Embed Size (px)
Citation preview

BrazilianNeurosurgery Arquivos Brasileiros de Neurocirurgia
EditorEberval Gadelha Figueiredo
ISSN 0103-5355
Number 2 • Volume 37 • Pages 81–162 • June 2018


Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
ISSN 0103-5355
Editor-in-Chief | Editor-Chefe
Eberval Gadelha Figueiredo
Emeritus Editors | Editores Eméritos
Milton ShibataGilberto Machado de Almeida†
Editorial Board | Conselho EditorialChairman | Presidente
José Marcus RottaManoel Jacobsen Teixeira
National Board | Conselho Nacional
Albedi BastosBelém, PA
Almir F. de AndradeSão Paulo, SP
Arnaldo ArrudaFortaleza, CE
Benedicto Oscar ColliRibeirão Preto, SP
Carlos TellesRio de Janeiro, RJ
Carlos Umberto PereiraAracaju, SE
Eduardo VellutiniSão Paulo, SP
Ernesto CarvalhoPorto, Portugal
Evandro de OliveiraSão Paulo, SP
Fernando Menezes BragaSão Paulo, SP
Francisco Carlos de AndradeSorocaba, SP
Hélio Rubens MachadoRibeirão Preto, SP
Hildo AzevedoRecife, PE
João Cândido AraújoCuritiba, PR
João Paulo FariasLisboa, Portugal
Jorge Luiz KraemerPorto Alegre, RS
José Alberto Gonçalves†
João Pessoa, PBJosé Alberto Landeiro
Rio de Janeiro, RJJosé Carlos Esteves Veiga
São Paulo, SPJosé Carlos Lynch Araújo
Rio de Janeiro, RJJosé Marcus Rotta
São Paulo, SPJosé Perez Rial
São Paulo, SPJose Weber V. de Faria
Uberlândia, MGLuis Alencar Biurrum Borba
Curitiba, PRManoel Jacobsen Teixeira
São Paulo, SPMarco Antonio Zanini
Botucatu, SPMarcos Barbosa
Coimbra, PortugalMarcos Masini
Brasília, DFMário Gilberto Siqueira
São Paulo, SPNelson Pires Ferreira
Porto Alegre, RSÓscar Luis Alves
Porto, PortugalPedro Garcia Lopes
Londrina, PRRicardo Vieira Botelho
São Paulo, SPRoberto Gabarra
Botucatu, SPSebastião Gusmão
Belo Horizonte, MGSérgio Cavalheiro
São Paulo, SPSergio Pinheiro Ottoni
Vitória, ESWaldemar Marques
Lisboa, Portugal
International Board | Conselho Internacional
Albert Sufi anovRussia
André G. MachadoUSA
Antonio de SallesUSA
Beatriz LopesUSA
Clement HamaniUSA
Daniel PrevedelloUSA
Felipe AlbuquerqueUSA
Jorge MuraChile
Kumar KakarlaUSA
Michael LawtonUSA
Nobuo HashimotoJapan
Oliver BozinovSwitzerland
Pablo RubinoArgentina
Paolo CappabiancaItaly
Peter BlackUSA
Peter NakajiUSA
Ricardo HanelUSA
Robert F. SpetzlerUSA
Rungsak SiwanuwatnThailand
Volker SonntagUSA
Yasunori FujimotoJapan

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
Volume 37, Number 2/2018
online www.thieme-connect.com/products
Original Articles | Artigos Originais81 Information Sources and Decision-Making in Neurosurgery: Results of a Survey of Members of the
Brazilian Neurosurgery Society Fontes de informação e tomadas de decisão em neurocirurgia: resultados de uma pesquisa de membros
da Sociedade Brasileira de NeurocirurgiaRodrigo Gorayeb, Maria João Forjaz, Antônio Gonçalves-Ferreira, Joaquim Ferreira
88 Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery: First Cases in Latin America in a Single Reference Center
Indicações de ácido 5-aminolevulínico e ressonância magnética intraoperatória em cirurgia de gliomas: primeiros casos na América Latina em um único centro de referênciaRicardo Ramina, Erasmo Barros da Silva Júnior, Felipe Constanzo, Maurício Coelho Neto
95 The Impact of Lectures (Given to Children from 9–11 Years) on the Recognition of Risk Situations for the Occurrence of Traumatic Brain Injury
O impacto de aulas expositivas (ministradas para crianças de 9 a 11 anos) sobre o reconhecimento de situações de risco para ocorrência de traumatismo crânioencefálicoVictor Frandoloso, Felipe T. da Silva, Camilla Donida Magnabosco
101 Epidemiology Profi le of Traumatic Spine Injury of a Spinal Cord Service in the State of Espírito Santo Avaliação do perfi l epidemiológico do traumatismo raquimedular de um serviço de coluna do estado do
Espírito SantoGabriela Scopel, Charbel Jacob Júnior, Marcus Alexandre Novo Brazolino, Igor Machado Cardoso, José Lucas Batista Júnior, Luciana Carrupt Sogame, Thiago Cardoso Maia, Tadeu Gervazoni Debom
Review Article | Artigo de Revisão105 Immunohistochemical Markers for Schwannomas, Neurofi bromas and Malignant Peripheral Nerve
Sheath Tumors—What Can the Recent Literature Tell Us? Marcadores imuno-histoquímicos para schwannomas, neurofi bromas e tumores malignos da bainha do
nervo periférico—o que a literatura recente pode nos dizer?José Fernando Guedes-Corrêa, Rodrigo Salvador V. Cardoso
Case Reports | Relatos de Caso113 Strictly Intraventricular Craniopharyngioma: Case Report and Literature Review Craniofaringioma puramente intraventricular: relato de caso e revisão da literatura
Marcelo Lemos Vieira da Cunha, Ana Luiza Brunelli Pletz
119 Recurrent Pituicytoma in a Pediatric Patient: A Case Report Pituicitoma recorrente em um paciente pediátrico: relato de caso
Miguel Ángel Maldonado-Morán, Jeisson Ospina, Juan Vega, Claudia Restrepo, Daniela Rico, Camilo Zubieta, Pedro Penagos
123 Hérnia medular idiopática atípica — relato de caso Atypical Idiopathic Spine Cord Herniation (ISCH) — Case Report
Heber Martim Vieira, Rodrigo Amaral, Luis Marchi, Gabriel Pokorny, Fernando Marcelino, Fabio Rosa, Angelo Guarçoni Netto, Nicholai Faulhaber, Rubens Jensen, Luiz Pimenta
Thieme Revinter Publicações Ltda

128 Hypopituitarism Secondary to an Arachnoid Cyst — Case Report Hipopituitarismo secundário a um cisto aracnoide — relato de caso
Eliezer Abreu Cunha, Anderson Rodrigo Souza, Manoel Jacobsen Teixeira, Eberval Gadelha Figueireido
131 Cerebral Proliferative Angiopathy: Case Report Angiopatia cerebral proliferativa: relato de caso
Luana Antunes Maranha Gatto, Rodrigo Tavares Brisson, Zeferino Demartini Jr, Gelson Koppe, Carlos Rocha Jr
134 Neuroparacoccidioidomycosis: Case Report and Literature Review Neuroparacoccidioidomicose: relato de caso e revisão da literatura
Marcus Vinicius de Morais, Sérgio Murilo Georgeto, Marcelo Lourenço Haddad, José Guilherme da Silva Amorim,Luis Guilherme Scaliante, Anderson Luiz de Paula, Igor Vasconcelos de Andrade, Paulo Henrique Pires de Aguiar
140 Intramedullary Dermoid Cyst of the Cervical Spinal Cord – C5–C7 Level Cisto dermoide intermedular da medula espinhal cervical – nível C5–C7
Palanisamy Seerangan, Aravinth Kumar Ashok, Jolarpettai Venugopal Mahendran
145 Meningioma of the Pineal Region — Diff erential Radiologic Aspects of Pineal Region Tumors Based on a Clinical Case
Meningioma da região da pineal – aspectos radiológicos diferenciais dos tumores da região pineal baseado em um caso clinicoTiago Marques Avelar, Aline Lariessy Campos Paiva, Márcio Alexandre Teixeira da Costa, Guilherme Brasileiro de Aguiar, João Luiz Vitorino, José Carlos Esteves Veiga
148 Palsy of the Contralateral Abducens Nerve after Aneurysm Surgery and Temporal Meningioma in the Presence of Petroclival Meningioma: A Case Report
Paresia de nervo abducente contralateral pós-cirurgia de aneurisma e de meningioma temporal em presença de meningioma petroclival: relato de casoPedro Ferreira Paiva Moreira, Anderson Rodrigo Souza, Manoel Jacobsen Teixeira, Eberval Gadelha Figueiredo
151 Schistosomal Cervical Myelopathy Mielopatia esquistossomótica cervical
Ronald Farias, Kléver Forte de Oliveira, George de Albuquerque Cavalcanti Mendes, Ussânio Mororó Meira
Technical Notes | Notas Técnicas154 Surgery of a Posterior Communicating Artery Aneurysm with Fetal-Type Circulation Cirurgia de um aneurisma da artéria comunicante posterior com circulação do tipo fetal
Nicolás González, Manuel Morales, Franco Ravera, Arturo Ruiz-aburto, Juan Vásquez, José Muller, Jhon Mosquera,Rodrigo Zapata
157 Endoscopic Endonasal Odontoidectomy: Nuances of Neurosurgical Technique Odontoidectomia endoscópica endonasal: nuances da técnica cirúrgica
Flavio Ramalho Romero, Rodolfo Brum Vieira, Bruno da Costa Ancheschi
Erratum| Errata162 Erratum - lnformation Sources and Decision-Making in Neurosurgery: Results of a Survey of Members
of the Brazilian Neurosurgery Society Errata - Fontes de informação e tomadas de decisão em neurocirurgia: resultados de uma pesquisa
de membros da Sociedade Brasileira de NeurocirurgiaRodrigo Gorayeb, Maria João Forjaz, Antônio Gonçalves-Ferreira, Joaquim Ferreira
Brazilian Neurosurgery | Arquivos Brasileiros de Neurocirurgia Volume 37, Number 2/2018

Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
Copyright © 2018 by Thieme Revinter Publicações Ltda, Rio de Janeiro, Brazil. Arquivos Brasileiros de Neurocirurgia is published four times a year in March, June, September, and December by Thieme-Revinter Publicações Ltda, Rua do Matoso, 170, Rio de Janeiro, 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.thieme.com/bns.
Arquivos Brasileiros de Neurocirurgia is an official publication of the Brazilian Neurosurgery Society (Sociedade Brasileira de Neurocirurgia) and the Portuguese Language Neurosurgery Societies. It is listed in LILACS and LILACS-Express (Latin-American and Caribbean Center on Health Sciencies Information), and Latindex (Regional Cooperative Online Information System for Scholarly Journals from Latin America, the Caribbean, Spain and Portugal). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0103-5355
The colored content of this issue is available online at www.thieme.com/bns.

Information Sources and Decision-Making inNeurosurgery: Results of a Survey of Membersof the Brazilian Neurosurgery Society
Fontes de informação e tomadas de decisão emneurocirurgia: resultados de uma pesquisa de membrosda Sociedade Brasileira de NeurocirurgiaRodrigo Gorayeb1 Maria João Forjaz2 Antônio Gonçalves-Ferreira3 Joaquim Ferreira4
1Laboratory of Clinical Pharmacology, Faculty of Medicine,Universidade de Lisboa, Lisboa, Portugal
2National School of Public Health, Institute of Health Carlos III andREDISSEC, Biscay, Spain
3Clínica Universitária de Neurocirurgia e Instituto de Anatomia,Faculty of Medicine, Universidade de Lisboa, Lisbon, Portugal
4 Instituto de Medicina Molecular, Lisbon, Portugal; Laboratory ofClinical Pharmacology and Therapeutics, Faculty of Medicine,Universidade of Lisboa, Lisbon, Portugal; Campus NeurológicoSénior, Torres Vedras, Lisbon, Portugal
Arq Bras Neurocir 2018;37:81–87.
Address for correspondence Rodrigo Gorayeb, Faculdade deMedicina, Universidade de Lisboa, Avenida Professor Egas Moniz,1649-028, Lisboa, Portugal (e-mail: [email protected]).
Keywords
► neurosurgery► evidence-based
medicine► source of information► decision-making
Abstract Introduction In all surgical disciplines, including neurosurgery, there are questionsabout the level of evidence supporting surgical practices and the mechanisms andadequacy of knowledge translation.Objectives To assess the perception of Brazilian neurosurgeons of informationsources and decision-making mechanisms related to their medical practices.Methods An online questionnaire was sent to the 2,400 members of the BrazilianNeurosurgical Society.Results A total of 32% of the neurosurgeons completed the questionnaire, 53%hadmorethan 10 years experience, 67% had worked in public hospitals, 34% had performed spinesurgeries, and 30% had performed brain tumor surgeries. The therapeutic decisions werebasedmostly on internship learning (54%) and personal professional experience (52%). Themost common informationsourceswere scientific abstracts (53%)and the Internet (47%). Atotal of 89%believed that evidence-basedmedicinewas relevant, 93%believedprotocols orguidelines were necessary, and 74% subscribed to amedical journal. Nonetheless, only 43%had protocols implemented in their services, 93% highly valued a surgeon’s personalexperience, and63%showed little familiaritywith the interpretationof scientificconcepts inthe literature. Among the respondents, 83% were willing to try an innovative treatmentalternative if it was shown to improve clinical outcomes and reduce severe complications.Conclusions The disparity in the responses highlights the need to implementrecommendations that improve decision-making mechanisms.
receivedMarch 18, 2018acceptedApril 24, 2018published onlineMay 25, 2018
DOI https://doi.org/10.1055/s-0038-1656716.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 81

Introduction
Neurosurgical practices, similarly to the practices of othermedical specialties, depend on the diffusion, acceptance, andestablishment of specific technical procedures and clinicalmanagement protocols. This is undertaken through the genera-tion of scientific data, ideally obtained through randomizedcontrolled trials (RCTs) or, in their absence, based on otherinformation sourceswith thehighest possible level ofevidence.1
Although an increasing number of clinical trials arereported in the scientific literature, there are insufficientquality RCTs in surgical specialties providing a high level ofevidence upon which to base clinical practice. This mayimply that surgeons tend to be conservative regarding theirown practices, only subtly modifying a procedure alreadyperformed with apparent success.2–5
Thus, from a more objective and analytical perspective,there is a great lack of evidence, that is, scientific demon-stration, for many surgical and neurosurgical procedures.Furthermore, in the literature, too many authors, commonprocedures, and personal opinions are published as consti-tuting scientific proof, which is clearly against good scien-tific practice.6 Therefore, the quality of publishedneurosurgical clinical trials is a cause of concern, as arethe difficulties regarding adequate knowledge translation orthe assessment of the scientific of proposed treatments inneurosurgery.7–12
To approach this topic, a survey of surgeons who aremembers of the Brazilian Neurosurgery Society (SBN, inthe Portuguese acronym) was conducted to assess the trans-
mission of scientific knowledge. Therefore, the primaryobjective of this study was to assess the perception of theneurosurgeons of the information sources and decision-making mechanisms related to their own medical practices.The secondary objectives were to characterize the impor-tance given to several sources of knowledge, to identify thewillingness of neurosurgeons to change their current prac-tices and the factors involved in this decision, to characterizetheir perception of scientific trials, and to identify differ-ences in the transmission of neurosurgical knowledge amongthe different groups of neurosurgeons.
Materials and Methods
In September 2015, using a cross-sectional observationaldesign, a questionnairewas sent to the 2,400members of theSBN. The questionnaire was specifically designed for thepresent study and was distributed through SurveyMonkey(SurveyMonkey, San Mateo, CA, US) tool. It contained 15questions divided into 5 sections: characterization of theparticipants; perception of the research in neurosurgery andthe decision-making process; theway knowledge is obtainedand transmitted; how neurosurgeons handle new therapeu-tic alternatives; and analysis of ethical considerations in theconception and implementation of clinical trials. The SBNsent a link to the online survey by email to all its members.Reminder emails were sent 3 times within 15 days. Duringthese twoweeks, a link and a request to fill out the question-naire were also available on the SBN website (see thecomplete questionnaire as supplemental material).
Resumo Introdução Em todas as disciplinas cirúrgicas, incluindo a neurocirurgia, existemquestões sobre o nível de evidência que apoia as práticas cirúrgicas e os mecanismos eadequação da translação do conhecimento.Objetivos Avaliar a percepção de fontes de informação e mecanismos de tomada dedecisão dos neurocirurgiões brasileiros em relação às práticas médicas.Métodos Um questionário on-line foi enviado aos 2.400 membros da SociedadeBrasileira de Neurocirurgia.Resultados Um total de 32% dos neurocirurgiões preencheram o questionário, 53%tinham mais de 10 anos de experiência, 67% trabalharam em hospitais públicos, 34%realizaram cirurgia de coluna, e 30%, de cérebro. As decisões terapêuticas basearam-seprincipalmente no aprendizado de estágio (54%) e na experiência profissional pessoal(52%). As fontes de informação mais comuns foram resumos científicos (53%) e aInternet (47%). Um total de 89% acreditava que a medicina baseada em evidências erarelevante, 93% acreditavam que protocolos ou diretrizes eram necessários, e 74%tinham assinaturas de uma revista médica. No entanto, apenas 43% apresentaramprotocolos implementados em seus serviços, 93% valorizaram a experiência pessoal deum cirurgião, e 63% mostraram pouca familiaridade com a interpretação de conceitoscientíficos na literatura. Entre os respondentes, 83% estavam dispostos a tentar umaalternativa de tratamento inovador se este demonstrasse melhorar os resultadosclínicos e reduzir as complicações graves.Conclusões A disparidade nas respostas destaca a necessidade de implementarrecomendações que melhorem os mecanismos de tomada de decisão.
Palavras-chave
► neurocirurgia► medicina baseada
em evidências► fonte de
informação► tomada de decisões
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al.82

The descriptive analysis of the response frequencies andthe comparison between subgroups of duration and place ofpractice was performed using confidence intervals in com-parative analyses and the Pearson chi-squared test for thecorrelations. For cases with 20% or more of the observationswith a response frequency lower than 5, the Fisher exact testwas used. Statistical analyses were performed using theStatistical Package for the Social Sciences (SPSS, IBM Corp.,Armonk, NY, US). version 20.0.
Responses were collected anonymously, jointly analyzed,andonlycomplete responses foreachquestionwereconsidered.The ethical committee of Faculdade de Medicina de Lisboa andthe board of directors of the SBN were consulted for approvaland saw no objections, and deferred the need for formalinformed consent.
Results
The response rate was 32% (769) of the questionnaires sent.Of these, 87.5% (660) had answers to all 15 questions, and22.5% (109) had partial answers.
More than half of the respondents (53.3%) reported havingover 10 years of clinical practice. Among those with less than10 years of practice, 15.6% were residents, 18.24% had lessthan 5 years of practice, and 12.7%, between 5 and 10 years.
Over 2/3 (67.8%) of the neurosurgeons performed activi-ties in public hospitals, and 37.4% worked exclusively in thepublic sector. Of the total number of surgeons, 30.4% workedequally between public and private practices, and only 13.2%worked exclusively in the private sector.
Themost frequent subspecialties of the respondents werespine (34.1%), followed by brain tumors, 29.3%. Other surgi-cal subdivisions did not present high response rates: vascular(7.8%), pediatrics (5.6%), and functional (3.3%).
Source of Information and Research Perception for theDecision-Making ProcessIn therapeutic decision-making, neurosurgeons reportedvaluing especially the education they had received duringtheir specialty residency (54.3%), as well as their personalprofessional experience (51.9%), while consultation of infor-
mation in the literature, protocols, and academic experienceswere reported by less than 30%. Concerning the sources ofinformation used weekly, 52.7% read scientific articleabstracts; 46.8% consulted information available on theInternet, 46.5% held rounds with colleagues, and 45% con-sulted textbooks (►Table 1).
Regarding the perception of the neurosurgeons of infor-mation related to their clinical practice, 87.9% believedevidence-based medicine (EBM) to be relevant or highlyrelevant, and 93.3% also considered the personal experienceof the surgeon relevant or highly relevant (►Table 2). Of allrespondents, 92.9% believed the implementation of protocolsfor clinical decision-making to be relevant or highly relevant,and 43.1% have protocols implemented in their neurosurgi-cal services. Furthermore, 73.6% of the surgeons subscribedto a medical journal.
Disposition to Change Current Clinical PracticeThe majority (82.6%) of the respondents showed a personalwillingness to modify their current clinical practice if thegoal was the improvement of long-term outcomes (74.7%)and a reduction in severe complications (62.1%). All otherreasons elicited less than 40% of responses. Thosewho statedthat they were “not willing” to change their current practicejustified this answer with the beliefs that there is a lack ofscientific evidence to support new procedures, and that thelearning curve of the use of a new techniquewithwhich theyare not familiar is too steep; both reasons obtained 48.2% ofresponses each.
Table 1 Frequency of consultation of sources of information
Response options Daily Weekly Monthly 1 or 2 times inthe past year
None in thepast year
Reading scientific article abstracts 17.6% 52.7% 23.4% 5.2% 1.1%
Consultation of information available on the web 34.1% 46.7% 15.5% 2.7% 0.9%
Discussions of therapies or management withneurosurgeon colleagues
33.2% 46.5% 12.3% 5.1% 2.0%
Consulting textbooks 19.1% 44.9% 27.1% 7.7% 1.1%
Participation in courses or workshops 1.0% 1.7% 17.4% 69.9% 9.9%
Participation in national symposiums and congresses 1.4% 0.6% 6.5% 78.8% 12.7%
Participation in international congresses 1.0% 0.3% 1.7% 44.5% 52.5%
Note: Lines by decreasing order for weekly responses, p < 0.005
Table 2 Importance of the surgeons’ professional experienceand EBM in neurosurgery
Responseoptions
Relevant Veryrelevant
Littlerelevant
Irrelevant
PersonalExperience
51.0% 42.0% 6.7% 0.0%
EBM 50.0% 37.9% 11.3% 0.8%
Abbreviation: EBM, evidence-based medicine.Note: p � 0.005.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al. 83

Perception of Clinical StudiesWhen requested to identify the most important types ofscientific studies, the respondents mainly valued cohortstudies (63.2%), followed by case-control studies (52.8%),observational studies (49.1%) and clinical trials (43.1%).The following criteria were used to classify scientific articlesas being excellent: levels and degrees of evidence (76.1%),rigorousness of the statistical analysis (56.1%), the existenceof a control group (52.3%), and the names of authors/insti-tutions (37% and 34.1% respectively). The number of authorsdid not influence the attributed value of the article.
Regarding controlled studies, 65.5% perceived that ran-domization improves the quality of controlled trials, and61.1% stated being aware that such studies are not commonin neurosurgery. The respondents reported an intermediatelevel of familiarity with academic concepts (►Table 3), withthe percentage varying between 40.7% and 51% for all con-cepts presented (clinical guidance norms, guidelines, clinicalcases, evidence-based medicine, therapeutic protocols, caseseries, evidence levels, systematic reviews, grades of recom-mendation, meta-analyses).
Comparison of Duration of PracticeWhen comparing groups by duration of clinical experience(� 10 years versus > 10 years), those with up to 10 years ofclinical experience favor EBM, the learning received duringresidency, and consultation of recently published literatureand guidelines, while those with over 10 years of clinicalexperience prefer personal opinions, case discussions withcolleagues, and attendance of international congresses.Therewere no statistical differences in responses by practicelocation (public versus private).
Discussion
Results from this cross-sectional survey indicate that Brazilianneurosurgeons valued especially the education they receivedduring their specialty residencyand their personal profession-
al experience, in detriment of consulting data in the literature,protocols, or academic experiences of others.
Evidence-based medicine was valued in the clinical prac-tice, as was personal clinical experience, and there is awillingness to modify current clinical practices to improvelong-term clinical outcomes and reduce complications. Themore experienced the surgeons, the more likely they were torely on their clinical experience, and the less likely they wereto rely on the scientific literature.5,13
Neurosurgeons inadequately stratified and validated thedifferent typesofclinical studies, althoughthere is apreferencefor scientific articles with high scientific evidence, and ran-domization is considered to improve the quality of controlledstudies.
When subdivided by duration of clinical experience, theyounger neurosurgeons prefer EBM, while their seniorsprefer personal experience. The 32% response rate was quitesuperior to other online medical questionnaires.14,15
The learning resources of the respondents withmore than10 years of clinical practice were mostly based, over theprevious year, on therapeutic conduct discussions withcolleagues, while the younger respondents were more likelyto refer to the published literature. These data corroborateprevious studies that point out that not only does learningundergo a historic evolution of its role and means of acqui-sition, but also that the development of competencies tosearch and use information to produce scientific knowledgemay generate practical changes.16
For those with the most experience, the individual profes-sional experience and the opinion of the colleagues of theneurosurgeon are considered a priority in the neurosurgeon’sday-to-day therapeutic decision-making, while the youngerneurosurgeonsprefer the education receivedduring residency,recently published literature, and guidelines.16 In the neuro-surgical sphere,17 there is a great emphasis and a tendency toprioritize the development of psychomotor faculties thatguarantee adequate performance of surgical techniques, leav-ing the cognitive aspects in the background, such as the
Table 3 Frequency of factors that influence the therapeutic decision-making in neurosurgery
Response options Always oralmost always
Most ofthe times
Somewhatfrequently
Never oralmost never
Education received during the specialty internship 54.3% 33.1% 11.7% 0.8%
Personal professional experience 51.9% 35.9% 11.3% 1.3%
Recent medical literature (published in the previous year) 34.7% 42.1% 20.6% 2.5%
Protocols or international guidelines 34.0% 35.8% 24.2% 6.3%
Medical visits 30.4% 28.5% 26.6% 14.5%
Protocols or guidelines/clinical guidance norms 27.1% 36.3% 28.7% 7.7%
Education received during the medical course 24.9% 24.3% 30.8% 18.0%
Continued education (courses and congresses) 24.0% 33.7% 37.4% 4.8%
Protocols from the place they work 23.6% 31.1% 26.6% 18.7%
Opinions of neurosurgeon colleagues 12.8% 25.5% 57.2% 4.4%
Abbreviation: EBM, evidence-based medicine.Note: Lines in decreasing order for the responses always or almost always; p � 0.05 and confidence interval: 3.5–3.7
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al.84

investment in obtaining scientific knowledge to back up deci-sion-makingwith logical rationales.Nonetheless, an interest inscientific investment to back up the decision-making processand the neurosurgical practice may be considered by someauthors as an ethical professional attitude.18
The concept of EBM was relevant to 87.9% of the respon-dents, while professional experiencewas important to 93.3%.This apparently irreconcilable dichotomy, valuing both pro-fessional experience and EBM, is not foreign to other authors.They perceive that the development of a surgeon as the onewho seeks better evidence for decision-making is long andneeds investment, requiring search in research databasesand libraries with up-to-date material, as well as contactwith centers of excellence and time spent with specialists tomaster the instruments of the evidence-based surgerypractice.16,19,20
Within this context, there is a tendency in the literature toconsider the professional with many years of experience insurgery as scientifically outdated and inclined to makedecisions based on empiricism and the outcomes of theirown practice.20,21
The adoption of EBM includes the potential to improveprofessional qualifications through the development of com-petencies, to contribute to fostering research, and to improvethe use of diagnostic methods and the objectivity of treat-ments. With that, the prognostic perspectives and the lifeexpectancy will likely improve, the cost of treatment may bereduced, and an improvement in the quality of life will ensueas a natural consequence of this process.5,17,19,22–24
Although the introduction of clinical guidelines is positivein the sense of facilitating the review of the vast availableevidence, which the great majority of the respondentsconsider important, the actual transference of this impor-tance to the organization by the implementation of theseguidelines is still not optimal in a significant number ofservices.25,26
The majority of the respondents appear to have enoughknowledge to orient themselves and seek relevant scientificstudies. Nevertheless, they do not seem familiar with theclassic concepts of study subtypes. Additionally, most sur-geons did not have a clear idea of concepts such as theprevalence of controlled studies, the advantage of theirrandom character and of randomization itself, or about thescientific levels of neurosurgery publications. Therefore, therelevance of enhancing scientific knowledgemust be pointedout, especially regarding RCTs, due to their importance.27,28
Some authors have analyzed the difficulties found insurgical clinical research standards, and indicatemany prob-lems in performing RCTs in surgery: the structural, cultural,and psychological resistance to the use of randomization, thevariability inherent to surgery that requires a precise defini-tion of the interventions, a strict monitoring of the quality,the surgery learning curves that pose difficulties to the timeand execution of randomized trials regarding new techni-ques, the comparison of surgical and non-surgical treat-ments, and, lastly, the rare, urgent and life-threateningsituations that result in difficulties in the recruitment,consent and randomization.2,3,6,11,27,29–32
Furthermore, it must be pointed out that the inadequatestratification of research studies by the respondents mustserve as awarning for the need of a greater clarification of thetrue understanding of the neurosurgeons of the differenttypes of studies, especially since theymentioned subscribingto at least one scientific journal.
Within the concepts presented, making better choicesregarding health and healthcare requires the best possibleevidence. Therefore, as rich and different digital data sourcesbecome broadly available for research, analytical tools growin power and sophistication.2,3,18,30,33
Research and health communities now have the opportu-nity to quickly and efficiently generate the scientific evi-dence necessary to support improved decision-making inhealth and healthcare, without reducing the importance ofthe opinions and qualitative information of the specialists asa complementary source of knowledge. Therefore, it isconsidered an opportunity to use qualitative methods tocomplement high quality quantitative data within a morefocused approach.2,3,18,30,33–35
Therefore, surgical research must consider daily clinicalsurgery and surgical translational research issues, introduc-ing new techniques and laboratory results in assisting thepatient, and require clinical surgeons with competency inresearch. Consequently, it is necessary to allocate majorefforts in developing and maintaining high-quality surgicalinvestigations in academic surgical departments, includingindividual career-advisory programs and clinical trial cen-ters aiming at attractive academic positions in surgery, andthe promotion of translational research, as a benefit topatient care.12,36,37
The present study is limited by the fact that only answersfrom a part of the SNB members were analyzed, and the factthat those who answered might belong to subgroups ofmembers who are more motivated or more familiar withwebsite platforms. However, the members of the SBNpresented a questionnaire response rate superior to thatof other similar studies,14,15 and were divided into 2 similargroups with more or less than 10 years of neurosurgicalexperience, with most working in the public service, andmainly performing spine or brain tumor surgeries. Theconcentration of respondents in the early years of theircareer adequately reflects the age distribution of specialistsin a country in which medical education in neurosurgeryhas increasingly progressed over the past 60 years.13 Theconcentration in public hospitals reflects their associationwith treatment resources to treat patients with greatercomplexity, while the preference for spine pathologiesreflects the normal distribution5,9,13,16,18 of neurosurgicalsubspecialties. Nonetheless, it is not impossible that therespondents may overestimate their use of resources inorder to unconsciously provide a positive view ofthemselves.
Although we have included a large sample of the Brazilianneurosurgery field, the extrapolation of the results must beconsidered with caution prior to the comparison of theresults with other national neurosurgeon samples or withother Brazilian surgeons.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al. 85

