosynostosis. Childs Nerv Syst 1997;13(02):64–67
14 Baranello G, Vasco G, Ricci D, Mercuri E. Visual function innonsyndromic craniosynostosis: past, present, and future. ChildsNerv Syst 2007;23(12):1461–1465
15 Clement R, Nischal K. Simulation of oculomotility in Craniosy-nostosis patients. Strabismus 2003;11(04):239–242
16 Hayward R. Venous hypertension and craniosynostosis. ChildsNerv Syst 2005;21(10):880–888
17 Weber J, Collmann H, Czarnetzki A, Spring A, Pusch CM. Morpho-metric analysis of untreated adult skulls in syndromic and non-syndromic craniosynostosis. Neurosurg Rev 2008;31(02):179–188
18 Renier D, Sainte-Rose C, Marchac D, Hirsch JF. Intracranial pres-sure in craniostenosis. J Neurosurg 1982;57(03):370–377
19 Agrawal D, Steinbok P, Cochrane DD. Long-term anthropometricoutcomes following surgery for isolated sagittal craniosynostosis.J Neurosurg 2006;105(5, Suppl)357–360
20 Inagaki T, Kyutoku S, SenoT, et al. The intracranial pressure of thepatients with mild form of craniosynostosis. Childs Nerv Syst2007;23(12):1455–1459
21 Kamdar MR, Gomez RA, Ascherman JA. Intracranial volumes in alarge series of healthy children. Plast Reconstr Surg 2009;124(06):2072–2075
22 Seruya M, Oh AK, Boyajian MJ, Posnick JC, Keating RF. Treatmentfor delayed presentation of sagittal synostosis: challenges per-taining to occult intracranial hypertension. J Neurosurg Pediatr2011;8(01):40–48
23 Smyth MD, Tenenbaum MJ, Kaufman CB, Kane AA. The “clam-shell” craniotomy technique in treating sagittal craniosynostosisin older children. J Neurosurg 2006;105(4, Suppl)245–251
24 Koizumi T, Komuro Y, Hashizume K, Yanai A. Cephalic index ofJapanese children with normal brain development. J CraniofacSurg 2010;21(05):1434–1437
25 Netherway DJ, Abbott AH, Anderson PJ, David DJ. Intracranialvolume in patients with nonsyndromal craniosynostosis. J Neu-rosurg 2005;103(2, Suppl)137–141
26 Sgouros S. Skull vault growth in craniosynostosis. Childs Nerv Syst2005;21(10):861–870
27 Mota M, Melo A, Burak C, Daltro C, Rodrigues B, Lucena R.[Anthropometric cranial measures of normal newborn]. ArqNeuropsiquiatr 2004;62(3A):626–629
28 Di Rocco C, Massimi L. Focus Session “Changing epidemiology inpediatric neurosurgery”. Childs Nerv Syst 2009;25(07):785
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Head Measurements for the Diagnosis of Craniosynostosis CostaVal et al. 95

Chronic Subdural Hematoma SpontaneousResolution
Resolução espontânea de hematoma subdural crônico
Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 George Santos dos Passos1
Luciano José Silveira Filho1 André Luiz Cicilini2 Neiffer Nunes Rabelo3
Luiz Antônio Araujo Dias Junior1 Carlos Umberto Pereira4 Luiz Antônio Araujo Dias5
1Department of Neurosurgery, Hospital Santa Casa, Ribeirão Preto,SP, Brazil
2Medical Student, Universidade de Ribeirão Preto - Unaerp, RibeirãoPreto, SP, Brazil
3Medical Student, Faculdade Atenas, Paracatu, MG, Brazil4Department of Neurosurgery, Fundação Beneficiente Hospital deCirurgia, Aracaju, Sergipe, Brazil
5Neurosurgeon and Professor, Department of Neurosurgery, HospitalSanta Casa, Ribeirão Preto, SP, Brazil
Arq Bras Neurocir 2017;36:96–100.
Address for correspondence Nicollas Nunes Rabelo, MD,Santa Casa de Ribeirão Preto, Ribeirão Preto, São Paulo, Brazil(e-mail: [email protected]).
Keywords
► chronic subduralhematoma
► spontaneousremission
► brain injury
Abstract Introduction Chronic subdural hematoma (CSH) is a hemorrhagic brain injury thatpersists for more than 21 days after its initial formation. The incidence is predominantlyamong the elderly population (> 65 years), and varies from 58 to 74/100,000 inhabitants.Spontaneous resolution is consideredvariable; in the literature series, it is < 1–20%ofcases.Objectives To expose the CSH pathophysiological mechanisms of spontaneousresolution and some treatments that lead to hematoma volume reduction.Methods Literature review between 1971 to 2016, using the PubMed, Medline, Embase,Scielo, LILACS andCochranedatabases using key-words,with inclusion andexclusion criteria.Discussion Spontaneous resolution of the CSH pathophysiology is controversial;however, it can be attributed to four basic mechanisms: 1) outer capsule membranematuration; 2) decreased fibrinolysis; 3) bidirectional flow of blood vessels; and 4)platelet plug. Some drugs, such as mannitol, corticosteroids, tranexamic acid andatorvastatin, contribute to CSH resolution, since they change the capsule membranepermeability, and inhibit the fibrinolytic and inflammatory systems.Conclusion Spontaneous resolution is unpredictable; in some cases, it has a largetemporal evolution (of up to 6 years). It occurs in small or laminar collections,asymptomatic or with transient neurological symptoms, and the pathophysiology isstill controversial to this day. Therefore, surgical treatment should remain the firstoption, even though the conservative management is adopted for some patients.Rigorous outpatient and radiological follow-up are recommended.
receivedFebruary 5, 2017acceptedMarch 27, 2017published onlineMay 22, 2017
DOI https://doi.org/10.1055/s-0037-1603512.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Review Article | Artigo de Revisão96

Introduction
Chronic subdural hematoma (CSH) is a generally cystic collec-tion composed of liquid blood contents. In several states ofcoagulation, it is coatedbya thinfibrous capsule just below thedura mater, which lasts for more than 21 days after its initialformation.1–3 The CSH incidence in the general population isestimated at 5–13.5 cases per 100,000 inhabitants per year. Itincreases with age, and can reach up to 58–74/100,000 in-habitants among the population over 65 years old.1–4
Chronic subdural hematoma is diagnosed through a com-puted tomography (CT) of the skul,l or through magneticresonance imaging (MRI), mainly in T2 phases (echo gradi-ent) and fluid attenuated inversion recovery (FLAIR). Theimages can be taken after monitoring the brain injury orsuggestive neurological signs and symptoms, such as pro-gressive headache, contralateral motor deficit, and behavior-al changes.5–7 The CSH is constantly changing, and this isreflected in changes in the pattern of the image exams.
Surgical treatment is the gold standard for symptomaticindividualswhodonot have surgical contraindications.2 Somecases receive conservative treatment with clinical measuresand serial radiological follow-up,which is an individual choicethat is considered dangerous in some situations.1,8,9However,spontaneous resolution may occur in some cases withoutsurgical intervention, which is rare. There are a few papersreported, and with an extremely variable epidemiology inci-dence: lower than 1% to � 20%. Another important variant
found in the literature was the time for CSH spontaneousresolution, which ranged from 3weeks to 6 years, followed byclinical and radiological follow-up.8–13
The objective of the present study is to establish a reviewexposing the pathophysiological mechanisms, the time ofevolution, and the conditions that lead to the spontaneousresolution of the chronic subdural hematoma.
Methods
Literature review using the PubMed, Medline, Embase,Scielo, LILACS and Cochrane databases between 1971 and2016. The search resulted in total 34 papers on CSH. Theincluded articles associated CSH with spontaneous resolu-tion. Articles with incomplete clinical data or no statisticalrelevance were not included in this paper.
Discussion
The cases of CSH that present spontaneous resolution arelocated in small areas, mainly in the frontal region. They canbe laminar or thin, with little or no mass effect, and havecontact with the cerebrospinal fluid; they can also be oldand asymptomatic, or cause mild neurological symp-toms.11,14,15 One study showed that the average volumeof the hematoma in the spontaneous resolution group wasof 43.1 ml, and the average degree of deviation from themidline was of 6 mm.13
Resumo Introdução O hematoma subdural crônico (HSDC) é uma lesão cerebral hemorrágicaque persiste por mais de 21 dias após o começo de sua formação. A sua incidência épredominantemente na população idosa (> 65 anos), e varia de 58–74 /100.000habitantes, e sua resolução espontânea é considerada rara e variável nas séries daliteratura em < 1–20% dos casos.Objetivos Expor os mecanismos fisiopatológicos que favorecem a resolução espon-tânea do HSDC e alguns tratamentos que favorecem a redução do volume dohematoma.Métodos Revisão bibliográfica entre 1971 e 2016, utilizando as bases de dadosPubMed, Medline, Embase, Scielo, LILACS e Cochrane, por meio de palavras-chave, comcritérios de inclusão e exclusão.Discussão A fisiopatologia da resolução espontânea dos HSDCs é controversa, porémpode ser atribuída a quatro mecanismos: 1) maturação da membrana externa dacápsula; 2) diminuição da fibrinólise; 3) fluxo bidireccional de vasos sanguíneos; e 4)tampão plaquetário. Alguns medicamentos, tais como manitol, corticoesteroides,ácido tranexâmico e atorvastatina, também podem favorecer a resolução dos HSDCs,uma vez que alteram a permeabilidade da membrana da cápsula e inibem os sistemasfibrinolítico e inflamatório.Conclusão A resolução espontânea é imprevisível; em alguns casos, tem amplaevolução temporal em até 6 anos. Ocorre em coleções pequenas ou laminares,assintomáticas ou com sintomas neurológicos transitórios, e sua fisiopatologia aindahoje é controversa. Portanto, o tratamento cirúrgico deve continuar sendo a primeiraopção, embora se adote uma conduta conservadora para alguns pacientes. Oseguimento ambulatorial e radiológico rigoroso é recomendado.
Palavras chave
► hematoma subduralcrônico
► resolução espontânea► lesão cerebral
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Chronic Subdural Hematoma Spontaneous Resolution Rabelo et al. 97

Spontaneous resolution of the CSH pathophysiology iscontroversial; however, it can be attributed to four basicmechanisms: 1) outer capsule membrane maturation; 2)decreased fibrinolysis; 3) bidirectional flow of blood vessels;and 4) platelet plug. Some drugs, such as mannitol, cortico-steroids, tranexamic acid and atorvastatin also contribute toCSH resolution.11,12,15
Maturation of the External Membrane of the CapsuleThe semipermeable external membrane allows the fibrob-lasts and cytokines chemotaxis pass into collection.1,8,16
Activated by platelet-derived growth factor (PDGF), andtransforming growth factor β (TGF-β). They differentiatetissue into myofibroblasts that are organized as a smoothmuscle tissue in the lesion.17
These cells reinforce the capsule structure by stabilizing itand favoring its maturation, organization or even calcificationover time. Maturation reduces the fibrinolytic system activityand microhemorrhages by leading to the secondary matura-tion of the blood vessels. Recurrent bleeding is the startingpoint and the mainmaintenance factor of the subdural hema-toma. Therefore, the main mechanism of resolution is thematuration of the external membrane.18–20
Decreased Fibrinolytic ActivityThe fibrinolytic system in hematoma formation is increasedand leads to recurrent bleeding. In this case, the dynamicequilibriumestablished between hemostasis andfibrinolysisis interrupted, with blood recirculation greater than theability to stanch. The larger the external membrane area,the vascularization and the greater the fibrinolytic activity,more blood will increase in the hematoma.16,20,21
With the maturation of the membrane, there should bea decrease in fibrinolytic activity and the liquefaction ofthe hematoma, and hemostasis should increase. Neovascu-larization stabilized by maturation should also be anadjuvant factor. Therefore, the collection becomes stableand resorbable.12,20
Bidirectional Flow of Blood VesselsWith thematuration of the externalmembrane of the capsuleand decreased fibrinolytic activity, the collection becomesmore resorbable. The blood vessels of the subdural membranehave communicating walls that allow bidirectional flow,favoring the progressive reabsorption of the hematoma.10,22
Platelet PlugThe increased size of the hematoma is made easier by thelarge number of gap junctions of the capsule vessels thatallow sporadic blood leakage and recurrent bleeding.22,23 Aplatelet plug, stimulated by myofibroblast collagen andvascular subendothelium molecules, occupies the gap junc-tions of the vessels, reducingmicrohemorrhages and the sizeof the subdural hematoma.22
The platelet thrombus is classically desecrated by initia-tion (platelet adhesion), extension (activation, adhesion andaggregation) and stabilization (thrombus stabilization), andis part of the primary hemostasis.23,24
DrugsMannitol is capable of changing capsule membrane perme-ability, thus avoiding the passage of proteins and granulocy-tes, preventing collection content increase by osmosis orchemotaxis. In a study with 20% intravenous mannitol, somepatients presented spontaneous cures over a period rangingfrom 30 to 100 days.5,25,26
Corticosteroids (CE) also change capsule membrane per-meability by the same mechanisms as mannitol. Corticos-teroids maturate and stabilize the outer membrane.Dexamethasone, for example, reduces the chance of relapsesin advanced age, of midline displacement, and of mixeddensity hematoma, which are independent factors forunilateral recurrence.27,28
In one of the reviewed studies, tranexamic acid was usedin patients submitted to hematoma drainage and in otherswho did not receive any type of treatment. In both cases, areduction of the collection was observed, and there were nocases of recurrence or increase. In another trial, spontaneousresolution was verified after 20 weeks of drug use. It isproposed that the tranexamic acid inhibits the fibrinolyticand inflammatory systems (via kallikrein); their role in thespontaneous resolution was previously explained.29,30
Atorvastatin, which has recently been investigated, caninduce spontaneous resolution of CSDHs mainly in women,with favorable grades in the Markwalder grading scale(grades 1 and 2) for evaluating the neurologic status of apatient with a CSH.31 In studies with experimental models,it has been proposed that atorvastatin induces increasedexpression of angiopoietin-1 and the vascular endothelialgrowth factor (VEGF), and reduces the expression of matrixmetallopeptidase 9 (MMP9) on the capsule outer membrane,leading to the conversion of fragile capillaries into maturevessels. This is an important contribution to hematomavolume stability, since microhemorrhages of fragile capillar-ies are a predominant factor to increase the hematoma andavoid its resolution.32,33 It is also known that atorvastatinwas able to decrease the amount of neutrophils in thecapsule and the cytokines (tumor necrosis factor alpha[TNF-α] and interleukin 6 [IL-6]) in brain tissue.34
In short, drug therapy is adjuvant, since spontaneousresolution can occur even without the use of drugs.
The present paper contributes with an algorithm showingthe chronic subdural hematoma pathophysiology interrela-tion (►Fig. 1).
Defining TherapyDrainage with immediate hematoma decompression isconsidered the first treatment. The surgical management,besides being therapeutic, reduces the chances of unfavor-able outcomes.8,9,13
Drainage is classically indicated for symptomatic indi-viduals (presenting with headache, motor deficit, alteredconsciousness, etc.) or those with imaging complications(midline deviation, basal cisterns’ compression or compres-sion of other structures of the central nervous system).8,9,13
Advanced age (> 85 years) is a contraindication fordrainage.34
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Chronic Subdural Hematoma Spontaneous Resolution Rabelo et al.98

The conservative treatment, with drugs and/or radiologicalfollow-up, is the choice of follow-up of some professionals forasymptomatic or symptomatic patients without neurologicaldeterioration. Some authors believe that in these cases therisksoutweigh thebenefits;manypatientswill needsurgery inthe future, and the risk of death is higher.8,9,13
Therefore, waiting for spontaneous resolution should notbe a definitive criterion for this type of conduct, since there isno predictability in its occurrence, or a safe period of time,and even the evidences of drug use need further studies andmeta-analyses.8,9,13
Conclusion
Generally, spontaneous resolution occurs in collections that:are located in small areas, especially in the frontal region; arelaminar; have little or no mass effect; are in contact with thecerebrospinal fluid; are old; and that cause no symptoms orlead to transient neurologic symptoms. Although its patho-physiology is not a consensus, externalmembranematurationis considered the initial and main event for its occurrence.Surgical management remains the first treatment option, andshould not be replaced by the conservative approach, with thepatient waiting for a spontaneous resolution. Therefore, the
risks outweigh the benefits, and there is no evidence in theliterature to support the effectiveness of this approach.
References1 Tanaka Y, Ohno K. Chronic subdural hematoma - an up-to-date
concept. J Med Dent Sci 2013;60(02):55–612 Sousa EB, Brandão LF, Tavares CB, et al. Epidemiological character-
istics of 778 patients who underwent surgical drainage of chronicsubdural hematomas in Brasília, Brazil. BMC Surg 2013;13:5
3 Marcikić M, Hreckovski B, Samardzić J, Martinović M, Rotim K.Spontaneous resolution of post-traumatic chronic subdural he-matoma: case report. Acta Clin Croat 2010;49(03):331–334
4 Lo W-L, Lee T-C, Fang P-S, Huang Y-H. Chronic subdural hema-toma in patients under age 65 years: A comparative study of agecohort. Formos J Surg 2013;46:10–14
5 Gattás GS. Imaging of traumatic brain injury. Rev Med São Paulo2011;4:157–168
6 Kim SC, Park SW, Ryoo I, et al. Contrast-enhanced FLAIR (fluid-attenuated inversion recovery) for evaluating mild traumaticbrain injury. PLoS One 2014;9(07):e102229
7 Fujioka S, Matsukado Y, KakuM, Sakurama N, Nonaka N, Miura G.[CT analysis of 100 cases with chronic subdural hematoma withrespect to clinical manifestation and the enlarging process of thehematoma (author’s transl)]. Neurol Med Chir (Tokyo) 198121(11):1153–1160
Fig. 1 Physiopathology of the spontaneous resolution of a chronic subdural hematoma.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Chronic Subdural Hematoma Spontaneous Resolution Rabelo et al. 99

8 Guevara DJE. Resolución espontánea de un hematoma subduralcrónico. Cir Cir 2000;68:23–25
9 Lee GS, Park YS, Min KS, Lee MS. Spontaneous Resolution of aLarge Chronic Subdural Hematoma Which Required SurgicalDecompression. J Korean Neurosurg Soc 2015;58(03):301–303
10 Parlato C, Guarracino A, Moraci A. Spontaneous resolution ofchronic subdural hematoma. Surg Neurol 2000;53(04):312–315,discussion 315–317
11 Baldawa SS, Nayak N. Spontaneous Resolution of Bilateral ChronicSubdural Hematoma. Turk Neurosurg 2015;25(05):835–836
12 Göksu E, Akyüz M, Uçar T, Kazan S. Spontaneous resolution of alarge chronic subdural hematoma: a case report and reviewof theliterature. Ulus Travma Acil Cerrahi Derg 2009;15(01):95–98
13 Kim HC, Ko JH, Yoo DS, Lee S-K. Spontaneous Resolution ofChronic Subdural Hematoma : Close Observation as a TreatmentStrategy. J Korean Neurosurg Soc 2016;59(06):628–636
14 Horikoshi T, Naganuma H, Fukasawa I, Uchida M, Nukui H.Computed tomography characteristics suggestive of spontaneousresolution of chronic subdural hematoma. Neurol Med Chir(Tokyo) 1998;38(09):527–532, discussion 532–533
15 Naganuma H, Fukamachi A, Kawakami M, Misumi S, Nakajima H,Wakao T. Spontaneous resolution of chronic subdural hemato-mas. Neurosurgery 1986;19(05):794–798
16 Rabelo NN, Silveira Filho LJ, Passos GS, et al. Acute ArterialHypertension in Patients undergoing Neurosurgery. Arq BrasNeurocir Rio de Janeiro Brazil 2016;35:296–303
17 Kawano N, Suzuki K. Presence of smooth-muscle cells in thesubdural neomembrane. J Neurosurg 1981;54(05):646–651
18 Ito U, Fujimoto T, Inaba Y. [Formation of the chronic subduralhematoma: 2. A patho-anatomical study of sequel of the trau-matic acute subdural hemorrhage (author’s transl)]. No ShinkeiGeka 1974;2(02):129–143
19 Franco RF. Fisiologia da coagulação, anticoagulação e fibrinólise.Medicina 2011;34:229–237
20 Yamashima T, Yamamoto S, Friede RL. The role of endothelial gapjunctions in the enlargement of chronic subdural hematomas.J Neurosurg 1983;59(02):298–303
21 Loh JK, Howng SL. Electron microscopic study on the outermembrane of chronic subdural hematoma. Kaohsiung J Med Sci1998;14(01):25–30
22 Yadav S, Storrie B. The cellular basis of platelet secretion:Emerging structure/function relationships. Platelets 2017;28(02):108–118
23 Gjerris F, Schmidt K. Chronic subdural hematoma. Surgery ormannitol treatment. J Neurosurg 1974;40(05):639–642
24 Suzuki J, Gjeris F, Schmidt K. Letter: Mannitol treatment ofsubdural hematomas. J Neurosurg 1974;41(06):785–786
25 Glover D, Labadie EL. Physiopathogenesis of subdural hematomas.Part 2: Inhibition of growth of experimental hematomas withdexamethasone. J Neurosurg 1976;45(04):393–397
26 Qian Z, Yang D, Sun F, Sun Z. Risk factors for recurrence ofchronic subdural hematoma after burr hole surgery: potentialprotective role of dexamethasone. Br J Neurosurg 2017;31(01):84–88
27 Iorio-Morin C, Blanchard J, Richer M, Mathieu D. Tranexamic Acidin Chronic Subdural Hematomas (TRACS): study protocol for arandomized controlled trial. Trials 2016;17(01):235
28 Kageyama H, Toyooka T, Tsuzuki N, Oka K. Nonsurgical treatmentof chronic subdural hematomawith tranexamic acid. J Neurosurg2013;119(02):332–337
29 Liu H, Liu Z, Liu Y, Kan S, Yang J, Liu H. Effect of atorvastatinon resolution of chronic subdural hematoma: a prospectiveobservational study [RETRACTED]. J Neurosurg 2016;29:1–10.DOI:10.3171/2015.12.JNS151991
30 Wang D, Li T, Wei H, et al. Atorvastatin enhances angiogenesis toreduce subdural hematoma in a rat model. J Neurol Sci 2016;362:91–99
31 Li T, Wang D, Tian Y, et al. Effects of atorvastatin on the inflam-mation regulation and elimination of subdural hematoma in rats.J Neurol Sci 2014;341(1-2):88–96
32 Wang D, Li T, Tian Y, et al. Effects of atorvastatin on chronicsubdural hematoma: a preliminary report from three medicalcenters. J Neurol Sci 2014;336(1-2):237–242
33 Munoz-Bendix C, Pannewitz R, Remmel D, et al. Outcomefollowing surgical treatment of chronic subdural hematoma inthe oldest-old population. Neurosurg Rev 2016 [Epub ahead ofprint.]
34 Rabelo NN, Silveira Filho LJ, Bithencurt BNS, et al. DifferentialDiagnosis between Neoplastic and Non-Neoplastic Brain Lesionsin Radiology. Arq Bras Neurocir 2016;35:45–61
The author George Santos dos Passos and his affiliationwere placed according to the Erratum published onlineon June, 2017 (DOI https://doi.org/10.1055/s-0037-1603944).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Chronic Subdural Hematoma Spontaneous Resolution Rabelo et al.100