Conclusion
The members of the SBN who answered the questionnairedid sowith an above-average response rate, with themajori-ty working in public settings, especially performing spine orbrain tumor surgeries. The results differ by duration ofexperience.
The most preferred information sources are weekly readingof scientific articles abstracts, discussing conducts with col-leagues, and consulting textbooks. Here, the older surgeonsprefer therapeutic discussionswith colleagues, and theyoungersurgeons prefer consulting the literature.
The least experienced neurosurgeons privilege the educa-tion received during their medical residency when makingtherapeutic decisions, the recent medical literature and na-tional and international guidelines, while those more experi-encedprefer to relyon their individual professional experience.
Neurosurgeons stated willingness to try innovative treat-ment alternatives, especially when taking into account theimprovement in outcomes and reduction in severe compli-cations. When changing practice was not considered, it wasdue to the lack of scientific evidence or to the risks of usingunfamiliar techniques.
The vast majority of the respondents attributed greatrelevance both to EBM and the personal experience of thesurgeon. They considered neurosurgical protocols as beingvery important, although less than half of the respondentshave protocols in place at their respective hospitals. Theyalso mentioned having little familiarity with the interpre-tation of scientific concepts in the literature, despite iden-tifying articles as being excellent due to their evidence level,highly strict statistical analysis and the existence of acontrol group.
All this demonstrates the need to implement recommen-dations to improve decision-making mechanisms. The SBNor another representing authority could eventually considerundertaking this responsibility.
References1 Lee K. The Philosophical Foundations ofModernMedicine. London:
Polgrave Macmillan; 20122 Ziewacz JE, McGirt MJ, Chewning SJ Jr. Adverse events in neuro-
surgery and their relationship to quality improvement. NeurosurgClin N Am 2015;26(02):157–165, vii
3 Solomon MJ, Laxamana A, Devore L, McLeod RS. Randomizedcontrolled trials in surgery. Surgery 1994;115(06):707–712
4 https://pt.surveymonkey.com/r/Preview/?sm=AZYhti6WuHOf_2FDJxGGyyXFmhOSKoFw2yoZDLJ3mQdUG6S2a_2FbQFn3zo5oLM9RSrz
5 Medeiros LR, Stein A. Medicina baseada em evidências e análise dedecisão na clínica cirúrgica. Revista AMRIGS 2001;45(1,2):45–50
6 Barker FG II. Editorial: Randomized clinical trials and neuro-surgery. J Neurosurg 2016;124(02):552–556, discussion 556–557
7 Weinstein JN, Lurie JD, Olson PR, Bronner KK, Fisher ES, MorganTS. United States’ trends and regional variations in lumbar spinesurgery: 1992-2003. Spine 2006;31(23):2707–2714
8 Agazzi E, Faye J. The Problem of the Unity of Science. London:World Scientific; 2001
9 Dantas AK. Avaliação do aprendizado em técnica cirúrgica empre-gando três estratégias de ensino. [Thesis]. São Paulo: Faculdade deOdontologia da Universidade de São Paulo; 2010
10 Heros RC. Randomized clinical trials. J Neurosurg 2011;114(02):277–278, discussion 278–279
11 Schöller K, Licht S, Tonn JC, Uhl E. Randomized controlled trials inneurosurgery–how good are we? Acta Neurochir (Wien) 2009;151(05):519–527, discussion 527
12 Vranos G, Tatsioni A, Polyzoidis K, Ioannidis JP. Randomized trialsof neurosurgical interventions: a systematic appraisal. Neurosur-gery 2004;55(01):18–25, discussion 25–26
13 Gusmão SS, Souza JG. História da Neurocirurgia no Brasil. SãoPaulo: Sociedade de Neurocirurgia do Brasil; 2008
14 Kongsved SM, Basnov M, Holm-Christensen K, Hjollund NH.Response rate and completeness of questionnaires: a randomizedstudyof Internet versus paper-and-pencil versions. JMed InternetRes 2007;9(03):e25
15 VanGeest JB, Johnson TP, Welch VL. Methodologies for improvingresponse rates in surveys of physicians: a systematic review. EvalHealth Prof 2007;30(04):303–321
16 Gasque KCGD. O papel da experiência na aprendizagem: perspec-tivas na busca e no uso da informação. Transinformacao 2008;20(02):149–158
17 Traynelis VC. The geometry of education: patterns for growth. ClinNeurosurg 2005;52:1–5
18 Isolan GR. A construção do conhecimento pelo jovem neurocir-urgião: ética, ciência e a importância do treinamento em labor-atório de microcirurgia. J Bras Neurocirurg 2009;20(03):314–334
19 Gomes MM. Medicina baseada em evidências: princípios e prá-ticas. Rio de Janeiro: Reichmann & Affonso; 2001:1–13
20 Schanaider A. Cirurgia baseada em evidências: modismo ounecessidade? Acta Cir Bras 2002;17(01):71–74
21 Black N. Evidence-based surgery: A passing fad? World J Surg1999;23(08):789–793
22 Gomes LF. EducaçãoMédica Contínua emMGF. Rev Port Clin Geral2003;19:89
23 O’Brien BJ, Heyland D, Richardson WS, Levine M, Drummond MF.Users’ guides to the medical literature. XIII. How to use an articleon economic analysis of clinical practice. B. What are the resultsand will they help me in caring for my patients? Evidence-BasedMedicine Working Group. JAMA 1997;277(22):1802–1806
24 Sauerland S, Lefering R, Neugebauer EA. The pros and cons ofevidence-based surgery. Langenbecks Arch Surg 1999;384(05):423–431
25 Santos P, Martins C, Sá L, Hespanhol A, Couto L. Motives forrequesting an electrocardiogram in primary health care. CienSaude Colet 2015;20(05):1549–1554
26 Santos P, Nazaré I, Martins C, Sá L, Couto L, Hespanhol A. AsNormas de Orientação Clínica em Portugal e os Valores dosDoentes. Acta Med Port 2015;28(06):754–759
27 Altman DG. Melhor relato de ensaios controlados randomizados:a declaração CONSORT. BMJ 1996;313:570–571
28 Begg C, Cho M, Eastwood S, et al. Melhorar a qualidade danotificação de ensaios controlados aleatórios: a declaração CON-SORT. JAMA 1996;276:637–639
29 Can OS, Yilmaz AA, HasdoganM, et al. Has the quality of abstractsfor randomised controlled trials improved since the release ofConsolidated Standards of Reporting Trial guideline for abstractreporting?A surveyof four high-profile anaesthesia journals. Eur JAnaesthesiol 2011;28(07):485–492
30 Cândido DNC, Barbosa FT. Qualidade dos ensaios clínicos aleatór-ios em Neurocirurgia publicados no Brasil. Arq Bras Neurocir2009;28(02):43–47
31 Mansouri A, Cooper B, Shin SM, Kondziolka D. Randomizedcontrolled trials and neurosurgery: the ideal fit or should alter-native methodologies be considered? J Neurosurg 2016;124(02):558–568
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al.86

32 Ioannidis JP, Haidich AB, PappaM, et al. Comparison of evidence oftreatment effects in randomized and nonrandomized studies.JAMA 2001;286(07):821–830
33 Haines SJ. Randomized clinical trials in neurosurgery. Neurosur-gery 1983;12(03):259–264
34 Califf RM, Robb MA, Bindman AB, et al. Transforming EvidenceGeneration to Support Health and Health Care Decisions. N Engl JMed 2016;375(24):2395–2400
35 Vollmar B. [Research as attractiveness parameter for youngsurgeons]. Chirurg 2012;83(04):319–322
36 Gittes GK. The surgeon-scientist in a newbiomedical research era.Surgery 2006;140(02):123–131
37 Menger MD, Schilling MK, Schäfers HJ, Pohlemann T, LaschkeMW. How to ensure the survival of the surgeon-scientist? TheHomburg Program. Langenbecks Arch Surg 2012;397(04):619–622
Erratum: The article has been corrected as per Erratum published on July 9, 2018. DOI of the Erratum is10.1055/s-0038-1667058.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Information Sources and Decision-Making in Neurosurgery Gorayeb et al. 87

Indications of 5-Aminolevulinic Acid andIntraoperative MRI in Glioma Surgery: FirstCases in Latin America in a Single Reference Center
Indicações de ácido 5-aminolevulínico e ressonância magnéticaintraoperatória em cirurgia de gliomas: primeiros casos naAmérica Latina em um único centro de referência
Ricardo Ramina1 Erasmo Barros da Silva Júnior1 Felipe Constanzo1 Maurício Coelho Neto1
1Department of Neurosurgery, Instituto de Neurologia de Curitiba,Curitiba, PR, Brazil
Arq Bras Neurocir 2018;37:88–94.
Address for correspondence Ricardo Ramina, PhD, Departamento deNeurocirurgia, Instituto de Neurologia de Curitiba, Rua JeremiasMaciel Perretto, 300, Curitiba, PR, Brazil, CEP: 81210310, Brazil(e-mail: [email protected]).
Keywords
► 5-aminolevulinic acid► brain cancer► extent of resection► glioma surgery► intraoperative MRI► glioblastoma
Abstract Introduction The improvement on the extent of resection (EOR) of gliomas with thecombination of 5-aminolevulinic acid (5-ALA) and intraoperative magnetic resonanceimaging (iMRI) has been demonstrated in previous studies. We present our results withthe combined use of 5-ALA and (iMRI) in the surgery of glial lesions.Methods A total of 64 cases of patients with intracranial gliomas who underwentimage-guided surgery using 5-ALA with and without (iMRI) were reviewed. All patientsunderwent an early postoperative MRI to evaluate the EOR. Other intra-operativetechniques (awake surgery, electrophysiological stimulation andmonitoring) were alsoperformed according to the location of the tumor.Results Atotal of 18 tumors didnot show intraoperative5-ALAfluorescence (according tothe World Health Organization [WHO] classification of tumors, 2 WHO-grade I, 14 WHO-grade II, 1 WHO-grade III and 1 WHO-grade IV), and 46 tumors showed intraoperative5-ALA fluorescence (3 WHO-grade II, 3 WHO-grade III, 40 WHO-grade IV). In 28 of the 465-ALA positive cases, a safe 5-ALA free resection was achieved. In the 5-ALA negative cases,the (iMRI) findings guided the EOR, and complete resection was achieved in 11 cases.Complete resection was opted out in gliomas infiltrating eloquent areas.Conclusions The combined use of 5-ALA and IMRI showed improved results in gliomasurgery, offering the safest maximal EOR. In the 5-ALA positive cases (mostly high-grade), fluorescence was a more useful tool. In the 5- ALA negative cases (mostly low-grade), the (iMRI) was decisive to guide the EOR of the tumor.
Resumo Introdução Emestudos anteriores, foi demonstradoumaperfeiçoamentonaextensãodaresecção (EDR) de gliomas com a combinação de ácido 5-aminolevulínico (5-ALA) e aimagem de ressonância magnética intraoperatória (iRM). Nossos resultados são apresen-tados com o uso combinado de 5-ALA e (iRM) para a cirurgia de lesões gliais.
receivedApril 2, 2018acceptedJune 5, 2018
DOI https://doi.org/10.1055/s-0038-1667182.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Original Article | Artigo OriginalTHIEME
88

Introduction
Extent of resection (EOR) is the most important prognosticfactor in glioma surgery,with complete resection of contrast-enhanced areas in high-grade gliomas (HGGs), and fluid-attenuated inversion recovery (FLAIR)/T2-weighted in low-grade gliomas (LGGs), as the primary goal to improve theoutcome of the patient.1–3 Image-guided surgery is decisiveto achieve these benefits, besides being considered a part ofthe standard care for patients with brain lesions.4 Intra-operative imagingmodalities, particularly fluorescence with5-aminolivulinic acid (5-ALA),5,6 seem to improve the EOR,especially in HGGs. Also, the benefits of combining both toolsseem relevant to improve overall survival (OS) and progres-sion-free survival (PFS).5–9
We present the first cohort study of patients who under-went surgeries guided by a combination of 5-ALA andintraoperative magnetic resonance imaging (iMRI) for intra-cranial gliomas in Latin America. The indications, the safetyprofile and the EOR based on preoperative image findingswere reviewed.
Methods
Between November 2015 and January 2018, 64 consecutive5-ALA fluorescence-guided surgeries with or without iMRIwere performed for intracranial gliomas, which were preop-eratively evaluated with magnetic resonance imaging (MRI),perfusionmagnetic resonance (MR), andMR spectroscopy, atInstituto de Neurologia de Curitiba (INC, in the Portugueseacronym), Brazil. In Brazil, 5-ALA as a pure salt is registeredby the National Agency for Sanitary Vigilance (ANVISA, in thePortuguese acronym) under the number CAS 0957, 106–60–5 Brazilian Common Denomination (DCB, in the Portugueseacronym) and is provided by Carbolution Chemicals (St.
Ingbert, Germany). All patients signed an informed consentform, and the studywas approved by the Institutional EthicalReview Board.
Preoperative EvaluationPatients with intracranial masses are routinely evaluatedwith standard MRI as well as with MR perfusion and spec-troscopy. The use ofMR tractography and functionalMRIwasevaluated according to the location of the lesion. Age, sex andfinal histopathological diagnosis were considered for analy-sis. Pre- and postoperative Karnofsky performance scale(KPS) scores and follow-up status were also documentedfor later studies concerning the OS and the PFS.
5-aminolivulinic Acid ProtocolAn oral dose of 20 mg/kg of 5-ALAwas administered 3 hoursbefore surgery, according to standardized protocols.10 Afterthe administration, the patient is guarded from direct lightfor 24 hours to avoid porphyria-like skin reactions. Besidesthis, the preoperative care remained unchanged.
Intraoperative CareIntraoperative image-guidance Brainlab Cranial Navigation(Brainlab® Kick® Purely Navigation, Munich, Germany) wasused in all cases. Electrophysiological stimulation and mon-itoring or awake surgery were performed for tumors ineloquent areas. The Zeiss OPMI PENTERO 800 (Carl Zeiss,Oberkochen, Germany) with a special blue-light filter wasused in all cases.
IntraoperativeMagnetic Resonance Imaging
The iMRI examswere performedwith a General Electric 1.5TSigna Excite MR (General Electric Inc., Boston, MA, US). Theimages were obtained according to the preoperative
Métodos Foram revisados 64 casos de gliomas intracranianos submetidos a cirurgiaguiada por imagem por meio do uso de 5-ALA, com ou sem RMI. Todos os pacientesforam submetidos a ressonância magnética (RM) pré-operatória para a avaliação daEDR do tumor. Outras técnicas intraoperatórias (cirurgia acordado, estimulaçãoeletrofisiológica e monitoração) também foram realizadas segundo a localização dotumor.Resultados Um total de 18 tumores não apresentaram fluorescência com o 5-ALA(segundo a classificação de tumores da OrganizaçãoMundial de Saúde [OMS], 2 com grauOMS I, 14 com grau II, 1 com grau III e 1 com grau IV) e 46 tumores foram fluorescentes(3 comgrau II, 3 comgrau III, 40 comgrau IV). Dos 46 casos positivos para 5-ALA, em28 foiobtida uma ressecção segura e livre. Nos casos negativos para 5-ALA, os achados da (iRM)orientaram a EDR, e alcançou-se ressecção total em 11 casos. A ressecção total foidescartada em gliomas com infiltração em áreas eloquentes.Conclusões O uso combinado de 5-ALA e (iRM) mostrou melhores resultados nacirurgia de gliomas, oferecendo uma EDR de segurança máxima. Nos casos positivospara 5-ALA (a maioria de grau alto), a fluorescência mostrou-se um instrumento maisútil. Nos casos negativos para 5-ALA (a maioria de grau baixo), a RMI foi decisiva paraorientar a EDR tumoral.
Palavras-chave
► ácido 5-aminolevulínico
► câncer de cérebro► extensão da ressecção► cirurgia de glioma► ressonância
magnéticaintraoperatória
► glioblastoma
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al. 89

diagnosis: T1-, T2-, diffusion-weighted and FLAIR images fornon-gadolinium-enhancing lesions (mostly low-gradetumors) and T1-, gadolinium-enhanced T1-, T2-, and diffu-sion-weighted images for gadolinium-enhancing lesions(mostly high-grade tumors).
Classification of 5-aminolivulinic Acid Extentof Resection
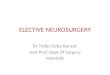
The fluorescence of the lesion was classified as 5-ALA posi-tive (►Fig. 1) or 5-ALA negative. For positive cases, intra-operative tumor resection was classified as ‘5-ALA free’when all fluorescent areas were resected, or ‘residual 5-ALA ’ when residual fluorescent tissue was left to avoidpostoperative deficits. An additional category of ‘5-ALAsuspicious’ was added for the cases in which the colorationat the end of the resection showed a weak fluorescence thatthe surgeon was not able to adequately evaluate as residualor as a mere infiltration of adjacent tissues.
Classification of the Intraoperative MagneticResonance Imaging Extent of Resection
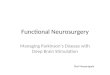
For 5-ALA negative cases, and for some 5-ALA positive orsuspicious cases, an IMRI exam was performed, and theimage findings were classified as complete or partial resec-tion by an experienced team of neuroradiologists (►Fig. 2).
Postoperative CareA complete brain MRI protocol was performed in the first24 hours after surgery.
Results
A total of 62 patients underwent 64 surgeries for intracranialglioma during the period covered by the present study. Thesamplewas composed of 43male and 21 female patients. Themean age was 51.25 years. All patients had a preoperativeKPS > 70% at the time of the procedure. ►Table 1 summa-rizes the 5-ALA and the IMRI EOR results.
Classification Based on 5-aminolivulinic AcidFluorescence
18 of the 64 cases (28.1%) were 5-ALA negative and 46(71.9%) were 5-ALA positive.
5-aminolivulinic Acid Positive Cases and Extent ofResectionOf the 46 cases 5-ALA positive cases, 18 (39.1%) achieved 5-ALA free resection; 18 (39.1%) achieved residual 5-ALA status;and in 10 cases (21.7%), the resection was classified as 5-ALAsuspicious, and the patients underwent a further iMRI examthat confirmed complete tumor removal in all cases.
5-aminolivulinic Acid Negative Cases andExtent of Resection Based on IntraoperativeMagnetic Resonance Imaging
The patients underwent iMRI exams, which showed com-plete resection in 11 (61.1%) cases, and partial resection in7 (38.9%) cases.
There were no complications related to the method in ourseries. The cases of partial tumor resection were due to aninfiltration of eloquent areas.
Histopathological Findings and 5-aminolivulinic AcidFluorescenceOf the 18 5-ALA negative cases, there was 1 case of pilocyticastrocytoma and 1 of angiocentric glioma (both WorldHealth Organization [WHO] grade I), 14 cases of WHO gradeII gliomas, 1 case ofWHO grade III glioma, and 1 case ofWHOgrade IV glioma. Of the 46 5-ALA positive cases, there were 3cases of WHO grade II gliomas, three cases of WHO grade IIIgliomas, and 40 cases of WHO grade IV gliomas. (►Table 2)
Discussion
The goal of surgical resection in brain gliomas is based ontwo principles: maximal tumor resection and functionalpreservation. Gross total resection (GTR) of HGGs andLGGs increases the median survival rate by 200% and 160%respectively, when compared of the survival rates of patientssubjected to subtotal resection (STR).11,12 Gross total resec-tion increases in 61% the likelihood of 1year survival, andincreases in 51% the likelihood of 12-month PFS whencompared with STR in newly-diagnosed glioblastoma.13
Nonetheless, an STR of at least 70% has shown to improvethe OS and seizure control, when seizures are present.11
Intraoperative magnetic resonance imaging emerged inthe 1990s,14–16 and has become an essential tool in gliomasurgery, allowing neurosurgeons to evaluate in real time theEOR and the feasibility of continuing resection without
Fig. 1 Surgery of a high-grade glioma with 5-ALA using white-light microscopy (A) and blue-light filter (B). Note the red fluorescence of thelesion. Arrowheads showing weak pink fluorescence, which is suggestive of infiltration.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al.90

disturbing eloquent areas. This has enabled an EOR of 99.78%in tumors adjacent to eloquent areas,17 but the associatedcosts and logistics required for this procedure has limited itsuse in most centers around the world.18
In 1998, the first series of intracranial tumors operated onwith 5-ALA was reported.19,20 A total of 44 clinical studiesusing 5-ALA for glioma surgery have been published; thesehave demonstrated a GTR of 65% with 5-ALA compared to aGTR of 35% for the group operated onwithout fluorescence.21
In addition, an increase in the PFS of 3.8 months in the 5-ALAgroupwas also achieved.21 Complete resections and improvedPFS were more frequently achieved with 5-ALA when com-pared to white light-only resections, which have a higher riskof early transient neurological deterioration.22,23 For 5-ALAfluorescence and low-field iMRI, class I evidence derived bothfrom randomized and controlled trials has demonstrated an
Fig. 2 Preoperative and intraoperative magnetic resonance imaging (MRI) of a right frontal glioblastoma, showing complete resection of thecontrast-enhancing lesion, which correlated with an intraoperative 5-ALA-free resection.
Table 1 Classification and results of 5-aminolevulinic acidfluorescence
5-ALA status iMRI
EOR Negative: 18 Complete: 11
Partial: 7
Positive: 46 Free: 18 Complete: 7
Partial: 0
Not Performed: 11
Residual: 18 Complete: 0
Partial: 5
Not Performed: 13
Suspicious: 10 Complete: 10
Partial: 0
Abbreviations: 5-ALA, 5-aminolevulinic acid; EOR, extent of resection;iMRI, intraoperative magnetic resonance imaging
Table 2 Histopathological findings and 5-aminolevulinic acid
5-ALA positive 5-ALA negative Total
Grade I 0 2 2
Grade II 3 14 17
Grade III 3 1 4
Grade IV 40 1 41
Abbreviation: 5-ALA, 5-aminolevulinic acid.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al. 91