Axis Screw Fixation – A Step-by-Step Review ofthe Surgical Techniques
Fixação do áxis com parafusos – uma revisão passo apasso das técnicas cirúrgicas
Andrei F. Joaquim1 K. Daniel Riew2
1Department of Neurology, Discipline of Neurosurgery, UniversidadeEstadual de Campinas (UNICAMP), Campinas, SP, Brazil
2Department of Orthopedics, Columbia University, New York, NY,United States
Arq Bras Neurocir 2017;36:101–107.
Address for correspondence Andrei Fernandes Joaquim, MD, PhD,Departamento de Neurologia, Universidade Estadual de Campinas,Rua: Tessália Vieira de Camargo, 126, Cidade Universitária,13083-887, Campinas, SP, Brazil (e-mail: [email protected]).
Introduction
Fixation of the axis may be necessary in cases of atlantoaxialinstability, secondary to different causes, such as congenital,trauma, neoplasm or inflammatory diseases.1 Additionally,the axis may be included in the spinal instrumentationprocedure requiring occipitocervical stabilization or evenextension of the subaxial cervical spine surgeries.1 Theclassic fixation of the atlantoaxial region, based on wiring
techniques, such as those described by Brooks-Jenkis, Sonn-tag, Gallie, and their variations, were associated with a highrate of nonunion (up to 30% of the patients), and the need ofwearing a postoperative cervical brace (such as a rigidcervical collar or a halo-vest) because of their limited abilityto restrict C1-2 motion properly.2–5 Due to these limitations,modern fixation of the axis is mainly based on more rigidconstructions, based on instrumentation of the axis usingpolyaxial screws.1,6
Keywords
► axis► screw► lamina► pars► pedicle► transarticular
Abstract In this article, we present the techniques of axis screw fixation (laminar, pars, pedicleand transarticular screws), discussing the indications and contraindications of eachone, as well as surgical tips and anatomical landmarks.
Palavras-chave
► áxis► parafuso► lâmina► pars► pedículo► transarticular
Resumo No presente artigo, apresentamos as técnicas de fixação do áxis com parafusos (lamina,parafusos de pars, pedículo e transarticular), discutindos as indicações e contra-indicações das mesmas, assim como dicas cirúrgicas e parâmetros anatômicosrelevantes.
receivedDecember 12, 2016accepted after revisionJanuary 27, 2017published onlineMarch 31, 2017
DOI https://doi.org/10.1055/s-0037-1601455.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Review Article | Artigo de Revisão 101

Screw-based constructs at C2 have higher rates of fusionand immediate stability, being much more efficient inrestricting motion of the atlantoaxial joint than wiringtechniques. The most commonly used screw-based fixationtechniques of the axis are: laminar, pedicular, pars inter-articularis and transarticular C1-2 screws.
In this article, we described these four screw techniquesused to stabilize the axis, discussing indications and contra-indications of each one, as well as surgical tips and anatomi-cal landmarks.
Basic Surgical Anatomy of the AxisThe axis has a large vertebral body that contains the odontoidprocess, also known as dens.7 The odontoid articulates withthe anterior arch of the atlas, held in place by the transverseligament. The axis also has two pars interarticularis (alsoknown as isthmus), two pedicles, the laminae and bilateraltransverse processes (►Fig. 1).7 According to Ebrahein et al,the pedicle of the axis must be defined as the portion thatgoes from beneath the superior facet and the anteromedialregion to the transverse foramen, whereas the pars inter-articularis is the portion between the inferior and thesuperior facets (►Fig. 1).7
C2 Laminar Screw Fixation
General ConsiderationsThefirst report of laminar screw fixation of the axis is recent,published in 2004 by Wright et al.8 This technique wasconsidered to be an alternative form of fixation for the �20% of patients who have anatomic anomalies that precludethe safe use of transarticular C1–2 screw or pedicular screwfixation due to the risk of vertebral artery injury.9,10
This technique is generally made without using intra-operative fluoroscopy (free hand technique) and does pose arisk to the vertebral artery. Successful treatment of cranio-cervical fusions, atlantoaxial fixation and axis inclusion insubaxial fixation has been extensively reported in the litera-ture.11,12 However, if a laminectomy of the axis is necessaryfor decompressing the spinal cord, obviously C2 laminarscrews cannot be used.1 Additionally, it has the disadvantageof the need to use head screw extension connectors in somecases, since the rods are generally far from the screw head,due to the oblique orientation of the laminar screws com-pared with subaxial cervical lateral mass screws.
Considering the dimensions of the axis for laminar screwplacement, Cassinelli et al evaluated 420 adult specimens of
Fig. 1 (A) Posterior view of C1–2-3. 1- Posterior tubercle of C1; 2- Lamina of C2; 3- Spinous process of C2; 4- pedicle of C2; 5- Superior facet jointof C2; 6- Inferior facet joint of C2; 7- Lateral mass of C1. The vertebral artery is illustrated. (B) Lateral View of C1–2-3. 1- Posterior tubercle of C1; 2-Lamina of C2; 3- Spinous process of C2; 4- pedicle of C2; 5- Superior facet joint of C2; 6- Inferior facet joint of C2; 7- Lateral mass of C1. Thevertebral artery is illustrated. (C) Anterior View of C1–2-3. 1- Anterior tubercle of C1; 2- Dens; 3- Body of the axis; 4- Pedicle of C2; 5- Lateral Massof C1; 6- Superior facet joint of C2. The vertebral artery is illustrated. (D) Posterior view of C2 – the green area represents the region of the parsinterarticularis (the area of C2 vertebra that connects the superior and the inferior facet joint) and the red area represents the pedicle, a bonebridge of C2 that connects the vertebral body with the posterior elements). (E) Anterior view of C2 – the green area represents the region of thepars interarticularis and the red area the pedicle of the axis.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew102

C2, and reported that themean laminar thicknesswas 5.77�1.31 mm.13 In 70.6% of the specimens, the laminar thicknesswas � 5 mm and in 92.6% of them thickness was � 4.0 mm.Considering screw length, the mean feasible screw length ofthe studied samplewas 24.6� 0.23 cm, andmore than 99% ofthe specimens could receive an estimated screw length of atleast 20 mm. This study suggested that this technique can beused in the vast majority of adult patients. In pediatricpatients, a computerized tomography (CT) based study of75 children of ages 2 to 10 years (24 to 120months old), all ofthem had a lamina thickness > 3.5 mm and only 1.2% of theaxis pedicleswere less than 3.5mm thick.14 The length of thelamina and the pedicle was � 12 mm in all cases. Thisanatomical study, as well as many clinical reports, suggeststhat laminar screws can be safety used in pediatric patientsrequiring C2 screw fixation.11,13,14
Surgical TechniqueThe patient is positioned prone with the head resting in ahead holder with neutral neck position (military tuck).1,15,16
Amidline incision ismade in the posterior cervical spine, justbelow the inion level to the cervical spine. A meticuloussubperiosteal dissection is required, as well as exposure ofthe posterior arch of C1, of the spinous process, the lateralmasses and the lamina of the axis. The junction of the spinousprocess and lamina is the entry point. On one side, a smallcortical hole is performed with high speed drill in the upperportion of the spinous process-lamina junction. For example,an upper hole in the spinous process-lamina junction of theright side is made for a left laminar screw. A hand drill is usedto guide the trajectory of the screw, based on preoperative CTscan study of the length of the lamina, aligned with long axisof the contra lateral lamina directed to the laminar surface,but not too much to avoid cortical breakthrough into thespinal canal. If the dorsal lamina is perforated, there is noproblem. In fact, in osteoporotic individuals, perforation ofthe dorsal cortex insures a bicortical screw with a strongerpurchase than a purely intra-laminar screw. A small ballprobe is then used to make sure that there was no spinalcanal violation. The screw inserted is generally 3.5 to 4 mm.On the other side, another hole is performed in the spinousprocess-lamina junction, but in its inferior portion, in orderto avoid crossing both screws at the midline. The sametrajectory is made on the other side, directing the longaxis of the lamina with a hand drill, followed by a ball probeto palpate the bone trajectory and then screw insertion.
A Penfield dissector may help to palpate the inner portionof the lamina that may help directing the hand drill prior toscrew insertion.
C2 Pars Interarticularis Screw and C2Transarticular Screw
General ConsiderationsThe trajectory of C2 pars screws and the entry point areexactly the same of transarticular screws, but the latter crossthe superior portion of facet joint of C2 directly to the centerof C1 lateral mass, having a greater length (average 20 to 30
mm) compared with pars screws (average 12 to 18 mm).17
Although commonly mistaken, one has to understand thedifference between pars and pedicle screws. Understandingthe starting points and trajectories of the two screws ismandatory to identify the best one for any given patient.
In a study of 50 CT scans of adults, Hoh et al reported thatalmost 99% of them were able to receive 14 mm length parsscrews, which may provide good fixation.12
Surgical TechniqueThe patient is positioned prone with the head fixed in a headholder with neutral neck position.1,15,16 A gauze roll is placedin the patient mouth after intubation to allow anteroposteriorfluoroscopy if transarticular screws placement is planned,according to the surgeon’s preferences. A midline incision ismade in the posterior cervical spine, just below the inion levelto the subaxial cervical spine. It is mandatory to perform ameticulous subperiosteal dissection and exposure of the pos-terior arch of C1 and also the spinous process, lateral massesand lamina of the axis. The C2–3 joint is minimally exposed.The entry point is found� 3 to 5mm above the C2-3 junction,asmedial aspossiblebutwithout violating thespinal canal andthemedial portionof thepars.17–19For pars screw technique,after performing a small hole with a drill, a hand drill is madeparallel to the pars interarticularis in a lateral fluoroscopy(generally, great craniocaudal inclination is required formain-taining a parallel trajectory to the pars). It is important toevaluate the foramen transversum:most of the times, they arejustanterior to theposterior vertebral line. Then, ahanddrill ora pedicle probe is carefully used. The more vertical thetrajectory, the greater the risk to the vertebral artery. Onecancontinuetill thedrill reaches theposterior vertebral lineonfluoroscopy to avoid injury to the vertebral artery. After handdrilling, the ball probe is inserted into the pars to check anycortical violation and, if therewas no violation, the pars screwis inserted.For transarticular screws, it ismandatory to checkthe size of the pars of the axis. Sciubba et al reported that thesize of the pars of C2may be evaluated using a parasagittal CTscan reconstruction – if the entire pars of C2 can be visualizedona single imageslice, thena transarticular screwcanbesafelyinserted. Since the average CT image cuts are 3mm, if it can bevisualized on at least 2 cuts, the pedicle is likely to be greaterthan 3 mm wide. Failure to identify an anomalous mediallylocated vertebral artery may result in catastrophic injury. Themedial and superior edges of the C2 pedicle are palpated toavoidbreaking the cortical bone. Removal of theC1–2articularcartilage is recommended to improve fusion rates, especially ifiliac crest autograft is not utilized. A threaded guide pin ispreferentially used, estimating the skin entry point lateral tothe neckwith lateral fluoroscopy in the trajectory of the screwthroughout the pars and into the lateral mass of C1. If neces-sary, an auxiliary lateral stab incision is performed, at approx-imately the T2–4 area. Therefore, the skinmust bepreppedoutto the mid-thoracic spine. This additional incision minimizesthe length of the main midline skin incision, especially whenonly atlantoaxial fusion is planned (not including the subaxialcervical spine). The trajectory of the pin guide is directedtoward the center of the atlas lateral mass (on anteroposterior
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew 103

view) and toward the anterior arch (on lateral view). The pinsare then measured for proper screw length selection. Wheninserting a cannulated screw, it is necessary to make sure thatthere is a good C1-2 alignment, without any distraction at theC1–2 joints (axial support in the vertex of the head may beperformed by the auxiliary surgeon to avoid joint distraction).If an auxiliary stab incision was used, the screwdriver shouldbe passed percutaneous and then the screwmust be locked tothe screwdriver near thescrewentry point, to avoid losing it inthe paraspinous muscles. Also, frequent fluoroscopic imagesshould be obtained to make sure that the guide wire is notadvanced during the drilling and screwing, as one can inad-vertently advance it into the cranium. After bilateral screwinsertion, the lamina of the axis and the posterior arch of theatlas aredecorticated for receivingbonegraft. A supplementedwiring technique in the posterior arch of C1 and the lamina ofC2 may be performed to improve fusion rates at surgeon’sdiscretion.17,18
Attention
• total reduction of the C1–2 joint is necessary for trans-articular screw placement. Preoperative traction may beused for reduction. In cases where total reduction is notpossible, lateral mass screw fixation of the atlas should beperformed, with another isolated C2 screw fixation tech-nique (pedicle, pars or lamina screws). One can alsoreduce the joint intraoperatively using cables under C1and around C2.
• checking the vertebral artery position on preoperative CTscan is mandatory: amedially located vertebral artery is aformal contraindication for transarticular screws.
• biplanar fluoroscopy is strongly recommended for trans-articular screws: poor visualization may increase thelikelihood of a malpositioned screw.
• excessive cranial angulation may result in violation of thecondyle-C1 joint; an inferior trajectory may result ininadequate fixation of the C1 lateral mass; a too medialtrajectory results in injury to the spinal cord and toolateral trajectory results in additional risk of vertebralartery injury.
• if one vertebral artery is injured, the surgeon should notinsert a contra lateral screw, since bilateral vertebralinjury may result in death or catastrophic stroke.17,18
C2 Pedicle Screw
General ConsiderationsThe pedicle is the region connecting the C2 vertebral bodywith the posterior elements of the axis and a true pediclescrew passes obliquely to the pedicle, toward the body of theaxis. The first description of the C2 transpedicular screwwasprobably made by Robert Judet, in France, in 1962.
Surgical TechniquePositioning and exposure are identical to the pars screw,described above. Since a pedicle screw starting point is morerostral, the C2–3 joint does not need to be exposed. The entrypoint is found in the transition between the lateral portions
of the lateral mass of C2, a little inferior (� 2 mm) to thetransition of the lateral mass-pars. If one draws an imaginaryline extending the rostral border of the C2 lamina, this is agood starting point in the cranial-caudal direction. This is ahigh and lateral entry point, potentially minimizing the riskof vertebral artery injury. With a dissector, the medial androstral portions of the pedicle of C2 are palpated, guiding thetrajectory of thehanding drill. Themedial and rostral corticalbone of the pedicle should not be violated. Canal penetrationoccurswith amedial violation and vertebral artery injury canoccur with a lateral violation. The caudal-rostral trajectory isparallel to the slope of the C2 pars, or may be guided bylateral cervical fluoroscopy, directed toward C2 body.20 Afterdrilling, a ball-tipped probe is used to make sure that therewas no cortical violation or excessive bleeding, and properscrew length is measured and inserted. Generally, venousbleeding suggests transverse foramen violation, and arterialbleeding suggests vertebral artery injury.
Attention
• similarly to transarticular screws, assessment of thewidth of the C2 pedicle is mandatory for transpedicularscrews: the same rule is valid, as reported by Sciubba et al:if the entire pedicle of C2 can be visualized on a singleimage slice of a parasagittal CT scan, that means that thepedicle is greater than 3 mmwide and pedicle screws canbe safely performed.20
• in fractures of the posterior elements of the axis, generallythe fracture’s line can be palpated with a Penfield dissec-tor. Surgeons must be aware of this to avoid deviation ofthe screw direction.
• up to 20% of patients do not have pedicles of a sufficientsize to receive a screw – in such cases, consider a parsscrew, a laminar screw or wiring/hook techniques.
►Fig. 2 and 3 illustrate the differences among the screwtechniques and an illustrative case is also presented in►Fig. 4.
Final Considerations
Biomechanical studies assessing insertional screw torqueand pull-out strength reported that C2 pedicle screws mayprovide the strongest fixation, followed by laminar and,finally, by pars screws.21 However, further studies are nec-essary to validate the biomechanical studies in clinicalcontext. In a large series of 167 patients, Parker et alevaluated the differences between C2 pedicle screws andC2 laminar screws (used when pedicle fixation presentedpotential anatomic risks).22 Grouping patients with upper(C1-2 or C1-2-3 fixation) and subaxial cervical spinefixation,they reported a higher rate of cortical violation with pediclescrews (11 cases, 7%, none requiring surgical revision) thanwith laminar screws (2 cases, 1.3%, 1 requiring a surgicalrevision) (p ¼ 0.018). It is worth noting that the pseudoarth-rosis rate was higher in the subaxial group receiving laminarfixation (4 patients were reoperated; 6.1%) than in thepedicle screw group (no reoperation). All of the pseudoarth-rosis occurred in the subaxial cervical spine group. They
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew104

Fig. 2 (A) Posterior view of C1–2-3. 1- Illustrated perspective of the trajectory of the C2 pedicle screw and entry point: we start in line with thecranial edge of the C2 lamina and just lateral to the midpoint of the C2 pars; the more caudal the starting point, the harder it is to get into thepedicle and the easier it is to hit the artery. 2- Trajectory of the C2 pars screw and entry point, just superior and slightly lateral to the medialjunction of the C2–3 joint (� 3 to 5 mm above the junction, as medial as possible but without violating the spinal canal and the medial portion ofthe pars). 3- Trajectory of the C2 transarticular screw, with the same entry point of C2 pars screw. (B) Lateral View of C1–2-3. 1- Lateralperspective of the trajectory of the C2 pars screw. (C) Lateral View of C1–2-3. 1- Lateral perspective of the trajectory of the C2 transarticularscrew. (D) Posterior view of C1–2-3. Illustrated perspective of the trajectory of bilateral C2 laminar screws and their respective entry points, inthe junction of the lamina and the spinous process.
Fig. 3 Illustrative pictures of the screw trajectories based on CT scan. (A) Axial view of the C2 CT scan. Laminar screws are illustrated. (B) Axialview of the C2 CT scan. 1- Pars screw (right) and 2- Pedicle screw (left). The vertebral artery is illustrated. (C) Lateral view of the sagittal CT scan.The trajectory of the C2 pars screw is illustrated. (D) Lateral view of the sagittal CT scan. The trajectory of the C2 transarticular screw isillustrated.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew 105

concluded that using laminar screws in extension of subaxialcervical spine groups may increase the risk of pseudoarth-rosis when comparedwith pedicle fixation. Regardless of thetype of screw, a sufficient length of axis screw fixationprovides rigid fixation with all the presented techniques.
Finally, spine surgeons should be familiar with all thescrew techniques for fixating the axis, as well as theirtechnical nuances, selecting the best option for each patient.
Conflicts of interestNo funds were received in support of this study. Nobenefits in any form have been or will be received froma commercial party related directly or indirectly to thesubject of this manuscript. The authors have no financialinterest in the subject of this article.
Quiz – Additional Information for Residents(►supplementary material)
References1 Joaquim AF, Ghizoni E, Anderle DV, Oliveira Ed, Tedeschi H. Axis
instrumentation: surgical results. Arq Neuropsiquiatr 2012;70(11):857–863
2 Farey ID, Nadkarni S, Smith N. Modified Gallie technique versustransarticular screw fixation in C1-C2 fusion. Clin Orthop RelatRes 1999;(359):126–135
3 Dickman CA, Sonntag VK. Posterior C1-C2 transarticular screwfixation for atlantoaxial arthrodesis. Neurosurgery 1998;43(02):275–280, discussion 280–281
4 Coyne TJ, Fehlings MG, Wallace MC, Bernstein M, Tator CH.C1-C2 posterior cervical fusion: long-term evaluation of resultsand efficacy. Neurosurgery 1995;37(04):688–692, discussion692–693
5 Rajinda P, Towiwat S, Chirappapha P. Comparison of outcomesafter atlantoaxial fusion with C1 lateral mass-C2 pedicle screwsand C1-C2 transarticular screws. Eur Spine J 2016 Oct 2
6 Jeanneret B, Magerl F. Primary posterior fusion C1/2 in odontoidfractures: indications, technique, and results of transarticularscrew fixation. J Spinal Disord 1992;5(04):464–475
7 Ebrahein NA, Fow J, Xu R, Yeasting RA. The location of the pedicleand pars interarticularis in the axis. Spine 2001;26(04):34–37
8 Wright NM. Posterior C2 fixation using bilateral, crossing C2laminar screws: case series and technical note. J Spinal DisordTech 2004;17(02):158–162
9 Mandel IM, Kambach BJ, Petersilge CA, Johnstone B, Yoo JU.Morphologic considerations of C2 isthmus dimensions for theplacement of transarticular screws. Spine 2000;25(12):1542–1547
10 Igarashi T, Kikuchi S, Sato K, Kayama S, Otani K. Anatomic study ofthe axis for surgical planning of transarticular screw fixation. ClinOrthop Relat Res 2003;(408):162–166
11 Singh B, Cree A. Laminar screw fixation of the axis in the pediatricpopulation: a series of eight patients. Spine J 2015;15(02):e17–e25
12 Hong JT, Yi JS, Kim JT, Ji C, Ryu KS, Park CK. Clinical and radiologicoutcome of laminar screw at C2 and C7 for posterior instrumen-tation–review of 25 cases and comparison of C2 and C7 intrala-minar screw fixation. World Neurosurg 2010;73(02):112–118,discussion e15
Fig. 4 Illustrative Case. (A) Lateral cervical X-ray shows destruction of the body of C2 (an osteolytic lesion, confirmed as a giant cell tumor afteran anterior cervical biopsy), with anterior dislocation of the atlas over C2. (B, C and D) sagittal CT scan showing destruction of the dens, body,pars and pedicle of C2, precluding screw fixation on these structures. (E) Coronal CT scan and the lytic injury (F) Intraoperative view of C1 lateralmasses screw fixation, bilateral laminar screws and C3 lateral masses screws. Note that connectors from the head of the C2 screws are used forattaching properly to the rods (G and H). Postoperative cervical X-rays (lateral and antero-posterior, respectively) with good alignment of theupper cervical spine. (I) Laminar screws in the axial CT scan.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew106

13 Cassinelli EH, Lee M, Skalak A, Ahn NU, Wright NM. Anatomicconsiderations for the placement of C2 laminar screws. Spine2006;31(24):2767–2771
14 Cristante AF, Torelli AG, Kohlmann RB, et al. Feasibility of in-tralaminar, lateral mass, or pedicle axis vertebra screws inchildren under 10 years of age: a tomographic study. Neurosur-gery 2012;70(04):835–838, discussion 838–839
15 Joaquim AF, Ghizoni E, Rubino PA, et al. Lateral mass screwfixation of the atlas: surgical technique and anatomy. WorldNeurosurg 2010;74(2-3):359–362
16 Mudo ML, Amantéa AV, Cavalheiro S, Joaquim AF. Intraoperativeradiological visualization of the occipito-cervical transition andupper cervical spine: technical note. Columna 2009;8:197–199
17 Yanni DS, Perin NI. Fixation of the axis. Neurosurgery 2010;66(3, Suppl)147–152
18 Menendez JA, Wright NM. Techniques of posterior C1-C2 stabi-lization. Neurosurgery 2007;60(01, Suppl 1):S103–S111
19 Puschak TJ, Anderson PA. Posterior C1–C2 Transarticular Screws.Tech Orthop 2002;17(03):296–305
20 Sciubba DM, Noggle JC, Vellimana AK, et al. Radiographic andclinical evaluation of free-hand placement of C-2 pedicle screws.Clinical article. J Neurosurg Spine 2009;11(01):15–22
21 Lehman RA Jr, Dmitriev AE, Helgeson MD, Sasso RC, Kuklo TR,Riew KD. Salvage of C2 pedicle and pars screws using theintralaminar technique: a biomechanical analysis. Spine 2008;33(09):960–965
22 Parker SL, McGirt MJ, Garcés-Ambrossi GL, et al. Translaminarversus pedicle screw fixation of C2: comparison of surgicalmorbidity and accuracy of 313 consecutive screws. Neurosurgery2009;64(05, Suppl 2):343–348, discussion 348–349
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Axis Screw Fixation Joaquim, Riew 107

Revisiting Retrograde Ventriculosinus Shunt as anAlternative for Treating Hydrocephalus in Children
Revisitando a derivação ventriculosinusal retrógrada comouma alternativa para tratamento de hidrocefalia emcrianças
Matheus Fernandes Oliveira1 Manoel JacobsenTeixeira1 Marcelo Lima Oliveira1 Edson Bor Seng Shu1
Fernando Campos Gomes Pinto1
1Nuerosurgery Division, Hospital das Clínicas, Faculdade de Medicina,Universidade de São Paulo, São Paulo, São Paulo, Brazil
Arq Bras Neurocir 2017;36:108–116.
Address for correspondence Matheus Fernandes Oliveira, PhD,Instituto de Assistência Médica ao Servidor Público Estadual, Av.Ibirapuera, 981 - Vila Clementino, 04038-034, São Paulo, SP, Brazil(e-mail: [email protected]).
Keywords
► hydrocephalus► ventriculosinus shunt► treatment► review
Abstract Introduction Retrograde ventriculosinus shunt (RVSS) is a useful option in the dailyroutine of neurosurgeons dealing with hydrodynamics. The objective of this manu-script is to review the main data about RVSS.Methods We performed a critical review. The keywords used were hydrocephalus,shunt, venous sinus, ventriculosinus shunt, retrograde ventriculosinus shunt, and sagittalsinus. The search was performed in the Medline (Pubmed) and EMBASE databases.Results Van Canneyt et al (2008) and Pinto et al (2016) performed experimentalstudies confirming the effectiveness of RVSS. El Shafei et al (1985, 1987, 2001) authorsreported several cases treated with efficacy and few complications. Oliveira et al (2015,2016) compared RVSS and ventriculoperitoneal shunt (VPS) in the treatment ofhydrocephalus after myelomeningocele repair in infants, with similar functionalresults. Oliveira et al (2015, 2016) also described the applicability of RVSS in situationswhen VPS is not feasible, or when the peritoneum is not useful.Discussion Retrograde ventriculosinus shunt is a safe and more physiological option,which requires the use of less prostheticmaterial. It is feasible and applicable. Especiallyin children, it generates a normotensive state after shunting, allowing centrifugal headgrowth, once there is no intracranial hypotension due to overdrainage, which mayreflect in long-term better psychomotor development.Conclusions The surgical technique of RVSS is feasible. The clinical results arecomparable with those of the VPS.
Resumo Introdução A derivação ventriculosinusal retrógrada (DVSR) deve ser uma opção narotina de neurocirurgiões que trabalham com hidrodinâmica. O objetivo deste estudo érevisar os principais dados sobre DVSR.
receivedNovember 3, 2016acceptedApril 12, 2017published onlineJune 12, 2017
DOI https://doi.org/10.1055/s-0037-1603808.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Review Article | Artigo de Revisão108

Introduction
Treating hydrocephalus has always been challenging, espe-cially in children. One century ago, there were no feasibleoptions to treat hydrocephalus, and the natural history of thedisease was death by intracranial hypertension or progres-sive enlargement of the cranial vault in infants.1–7
The Twentieth Century witnessed a dramatic change inthe comprehension of the disease, the surgical apparatus andthe development of materials to enable shunting of thecerebrospinal fluid (CSF) from the ventricles to other sterilebody cavities. From neuroendoscopy to shunt valve technol-ogies, we could follow significant changes in the paradigmsof the treatment of hydrocephalus.2,8–27
However, since the 1990s, a few improvements changedthe learning curves and the outcome of the hydrocephalustreatment. Currently, ventriculoperitoneal shunt (VPS) isthe mainstay for treatment, as well as endoscopic thirdventriculostomy (ETV), which is advocated in specificcases. Over the past decades, shunt revision rates becamestable, reaching over 70% of cases in a lifetime. Endoscopicthird ventriculostomy also has known limitations, espe-cially in patients with myelomeningocele and Chiaritype II.5–7,28
Ventriculosinus shunt (VSS), specifically when performedin a direction opposite to the blood flow, as described byIsmail El Shafei in the 1980’s, is a useful option in the dailyroutine of neurosurgeons dealing with hydrodynamics. Al-though recent experiences with VSS are scarce, we believethey should be discussed once more and linked to the classicstudies by El Shafei.6,7,29–31
The objective of this manuscript is to discuss new clinicaldata about retrograde ventriculosinus shunt (RVSS) and linkthem to the pertinent literature.
Methods
We performed a critical review to address the application,advantages and disadvantages of RVSS to treat hydrocephalus,especially in children. The keywords usedwerehydrocephalus,shunt, venous sinus, ventriculosinus shunt, retrograde ventri-culosinus shunt, and sagittal sinus. Thesearchwasperformed inthe Medline (Pubmed) and EMBASE databases.
All manuscripts were included. A review of the retrievedreferences was also performed to find crossed references.Any references known by the authors were also included.
Results
Since Toma et al5 published a full review about VSS in 2010,only 5 manuscripts updated the subject, 1 by El-Shafei et al,and 4 by Oliveira et al and Pinto et al. In the present article,we discuss the evolution of the technique and its currentresults.6,8,10,22,25,28,32–34
ReviewGartner, in 1896, suggested that the most physiological wayto treat hydrocephalus would be a connection of the ven-tricles with the venous blood system of the head and neck.Portnoy proposed that the perfect system to treat hydro-cephalus would be the one that allowed for CSF drainage,could keep intracranial pressure (ICP) normal, andwould notcause complications.3,5,14,20,26,27
Ventriculoperitoneal shunt (VPS) is the preferred optionto treat hydrocephalus, even though it has a revision rate ofmore than 70% of patients throughout their lifetime, and of30% of patients in thefirst year. An important complication isthe siphoning phenomenon, which leads to over drainageand subdural effusions.35,36
Métodos Realizamos uma revisão crítica. As palavras-chave usadas foram hydroce-phalus shunt, venous sinus, ventriculosinus shunt, retrograde ventriculosinus shunt, esagittal sinus. A busca foi feita nas bases de dados Medline (Pubmed) e EMBASE.Resultados Van Canneyt et al (2008) e Pinto et al (2016) realizaram estudosexperimentais confirmando a eficiência do DVSR. El Shafei et al (1985, 1987, 2001)relataram vários casos tratados com eficiência e poucas complicações. Oliveira et al(2015, 2016) compararam DVSR e derivação ventriculoperitoneal (DVP) no tratamentode hidrocefalia após reparo de mielomeningocele em crianças, obtendo resultadosfuncionais similares. Oliveira et al (2015, 2016) também descreveram a aplicabilidadedo DVSR em situações em que o DVP não é possível, ou o peritônio é hostil.Discussão A DVSR é uma opção segura e mais fisiológica, que requer menos materialprotético; é factível e aplicável. Particularmente em crianças, gera um estado normo-tenso após o shunt, permitindo crescimento cefálico centrífugo, uma vez que não hámais hipotensão intracraniana devido à hiperdrenagem, o que pode refletir em melhordesenvolvimento psicomotor em longo prazo.Conclusões A técnica cirúrgica DVSR é viável. Os resultados clínicos se são comparáv-eis à DVP.
Palavras-chave
► hidrocefalia► shunt ventrículo-
sinusal► tratamento► revisão
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al. 109

Siphoning leads to over drainage of the intracranial CSF intothe distal site when the patient with VPS is in the orthostaticposition. To solve this problem, anti-siphoning devices (ASDs)were added to the VPS line, increasing the pressure of thedrainage systemas the patient raises the head, thus decreasingthe drainage of the CSF. Some of them include gravitationaldevices, which change the pressure of thewhole liquid columnaccording toa rangeofheadpositions, allowingdifferentgradesof additional pressure. However, such solutions did not elimi-nate thehydrodynamic phenomenon of siphoning, and signifi-cantly increased the cost of the prosthesis.8–18,29,32–44
In thebeginningof theXXI century, Aschoff stated that therewere more than 300 shunt systems available; however, nonecould reachwhatwasproposedbyGartnerandPortnoy. Severalsites to perform the shunt were also tried, from the gallbladderto the bladder, but the peritoneal cavity was the site in whichthe procedure reached higher accuracy and effectiveness.5
In the 1940’s, Ingraham induced hydrocephalus in dogsand performed treatment with an anterograde ventriculo-jugular shunt; however, the distal end of the catheter ob-structed due to siphoning. When positioning the catheteragainst the blood flow, the catheter flow would be laminar,and there would be no turbulence zone, which wouldprevent blood clotting and catheter obstruction.14
This hemodynamic principle was demonstrated in thestudies by El Shafei and El-Rifaii. Another principle that wasalso demonstrated by these authors was the fact that theinternal jugular vein, which collapses in the orthostaticposition, has the capacity to work as a physiological anti-siphoning system. Thus, to use this natural property, anyventriculovenous shunt catheter should have the distalextremity located proximally to the internal jugular vein,in the opposite direction of the blood stream. Thus, there isan improvement in hemodynamics with the removal of theregions of turbulence, and the avoidance of back flow andthrombosis (►Fig. 1).8,29,32–34,40–44
RVSS Technique and VariationsEl-Shafei et al pioneered the technique by performing apuncture in the retrograde direction of the blood flow inthe superior sagittal sinus (SSS) using the pressure impact ofthe blood flow in the dural sinuses to maintain the CSFpressure greater than the dural sinus pressure, regardless ofchanges in posture or intrathoracic pressure (►Fig. 2). Theseauthors modified their technique later by adding a valve ofvery low pressure, recognizing that, in the event of a reduc-tion in intracranial pressure (ICP) due to lumbar puncture orsudden change of heart output, some retrograde flow ofvenous blood to the distal catheter could hinder the shunt.They also broke new ground by using transcranial Doppler(TCD) data to indirectly evaluate cerebral hydrodynamicsthrough the cerebral blood flow velocities.8,29,32–34,40–44
The surgical technique as described by El-Shafei et alinvolves two cranial burr holes in the same arcuate incisionin the scalp on the parietal region. One burr hole is in theposterior parietal bone (Frazier point), and the other, in themiddle third of the sagittal sinus. A small opening is made inthe dura mater of the parietal incision, the lateral ventricle is
punctured, and then, a small opening is made in the sagittalsinus, and the catheter is inserted � 2 cm against thedirection of the blood flow (►Fig. 3). El-Shafei et al publishedthe results with the use of a single catheter and with theassociation of a very low pressure gradient valve (just to addanother mechanism to avoid back flow).8,29,32–34,40–44
In the small but increasingexperienceofour group,wehaveadopted the classic techniqueby El-Shafei et alwith avalveless
Fig. 1 In the upstream region of the obstacle, there will be an impactzone, whereas in the downstream region, there will be a weak zone.
Fig. 2 RVSS design.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al.110

catheter. However, in adult patients, we have changed land-marks for ventricular and superior sagittal sinus (SSS) punc-ture. We used a frontal incision to enable the puncture inKocher’s point, and another incision over the SSS to allow for1burr hole in the middle third of the sagittal sinus, � 3 cmbehind thebregma.The lateral ventricle ispunctured, and thena small opening ismade in the SSS, and the catheter is inserted� 2 cm against the direction of the blood flow. The catheterused to perform the shunt is, by convenience, the PS Medicalvalve (Medtronic, Dublin, Ireland) ventricular catheter, whichis already in routine use at our institution. The ventricular
catheter is the only one applied without the use of a valvesystem (►Fig. 4).10,21,22
Another potential option designed by our group, but withlimited application until now, is the fragmentation of thecatheter in two parts: one catheter for the ventricularpuncture, and another for the SSS puncture. Then, themarginof one catheter has a connector to allow the connection ofboth catheters. The last variation with no clinical applica-tions described in the literature is a combination of twocatheters of different diameters connected as describedbefore (►Fig. 5). Using this rationale, it would be possible
Fig. 3 Phases of the surgical technique. Positioning and arcuate incision. Opening with medial and lateral burr holes. Catheterization of lateralventricle and superior sagittal sinus. Hemostasis. Closure with pericranium and skin closure.
Fig. 4 Retrograde ventriculosinus shunt after failed ventriculoperitoneal shunt. Left ventricular puncture followed by burr hole over the SSS andpuncture.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al. 111

to increase or decrease flow resistance and, therefore, therisk of back flow. However, these ideas should be furtherdiscussed in experimental and clinical bases.10,21,22
Experimental Basis for RVSSVan Canneyt et al performed an experimental study to analyzeRVSS. Firstly, an experimentalmodel of the cerebral ventricles,the arachnoid villi, the cortical veins, and the SSS was built.Secondly, a numerical model of the cortical veins and the SSSwas built. No over drainage was found in the antegrade or theretrogradepositions of the shunt. Blood reflowwasonly foundwhilemimicking lumbar puncture or changes in positionwiththe experimentalmodel (lowering the intracranial pressure orincreasing the sinus pressure rapidly). These authors sug-gested that the main advantages of this method include shortlength of derivation and prevention of siphoning. After anexperimental analysis, they concluded that when the catheteris placed in an anterograde manner, the pressure at thecatheter tip is 3.3 Pa, which is lower than that of the SSS. Inthe backward position, the catheter tip pressure was 16.7 Pa,serving as a protection against overdrainage.6,12–15,25,26
Pinto et al proposed and designed an animal experimentalmodel for RVSS using mongrel dogs and inducing hydroceph-alus with kaolin. They stated that the RVSS technique wasfeasibleandevensimple,not requiringa large learningcurve.25
In the dogs with the RVSS model, they could successfullyinduce hydrocephalus and its clinical features. The surgicalprocedure finished with no remarks, however they failed topredict that the external diameter of the catheter used(2.5 mm) would prevent the normal blood flow through theSSS, which also has a 2.5 mm caliber, resulting in cerebralvenous infarction due to venous blood stasis and drainageblocking of thehypertensive CSFaccumulated in theventricles(►Fig. 6). Thus, they proposed changing the external diameterof the catheter to adapt to canine anatomy and proportions.25
Clinical Basis for RVSSEl Shafei is surely the most important name in the experi-mental and clinical development of RVVSs. Thefirst article hepublished (along with another author) in 2001 included 56
patients and was followed by a second article with otherauthors in 2005, which included 54 patients, producing atotal of 110 patients reviewed retrospectively; 99 patientshad valveless catheters, and 11 had catheters with lowpressure valves.8–13,29,32–34,40–44
In 2010, they published the last experience. During the past40 years, 229 RVVSs were implanted; 219 patients (95.63%)benefited from the shunt, and only 2 of them needed a singleshunt revision. The manifestations of increased intracranialpressure disappeared, different degrees of regression of theventriculomegaly occurred in patients with closed craniums,but not in infants and young childrenwith open craniums, andthere were no problems related to improper CSF drainage orvenous thrombosis. The follow-up period is of up to 40 years(mean 9 years 8 months).8–13,29,32–34,40–44
El-Shafei showed that, in children, the clinical improvementoccurred immediately after shunt insertion with normoten-sive fontanelle and disappearance of the hairy scalp engorgedveins, with gradual relief of eye signals. The psychomotordevelopmentof thepatientswas satisfactory.8–12,29,32–34,40–44
Paul C. Sharkey, in 1965, published his experience with 4pediatric patients. Fourteen years later, in 1979, Cecil J. Hashpublished a series of 36 procedures. And Wen reported 15cases of obstructive hydrocephalus in 1965, and thenchanged his technique in 52 patients in the pediatric agegroup, and published the results in 1982.5
Børgesen, Gjerris and Agerlin also applied the technique.Thefirst serieswas published in 2001. The second articlewaspublished in 2004 with two extra authors, and included thefollow-up results of 45 patients from Denmark, Italy andNorway.1,5,45
Most series treated all kinds of hydrocephalus in childrenand adults of all age groups. However, cases of spina bifidawere excluded. All authors reported clinical and radiologicalimprovement. The clinical findings, such as headache, nau-sea, vomiting and papilledema changed after the surgery.5
The follow-up period and shunt revisionswere variable. Therevision rate varied between 11.8% and 37.5%. Most patientshada shorter follow-upperiod. Inhealthyyoung children, braingrowth causes an increase in the thickness of the cerebral
Fig. 5 Option for retrograde ventriculosinus shunt catheter, with twocatheters of different diameters connected.
Fig. 6 Catheterization of the superior sagittal sinus (SSS) in a caninemodelof retrograde ventriculosinus shunt. The catheter had almost the samediameter as the SSS, so there was venous blockage and infarction.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al.112
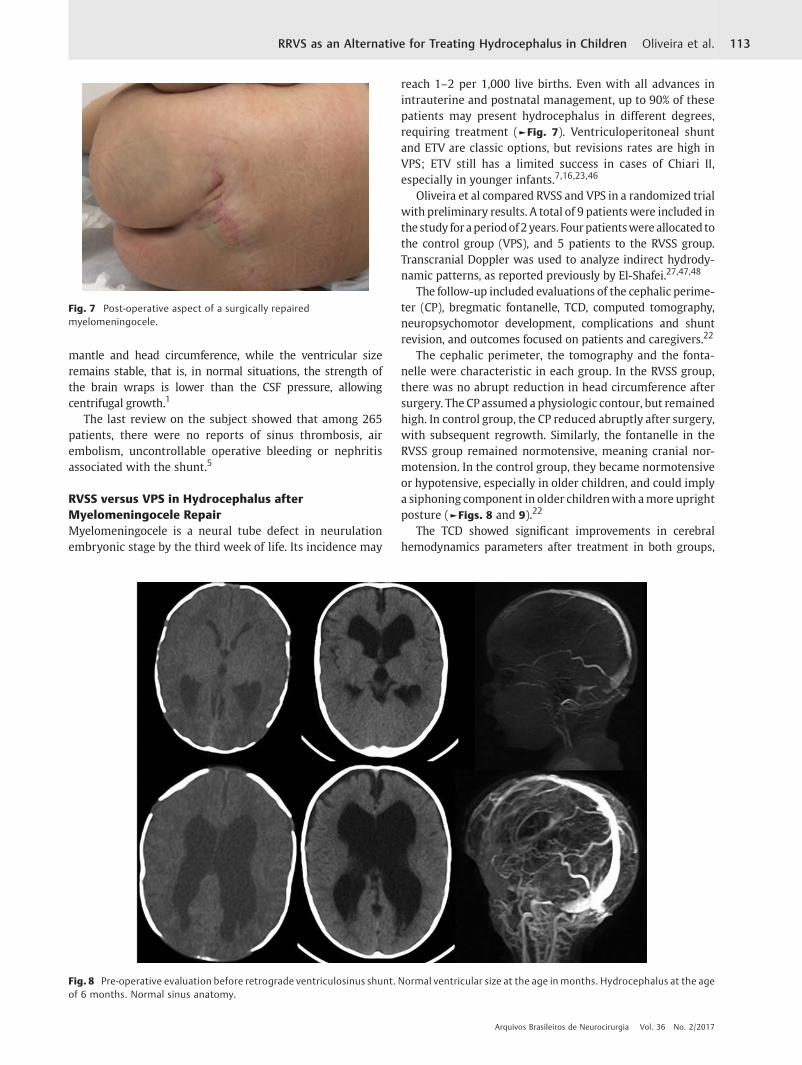
mantle and head circumference, while the ventricular sizeremains stable, that is, in normal situations, the strength ofthe brain wraps is lower than the CSF pressure, allowingcentrifugal growth.1
The last review on the subject showed that among 265patients, there were no reports of sinus thrombosis, airembolism, uncontrollable operative bleeding or nephritisassociated with the shunt.5
RVSS versus VPS in Hydrocephalus afterMyelomeningocele RepairMyelomeningocele is a neural tube defect in neurulationembryonic stage by the third week of life. Its incidence may
reach 1–2 per 1,000 live births. Even with all advances inintrauterine and postnatal management, up to 90% of thesepatients may present hydrocephalus in different degrees,requiring treatment (►Fig. 7). Ventriculoperitoneal shuntand ETV are classic options, but revisions rates are high inVPS; ETV still has a limited success in cases of Chiari II,especially in younger infants.7,16,23,46
Oliveira et al compared RVSS and VPS in a randomized trialwith preliminary results. A total of 9 patientswere included inthestudy foraperiodof2years. Fourpatientswere allocated tothe control group (VPS), and 5 patients to the RVSS group.Transcranial Doppler was used to analyze indirect hydrody-namic patterns, as reported previously by El-Shafei.27,47,48
The follow-up included evaluations of the cephalic perime-ter (CP), bregmatic fontanelle, TCD, computed tomography,neuropsychomotor development, complications and shuntrevision, and outcomes focused on patients and caregivers.22
The cephalic perimeter, the tomography and the fonta-nelle were characteristic in each group. In the RVSS group,there was no abrupt reduction in head circumference aftersurgery. The CP assumed a physiologic contour, but remainedhigh. In control group, the CP reduced abruptly after surgery,with subsequent regrowth. Similarly, the fontanelle in theRVSS group remained normotensive, meaning cranial nor-motension. In the control group, they became normotensiveor hypotensive, especially in older children, and could implya siphoning component in older childrenwith amore uprightposture (►Figs. 8 and 9).22
The TCD showed significant improvements in cerebralhemodynamics parameters after treatment in both groups,
Fig. 7 Post-operative aspect of a surgically repairedmyelomeningocele.
Fig. 8 Pre-operative evaluation before retrograde ventriculosinus shunt. Normal ventricular size at the age in months. Hydrocephalus at the ageof 6 months. Normal sinus anatomy.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al. 113
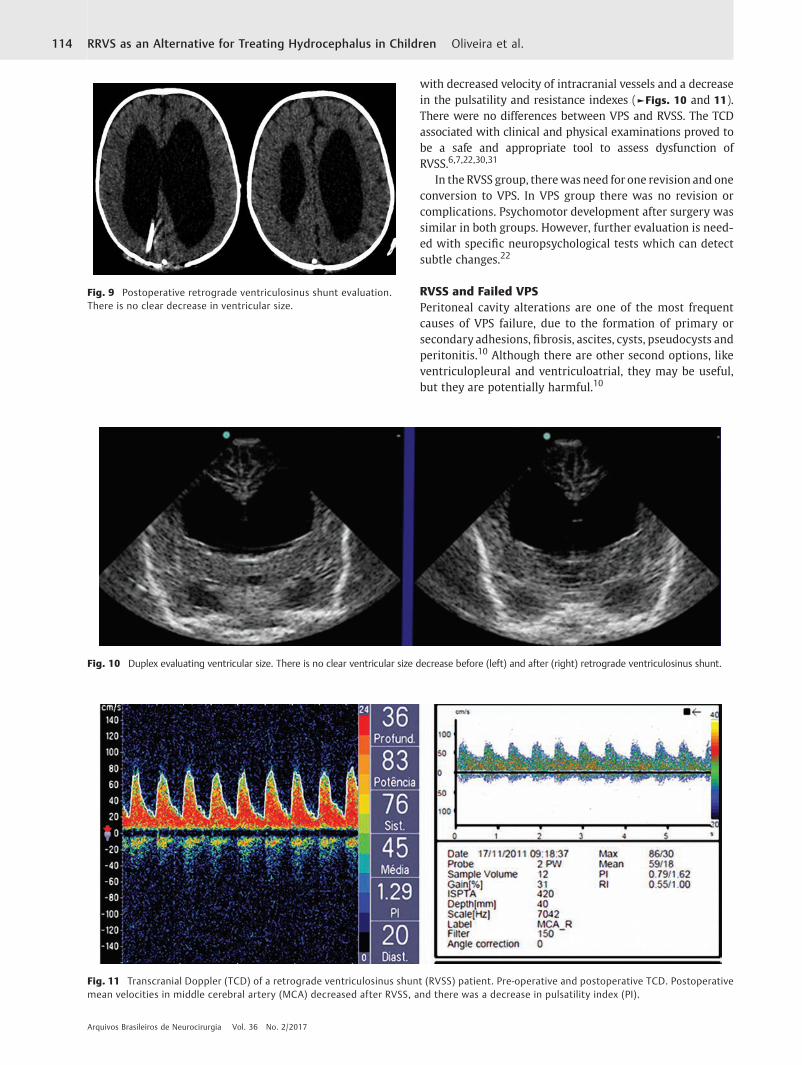
with decreased velocity of intracranial vessels and a decreasein the pulsatility and resistance indexes (►Figs. 10 and 11).There were no differences between VPS and RVSS. The TCDassociated with clinical and physical examinations proved tobe a safe and appropriate tool to assess dysfunction ofRVSS.6,7,22,30,31
In the RVSS group, therewas need for one revision and oneconversion to VPS. In VPS group there was no revision orcomplications. Psychomotor development after surgery wassimilar in both groups. However, further evaluation is need-ed with specific neuropsychological tests which can detectsubtle changes.22
RVSS and Failed VPSPeritoneal cavity alterations are one of the most frequentcauses of VPS failure, due to the formation of primary orsecondary adhesions, fibrosis, ascites, cysts, pseudocysts andperitonitis.10 Although there are other second options, likeventriculopleural and ventriculoatrial, they may be useful,but they are potentially harmful.10
Fig. 9 Postoperative retrograde ventriculosinus shunt evaluation.There is no clear decrease in ventricular size.
Fig. 11 Transcranial Doppler (TCD) of a retrograde ventriculosinus shunt (RVSS) patient. Pre-operative and postoperative TCD. Postoperativemean velocities in middle cerebral artery (MCA) decreased after RVSS, and there was a decrease in pulsatility index (PI).
Fig. 10 Duplex evaluating ventricular size. There is no clear ventricular size decrease before (left) and after (right) retrograde ventriculosinus shunt.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al.114