Table 3 Surgical information of 64 cases
Sex, Age Histopathological diagnosis WHO grade 5-ALA fluorescence 5-ALA EOR IMRI EOR PO MRI EOR
M, 73 Glioblastoma IV Positive Free C C
F, 34 Diffuse astrocytoma II Positive Residual N/P P
F, 70 Glioblastoma IV Positive Suspicious C C
F, 63 Glioblastoma IV Positive Residual N/P P
M, 35 Glioblastoma IV Positive Free C C
M, 31 Glioblastoma IV Positive Residual P P
F, 71 Glioblastoma IV Positive Suspicious C C
M, 74 Glioblastoma IV Positive Residual N/P P
M, 58 Glioblastoma IV Positive Free N/P C
M, 23 Diffuse astrocytoma II Negative N/A C C
M, 17 Pilocytic astrocytoma I Negative N/A C C
F, 26 Diffuse astrocytoma II Negative N/A P P
M, 52 Glioblastoma IV Negative N/A C C
M, 73 Glioblastoma IV Positive Suspicious C C
M, 58 Glioblastoma IV Positive Suspicious C C
M, 69 Diffuse astrocytoma II Positive Free C C
M, 71 Glioblastoma IV Positive Suspicious C C
M, 51 Glioblastoma IV Positive Suspicious C C
M, 60 Glioblastoma IV Positive Residual N/P P
M, 35 Diffuse astrocytoma II Negative N/A P P
F, 56 Anaplastic astrocytoma III Positive Residual N/P P
F, 30 Diffuse astrocytoma II Negative N/A C C
M, 73 Glioblastoma IV Positive Free N/P C
F, 58 Glioblastoma IV Positive Free N/P C
M, 51 Glioblastoma IV Positive Free N/P C
M, 52 Glioblastoma IV Positive Residual N/P P
M, 59 Anaplastic oligodendroglioma III Positive Residual N/P P
M, 57 Glioblastoma IV Positive Residual P P
F, 46 Glioblastoma IV Positive Suspicious C C
M, 52 Glioblastoma IV Positive Residual P P
M, 31 Glioblastoma IV Positive Residual P P
F, 65 Glioblastoma IV Positive Free N/P C
M, 50 Oligodendroglioma II Negative N/A C C
M, 50 Oligodendroglioma II Negative N/A C C
F, 74 Glioblastoma IV Positive Free N/P C
M, 32 Diffuse astrocytoma II Positive Free N/P C
M, 69 Diffuse astrocytoma II Negative N/A P P
M, 45 Glioblastoma IV Positive Free C C
F, 71 Glioblastoma IV Positive Residual N/P P
F, 39 Glioma with astroblastoma-like components
IV Positive Free N/P C
M, 52 Anaplastic astrocytoma III Negative N/A C C
M, 62 Glioblastoma IV Positive Suspicious C C
M, 38 Glioblastoma IV Positive Residual N/P P
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al.92

increase in the EOR.23,24 However, some authors have shownconflicting results. Hauser et al,7 using both iMRI and 5-ALA,found contrast-enhancement after complete resection of fluo-rescent tissue in 91.7%of thepatients, and the use of 5-ALAdidnot improve the OS or the PFS. Tsugu et al5 reported a similarEOR on postoperative 1.5-T MRI between the groups of fluo-rescence only (91.8%) versus fluorescence plus subsequentiMRI (92.6%). Eyüpoglu et al25 reported an improved EOR bycombining 5-ALA and iMRI in malignant gliomas close toeloquent areas, with residual tumors observed on iMRI examsin 32.4% of the patients upon completion of 5-ALA-guidedresection. They proposed that the missing fluorescent areaswere due to layers of overlying, non-fluorescent tissue. Cobur-ger et al26 reported a significant advantage of 5-ALA fluores-cence over iMRI,with higher rates of sensitivity (91% for 5-ALAversus 66% for iMRI) and specificity (80% for 5-ALAversus 60%for iMRI).
In thepresent article, 5-ALAwasused inall cases (►Table 3),but its indication can be based on preoperative MRI (includingadvancedMRI techniques), suggestinganHGG.Tumorswithoutcontrast enhancement and without ‘hot areas’ on MRI perfu-sion, suggesting a low-grade lesion, canbechosen for iMRI only.The results of the 5-ALA response and of the histopathologicalfindings in our series are in line with the literature.
Incases inwhich5-ALAwasnegative, iMRIwas immediatelyused to evaluate the EOR. Moreover, the ‘residual 5-ALA’patients who underwent an iMRI exam had an early corrobo-ration of residual tumor, which was directly related with thenon-resected strong red fluorescent tissue. Zones with weakfluorescence (pink), although representing a tissue-infiltratingtumor, do not necessarily correspond to a residual lesion in theiMRI evaluation. In our series, the choice for iMRI in 5-ALApositive cases was based on the suspicion of these areas.27–30
As discussed before, both methods, 5-ALA and iMRI, can workinsynergyespecially to clarifydubious transoperativefindings.The choice ofoneof themethodsmaybebasedonpreoperativeimagefindings and costs limitations. The OS and the PFS of ourseries will be the subject of a later publication.
Conclusion
In glioma surgery, 5-ALA fluorescence and iMRI are essentialtools for safe tumor removal, increasing GTR and, possibly,resulting in an improvement in the PFS. For 5-ALA positivetumors, mostly HGGs, fluorescence could guide the EOR, andthe iMRI could work in synergy if the neurosurgical teamconsiders it necessary. On the other hand, 5-ALA negativetumors, mostly LGGs, directly benefited from the use of iMRI
Table 3 (Continued)
Sex, Age Histopathological diagnosis WHO grade 5-ALA fluorescence 5-ALA EOR IMRI EOR PO MRI EOR
F, 56 Glioblastoma IV Positive Residual N/P P
M, 32 Diffuse astrocytoma II Negative N/A C C
M, 23 Angiocentric glioma I Negative N/A C C
M, 43 Diffuse astrocytoma II Negative N/A P P
M, 53 Oligodendroglioma II Negative N/A P P
F, 53 Oligodendroglioma II Negative N/A P P
M, 64 Oligodendroglioma II Negative N/A C C
F, 55 Glioblastoma IV Positive Suspicious C C
M, 35 Diffuse astrocytoma II Negative N/A P P
M, 40 Anaplastic oligodendroglioma III Positive Free N/P C
F, 54 Glioblastoma IV Positive Suspicious C C
M, 46 Glioblastoma IV Positive Free C C
M, 51 Glioblastoma IV Positive Residual N/P P
M, 49 Glioblastoma IV Positive Residual N/P P
F, 39 Glioma with astroblastoma-like components
IV Positive Residual N/P P
M, 54 Glioblastoma IV Positive Free C C
M, 75 Glioblastoma IV Positive Free N/P C
F, 29 Diffuse astrocytoma II Negative N/A C C
F, 73 Glioblastoma IV Positive Residual P P
M, 41 Glioblastoma IV Positive Free N/P C
M, 51 Glioblastoma IV Positive Free N/P C
Abbreviations: 5-ALA, 5-aminolevulinic acid; C, complete removal; EOR, extent of resection; F, female; iMRI, intraoperative magnetic resonanceimaging; M,male; iRM, magnetic resonance imaging; N/P, not performed; N/A, not applicable; P, partial removal; PO, postoperative; WHO, WorldHealth Organization.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al. 93

to improve the EOR. Both methods canwork in harmony andwith a safe and practical learning curve for the neurosurgicalteam.
Conflicts of InterestThe authors have no conflicts of interest to disclose.
References1 LacroixM, Abi-Said D, Fourney DR, et al. Amultivariate analysis of
416 patients with glioblastoma multiforme: prognosis, extent ofresection, and survival. J Neurosurg 2001;95(02):190–198. Doi:10.3171/jns.2001.95.2.0190
2 BlochO,HanSJ, ChaS,et al. Impactofextentofresectionfor recurrentglioblastoma on overall survival: clinical article. J Neurosurg 2012;117(06):1032–1038. Doi: 10.3171/2012.9.JNS12504
3 Eseonu CI, ReFaey K, Garcia O, RaghuramanG, Quinones-HinojosaA.Volumetric analysis of extent of resection, survival, and surgicaloutcomes for insular gliomas.WorldNeurosurg 2017;103:265–274.Doi: 10.1016/j.wneu.2017.04.002
4 Barone DG, Lawrie TA, Hart MG. Image guided surgery for theresection of brain tumours. Cochrane Database Syst Rev 2014;(01):CD009685. Doi: 10.1002/14651858.CD009685.pub2
5 TsuguA, IshizakaH,MizokamiY, et al. Impactof thecombinationof5-aminolevulinic acid-induced fluorescence with intraoperative mag-netic resonance imaging-guidedsurgery forglioma.WorldNeurosurg2011;76(1-2):120–127. Doi: 10.1016/j.wneu.2011.02.005
6 Gessler F, Forster MT, Duetzmann S, et al. Combination of Intrao-perative Magnetic Resonance Imaging and Intraoperative Fluor-escence to Enhance the Resection of Contrast Enhancing Gliomas.Neurosurgery 2015;77(01):16–22, discussion 22. Doi: 10.1227/NEU.0000000000000729
7 Hauser SB, Kockro RA, Actor B, Sarnthein J, Bernays RL. Combining5-Aminolevulinic Acid Fluorescence and Intraoperative MagneticResonance Imaging in Glioblastoma Surgery: A Histology-BasedEvaluation. Neurosurgery 2016;78(04):475–483. Doi: 10.1227/NEU.0000000000001035
8 Quick-Weller J, Lescher S, Forster MT, Konczalla J, Seifert V, Senft C.Combination of 5-ALA and iMRI in re-resection of recurrent glio-blastoma. Br J Neurosurg 2016;30(03):313–317. Doi: 10.3109/02688697.2015.1119242
9 Schatlo B, Fandino J, Smoll NR, et al. Outcomes after combined use ofintraoperative MRI and 5-aminolevulinic acid in high-grade gliomasurgery.Neuro-oncol2015;17(12):1560–1567.Doi:10.1093/neuonc/nov049
10 Stummer W, Stepp H, Wiestler OD, Pichlmeier U. Randomized,Prospective Double-Blinded Study Comparing 3 Different Dosesof 5-Aminolevulinic Acid for Fluorescence-Guided Resections ofMalignant Gliomas. Neurosurgery 2017;81(02):230–239. Doi:10.1093/neuros/nyx074
11 Chaichana KL, Jusue-Torres I, Navarro-Ramirez R, et al. Establish-ing percent resection and residual volume thresholds affectingsurvival and recurrence for patients with newly diagnosed intra-cranial glioblastoma. Neuro-oncol 2014;16(01):113–122. Doi:10.1093/neuonc/not137
12 McGirt MJ, Chaichana KL, Gathinji M, et al. Independent associa-tion of extent of resection with survival in patients with malig-nant brain astrocytoma. J Neurosurg 2009;110(01):156–162. Doi:10.3171/2008.4.17536
13 Brown TJ, Brennan MC, Li M, et al. Association of the extent ofresection with survival in glioblastoma: A systematic review andmeta-analysis. JAMA Oncol 2016;2(11):1460–1469. Doi: 10.1001/jamaoncol.2016.1373
14 Alexander E III, Moriarty TM, Kikinis R, Jolesz FA. Innovations inminimalism: intraoperativeMRI. ClinNeurosurg 1996;43:338–352
15 Black PM, Moriarty T, Alexander E III, et al. Development andimplementation of intraoperative magnetic resonance imaging and
its neurosurgical applications. Neurosurgery 1997;41(04):831–842,discussion 842–845. Doi: 10.1097/00006123-199710000-00013
16 Nimsky C, Ganslandt O, Kober H, Buchfelder M, Fahlbusch R.Intraoperative magnetic resonance imaging combinedwith neuro-navigation: a new concept. Neurosurgery 2001;48(05):1082–1089,discussion 1089–1091. Doi: 10.1097/00006123-200105000-0002
17 Reyns N, Leroy HA, Delmaire C, Derre B, Le-Rhun E, Lejeune JP.Intraoperative MRI for the management of brain lesions adjacentto eloquent areas. Neurochirurgie 2017;63(03):181–188. Doi:10.1016/j.neuchi.2016.12.006
18 Ramina R, Coelho Neto M, Giacomelli A, et al. Optimizing costs ofintraoperative magnetic resonance imaging. A series of 29 gliomacases. Acta Neurochir (Wien) 2010;152(01):27–33. Doi: 10.1007/s00701-009-0430-2
19 Stummer W, Stepp H, Möller G, Ehrhardt A, Leonhard M, ReulenHJ. Technical principles for protoporphyrin-IX-fluorescenceguided microsurgical resection of malignant glioma tissue. ActaNeurochir (Wien) 1998;140(10):995–1000
20 Stummer W, Stocker S, Wagner S, et al. Intraoperative detection ofmalignantgliomasby5-aminolevulinicacid-inducedporphyrinfluor-escence. Neurosurgery 1998;42(03):518–525, discussion 525–526
21 Senders JT, Muskens IS, Schnoor R, et al. Agents for fluorescence-guided glioma surgery: a systematic review of preclinical andclinical results. Acta Neurochir (Wien) 2017;159(01):151–167.Doi: 10.1007/s00701-016-3028-5
22 StummerW, Tonn JC,MehdornHM, et al; ALA-Glioma StudyGroup.Counterbalancing risks and gains from extended resections inmalignant glioma surgery: a supplemental analysis from the ran-domized 5-aminolevulinic acid glioma resection study. Clinicalarticle. J Neurosurg 2011;114(03):613–623. Doi: 10.3171/2010.3.JNS097
23 StummerW, Pichlmeier U, Meinel T,Wiestler OD, Zanella F, ReulenHJ; ALA-Glioma Study Group. Fluorescence-guided surgerywith 5-aminolevulinic acid for resection of malignant glioma: a rando-mised controlled multicentre phase III trial. Lancet Oncol 2006;7(05):392–401
24 Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Intraopera-tive MRI guidance and extent of resection in glioma surgery: arandomised, controlled trial. Lancet Oncol 2011;12(11):997-–1003. Doi: 10.1016/S1470-2045(11)70196-6
25 Eyüpoglu IY, Hore N, Savaskan NE, et al. Improving the extent ofmalignant glioma resection by dual intraoperative visualizationapproach. PLoS One 2012;7(09):e44885. Doi: 10.1371/journal.pone.0044885
26 Coburger J, Engelke J, Scheuerle A, et al. Tumor detection with 5-aminolevulinic acid fluorescence and Gd-DTPA-enhanced intrao-perative MRI at the border of contrast-enhancing lesions: aprospective study based on histopathological assessment. Neu-rosurg Focus 2014;36(02):E3. Doi: 10.3171/2013.11.FOCUS13463
27 Stummer W, Novotny A, Stepp H, Goetz C, Bise K, Reulen HJ.Fluorescence-guided resection of glioblastoma multiforme byusing 5-aminolevulinic acid-induced porphyrins: a prospectivestudy in 52 consecutive patients. J Neurosurg 2000;93(06):1003–1013. Doi: 10.3171/jns.2000.93.6.1003
28 Panciani PP, FontanellaM, Schatlo B, et al. Fluorescence and imageguided resection in high grade glioma. Clin Neurol Neurosurg2012;114(01):37–41. Doi: 10.1016/j.clineuro.2011.09.001
29 Díez Valle R, Tejada Solis S, Idoate Gastearena MA, García de EulateR, Domínguez Echávarri P, Aristu Mendiroz J. Surgery guided by 5-aminolevulinicfluorescence inglioblastoma: volumetric analysisofextent of resection in single-center experience. J Neurooncol 2011;102(01):105–113. Doi: 10.1007/s11060-010-0296-4
30 Roberts DW, Valdés PA, Harris BT, et al. Coregistered fluorescence-enhanced tumor resection of malignant glioma: relationshipsbetween δ-aminolevulinic acid-induced protoporphyrin IX fluores-cence, magnetic resonance imaging enhancement, and neuropatho-logical parameters. Clinical article. J Neurosurg 2011;114(03):595–603. Doi: 10.3171/2010.2.JNS091322
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Indications of 5-Aminolevulinic Acid and Intraoperative MRI in Glioma Surgery Ramina et al.94

The Impact of Lectures (Given to Children from9–11 Years) on the Recognition of Risk Situationsfor the Occurrence of Traumatic Brain Injury
O impacto de aulas expositivas (ministradas para crianças de9 a 11 anos) sobre o reconhecimento de situações de risco paraocorrência de traumatismo crânioencefálico
Victor Frandoloso1 Felipe T. da Silva1 Camilla Donida Magnabosco1
1Universidade do Planalto Catarinense, Lages, SC, Brazil
Arq Bras Neurocir 2018;37:95–100.
Address for correspondence Victor Frandoloso, Medical Student, RuaFernando Ataíde, 811, Bairro Sagrado Coração de Jesus, CEP: 88508-120, Lages, SC, Brazil (e-mail: [email protected]).
Keywords
► trauma► accidents► prevention
Abstract Introduction It is believed that the prevention of head trauma (TBI) can be achievedwith campaigns to raise awareness about safety measures.Methods Longitudinal, observational and analytical cohort study. Standardizedquestionnaires were administered to students from 4th to 6th grade elementaryschool, before and immediately after the intervention. Items on habits//exposure toTCEs were analyzed categorically as theoretical knowledge were evaluated semi-continuously. A randomly selected subgroup was subjected to the same questionnairespast 9 months of educational lectures.Results A total of 117 students (55 girls) were interviewed initially (4th [n¼ 14/117],5th [n¼ 54/117] and 6th [n¼ 49/117] series, average age of 9.8, 10, 7 and 11.8 years).Of these, 22 students were submitted to the late posttest (7th grade, 12.7 years onaverage). Among the participants, 37% (43/116) students had already suffered/knewsomeone who suffered TBI, 58% (18/31) were involved in traffic accidents and 42% (13/31) were involved in accidents with bicycle, skates or skateboard. Among thesesubjects, 90.3% reported occasional use or never having used protection duringplay. A significant discrepancy was detected between safety habits and theoreticalknowledge related to helmet use and the use of seat belts (effective use versus hits onknowledge of respectively 37% versus 61%, and 70% versus 92%). In the theoreticalevaluation, improvement was observed only with regard to the importance of helmetusage (61% in the pretest, 72% in the immediate posttest and 95% in the late posttest).Conclusion The high rate of experience with TBI coupled with the significantdiscrepancy between habits and knowledge regarding trauma prevention stress theneed for effective measures leading to their actual implementation. The interventionincreased awareness about the importance of helmet usage, suggesting partialeffectivity from a theoretical standpoint.
receivedJuly 24, 2015acceptedOctober 21, 2015published onlineFebruary 4, 2016
DOI https://doi.org/10.1055/s-0038-1666877.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 95

Introduction
The aim of trauma prevention programs is to provide atransformation in the knowledge, attitude and behavior ofa previously identified segment of society. Offering informa-tion to potential victims is not enough to prevent trauma. Aprogram must be implemented to influence the attitude ofsociety, and more importantly, change its behavior.1–3
Trauma is now one of the main causes of child morbidityand mortality in developed countries and also in Brazil,where it already has a prominent place in statistics.4 Thebest way to fight the disease, the trauma and its consequen-ces is through accident prevention. Although falls are almostimpossible to be prevented, there are practical and basicnorms that are universally useful. On the other hand, theincidence of other accidents, such as slab falls, washing tanksyndrome and traffic accidents can be minimized throughawareness campaigns organized by specialty societies andperformed jointly with the public authorities.4,5
Several attempts have failed to pursue the ideal teachingmethodology for an accident prevention program that actu-ally causes changes in behavior. The literature shows that it ischallenging to find the reasonswhy it is so difficult to changeyoung people’s attitudes toward injury prevention.
Based on these premises and adapting to the Americaneducational model Think First, which aims to avoid injuries tothe brain, spinal cord and other traumatic injuries, the Socie-
dade Brasileira deNeurocirurgia (Brazilian Society of Neurosur-gery, SBN, in the Portuguese acronym) started in 1995 theeducational projectPenseBem (“ThinkWell”) for thepreventionof traumatic brain injury (TBI). The project aims to expandknowledge in the area of primary prevention of TBI and reducethe severity of traumas, especially among children aged 10 to14 years in elementary/middle school. To this end, videos, CDs,stickers,bannersandeducationalbrochureshavebeencreated.6
The SBN’s Pense Bem project addresses the importance ofpreventing brain injury. The goal is to raise awareness amongstudents (aged between 9 and 11 years) regarding the identifi-cation of risk situations for the occurrence of TBI. The applica-tion of a standardized questionnaire (research instrument)aims to estimate the impact of this educational interventionimmediately after its application and in the medium term. Byusing these data, it will be possible to approach the schoolenvironment inpublic institutionsof themunicipalityof Lages,SC, to evaluate the understanding of children between 9 and11 years old regarding risk situations for the occurrence of TBI.
Material and Methods
Observational, analytical and longitudinal study, analyzing acohort initially sampled for convenience. Sampling for thelate posttest was performed using a randomly selectedsubgroup of the initial cohort.
Resumo Introdução Acredita-se que a prevenção de traumatismo cranioencefálico (TCE)possa ser alcançada com campanhas de conscientização sobre medidas de segurança.Métodos Estudo de coorte, longitudinal, observacional e analítico. Questionáriospadronizados foram aplicados a estudantes da quarta a sexta série do primeiro grau,antes e imediatamente após a intervenção. Itens sobre hábitos e/ou exposição a TCEforam analisados categoricamente, enquanto conhecimentos teóricos foram avaliadossemicontinuamente. Um subgrupo escolhido aleatoriamente foi submetido aos mes-mos questionários depois de 9 meses das palestras educacionais.Resultados Um total de 117 alunos (55 meninas) foram entrevistados inicialmente(4ª [n ¼ 14/117], 5ª [n ¼ 54/117] e 6ª [n ¼ 49/117] séries, commédia de idades de 9,8;10,7; e 11,8 anos, respectivamente). Destes, 22 alunos foram submetidos ao pós-testetardio (7ª série, 12,7 anos em média). Dos alunos que responderam ao questionário,37% (43/116) já tinham sofrido e/ou conheciam alguém que sofreu TCE; 58% (18/31) seenvolveram em acidentes de trânsito; e 42% (13/31) em acidentes com bicicleta, patinsou skate. Destes, 90,3% fizeram uso eventual ou nunca fizeram uso de proteção duranteatividades lúdicas. Foi detectada discrepância significativa entre hábitos de segurança econhecimento teórico referente ao uso de capacete e cinto de segurança (uso efetivoversus acertos sobre conhecimento de, respectivamente, 37% versus 61% e 70% versus92%). Na avaliação teórica, houve melhora significativa apenas no quesito sobre aimportância do uso de capacete (61% no pré-teste, 72% no pós-teste imediato e 95% nopós-teste tardio).Conclusão A alta taxa de experiências com TCE somada à significativa discrepânciaentre hábitos e conhecimentos para evitar traumas salienta a necessidade de imple-mentação de medidas efetivas. A intervenção permitiu aumentar a percepção sobre aimportância do uso de capacete, sugerindo efetividade do ponto de vista teórico.
Palavras-chave
► trauma► acidentes► prevenção
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
The Impact of Lectures (Given to Children from 9–11 Years) Frandoloso et al.96

The educational intervention was performed togetherwith the project “Pense Bem: Prevention of Traumatic BrainInjury in Children.” The classes were performed following astandard protocol, once in each class, lasting 10minutes. Thestandardized questionnaire was applied at two moments toall enrolled students: pretest and immediate posttest (that is,shortly after the intervention). Subsequently, one class wasrandomly selected for the late posttest (that is, 9 monthspostintervention) (►Fig. 1).
A statistical analysis for comparing the correctness ratesbetween pre and posttest, as well as the composition of thegroups in terms of gender, was performed by applying theKappa test for paired samples. The comparison betweenthe results of the immediate and late posttestswas performedwith theFisher exact test for independent samples. The level ofsignificance was preestablished at 0.05. The analyzes wereperformedusing theBioEstat 5.3 software (Instituto deDesen-volvimento Sustentável Mamirauá, Tefé, AM, Brazil).
Results
Inall, 117studentsansweredthepretest;55ofwhomweregirls.Students of the 4th, 5th and 6th grades of elementary/middle
school (mean age of 9.8, 10.7 and 11.8 years, respectively) wereinterviewed. Regarding the distribution, the subjects werepredominantly in the 6th (n ¼ 49/117) and 5th grades (n ¼54/117), and fewer in the 4th grade (n ¼ 14/117) (►Table 1).
Among the students, 37% (43/116) had already sufferedor knew someone who had suffered some type of TBI. Ofthese, 58% (18/31)were involved in traffic accidents; and 42%(13/31) in bicycle accidents, skating or skateboarding. Sixcases were reported to have suffered falls, two suffered TBIfrom soccer, two from hammer strikes, two from stonestrikes and two from fights (►Table 2).
In the late posttest, applied 9 months later to a randomsample (for convenience) obtained from the initial sample,studentsanswered thequestions correctly, as seen in►Table 3.
Among the items investigating theoretical knowledge,scores close to 90–100% were observed in questions 1 to 3(see attached questionnaire). On the other hand, the itemreferring to the use of helmet (4) showed an improvement inthe score, both between pretest and immediate posttest, aswell as between immediate and late posttests (►Table 3).
Regarding the change in habits between pretest and lateposttest, an increase in the percentage of students reportingseat belt use was observed. The other habits did not show a
School:______________________________________Grade:____________ Date of Birth:________________ Gender: M ( ) F ( )
1) Do you ride a bike, skate or skateboard?YES ( ) NO ( )
2) If yes, do you wear any protective gear (helmet, knee pads, elbow pads) when riding?ALWAYS ( ) SOMETIMES ( ) NEVER ( )
3) Do you usually ride in a car?YES ( ) NO ( )
4) When you ride in a car, how often do you wear a seat belt?ALWAYS ( ) SOMETIMES ( ) NEVER ( )
5) Have you ever ridden with drivers who had consumed alcohol?ALWAYS ( ) SOMETIMES ( ) NEVER ( )
6) Have you, a family member or anyone you know ever had a head injury (head banging followed by vomiting, fainting, or severe pain)?YES ( ) NO ( )
7) Did you or the person see a doctor?YES ( ) NO ( )How was you/the person injured?a) Diving.b) Traffic accident.c) Bicycle/skating/skateboarding accident.d) Other. Which? __________________________________________________________
Fig. 1 Questionnaire applied.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
The Impact of Lectures (Given to Children from 9–11 Years) Frandoloso et al. 97

significant increase in the effective implementation of secu-rity measures. Nevertheless, there is a tendency, albeitspurious, for an increase in the use of personal protectiveequipment (PPE) and a reduction in drivers under the influ-ence of alcohol (►Table 4).
Discussion
The extension project “Pense Bem: Prevention of TraumaticBrain Injury in Children”was applied to children from fourthto sixth grades. Like other trauma prevention programs, itaims to provide a transformation in the knowledge, attitudeand behavior of a previously identified segment of society.Simply offering information to potential victims is notenough to prevent trauma. A programmust be implementedto influence the attitude of society and, more importantly, tochange its behavior.1
Salvarani2 conducted an intervention program based onthe Pense Bem project in Maringá, Paraná, Brazil. The pro-gram sought the participation of public agencies and privateinstitutions to establish a network of information facilitatorsand multipliers, and to reduce the absolute number andseverity of TBI in the municipality. For this, educationalhandouts were distributed, and lectures and videos werepresented. After the intervention was completed, the resultsdid not indicate an absolute decrease in the number of trafficaccidents and victims. The impact of the program wasverified by the reduction of the trauma severity in thesevictims. Besides the decrease inmortality in 27.2%, therewasa decrease in the severity of trauma in general, and in thenumber of cases and severity of TBI.
Falavigna et al7,8 performed two interventional studiesbased on the Pense Bem project in Caxias do Sul, Rio Grandedo Sul, Brazil. In 2012, their randomized study used 1,049high school students, with application of pretest, immediateand short-term posttests. The attitude toward injury preven-tion did not show any change in the population. In 2014, theresearchers opted for a randomized, eight-step study usingeducational interventions from different society groups andtargeting fifth graders and sophomores in public and privateschools. Their work did not modify most of the attitudestoward injury prevention.
Table 1 Population characteristics
School Grade Age Gender
Male Female
CAIC NSP 4th (14 students) 9.8 years 5 9
CAIC NSP 5th (29 students) 10.7 years 18 11
CAIC NSP 6th (32 students) 11.5 years 14 18
CAIC ID 5th (25 students) 10.7 years 13 12
CAIC ID 6th (17 students) 12.1 years 12 5
Total 117 students 10.9 years 62 55
Abbreviations: CAIC ID, Centro de Atenção Integral à Criança e aoAdolescente Irmã Dulce (Center for Integral Attention to Children andAdolescents Sister Dulce); CAIC NSP, Centro de Atenção Integral àCriança e ao Adolescente Nossa Senhora dos Prazeres (Center forIntegral Attention to Children and Adolescents Nossa Senhora dosPrazeres).
Table 2 Previous experiences with traumatic brain injury
TBIa Medicalassistanceb
How was theperson injured?
Yes 37% 89%
No 63% 11%
Diving 0%
Traffic accidents 58%
Cycling, skating orskateboardingaccidents
42%
Other. Which? Fall, soccer,hammer, stone,fight.
Abbreviations: TBI, traumatic brain injury.Notes: aHave you, a family member or anyone you know ever had a headinjury (head banging followed by vomiting, fainting, or severe pain)?bDid you or the person see a doctor? (Pretest questionnaire, Annex B).
Table 3 Distribution of responses in the immediate and lateposttests according to each alternative
Correct responses Pretest Immediateposttest
Lateposttest
Traffic—automobile(seat belt use)
93.2% 93% 100%
Traffic—pedestrians(using crosswalk)
88% 89% 100%
Domestic(oven, stairs or couch)
89% 91% 95%
Sports(helmet use)
�61% 72%#�95%#
Notes: � p < 0.05; � Kappa test; # Fisher exact test.
Table 4 Habits of the participants in terms of use of safetyequipment
Habits Preintervention Postintervention
Leisure activities(cycling, skating,or skateboarding)
76% (89/117) 79% (19/24)
Use of personalprotective equipment
37% (39/106) 47% (9/19)
Use of automobile 91% (106/117) 96% (23/24)
Seat belt use 70% (81/117) 91%� (22/24)
Driving under theinfluence of alcohol
11% (13/117) 4% (1/24)
Note: � p < 0.05, Kappa test for independent samples.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
The Impact of Lectures (Given to Children from 9–11 Years) Frandoloso et al.98

Neither Falavigna et al7,8 nor Salvarani2 obtained theexpected results in their studies. These authors pointed outthat it is a challenge to find out why it is so difficult to changeyoung people’s attitudes toward injury prevention. On theother hand, the questionnaire employed, as well as the educa-tional interventions, were performed in a complex way. Forexample, the questionnaire contained questions about neuro-anatomy, an unnecessary knowledge in the prevention of TBI.
This study investigated the degree of change in the patternof responses to standardized questionnaire (pretest, immedi-ate and late posttests). The questionnaire (in the annex) wasformulated in simple language,with easy theoretical questionsand answer options, short and compatible with the compre-hension of students in the researched age group. Questionsabout habits, however, were formulated differently. Thoseincluded categorical and closed answers, to conceal the possi-ble connection between habits and theoretical knowledge.This measure was taken to exclude the eventual possibility ofstudents trying to “guess” the answers in the two differentsegments of the questionnaire. Likewise, habits were ques-tioned9monthsapart andwithoutprior notice, soas to reducethe memory bias. Following this method, an improvement inthe number of correct answers for question 4 of the segment(use of helmet) on theoretical knowledge was observed. Thescores rose from 61 to 72% and finally reached 93% in thepretest, immediate and late posttests, respectively. On theother hand, questions 1 to 3 showed high rates of rightanswers, very close to 100%. This homogeneous and correctpattern suggests that the previous measures seem obvious.
In relation to the comparison between security measuresand theoretical knowledge, a disconnection of extremeimportance was observed. When asked about their habits,90% of students did not wear any protection on a regularbasis. This finding supports the theory that the students didnot realize the connection between the portions of theoryand the habits of the questionnaire. In addition, the increasein theoretical correctness rates suggests an effectiveness ofthe intervention inmaking students aware of the importanceof using helmets.
Activities with potential risk of progressing to TBI wereconsidered in the study. Leisure activities (cycling, skating,skateboarding), as well as the use ofmotor vehicles, canmoreeasily result in TBI in cases of disobedience of safety stand-ards. The degree of exposure to risk in leisure and locomotionactivities were respectively 76 and 91%. Thus, a high degreeof vulnerability was observed in the studied population.
Silveira9 tried to know needs of the TBI children care and,using an integrative review, found predominance of pre-school and school-age male victims, automobile accidents,and falls (including leisure activities). Considering that 90%of the children reported engaging in activities withoutprotective measures (helmet), intervention in this aspectsounds promising, especially because it is a cost-effectivemeasure. In comparison, 57% of respondents used cars insituations of potential risk, reinforcing the need to supple-ment knowledge in both areas, perhaps with more emphasison leisure activities. That is partially due to the passiveness ofstudents, being passengers in those situations. Thus, the
most appropriate targets for campaigns in the case of auto-mobiles would be adults. Since the child, when playing, isoften themain actor (often in the absence of adults), it crucialto emphasize the safety aspects of helmet use.
When identifying the main external causes among chil-dren under 15 in outpatient and inpatient settings and death,Martins and Andrade10 established that head and neckcorrespond to the most affected regions of the body.
Among general injuries, TBI corresponded to 34.7% ofemergency room visits, 37.4% of hospitalizations and 50%of deaths.
In our study, another interesting finding relates to theexperiences of TBI respondents. Of the 37% who respondedpositively to this question, 58% reported an automobile acci-dent (versus 42% with bicycles). In addition, 89% of those whoreported TBI needed medical care, pointing to the severity ofthese events. Considering that adults should be thoroughlyoriented about the use of the seat belt and the non-use ofalcohol at the wheel, we can make a reciprocal consideration,that is, children could act as vectors for changing attitudeswithin the family. The use of helmets and the care taken at thewheel were therefore equally important in terms of damages.
Nevertheless, there was an improvement only regardingseat belt use. However, some improvement, although notsignificant, could be observed in the indicators referring toother safety habits. Therefore, future studies may betterelucidate ways to effectively change habits for TBI prevention.
The present study also presents limitations. The initiallystipulated sample size, as well as the sampling strategy couldnot be met. This happened due to abnormal weather con-ditions (hail) that affected the normal activities of publicschools during the periodwhen the lectureswere to be givenand data were to be collected. Thus, sampling was notrepresentative of the students’ population of themunicipali-ty of Lages as a whole, affecting the generalization of theresults (external validity of the study). In addition, the powerof applied statistical tests (and therefore the chance ofincurring type one error) were compromised. Although thechoice of the subgroup undergoing the late posttest wasinitially random, it can be ascertained that the group hadmore mature students than the sample submitted to theinitial phase of the study (chance of incurring type 2 error).In addition, the time elapsed between the initial interventionand the delayed intervention may have led, per se, to animprovement in the rate of correctness, since the studentsmatured during this period. This may affect the internalvalidity of the results, since it generates selection bias,limiting the power of the applied statistical test.
Nevertheless, within the limitations listed here, all possi-ble efforts were made to comply with the protocol initiallyproposed.
Conclusion
The high rate of experienceswith TBI added to the significantdiscrepancy between habits and knowledge to avoid trauma,emphasizing the need to implement effective measures forits prevention. The intervention allowed to increase the
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
The Impact of Lectures (Given to Children from 9–11 Years) Frandoloso et al. 99

perception about the importance of the use of helmet,suggesting effectiveness from the theoretical point of view.The present study presents important limitations imposedby logistical issues. Nevertheless, all possible measures weretaken to get close to the originally proposed protocol.
Final NotesThis study was supported by the Brazilian National Coun-cil for Scientific and Technological Development (CNPq, inthe Portuguese acronym), within the framework of theInstitutional Scholarship Program of Scientific Initiation(Programa Institucional de Bolsas de Iniciação CientíficaPIBIC, in the Portuguese acronym) 2014/2015.
AcknowledgmentsTo the Secretary of Education of theMunicipality of Lages,Marimília Casa Costa Coelho. To the Academics and Pro-fessors of theMedicine School of Universidade do PlanaltoCatarinense, participants of the Extension Project PenseBem and to Sociedade Brasileira de Neurocirurgia (Brazi-lian Society of Neurosurgery).
References1 NAEMT. Atendimento pré-hospitalar ao traumatizado - PHTLS;
[translated by Renata Scavone et al.] 7.ed. Rio de janeiro: Elsevier;2011
2 Salvarani CP. Impacto de um projeto de intervenção de acidentesde trânsito em um município no interior do Brasil [thesis].Faculdade de Medicina de Ribeirão Preto/USP, 2006
3 Greene A, Barnett P, Crossen J, Sexton G, Ruzicka P, Neuwelt E.Evaluation of the THINK FIRST For KIDS injury prevention curri-culum for primary students. Inj Prev 2002;8(03):257–258
4 Lopez FA, Júnior DC. Tratado de pediatria: sociedade brasileira depediatria. 2.ed. Barueri, SP: Manole; 2012
5 Farage L, Colares VS, Capp NetoM,MoraesMC, BarbosaMC, BrancoJdeA Jr. As medidas de segurança no trânsito e a morbimortalidadeintra-hospitalar por traumatismo craniencefálico no Distrito Fed-eral. Rev Assoc Med Bras (1992) 2002;48(02):163–166
6 Brasileira de Neurocirurgia S. (SBN). See: http://www.sbn.com.br/index/institucional/pense-bem Last access: 26 de abr. 2014
7 Falavigna A, Teles AR, Velho MC, et al. Impact of an injuryprevention program on teenagers’ knowledge and attitudes:results of the Pense Bem-Caxias do Sul Project. J NeurosurgPediatr 2012;9(05):562–568
8 Falavigna A, Medeiros GS, Canabarro CT, et al. How can we teachthem about neurotrauma prevention? Prospective and rando-mized “Pense Bem-Caxias do Sul” study with multiple interven-tions in preteens and adolescents. J Neurosurg Pediatr 2014;14(01):94–100
9 Silveira AG. Trauma cranioencefálico na criança: uma revisãointegrativa. Trabalho de conclusão de curso da escola de enfer-magem da Universidade federal do Rio Grande do Sul, PortoAlegre, 2013
10 Martins CBG, Andrade SM. Causas externas entre menores de 15anos em cidade do sul do Brasil: atendimentos em pronto-socorro,internações e óbitos. Rev Bras Epidemiol 2005;8(02):194–204
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
The Impact of Lectures (Given to Children from 9–11 Years) Frandoloso et al.100

Epidemiology Profile of Traumatic Spine Injury of aSpinal Cord Service in the State of Espírito Santo
Avaliação do perfil epidemiológico do traumatismoraquimedular de um serviço de coluna do estado doEspírito Santo
Gabriela Scopel1 Charbel Jacob Júnior2 Marcus Alexandre Novo Brazolino2 Igor Machado Cardoso2
José Lucas Batista Júnior2 Luciana Carrupt Sogame1 Thiago Cardoso Maia2 Tadeu Gervazoni Debom2
1Department of Orthopedy, Santa Casa de Misericórdia, Vitória,ES, Brazil
2Department of Spinal Cord Surgery, Santa Casa de Misericórdia,Vitória, ES, Brazil
Arq Bras Neurocir 2018;37:101–104.
Address for correspondence Charbel Jacob Junior, MD,Departamento de Cirurgia da Coluna, Hospital Santa Casa deMisericórdia de Vitória, Rua Doutor João Santos Neves, 143, VilaRubim, Vitória, ES, Brazil, CEP: 29025-023(e-mail: [email protected]).
Keywords
► epidemiology► spinal cord injuries
Abstract Objective To analyze the epidemiological profile of patients with traumatic spinalcord injury (SCI) undergoing surgical procedures in the state of Espírito Santo, Brazil.Methods A cross-sectional, descriptive study was performed based on the analysis of70medical records of patients who underwent surgery due to traumatic SCI in the stateof Espírito Santo, Brazil.Results Males comprised 79% of the patients. The average age of the occurrence ofthe traumatic SCI was 44 years; automobile accidents were the main cause of trauma(44%). Half of the patients had lesions in the cervical region, and 46% were classified asFrankel A, according to the Frankel scale. In the first 60 days after surgery, the maincomplication presented by the patients was urinary tract infection (UTI). Half of thepatients were from the metropolitan area.Conclusion Patients undergoing surgery for traumatic SCI in the state of Espírito Santoare predominantly men, with a mean age of 44 years, with cervical spine injury due to caraccidents, from the metropolitan area, and whose main complication was UTI.
Resumo Objetivo Analisar o perfil epidemiológico dos pacientes com traumatismo raquime-dular (TRM) submetidos a procedimentos cirúrgicos no estado do Espírito Santo, Brasil.Métodos Foi realizado um estudo transversal e descritivo, baseado na análise de 70prontuários de pacientes submetidos a procedimento cirúrgico em decorrência de TRMno estado do Espírito Santo, Brasil.Resultados Um total de 79% dos pacientes era do sexo masculino. A média de idadefoi de 44 anos, sendo acidente automobilístico a causa principal de trauma (44%).Metade dos pacientes apresentou lesão em região cervical, e 46% foram classificados
receivedSeptember 25, 2015acceptedNovember 23, 2015published onlineJanuary 22, 2016
DOI https://doi.org/10.1055/s-0038-1666876.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 101

Introduction
Traumatic spinal cord injuries (SCIs) comprise spinal injuriesin any part of the spinal column that contains the spinalcord.1 They may result in motor, sensory, sphincter andautonomic dysfunction below the level of the lesion. Theevaluation of neurological lesions is established by theFrankel scale, and they are graded as complete lesion, incom-plete lesion and normal function.2 The severity of the lesionis classified as complete or incomplete according to thenorms established by the American Spinal Cord InjuryAssociation (ASIA), the complete lesion corresponding tothe total absence of motor and sensory functions belowthe level of the lesion.3
The complications of SCIs include pulmonary complica-tions, spasms, pain and urinary tract infections (UTIs),among others. The most common cause of death in thesepatients is pneumonia.4,5 Several studies indicate that UTI isthe most common complication, followed by pain andspasms.3 The prevalence of pain after a SCI varies consider-ably, and is seen in about one-half to two-thirds of thepatients.5
There is no official notification of SCI cases. However, it isestimated that the annual incidence is 21 patients permillion inhabitants.6 In developing countries, the incidenceis 25.5 cases per million every year.7 Men are most affect-ed,7,8 corresponding to 82.8% of all cases. The average age is32.4 years in developing countries.7 Since SCIs affect mostlyyoung and economically active people, they end up inter-rupting the individual’s professional activity at the peak ofthe potential for economic gain, generating a high cost tosociety.7,9
The two main causes of SCIs pointed out in internationalstudies are automobile accidents and falls (41.4% and 34.9%respectively), followed by violence and sports accidents.7,10
National studies diverge from classic statistics, having gun-shot wounds in second place among the causes of SCIs,followed by falls and cold steel wounds.9
The adequate time for surgical intervention after a SCIremains controversial. Several studies did not show a clearimprovement in the neurological prognosis; however, there isevidence of clinical safety in early surgical intervention.11–14
Brazil’s currently available epidemiological data are rela-tively scarce and conflicting with the literature.9,15 There-fore, we have proposed to evaluate the epidemiologicalprofile of patients with SCIs submitted to a surgical proce-dure in the state of Espírito Santo.
Materials and Methods
A cross-sectional, descriptive study was performed based onthe analysis of 70 records of patients submitted to a surgicalprocedure due to SCIs in the state of Espírito Santo fromFebruary 2011 to February 2015.
The selected patients were admitted to several private andpublichospitals in thestateofEspíritoSanto, andwere referredby the central regulation of beds or by spontaneous demand.The following variables were analyzed: age, gender, patientorigin, fracture level, neurological level, trauma mechanismand complications in the first 60 days after surgery.
Data were collected and distributed in projections usingthe Microsoft Excel (Microsoft Corporation, Redmond, WA,US) software to evaluate the distribution of each analyzedpiece of data. The percentiles and absolute numbers ofaffection of each analyzed event were considered.
Results
A total of 70 records were analyzed, and 79% of themcorresponded to male patients (n ¼ 55). The mean age was44 years, ranging from 14 to 75 years. Young people (20–24years old) constituted 32% of the cases, followed by adults(31–59 years old; 28%); young adults (25–30 years old; 20%);adolescents (10–19 years old; 12%); and the elderly (over60 years old; 8%) (►Table 1).
Among the trauma mechanisms, automobile accidentsrepresented 44% of the total, followed by gunshot wounds(GSWs), which corresponded to 27% of the cases. Falls anddives occupied the third and fourth places respectively(►Table 2). Half of the patients in the sample presentedlesions in the cervical region, and 26%, in the thoracolumbarregion. The thoracic segment was the third most affected
como Frankel A, de acordo com a escala Frankel. Nos primeiros 60 dias após a cirurgia, aprincipal complicação apresentada pelos pacientes foi infecção do trato urinário (ITU).Metade dos pacientes era proveniente da região metropolitana do estado.Conclusão Os pacientes submetidos a procedimento cirúrgico por TRM no estado doEspírito Santo são predominantemente homens, com idade média de 44 anos, lesão dacoluna cervical por acidente automobilístico, e provenientes da região metropolitana.A principal complicação apresentada foi ITU.
Palavras Chave
► epidemiologia► traumatismo
raquimedular
Table 1 Sample distribution by age
Age (years) Classification (BrazilianMinistry of Health)
%
10–19� Adolescent 12
20–24� Young 32
25–30� Young adult 20
31–59� Adult 28
� 60� Elder 08
Note: �Standard deviation.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Epidemiology Profile of Traumatic Scopel et al.102

site, and the lumbar segment was affected in only 4% of thecases (►Table 3).
According to the Frankel scale, 46% of the patients wereclassified as Frankel A. Frankel C was the second mostfrequent classification, with 19 cases, followed by FrankelE, B and D, with 9, 8 and 2 cases respectively (►Table 4).
During the first 60 days after surgery, the patients werechecked for the presence of complications. Out of the 70patients, 36 had complications during this period. The mostfrequent was UTI, with 18 cases, followed by the presence ofpressure ulcer, which occurred in 10 cases. A total of 4patients developed pneumonia, and 1 had cardiac compli-cations. During the first 2 months after surgery, 3 patientshad an association of UTI and eschar (►Table 5).
As to the origin, 35 patients came from the metropolitanregion of the state capital of Vitória. The others came from thecentral region (18 patients), the southern region (4 patients)and the northern region (7 patients) of the State of EspíritoSanto. A total of 6 patients came from other states (►Table 6).
Discussion
Spinal cord injury is a disease that presents a devastatingpotential not only for patients and families, but also for theeconomy, since it involves a huge financial health cost.15
An adequate analysis of the distribution and prevalence ofSCIs is of paramount importance for the planning anddevelopment of strategies to approach polytrauma and forthe implementation of measures to increase populationawareness.
In the present study, there was a predominance of malepatients (79%), which in line with the data from the litera-ture.7–9,15,16 The mean age of the most affected patients indeveloping countries is 32.4 years old, according to a study byRahimi-Movaghar et al.7 The average age found in thepresent study, was higher: 44 years old. However, consider-ing the classification of the Brazilian Ministry of Health, bothaverages place these patients within the age group of adults(31–59 years old).
Fractures occurred mostly at the cervical level (50%),which similar to in the findings of national and internationalstudies.8,9,17 About 4.5% of the patients in one study hadmore than one fracture at different medullar levels.18 There-fore, due to the high frequency of cervical fractures and theirgreat impact on the neurological status and the quality of lifeof the patients, protection of the cervical spine in the initialcare becomes essential.
Regarding the severity of the neurological deficit, themajority of patients (46%) were classified as Frankel A, dueto the absence of any motor or sensory function belowthe lesion. This neurological picture was also observed innational studies.15
Table 2 Sample distribution by injury mechanism
Injury mechanism Total of patients (70) %
Gunshot wound 19 27
Automobile accident 31 44
Fall 15 22
Diving 5 7
Table 3 Sample distribution by injury level
Injury level Total of patients (70) %
Cervical 35 50
Thoracic 14 20
Thoracolumbar� 19 26
Lumbar 2 4
Note: �Transition region between the thoracic and lumbar regions(fractures of D11 to L1).
Table 4 Classification of spinal cord injuries according to theFrankel scale
Frankel Total of patients (70) %
A 32 46
B 8 11
C 19 27
D 2 3
E 9 13
Table 5 Sample distribution of clinical complications withinthe first 60 days after surgery
Clinical complications until60 days postsurgery
Total of patients (70)
UTI 18
Pressure ulcer 10
Pneumonia 4
Cardiac 1
UTI and eschar 3
Abbreviation: UTI, urinary tract infection.
Table 6 Distribution of the sample according to the origin ofthe patient with spinal cord injury
Patient origin Total ofpatients (70)
%
Metropolitan area of thecapital city of Vitória
35 50
Central region of theState of Espírito Santo
18 25
Southern region of theState of Espírito Santo
4 5
Northern region of theState of Espírito Santo
7 11
Other states 6 9
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Epidemiology Profile of Traumatic Scopel et al. 103

The two main causes of SCIs in the present study (auto-mobile accidents and gunshot wounds) are similar to thosefound in the epidemiological analysis of national data.9
However, this result differs from the international figures,in which falls appear as the second main cause of SCIs.7,10 Indeveloped countries, the proportion of trauma by automo-bile accident is stable, with a tendency to decrease, which isjustified in part by the better infrastructure and greatersafety provided by their automotive vehicles.19
Among the complications, UTI was the most frequent,present in 26% of the cases with complications, a resultsimilar to those reported in several international studies.3
Pagliacci et al20 suggest that 53.7% of SCI patients presentedurologic complications in the first 6 months posttrauma.
The origin of the patients was evaluated according to themacro-regional division of the state of Espírito Santo,21 withthe majority of patients submitted to surgery for traumaticSCI (75%) coming from themetropolitan region of the capitalcity of Vitória and the central region of the state of EspíritoSanto (►Table 6). The southern region of the state had lessreferrals, probably due to the proximity to the city of Rio deJaneiro. A total of 9% of the patients came from another state(southern region of the state of Bahia), since the closestreference center for these patients is located in Vitória.
Conclusion
The patients submitted to a surgical procedure for SCI in thestate of Espírito Santo are predominantly men, with a meanage of 44 years, cervical spine injury due to automobileaccidents, classified as Frankel A, and originally from themetropolitan regionof the city of Vitória. The main compli-cation presented was UTI.
Conflicts of InterestThe authors declare that there are no conflicts of interestin the present work.
References1 Silveira PR. Trauma raquimedular: diagnóstico e tratamento nas
emergências. Rev Bras Med 2000;78:17–372 Frankel HL, Hancock DO, Hyslop G, et al. The value of postural
reduction in the initial management of closed injuries of the spinewith paraplegia and tetraplegia. I. Paraplegia 1969;7(03):179–192
3 Yang R, Guo L, Wang P, et al. Epidemiology of spinal cord injuriesand risk factors for complete injuries in Guangdong, China: aretrospective study. PLoS One 2014;9(01):e84733
4 Sousa EPD, Araujo OF, Sousa CLM, Muniz MV, Oliveira IR, NetoNGF. Principais complicações do Traumatismo Raquimedular nospacientes internados na unidade de neurocirurgia do Hospital deBase doDistrito Federal. Com. Ciênc Saúde (Porto Alegre) 2013;24(04):321–330
5 Pereira CU, Carvalho LFP, Santos EAS. Complicações clínicas dotraumatismo raquimedular: pulmonares, cardiovasculares, genitur-inárias e gastrointestinais. Arq Bras Neurocir 2010;29(03):110–117
6 Botelho RV, Albuquerque LDG, Junior RB, Júnio AA. Epidemiologyof traumatic spinal injuries in Brazil: systematic review. Arq BrasNeurocir 2014;33(02):100–106
7 Rahimi-Movaghar V, Sayyah MK, Akbari H, et al. Epidemiology oftraumatic spinal cord injury in developing countries: a systematicreview. Neuroepidemiology 2013;41(02):65–85
8 Stephan K, Huber S, Häberle S, et al; TraumaRegister DGU. Spinalcord injury–incidence, prognosis, and outcome: an analysis of theTraumaRegister DGU. Spine J 2015;15(09):1994–2001
9 Pereira CU, Jesus RM. Epidemiologia do Traumatismo Raquimed-ular. J Bras Neurocirurg 2011;22(02):26–31
10 Hagen EM, Rekand T, Gilhus NE, Grønning M. Traumatic spinalcord injuries–incidence, mechanisms and course. Tidsskr NorLaegeforen 2012;132(07):831–837
11 Cadotte DW, Fehlings MG. Spinal cord injury: a systematic reviewof current treatment options. Clin Orthop Relat Res 2011;469(03):732–741
12 Albert TJ, Kim DH. Timing of surgical stabilization after cervicaland thoracic trauma. Invited submission from the Joint SectionMeeting on Disorders of the Spine and Peripheral Nerves,March 2004. J Neurosurg Spine 2005;3(03):182–190
13 Vaccaro AR, Daugherty RJ, Sheehan TP, et al. Neurologic outcomeof early versus late surgery for cervical spinal cord injury. Spine1997;22(22):2609–2613
14 Rutges JP, Oner FC, Leenen LP. Timing of thoracic and lumbarfracture fixation in spinal injuries: a systematic review of neu-rological and clinical outcome. Eur Spine J 2007;16(05):579–587
15 Júnior MFS, Bastos BPR, Jallageas DN, Medeiros AAA. Perfilepidemiológico de 80 pacientes com traumatismo raquimedular,internados no Hospital do Pronto-Socorro Municipal de Belém,PA, no período de janeiro a setembro de 2002. J Bras Neurocirurg2002;13(03):92–98
16 Rahimi-Movaghar V, Saadat S, Rasouli MR, et al. Prevalence ofspinal cord injury in Tehran, Iran. J Spinal CordMed 2009;32(04):428–431
17 Pickett GE, Campos-BenitezM, Keller JL, Duggal N. Epidemiology oftraumatic spinal cord injury inCanada. Spine2006;31(07):799–805
18 Calenoff L, Chessare JW, Rogers LF, Toerge J, Rosen JS. Multiplelevel spinal injuries: importance of early recognition. AJR Am JRoentgenol 1978;130(04):665–669
19 Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map fortraumatic spinal cord injury epidemiology: update 2011, globalincidence rate. Spinal Cord 2014;52(02):110–116
20 Pagliacci MC, Franceschini M, Di Clemente B, Agosti M, Spizzi-chino L; GISEM. A multicentre follow-up of clinical aspects oftraumatic spinal cord injury. Spinal Cord 2007;45(06):404–410
21 www.es.gov.br/Banco%20de%20Documentos/mapas/Divisao-Regio-nal_Macrorregioes.jpg
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Epidemiology Profile of Traumatic Scopel et al.104