Oliveira et al described three cases of RVSS applied insituations when VPS is not feasible, or the peritoneum is notuseful. In one case, there was refractory ascites; in another, aperitonitis, and in the last, pseudocyst formation. In all threecases, the patients were adults and tolerated RVSS to treatthe underlying hydrocephalus. One patient needed revisionsurgery to reposition the catheter, which was not inside theSSS. Although applied in adults, this experience also shedslight over the potential use of RVSS in children with a hostileperitoneum.10
Discussion
Retrograde ventriculosinus shunt is a safe and more physio-logical option that requires the use of less prosthetic mate-rial. It is feasible and applicable, as long as there is perviousSSS to allow drainage of excessive CSF. It uses a natural anti-siphon device (internal jugular vein), and enables CSF drain-age inside the venous system.Manipulation of the SSS is saferthan usually believed, and one important matter is that thedural opening for the ventricular puncture should be justenough to catheterize the ventricle and avoid creating CSFleakage.8–24,29,32–34,40–44
The main advantages are the use of less prosthetic mate-rial, the safety and efficacy, respecting hydrodynamics andavoiding over drainage. The main disadvantages are: thenecessary learning curve and the possibility of retrogradeflow if a lumbar puncture is performed (which can be solvedif a low-pressure valve is added to the shunt system).Complications like dysfunction and infection are not com-mon, and overdrainage is an unlikely event.8,29,32–34,40–44
In RVSS, although there is no immediate and markedventricular size decrease (which is common in VPS), thereis stable ventricular size with improved hemodynamics andhydrodynamics revealed by a decrease in the pulsatilityindex (PI) after surgery, which is maintained in the latefollow-up. In patients with increased PI there was alsoclinical impairment, which was indicative of the need of arevision surgery.8,29,32–34,40–44,49
Especially in children, RVSS generates a normotensive stateafter shunting, allowing centrifugal headgrowth, once there isno intracranial hypotension due to over drainage, which mayreflect in long-term better psychomotor development. Addi-tionally, there is no need to operate the abdomen, avoidingcomplications of disabsortive peritoneum.12–24,49
In our sample, TCD was used successfully for diagnosticand follow-up evaluation of hemodynamics and hydrody-namics in the pre- and postoperative phases of RVSS. It wastechnically feasible in all patients, correlated closely withother clinical and imaging parameters, and was sensitive forthe identification of system malfunction.49
Conclusions
The surgical technique of RVSS is feasible. The clinical resultsare comparable with those of VPS. To date, we believe itshould be performed especially after myelomeningocele
repair in young infants, and as an alternative to failed VPSafter multiple revisions.
Conflicts of InterestThe authors have no conflicts of interest to report.
References1 Børgesen SE, Gjerris F, Agerlin N. Shunting to the sagittal sinus.
Acta Neurochir Suppl (Wien) 2002;81:11–142 Rainov NG, Weise JB, Burkert W. Transcranial Doppler sonogra-
phy in adult hydrocephalic patients. Neurosurg Rev 2000;23(01):34–38
3 Rekate HL. Selecting patients for endoscopic third ventriculost-omy. Neurosurg Clin N Am 2004;15(01):39–49
4 Samadani U,Mattielo JA, Sutton LN. Ventriculosagittal sinus shuntplacement: technical case report. Neurosurgery 2003;53(03):778–779, discussion 780
5 Toma AK, Tarnaris A, Kitchen ND, Watkins LD. Ventriculosinusshunt. Neurosurg Rev 2010;33(02):147–152, discussion 153
6 Van Canneyt K, Kips J, Mareels G, Baert E, Van Roost D, Verdonck P.Experimentalandnumericalmodellingof theventriculosinusshunt(El-Shafei shunt). Proc Inst Mech Eng H 2008;222(04):455–464
7 Warf BC. Hydrocephalus associated with neural tube defects:characteristics, management, and outcome in sub-Saharan Africa.Childs Nerv Syst 2011;27(10):1589–1594
8 el-Shafei IL. Ventriculovenous shunt against the direction of bloodflow: a new approach for shunting the cerebrospinal fluid to thevenous circulation. Childs Nerv Syst 1985;1(04):200–207
9 Faggin R, Bernardo A, Stieg P, Perilongo G, d’Avella D. Hydroce-phalus in infants less than six months of age: effectiveness ofendoscopic third ventriculostomy. Eur J Pediatr Surg 2009;19(04):216–219
10 OliveiraMF, TeixeiraMJ, Reis RC, Petitto CE, Gomes Pinto FC. FailedVentriculoperitoneal Shunt: Is Retrograde Ventriculosinus Shunta Reliable Option? World Neurosurg 2016;92:445–453
11 Fox JL, McCullough DC, Green RC. Effect of CSF shunt on ICP andCSF dynamics. II. A new technique of pressure measurement,results and concepts. J Neurol Neurosurg Psychiatry 1973;30:302–312
12 Gupta N, Park J, Solomon C, Kranz DA, Wrensch M, Wu YW. Long-termoutcomes in patientswith treated childhood hydrocephalus.J Neurosurg 2007;106(5, Suppl)334–339
13 Hash CJ, Shenkin HA, Crowder LE. Ventricle to sagittal sinus shuntfor hydrocephalus. Neurosurgery 1979;4(05):394–400
14 Ingraham FD,Matson DD, Alexander F Jr, Woods RP. Studies in thetreatment of experimental hydrocephalus. J Neuropathol ExpNeurol 1948;7(02):123–143
15 Jindal A, Mahapatra AK. Correlation of ventricular size andtranscranial Doppler findings before and after ventricular peri-toneal shunt in patientswith hydrocephalus: prospective studyof35 patients. J Neurol Neurosurg Psychiatry 1998;65(02):269–271
16 Kadri H, Mawla AA. Variations of endoscopic ventricular anatomyin children suffering from hydrocephalus associated with mye-lomeningocele. Minim Invasive Neurosurg 2004;47(06):339–341
17 Kestle JR, Walker MLJ; Strata Investigators. A multicenter pro-spective cohort study of the Strata valve for the management ofhydrocephalus in pediatric patients. J Neurosurg 2005;102(2,Suppl)141–145
18 Kondageski C, Thompson D, Reynolds M, Hayward RD. Experiencewith the Strata valve in the management of shunt overdrainage.J Neurosurg 2007;106(2, Suppl)95–102
19 Lo P, Drake JM. Shunt malfunctions. Neurosurg Clin N Am 2001;12(04):695–701, viii
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al. 115

20 Nulsen FE, Spitz FB. Treatment of hydrocephalus by direct shuntfrom ventricle to jugular vein. Surg Forum Am Coil Surg 1951;2:399–408
21 Oliveira MF, Saad F, Reis RC, Rotta JM, Pinto FC. Programmablevalve represents an efficient and safe tool in the treatment ofidiopathic normal-pressure hydrocephalus patients. Arq Neurop-siquiatr 2013;71(04):229–236
22 Oliveira MF, Teixeira MJ, Norremose KA, et al. Surgical techniqueof retrograde ventricle-sinus shunt is an option for the treatmentof hydrocephalus in infants after surgical repair of myelomenin-gocele. Arq Neuropsiquiatr 2015;73(12):1019–1025
23 Pavez A, Salazar C, Rivera R, et al. Description of endoscopicventricular anatomy in myelomeningocele. Minim Invasive Neu-rosurg 2006;49(03):161–167
24 Pinto FC, Pereira RM, Saad F, Teixeira MJ. Performance of fixed-pressure valve with antisiphon device SPHERA(®) in hydroce-phalus treatment and overdrainage prevention. Arq Neuropsi-quiatr 2012;70(09):704–709
25 Pinto FCG, Becco R, Alho EJL, et al. The retrograde ventriculo-sinusshunt in an animal experimentalmodel of hydrocephalus. PediatrNeurosurg 2016;51(03):142–148
26 Portnoy HD, Schulte RR, Fox JL, Croissant PD, Tripp L. Anti-siphonand reversible occlusion valves for shunting in hydrocephalus andpreventing post-shunt subdural hematomas. J Neurosurg 1973;38(06):729–738
27 Pudenz RH, Russell FE, Hurd AH, Shelden CH. Ventriculo-auricu-lostomy; a technique for shunting cerebrospinal fluid into the rightauricle; preliminary report. J Neurosurg 1957;14(02):171–179
28 Teo C, Jones R.Management of hydrocephalus byendoscopic thirdventriculostomy in patients with myelomeningocele. PediatrNeurosurg 1996;25(02):57–63, discussion 63
29 El Shafei IL, El Shafei HI. The retrograde ventriculo-sinus shunt(El Shafei RVS shunt). Rationale, evolution, surgical technique andlong-term results. Pediatr Neurosurg 2005;41(06):305–317
30 Wen HL. Ventriculo-superior sagittal sinus shunt for hydroce-phalus. Surg Neurol 1982;17(06):432–434
31 Zemack G, Romner B. Seven years clinical experience with theCodmanHakimprogrammable valve: a retrospective study of 583patients. J Neurosurg 2000;92:941–948
32 el-Shafei IL, el-Rifaii MA. Ventriculojugular shunt against thedirection of blood flow. II. Theoretical and experimental basisfor shunting the cerebrospinal fluid against the direction of bloodflow. Childs Nerv Syst 1987;3(05):285–291
33 el-Shafei IL, el-Rifaii MA. Ventriculojugular shunt against thedirection of blood flow. I. Role of the internal jugular vein as anantisiphonage device. Childs Nerv Syst 1987;3(05):282–284
34 El-Shafei IL, El-Shafei HI. The retrograde ventriculosinus shunt:concept and technique for treatment of hydrocephalus by shunt-ing the cerebrospinal fluid to the superior sagittal sinus against
the direction of blood flow. Preliminary report. Childs Nerv Syst2001;17(08):457–465, discussion 466
35 Browd SR, Ragel BT, Gottfried ON, Kestle JR. Failure of cerebrosp-inal fluid shunts: part I: Obstruction and mechanical failure.Pediatr Neurol 2006;34(02):83–92
36 Browd SR, Gottfried ON, Ragel BT, Kestle JR. Failure of cerebrosp-inal fluid shunts: part II: overdrainage, loculation, and abdominalcomplications. Pediatr Neurol 2006;34(03):171–176
37 Choux M, Camboulives J, Rigaut F. [Prevention of infections inventriculoperitoneal shunts in children]. Ann Fr Anesth Reanim1992;11(06):699–704
38 de Souza RB, Pinto FC. Could craniometric measurements explainthe growth of the superior sagittal sinus? Pediatr Neurosurg2012;48(04):225–228
39 Eklund A, Koskinen LO, Malm J. Features of the Sinushunt and itsinfluence on the cerebrospinal fluid system. J Neurol NeurosurgPsychiatry 2004;75(08):1156–1159
40 El Shafei IL. Ventriculo-venous shunt to the proximal segment of anoccluded neck vein. A new method for shunting the cerebrospinalfluid to the venous circulation. Surg Neurol 1975;3(05):237–244
41 El Shafei IL. Ventriculovenous shunt to the proximal segment of aligated neck vein. A new surgical technique for shunting thecerebrospinal fluid to the venous circulation (preliminary report).Childs Brain 1975;1(05):311–323
42 Elgamal EA. Natural history of hydrocephalus in children withspinal open neural tube defect. Surg Neurol Int 2012;3:112
43 El-Shafei IL, El-Shafei HI. The retrograde ventriculovenous shunts:the El-Shafei retrograde ventriculojugular and ventriculosinusshunts. Pediatr Neurosurg 2010;46(03):160–171
44 el-Shafei IL. Ventriculojugular shunt against the direction of bloodflow. III. Operative technique and results. Childs Nerv Syst 1987;3(06):342–349
45 Børgesen SE, Pieri A, Cappelen J, Agerlin N, Gjerris F. Shunting tothe cranial venous sinus using the SinuShunt. Childs Nerv Syst2004;20(06):397–404
46 Adzick NS, Thom EA, Spong CY, et al; MOMS Investigators.A randomized trial of prenatal versus postnatal repair of myelo-meningocele. N Engl J Med 2011;364(11):993–1004
47 Alexandrov AV, Sloan MA, Tegeler CH, et al; American Society ofNeuroimagingPracticeGuidelinesCommittee. Practice standards fortranscranial Doppler (TCD) ultrasound. Part II. Clinical indicationsand expected outcomes. J Neuroimaging 2012;22(03):215–224
48 Behrens A, Lenfeldt N, Ambarki K, Malm J, Eklund A, Koskinen LO.Transcranial Doppler pulsatility index: not an accurate method toassess intracranial pressure.Neurosurgery2010;66(06):1050–1057
49 de Oliveira MF, Teixeira MJ, de Lima Oliveira M, Seng-Shu EB,Norremose KA, Gomes Pinto FC. Transcranial Doppler in theevaluation of infants treated with retrograde ventriculosinusshunt. Childs Nerv Syst 2016;32(11):2133–2142
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
RRVS as an Alternative for Treating Hydrocephalus in Children Oliveira et al.116
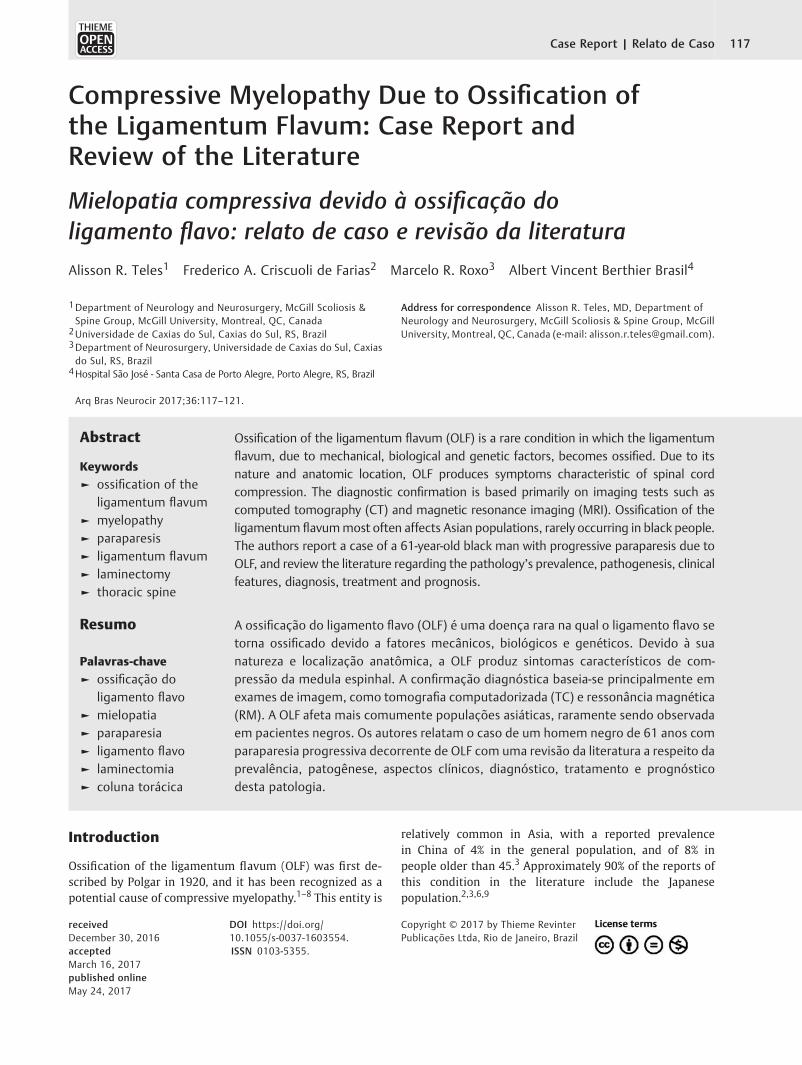
Compressive Myelopathy Due to Ossification ofthe Ligamentum Flavum: Case Report andReview of the Literature
Mielopatia compressiva devido à ossificação doligamento flavo: relato de caso e revisão da literatura
Alisson R. Teles1 Frederico A. Criscuoli de Farias2 Marcelo R. Roxo3 Albert Vincent Berthier Brasil4
1Department of Neurology and Neurosurgery, McGill Scoliosis &Spine Group, McGill University, Montreal, QC, Canada
2Universidade de Caxias do Sul, Caxias do Sul, RS, Brazil3Department of Neurosurgery, Universidade de Caxias do Sul, Caxiasdo Sul, RS, Brazil
4Hospital São José - Santa Casa de Porto Alegre, Porto Alegre, RS, Brazil
Arq Bras Neurocir 2017;36:117–121.
Address for correspondence Alisson R. Teles, MD, Department ofNeurology and Neurosurgery, McGill Scoliosis & Spine Group, McGillUniversity, Montreal, QC, Canada (e-mail: [email protected]).
Introduction
Ossification of the ligamentum flavum (OLF) was first de-scribed by Polgar in 1920, and it has been recognized as apotential cause of compressive myelopathy.1–8 This entity is
relatively common in Asia, with a reported prevalencein China of 4% in the general population, and of 8% inpeople older than 45.3 Approximately 90% of the reports ofthis condition in the literature include the Japanesepopulation.2,3,6,9
Keywords
► ossification of theligamentum flavum
► myelopathy► paraparesis► ligamentum flavum► laminectomy► thoracic spine
Abstract Ossification of the ligamentum flavum (OLF) is a rare condition in which the ligamentumflavum, due to mechanical, biological and genetic factors, becomes ossified. Due to itsnature and anatomic location, OLF produces symptoms characteristic of spinal cordcompression. The diagnostic confirmation is based primarily on imaging tests such ascomputed tomography (CT) and magnetic resonance imaging (MRI). Ossification of theligamentum flavummost often affects Asian populations, rarely occurring in black people.The authors report a case of a 61-year-old black man with progressive paraparesis due toOLF, and review the literature regarding the pathology’s prevalence, pathogenesis, clinicalfeatures, diagnosis, treatment and prognosis.
Palavras-chave
► ossificação doligamento flavo
► mielopatia► paraparesia► ligamento flavo► laminectomia► coluna torácica
Resumo A ossificação do ligamento flavo (OLF) é uma doença rara na qual o ligamento flavo setorna ossificado devido a fatores mecânicos, biológicos e genéticos. Devido à suanatureza e localização anatômica, a OLF produz sintomas característicos de com-pressão da medula espinhal. A confirmação diagnóstica baseia-se principalmente emexames de imagem, como tomografia computadorizada (TC) e ressonância magnética(RM). A OLF afeta mais comumente populações asiáticas, raramente sendo observadaem pacientes negros. Os autores relatam o caso de um homem negro de 61 anos comparaparesia progressiva decorrente de OLF com uma revisão da literatura a respeito daprevalência, patogênese, aspectos clínicos, diagnóstico, tratamento e prognósticodesta patologia.
receivedDecember 30, 2016acceptedMarch 16, 2017published onlineMay 24, 2017
DOI https://doi.org/10.1055/s-0037-1603554.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 117
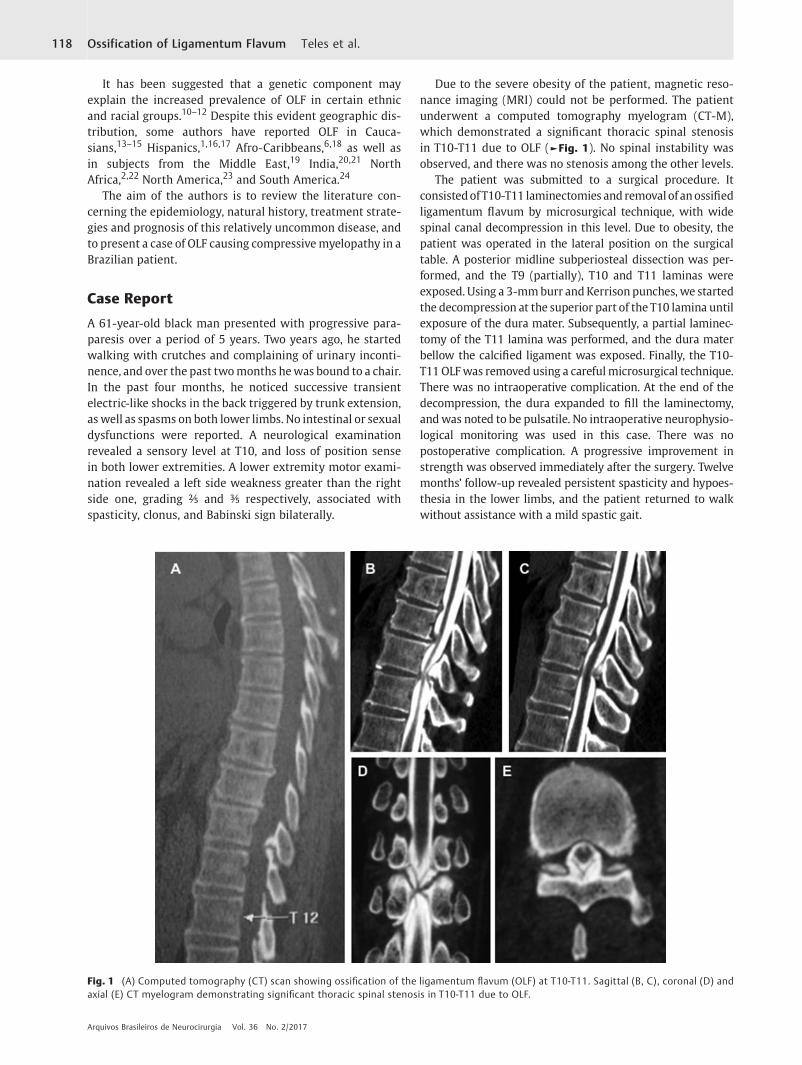
It has been suggested that a genetic component mayexplain the increased prevalence of OLF in certain ethnicand racial groups.10–12 Despite this evident geographic dis-tribution, some authors have reported OLF in Cauca-sians,13–15 Hispanics,1,16,17 Afro-Caribbeans,6,18 as well asin subjects from the Middle East,19 India,20,21 NorthAfrica,2,22 North America,23 and South America.24
The aim of the authors is to review the literature con-cerning the epidemiology, natural history, treatment strate-gies and prognosis of this relatively uncommon disease, andto present a case of OLF causing compressivemyelopathy in aBrazilian patient.
Case Report
A 61-year-old black man presented with progressive para-paresis over a period of 5 years. Two years ago, he startedwalking with crutches and complaining of urinary inconti-nence, and over the past twomonths hewas bound to a chair.In the past four months, he noticed successive transientelectric-like shocks in the back triggered by trunk extension,as well as spasms on both lower limbs. No intestinal or sexualdysfunctions were reported. A neurological examinationrevealed a sensory level at T10, and loss of position sensein both lower extremities. A lower extremity motor exami-nation revealed a left side weakness greater than the rightside one, grading ⅖ and ⅗ respectively, associated withspasticity, clonus, and Babinski sign bilaterally.
Due to the severe obesity of the patient, magnetic reso-nance imaging (MRI) could not be performed. The patientunderwent a computed tomography myelogram (CT-M),which demonstrated a significant thoracic spinal stenosisin T10-T11 due to OLF (►Fig. 1). No spinal instability wasobserved, and there was no stenosis among the other levels.
The patient was submitted to a surgical procedure. ItconsistedofT10-T11 laminectomies and removal of anossifiedligamentum flavum by microsurgical technique, with widespinal canal decompression in this level. Due to obesity, thepatient was operated in the lateral position on the surgicaltable. A posterior midline subperiosteal dissection was per-formed, and the T9 (partially), T10 and T11 laminas wereexposed. Using a 3-mmburr and Kerrison punches, we startedthe decompression at the superior part of the T10 lamina untilexposure of the dura mater. Subsequently, a partial laminec-tomy of the T11 lamina was performed, and the dura materbellow the calcified ligament was exposed. Finally, the T10-T11 OLFwas removed using a carefulmicrosurgical technique.There was no intraoperative complication. At the end of thedecompression, the dura expanded to fill the laminectomy,andwas noted to be pulsatile. No intraoperative neurophysio-logical monitoring was used in this case. There was nopostoperative complication. A progressive improvement instrength was observed immediately after the surgery. Twelvemonths’ follow-up revealed persistent spasticity and hypoes-thesia in the lower limbs, and the patient returned to walkwithout assistance with a mild spastic gait.
Fig. 1 (A) Computed tomography (CT) scan showing ossification of the ligamentum flavum (OLF) at T10-T11. Sagittal (B, C), coronal (D) andaxial (E) CT myelogram demonstrating significant thoracic spinal stenosis in T10-T11 due to OLF.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Ossification of Ligamentum Flavum Teles et al.118