Immunohistochemical Markers for Schwannomas,Neurofibromas andMalignant Peripheral Nerve SheathTumors—What Can the Recent Literature Tell Us?
Marcadores imuno-histoquímicos para schwannomas,neurofibromas e tumores malignos da bainha do nervoperiférico—o que a literatura recente pode nos dizer?
José Fernando Guedes-Corrêa1 Rodrigo Salvador V. Cardoso1
1 Division of Neurosurgery, Hospital Universitário Gaffrée e Guinle,Rio de Janeiro, RJ, Brazil
Arq Bras Neurocir 2018;37:105–112.
Address for correspondence Rodrigo Salvador Cardoso, ClinicalFellow, Divisão de Neurocirurgia, Hospital Universitário Gaffrée eGuinle, Rua Jardim Botânico, 700, Sala 407, Jardim Botânico, Rio deJaneiro, RJ, 22461-000, Brazil (e-mail: [email protected]).
Keywords
► immuno-histochemistry
► biomarker► nerve sheath
neoplasm(s)► schwannoma► neurofibroma► malignant peripheral
nerve sheath tumor
Abstract Introduction Schwannomas and neurofibromas are the two most common benignneoplasms of the peripheral nerve sheath, and although they are generally easy todistinguish, in some cases, they can closely resemble one another. Furthermore,malignant peripheral nerve sheath tumors (MPNSTs), another example of peripheralnerve sheath neoplasm, may likewise constitute, due to their morphology and lack ofspecific immunohistochemical markers, a challenging diagnostic.Objective To bring attention to new and promising biomarkers for schwannomas,neurofibromas and MPNSTs and to outline, based on the recent literature, aimmunohistochemical profile for each neoplasm at hand, as well as to emphasizethe need for further studies that could help us understand their diagnostic potentialand disrupt our dependence of limited and nonspecific biomarkers.Methods An overview of the recent literature published in English on both theclassical promising immunohistochemical markers of schwannomas, neurofibromasand MPNSTs was performed. We discarded case reports.Conclusions There is still a lack of specific biomarkers for peripheral nerve tumors.However, plenty of new immunohistochemical markers have been coming to lightwith presumed higher specificity andmore diverse helpful uses than the classical ones.For example, Sox10 is a good biomarker for differentiating schwannomas andneurofibromas from sarcomas, calretinin schwannomas from neurofibromas, TLE1and HMGA2 MPNSTs from sarcomas, and nestin, EGFR, p16 and Ki-67 MPNSTs fromdifferent types of schwannomas and neurofibromas. There is still need for furtherstudies; however, the potential of some of these promising markers, among others,should not be disregarded.
receivedMarch 29, 2018acceptedJune 5, 2018
DOI https://doi.org/10.1055/s-0038-1667180.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Review Article | Artigo de Revisão 105

Introduction
Schwannoma and neurofibroma are the two most frequentbenign tumors that arise from the peripheral nerves.1
Schwannomas are benign neoplasms usually encapsulat-ed and composed exclusively of immature Schwann cells thatarise from the peripheral nerve sheath,2 whereas neuro-fibromas, the most frequent benign tumors in neurofibro-matosis type 1 (NF1), contain, besides malignant peripheralnerve sheath tumor (MPNST), proliferating Schwann cellsand other local supporting elements of the nerve fibers,including perineurial cells, fibroblasts, axons, blood vesselsand infiltration of mast cells.1,3,4
Although these tumors are generally easy to distinguishby standard light microscopy, in some cases, they mightclosely resemble one another.1
On the other hand,MPNSTs aremalignant neoplasmswithnerve sheath differentiation that originate from the periph-eral nerve sheath or the adjacent extraneural soft tissue. Dueto their morphologic heterogeneity and lack of specificimmunohistochemical or molecular criteria, the diagnosisof MPNST is often challenging, including various sarcomasand benign peripheral nerve sheath tumors, such as cellularschwannoma or atypical/cellular neurofibroma.1,4–7
Besides the well-sedimented lack of specific markers forperipheral nerve sheath tumors,4,6–9 they also share somebiomarkers,whichmakesthediagnosisevenharder.1Thus, it isnecessary to outline the antigen patterns for each in order toreduce the risk formisdiagnosis,10when themicroscopy is notenough. This process must be followed not only for schwan-nomas, neurofibromas and MPNSTs, but also between each ofthese three and their related possible differential diagnoses.
Immunohistochemistry is an ordinary tool in the diagnosisof soft tissue tumors. It is a valuable resource when a carefulassessment of histopathology and formulation of differentialdiagnosis are inconclusive and there still are differential diag-nostic possibilities. Conversely, the use of diagnostic immuno-histochemistry regardlessof thehistologicalcontext frequentlyresults in serious errors and is strongly discouraged.11
Schwannomas, neurofibromas andMPNSTs are soft tissuetumors and often have histopathological differential diagno-sis with other soft tissue tumors,6,11 with which they sharemultispecific markers and antigenic complexities of manytumor types11 and hence, there is a need of new and specificbiomarkers for these cases.
In this review we will briefly expose the common expectedhistology of the schwannoma, neurofibroma and MPNST, aswell as their variants, followedbythemaindifferentialdiagnosis
Resumo Introdução Schwannomas e neurofibromas são as duas neoplasias benignas maiscomuns a acometer o tecido nervoso periférico, e apesar de geralmente seremfacilmente distinguíveis, em alguns casos, elas podem ser muito semelhantes. Alémdisso, os tumores malignos da bainha dos nervos periféricos (TMBNPs), outro exemplode neoplasia da bainha do nervo periférico, podem damesma forma constituir, pela suamorfologia e falta de marcadores imuno-histoquímicos específicos, um diagnósticodesafiador.Objetivo Chamar a atenção para novos e promissores biomarcadores para schwan-nomas, neurofibromas e TMBNPs e delinear, a partir da literatura atual, um perfilimuno-histoquímico para cada neoplasia em questão, além de enfatizar a necessidadede futuros estudos que possam elucidar-nos acerca de seu potencial diagnóstico e, porventura, romper nossa dependência de biomarcadores inespecíficos e limitados.Método Foi feita uma revisão da literatura recente incluindo artigos em língua inglesasobre os marcadores imunohistoquímicos clássicos e os promissores para schwanno-mas, neurofibromas e TMBNPs. Descartamos relatos de caso.Conclusão Ainda há uma falta de biomarcadores específicos para as neoplasias acima.Contudo, vários novos marcadores imuno-histoquímicos têm surgido, e com futurosestudos poderemos talvez definir biomarcadores específicos e indispensáveis para oscasos desafiadores de neurofibromas, schwannomas e TMBNPs. Por exemplo, o Sox10 éum bom biomarcador para diferenciar schwannomas e neurofibromas de sarcomas; acalretinina é um bom marcador para diferenciar schwannomas de neurofibromas; osbiomarcadores TLE1 e HMGA2 podem ajudar a diferenciar TMBNPs de sarcomas, e anestina, o receptor do fator de crescimento epidérmico (EGFR), o gene p16 e a proteínaKi-67 podemdiferenciar TMBNPs de diferentes tipos de schwannomas e neurofibromas.Ainda há necessidade de novos estudos; contudo, o potencial de alguns dessesmarcadores, dentre outros, não deveria ser negligenciado.
Palavras-chave
► imuno-histoquímica► biomarcador► tumor(es) do
sistema nervosoperiférico
► schwannoma► neurofibroma► tumor maligno da
bainha do nervo
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso106

in each situation. Then, a discussion about the well-establishedand recent promising markers will be built to set a layout(►Table 1) of alternative and more embracing immunohis-tochemistry to avoid misdiagnosis and draft more preciselytherapeutic schemes and prognosis.
Method
This article aims to outline updated useful biomarkers for themost common benign peripheral nerve tumors, schwannomaand neurofibroma,1 aswell as forMPNSTs. For such, we lookedup through the Google Scholar and the PubMed Central (PMC)research platforms for articles published in English during thelatter 15 years. We resorted to the Boolean Operators, always
using the terms Schwannoma, Neurofibroma, Malignant Pe-ripheral Nerve Sheath Tumor orMPNSTwith thewordsMarker,Biomarker, Immunohistochemistry or immunohistochemical, aswell as sorted the results by relevance. Thearticleswhichbringwell consolidated biomarkers in the literature, recent alterna-tive biomarkers with good results so far, or useful discussionabout thepathologyof thestudied tumorswerecontemplated.Case reports were discarded. In the end, 25 articles publishedin the last 15 years were selected.
Discussion
Schwannoma (►Figs. 1 and 2)Schwannomas are benign neoplasms that arise from theSchwann cells of the peripheral nerve sheath. They are wellcircumscribed masses with a variable admixture of compactspindle-cell areas with nuclear palisading and Verocay bodies(Antoni A), and reticular paucicellular areas (Antoni B).1,6,12
Neurofibromatosis type 2 (NF2) and schwannomatosis aregenetically distinct disorders that are related to predispositionof developing nerve sheath tumors, mainly schwannomas.8
Table 1 Useful immunophenotypic features in the differentialdiagnosis of schwannoma, neurofibromaandmalignant peripheralnerve sheath tumor
IHC Marker Schwannoma Neurofibroma MPNST
S100 þþþ þþ þ/þþþ (only inthe epithelioidMPNST)
CD34 þþþ(AntoniA areas)
þþþ þ/þþ
Sox10 þþþ þþþ þ/þþEMA þ 0/þ 0 (except for
MPNST withperineurialdifferentiation)
Calretinin þþþ þGFAP þ þ þNSE
Leu7 0/þ 0/þGAP43 0/þ 0/þRTK/AXL
TLE1 þþþ þ/þþ þ/þþPodoplanin þþ
(Antoni A)0 (except foratypical)
þ/þþ
CD56/PGP9.5 þþ þþ þþNestin 0/þ þþ þþHMGA2 þ/þþEGFR 0 þ/þþp16 þ/þþ 0/þ 0/þNeurofibromin 0 (except for a
few low-gradecases of MPNST)
Ki-67 þ/þþ þþ/þþþP57NTR þ þþSox2 þþ þþ
Abbreviations: þ, weak expression of the marker; þþ, moderateexpression of the marker; þþþ, strong expression of the marker;0, no expression of the marker; Blank space, no informationcontemplated by this review of the marker; EGFR, epidermal growthfactor receptor; EMA, epithelial membrane antigen; GAP43, growthassociated protein 43; GFAP, glial fibrillary acidic protein; HMGA2 highmobility group AT-hook 2; IHC, NSE, neuron-specific enolase; MPNST,malignant peripheral nerve sheath tumor; RTK, receptor tyrosinekinases; TLE1, transducin-like enhancer of split 1.
Fig. 2 Intraoperative photograph of the left fibular nerve afterresection. Same patient of ►Fig. 1.
Fig. 1 Intraoperative photograph of a schwannoma of the left fibularnerve before resection. The patient is a 42-year-old non-neurofibro-matosis male.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso 107

In the NF2 syndrome (1:33.000), there are alterations inthe NF2 gene coding for theMerlin tumor suppressor proteinthat cause all tumors in the syndrome.2,8,13 Neurofibroma-tosis type 2 patients mainly suffer from bilateral vestibularschwannomas, meningiomas, gliomas and peripheralschwannomas.8,14
Schwannomas rarely suffer malignant degeneration andwhen they do, they turn into epithelioidMPNSTs, which havea strong diffuse expression of S100.4,6
On the other hand, in the schwannomatosis, (recentlylinked tomutations in the SMARCB1 tumor suppressor gene)schwannomas are the only tumor entity observed.8
Cellular schwannoma is a variant of schwannoma com-posed basically of compact, fascicular growth pattern, pro-liferating Schwan cells with variable hyperchromasia andpleomorphism and absence of Verocay bodies.5,6,12 Becauseof its high cellularity, fascicular growth proliferation andincreased mitotic activity, and occasionally more aggressivebehavior, the cellular schwannoma can be a differentialdiagnosis of spindled (regular) MPNST. Besides, the cellularschwannoma presents morphologic similarities with fibro-sarcoma, leiomyosarcoma, and synovial sarcoma, particular-ly in cases with monophasic histology or in needle biopsyspecimens5,6,15
There is a rare variant of schwannoma, the melanoticschwannoma, whose histology is composed of melanin-producing cells with ultrastructural features of Schwanncells. Its immunohistochemistry is strongly positive for S-100, Leu-7, HMB-45, Melan-A and vimentin.16
Neurofibroma (►Figs. 3, 4, 5 and 6)Neurofibromas are a benign peripheral nerve sheath tumor,whoseprimaryneoplasticcellularcomponentsaretheSchwanncells, but they also have nonneoplastic peripheral nerve com-ponents, such as fibroblasts CD34 þ ,3,4,6,8,10,11,17 perineurialcells, blood vessels, axons and mast cells.1,3,4 A total of 10% ofneurofibromas are associated with neurofibromatosis 1.6
Neurofibromatosis 1 (NF1) is the most common geneticdisorder of the nervous system, affecting 1 out of 3,500 new-
Fig. 3 Intraoperative photograph of a plexiform neurofibroma of theright tibial nerve before resection. The patient is a 34-year-oldNF-1male.
Fig. 4 Surgical specimen of a plexiform neurofibroma. Same patientof ►Fig. 3.
Fig. 5 Intraoperative photograph of a neurofibroma of the left sciaticnerve before resection. The patient is a 56-year-old non-neurofibro-matosis female.
Fig. 6 Intraoperative photograph of the left sciatic nerve afterresection. Same patient of ►Fig. 5.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso108

borns worldwide.3,18,19 Neurofibromatosis 1 is an autosomaldominant tumor suppressor disorder8,15 of the Ras signaltransduction pathway,3,18 in which the loss of Schwann cellsleads to a cascade of interactions with the neighboring cells inthe microenvironment and additional cell autonomous modifi-cations, resulting in the formation of multiple neurofibromas.3
There are three specific clinicopathologic subtypes ofneurofibromas based on architectural growth pattern: local-ized, diffuse and plexiform.6
The two localized types of neurofibroma are the localizedcutaneous neurofibromas (LCNs), or dermal neurofibroma,and the localized intraneural neurofibromas (LINs). The LCNsare the most common subtype, occurring sporadically inalmost all cases, and virtually in all NF1 individuals, primari-ly around puberty. They consist of an intracutaneous rela-tively well-circumscribed nodule that grows near thebudding of the nerve. The LINs are similar to the LCNsat the structural and citollogic level, but instead of theskin, they involve the nerve, and can also arise in a majornerve, typically causing a fusiform expansion of the nervetrunk.3,4,6,8,19,20
The diffuse neurofibroma (DFN) consists of a plaque-likeelevation of the skin, usually in thehead and neck region, thatspreads through the subcutaneous tissue. Despite its infil-trative growth, it rarely suffers malignant degeneration.6,20
Conversely, the plexiformneurofibroma (PXN) has a poten-tial of 5 to 13% for malignant transformation and is practicallypathognomonic of NF1. Actually, NF1 patients have a 25 to50%chance of developing PXN. The PXN is a variant of neurofibro-ma that involves numerous adjacent nerve fascicles or multi-ple components of a nerve plexus.3,4,6,18,19
Still, there is themassive soft-tissue neurofibroma (MSTN),a very rare type of PXN often associated to NF1, which ischaracterized by large size, infiltration of soft tissue andskeletalmuscle, frequently involving large anatomical regions.When under the microscopy light, it demonstrates the pres-ence of cellular component. Despite its aggressive appearance,the MSTN hardly suffers malignant degeneration.4,6
There are two variants of neurofibroma with unusualfeatures, the atypical neurofibroma, with degenerative cy-tological atypia, and the cellular neurofibroma,with increasedcellularity. They are differential diagnoses of MPNST, mainlythe low-grade examples, but while the cellular neurofibromalacks the cytological atypia, the atypical neurofibroma lacksincreased cellularity or mitotic activity, and both presentslowermitoticfigures thanMPNST. Still, Naber et alwrite aboutthe hypothesis that the atypical neurofibroma is actually atransition between a neurofibroma and a MPNST.8
There are many different possible differential diagnosesfor neurofibroma, including schwannoma, nerve sheathmyxoma, neurothekeoma, ganglioneuroma and traumaticneuroma as well as variety of non-nerve sheath tumors, inparticular dermatofibrosarcoma protuberans (DFSP) anddesmoplastic malignant melanoma.6
MPNST (►Fig. 7)Malignant peripheral nerve sheath tumors (MPNSTs) areneural crest-malignant neoplasms with nerve sheath differ-
entiation, which arise from the peripheral nerve sheath oradjacent extraneural soft tissue.5,9,15,21 Due to their morpho-logic heterogeneity and lack of specific immunohistochemicalormolecular criteria, the diagnosis ofMPNSTs is often challeg-ing.4 They arise most frequently in the proximal segments ofthe extremities, in the major nerve trunks (such as the sciaticnerve) followedby the trunk, head andneck.4And50 to 66% ofthe MPNSTs arise from neurofibromas, mostly of PXNs.7
The MPNST is a tumor derived from the Schwann cells orpluripotent cells of the neural crest. It displays a heterogenouscellular morphology (including spindle, epithelioid, pleomor-phic or small round cells).8 Generally, the MPNST presentsalternating areas of hyper or hypo cellularity or a diffusegrowth pattern of spindle cells.7,15 The histologic features ofthe MPNST are frequently, but not specifically, fascicles;neuroD whorls; palisades or rosette-like arrangements; peri-neurial/intraneural spread, when associated with nerve peri-vascular hypercellularity; subendothelial infiltration of tumorcells; hemorrhage, and necrosis areas.4–6
There is a rare subtypeofMPNST, theepithelioidMPNST, thatderives more often from a preexisting schwannoma, which hassuffered amalignantdegeneration.4,6 In the epithelioid subtype,heterologous differentiation is observed in 15% of the MPNSTs,and it includes rhabdomyoblasts, cartilaginous and osseouscomponents,or lesscommonly, smoothmuscle, glandular (oftenwith a neuroendocrine foci) or liposarcomatous components,7
particularly in patients with NF1.6 However, there is a certaincontroversy regarding the frequency of the rhabdomyosarcom-atousdifferentiation;whileRodriguezet al state that it is the lessfrequent,6 Guo et al describe it as the most common one.7
The differential diagnosis is extensive, including benignperipheral nerve sheath tumors and various sarcomas,5 suchas atypical and cellular neurofibroma, cellular schwannoma,synovial sarcoma, fibrosarcoma, rhabdomyosarcoma, leio-myosarcoma, dedifferentiated liposarcoma, clear cell sarco-ma or ossifying fibromyxoid tumor of soft parts.6
S100Although S100 is considered important to separate neo-plasms with neural crest origin from the non-neural ones,1
Fig. 7 Intraoperative photograph of a MPNST of the right femoralnerve. The patient is a 16-year-old non-neurofibromatosis female.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso 109

it is a well-known non-specific immunohistochemical mark-er, as S100 is also expressed for non-neural and non-mela-nocytic sarcomas, such as synovial sarcoma (15%), Ewingsarcoma (21%), rhabdomyosarcoma (24%), chondromyosar-coma (75%) and extraskeletalmyxoid chondrosarcoma (45%),according to Karamchandani et al.15 The immunohistochem-ical staining for S-100 protein is more uniform and pro-nounced in schwannomas than in neurofibromas,1 wherebyMPNST has a scattered expression of S100, seen in only 50 to60% of the cases, and themajority of high-grade examples arenegative.4,7,9,10 Thus, when there is a diffuse expression ofS100 in a suspect MPNST sample, it suggests melanoma orcellular schwannoma,4 except for the epithelioid MPNST,which expresses diffuse S100.4,6 In this case, the differentialdiagnoses would be melanoma, clear cell sarcoma, epitheli-oid sarcoma and carcinoma. The absence of melanocyticmarkers, such as MelanA or HMB45, helps to discard mela-noma and clear cell sarcoma, while the lack of low weightcytokeratin expression distinguishes epithelioid MPNSTfrom epithelioid sarcoma and carcinoma.6
Ultimately, when cellular schwannoma assumes a moreaggressive behavior, it can mimic MPNST. In this situation,the usage of S100 immunohistochemistry is crucial, ascellular schwannoma usually expresses strong diffuseS100, while MPNST rarely does.6
CD34The transmembrane phosphoglycoprotein CD34 is ubiqui-tously expressed in the fibroblasts of all subtypes of neuro-fibromas,3,4,6,8,10,11,17 and in the Antoni A areas (compactareas) of the schwannomas.8
The MPNST, on the other hand, has a weak to mediumintensity of expression of the protein, and apparently has akind of inverse expression relation with podoplanin: whenCD34 is highly expressed in MPNST the, the expression ofpodoplanin is weak and vice versa.8
Furthermore, CD34 is also expressed in various types oftumors, such as fibroblastic, myofibroblastic, fibrohistio-cytic, vascular, neural, adipocytic, smooth muscle, melano-cytic and epithelial lesions.4
Therefore, CD34 may not be a good biomarker for differ-entiating peripheral nerve benign lesions, and these fromother lesions.
Sox10Sox10 is useful to distinguish nerve sheath neoplasms frommesenchymal tumors, given the fact that the marker is rarelyseen innon-schwannianornon-melanocytic tumors.4,6,9,10,20,22
Sox10 has been considered a specific marker for schwannomasand neurofibromas9 and, it assists in the differentiation, in theintracranial space, of schwannomas and neurofibromas frommeningioma, which expresses 20 to 30% S-100 protein, orgastrointestinal (GI) schwannomas from GI stromal tumors(that are occasionally S100-protein positive). Still, Karamchan-daniet al suggest that Sox10 isausefulmarker fordifferentiatingcellular schwannoma from fibrosarcoma, leiomyosarcoma, andsynovial sarcoma.15 However, Sox10 is not a reasonable bio-marker for MPNST, as less than half of MPNSTs express Sox10,
which corresponds to entrapped or residual Schwann cells , andthe high-grade MPNST examples are nearly all S100 nega-tive.10,20 Although Sox10 expression is also not exclusive ofneural-crest tumors,9,10 it is pointed by several authors to be amore specific marker than S100.9,10 Moreover, it is suggestedthat Sox10 is used in combination with S100 when diagnosingMPNST, though even using both, there is a non-stainingchance.9,10,20 Thus, the study and, hence, a set of a immunohis-tochemical identities are crucial to avoidmisdiagnosis of neuralcrest tumors, mainly the MPNSTs.
EMAEpithelial membrane antigen (EMA) is normally expressed inperineurial cells; therefore, it is positive stained in perineurio-masandMPNSTwithperineurial differentiation, but negative inschwannomas, neurofibromas or other types of MPNST.1,6,11,12
CalretininAlthough neurofibromas and schwannomas are generallyeasy to distinguish by standard light microscopy, when theschwannoma does not display the characteristic palisadingnucleus, and it consists only (or mostly) of Antoni B areas, itcan be hard to differentiate it from a neurofibroma.
Furthermore, as S-100 might not reliably distinguishthese two neoplasms, calretinin is a good alternative. Sam-son et al have shown that whereas the schwannoma gener-ally presents a positive staining of calretinin, with a strongstaining, neurofibromas rarely stain, andwhen they do, it is aweek staining.1 Therefore, calretinin is suggested to be apromising immunohistochemical tool for the differentiationbetween schwannomas and neurofibromas.
GFAP, Neuron-specific Enolase, Leu-7 and GAP43Neuron-specific enolase (NSE) is a nonspecific biomarkersupportive of nerve sheath differentiation.4 Schwannomaand neurofibroma normally do not, but occasionally can,present Leu-7 and the glial fibrillary acidic protein(GFAP).4,20,22 Le LQ et al stained Schwann cells of mouseplexiformneurofibromawith anti-growth associated protein43 (GAP43), suggesting that in can be used in the immuno-histochemical diagnosis of human neurofibromas.3
RTK and AXLReceptor tyrosine kinase (RTKs) is a receptor expressed onthe cellularmembrane of neurofibromas andMPNSTs, and itsexterior portion is called AXL, whose ligand is the GAS6.Johansson et al have shown that MPNST and neurofibromas,the plexiform and nodular subtypes as well as the dermalsubtype, related to NF1 or not, may express increased AXLprotein on their surface. Furthermore, they suggest thatelevated levels of soluble AXL in the plasma (sAXL) can bedetected in the presence of PXNandMPNST, aswell as highernumbers of dermal neurofibromas are followed by higherlevels of sAXL. Therefore, according to the latter data, sAXLcould be used as a burden marker for neurofibroma.19
However, AXL is not exclusively expressed by neurofibromasand MPNST, thus, it is more a burden marker, than adiagnostic tool.19
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso110

TLE1Transducin-like enhancer of split 1 (TLE1) is commonlyexpressed by peripheral nerve sheath tumors, including100% of schwannomas, 33% of neurofibromas, and (in amore variable andweaker way) 30% ofMPNST.4,6 Therewith-al, TLE1 typically has a strong diffuse expression in synovialsarcoma.3,6 Thus, the difference between the conformationand intensity of the TLE1 expression in the MPNST andsynovial sarcoma could be a discriminatory marker.3,4,6
PodoplaninPodoplanin is a mucin-type transmembrane glycoprotein,expressed in various human cell types as well as in varioustumors, such as hemangioblastomas, tissue of testis, germ celltumors, ovarian serous carcinomas and squamous cell carci-nomas. It has been associated with invasion potential ofadjacent tissue, and hence, podoplanin is highly expressed inthe invasive front of the MPNST. The glycoprotein is negativefor dermal and plexiform neurofibromas, except for the peri-neurial cells, and positive in the compact area of atypicalneurofibroma. Podoplanin is alsopositive inAntoniA (cellular)areas, but not in the Antoni B (reticular) areas of the schwan-nomas. Moreover, the difference between the staining patternof schwannomatosis and NF2-associated tumors, and vestibu-lar schwannoma tumors was not statically relevant.6,8
CD56 and PGP 9.5CD56 and PGP 9.5 are sensitive biomarkers for peripheralnerve sheath tumors, like schwannomas and neurofibromas;thereby, they could be used as trial markers. However, theirexpression is not specific for MPNST.7,23
NestinNestin, an intermediatefilament protein expressed in neuro-ectodermal stem cells,4,7 has shown higher sensitivity forMPNST,7 with more extensive pattern with cytoplasmaticstaining than other neural markers4 (such as CD56, PGP 9.5or S100), whereas with weak or no expression in benignnerve sheath tumors and other sarcomas.4,7 On the otherhand, Shimada et al found similar expression of nestin inrhabdomyosarcoma, leiomyosarcoma and desmoplasticmel-anoma.24 And hence, nestin, if in combination with othermarkers, may be an useful marker in the diagnosis of MPNST.
HMGA2The high mobility group AT-hook 2 (HMGA2) has beenconsidered as a specific biomarker for MPNST when com-pared with its close morphologic mimic, such as synovialsarcoma; therefore, immunohistochemical staining ofHMGA2 could be a useful marker to separate MPNST fromsynovial sarcoma.4,7,23
EGFR, p16, Neurofibromin and Ki-67Pekmezci et al have evaluated several possible useful biomark-ers for thedifferential diagnosis ofMPNSTandcellular schwan-noma and concluded that these 4 biomarkers had promisinguse: epidermal growth factor receptor (EGFR), Ki-67, p16 andneurofibromin.5
Epidermal growth factor receptor is considered an impor-tant component in the pathogenesis of MPNST.5 Pekmezciet al have shown that the expression of EGFR is exclusive ofthe MPNST in comparison with cellular schwannoma (31%and 0%, respectively). Furthermore, other authors had previ-ously showed a lackof EGFR expression in schwannomas, in ageneral way.5
They show that there is a substantial loss of neurofibro-min (the neurofibromatosis type 1 protein product) inalmost all MPNST, except for few low-grade cases, while itis retained in other spindle-cell tumors.5
The same authors also observed a significant loss ofexpression of p16 in MPNST (73%) against a total preserva-tion in cellular schwannoma.5 The biomarker p16 is typicallyexpressed in neurofibromas, and its loss could actually pointto amalignization.6 The amplified expression of EGFR as wellas the loss of expression of p16 and neurofibromin can helpwith the differential diagnosis of MPNST.5
Lastly, Pekmezci et al observed that in cellular schwan-noma slices demonstrating variable labeling with focalstained areas, MPNST showed a diffuse expression. Settinga sensitivity of 87% and a specificity of 96% for Ki-67.5 TheKi-67 usage was also cited by Rodriguez et al.5,6 Actually,some authors are already using the Ki-67 expression inaddition to theWorld Health Organization (WHO) classifica-tion of tumors of soft tissue and bone as a criterium to denotemalignancy in perineuriomas.25,26
p57NTR and SOX2: still an Obscure AreaPekmezci et al highlight SOX2 and p57NTR, two neural stem-cell proteins, as promising biomarkers: p57NTR has beenfound more often in MPNSTs than in schwannomas andhealthy tissue, but when comparing their conclusions withthose of other authors, we found that there is still controver-sy in the literature. On the other hand, SOX2 has been shownin their study as a marker for both MPNSTs and schwanno-mas, while lacking expression in normal peripheral nervetissue. However, further studies are needed for a betterunderstanding of its role in peripheral nerve tissue tumors.5
Conclusions
The classical markers, such as S100 and CD34, are stillimportant in the differentiation between schwannomas,neurofibromas and MPNST. However, there are some newmore specific biomarkers that can help with a challengingdiagnosis: Sox10, CD56, PGP 9.5 and nestin can assist in thedifferentiation, in the intracranial space or in the GI tract,between schwannomas and neurofibromas, and some otherlocal possible tumors as well as benign peripheral nervesheath tumors and MPNSTs. Calretinin is a good choice fordistinguishing schwannomas from neurofibromas. Transdu-cin-like enhancer of split 1 andHMGA2 seem to be promisingalternatives for differentiating MPNSTs from sarcomas (forexample, synovial sarcoma); nestin, EGFR, p16 and Ki-67 canpossibly help to differentiate MPNSTs from cellular schwan-nomas, and neurofibromin can help to distinguish MPNSTsfrom neurofibromas.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso 111

Furthermore, some markers presented here may havemore utilities other than just diagnosing. The marker AXLcan be used as a burden marker for MPNST as well as for theplexiform, nodular and dermal subtypes of neurofibromas.Lastly, podoplanin can help the physician to analyze theinvasion of adjacent tissues by MPNSTs.
As it stands, there is a lack of specific biomarkers forperipheral nerve tumors. However, some new promisingbiomarkers have been coming to light, that require furtherstudies and evidences for their applicability to be betterclassified.
Financial and Material SupportWe did not receive any financial and/or material supportfrom any granting organization or specific funding.
Conflicts of InterestThe authors of the current paper report no conflicts ofinterest concerning the materials or methods used in thisstudy, or the finding described in this paper.
References1 Fine SW, McClain SA, Li M. Immunohistochemical staining for
calretinin is useful for differentiating schwannomas from neuro-fibromas. Am J Clin Pathol 2004;122(04):552–559
2 ShivaneA, ParkinsonDB, Ammoun S, HanemannCO. Expression ofc-Jun and Sox-2 in human schwannomas and traumatic neuro-mas. Histopathology 2013;62(04):651–656
3 Le LQ, Liu C, Shipman T, Chen Z, Suter U, Parada LF. Susceptiblestages in Schwann cells for NF1-associated plexiform neurofi-broma development. Cancer Res 2011;71(13):4686–4695
4 Thway K, Fisher C. Malignant peripheral nerve sheath tumor:pathology and genetics. Ann Diagn Pathol 2014;18(02):109–116
5 Pekmezci M, Reuss DE, Hirbe AC, et al. Morphologic and immuno-histochemical featuresofmalignantperipheralnervesheath tumorsand cellular schwannomas. Mod Pathol 2015;28(02):187–200
6 Rodriguez FJ, Folpe AL, Giannini C, Perry A. Pathology of peripheralnerve sheath tumors: diagnostic overview and update on selecteddiagnostic problems. Acta Neuropathol 2012;123(03):295–319
7 Guo A, Liu A, Wei L, Song X. Malignant peripheral nerve sheathtumors:differentiationpatternsand immunohistochemical features- a mini-review and our new findings. J Cancer 2012;3:303–309
8 Naber U, Friedrich RE, Glatzel M, Mautner VF, Hagel C. Podoplaninand CD34 in peripheral nerve sheath tumours: focus on neurofi-bromatosis 1-associated atypical neurofibroma. J Neurooncol2011;103(02):239–245
9 Nonaka D, Chiriboga L, Rubin BP. Sox10: a pan-schwannian andmelanocytic marker. Am J Surg Pathol 2008;32(09):1291–1298
10 Miettinen M, McCue PA, Sarlomo-Rikala M, et al. Sox10–a markerfor not only schwannian and melanocytic neoplasms but alsomyoepithelial cell tumors of soft tissue: a systematic analysis of5134 tumors. Am J Surg Pathol 2015;39(06):826–835
11 MiettinenM. Immunohistochemistryof soft tissue tumours - reviewwithemphasison10markers.Histopathology2014;64(01):101–118
12 Skovronsky DM, Oberholtzer JC. Pathologic classification of periph-eral nerve tumors. Neurosurg Clin N Am 2004;15(02):157–166
13 Schulz A, Zoch A, Morrison H. A neuronal function of the tumorsuppressor protein merlin. Acta Neuropathol Commun 2014;2(01):82
14 Caltabiano R, Magro G, Polizzi A, et al. A mosaic pattern of INI1/SMARCB1 protein expression distinguishes Schwannomatosisand NF2-associated peripheral schwannomas from solitary per-ipheral schwannomas and NF2-associated vestibular schwanno-mas. Childs Nerv Syst 2017;33(06):933–940
15 Karamchandani JR, Nielsen TO, van de RijnM,West RB. Sox10 andS100 in the diagnosis of soft-tissue neoplasms. Appl Immunohis-tochem Mol Morphol 2012;20(05):445–450
16 Zhang HY, Yang GH, Chen HJ, et al. Clinicopathological, immuno-histochemical, and ultrastructural study of 13 cases of melanoticschwannoma. Chin Med J (Engl) 2005;118(17):1451–1461
17 Kleinschmidt-DeMasters BK, Tihan T, Rodriguez F. DiagnosticPathology:Neuropathology. ElsevierHealth Sciences 2016:528–545
18 Jett K, Friedman JM. Clinical and genetic aspects of neurofibro-matosis 1. Genet Med 2010;12(01):1–11
19 Johansson G, Peng PC, Huang PY, et al. Soluble AXL: a possiblecirculating biomarker for neurofibromatosis type 1 related tumorburden. PLoS One 2014;9(12):e115916
20 Weiss SW, Goldblum JR, Folpe AL. Enzinger and Weiss’ soft tissuetumors. Philadelphia: Saunders/Elsevier; 2014
21 Henderson SR, Guiliano D, Presneau N, et al. A molecular map ofmesenchymal tumors. Genome Biol 2005;6(09):R76
22 Ferner RE. Neurofibromatosis 1 and neurofibromatosis 2: a twentyfirst century perspective. Lancet Neurol 2007;6(04):340–351
23 Hui P, Li N, Johnson C, et al. HMGA proteins in malignantperipheral nerve sheath tumor and synovial sarcoma: preferen-tial expression of HMGA2 in malignant peripheral nerve sheathtumor. Mod Pathol 2005;18(11):1519–1526
24 Shimada S, Tsuzuki T, Kuroda M, et al. Nestin expression as a newmarker in malignant peripheral nerve sheath tumors. Pathol Int2007;57(02):60–67
25 Hayashi T, Hirose T, Nishimura Y, Fukuoka J, Kishikawa M. Hybridschwannoma/perineurioma of the spinal nerve:multifocal occur-rence, and recurrence as an intraneural perineurioma. Pathol Int2013;63(07):368–373
26 Fletcher CDM, Unni KK, Martens F. World Health Organizationclassification of tumors. Pathology and Genetics of Tumors of SoftTissue and Bone. IARC Press; 2002
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Immunohistochemical Markers for Schwannomas, Neurofibromas and MPNST Guedes-Corrêa, Cardoso112

Strictly Intraventricular Craniopharyngioma:Case Report and Literature Review
Craniofaringioma puramente intraventricular: relato decaso e revisão da literatura
Marcelo Lemos Vieira da Cunha1 Ana Luiza Brunelli Pletz2
1Department of Neurosurgery, Hospital Regional do Oeste, Chapecó,SC, Brazil
2Course of Medicine, Universidade Federal do Paraná, Curitiba, PR,Brazil
Arq Bras Neurocir 2018;37:113–118.
Address for correspondence Marcelo Lemos Vieira da Cunha, MD, RuaLauro Muller, 224-E, Apto. 501, Centro, Chapecó, SC, Brazil CEP:89801- 600 (e-mail: [email protected]).
Introduction
Patient LMBG, female, 38 years old, underwent a stereotacticbiopsy in another service in 1997 due to an intraventricularexpansive lesion. The result of the pathology examination atthe timewas oligodendroglioma. Radiotherapywas used as acomplementary therapy. There was a loss of follow-up withthe team responsible for the first treatment after the com-
pletion of the radiotherapy. The patient was admitted to ourservice in 2013, after the onset of a refractory headache30 days before admission. There was an association withnausea and vomiting around 15 days after the onset of theheadache, as well as evolution with paraparesis in the lowerlimbs. Five days before the referral to our service, the patientpresented with speech difficulties and fainting. At the
Keywords
► strictlyintraventricularcraniopharyngioma
► third ventricle► transcallosal
approach
Abstract Strictly intraventricular craniopharyngiomas are a rare topographical variety of cra-niopharyngiomas. The correct diagnosis is important in order to define the surgicalplanning, as the surgical access is different for suprasellar tumors with secondaryinvasion of the third ventricle. An image diagnosis may be difficult, though suggestivepatterns exist. The aim of the present case report and literature review is to add to thescarce literature on strictly intraventricular craniopharyngiomas, as well as to remindthe neurosurgeon of this rare diagnosis so that the proper treatment is provided.
Palavras-chave
► craniofaringiomapuramenteintraventricular
► terceiro ventrículo► acesso transcaloso
Resumo Craniofaringiomas puramente intraventriculares constituem uma rara variedade topo-gráfica dos craniofaringiomas. O diagnóstico correto é fundamental para a definição doplano cirúrgico, posto que o acesso a este tipo de tumor difere dos tumoressuprasselares com invasão secundária do terceiro ventrículo. A confirmação porneuroimagem pode ser difícil, embora existam características sugestivas. A presentedescrição de caso, bem como a revisão de literatura, visa contribuir com a escassaliteratura a respeito de craniofaringiomas puramente intraventriculares, além deremeter o neurocirurgião a este diagnóstico raro para a adoção da conduta corretade tratamento.
receivedNovember 10, 2013acceptedAugust 7, 2015published onlineOctober 28, 2015
DOI https://doi.org/10.1055/s-0035-1564825.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 113

physical examination, she was wry, but with motor dyspha-sia. She had grade III symmetrical paraparesis in the lowerlimbs and grade I paresthesia in the lower limbs. There wereno signs of pyramidal release and no involvement of thecranial nerves or of the cerebellar function. The deep reflexeswere present and symmetrical. An imaging study was per-formed, showing an intraventricular solid-cystic expansivelesion (►Figs. 1, 2, 3). The patient underwent a microneur-osurgical treatment with a transcallosal approach withoutintercurrences. Lesion resection was evidenced (►Fig. 4).
The postoperative period elapsedwith motor aphasia with-out new deficits. The patient was discharged on the seventhpostoperativeday.Afteranewpathological study, a craniophar-yngioma of the adamantinomatous subtype was evidenced.
Discussion
Purely intraventricular craniopharyngiomas are very rare. Theincidence in the literature varies between 0.1 and 16.6%,with an average of 2.8% of all craniopharyngiomas. ►Table 1
defines the frequency of purely intraventricular craniophar-yngiomas in several studies.1 The first case was described in1953byDobos,2 and since then there are fewcases described inthe literature. Until the 1990s, only 22 cases had been de-scribed.3 In some cases described prior to the use of magneticresonance imaging (MRI) in the diagnosis of these lesions, aninaccurate topographic classification of the tumorwaspresent,which led to an incorrect diagnosis of a primarily suprasellartumor with secondary invasion of the third ventricle as intra-ventricular and vice versa. The craniopharyngiomas thataffect the ventricular cavity must be differentiated in termsof their topography, and can be classified into four groups:pseudointraventricular, secondary intraventricular, not strictlyintraventricular and pure intraventricular craniopharyngio-mas. Pseudointraventricular craniopharyngiomas are supra-
sellar tumors that push the lower wall of the third ventricleupwards, while secondary intraventricular craniopharyngio-mas are suprasellar masses that invade the intraventricularcavity as they traverse the lower wall of the third ventricle.Regarding the intraventricular craniopharyngiomas, most oftheminvadethefloorof the thirdventricle,which is replacedbythe tumor,with themarginsof theventricle remaining intact inonly a small portion of cases, which are defined as purely
Fig. 2 Axial cut of contrast-enhanced magnetic resonance imaging ofthe brain showing a solid-cystic intraventricular lesion with 5.3 cm oflaterolateral length.
Fig. 1 A sagittal section of contrast-enhanced T1-weighted magneticresonance imaging showing evidence of corpus callosum and of asolid-cystic intraventricular lesion with 6.1 cm of anteroposteriorlength.
Fig. 3 Coronal computed tomography corneal magnetic resonanceimaging cut in contrast showing a solid-cystic intraventricular lesionwith 2.8 cm of cranial caudal length.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Strictly Intraventricular Craniopharyngioma Cunha, Pletz114

intraventricular craniopharyngiomas. Another difference be-tween intraventricular tumors lies in the pattern of adhesion tothe ventricle floor. While pure intraventricular tumors usuallyconnect to theventricularfloorbyapedunculated, vascularizedand non-reactive gliosis process (in 48% of the cases), non-purely intraventricular tumors present an extensive and firmadhesion to the floor and lateral walls of the third ventricle,without a leptomeningeal layer separating the neural tissuefrom the tumor wall (in up to 64% of the cases).2
Two subtypes of craniopharyngiomas were described:adamantinomatous and papillary, with histopathological andradiological differences, which are summarized in ►Tables 2
and3.4Theadamantinomatoussubtypeaffectsmainlychildren,although it can affect adults. It is heterogeneous, with solid andcystic parts, with an irregularly lobed smooth surface. In itsinterior, it presents a brownor yellowish liquidwith cholesterolcrystals, solid areas with granular consistency, keratin andcalcium microcysts, and the peritumoral brain tissue presentsdense gliosis, rich inRosenthalfibers,which are small islands oftumor cells distant from the tumor mass.3 In the MRI exams,precontrast T1 images frequently reveal single or multiplehyperintense cysts with peripheral enhancement; and in T2,
the cysts may be hypointense or hyperintense.4 These cystscontain cholesterol, triglycerides, metahemoglobin, protein,and desquamative epithelium. Adamantinomatous tumorsare more strongly associated with non-purely intraventricularcraniopharyngiomas.2
The papillary subtype affects almost exclusively adults,with a peak between the ages of 40 and 45 years old,3 and
Fig. 4 Three axial sections, in sequence, of contrast tomography with lesional resection.
Table 1 Percentageofpurely intraventricular craniopharyngiomasin relation to all craniopharyngiomas in several studies
Series % PIVC
Behari et al5 8.0
Steno et al10 1.3
Tomita, Bowman11 16.6
Zuccaro12 1.3
Lena et al13 2.1
Shi et al14 8.0
De Divitiis et al15 0.1
Zhang et al16 2.4
Pan et al17 4.6
Abbreviations: PIVC, purely intraventricular craniopharyngioma.
Table 2 Histopathological differences between craniopharyn-giomas of the adamantinomatous and squamous-papillarysubtypes based on the World Health Organization classification ofbrain tumors
Histopathology Adamantinomatous(solid-cystic mix)
Squamous-papillary(predominantly solid)
Displacement oradhesionto adjacentvessels or cranialnerves
þ —
Calcifications þ Rare
Cyst withcholesterol
þ —
Keratin nodule þ —
Cholesterolcracks
þ —
Necrotic flaresand fibrosis
þ —
Keratin-positivesquamousepithelium with:
Peripheral cellularpalladium
þ —
Starry reticle þ —
Papillaryformations
— þ
Inflammatoryreaction
þ —
Brain invasion þþþ þ
þ, present; �, absent; þþþ, extremely common.Source: Sartoretti-Schefer et al.4
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Strictly Intraventricular Craniopharyngioma Cunha, Pletz 115

shows a tendency to affect the 3rd ventricle (40% of thecases).2 In themacroscopy exam, it is a predominantly cystic,thin-walled tumor. Histologically, anastomotic cords ofpavement epithelium are verified within a loose connectivetissue stroma; in the center, keratinized cells are found; nokeratoid nodules, calcifications or cholesterol crystals arefound; the peritumoral brain tissue presents slight gliosis,and is devoid of tumor cells.3 If there are cysts, they appear ashypointense signs on T1 images with no MRI contrast.Calcifications can occur in both subtypes, although theyare more frequent in adamantinomatous craniopharyngio-mas, which also have a higher recurrence rate,4 partlyexplained by the characteristics of the peritumoral tissue.
Perhaps, this characteristic of the adamantinomatoussubtype explains the latency period found in our case.
Intraventricular craniopharyngiomas affect a higher agegroup than the suprasellar classics. Due to their slow growthand intracavitary location, the obstruction to cerebrospinalfluid flow and the invasion of vital structures occur later,delaying the diagnosis.5,6 This topographic variety presentsother differences in relation to the suprasellar tumors. Whilevisual and endocrine disorders are quite common in supra-sellar tumors, with a prevalence of 70% to 90%, the frequencyis significantly lower in the intraventricular (28% and 27%respectively); the opposite occurs with psychiatric symp-toms, with an incidence of 40% in purely intraventriculartumors, and an incidence of < 15% in the suprasellartumors.2,3,5,6 Memory loss affects up to 33% of the patientswith this rare tumor. These differences can be explained bythe position of the tumor, involving the third ventricle floor,the mammillary bodies and the hypothalamus. Involvementof the third ventricle and of the hypothalamus is oftenassociated with obesity, sexual dystrophy and diabetesinsipidus.1 These patients may present with headache andvomiting due to increased intracranial pressure.5,6 Visualimpairment is more common in suprasellar tumors; in theintraventricular space, it results from chiasmatic compres-
sion by the bulging of the terminal lamina and the chiasmaticrecess of the third ventricle.5
Behari et al5 reported six cases of purely intraventricularcraniopharyngiomas. In all cases, the diagnosis was con-firmed preoperatively by an MRI exam. A total of 4 patientspresented cystic lesions, and 2 presented solid lesions. All ofthe patients presented with intracranial hypertension andpapilledema. All of the patients were submitted to surgery,by different approaches, and two patients received radio-therapy for residual lesions. One patient died from septice-mia in the perioperative period. During the follow-up, whichlasted up to 36months, the computed tomography (CT) scansdid not show recurrence or lesion growth. Tayari et al6
reported the case of a 22-year-old female patient complain-ing of chronic headache with papilledema. A preoperativeMRI demonstrated a large lesion in T1 and hypointense in T2in the third ventricle, obstructing the foramen of Monro. Thepatient underwent a transcallosal surgery, and the diagnosiswas confirmed by anatomopathology, which revealed amixed papillary tumor. During the follow-up, which lasted9 months, there was no recurrence or lesion growth.
The correct topographic diagnosis of craniopharyngiomasis fundamental to establish the surgical plan, since the accessis different for suprasellar and intraventricular tumors. Theerror in the topographic diagnosis of the tumor leads to aninadequate surgical approach.2 Both subtypes of craniophar-yngiomas can be accessed via the pterional or the subfrontalapproaches, which may include orbitozygomatic or clinoidalosteotomy. In the case of suprasellar tumors, the opening ofthe terminal lamina is usually not necessary, whereas theintraventricular tumors are accessed through this structure.5
Magnetic resonance imaging and tomography should dem-onstrate the floor of the third ventricle intact, an evidentsuprasellar cistern, a hypophyseal stem within normality,and no seal changes. Tumor calcification,which is common insuprasellar tumors (50–80%), is rare in the intraventricularvariety.5 Confirmation through neuroimaging can be
Table 3 Clinical and radiological (magnetic resonance) characteristics typical of adamantinomatous and squamous-papillarycraniopharyngiomas
Adamantinomatous craniopharyngioma Scaly-papillary craniopharyngioma
Site Suprasellar Intrasellar/suprasellar or suprasellar
Age Children (occasionally adults) Adults
Tissue structure Predominantly cystic† Predominantly solid�
Tumor cyst in T1 imagewithout contrast
Hyperintense cyst (classic);�
possible hypointensive cystHypointense cyst, if any
�
Tumor form Predominantly lobed�
Predominantly spherical�
Coating of subarachnoid arteries Yes�
No
Tumor recurrence þþþ þCalcifications þþþ þ
þþþ, extremely common; þ, common.Source: Sartoretti-Schefer et al.4
Notes:�These radiological features are statistically significant for differentiation between adamantinomatous and squamous-papillary cranio-
pharyngiomas by Fisher Exact Test. †These radiological features show a trend toward statistical significance for differentiation betweenadamantinomatous and squamous-papillary craniopharyngiomas by Fisher Exact Test.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Strictly Intraventricular Craniopharyngioma Cunha, Pletz116

difficult, since at the time of the diagnosis the tumors aregenerally large and have already invaded the third ventricle,making the anatomic differentiation between the ventricularand tumor margins difficult. There are data, however, thatsuggest and should raise the suspicion of intraventricularcraniopharyngioma: rounded, solid or cystic tumor withhomogeneous signal intensity.2
Ideally, there should be a preoperative differentiationbetween exclusively intraventricular tumors (purely intra-ventricular or not), but, evenwith current diagnostic resour-ces, this does not usually occur, since it is difficult to definethe extra or subpolar involvement of the ventricle by thecraniopharyngioma though a preoperative MRI.1
In the postoperative period, however, the MRI identifiesthe integrity of the floor and the situation of the thirdventricle, enabling the differential diagnosis between thesetopographic subtypes.2
Some characteristics of non-purely intraventriculartumors are the predominantly adamantinomatous histolog-ical pattern, extensive adhesions to the floor of the thirdventricle, and worse surgical outcome due to the proximityof the hypothalamus.2
The main differential diagnoses with tumors that originateprimarily in the ventricle include colloid cyst, ependymoma,choroid plexus papilloma, astrocytoma, and meningioma.5,6
Although imaging methods are fundamental in the diagnosisof brain pathologies, the histopathological diagnosis is onlypossible with a biopsy. There are reports in the literature ofcases in which a diagnosis based on imaging methods alonewould be incorrect in between 13% and 26% of the cases.7
There are several indications for stereotactic biopsy, in-cluding the collection of intracranial expansive lesions,drainage of cysts, abscesses and hematomas, resection ofbrain lesions in eloquent areas, radiosurgery, implantation ofradioactive isotopes, among others.8
Although the correct diagnosis can be observed in themajority of cases, difficulties in the interpretation of thestereotactic biopsymay lead to diagnostic errors, as occurredwith the patient reported in the present study. According toPittella,8 the main situations that can lead to error are: thickand hypercellular smears of normalwhitematter, simulatinga low grade glioma; reactive gliosis with Rosenthal fibersaround craniopharyngiomas, simulating astrocytoma; pos-terior fossa lesions containing neurons of the granular layer,mimicking medulloblastoma, lymphoma, or an inflammato-ry process by generating densely cellular and small cellsmears; poorly differentiated primary neoplasms versusmetastases; and the correctness in the classification andgraduation of the neoplasia.
The treatment of choice is surgical, and the access tointraventricular craniopharyngiomas presents a greatertechnical difficulty in relation to the suprasellar tumors,because it is necessary to cross healthy structures to accessthe ventricle. The surgical difficulty is elevated by complextopographic relationships with vital neurovascular struc-tures. An adequate exposure of the tumor to direct visionthroughout the surgical procedure is important to avoidtraumatic and ischemic hypothalamic lesions.1 The main
techniques described are transcallosal, frontal transcorticaland the terminal lamina approach. The latter has low mor-bidity, but is related to lower success rates in total massresection.2 Invasion of thewalls of the third ventricle and theproximity of the hypothalamus increase the risk of sequelae,and the maintenance of the anatomical integrity of theventricular walls is essential.1 In cases of extensive andfirm adhesion to the third ventricle, and with characteristicsof non-purely intraventricular tumors, Pascual et al2 advisedagainst radical tumor excision to avoid hypothalamic lesions.There are reports in the literature of the successful use ofradiotherapy after surgery with partial resection of thecraniopharyngioma. Behari et al5 described two cases inwhich tomography during the follow-up showed the totalresolution of the lesions after radiotherapy. Stereotacticradiosurgery is associated with a progressive shrinkage ofthe tumor mass with a normalization of the ventricle for-mat.1 If possible, an MRI exam of the brain should beperformedwithin the first 72 hours postoperatively to verifythe presence of residual tumor and of complications such ashypothalamic and vascular lesions.9
Conclusion
Purely intraventricular craniopharyngiomas are a rare topo-graphic variety of craniopharyngiomas. The diagnostic ex-amination of choice is MRI. The preoperative differentiationfrom the suprasellar tumors with secondary invasion of theventricle walls is fundamental for the correct surgical plan-ning. The differentiation between intraventricular subtypes– purely intraventricular or not – is difficult to achievepreoperatively through an MRI exam. The postoperativeexamination can make the differential diagnosis most ofthe time. Stereotactic biopsy is of great value in the neuro-surgical practice, but it has limitations in the precise diag-nosis. The treatment of choice is always the completeresection of the tumor, and adjuvant radiotherapy can beperformed in cases of incomplete resection.
References1 Pascual JM, Prieto R, Carrasco R. Infundibulo-tuberal or not
strictly intraventricular craniopharyngioma: evidence for amajortopographical category. Acta Neurochir (Wien) 2011;153(12):2403–2425, discussion 2426
2 Pascual JM, González-Llanos F, Barrios L, Roda JM. Intraventricularcraniopharyngiomas: topographical classification and surgicalapproach selection based on an extensive overview. Acta Neu-rochir (Wien) 2004;146(08):785–802
3 Zanon-Collange N. Craniofaringioma: atualização terapêutica.Sociedade de Neurocirurgia de São Paulo; 2006
4 Sartoretti-Schefer S, Wichmann W, Aguzzi A, Valavanis A. MRdifferentiation of adamantinous and squamous-papillary cranio-pharyngiomas. AJNR Am J Neuroradiol 1997;18(01):77–87
5 Behari S, Banerji D, Mishra A, et al. Intrinsic third ventricularcraniopharyngiomas: report on six cases and a review ofthe literature. Surg Neurol 2003;60(03):245–252, discussion252–253
6 Tayari N, Etemadifar M, Hekmatnia A, Mahzouni P, Maghzi AH,Rouzbahani R. Intrinsic third ventricular craniopharyngioma:Acasereport. Int J Prev Med 2011;2(03):178–185
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Strictly Intraventricular Craniopharyngioma Cunha, Pletz 117