Discussion
The ligamentum flavum consists of a group of paired liga-ments that connect adjacent spinal column laminae, extend-ing from C2 to S1.1 In OLF, the ligamentum flavum becomesossified through a process of ectopic bone formation, whichoccurs through hypertrophy of the ligament, proliferation ofchondrocytes and ossification, characterizing a process ofendochondral ossification.25,26
Even though 90 years have passed since its first descrip-tion, the pathophysiology of OLF is not yet totally under-stood.14 Many authors have postulated that it derivesbroadly from mechanical stress, but other metabolic andgenetic factors may also be of relevance.3,10,11,27–32 Histo-logically, the lesion often presents with degeneration anddisorganization of elastic fibers.12,25,26,33,34 Yoshida et al33
and Yayama et al12 have shown increased production ofcollagen fibers in the lesion. Several authors demonstratedthat altered expression of bone morphogenetic protein(BMP-2), transforming growth factor β (TGF-β) may play arole in the process that leads to OLF.12,27,28 It has beenshown that genetic polymorphism in collagen-related genesmay also contribute in that aspect.29,30 Although OLF hasbeen reported as an isolated form of spinal column ossifi-cation, many publications proposed the existence of aninterrelation with conditions such as diffuse idiopathicskeletal hyperostosis (DISH), ankylosing spondylitis, andmetabolic disorders. Disorders such as hypoparathyroidism,X-linked hypophosphatemia, Paget’s disease, vitamin D-resistant rickets, non-insulin-dependent diabetes mellitus,and calcium and fluoride derangements, as well as otherspinal ligamentous ossifications.4,5,20,34–46 Finally, it hasbeen suggested that the genetic background may explainthe increased prevalence of OLF in certain ethnic and racialgroups.10–12
Ossification of the ligamentum flavum is a major cause ofmyelopathy in Japan. An epidemiological study conducted bySato et al in Japan showed that 64% of surgeries for thoracicmyelopathy were due to OLF.47 Another similar study inJapan showed the presence of OLF in 52% of thoracicmyelopathy surgical procedures.48 Guo et al3 reported theprevalence of OLF in 1,736 Chinese volunteers using theMRI.They demonstrated a prevalence of OLF in 3.8% (66 volun-teers) of the sample. Of the 92 affected segments, 87 (94.5%)were located in the thoracic region, with more than half ofthose (48 segments) located on the lower thoracic spine. Inthat study, isolated OLF was present in 68.2% of the cases,with continuous and non-continuous multilevel lesionspresent in 16.7% and 15.2% of the cases respectively.
Several other authors have asserted the isolated form asthe most prevalent, and that the lower thoracic spine,specially T9-T10 and T10-T11, is the most affectedregion.1,2,6,12,14,49 These data are also supported by a reviewpublished by Xu et al.14 This prevalence occurs probablybecause this transitional level presents a high load and lessanatomic protection from the rib cage, making it more proneto degenerative processes and mechanical stress, which inturn leads to ossification.3,31,32
Ossification of the ligamentum flavum is very rare amongblack patients, with only a few reports in the literature.8,50–54
In 1998, Pascal-Mousselard et al reported an unusual OLFin the thoracic spine in a black patient presenting withprogressive spastic paraparesis.8 Because of its rarity in blackpatients, OLF is a diagnosis of exclusion in this population.
When OLF lesions are small, patients may be asymptom-atic.3Once the lesions grow enough to significantly affect thespinal canal, patients often present with symptoms second-ary to myelopathy. These include motor and sensory dys-functions and bladder impairment.1,2 Since the majority ofthese cases occurs at lower thoracic levels,5,55 the mostcommon symptoms are uni- or bilateral lower limb weak-ness,2,6,8,12,14,18,56 pain6,8,18,56 and sensorial loss,2,6,8,56
unsteady gait,6,8,14 brisk reflexes with positive Babinski,8,56
and urinary frequency and urgency, often accompanied byincontinence.6,8,14,18,56 In cases in which OLF presents atupper levels, upper limb and neck involvement may occur.1,6
Advanced OLF can also cause paraplegia, as reported by BenHamouda et al2 and Okada.5
Plain radiographs are not sensitive enough to diagnoseOLF in most of the cases, since its radiopaque shadow can beobscured by bony structures.4 Computed tomography andMRI are the best imaging modalities to establish the diagno-sis.14 Computed tomography is more accurate,14 revealingcharacteristic intense radiodense lines along the laminae.1,6
The lesionmost commonly presents in a V-shaped fashion onaxial imaging,1,2,6 but itmayalso present as nodular,mound-shaped lesions.14,57 The CT is also useful in determining if thedura-mater is involved in the OLF or not.1 Both the T1- andT2-wheigted MRIs are used mostly to evaluate spinal cordinvolvement, showing a hyperintense signal in the affectedparts. 1,2,6,15,58. The ossification itself presents a hypointensesignal in this imaging modality.2,3,14 A myelogram candetermine the presence of spinal cord compression, but itoften fails to define the nature of the lesion. Thus, themyelogram is often accompanied by CT imaging.2,6,8 Aretrospective analysis by Muthukumar et al59 establishedtwo radiological signs of dural ossification related to OLF: the“tram track sign” and the “comma sign.” The former consistsof a hyperdense bony excrescence with a hypodense center,with the latter being evidence of ossification on one half ofthe circumference of the dura mater.59
Ossification of the ligamentum flavum can often beconfused with calcification of the ligamentum flavum(CLF),2,6which is a rare disease that occurs through a depositof calcified granules along the ligamentum flavum, with nobone formation.2 Since both lesions appear as hypointenseformations on the T1- and T2-weighted MRIs, the diagnosiscan be confirmed according to CT imaging, with CLF beingdiscontinuous with the laminae, opposite to OLF.3,4,14,60 It’salso worth noting that the majority of cases of CLF occur inthe cervical spine.2,61
To this date, there are no efficient pharmacological thera-pies to treat OLF.14 Due to the nature of the disease, thetreatment consists mostly of simple surgical decompres-sion.1,2,6,14,49 The majority of these cases does not presentwith spinal instability and does not require instrumented
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Ossification of Ligamentum Flavum Teles et al. 119

fusion. The literature suggests laminectomy, laminoplasty, orfenestration at the affected level (or levels) as valuable surgicaltechniques.1,5,6,14,32,49,62 A large retrospective study byLi et al32 compared the outcomes of laminoplasty and lam-inectomy. The authors described a 25% improvement with theformer technique against an 83% improvement with the latter.Fenestrationmay be performed in situations inwhich the OLFis laterally located and not fused at the middle of the spinalcanal, often presenting with radicular pain.2,49
Adherence of the dura is reported in 11 to 62% of OLFsurgeries.59 Meningeal involvement can often difficult thesurgical procedure.32 Cerebrospinal fluid leakage followingdisruption of the dura mater is one of the major intra-operative complications.1,49 Cerebrospinal fluid (CSF) leak-age can lead to CSF fistula formation, pseudomeningocele,meningitis, arachnoiditis and epidural abscess.63
Inamasu and Guiot64 recently conducted a systematicreview concerning the factors that influence the outcomeafter surgery for OLF. The authors reviewed 31 articles, andsuggested that gender, age, the level of the ossified lesion, thenumber of OLF-affected segments, the coexistence of anossified posterior longitudinal ligament, OLF classificationon CT, and the presence of a high intensity signal are unlikelyto modify the outcome after surgery. They also suggestedthat the duration of the symptoms and the neurological scoremay influence the outcome. Altogether, the literature strong-ly suggests that the preoperative duration of the symp-toms,48,49,55 the severity of the neurological deficit,48,49
and the presence of hyperintense signals6,15,65 in the spinalcord can influence the outcome. This was reaffirmed in aretrospective analysis of 85 cases conducted by Li et al.7
Surgical decompression, particularly through laminectomy,generally results in improvement or disappearance of thesymptoms in most cases.2,6,14,32,49
Conclusion
Ossification of the ligamentum flavum has been well-estab-lished as a cause of myelopathy. The pathogenetic mecha-nisms of the disease are not well understood, but they mostlikely include different mechanical and biological factors.Although OLF is more common in Asian populations, it canalso be present in different ethnic groups.We reported a rarecase of thoracic OLF in a black patient. Symptomatic patientsshould be surgically treated.
References1 Christiano LD, Assina R, Goldstein IM. Ossification of the liga-
mentumflavum: a unique report of aHispanicwoman. NeurosurgFocus 2011;30(03):E15
2 Ben Hamouda K, Jemel H, Haouet S, Khaldi M. Thoracic myelo-pathy caused by ossification of the ligamentum flavum: a reportof 18 cases. J Neurosurg 2003;99(2, Suppl)157–161
3 Guo JJ, Luk KD, Karppinen J, Yang H, Cheung KM. Prevalence,distribution, and morphology of ossification of the ligamentumflavum: a population study of one thousand seven hundred thirty-six magnetic resonance imaging scans. Spine 2010;35(01):51–56
4 Okada G, Hosoi S, Kato K, et al. Case report 779. Carbonate apatitecalcification of ligamentum flavum. Skeletal Radiol 1993;22(03):211–213
5 Okada K, Oka S, Tohge K, Ono K, Yonenobu K, Hosoya T. Thoracicmyelopathy caused by ossification of the ligamentum flavum.Clinicopathologic study and surgical treatment. Spine 1991;16(03):280–287
6 Pascal-Moussellard H, Cabre P, Smadja D, Catonné Y. Symptomaticossification of the ligamentum flavum: a clinical series from theFrench Antilles. Spine 2005;30(14):E400–E405
7 Li Z, Ren D, Zhao Y, et al. Clinical characteristics and surgicaloutcome of thoracic myelopathy caused by ossification of theligamentum flavum: a retrospective analysis of 85 cases. SpinalCord 2016;54(03):188–196
8 Pascal-Mousselard H, Smadja D, Cabre P, Raynaud M, Catonne Y.Ossification of the ligamenta flava with severe myelopathy in ablack patient. A case report. Spine 1998;23(14):1607–1608
9 Mobbs RJ, Dvorak M. Ossification of the ligamentum flavum: dietand genetics. J Clin Neurosci 2007;14(07):703–705
10 Sakou T, Taketomi E, Matsunaga S, Yamaguchi M, Sonoda S,Yashiki S. Genetic study of ossification of the posterior long-itudinal ligament in the cervical spine with human leukocyteantigen haplotype. Spine 1991;16(11):1249–1252
11 Koga H, Sakou T, Taketomi E, et al. Geneticmapping of ossificationof the posterior longitudinal ligament of the spine. Am J HumGenet 1998;62(06):1460–1467
12 Yayama T, Uchida K, Kobayashi S, et al. Thoracic ossification of thehuman ligamentum flavum: histopathological and immunohis-tochemical findings around the ossified lesion. J Neurosurg Spine2007;7(02):184–193
13 Parekh HC, Gurusinghe NT, Perera SS, Prabhu SS. Ossification ofthe ligamentum flavum in a Caucasian: case report. Br J Neuro-surg 1993;7(06):687–690
14 Xu R, Sciubba DM, Gokaslan ZL, Bydon A. Ossification of theligamentum flavum in a Caucasian man. J Neurosurg Spine 2008;9(05):427–437
15 van Oostenbrugge RJ, Herpers MJ, de Kruijk JR. Spinal cordcompression caused by unusual location and extension of ossifiedligamenta flava in a Caucasian male. A case report and literaturereview. Spine 1999;24(05):486–488
16 Toledo JA, Isseldyk FV, Re M, Garrote M. Ossification of theligamentum flavum as cause of thoracic cord compression:Case report of a Latin American man and review of the literature.Surg Neurol Int 2013;4:119
17 Cabrera-Aldana EE, De la Garza Ramos R, Zuluaga Gómez A,Rosales-Olivares LM, Reyes-Sánchez A. Multilevel thoracic ossi-fication of the ligamentum flavum in a Hispanic woman withachondroplasia. Spine J 2016;16(11):e749–e750
18 Chana JS, Afshar F. Thoracic spondylosis presenting with spasticparaparesis. Postgrad Med J 1996;72(846):243–244
19 al-Orainy IA, Kolawole T. Ossification of the ligament flavum. EurJ Radiol 1998;29(01):76–82
20 Gupta RK, Agarwal P, Kumar S, Surana PK, Lal JH, Misra UK.Compressive myelopathy in fluorosis: MRI. Neuroradiology1996;38(04):338–342
21 Sushil P, Anant K. Ossified-calcified ligamentum flavum causingdorsal cord compression with computed tomography-magneticresonance imaging features. Surg Neurol 1994;41(06):441–442
22 Jaffan I, Abu-Serieh B, Duprez T, Cosnard G, Raftopoulos C.Unusual CT/MR features of putative ligamentum flavum ossifica-tion in a North Africanwoman. Br J Radiol 2006;79(944):e67–e70
23 Kruse JJ, Awasthi D, Harris M, Waguespack A. Ossification of theligamentum flavum as a cause of myelopathy in North America:report of three cases. J Spinal Disord 2000;13(01):22–25
24 Gondim J, Ramos Júnior F. [Thoracic spinal cord compression attwo levels due to ligamentum flavum calcification. Case report].Arq Neuropsiquiatr 1998;56(02):312–316
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Ossification of Ligamentum Flavum Teles et al.120

25 Uchida K, Yayama T, Cai HX, et al. Ossification process involvingthe human thoracic ligamentum flavum: role of transcriptionfactors. Arthritis Res Ther 2011;13(05):R144
26 Yin X, Chen Z, Guo Z, Liu X, Yu H. Tissue transglutaminaseexpression and activity in human ligamentum flavum cellsderived from thoracic ossification of ligamentum flavum. Spine2010;35(20):E1018–E1024
27 Moon SH, Park SR, Kim H, et al. Biologic modification of ligamen-tum flavum cells by marker gene transfer and recombinant hu-man bonemorphogenetic protein-2. Spine 2004;29(09):960–965
28 Hayashi K, Ishidou Y, Yonemori K, et al. Expression and localizationof bone morphogenetic proteins (BMPs) and BMP receptors inossification of the ligamentum flavum. Bone 1997;21(01):23–30
29 Kong Q, Ma X, Li F, et al. COL6A1 polymorphisms associated withossification of the ligamentum flavum and ossification of theposterior longitudinal ligament. Spine 2007;32(25):2834–2838
30 Tanaka T, Ikari K, Furushima K, et al. Genomewide linkage andlinkage disequilibrium analyses identify COL6A1, on chromo-some 21, as the locus for ossification of the posterior longitudinalligament of the spine. Am J Hum Genet 2003;73(04):812–822
31 Tsukamoto N, Maeda T, Miura H, et al. Repetitive tensile stress torat caudal vertebrae inducing cartilage formation in the spinalligaments: a possible role of mechanical stress in the develop-ment of ossification of the spinal ligaments. J Neurosurg Spine2006;5(03):234–242
32 Li F, Chen Q, Xu K. Surgical treatment of 40 patients with thoracicossification of the ligamentum flavum. J Neurosurg Spine 2006;4(03):191–197
33 Yoshida M, Shima K, Taniguchi Y, Tamaki T, Tanaka T. Hypertro-phied ligamentum flavum in lumbar spinal canal stenosis. Patho-genesis andmorphologic and immunohistochemical observation.Spine 1992;17(11):1353–1360
34 Ono K, Yonenobu K, Miyamoto S, Okada K. Pathology of ossifica-tion of the posterior longitudinal ligament and ligamentumflavum. Clin Orthop Relat Res 1999;(359):18–26
35 Tomita K, Kawahara N, Baba H, Kikuchi Y, Nishimura H. Circumsp-inal decompression for thoracic myelopathy due to combinedossification of the posterior longitudinal ligament and ligamen-tum flavum. Spine 1990;15(11):1114–1120
36 Hukuda S, Mochizuki T, Ogata M, Shichikawa K. The pattern ofspinal and extraspinal hyperostosis in patients with ossificationof the posterior longitudinal ligament and the ligamentum fla-vum causing myelopathy. Skeletal Radiol 1983;10(02):79–85
37 Ehara S, Shimamura T, Nakamura R, Yamazaki K. Paravertebralligamentous ossification: DISH, OPLL and OLF. Eur J Radiol 1998;27(03):196–205
38 Kojima T, Oonishi I, Kurokawa T. Ossification of the ligamentumflavum in the thoracolumbar spine of young adults report of twocases. Int Orthop 1992;16(01):75–79
39 Ishida Y, Kawai S. Effects of bone-seeking hormones on DNAsynthesis, cyclic AMP level, and alkaline phosphatase activity incultured cells from human posterior longitudinal ligament of thespine. J Bone Miner Res 1993;8(11):1291–1300
40 Terakado A, TagawaM, Goto S, Yamazaki M, Moriya H, Fujimura S.Elevation of alkaline phosphatase activity induced by parathyroidhormone in osteoblast-like cells from the spinal hyperostoticmouse TWY (twy/twy). Calcif Tissue Int 1995;56(02):135–139
41 Wang Z, Li XD, Li MQ, Wang QP. Changes in basic metabolicelements associated with the degeneration and ossification ofligamenta flava. J Spinal Cord Med 2008;31(03):279–284
42 Li H, Jiang LS, Dai LY. Hormones and growth factors in thepathogenesis of spinal ligament ossification. Eur Spine J 2007;16(08):1075–1084
43 Matsui H, Katoh Y, Tsuji H. Untreated hypophosphatemic vitaminD-resistant rickets with symptomatic ossification of the ligamen-tum flavum. J Spinal Disord 1991;4(01):110–113
44 Vera CL, Cure JK, Naso WB, et al. Paraplegia due to ossification ofligamenta flava in X-linked hypophosphatemia. A case report.Spine 1997;22(06):710–715
45 Epstein NE. Ossification of the yellow ligament and spondylosisand/or ossification of the posterior longitudinal ligament of thethoracic and lumbar spine. J Spinal Disord 1999;12(03):250–256
46 Kim TJ, Kim TH, Jun JB, Joo KB, UhmWS. Prevalence of ossificationof posterior longitudinal ligament in patients with ankylosingspondylitis. J Rheumatol 2007;34(12):2460–2462
47 Sato T, Kokubun S, Tanaka Y, Ishii Y. Thoracic myelopathy in theJapanese: epidemiological and clinical observations on the casesin Miyagi Prefecture. Tohoku J Exp Med 1998;184(01):1–11
48 Aizawa T, Sato T, Sasaki H, Kusakabe T, Morozumi N, Kokubun S.Thoracic myelopathy caused by ossification of the ligamentumflavum: clinical features and surgical results in the Japanesepopulation. J Neurosurg Spine 2006;5(06):514–519
49 Aizawa T, Sato T, Sasaki H, et al. Results of surgical treatment forthoracic myelopathy: minimum 2-year follow-up study in 132patients. J Neurosurg Spine 2007;7(01):13–20
50 EpsteinN.Thoracicossificationof theposterior longitudinal ligament,ossification of the yellow ligament from T9-T12 with superimposedacuteT10/T11discherniation:controversies insurgicalmanagement.J Spinal Disord 1996;9(05):446–447, discussion 447–450
51 RivierezM, Vally P. [Ossification of ligamentum flavumunmaskedby acute paraplegia]. Neurochirurgie 2001;47(06):572–575
52 Sagar H, Fernandez-Madrid F, Kupsky W. Rare cause of thoracicmyelopathy: ossified ligamentum flavum. J Clin Rheumatol 2010;16(07):326–329
53 Suojanen JN, Lipson SJ. Spinal cord compression secondary toossified ligamentum flavum. J Spinal Disord 1989;2(04):238–240
54 WisemanDB,Stokes JK,ToselliRM.Paraparesis inablackmanbroughton by ossification of the ligamentum flavum: case report and reviewof the literature. J Spinal Disord Tech 2002;15(06):542–545
55 ShiokawaK,Hanakita J, SuwaH, SaikiM,OdaM,KajiwaraM.Clinicalanalysis and prognostic study of ossified ligamentum flavumof thethoracic spine. J Neurosurg 2001;94(2, Suppl)221–226
56 Shiraishi T, Crock HV, Lewis P. Thoracic myelopathy due toisolated ossification of the ligamentum flavum. J Bone JointSurg Br 1995;77(01):131–133
57 Omojola MF, Cardoso ER, Fox AJ, Drake CG, Durward QJ. Thoracicmyelopathy secondary to ossified ligamentum flavum. J Neuro-surg 1982;56(03):448–450
58 Sugimura H, Kakitsubata Y, Suzuki Y, et al. MRI of ossification ofligamentum flavum. J Comput Assist Tomogr 1992;16(01):73–76
59 Muthukumar N. Dural ossification in ossification of the ligamen-tum flavum: a preliminary report. Spine 2009;34(24):2654–2661
60 Miyasaka K, Kaneda K, Sato S, et al. Myelopathy due to ossificationor calcification of the ligamentum flavum: radiologic and histo-logic evaluations. AJNR Am J Neuroradiol 1983;4(03):629–632
61 Muthukumar N, Karuppaswamy U, Sankarasubbu B. Calcium pyr-ophosphate dihydrate deposition disease causing thoracic cordcompression: case report. Neurosurgery 2000;46(01):222–225
62 Sanghvi AV, Chhabra HS, Mascarenhas AA, Mittal VK, Sangondi-math GM. Thoracicmyelopathy due to ossification of ligamentumflavum: a retrospective analysis of predictors of surgical outcomeand factors affecting preoperative neurological status. Eur Spine J2011;20(02):205–215
63 Kalevski SK, Peev NA, Haritonov DG. Incidental Dural Tears inlumbar decompressive surgery: Incidence, causes, treatment,results. Asian J Neurosurg 2010;5(01):54–59
64 Inamasu J, Guiot BH. A review of factors predictive of surgicaloutcome for ossification of the ligamentum flavum of the thoracicspine. J Neurosurg Spine 2006;5(02):133–139
65 Kuh SU, Kim YS, Cho YE, et al. Contributing factors affecting theprognosis surgical outcome for thoracic OLF. Eur Spine J 2006;15(04):485–491
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Ossification of Ligamentum Flavum Teles et al. 121

Arachnoid Cyst with a Non-traumatic AcuteSubdural Hematoma in an Eleven-year-oldPatient
Cisto aracnoide associado a hematoma subdural agudonão traumático em um paciente de onze anos de idade
Gabriel Flamarin Cavasana1 Rodrigo Mendonça1 Fabricio Willian Mantelo Zanini1
1Neurosurgery Department of Santa Casa de Misericórdia deAraçatuba, SP, Brazil
Arq Bras Neurocir 2017;36:122–124.
Address for correspondence Gabriel Flamarin Cavasana, MedicalStudent, Rua Ipanema, 67, Apto 52-C, São Paulo, SP 03164200, Brazil(e-mail: [email protected]).
Introduction
The arachnoid cyst is presumably a congenital malformationand represents only 1% of all intracranial lesions.1 Its ruptureand bleeding are rare, usually occurring in young adults andassociated with trauma. Risk of hemorrhage does not exceed0.04%/ year.2 We report a case of an eleven-year-old boy witha previously asymptomatic arachnoid cyst that suddenlypresented a non-traumatic acute subdural hematoma andintra-cystic hemorrhage.
Case
An eleven-year-old boy had a sudden episode of headache ofmoderate intensity accompanied by nausea. The child deniedany history of chronic headache before this episode. Thesymptoms began appearing at a monthly frequency. Everytime, the boys parents would medicate symptoms with oralanalgesic, after which he evolved with improvement. Afterfivemonths, the headache episodes becameweekly andmoreintense associated with nausea and vomiting, varying in
Keywords
► neurosurgery► arachnoid cysts► acute subdural
hematoma
Abstract A non-traumatic intra-cystic hemorrhage in an arachnoid cyst is a rare event, with fewcases reported in the literature. We present a case of an eleven-year-old boy patient,which presented a spontaneous acute subdural hematoma and intra-cystic hemorrhageafter a strong headache episode. The results were evidenced by a computed tomogra-phy (CT) scan and surgical findings. We perform a brief literature review on thearachnoid cyst and its suggested treatments. In our case, the patient underwent asurgical treatment with a complete resolution of the case.
Palavras-chave
► neurocirurgia► cisto aracnoide► hematoma subdural
agudo
Resumo Sabe-se que uma hemorragia intracística não traumática em um cisto aracnoide é umacontecimento raro, com poucos casos relatados na literatura. Nós apresentamos ocaso de um menino de onze anos de idade, o qual apresentou espontaneamente umhematoma subdural agudo acompanhado de hemorragia intracística após um forteepisódio de dor de cabeça. Os resultados foram evidenciados através de umatomografia computadorizada e dos achados cirúrgicos. Foi feita uma breve revisãoda literatura sobre cisto aracnoide e seus respectivos tratamentos sugeridos. Em nosso
receivedJune 29, 2015acceptedNovember 23, 2015published onlineFebruary 12, 2016
DOI https://doi.org/10.1055/s-0035-1571137.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de Caso122

location. Oral analgesics were no longer effective to solve thepain. There were no other associated symptoms. The parentsdecided to take the patient to the emergency service, wherehe had a cranial CTscan. This one showed an arachnoid cyst inthe middle fossa of the left cerebral hemisphere, withoutsigns of complications (►Fig. 1). The local neurologist evalu-ated him and initiated a conservative treatment of theheadache. After about a month with worsening symptoms,the patient returned to the emergency service, where he hada new cranial CT scan that showed an acute subdural hema-toma (►Fig. 2). He was referred to the neurosurgeon localservice, where there was a decision made to hospitalize thepatient and provide surgical treatment.
The surgical techniquewas decompressive craniotomywitha question-mark incision and a whole hematoma evacuation.There was intracystic hemorrhage observed during the sur-gery. The patient remained in the pediatric intensive care unitdue to postoperative support, showing gradual improvement.Thepatient received amedical discharge after sevendays. After30 days, hehad a newCT. This last CTscan showedno bleeding.Based on the CT findings and the absence of pathological signsand symptoms, we concluded there had been a completeresolution of the condition (►Figs. 3–4.
Discussion
Intracranial arachnoid cysts are relatively common findingsin neuroimaging studies among the pediatric population,primarily in boys.3 The most accepted hypothesis statesthat the arachnoid cyst is a congenital malformation.1
The arachnoid cyst corresponds to 1% of all non-traumaticintracranial lesions. The most common location is the middlecranial fossa.4 It is presumably formed by a division of thearachnoid membrane caused by an increase in cerebrospinalfluid (CSF) pressure.1 Other hypotheses are: 1-dysgenesisembryo in the formation of the arachnoid, secondary to a
primary disorder of the mesenchyme adjacent to the neuraltube; 2-agenesis, located atrophy or hypoplasia of the brainresulting in the secondary expansion of the CSF space; 3-located disorder secondary to infectious/inflammatory pro-cess, traumatic or hemorrhagic.5 Most imaging studies find-ings are incidental due to the asymptomatic clinic nature ofthe arachnoid cysts. The risk of bleeding does not exceed0.04% per annum.2When bleeding does occur, most cases areassociated with head injury. In this case, there was no reportof injury, which makes this case even rarer. The most plausi-ble hypothesis was spontaneous bleeding. According to Patelet al, the source of the bleeding was in the communicatingvessels between the dura and the outer face of the cysticmembrane.6 Bleeding may occur not only in the cyst, but inthe subdural and epidural extra space as well.1 However,intra-cystic hemorrhage is an extremely rare complication,
Fig. 1 Arachnoid cyst without bleeding. Exam date: May 28, 2014.
Fig. 2 Acute subdural hemorrhage. Exam date: July 4, 2014.
Fig. 3 The CT scan after a month of the craniotomy showing theresolution of the subdural hemorrhage. Exam date: August 6, 2014.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Arachnoid Cyst with a Non-traumatic Acute Subdural Hematoma Cavasana et al. 123

which still remains with its pathogenesis unknown.1 Thiscomplication was visibly present in our patient.
In a case-control study, we observed that the larger thecyst size, especially if the cysts have a maximum diameterlarger than 5 cm, the greater the chance of disruption andassociated complications, such as hygroma, subdural hema-toma, and intra-cystic bleeding.7
Moreover, signs of intracranial hypertension, seizures,macrocrania, and delayed development in the last thirtydays must be considered warning signs of cyst rupture.2
Based on the literature reviewed, treatment is essentiallysurgical, although largely contingent on the patients symp-toms. Surgery is indicated when there are important symp-toms and/or complications of the disease. In asymptomaticpatients, there is no consensus in the literature for thesurgical treatment.
We found that patients with symptomatic arachnoid cystscan safely undergo a key-hole craniotomy and drainageprocedure with reported success.6,8
Conclusion
Arachnoid cysts are usually incidental findings in neuroim-aging and more common in pediatric patients, appearingasymptomatic in most cases. Its pathophysiology is currentlynot well explained. The diagnosis iswell established by a headCT without contrast or MRI. The literature also suggests thatvascular imaging tests should be requested for patients witharachnoid cyst who presented headache.9
The most common symptom in this case is the headache.Treatment is primarily surgical in symptomatic cases and/orwhen complications are present. Patients with arachnoid cystwith presence of warning signs should be investigated forrupture and bleeding of the lesion.
Complementary InformationWe conducted this study at the institution Santa Casa deMisericórdia de Araçatuba, in the town of Araçatuba, in thestate of São Paulo, Brazil.
References1 Akyuz M, Goksu E, Aralasmak A, Tuncer R. Retroclival arachnoid
cyst presenting with haemorrhage: a brief report of a special case.Acta Neurochir (Wien) 2010;152(1):161–162
2 Henriques JGB, Pianetti Filho G, Henriques KSW, et al. Spontane-ous acute subdural hematoma contralateral to an arachnoid cyst.Arq Neuropsiquiatr 2007;65(4A, 4a)1034–1036
3 Hong JC, Kim MS, Chang CH, Kim SH. Arachnoid cyst withspontaneous intracystic hemorrhage and chronic subdural hema-toma. J Korean Neurosurg Soc 2008;43(1):54–56
4 Iaconetta G, Esposito M, Maiuri F, Cappabianca P. Arachnoid cystwith intracystic haemorrhage and subdural haematoma: casereport and literature review. Neurol Sci 2006;26(6):451–455
5 Zanini MA, Gabarra RC, Faleiros AT, Freitas CC, Alves A. [Cerebralaneurysm and arachnoid cyst: about a case with intracystichemorrhage]. Arq Neuropsiquiatr 2000;58(2A):330–335
6 Patel RA, Levy ML, Crawford JR. Spontaneous subdural haemor-rhage in a childwith bilateral middle cranial fossa arachnoid cysts.BMJ Case Rep 2013;2013:xx
7 Cress M, Kestle JR, Holubkov R, Riva-Cambrin J. Risk factors forpediatric arachnoid cyst rupture/hemorrhage: a case-controlstudy. Neurosurgery 2013;72(5):716–722, discussion 722
8 Scheel M, Bauknecht HC. Teaching neuroimages: head bangingwithout head trauma: subdural hemorrhage in association witharachnoid cysts. Neurology 2011;76(12):e60
9 Shimizu J, Matsumoto M, Yamazaki E, Yasue M. An aneurysmrupturing into a middle cranial fossa arachnoid cyst presenting asan intracystic hemorrhage. J Stroke Cerebrovasc Dis 2012;21(3):243–244
Fig. 4 Arachnoid cyst without bleeding. Exam date: August 6, 2014.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Arachnoid Cyst with a Non-traumatic Acute Subdural Hematoma Cavasana et al.124
Intramedullary Spinal Capillary Hemangioma:Case Report
Hemangioma capilar intramedular: relato de caso
Leonardo Welling1 Mariana S. Welling1 Eberval G. Figueiredo2
1Universidade Estadual de Ponta Grossa, Ponta Grossa, Paraná, Brazil2Universidade de São Paulo, São Paulo, São Paulo, Brazil
Arq Bras Neurocir 2017;36:125–127.
Address for correspondence Leonardo Welling, PhD, UniversidadeEstadual de Ponta Grossa, Av. General Carlos Cavalcanti, 4748,Uvaranas, Ponta Grossa, PR, 84030-900 Brazil(e-mail: [email protected]).
Introduction
Capillary hemangiomas involving the neuraxis are very un-common. In the spinal cord, they are located mainly intra-dural and extramedullary.1 According to the literature,
vascular lesions account for approximately 6%–7% of all intra-dural spinal tumors, although intramedullary capillary areextremely rare.2 To our knowledge, only four cases in conusmedullaris have been previously described since the earliestpublication in 1987.3
Keywords
► intramedullary► spinal► tumor
Abstract Capillary hemangiomas involving the neuraxis are very uncommon. In the spinal cord,they are located mainly intradural and extramedullary. To our knowledge, only fourcases in conus medullaris have been previously described. In our case, a 46-year-old manwas admitted with back pain, sphincter disturbances, as well as progressive weaknessand numbness on the lower extremities. Magnetic resonance imaging revealed anundefined intramedullary lesion on the conus medullaris. The patient underwentmicrosurgery, which achieved complete removal. Histopathological diagnosis wascompatible with capillary hemangioma. His postoperative course was uneventful andall symptoms, including bladder dysfunction clearly regressed. The treatment ofintramedullary capillary hemangiomas is very critical in preventing unnecessarymorbidity, providing accurate information with respect to prognosis, and establishesa regular outpatient follow-up. The natural history of this lesion involving the spinal cordis not well described, although they are common elsewhere in the body.
Palavras-chave
► intramedular► medula► tumor
Resumo Hemangiomas capilares que envolvem o neuroeixo são raros. Quando localizados nacoluna vertebral, geralmente são intradurais e extramedulares. Até a presente datasomente 4 casos de hemangiomas no cone medular foram descritos. O caso refere-se aum homem de 46 anos com dor lombar, alterações esfincterianas, fraqueza eparestesias em membros inferiores de evolução progressiva. Ressonância magnéticademonstrou lesão no cone medular de aspecto indefinido. Submetido a remoçãomicrocirúrgica completa. Histopatológico compatível com hemangioma capilar. O pós-operatório ocorreu sem intercorrências e houve recuperação dos déficits, inclusive dadisfunção esfincteriana. O tratamento dessa lesão não deve acrescentar morbidade. Ahistória natural dessa lesão na medula espinhal ainda não está definida, apesar de seruma lesão comum em outras partes do organismo.
receivedAugust 1, 2015acceptedOctober 7, 2015published onlineDecember 14, 2015
DOI https://doi.org/10.1055/s-0035-1570100.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 125

Case Report
A46-year-oldmanwas admittedwith intermittent back pain of12 months’ duration, which was intractable to medical treat-ment. The pain got worse and the patient presented withsphincter disturbances as well as progressive weakness andnumbness on the lower extremities three months prior to hisadmission. Aneurological examination showed amusclepower
of Grade ⅘ of the bilateral lower limbs. Magnetic resonanceimaging (MRI) of the lumbar spine revealed an undefinedintramedullary lesion on the conus medullaris. The lesionwas 24 mm (height), 15 mm (anterior-posterior), 19 mm(latero-lateral) in size. The lesionwas isointense onT1-weight-ed images and mildly hypertensive on T2-weighted images,with marked enhancement after contrast material injection(►Fig. 1A, 1B). The patient underwent microsurgery and
Fig. 1 MRI of the lumbar spine. The lesion was mildly hyperintense on T2-weighted images, with marked enhancement after contrast materialinjection.
Fig. 2 (A) MRI of the thoracic spine performed after 6 months revealed no residual lesion. (B) Histopathological diagnosis was compatible withcapillary hemangioma. (C) Tumor section with CD31 immunostaining showing positive staining.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Intramedullary Spinal Capillary Hemangioma Welling et al.126

complete remove was achieved. Histopathological diagnosiswas compatible with capillary hemangioma (►Fig. 2B, 2C). Hispostoperative coursewas uneventful and all symptoms, includ-ing bladder dysfunction clearly regressed. MRI of the thoracicspine performed after 6 months revealed no residual lesion(►Fig. 2A).
Discussion
Capillary hemangiomas are benign tumors that are most oftenencountered in the skin and soft tissues.3 To our knowledgeonly four cases in conus medullaris have been previouslydescribed (►Table 1).2,4–6 Similar to those of common intra-medullary tumors, the clinical symptoms of intramedullarycapillary hemangiomas are sensory, motor, or sphincter dys-functions, which eventually appear in the late stages of lesionprogression. Furthermore, pain is the most common initialsymptom in patients with intramedullary capillary hemangio-mas, and the duration of illness is usually longer (> 6 months)than intramedullary gliomas.1 The main differential diagnosisis cavernous angiomas. Capillary hemangiomasusually presentwith slowly progressive worsening of symptoms, while cav-ernous angiomas are often associated with acute neurologicaldeterioration due to bleeding.1,3
The treatments of intramedullary capillary hemangiomasis very critical in preventing unnecessary morbidity, provid-ing accurate information with respect to prognosis, andestablish a regular outpatient follow-up. The natural history
of this lesion involving the spinal cord is not well described,although they are common elsewhere in the body.3
Conclusion
The present case suggests that capillary hemangiomas shouldbe considered in the differential diagnosis of a patient withintramedullary spinal vascular lesions. Complete resectionusing standardmicro-neurosurgical techniques is the goal fortreatment of intramedullary capillary hemangiomas.
References1 Wu L, Deng X, Yang C, Xu Y. Intramedullary spinal capillary
hemangiomas: clinical features and surgical outcomes: clinicalarticle. J Neurosurg Spine 2013;19(4):477–484
2 Nowak DA, Widenka DC. Spinal intradural capillary haeman-gioma: a review. Eur Spine J 2001;10(6):464–472
3 Abe M, Tabuchi K, Tanaka S, et al. Capillary hemangioma of thecentral nervous system. J Neurosurg 2004;101(1):73–81
4 Andaluz N, Balko MG, Stanek J, Morgan C, Schwetschenau PR.Lobular capillary hemangioma of the spinal cord: case report andreview of the literature. J Neurooncol 2002;56(3):261–264
5 Mawk JR, Leibrock LG, McComb RD, Trembath EJ. Metamericcapillary hemangioma producing complete myelographic blockin an infant. Case report. J Neurosurg 1987;67(3):456–459
6 Roncaroli F, Scheithauer BW, KraussWE. Capillary hemangioma ofthe spinal cord. Report of four cases. J Neurosurg 2000;93(1, Suppl)148–151
Table 1 Cases previously published (in conus medullaris)
Author/ year Age Sex Symptoms Treatment Outcome
Mawk et al.5 7 months M Lower extremity apraxia Subtotal removal Recovery at 3 weeks
Roncaroli et al.6 53 M Back and leg pain Subtotal removal Little improvement at 1.5 years
Roncaroli et al.6 74 M Lower extremity weakness Subtotal removal No improvement at 1 year
Andaluz et al.4 41 M Back pain Total removal Good recovery at 6 months
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Intramedullary Spinal Capillary Hemangioma Welling et al. 127

Retrograde Endovascular Approach for TreatingUnruptured Basilar Apex Aneurysms: Two CaseReports and Review of Literature
Acesso endovascular retrógrado no tratamento deaneurismas não rotos do ápice basilar: relato de doiscasos e revisão da literatura
Marcus Alexandre Rotta1 Guilherme M. Dias1 André Luiz Rezende1 Felix H. Pahl1
Matheus Fernandes Oliveira1 José Marcus Rotta1
1Department of Neurosurgery, Hospital do Servidor Público Estadualde São Paulo, IAMSPE, São Paulo, São Paulo, Brazil
Arq Bras Neurocir 2017;36:128–132.
Address for correspondence Matheus Fernandes Oliveira, MD,Department of Neurosurgery, IAMSPE, Av. Loefgreen 700, Apto 103,Vila Mariana, São Paulo, São Paulo, Brazil, 04040-000(e-mail: [email protected]).
Keywords
► endovascular► aneurysm► treatment
Abstract Background Treatment of target lesions when parent vessels are injured or diseasedmay be quite difficult. Moret et al have proposed an endovascular technique based onretrograde transcirculation approach through communicating vessels.Methods We report on the first Brazilian experience with retrograde endovascularapproach, to the best of our knowledge.Results The two cases illustrate difficult anterograde approach techniques to treatbasilar apex aneurysms. In the first case, tortuosity and angulation of both vertebralarteries associated to stenosis did not allow an anterograde approach. In the secondcase, after a SAH of a basilar apex aneurysm treated more than a decade ago withbilateral vertebral artery trapping, the patient underwent a retrograde approach.Conclusion For this approach, follow-up data are still lacking and complications areusually more common than in anterograde approach. Nevertheless, in select cases, itmay be applied by experienced hands with acceptable risks when no other treatmentoption (surgical or endovascular) is available.
Palavras-chave
► endovascular► aneurisma► tratamento
Resumo Introdução O tratamento de lesões específicas quando vasos são danificados, ficamdoentes ou inacessíveis pode se tornar bastante difícil. Moret et al propuseram umatécnica endovascular baseada no acesso retrógrado pelos vasos comunicantes.Métodos Primeira experiência Brasileira em acesso endovascular retrógrado, segundoos autores do presente estudo.Resultados Os dois casos demonstram técnicas de difícil acesso anterógrado paratratar aneurismas do ápice basilar. No primeiro caso, a tortuosidade e a angulação deambas as artérias vertebrais associadas à estenose não permitiram acesso anterógrado.No segundo caso, após hemorragia subaracnóidea do aneurisma de ápice basilar
receivedAugust 12, 2015acceptedOctober 8, 2015published onlineDecember 14, 2015
DOI https://doi.org/10.1055/s-0035-1570116.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de Caso128