7 Arbit E, Galicich JH. Importance of image-guided stereotacticbiopsy to confirm diagnosis in an oncological setting. Ann SurgOncol 1994;1(05):368–372
8 Pittella JEH. Biópsia estereotáxica no diagnóstico de tumorescerebrais e lesões não neoplásicas: indicações, acurácia e dificul-dades diagnósticas. J Bras Patol Med Lab 2008;44(05):343–354
9 Curran JG, O’Connor E. Imaging of craniopharyngioma. ChildsNerv Syst 2005;21(8-9):635–639
10 Steno J, Malácek M, Bízik I. Tumor-third ventricular relationshipsin supradiaphragmatic craniopharyngiomas: correlation of mor-phological, magnetic resonance imaging, and operative findings.Neurosurgery 2004;54(05):1051–1058, discussion 1058–1060
11 Tomita T, Bowman RM. Craniopharyngiomas in children: surgicalexperience at Children’s Memorial Hospital. Childs Nerv Syst2005;21(8-9):729–746
12 Zuccaro G. Radical resection of craniopharyngioma. Childs NervSyst 2005;21(8-9):679–690
13 Lena G, Paz Paredes A, Scavarda D, Giusiano B. Craniopharyn-gioma in children:Marseille experience. Childs Nerv Syst 2005;21(8-9):778–784
14 Shi XE,WuB, Zhou ZQ, FanT, Zhang YL.Microsurgical treatment ofcraniopharyngiomas: report of 284 patients. Chin Med J (Engl)2006;119(19):1653–1663
15 de Divitiis E, Cappabianca P, Cavallo LM, Esposito F, de Divitiis O,Messina A. Extended endoscopic transsphenoidal approach forextrasellar craniopharyngiomas. Neurosurgery 2007;61(05,Suppl 2):219–227, discussion 228
16 Zhang YQ, Ma ZY, Wu ZB, Luo SQ, Wang ZC. Radical resection of202 pediatric craniopharyngiomas with special reference to thesurgical approaches and hypothalamic protection. Pediatr Neu-rosurg 2008;44(06):435–443
17 Pan J, Qi S, Lu Y, et al. Intraventricular craniopharyngioma:morphological analysis and outcome evaluation of 17 cases.Acta Neurochir (Wien) 2011;153(04):773–784
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Strictly Intraventricular Craniopharyngioma Cunha, Pletz118

Recurrent Pituicytoma in a Pediatric Patient:A Case Report
Pituicitoma recorrente em um paciente pediátrico:relato de caso
Miguel Ángel Maldonado-Morán1 Jeisson Ospina2 Juan Vega3 Claudia Restrepo4 Daniela Rico5
Camilo Zubieta6 Pedro Penagos6
1Universidad Militar Nueva Granada, Bogotá, Colombia2Department of Neurological Surgery, Hospital Infantil Universitariode San José, Fundación Universitaria Ciencias de la Salud (FUCS),Bogotá, Colombia
3Hospital Militar Central, Bogotá, Colombia4Department of Neurological Surgery, Universidad Militar NuevaGranada, Bogotá, Colombia
5Department of Neurological Surgery, Universidad El Bosque, Bogotá,Colombia
6Department of Neurological Surgery, Instituto Nacional deCancerología, Bogotá, Colombia
Arq Bras Neurocir 2018;37:119–122.
Address for correspondence Miguel Ángel Maldonado Morán,Universidad Militar Nueva Granada, Bogotá, Colombia(e-mail: [email protected]).
Keywords
► pituicytoma► pituitary tumor► pituitary stalk tumors► pediatric brain tumor
Abstract Pituicytoma is a rare tumor that arises from the glial cells of the neurohypophysis. For along time, it was believed that pituicytomas only appeared in adults. Currently, at leastthree cases of this entity occurring in children have been reported in the literature. Theaim of the present report is to describe the case of a 5-year-old girl who presented to theemergency department with visual disturbances, and the diagnosis was a recurrentpituicytoma. Therefore, the clinical presentation, the radiological features of thetumor, and the corresponding surgical management are described. Additionally, abrief review of the management of this unusual entity was performed.
Palavras-chave
► pituicitoma► tumor pituitário► tumores da haste
hipofisária► tumor cerebral
pediátrico
Resumo O pituicitoma é um tumor raro que surge das células gliais da neurohipófise. Durantemuito tempo, acreditou-se que os pituicitomas só aparecessem em adultos. Atual-mente, pelo menos três casos desta entidade ocorrendo em crianças foram relatadosna literatura. O objetivo do presente artigo é descrever o caso de umamenina de 5 anosque chegou à emergência com distúrbios visuais, e o diagnóstico foi um pituicitomarecorrente. A apresentação clínica, as características radiológicas do tumor, e ocorrespondente manejo cirúrgico foram, portanto, descritos. Além disso, foi realizadauma breve revisão do tratamento desta entidade incomum.
receivedJanuary 28, 2018acceptedApril 24, 2018published onlineJune 11, 2018
DOI https://doi.org/10.1055/s-0038-1660465.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 119

Introduction
The term pituicytoma refers to an infundibuloma that arisesfrom the glial cells of the neurohypophysis and/or thepituitary stalk, also called pituicytes.1–3 In the literature,there are less than 80 cases reported that meet all of theWorld Health Organization’s (WHO) classification criteria forthis type of tumor.3 There is no clinical guideline for thediagnosis and management of this rare entity. The 2016WHO classification of tumors of the central nervous systemclassifies the pituicytoma as a grade 1 (borderline, unspeci-fied, or uncertain behavior) tumor.4 In the classical descrip-tion, the pituicytoma has been considered a condition thatoccurs only in adults,2 so in cases like the one reported in thepresent study, in a pediatric patient, the diagnosis becomesvery challenging. To our knowledge, there are only four casesdescribed in the pediatric population,2,5–7 and we did notfind any reports about the management of recurrent pitui-cytoma in a pediatric patient.
Materials and Methods
A complete description of the pertinent information fromclinical records was made, all of the available histologicsamples were taken, and all diagnostic imaging examswere performed. The patient was admitted to the InstitutoNacional de Cancerología, in Bogota, Colombia. A completemultidisciplinary assessment was performed by pediatri-cians, a pediatric oncologist, pediatric endocrinologists andneurosurgeons. A preoperative magnetic resonance imaging(MRI) of the brain and of the sellar region as well as acomplete endocrinology evaluation were performed.
The present work is based on the general principles ofhuman research ethics set forth in the Helsinki declaration;the purpose of the present study is to obtain scientificknowledge for a better diagnosis and a more precise evalua-tion that may eventually help to predict or improve theneurological outcome of these patients. It adopts resolution8,430/1993 of the ColombianMinistry of Health, and is basedon the definitions of risk contained in the correspondingarticle of that law, forwhich it classifies the present studyas arisk-free research, since it is a retrospective study based onmedical records. Authorization was requested to the parentsof the patient to includeher information in the present study,preserving her identity both in the analysis of the informa-tion and in the images presented. The informed consent wasfully filled by her parents for the publication of clinical andradiologic information in this manuscript.
Case Report
This is a case of a Hispanic 5-year-old girl who presented tothe emergency department with a 3-month clinical course ofdecreased visual acuity and nystagmus. A contrast-enhancedMRI of the headwas performed, showing a tumor in the sellaturcica. Tumor resection was indicated, but the parentsrejected any surgical intervention in her first consultation.Two years later, the patient presented again to the emergen-
cy department in a different institutionwith bilateral amau-rosis and aggressiveness. Her parents accepted surgicaltreatment in the second consultation, and an urgent resec-tion was performed via frontal craniotomy, completing atotal cyst drainagewith resection of the nodular component.A non-conclusive pathology report was obtained at first. Inthe immediate postoperative period, there was no improve-ment in her symptoms. After a few months, the patient wasreferred to the Instituto Nacional de Cancerología for multi-disciplinary management with pediatric oncology and on-cologic neurosurgery. Upon admission to our institution, afistula containing cerebrospinal fluid was detected. Men-strual disorders, as well as obesity and early gynecomastiawere also recorded. A contrast-enhanced MRI of the brainwas performed. The tumor was hypointense in T1, hypoin-tense in T2, with heterogeneous enhancement with gadolin-ium of the nodular component. A cystic component was alsonoted within the anterior cranial fossa (►Fig. 1).
A surgical decision-making group, including the pediat-ric oncology, endocrinology, and neurosurgery departmentsconcluded that the first diagnostic possibility was an ada-mantinomatous craniopharyngioma, and a new surgicalresection should be performed. Consequently, the patientunderwent a new surgical procedure, with a right trans-cranial subfrontal approach. A near gross total resectionwas performed, achieving � 95% cytoreduction of the solidcomponent (►Fig. 1). Pathology results reported an astro-cytic glioma (grade 1 of the 2016 WHO classification),consistent with a pituicytoma (►Figs. 2, 3). Immunochem-istry samples demonstrated endomysial antibodies (EMAs)and chromogranin negativity, with a proliferation index Ki-67 lower than 3%. Furthermore, the adjuvant treatmentwith radiotherapy was completed. Postoperatively, the pa-tient persisted with central hypothyroidism and hypocor-tisolism, receiving hormonal substitution. In the clinicalexamination, improvement in visual acuity and betterbehavior were noted, with a Lansky/Play performance scalescore of 80%.
Fig. 1 (A) Preoperative contrast-enhanced magnetic resonanceimaging (MRI) of the head showing a recurrent pituicytoma in apediatric patient. A sealed lesion with a large solid component(arrow), with heterogeneous enhancement, is noted. An interhemi-spheric frontal cyst is also observed (arrowhead). (B) Postoperativecontrast-enhanced MRI of the head in the two-year follow-up. Dis-appearance of the suprasellar interhemispheric solid component isobserved. The partial residual cystic component of the interhemi-spheric frontal lesion is denoted (arrowhead).
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Recurrent Pituicytoma in a Pediatric Patient Maldonado-Morán et al.120

Discussion
Pituicytomas are tumors of the nucleated cells that arise fromthe pituitary neurohypophysis and the infundibulum (pitui-cytes), which are located in the sellar and suprasellar regions,8
and are grouped as tumors of the sellar region.4 They occurpredominantly in adults, between the 4th and the 5th decadesof life, and have a slight preponderance on males (1.3:1).3
Moreover, a pituicyte is a glial cell located in the neurohy-pophysis near the hypothalamus. It is closely related to multi-ple vessels, and has different axon connections. It is believedthat pituicytesplaya role in the regulationofhormonal releaseand secretion of endocrine cells.8 Pituicytes also serve as asupport for oxytocin- and vasopressin-producing neurons.There are five types of cells: oncocytic, major, ependymal,dark and granular.5,9 The neoplasms arising from these cellsare considered benign lesions with a progressive course, withno reports of malignant transformation.5
Pituicytomas are very rare and, to the best of our knowl-edge, there are only 78 cases of pituicytomas reported in theliterature. Only four of them occurred in the pediatricpopulation. A total of 3 occurred in girls, and 1 in a 13-year-old boy with a giant pituicytoma.2 The youngest case isthat of a 7-year-old girl.5 To date, the patient in our report isthe youngest patient with a pituicytoma reported in theliterature, being the fifth case of a pediatric pituicytoma.
The clinical presentation in these patients is attributableto the local compression of the tumor. The most commonsymptoms includeheadache, visual field disorders and visualalterations due to compression of the chiasm. Lower stalk orposterior pituitary lesions produce temporary diabetesinsipidus and endocrine disorders like hypopituitarism, sex-ual dysfunction, menstrual disorders and gynecomastia.4,9
Our case presented with menstrual disorders, obesity andgynecomastia, which are symptoms with an incidence ofpresentation of 3,8%, 1% and 9% respectively,2 which makesour report even more interesting.
The pathologic profile is marked by a proliferation offusiform bipolar elongated cells, with low cell proliferation,low atypia, and paucity of mitotic figures. Pituicytoma cellstend to be swirling. The literature shows that many cells arepositive for vimentin.3 Additional diffuse S-100 proteininmunoreactivity and glial fibrillary acidic protein (GFAP)staining are usually present. The anterior pituitary hormonemarkers are mostly negative, and they are used for differen-tial diagnosis with pituitary adenomas.2,8 These tumors arealso negative for EMA and chromogranin. The proliferationindex Ki-67 is low, usually below 3%.10
Regarding the imaging features, an adequate imagingprotocol is mandatory to characterize these tumors. Thefirst step is to perform a computed tomography (CT), whichusually shows an isointense mass located within the sellaror suprasellar regions, without evidence of calcification orbony erosion, with strong enhancement after contrast ad-ministration.2 Nevertheless, MRI is the diagnostic modalityof choice. Mostly, the tumors are presented as solid, well-defined oval masses, located in the posterior sellar region.They show isointense signal on T1 and low hyperintensesignal on T2. After contrast administration, a homogeneousor heterogeneous pattern of enhancement can be pres-ent.1,3,11 The location within the posterior aspect of thepituitary gland, clearly displacing the adenohypophysisforward, is characteristic. In 50% of the cases the locationis purely suprasellar, followed by 40% with suprasellarextension.1 This sellar mass is challenging to distinguishfrom other lesions. According to the review by Covingtonet al,12 only pituicytomas can be purely intrasellar. TheDifferential diagnoses include pituitary adenoma, pilocyticastrocytoma, meningioma, granular cell tumors, cranio-pharyngioma, hamartoma and germinoma.1,4,11
The gold standard treatment of these tumors is surgery.1
The aim of the surgery is to perform a total resection of thetumor. There is a very low recurrence rate (4,3%).8,9
Chakraborti et al showed no recurrence after gross totalresection in a follow-up period varying from 3 months to7 years.5 In their review, they reported 67 procedures, withthe trans-sphenoidal approach being the most common,followed by the frontotemporal approach. They describedthe tumors and demarcated solid pink masses. Gross totalresection was not achieved due to hypervascularity,which remains the most common intraoperative chal-lenge.5 Since these tumors are vascular, preoperative em-bolization of arterial feeders has been reported, in order tofacilitate total removal.13 The most common postoperative
Fig. 2 These histological samples (A, panoramic view; B, zoom view)show tumor cells with glial differentiation, with the characteristicfusiform cell proliferation, with a fibrillary fundus and the presence ofcalcifications, without atypia or mitosis.
Fig. 3 Immunochemistry samples showing (A) S100 positivity and (B)glial fibrillary acidic protein (GFAP) positivity, consistent with apituicytoma.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Recurrent Pituicytoma in a Pediatric Patient Maldonado-Morán et al. 121

complications are diabetes insipidus, hypopituitarism,visual deficit and hypotiroidism.2
Most tumors behave in a benign fashion if total resection isperformed. The cases with gross total resection do not showrecurrence.14 Nevertheless, the data in the literature is limit-ed.8,9Someauthors estimate39%of recurrence inpatientswhounderwent subtotal resection over periods ranging from5 months to 7 years. There is restricted experience regardingadjuvant chemotherapy or radiation therapy in the manage-ment of cases undergoing complete resection, whereas con-troversy exists regarding cases with partial removal, as well asregarding the benefit of radiotherapy because of the high ratesof recurrence.2 A close follow-up with MRI for patients withresidual tumors is recommended.2 Stereotactic radiotherapyhas been considered for cases with aggressive behavior, orwhen a second surgical approach is unachievable because ofsize and location. Besides, the side effects of radiation, whichinclude hypopituitarism, optic neuropathy, necrosis, vasculardamage, and induction of other types of brain tumors, alwayshavetobeconsidered.1Noclinicalguidelineofmanagement forrecurrent pituicytomas exists. We believe that a transcranialsubfrontal/frontotemporal approach is a feasible option forrecurrent cases. In our case, the patient recovered from hervisual symptoms, and only a cystic component of the lesionpersisted after the second intervention. Complimentary radio-therapy was not needed, though. The behavior of this residualcyst remains unclear, and additional follow-up is needed.
Conclusions
A Pituicitomas are a very rare type of tumors, even more inpediatric patients. As this entity is not common in youngpatients the diagnosis could be very challenging, but with thecorrect histopathology tools we could did it. Surgery is thegold standard treatment. We present in this report a case ofadequate surgical treatmentwith a frontotemporal approachfor a recurrent pituicytoma in a very young patient, theyoungest (to our knowledge) in the literature.
Conflicts of InterestNone to declare.
References1 Teti C, Castelletti L, Allegretti L, et al. Pituitary image: pituicy-
toma. Pituitary 2015;18(05):592–5972 Tian Y, Yue S, Jia G, Zhang Y. Childhood giant pituicytoma: a report
and reviewof the literature. Clin Neurol Neurosurg 2013;115(10):1943–1950
3 Ellis JA, Tsankova NM, D’Amico R, et al. Epithelioid pituicytoma.World Neurosurg 2012;78(1-2):E1–E7
4 Louis DN, Perry A, Reifenberger G, et al. The 2016 WorldHealth Organization Classification of Tumors of the CentralNervous System: a summary. Acta Neuropathol 2016;131(06):803–820
5 Chakraborti S, Mahadevan A, Govindan A, et al. Pituicytoma:report of three cases with review of literature. Pathol Res Pract2013;209(01):52–58
6 Yilmaz Ö, Turan A, Yiğit H, Duymuş M, Koşar U. Case of pituicy-toma in childhood. Childs Nerv Syst 2012;28(01):11–12
7 Cambiaso P, Amodio D, Procaccini E, et al. Pituicytoma andCushing’s Disease in a 7-Year-Old Girl: A Mere Coincidence?Pediatrics 2015;136(06):e1632–e1636
8 Kowalski RJ, Prayson RA, Mayberg MR. Pituicytoma. Ann DiagnPathol 2004;8(05):290–294
9 Yang X, Liu X, Li W, Chen D. Pituicytoma: A report of three casesand literature review. Oncol Lett 2016;12(05):3417–3422
10 Brat DJ, Scheithauer BW, Staugaitis SM, Holtzman RN, Morgello S,Burger PC. Pituicytoma: a distinctive low-grade glioma of theneurohypophysis. Am J Surg Pathol 2000;24(03):362–368
11 Hammoud DA, Munter FM, Brat DJ, Pomper MG. Magnetic reso-nance imaging features of pituicytomas: analysis of 10 cases.J Comput Assist Tomogr 2010;34(05):757–761
12 Covington MF, Chin SS, Osborn AG. Pituicytoma, spindle celloncocytoma, and granular cell tumor: Clarification and meta-analysis of theworld literature since 1893. AJNR Am J Neuroradiol2011;32:2067–2072
13 Furtado SV, Ghosal N, Venkatesh PK, Gupta K, Hegde AS. Diag-nostic and clinical implications of pituicytoma. J Clin Neurosci2010;17(07):938–943
14 Pirayesh IslamianA, Buslei R, SaegerW, Fahlbusch R. Pituicytoma:overview of treatment strategies and outcome. Pituitary 2012;15(02):227–236
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Recurrent Pituicytoma in a Pediatric Patient Maldonado-Morán et al.122

Hérnia medular idiopática atípica — relato de caso
Atypical Idiopathic Spine Cord Herniation (ISCH) — Case Report
Heber Martim Vieira1 Rodrigo Amaral1 Luis Marchi1 Gabriel Pokorny1 Fernando Marcelino1
Fabio Rosa1 Angelo Guarçoni Netto1 Nicholai Faulhaber1 Rubens Jensen1 Luiz Pimenta1
1 Instituto de Patologia da Coluna (IPC), São Paulo, SP, Brasil
Arq Bras Neurocir 2018;37:123–127.
Address for correspondence Gabriel Pokorny, BSc, Instituto dePatologia da Coluna (IPC), R. Vergueiro, 1421, São Paulo, SP, Brazil(e-mail: [email protected]).
Introdução
Hérnia medular idiopática (HMI) é uma condição rara demielopatia, que acomete tipicamente pacientes do sexofeminino de meia idade. Essa condição foi descrita pelaprimeira vez por Wortzman em 1974,1 e teve menos de174 casos descritos na literatura até 2016.2 A HMI consiste
em um defeito de fechamento dos folhetos da dura-máter,mais frequentemente em sua porção ventral, resultando emuma herniação do conteúdo medular, podendo ser de natu-reza congênita ou adquirida, provocada por trauma ou pós-procedimento cirúrgico, mas sua patogênese ainda é incerta.A história habitual da doença é de uma mielopatia deevolução lenta e progressiva, com a apresentação clínica da
Palavras-Chave
► coluna vertebral► medula espinhal► canal vertebral► hérnia► hérnia medular► microcirurgia
Resumo A hérniamedular idiopática (HMI) é uma causa rara demielopatia progressiva que afetaprincipalmente mulheres de meia idade com apresentação clínica típica com aSíndrome de Brown-Sequard. Possui etiologia incerta, sendo a teoria mais aceita ade ser um defeito congênito na dura-máter que leva a uma herniação lenta eprogressiva da medula que ocasiona uma lesão evolutiva, podendo levar a um déficitirreversível quando subdiagnosticado e não tratado da forma ideal. A realização daressonância magnética é fundamental para o diagnóstico, e a cirurgia é o tratamentode escolha para reverter e cessar os sintomas mielopáticos. O presente artigo mostraum caso de uma apresentação atípica da localização do defeito dural e da herniação,não descrita ainda na literatura, levando a uma apresentação neurológica e anatômicaincomum para esta patologia, obrigando a realizar um planejamento cirúrgicoespecífico para tal caso.
Keywords
► spine► spinal cord► spinal canal► hernia► spinal cord herniation► microsurgery
Abstract Idiopathic medullary hernia is a rare cause of progressive myelopathy, primarilyaffecting middle-aged women, typical clinical presentation with Brown-SequárdSyndrome. Its etiology is uncertain, but the most accepted theory is that a congenitaldefect in the dura mater leads to a slow and progressive spinal cord herniation, causingan evolutionary spinal cord injury, which can lead to an irreversible deficit whenunderdiagnosed and not treated adequately. Magnetic resonance imaging is essentialfor the diagnosis, and surgery is the treatment of choice to reverse and stopmyelopathy symptoms. The present article shows a case of an atypical presentationof the location of the dural defect and herniation, not yet described in the literature,leading to an unusual neurologic and anatomical presentation for this pathology,requiring a specific planning for this case.
receivedFebruary 26, 2018acceptedApril 3, 2018published onlineMay 18, 2018
DOI https://doi.org/10.1055/s-0038-1655745.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 123

síndrome de Brown-Sequard na grande maioria dos casos. ODiagnóstico da Hérnia Medular é feito por meio de resso-nância magnética, onde é visto um deslocamento do con-teúdo medular por um defeito dural, este deslocamentoocorre mais frequentemente para porção anterior da coluna.
Este relato demonstra o caso de uma paciente com umaapresentação clínica e anatômica atípica de HMI, que possuiuma variação posicional da lesão, sendo esta de caráterlateral, fugindo do típico deslocamento ventral. O caso foitratado cirurgicamente em nossa instituição, sendo neces-sários planejamento e abordagem diferenciados para omesmo.
Os autores descrevem a técnica cirúrgica para esta varia-ção da apresentação, bem como os achados clínicos, radio-lógicos, intraoperatórios e a evolução no acompanhamentopós-operatório.
Apresentação do caso
Apresentação clínica e radiológicaPaciente do sexo feminino, de 38 anos de idade, sem comor-bidades, com queixa de parestesia no membro inferioresquerdo na região do quadríceps há 2 anos, evoluindolentamente com piora progressiva nos últimos 6 meses,associado a fraqueza na perna esquerda, dificuldade dedeambular e piora da parestesia. Nega trauma ou procedi-mento cirúrgico prévio. Ao exame físico, apresenta forçamotora grau IV no membro inferior esquerdo, proximal edistal, presença de hiperreflexia patelar e aquileu à esquerda,parestesia no quadríceps, sinal de Babinski presente e mar-cha claudicante no membro inferior esquerdo. Fugindo àapresentação típica da Síndrome de Brown-Sequard, já queapresentava alteração sensitiva e motora do mesmo lado enão apresentava alteração termo-álgica, apenas parestesia.
O estudo por RM da coluna torácica evidencia umaherniação medular ao nível de T9-T10 que se estende peloneuroforame à esquerda (►Fig. 1), com saída do conteúdo
medular por uma falha dural, com orifício de 12 mm dedimensão, para o interior do forame adjacente, englobando araiz de T9 esquerda, ausência de coluna liquórica à esquerdae deformação medular, com significante herniação do funí-culo lateral esquerdo.
A abordagem cirúrgica foi indicada devido a uma combi-nação de fatores que incluem piora clínica, déficit motor epresença de mielopatia.
Procedimento cirúrgicoComo este caso apresenta uma herniação lateral pelo foramee engloba a raiz adjacente, foi optado por realizar umaartrectomia por via posterior, facilitando a abordagem aoforame a fim de reduzir o volume que se encontrava em suamaior parte foraminal; radiculotomia à esquerda; correçãodo defeito dural e instrumentação de T9-T10-T11, devido àinstabilidade gerada pela ampla laminectomia e ressecção dafaceta para evitar cifose segmentar.
O procedimento cirúrgico foi realizado sob anestesia gerale sob monitorização com potenciais evocados somatossen-sitivo e motor. O paciente foi posicionado em decúbitoventral horizontal com coxins pélvico e subescapular. Oacesso cirúrgico foi feito por linha média posterior comdissecção da musculatura paraespinal.
Foi realizada ampla laminectomia do nível T9 ao nível T11e facetectomia da articulação de T9-T10 à esquerda. Com estaressecção foi possível a exposição e observação do saco durale retração do mesmo para a esquerda. Assim, foi possível avisualização da massa com extensão para o neuroforameadjacente, demonstrada na ►Fig. 2.
Foi realizada uma durotomia, aproximadamente 5 cm, ereparo em ambas as bordas da dura-máter com fio nylon 3–0,com ampla exposição do conteúdo intradural, auxiliando aressecção dos ligamentos denteados, exposição da medula edo conteúdo herniado, assim como visualização interna dafalha dural. Após abertura dural, foi observado deslocamentomedular com herniação lateral pelo orifício dural esquerdo,
Fig. 1 Imagens sagital (A) e axial (B) de ressonância nuclear magnética ponderada em T2 demostram herniação medular ao nível de T9-T10através de falha dural para o interior do neuroforame da raiz de T9 à esquerda.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hérnia Medular Idiopática Atípica Vieira et al.124

englobando a raiz emergente pelo forame ao nível T9,confirmando o diagnóstico de HMI (►Fig. 3).
Com auxílio de um dissector Rhoton e ummicroscópio, foirealizada microcirurgia com ressecção dos ligamentos den-teados à esquerda, um nível acima e abaixo, possibilitandotração da medula e redução do volume herniado. Observadaa ausência de plano para dissecção da raiz de T9, optou-seentão pela sua radiculotomia. Foi realizado o fechamento doorifício com substituto dural e duroplastia com fio monofi-lamentar 5–0 (►Fig. 4).
Suplementação posterior e fixação pedicular devido alaminectomia de três vértebras consecutivas e artrectomiaà esquerda, a fim de evitar uma possível evolução comacentuação da cifose. Para tal, foram utilizados seis parafusostranspediculares e duas hastes nos níveis de T9, T10 e T11(►Fig. 5), de acordo com a técnica de Roy-Camille.
Os potenciais evocados mantiveram-se sem alteraçõesdurante o procedimento cirúrgico. A cirurgia teve duraçãototal de 5 horas e perda sanguínea estimada em 800 mL, apaciente foi encaminhada para a UTI imediatamente após acirurgia.
No primeiro dia pós-operatório, a paciente apresentoupiora da força e da sensibilidade em ambas as pernas. Pormeio de novo estudo de imagem, diagnosticou-se um hema-toma extradural na região dorsal, que exercia efeito demassa. A paciente foi então encaminhada para o centrocirúrgico para drenagem do hematoma e revisão da hemos-tasia. Após reabertura da sutura da pele e do tecido subcu-tâneo, foi feita a drenagem espontânea de um coáguloextradural de 50 mL de volume. Uma vez que realizadas a
Fig. 2 Imagem intraoperatória do acesso posterior: laminectomia T9-T10-T11, saco dural com presença de massa lateral com extensão aoneuroforame de T9
Fig. 3 1 Imagem axial de tomografia computadorizada pré-operatóriaao nível de T9 e2 fotografia intraoperatória pós-durotomia e resseçãodos ligamentos denteados. Nas figuras são indicadas as seguintesestruturas anatômicas: (A) cordão medular, (B) herniação medular,(C) orifício dural e (D) dura-máter.
Fig. 4 Imagem intraoperatória mostrando fechamento comreconstrução (duroplastia) expansiva do espaço dural utilizando“wrap” com substituto.
Fig. 5 Radiografias pós-operatórias evidenciando a instrumentaçãotranspedicular em T9, T10 e T11. (A) Anteroposterior e (B) Lateral.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hérnia Medular Idiopática Atípica Vieira et al. 125