Introduction
Although endovascular treatment has progressively advancedover the last years, the treatment of target lesions whenparent vessels are injured, diseased, or tortuous may be quitedifficult. In this sense, Moret et al1 have proposed an endo-vascular technique based on the retrograde transcirculationapproach through communicating vessels.2,3 It involves thenavigation of a catheter, balloon, or stent delivery deviceeither from one arterial side to the other or from the anteriorto the posterior circulation.2–5
We report two cases treated with the retrograde endo-vascular approach, which are the first Brazilian experiences,to the best of our knowledge.
Case 1
A 67-year-old white woman presented for neuroradiologicalinvestigation of a 6-month history of progressively worseningpulsatile headache. Her past medical history was positive forsmoking, diabetes mellitus, and arterial hypertension. She deniedany family history of intracranial aneurysms. Her clinical andneurological examinations were unremarkable. Magnetic reso-nance imaging (MRI) of thebrain revealeda saccular aneurysmof�6mm in the basilar artery apex. She was then forwarded for acerebral angiogram (►Fig. 1), which disclosed a solitary saccularaneurysm in the basilar apex.
Due to the size and location of aneurysm, associated withother risk factors like smoking and hypertension, we proposed
tratado há mais de uma década com oclusão de artéria vertebral bilateral, realizou-seum acesso retrógrado.Conclusão Para este acesso, dados subsequentes ainda são necessários, e complica-ções ainda são mais comuns que em acesso anterógrado. Mesmo assim, pode seraplicado em casos específicos com riscos aceitáveis e em mãos experientes, quandonenhum outro tratamento (cirúrgico ou endovascular) seja possível.
Fig. 1 (A) Angiogram of patient number 1, which disclosed accentuated angulation of tortuosity of vertebral arteries. (B) Retrograde approachrevealing basilar apex aneurysm. (C) Embolization performed with coils through retrograde approach.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Retrograde Endovascular Approach for Treating Unruptured Basilar Apex Aneurysms Rotta et al. 129

aneurismal treatment by endovascular approach. During theendovascular approach, it was very difficult to catheterizebothvertebral arteries due to extreme tortuosity and segmentalstenosis (►Fig. 1A). When we achieved catheterization of theleft vertebral artery, the endovascular catheter interrupted theblood flow and, thus, we aborted the procedure. Although wecould have attempted angioplasty and stenting of proximalvertebral artery to allow catheter progression, such a proce-dure usually entails a high probability of late restenosis and,consequently, unsuccessful stenting.
Therefore, the endovascular team catheterized the leftcarotid artery with a Simmons catheter to approach aneurys-mal sac, reaching the aneurysm by a retrograde transcircu-lation approach (►Fig. 1B). Despite being amore complex andtechnically difficult procedure given that anterior circulationwas also affected by atherosclerotic plaques, we performedembolization cautiously with slow progression of catheterand gentle manipulation, which resulted in success withoutcomplications (►Fig. 1C). The patient recovered well and wasdischarged without deficits.
Fig. 2 MRI of patient number 2 in three moments: (A) after aneurismal diagnosis; (B) after trapping of vertebral arteries and worsening ofsymptoms, revealing perianeurysmal edema in FLAIR; (C) in immediate post retrograde approach embolization, showing decrease inperianeurysmal edema.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Retrograde Endovascular Approach for Treating Unruptured Basilar Apex Aneurysms Rotta et al.130

Case 2
A 62-year-old white woman presented with progressiveheadache for two years in 2001. Her past medical historywas negative for smoking, alcohol intake, and medicationuse. She mentioned having diabetes mellitus and arterialhypertension. Moreover, she denied any family history ofintracranial aneurysms and her clinical and neurologicalexaminations were unremarkable. Brain MRI showed asaccular aneurysm of �20 mm at the basilar apex(►Fig. 2A). At the time, an angiogram revealed a giantbasilar artery apex aneurysm (►Fig. 3A). The patient wasforwarded for aneurysmal treatment, but missed follow-up.
Oneyear later, shewas admitted to our emergency roomwithsubarachnoid hemorrhage (SAH) Fisher IV and Hunt Hess IV. Atthe time, we proposed aneurysmal treatment by endovascularapproach. We performed an endovascular trapping of bothvertebral arteries with coils (►Fig. 3B). The patient was dis-chargedwith a GOS of 4 and recoveredwell, maintaining annualfollow-up. In2005, thefollow-upangiogramevidencedapartiallythrombosed giant basilar apex aneurysm filling from anteriorcirculation (►Fig. 3C). Nonetheless, the patient remainedasymptomatic.
Six months prior to this present study conclusion, she hadbegun complaining of pulsatile headache and gait disturbance.Her clinical andneurological examinations revealed a right-sidedcomplete hemiparesis (Grade IV). Brain MRI showed a partiallythrombosed aneurysm increasing in size and with remarkableperineurysmal edema (►Fig. 2B). Another angiogram revealed abasilar artery apex aneurysm (►Fig. 3D). At this point, since theaneurysm was increasing and the patient was symptomatic, adecision was made to perform treatment.
During the endovascular approach, given that both vertebralarteries were trapped, it was necessary to reach both carotidarteries and perform a retrograde treatment (►Fig. 3D). Bothposteriorcommunicatingarterieswerepatentandlarge,allowingforembolizationofaneurysmwithcoilsandposteriorpositioningof right P1 to left P1 with Solitaire stent without complications(►Fig. 3D). The patient recovered well and was dischargedwithout new deficits. Immediate post-procedure MRI revealeddecreased perianeurysmal edema (►Fig. 2C).
Discussion
Both cases discussed here illustrated difficult anterogradeapproach techniques to treat basilar apex aneurysms. In thefirst case, tortuosity and angulation of both vertebral arteries
Fig. 3 Angiogram of patient number 2: (A) after basilar apex aneurysm diagnose and before vertebral trapping; (B) after vertebral trapping,revealing retrograde filling of aneurysm with partially thrombosed component; (C) follow-up angiogram, disclosing increasing size of aneurysm;(D) at the onset of symptoms and during retrograde approach embolization with stent delivery.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Retrograde Endovascular Approach for Treating Unruptured Basilar Apex Aneurysms Rotta et al. 131

associated with stenosis did not allow an anterograde ap-proach. In the second case, after a SAH of a basilar apexaneurysm treated more than a decade ago with bilateralendovascular vertebral artery trapping, the approach usedwas the retrograde. Both cases recovered well withoutcomplications.
Transcirculation catheterization, also knownas the retrogradeapproach, involves the navigation of a catheter, a balloon, or astent delivery device either from one arterial side to the other, orfrom the anterior to the posterior circulation.1–5 The rationalebehind it lies on the existence of patent collateral circulation.Thus, adequate patency is required either for the posterior(PComA) and anterior communicating arteries (ACoA) or forboth vertebral arteries (VAs).
In all cases, a special set must be ready to perform retrogradeapproach. The most important difference is that, once targetlesions are reached against the bloodstream, two proximalarteries must be punctured: one to manipulate the catheterand the other to provide intravenous contrast and guide retro-grade navigation. In our first case, retrograde approach wasperformed through carotid artery and contrast was injected byvertebral artery. In the second case, we used one carotid for theretrograde approach and the other for contrast injection.
Then, navigation may be divided in two parts, one alongthe bloodstream and the other against bloodstream. Whilethe first is a common approach, the latter must be conductedwith slow progression of the catheter and gentle manipula-tion, to avoid vessel injury. We prefer using Simmons cath-eters, which allows gentle movements. Catheter size shouldnot be different from those applied in anterograde ap-proaches. Smaller sizes increase difficulty of catheter pro-gression and larger sizes, although easier to navigate, mayincrease risks for vascular insufficiency in vessels alreadyinjured and overloaded.
When reaching the target lesion, it is necessary tostrengthen precautions during treatment, since the cathetermay shift during coiling and the coils may migrate distally.
Such a technique is particularly effective for treating wide-necked basilar apex, ACoA aneurysms, aneurysms involving afetal PComA, superior cerebellar artery (SCA) aneurysms,intracranial vertebral artery (V4 segment) aneurysms, carotidterminus aneurysms, and posterior inferior cerebellar artery(PICA) aneurysms.1–3 Simultaneous angiography through thetwo target brachiocephalic vessels delineates adequately theroute of catheterization. Transcirculation navigation of acatheter, a balloon, or a stent-deployment device facilitatesprimary coiling of the aneurysm. The technique describedwas developed to allow optimal treatment of aneurysms thatotherwise were difficult or impossible to access.2–5
Moret et al1 have pioneered the technique and reached theresult of completelyor near completelycoiled aneurysms in all 12cases described.1 Two complications occurred as a result oftreatment. One patient developed status epilepticus and thesecond complication occurred in a patient with an ICA terminus
aneurysm who developed a thrombus within the M1 arterialsegment, which was treated with thrombolysis.1
Moret et al emphasized the role of three-dimensionalangiography for the success of transcirculation catheteriza-tion.1 Not only can three-dimensional angiography demon-strate the optimal working angle for parent vesselpreservation during coiling, but it can also be used to opti-mize visualization of the transcirculation route.1
Albuquerque et al2 stated that these techniques are invalu-able in the treatment of complex cerebral aneurysms. Theiruse, however, should be reserved for patients for whom therisks of leaving their aneurysms untreated are high.2 Thecomparative morbidity and mortality associated with a con-ventional surgical approach should also be weighed againstthe risks of these technically challenging endovascular ap-proaches. Their series was the largest number of patientstreated through transcirculation routes.2
Other reports have documented the transcirculationdeployment of stents for the treatment basilar apex aneur-ysms, ICA terminus aneurysms, and ACoA aneurysms.3–5
Conclusions
Long-term follow-up in patients treatedwith this technique isnot yet available. Additionally, complications are usuallymore common than those in anterograde approach.1,2 Nev-ertheless, in select cases with better indication for endovas-cular procedures (such as basilar apex aneurysms), it may beapplied with acceptable risks in experienced hands when noother treatment option (surgical or endovascular) is available.
Conflicts of InterestThe authors declare no conflicts of interest.
References1 Moret J, Ross IB, Weill A, Piotin M. The retrograde approach: a
consideration for the endovascular treatment of aneurysms. AJNRAm J Neuroradiol 2000;21(2):262–268
2 Albuquerque FC, Gonzalez LF, Hu YC, Newman CB, McDougallCG. Transcirculation endovascular treatment of complex cere-bral aneurysms: technical considerations and preliminaryresults. Neurosurgery 2011;68(3):820–829, discussion 829–830
3 Caplan J, Huang J, Tamargo R, Radvany M. E-032 retrograde stent-assisted coil embolization of posterior communicating arteryaneurysms. J Neurointerv Surg. 2014;6(Suppl 1):A52
4 Cho YD, Kim KM, Lee WJ, Kang HS, Kim JE, Han MH. Retrogradestenting through the posterior cerebral artery in coil embolizationof the posterior communicating artery aneurysm. Neuroradiology2013;55(6):733–739
5 Heye S, Stracke CP, Nordmeyer H, Heddier M, Stauder M, Chapot R.Retrograde access to the posterior inferior cerebellar artery inballoon-assisted coiling of posterior inferior cerebellar arteryaneurysms. J Neurointerv Surg 2015;7(11):824–828
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Retrograde Endovascular Approach for Treating Unruptured Basilar Apex Aneurysms Rotta et al.132

Disc Herniation and Cyst Gas: A Rare AssociationCausing Radicular Compression
Herniação de gás intraespinal: uma associação raracausando compressão radicular
Cherkaoui Mandour1 Miloudi Gazzaz1 Brahim el Mostarchid1
1Department of Neurosurgery; Military Hospital Mohammed V,Rabat, Morocco
Arq Bras Neurocir 2017;36:133–135.
Address for correspondence Cherkaoui Mandour, MD, Department ofNeurosurgery, Military Hospital Mohammed V, Rabat 10000, Morocco(e-mail: [email protected]).
Keywords
► disc herniation► gas pseudocyst► sciatica
Abstract Introduction Intraspinal gas is a common clinical finding, but an epidural gaspseudocyst in association with lateral disc herniation compressing a nerve root is anexceptional observation.Case Report A 49-year-old man was admitted to our department presenting withsciatica. The neurological examination demonstrated moderate lumbar pain withoutneurological deficit. A lumbosacral computed tomography showed the presence ofdegenerated disc herniation and epidural gas collection.Discussion The pathological association between the cyst and the hernia is probablydue to the migration of gas pumped from the intervertebral space through a breakingpoint or lower in the annulus fibrosis, involving its contiguity with the herniated disc.Conclusion An association between a disc herniation and a gas pseudocyst can be acause of sciatica.
Palavras-Chave
► hérnia discal► pseudocisto de gás► ciática
Resumo Introdução O gás intraespinal é um achado clínico comum, mas um pseudocistoepidural de gás associado a herniação discal lateral comprimindo uma raiz nervosa éuma observação excepcional.Relato de caso Um homem de 49 anos de idade foi admitido em nosso departamentoapresentando sintomas de ciática. O exame neurológico demonstrou dor lombarmoderada sem déficit neurológico. A tomografia computadorizada lombossacralmostrou presença de hérnia discal degenerada e coleta epidural de gás.Discussão A associação patológica entre o cisto e a hérnia é provavelmente devida àmigração do gás bombeado do espaço intervertebral através de um ponto de rupturaou menor na fibrose do anel, envolvendo a sua contiguidade com o disco herniado.Conclusão Uma associação entre uma hérnia de disco e um pseudocisto de gás podeser uma das causas de ciática.
receivedFebruary 18, 2017acceptedApril 7, 2017
DOI https://doi.org/10.1055/s-0037-1603986.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 133

Introduction
The most common causes of lumbar radiculopathy are inter-vertebral disc herniation and lumbar canal stenosis.1 Intra-spinal extradural masses like disc cysts, perineural cysts,synovial cysts, and ganglion cysts are rare causes.1
Intraspinal gas has been reported in several situations,including craniocervical trauma, epidural anesthesia, spinalsurgery, infection and tumors.2 First reported in 1980 byGulati and Weinstein,3 an association between disk hernia-tion and gas pseudocyst has rarely been reported ever since.We report a case of this unusual clinical presentation.
Case Report
A 49-year-old Moroccan man was admitted to our depart-ment presenting with sciatica for 10 days. The neurologicalexamination objectified a moderate low back pain withoutneurological deficit. A lumbosacral spine computed tomog-raphy scan (►Fig. 1: Panel A and B) showed the presence of adegenerated disc hernia and an epidural gas collection withevidence of root compression. The patient refused surgeryafter improvement achieved under medical treatment.
Discussion
Gas in the intervertebral disk space is a relatively commonradiologic finding, seen in 46% of cases on computed tomog-raphy examinations.4 However, the existence of gas withinthe spinal canal has been seen in only a few cases in theliterature worldwide,5 and an epidural gas pseudocyst com-pressing a nerve root associatedwith a lateral disc herniationis also a rare clinical presentation.6,7
This pathological association between the cyst and thehernia is probably due to the migration of gas pumped from
the intervertebral space through a breaking point in the annu-lus fibrosis, involving its contiguity with the herniated disc.8
The vacuum phenomenon in the intervertebral disk spaceand gas accumulation in the epidural space can be bettercharacterized with CT by its typical attenuation values. Also,associated findings include osteophytes of adjacent vertebralbodies and degeneration of discs;6 but magnetic resonanceimaging is a good modality for evaluation of the interverte-bral disc, the spinal cord and the nerve roots.9
Surgery is the preferred treatment in chronic encapsulatedlesions thatdonot resolvewithconservativemanagement.10,11
Conclusion
Through this clinical case, wefind that an association betweenadischerniationandanepiduralgaspseudocyst canbea causeof sciatica.
References1 Jeong GK, Bendo JA. Lumbar intervertebral disc cyst as a cause of
radiculopathy. Spine J 2003;3(03):242–2462 Ilica AT, Kocaoglu M, Bulakbasi N, Kahraman S. Symptomatic
epidural gas after open diskectomy: CT and MR imaging findings.AJNR Am J Neuroradiol 2006;27(05):998–999
3 Gulati AN, Weinstein ZR. Gas in the spinal canal in associationwith the lumbosacral vacuum phenomenon: CT findings. Neuror-adiology 1980;20(04):191–192
4 Belfquih H, El Mostarchid B, Akhaddar A, gazzaz M, Boucetta M.Sciatica caused by lumbar epidural gas. Pan Afr Med J 2014;18:162
5 Lardé D, Mathieu D, Frija J, Gaston A, Vasile N. Spinal vacuumphenomenon: CT diagnosis and significance. J Comput AssistTomogr 1982;6(04):671–676
6 Hidalgo-Ovejero AM, Martinez-Grande M, Garcia-Mata S; HI-DALGO OVEJERO A.M. Disc herniation with gas. Spine 1994;19(19):2210–2212
Fig. 1 Sagittal reformatted (Panel A) and axial reformatted (Panel B) computed tomography image of lumbosacral spine showing clearly alateral disc herniation and gas pseudocyst with evidence of root compression.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Disc Herniation and Cyst Gas Mandour et al.134

7 Battal B, Bozlar U, Sanal H, Saglam M, Bulakbasi N, Ustunsoz B.Symptomatic epidural gas accumulation originating fromvacuumphenomenon in the intervertebral disc: CT imaging findings. TheInternet Journal of Radiology. 2008;10(01):1–4
8 Salpietro FM, Alafaci C, Collufio D, et al. Radicular compression bylumbar intraspinal epidural gas pseudocyst in association withlateral disc herniation. Role of the posterior longitudinal liga-ment. J Neurosurg Sci 2002;46(02):93–95, discussion 95
9 Giraud F, Fontana A, Mallet J, Fischer LP, Meunier PJ. Sciaticacaused by epidural gas. Four case reports. Joint Bone Spine 2001;68(05):434–437
10 Tamburrelli F, Leone A, Pitta L. A rare cause of lumbar radiculo-pathy: spinal gas collection. J Spinal Disord 2000;13(05):451–454
11 Demierre B, Ramadan A, Hauser H, Reverdin A, Rilliet B, Berney J.Radicular compression due to lumbar intraspinal gas pseudocyst:case report. Neurosurgery 1988;22(04):731–733
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Disc Herniation and Cyst Gas Mandour et al. 135

Orbital Lymphangioma: Case Report andManagement Paradigms
Linfoma de órbita: relato de caso e paradigmas domanejo clínico
Alex Roman1 Larissa Bianchini1 Bárbara Battistel1 Miguel Franzoi Neto1 Daniela Schwingel1
1Hospital São Vicente de Paulo, Passo Fundo, RS, Brazil
Arq Bras Neurocir 2017;36:136–140.
Address for correspondence Alex Roman, MD, Hospital São Vicentede Paulo, R. Teixeira Soares, 808, Centro, Passo Fundo, RS, 99010-080,Brazil (e-mail: [email protected]).
Keywords
► orbitallymphangioma
► sildenafil► orbital tumors
Abstract Introduction Lymphangioma is a rare congenital vascular malformation of the headand neck region isolated from the systemic circulation. It has a benign etiology, andrepresents 1–3% of all orbital tumors. These hamartomas often present in the pediatricpopulation with a slightly female predilection. They have a lymphocytic composition,and may increase in size with episodes of viral infection, causing proptosis.Discussion The management of this lesion is controversial, hardly curative, anddepends on the clinical presentation. The treatment options include partial surgicalresection of the major cyst, needle aspiration, surgical debulking, systemic steroids,sildenafil, intralesional injection of the sclerosing agents, and local radiotherapy.Case Report In the present report, we describe an uncommon case of lymphangiomain a 6-year-old female who was first submitted to neurosurgery for tumor resection andreceived sildenafil therapy later, with promising results.Conclusion The treatment of orbital lymphangiomas remains a controversial topic,and the use of sildenafil along with needle aspiration and microsurgical removal is aviable option of treatment. However, many issues, such as the ideal duration of thetherapy, the dosage regimen and the recurrence rate, still remain unclear. Our casereport adds promising data on this pathology, even though larger trials are needed toproperly elucidate the remaining questions.
Palavras-chave
► linfangioma de órbita► sildenafil► tumores de órbita
Resumo Introdução Linfangioma é uma malformação vascular rara congênita da cabeça e daregião cervical isolada da circulação sistêmica. Apresenta uma etiologia benigna erepresenta 1–3% de todos tumores orbitais. Estes hematomas geralmente se apre-sentam na população pediátrica com uma pequena predileção pela populaçãofeminina. Têm uma composição linfocítica e podem aumentar em tamanho comepisódios de infecções virai causando proptose.Discussão O manejo destas lesões é controverso, dificilmente curativo e depende naapresentação clínica. Opções de tratamento compreende ressecção cirúrgica parcialdo cisto de maior volume, aspiração por agulha de punção, redução cirúrgica,
receivedJanuary 23, 2017acceptedMarch 16, 2017published onlineMay 31, 2017
DOI https://doi.org/10.1055/s-0037-1603556.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Miscellaneous | Artigo de Atualização136

Introduction
Lymphangioma is a rare congenital vascular malformationof the head and neck region isolated from the systemiccirculation.1 It has a benign etiology, and represents 1–3% ofall orbital tumors.2 These hamartomas often present in thepediatric population with a slightly female predilection.They have a lymphocytic composition, and may increase insize with episodes of viral infection, causing progressiveproptosis.2–4 The management of this lesion is controver-sial, hardly curative, and depends on the clinical presenta-tion. The treatment options include partial surgicalresection of the major cyst, needle aspiration, surgicaldebulking, systemic steroids, sildenafil, intralesional injec-tion of the sclerosing agents, and local radiotherapy.5–7 Inthe present study, we describe an uncommon case oflymphangioma in a 6-year-old female who was first sub-mitted to neurosurgery for tumor resection and receivedsildenafil therapy later.
Case Report
A 6-year-old female patient presented to the neurosurgerydepartment referring right eye redness. She did not have anyknowncomorbidities orallergies. Thepatient’s father reportedthe symptoms had been present for approximately tenmonths, and had had an insidious and progressive courseduring this period. Upon examination, the patient’s eyelids,extra ocular movement and pupillary, as well as consensuallight reflex were preserved, the cornea had no signs ofinflammatory reaction, and there was tarsal-conjunctivalhyperemia. A magnetic resonance imaging (MRI) exam ofthehead andorbit revealed a largemultiloculatedmass lesion,the presence of subtle septations inside the right orbit, infero-lateral eyeball displacement, and slight stretch of the opticnerve’s extrinsic muscles (►Fig. 1). The lesion partially sur-rounded the optic nerve, and had dimensions of 3.4 cm x2.2 cm x 3.2 cm. It had no significant contrast enhancement,and an apparently liquid content. The patient was furtherinvestigated and submitted to a biopsy of the retro-orbitaltissue, which confirmed the diagnosis of lymphangioma. The
initial management indicationwas amicrosurgical procedure,with posterior pharmacological therapy. A right modifiedfronto-orbitozygomatic craniotomy approach was the choicefor accessing theorbit,with special attention to roofand lateralwall removal (►Fig. 2). The tumor was properly identifiedwith posterior cystic dissection and removal of the solidcomponent, as well as drainage of the fluid contents of thecystic portions of the lesion. After surgery, hydrocortisone (2.5mg/kg/day for 3 days) and sildenafil were prescribed, initiallyinadose of0.5mL/Kgofbodymassweight, taken3 times aday,later increasing the dose to 1mL/Kg (2.5mg/mL) of bodymassweight, and then increasing thedoseupto10 mg3 timesaday,according to EuropeanMedicine Agency (EMA) protocols. Thepatient evolved satisfactorily in the postoperative period,withpreservation of visual acuity and ocular motility, and signifi-cant improvement of the right-sided proptosis.
Discussion
Lymphangiomas display a singular combination of clinical,radiologic and histopathological features. The patients maypresent with either slowly progressive symptoms, or suddenpain and tumor enlargement precipitated by an acutehemorrhage.8Wright et al1 reported that the most prevalentmanifestation in patients is mass effect (42%), followed byhemorrhage (37%), ocular motility changes (28%), and prop-tosis (15%). In advanced stages of the disease, the patientsmay also develop ophthalmoplegia and amaurosis.9 Histo-pathologically, the orbital lymphangioma is a cystic non-capsulated lesion with irregular thin-walled vascular chan-nels (►Fig. 3), not proliferative, and with an attenuatedendothelial layer and collections of lymphocytes. The cystis classified as microcystic or macrocystic when it is smalleror greater than 10 mm in diameter respectively.1
Thepathogenesis of thesetumors remainsunclear. Recently,newadvances on the understanding of lymphatic biology havesuggested the role of lymphangiogenesis dysregulation in thedevelopment of this tumor.10 Angiopoietin 2, forkhead boxprotein C2 (FOX C2), lymphatic vessel endothelial hyaluronanreceptor 1 (LYVE 1), prospero homeobox 1 (PROX1),
esteroides sistêmicos, Sildenafil, administração intralesional de agentes esclerosantes,e radioterapia local.Relato de Caso No presente relato, descrevemos um caso incomum de linfangiomaem uma paciente feminina de seis anos de idade, inicialmente submetida a procedi-mento neurocirúrgica para ressecção tumoral, com posterior terapia com Sildenafil,apresentando resultados promissores.Conclusão O tratamento de linfangiomas de órbita permanece um tópico contro-verso, e o uso de Sildenafil em conjunto com aspiração por agulha de punção eressecção microcirúrgica é uma opção viável de tratamento. Entretanto, muitasquesitos tais como tempo de terapia, regime de dose e taxa de recorrência perma-necem incertos. Nosso relato de caso contribui com dados promissores referente a estapatologia, ainda que ensaios maiores são necessários para elucidação apropriadaacerca das questões pendentes.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Orbital Lymphangioma: Management Paradigms Roman et al. 137

podoplanin and vascular endothelial growth factor C (VEGF-C)are some of the gene products critical to lymphatic embryo-genesis.11 Genetic disorders that possibly correlate with lym-phangiomas at different sites havebeen reported aswell. Theseinclude neurofibromatosis type 1,12 Klippel-Trenaunay syn-drome,13 and tuberous sclerosis complex.14 Orbital lymphan-gioma was related in association with persistent fetalvasculature15 and retinal and iris malformations,16 amongother vascular system abnormalities.
Several imagingmethodsmay suggest the diagnosis of thetumor. Ultrasonography reveals a nonspecific irregularorbital lesion with low internal reflectivity, and has a rele-vant role mainly in young children.2 Contrast-enhancedcomputed tomography (CT) may show the presence ofcalcifications within the lesion, and provides useful informa-tion on the condition of the orbital wall, enabling theappropriate surgical resection. Magnetic resonance imagingis the best method to evaluate soft tissues and identify cysticfluid levels corresponding to hemorrhages of distinct ages.Old bleedings appear hyperintense in T1- and T2-weightedimages, and recent ones appear hypointense.10,11
Although there are many treatment modalities for orbitallymphangiomas currently available, there is not a well-established one. Furthermore, it is not completely definedif asymptomatic patients should be submitted to any sort ofprocedure. Spetzler et al12 concluded it is difficult to justify
early intervention in asymptomatic patients given thebenignbiology and high likelihood of recurrence of these lesions.Most authors agree intervention is required when there isvisual impairment, severe pain secondary to intraorbitalhypertension, repeated hemorrhagic episodes or significantcosmetic deformity.6,7,13 Total removal of lymphangiomaswithout orbit exenteration represents a surgical challengebecause they tend to infiltrate into the orbital structures, andmay result in severe bleeding during the procedure. There-fore, the goal of the surgery is rather to prolong the disease-free survival time and offer to the patient an improvement inquality of life. The pterional craniotomy is one of themost-often used routes to access the lesion. Alternatively, amodified frontotemporal orbitozygomatic approach mayalso be performed, as it was done in our patient. Thisapproach allows for an adequate exposure of the superiorand lateral orbital walls and reduces the need for retractionand manipulation of the orbital contents.8,12 Other treat-ment options are subtotal resection14, sclerosing agents, asOK-43215 or sodium morrhuate,16 as well as fractionatedβ-irradiation, but this may carry a unwanted risk of opticnerve damage. Moreover, percutaneous needle aspirationcan be executed with a significant recurrence rate.6 Thebenefit of sildenafil for the management of cystic lymphaticanomalies was first described by Swetman et al.5 This druginhibits phosphodiesterase-5, and produces vasodilation
Fig. 1 A and C: preoperative T2-weighted image (T2WI) MRI showing a large left intraorbital multiloculate lesion, with solid and cysticcomponents. B and D: postoperative T2WI MRI showing reduction in volume of the lesion, with diminished proptosis.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Orbital Lymphangioma: Management Paradigms Roman et al.138

followed by relaxation of the smooth muscles, cysticdecompression and normalization of endothelial dysfunc-tion, leading to lymphatic vasculature dilation and to theopening of the lymphatic spaces, potentially producing adecrease in lymphangioma volume and, therefore, raisingthe question about the further potential roles of sildenafil
in other vascular pathologies. We found only one otherreport in the literature of two cases in which sildenafilwas used specifically for orbital lymphangiomas.Both case studies showed an improvement in lesion sizeand symptoms, and had no adverse effects during thefollow-up period.17
Fig. 3 A and B: histopathology of the infraorbital mass, with hemangyomatose appearance, depicting different sized vessels with blood cells anddifferent staged hemorrhagic content, without any cell atypia.
Fig. 2 A and B before and after the removal of the orbital roof and lateral wall, with a modified frontoorbitozygomatic approach. C and D theextension of bony removal may be seen respectively in the outer and inner sides of the bone flap.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Orbital Lymphangioma: Management Paradigms Roman et al. 139

Conclusion
Sildenafil may be a viable non-invasive option for the treat-ment of orbital lymphangiomas, along with needle aspira-tion and microsurgical removal. However, many issues, suchas the ideal duration of the therapy, the dosage regimen andthe recurrence rate still remain unclear. Our case report addspromising data on this tumor, even though larger trials areneeded to properly elucidate the remaining questions.
References1 Wright JE, Sullivan TJ, Garner A, Wulc AE, Moseley IF. Orbital
venous anomalies. Ophthalmology 1997;104(06):905–9132 Guinto G, Guinto-Nishimura Y. Orbital lymphangiomas. World
Neurosurg 2014;81(5-6):708–7093 Seregard S, Sahlin S. Panorama of orbital space-occupying lesions.
The 24-year experience of a referral centre. Acta OphthalmolScand 1999;77(01):91–98
4 Alvi S, Kanona H, Penney S, Rothera MP, Bruce IA. Lymphaticmalformations. Otorhinolaryngologist 2014;7(02):95–99
5 Swetman GL, Berk DR, Vasanawala SS, Feinstein JA, Lane AT,Bruckner AL. Sildenafil for severe lymphatic malformations.N Engl J Med 2012;366(04):384–386
6 Sekhar LN, Tariq F. Orbital lymphangiomas: surgical treatmentand clinical outcome. World Neurosurg 2014;81(5-6):710–711
7 Nassiri N, Rootman J, Rootman DB, Goldberg RA. Orbital lympha-ticovenous malformations: Current and future treatments. SurvOphthalmol 2015;60(05):383–405
8 Simas N, Farias JP. Orbital lymphangiomas: surgical treatment andclinical outcomes.World Neurosurg 2014;81(5-6):842.e5–842.e10
9 Reem RE, Golden RP. Periocular hemangiomas and lymphangio-mas. Pediatr Clin North Am 2014;61(03):541–553
10 Bilaniuk LT. Vascular lesions of the orbit in children. Neuroima-ging Clin N Am 2005;15(01):107–120
11 Pahwa S, Sharma S, Das CJ, Dhamija E, Agrawal S. IntraorbitalCystic Lesions: An Imaging Spectrum Vol. 44. Elsevier; 2015
12 Russin JJ, Rangel-Castilla L, Kalani MYS, Spetzler RF. Surgicalmanagement, outcomes, and recurrence rate of orbital lymphan-giomas. J Clin Neurosci 2015;22(05):877–882
13 Pitz S, Dittrich M. Orbital lymphangioma. Br J Ophthalmol 2000;84(01):124–125
14 Saha K, Leatherbarrow B. Orbital lymphangiomas: a review ofmanagement strategies. Curr Opin Ophthalmol 2012;23(05):433–438
15 Yoon JS, Choi JB, Kim SJ, Lee SY. Intralesional injection of OK-432for vision-threatening orbital lymphangioma. Graefes Arch ClinExp Ophthalmol 2007;245(07):1031–1035
16 Kahana A, Bohnsack BL, Cho RI, Maher CO. Subtotal excision withadjunctive sclerosing therapy for the treatment of severe symp-tomatic orbital lymphangiomas. Arch Ophthalmol 2011;129(08):1073–1076
17 Gandhi NG, Lin LK, O’Hara M. Sildenafil for pediatric orbitallymphangioma. JAMA Ophthalmol 2013;131(09):1228–1230
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 2/2017
Orbital Lymphangioma: Management Paradigms Roman et al.140

Cervicomedullary Junction EpendymomaAssociated with NF2: A Case Report andLiterature Review
Ependimoma da junção cervicobulbar associado aneurofibromatose tipo II: relato de caso e revisão deliteratura
Otávio T. da Silva1
1Departament of Neurology, Neurosurgical division, UniversidadeEstadual de Campinas (Unicamp), Campinas-SP, Brazil
Arq Bras Neurocir 2017;36:141.
Address for correspondence Otávio T. da Silva, MD, DepartamentoNeurologia, Universidade Estadual de Campinas, Rua Tessália Vieirade Camargo, 126, Cidade Universitária, 13083-887 - Campinas,SP – Brasil (e-mail: [email protected]).
Dear Dr. Eberval Gadelha,I am grateful for the publication of our article Cervicomedul-
lary Junction Ependymoma Associated with NF2: a Case Reportand Literature Review (doi: 10.1055/s-0036-1597574), in thelast issueofBrazilianNeurosurgery,number1, volume36,2017.
However, I would like to express an acknowledgementregarding Figure number 2, as it was the work of Dr. RogerNeves Mathias, kindly given to Dr. Helder Tedeschi as acontribution to the referred study and to academic produc-tion as a whole. On behalf of all authors, I express ourgratitude for the images, in particular the one used on theissue cover.
Thanks,
Prezado Dr. Eberval Gadelha,Agradeço pela publicação de nosso artigo Ependimoma da
junção cervicobulbarassociadoaneurofibromatose tipo II: relatode caso e revisão de literatura (doi: 10.1055/s-0036-1597574),na última edição da Arquivos Brasileiros de Neurocirurgia,número 1, volume 36, 2017.
Entretanto, gostaria de fazer uma retratação referente àFigura número 2, feita por Dr. Roger Neves Mathias, egentilmente cedida ao Dr. Helder Tedeschi, como contrib-uição para o referido estudo, e para a produção acadêmica emgeral. Em nome dos autores, agradeço pela imagem, partic-ularmente a usada na capa da edição.
Grato.
receivedMarch 24, 2017acceptedMarch 27, 2017published onlineMay 24, 2017
DOI https://doi.org/10.1055/s-0037-1603555.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Letter to the Editor | Carta ao Editor 141

Erratum: Chronic Subdural HematomaSpontaneous Resolution
Errata: Resolução espontânea de hematoma subduralcrônico
Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 George Santos dos Passos1
Luciano José Silveira Filho1 André Luiz Cicilini2 Neiffer Nunes Rabelo3
Luiz Antônio Araujo Dias Junior1 Carlos Umberto Pereira4 Luiz Antônio Araujo Dias5
1Department of Neurosurgery, Hospital Santa Casa, Ribeirão Preto,SP, Brazil
2Medical Student, Universidade de Ribeirão Preto - Unaerp, RibeirãoPreto, SP, Brazil
3Medical Student, Faculdade Atenas, Paracatu, MG, Brazil4Department of Neurosurgery, Fundação Beneficiente Hospital deCirurgia, Aracaju, Sergipe, Brazil
5Neurosurgeon and Professor, Department of Neurosurgery, HospitalSanta Casa, Ribeirão Preto, SP, Brazil
Arq Bras Neurocir 2017;36:142.
Address for correspondence Nicollas Nunes Rabelo, MD, Santa Casade Ribeirão Preto, Ribeirão Preto, São Paulo, Brazil(e-mail: [email protected]).
ERRATUM Rio de Janeiro, May 23, 2017
Dear readers,In the article Chronic Subdural Hematoma Spontaneous Resolution (doi: 10.1055/s-0037-1603512),1 published online in Arq Bras Neurocir in May 2017, where it reads:Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 Luciano José Silveira Filho1 André LuizCicilini2 Neiffer Nunes Rabelo3 Luiz Antônio Araujo Dias Junior1 Carlos Umberto Pereira4
Luiz Antônio Araujo Dias5
It should read:Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 George Santos dos Passos1 LucianoJosé Silveira Filho1 André Luiz Cicilini2 Neiffer Nunes Rabelo3 Luiz Antônio Araujo DiasJunior1 Carlos Umberto Pereira4 Luiz Antônio Araujo Dias5
Prezados leitores,No artigo Chronic Subdural Hematoma Spontaneous Resolution (doi: 10.1055/s-0037-1603512),1 publicado online em Arq Bras Neurocir em maio de 2017, onde se lê:Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 Luciano José Silveira Filho1 André LuizCicilini2 Neiffer Nunes Rabelo3 Luiz Antônio Araujo Dias Junior1 Carlos Umberto Pereira4
Luiz Antônio Araujo Dias5
Lê-se:Nícollas Nunes Rabelo1 Vitor Hugo Honorato Pereira1 George Santos dos Passos1 LucianoJosé Silveira Filho1 André Luiz Cicilini2 Neiffer Nunes Rabelo3 Luiz Antônio Araujo DiasJunior1 Carlos Umberto Pereira4 Luiz Antônio Araujo Dias5
DOI https://doi.org/10.1055/s-0037-1603944.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Erratum142

Instructions to Authors
ISSN 0103-5355
Brazilian Neurosurgery (Arquivos Brasileiros de Neurocirurgia), an official journal of the Brazilian Society of Neurosurgery (Sociedade Brasileira de Neurocirurgia) and Portuguese Language Neurosurgery Society (Sociedades de Neurocirurgia de Língua Portuguesa), aims to publish scientifi c works in Neurosur-gery and related fi elds, unpublished and exclu-sive. The journal publishes papers written in Portuguese with abstracts in English or written in English with Portuguese abstracts.
Submitted articles shall be placed as one of the following categories:
• Original: result of clinical, epidemiological or experimental research. Abstracts of theses and dissertations.
• Review: review and update synthesis of spe-cifi c themes, with critical analysis and con-clusions. Databases and the period range must be specifi ed.
• Case Report: presentation, analysis and discus-sion of cases that present relevant interest.
• Technical Note: note on surgery techniques and/or surgical instruments.
• Miscellaneous: neurosurgery history, pro-fessional practice, medical ethics and other pertinent matters to the journal purpose.
• Letter to the Editor: critics and comments pre-sented in a brief ethical and instructive man-ner about published content in this journal. The copyright is safe to authors of the aimed subject. Letters, when accepted, will be pub-lished with authors reply.
General standards for publishing
• Article fi les for publishing must be submit-ted to the Editor, via http://www.editorial-manager.com/bns/.
• All articles will have a double blinded peer-review process, and no Article Publishing Charge (APC) – society funded. More about Open Access at http://open.thieme.com.
• Only new unpublished manuscripts will be ac-ceptable. Submitted articles must not be fullyor partially submitted to any other journal.
• The editorial board may reject or suggest changes in order to improve the clarity and structure of the text and maintain uniform-ity with the journal policy.
• Copyrights of articles published in the journal will belong exclusively to the Brazilian Neurosurgery and Thieme Publicações Ltda. The reproduction of articles or illustrations without prior consent is prohibited.
Standards for submission
Authors must send the following fi les:
1. Pub Letter (text fi le) stating the article has not yet been published partially or fully or submitted concomitantly to other journal.
2. Manuscript (text fi le).
3. Figures (Tiff , Jpeg, Pdf, Indd) sent in separate fi les with minimum resolution of 300 dpi.
4. Tables, charts and graphics (text fi le) sent separately.
Standards for articles structure
Articles must be structured with all the follow-ing items and paginated accordingly:
1. Title page: article title both in Portuguese and English; full name of all authors; academic or professional affi liation of each author; institutions names where the study took place; running title; corresponding author name, degree, full address, e-mail and phone number; followed by ICMJE CoI forms (http://www.icmje.org/confl icts-of-interest/).
2. Abstract: original articles need structured abstract with 250 words at the most: objec-tive, methods, results and conclusions; review articles, case reports, technical notes and miscellaneous need no structured abstract. Following the abstract comes keywords (six at the most), based on MeSH (Medical Subject Headings), published in Medline and available at: www.ncbi.nlm.nih.gov/mesh/.
3. Portuguese abstract: Portuguese version of title, abstract and keywords based on DeCS (Descritores em Ciências da Saúde, http://decs.bvs.br).
4. Main text: introduction; casuistry or mate-rial and methods; results; discussion; conclu-sion; acknowledgments.
5. References: number references as they are fi rst cited in the text with Arabic numerals. Use Vancouver style; list all authors until the sixth, using et al. after the third when more than six; when reference authors are cited in the text cite the fi rst and et al. for references with more that two authors; unpublished data or personal communication must be cited as such between parentheses and cannot be listed as reference; use journal abbreviation from Index Medicus; use the following examples:
Journal Article
Agner C, Misra M, Dujovny M, Kherli P, Alp MS, Ausman JI. Experiência clínica com oxime-tria cerebral transcraniana. Arq Bras Neurocir 1997;16(1):77–85
Book Chapter
Peerless SJ, Hernesniemi JA, Drake CG. Surgical management of terminal basilar and posterior cerebral artery aneurysms. In: Schmideck HH, Sweet WH, editors. Operative neurosurgical techniques. 3rd ed. Philadelphia: WB Saunders;1995:1071–86.
Book
Melzack R. The puzzle of pain. New York: Basic Books Inc Publishers; 1973.
Theses and dissertations
Pimenta CAM. Aspectos culturais, afetivos e terapêuticos relacionados à dor no câncer. [thesis]. São Paulo: Escola de Enfermagem da Universidade de São Paulo; 1995.
Annals and other congresso publications
Corrêa CF. Tratamento da dor oncológica. In: Corrêa CF, Pimenta CAM, Shibata MK, editores. Arquivos do 7º Congresso Brasileiro e Encontro Internacional sobre Dor; 2005 outubro 19–22; São Paulo, Brasil. São Paulo: Segmento Farma. pp. 110–20.
Available Article in ahead of print
International Committee of Medial Journal Editors. Uniform requirements for manuscripts submitted to biomedical journals. Writing and editing for biomedical publication. Updated October 2007. Available at: http://www.icmje.org. Access in: June 12, 2008.
6. Tables and charts: numbered by Arabic numerals according to its citation in the text; edited in double space, using separate sheets per table/chart; title right above; note, abbreviations, legends must follow right under;introduce only essential tables and charts; files must come separately.
8. Figures: digital formats (Tiff , Jpeg, Pdf, Indd) with minimum resolution of 300 dpi (trim 7.5 or 15 cm).
9. Legends and captions: numbered by Ara-bic numerals according to its citation in the text; edited in double space, using separate fi les; identify eventual labels present in the fi gure (arrows, characters, lines etc.); image previously published must have publisherauthorization and credits.
10. Ethics standards: No data or image identify-ing a patient can be used without formal consent; studies using human beings or animal trials must follow ethical standards from the International Committee of Medical Journals Editors – ICMJE, as well as approval of original institution’s Eth-ics Committee; confl icts of interest must have aICMJE form fi lled in by all authors (http://www.icmje.org/confl icts-of-interest/); commercial marks should be avoided; authors are the sole responsible for opinions and concepts in the published articles, as well as for the reference accuracy.
11. Other information: PDF proof will be sent to corresponding author for eventual queries and/or approval within 72 hours; except measure units, acronyms must be spelled out after its fi rst time mentioned.
Secretariat: R. Abílio Soares, 233/143, Paraíso. 04005-001, São Paulo, SP, Brazil. Phone:(+55 11) 3051-6075.Home page: www.sbn.com.br. e-mail: [email protected]


ADQUIRA JÁ EM http://www.thiemerevinter.com.br
Siga-nos: Facebook/ThiemeRevinter
NEUROLOGIARevisão e Preparação para Concursos e Provas de Título de Especialização – Segunda Edição
Nizar Souayah
496 Páginas – Papel CouchéFormato 21 x 28 cmBrochura – Peso 1.370gRicamente IlustradoISBN: 978-85-372-0617-1Ano de Lançamento: 2015 Especialidade: NeurologiaPreço: R$ 282,99RE1658
MANUAL DE NEUROLOGIADiagnóstico e TratamentoOitava Edição
Martin A. SamuelsAllan H. Ropper
636 Páginas – Papel CouchéFormato 14 x 21 cmBrochura – Peso 855gRicamente Ilustrado ISBN: 978-85-372-0614-0Ano de Lançamento: 2015 Especialidade: NeurologiaPreço: R$ 207,99RE1659
NEUROLOGIA – CURRENT Diagnóstico e TratamentoSegunda Edição
John C. M. Brust
600 Páginas – Papel CouchéFormato 21 x 28 cmBrochura – Peso 1,630gRicamente Ilustrado ISBN: 978-85-372-0631-7Ano de Lançamento: 2016Especialidade: NeurologiaPreço: R$ 259,99RE1701
O melhor conteúdo em Neurologia!