drenagem e a coagulação de vasos do plexo epidural queapresentavam sangramento de pequena monta, a pacientefoi então encaminhada novamente para a UTI, onde perma-neceu por 1 dia.
Após a cirurgia de revisão, a paciente apresentou fístulaliquórica de baixo débito, com resolução espontânea noterceiro dia após medidas clínicas e tratamento conservadorcom curativo compressivo, repouso no leito, decúbito zero erestrição de volume. A paciente recebeu alta no décimo diapós-operatório após a internação, com resolução da fístula,ferida seca, sem queixas álgicas, mantendo pouca parestesiano trajeto torácico lateral esquerdo, melhora da força motorae da parestesia no membro inferior esquerdo, deambulandosem alterações.
A paciente mantém acompanhamento ambulatorialseriado, com reversão do déficit motor e parestesia nomembro inferior esquerdo já no primeiro retorno em 15dias e reversão da parestesia torácica lateral esquerda após 3meses. A pacientemanteve ainda hiperreflexia patelar 2þ atéo acompanhamento em 1 ano.
O estudo de imagem por ressonância magnética realizado3 meses após o procedimento demonstrou redução docordão medular e movimentação do líquido cefalorraqui-diano na porção lateral esquerda do canal medular (►Fig. 6).
Discussão
A HMI é uma causa rara de mielopatia torácica e muitas vezessub diagnosticada. Sua fisiopatologia exata é desconhecida.Várias teorias foram levantadas: defeito ou erosão dural,secundária a cistos aracnoides, tumores, duplicidade dadura-máter, pós-operatório ou trauma. Sendo que a teoriamais aceita tem sido a descrita por Inoue et al,3 a qual classificaa HMI comoumdefeito dural congênito; segundo os autores, aHMI é mais comum no ápice da cifose torácica, entre os níveisT3-T7, e a herniação em quase todos os casos é voltada para aregião ventral em direção ao disco. Essa teoria ainda propõe
que a abertura de um orifício e a protrusão medular sãofacilitadas pela posição mais anterior da medula no ápice dacifose torácica associada à pulsação liquórica, aosmovimentosdeflexão e extensão, à expansão torácica durante a respiraçãoe aos batimentos cardíacos.3 Como advento de uma protrusãoinicial, a pressão negativa do espaço extradural contribui paraa herniação progressiva e o estrangulamento da medula nasmargens do orifício, levando a uma isquemia medular evolu-tiva, afetando inicialmente o trato o espinotalâmico e poste-riormente o trato córticoespinhal.
Como a localização mais frequente da herniação medular éanterior ou anterolateral, a apresentação clínicamais comum éa Síndrome de Brown-Sequárd progressiva, com cerca de 70%dos casos tendo duração média dos sintomas de 40 meses.2,4,5
Outros pacientes podem apresentar paraparesia, alteraçõesesfincterianas, distúrbios da sensibilidade, dorsalgia e dor nopeito. Esta patologia afeta principalmente adultos de meiaidade compredileção discreta pelo sexo feminino.6 Os achadosclínicose radiológicoscontribuemparaadecisãodaabordagemcirúrgica, que apresenta uma alta taxa de melhora, principal-mente dos sintomas motores, em 80%, e sensitivos, em 35%.7–9
A descrição de casos de HMI na literatura é esparsa. Sum-mers e colaboradores,2 em uma revisão sistemática, identifi-caram 174 casos relatados na literatura, sendo que a grandemaioria deles trata-se de herniações com padrão ventral ouventro-lateral, e apenas um caso dorsal, mas não é descritonenhum caso com herniação lateral pelo forame radicular, oque individualiza o caso relatado no presente trabalho. Nossocaso apresenta uma variação da localização da HMI, umavolumosa herniação do fúniculo lateral em conjunto com araiz de T9pelo forame esquerdo, obliterando a coluna liquóricalateral; por este motivo, associado a sinais clínicos de déficitmotor e mielopatia, foi optado por abordagem cirúrgica.
Várias técnicas são descritas para o tratamento de HMI.Como a grande maioria das apresentações são de padrãoventral, o acesso dorsal é o mais utilizado.10 A estratégiacirúrgica deve ser individualizada para cada paciente. Porém,
Fig. 6 Imagens axiais de ressonância nuclear magnética ponderada em T2 ao nível do disco intervertebral de T9-T10 após 3 meses de cirurgia. Épossível notar a redução da hérnia medular foraminal esquerda.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hérnia Medular Idiopática Atípica Vieira et al.126

independente da causa ou da localização, a proposta básicaserá a redução do volume herniado mantendo a anatomia omais próximo do normal, a fim de evitar recorrência e piorada função neurológica.11,12
Por se tratar de uma HMI lateral, algumas alterações noprocedimento cirúrgico foram necessárias. O acesso se man-teve posterior e mediano. Para chegar ao sítio da herniaçãoentrando pelo forame, os cirurgiões tiveramque realizar umaartrectomia unilateral total de T9-T10, de forma a permitirvisualização da raiz e facilitar na redução, já que a maiorparte do conteúdo extradural encontrava-se foraminal.Como não existia plano de clivagem entre a medula e araiz, não foi possível a dissecção e preservação da raiz, sendooptado pela radiculotomia desta estrutura para atingir a totalredução do volume herniado.
Os casos descritos na literatura são em sua grandemaioriade poucas séries, com relato um a três casos ou revisão daliteratura, não sendo amplamente relatadas as complicaçõese intercorrências mais comuns. A piora do déficit motor e damielopatia são as complicações mais temidas; além dessas,cifose secundária a laminectomia, infecção pós-operatória efístula também podem ocorrer. A recorrência da herniação éextremamente rara, descrita em apenas um caso na litera-tura, com retorno da Síndrome de Brown-Sequard após 10anos da cirurgia corretiva.10
Mesmo apresentando complicações pós-operatórias, apaciente descrita neste artigo evoluiu commelhora do déficitmotor e da sensibilidade já no pós-operatório e no acompa-nhamento em 6 meses, com reversão do déficit motor e daparestesia no membro inferior esquerdo, marcha atípica,resolução da parestesia torácica esquerda, mantendo hiper-reflexia patelar esquerda e com relato de melhora total dossintomas iniciais.
Conclusão
A HMI é uma patologia rara, com variação tanto na localiza-ção da lesão quanto nos sintomas clínicos correspondentes.Neste artigo relatamos um caso atípico de HMI, nunca antesrelatado na literatura, nos obrigando a programar umaabordagem cirúrgica diferenciada. Cabe ao cirurgião decoluna saber identificar e diagnosticar um caso de HMI,tendo em mente que esta pode ter diferentes apresentaçõesclínicas e anatômicas. Sendo assim, a estratégia de manejo
terapêutico e cirúrgico deve ser individualizado, e a aborda-gem cirúrgica, quando necessária, pode levar a resultadosclínicos satisfatórios, compreservação da função neurológicaatravés da correção da lesão envolvida.
Conflitos de interesseDr. Amaral reports personal fees from NuVasisve, outsidethe submittedwork. Dr. Jensen reports personal fees fromNuVasisve, outside the submitted work. Dr. Luiz Pimentareports personal fees from NuVasive, outside the sub-mitted work. All the other authors declare that they haveno conflicts of interest to report.
Referências1 White BD, Firth JL. Anterior spinal hernia: an increasingly recog-
nised cause of thoracic cord dysfunction. J Neurol NeurosurgPsychiatry 1994;57(11):1433–1435
2 Summers JC, Balasubramani YV, Chan PCH, Rosenfeld JV. Idio-pathic spinal cord herniation: Clinical review and report of threecases. Asian J Neurosurg 2013;8(02):97–105
3 Inoue T, Cohen-Gadol AA, Krauss WE. Low-pressure headachesand spinal cord herniation. Case report. J Neurosurg 2003;98(1,Suppl)93–95
4 Nakamura M, Fujiyoshi K, Tsuji O, et al. Long-term surgical out-comes of idiopathic spinal cord herniation. J Orthop Sci 2011;16(04):347–351
5 Batzdorf U, Holly LT. Idiopathic thoracic spinal cord herniation:report of 10 patients and description of surgical approach. J SpinalDisord Tech 2012;25(03):157–162
6 Najjar MW, Baeesa SS, Lingawi SS. Idiopathic spinal cord hernia-tion: a new theory of pathogenesis. Surg Neurol 2004;62(02):161–170, discussion 170–171
7 Parmar H, Park P, Brahma B, Gandhi D. Imaging of idiopathicspinal cord herniation. Radiographics 2008;28(02):511–518
8 Rivas JJ, de la Lama A, Gonza Lez P, Ramos A, Zurdo M, Alday R.[Spontaneous spinal cord herniation]. Neurocir Astur Spain. Out-ubro de 2004;15(05):484–489
9 Sioutos P, Arbit E, Tsairis P, Gargan R. Spontaneous thoracic spinalcord herniation. A case report. Spine 1996;21(14):1710–1713
10 Selviaridis P, Balogiannis I, Foroglou N, Hatzisotiriou A, Patsalas I.Spontaneous spinal cord herniation: recurrence after 10 years.Spine J 2009;9(03):e17–e19
11 Borges LF, ZervasNT, Lehrich JR. Idiopathic spinal cord herniation:a treatable cause of the Brown-Sequard syndrome–case report.Neurosurgery 1995;36(05):1028–1032, discussion 1032–1033
12 Chaichana KL, Sciubba DM, Li KW, Gokaslan ZL. Surgical manage-ment of thoracic spinal cord herniation: technical consideration.J Spinal Disord Tech 2009;22(01):67–72
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hérnia Medular Idiopática Atípica Vieira et al. 127

Hypopituitarism Secondary to an ArachnoidCyst — Case Report
Hipopituitarismo secundário a um cistoaracnoide — relato de caso
Eliezer Abreu Cunha1 Anderson Rodrigo Souza1 Manoel Jacobsen Teixeira1
Eberval Gadelha Figueireido1
1Division of Neurosurgery, Faculdade de Medicina da Universidade deSão Paulo (FMUSP), São Paulo, SP, Brazil
Arq Bras Neurocir 2018;37:128–130.
Address for correspondence Eliezer Abreu Cunha, Divisão deNeurocirurgia, Faculdade de Medicina da Universidade de São Paulo(FMUSP), Av. Dr. Arnaldo, 455 - Cerqueira César, São Paulo, SP, 01246-903, Brazil (e-mail: [email protected]).
Keywords
► arachnoid cysts► hypopituitarism► sellar
Abstract Arachnoid cysts (ACs) are a rare condition of mass effect injury and are usually found inthe Sylvian fissure. However, rarely, they can appear in the sellar area, causingsymptoms of compression. Due to the mass effect, the sellar arachnoid cyst (SAC)may cause headaches, visual disturbances, hypopituitarism, precocious puberty, andthe “bobble-head doll” syndrome.We present the case of JNS, 61 years old, male. The patient presented withhypotestosteronism, hypothyroidism, hypocortisolism and bitemporal hemianopsia.The magnetic resonance imaging scans revealed a mass above the pituitary gland,compatible with a SAC. A surgical excision was performed with removal of the capsuleand fenestration within the subarachnoid spaces for emptying the cyst. After theprocedure, the patient presented great clinical improvement. The rarity of the casecalls attention to the fact that SACs should be thought of as a differential diagnosis incases of hypopituitarism.
Palavras-chave
► cistos aracnoides► hipopituitarismo► selar
Resumo Cistos aracnoides são uma condição rara de lesão de efeito demassa e que comumenteaparecem na região da fissura silviana. No entanto, raramente, podem aparecer naregião selar, ocasionando sintomas de compressão. Devido ao efeito de massa, podemcausar dores de cabeça, distúrbios visuais, hipopituitarismo, puberdade precoce esíndrome da “bobble-head doll. ”Apresentamos o caso de JNS, 61 anos, do sexo masculino. Paciente com hipotestoste-ronismo, hipotiroidismo, hipocortisolismo e hemianopsia bitemporal. As imagens deressonância magnética (RM) revelaram uma massa acima da hipófise, mostrando umcisto aracnoide selar. O paciente foi submetido a excisão cirúrgica com fenestraçãodentro dos espaços subaracnoides para esvaziamento do cisto e apresentou grandemelhora clínica após o procedimento. A raridade deste caso chama atenção para o fatode que o cisto aracnoide selar deve ser considerado como um diagnóstico diferencialem casos de hipopituitarismo.
receivedDecember 1, 2017acceptedJanuary 23, 2018published onlineApril 18, 2018
DOI https://doi.org/10.1055/s-0038-1642605.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de CasoTHIEME
128

Introduction
The arachnoid cyst (AC) is a mass-effect lesion in the centralnervous system. Arachnoid cysts can expand in the spacebetween the pia-mater and the arachnoid membrane (sub-arachnoid space).1 They correspond to� 1% of all intracraniallesions (withmass effect) in adults and� 3% in children, withan occurrence of 5 in 1,000 autopsies.2 In most cases, ACs arepresent at birth (congenital); therefore, they are sometimesalso called primary. The other cases are called secondarycysts. Approximately half of the cases occur in the Sylvianfissure area, and 9% of the cysts are located in the sellar andsuprasellar regions.1,2
Arachnoid cysts, for the most part, are asymptomatic andare usually found during imaging tests. However, due to theirmass effect, they can cause headaches, visual disturbances,hypopituitarism, precocious puberty and “bobble-head doll”syndrome.2 Due to their rarity and symptomatology ofhypopituitarism, it is necessary to report such cases in orderto better understand their physiopathology and surgicaloutcomes.
Case Report
JNS, 61, started the picture with low libido, sexual dysfunc-tion, asthenia, weakness and constipation. The endocrinolo-gist did hormonal dosage, resulting in hypotestosteronism(150 ng/dL) and hypothyroidism (TSH 2.3 µg/dL; FT4I 0.5 ng/dL; T3 55 ng/dL), beginning with hormone replacement. Theendocrinologist ordered magnetic resonance imaging (MRI)one year after the onset of the condition. The MRI scansshowed a sellar arachnoid cyst (SAC) compressing the pitui-tary gland and chiasm. It is important to remember that MRIis the exam of choice for diagnosis of AC.2 Subsequently, hedeveloped laboratorial hypocortisolism (4.2 µg/dL) andvisual disturbance of partial blindness, in which vision ismissing in the outer half of both the right and left visualfields, presenting a clinical picture of hypopituitarism, andbitemporal hemianopsia. Surgical treatment was indicated,and the excision was performed with removal of the capsuleand consequent fenestrationwithin the subarachnoid spacesfor cyst emptying. The result was an improvement in theclinical picture (►Fig. 1A-B and ►Table 1).
Discussion
Due to the rarity of the SAC, it is necessary to discuss thissubject so that it is better understood. Arachnoid cysts, forthe most part, are asymptomatic and are usually foundduring imaging tests. When symptoms occur, they are linkedto the compression of structures by mass effect. The mainlocation of the cysts is in the Sylvian fissure, 49% of the cases,later it is cerebellopontine angle, with 11%; supracolliculararea,with 10%; or vermis, 9%; sellar and suprasellar region, at9%; interhemispheric fissure, with 5%; cerebral convexity, 4%and interpeduncular fossa, 3%.3 In the case of our patient, thelocalization was sellar, which generated the compression ofthe pituitary and the optic chiasm.
There is some discussion about the etiology of SACs. It hasbeen suggested that they develop between the layers of thearachnoid, as well as other intracranial ACs; thus, it wouldoriginate above the diaphragm and expand through itsaperture or would develop from an under-diaphragmaticarachnoid layer.4 Another hypothesis is that it originatesfrom a defective diaphragmatic membrane through whichthere is a herniation of the arachnoid membrane, this defectmay close due to meningitis, inflammation or hemorrhagecreating a non-communicating cyst.5,6
Fig. 1 (A, B) Magnetic resonance imaging scan showing arachnoidcyst with hyposignal at T1 in coronal cut (F1) and sagittal section (F2).Note the compression of the pituitary gland.
Table 1 Dosing og hormones
Hormone At the timeof diagnosis
After thetreatment
Free thyroxine index 0.5 ng/dL 1.6 ng/dL
Total T3 55 ng/dL 93 ng/dL
TSH 2.3 µg/dL 8.2 µg/dL
Cortisol 4.2 µg/dL 14.8 µg/dL
Free testosterone 150 ng/dL 412 ng/dL
Abbreviation: TSH, thyroid stimulating hormone.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hypopituitarism Secondary to an Arachnoid Cyst Cunha et al. 129

Considering that the initial condition was presented withhypopituitarism, the research is done with hormonal dos-age and with imaging exam, which was performed in ourcase. Possible differential diagnoses are tumors that com-press the pituitary gland, pituitary tumors and vascularalterations, such as apoplexy. Compared with other sellarcystic lesions, such as cystic adenomas, craniopharyngiomaand Rathke cyst, SACs are very rare in this location, with fewcases reported.7
Compared with other intracranial ACs, SACs present atlater ages. Headache and visual disturbances are more com-mon to be presented, while endocrine symptoms are lesscommon.5,8,9 The SAC is characterized by a pure cystic lesionwith no contrast enhancement and no calcification and witha typical spontaneous leakage of cerebrospinal fluid, which ishyposignal on T1 and hypersignal on T2-weighted images.10
The patient presented symptoms of hypopituitarism andcompatible imaging exam, showing a rarity in the case dueto a greater rarity of the presented symptoms in relation tothe usual symptoms, that were not perceived.
The surgical indication for SAC is identical to that of anon-secreting adenoma: signs of compression or severeheadache. Transcranial or transsphenoidal pathways, whichis the technique most commonly chosen, can be used toestablish the diagnosis and remove the lesion.7 In this case,there was surgical indication because the patient presentedsigns of pituitary compression. The minipterional pathwaywas selected, and the fenestration was performed, in whichthe AC communicates with the cistern, draining the fluidand preventing the cyst from growing again. The excision ofthe cyst wall and fenestration within the subarachnoidspaces allow direct inspection of the cyst and avoid theplacement of a permanent shunt in some cases. In thepostoperative period, the cyst did not appear on the imag-ing examination and clinical improvement of the symptomswas observed.
Conclusion
Although it is a rare cyst in this location, it is a differentialdiagnosis that must be thought of in cases of sellar lesions aswell as in cases of hypopituitarism, even though the AC rarelycauses endocrine disorders.
Conflict of InterestAuthors declare no conflict of interest.
References1 Murakami M, Okumura H, Kakita K. Recurrent intrasellar ara-
chnoid cyst. Neurol Med Chir (Tokyo) 2003;43(06):312–3152 Zieliński G, Podgórski JK, Koziarski A, Potakiewicz Z. [Intrasellar
arachnoid cyst. A case report and review of the literature]. NeurolNeurochir Pol 2006;40(04):347–352, discussion 353
3 Rengachary SS, Watanabe I. Ultrastructure and pathogenesis ofintracranial arachnoid cysts. J Neuropathol Exp Neurol 1981;40(01):61–83
4 Meyer FB, Carpenter SM, Laws ER Jr. Intrasellar arachnoid cysts.Surg Neurol 1987;28(02):105–110
5 Dubuisson AS, Stevenaert A, Martin DH, Flandroy PP. Intrasellararachnoidcysts.Neurosurgery2007;61(03):505–513,discussion513
6 Hornig GW, Zervas NT. Slit defect of the diaphragma sellae withvalve effect: observation of a “slit valve”. Neurosurgery 1992;30(02):265–267
7 Güdük M, HamitAytar M, Sav A, Berkman Z. Intrasellar arachnoidcyst: A case report and review of the literature. Int J Surg Case Rep2016;23:105–108
8 Shim KW, Park EK, Lee YH, Kim SH, Kim DS. Transventricularendoscopic fenestration of intrasellar arachnoid cyst. Neurosur-gery 2013;72(04):520–528, discussion 528
9 Iqbal J, Kanaan I, Al Homsi M. Non-neoplastic cystic lesions of thesellar region presentation, diagnosis and management of eightcases and review of the literature. Acta Neurochir (Wien) 1999;141(04):389–397, discussion 397–398
10 Elliott RE, Tanweer O, Rubin BA, Koslow M, Mikolaenko I, WisoffJH. Suprasellar hamartoma and arachnoid cyst. World Neurosurg2013;80(06):e401–e407
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Hypopituitarism Secondary to an Arachnoid Cyst Cunha et al.130

Cerebral Proliferative Angiopathy: Case Report
Angiopatia cerebral proliferativa: relato de caso
Luana Antunes Maranha Gatto1 Rodrigo Tavares Brisson2 Zeferino Demartini Jr3 Gelson Koppe4
Carlos Rocha Jr5
1Hospital Universitário Cajuru, Curitiba, PR, Brazi2Division of Neurology, Department of InterventionalNeuroradiology, Hospital Universitário Cajuru, Curitiba, PR, Brazil
3Department of Neurosurgery and Interventional Neuroradiology,Hospital Universitário Cajuru, Curitiba, PR, Brazil
4Department of Interventional Neuroradiology, HospitalUniversitário Cajuru, Curitiba, PR, Brazil
5Department of Neurology, Neurosurgery, InterventionalNeuroradiology, Campo Grande, MS, Brazil
Arq Bras Neurocir 2018;37:131–133.
Address for correspondence Luana Antunes Maranha Gatto, HospitalUniversitário Cajuru, Av. São José, 300 - Cristo Rei, Curitiba - PR, 80050-350, Brazil (e-mail: [email protected]).
Keywords
► intracranialarteriovenousmalformations
► central nervoussystem vascularmalformations
► therapeuticembolization
► endovascularprocedures
Abstract Proliferative angiopathy (PA) is a rare cerebral vascular disease in which anomalousvessels continually recruit additional feeder arteries, amid a functional brain parenchy-ma. We report the case of a young woman with progressive history of headache, motordeficit, seizures and drowsiness. She received a misdiagnosis of brain arteriovenousmalformation (AVM) and evolved with dysarthria and cognitive decline after anunsuccessful embolization performed at another institution. We opted for conserva-tive treatment with periodic control by imaging tests. Proliferative angiopathy differs innatural history, prognosis, histopathology and treatment of the usual AVMs. Endovas-cular procedures aggravate the neurological deficits, which are usually progressive andtend to worsen over time.
Palavras-chave
► malformaçõesarteriovenosasintracranianas
► malformaçõesvasculares do sistemanervoso central
► embolizaçãoterapêutica
► procedimentosendovasculares
Resumo A angiopatia proliferativa (AP) é uma doença vascular cerebral rara em que vasosanômalos recrutam continuamente artérias nutridoras adicionais em um parênquimacerebral normal. Relatamos um caso de umamulher jovem com história progressiva decefaleia, déficit motor, convulsões e sonolência. Ela recebeu um diagnóstico incorretoda malformação arteriovenosa (MAV) cerebral e evoluiu com disartria e declíniocognitivo após uma embolização malsucedida realizada em outra instituição. Optamospelo tratamento conservador com controle periódico por testes de imagem. A APdifere das MAVs usuais em relação a história natural, prognóstico, histopatologia etratamento. Os procedimentos endovasculares agravam os déficits neurológicos, quegeralmente são progressivos e tendem a piorar ao longo do tempo.
receivedOctober 24, 2017acceptedJanuary 23, 2018published onlineApril 17, 2018
DOI https://doi.org/10.1055/s-0038-1642604.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 131

Introduction
Diffuse arteriovenous malformations (AVMs) of the centralnervous system, also called proliferative angiopathy (PA), arelarge lesions that can occupy an entire cerebral hemisphereand causemainly intractable seizures,motordeficits andothersymptoms. In PA, anomalous vessels continue to recruit addi-tional feeder arteries,1 making their architecture, naturalhistory, clinical presentation and treatment distinct fromusual AVMs.2 The cerebral PA is associated with the presenceof a viable cerebral parenchyma, inwhich it differs from usualAVMs and has important implications in the therapeuticdecision in patients with this rare vascular pathology.2,3
Attempts to treat this condition are indicated in extremecases,such as intractable epileptic seizures, for example, althoughwith great risks of aggravating the neurological deficits.2,4Wereport a case of PA in an adolescent, its evolution andmanage-ment regarding clinical and imaging findings.
Case Report
A 15-year-old female patient presented with 5 years of head-ache and progressive right hemiparesis. One year earlier, shehad been admitted at her city’s hospital after generalizedseizure and progressive drowsiness, and that was when shereceived themisdiagnosis of brainAVMthrougha simplebraincomputed tomography (CT). An unsuccessful embolizationwith n-butyl cyanoacrylate was attempted, evolving withcognitive worsening and dysarthria. The patient was referred
to our interventional neuroradiologydepartment presenting aproportionate right hemiparesis (muscle strength grade 4/5),spasticity, postural instability, right ataxia; exacerbated deepappendicular reflexes on the right side (grade 3/4), withplantar cutaneous reflex in extension bilaterally. The cerebraldigital subtraction angiography (DSA) (►Fig. 1) showed thenidus of a bulky vascularmalformation affecting the entire lefthemisphere fed by right anterior, middle and posterior cere-bral arteries, and superficial venous drainage (Spetzler-Martingrade V). No flow or intranidal aneurysmswere identified. Anencephalic magnetic resonance image (MRI) (►Fig. 2) evi-denced an extensive vascular malformation with numerousectasias and “flow void” affecting the entire left hemisphere.We opted for conservative treatment with outpatient follow-up and periodic control by imaging tests.
Discussion
Cerebral PA has been described in a series of cases, predomi-nantly affecting young adult female patients, with onset ofsymptoms, onaverage, at 17years-oldand representing�3.4%of the diagnosed vascular malformations.2 The most commonform of clinical presentation are seizures; other less frequentpresentations areheadache, intracranial hemorrhageand focalneurologicdeficits.2,3,5–8Theusualmorphologyoncerebral CTorMRI is characterizedbydiffusevascular lesions interspersedwith normal brain parenchyma. The DSA of cerebral vesselsdoes not show dominance of a feeder artery; the nidus isgenerally larger than 6 cm with difficult delimitation; and
Fig. 1 Angiography. (a) RICA AP; (b) RICA RAO; (c) LICA AP; (d) LICA Lat; (e) LICA Lat late phase; (f) RVA AP; (g) RVA Lat. Abbreviations: AP,anteroposterior; Lat, lateral; LICA, left internal carotid artery; RAO, right anterior oblique; RICA, right internal carotid artery; RVA, right vertebralartery.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Cerebral Proliferative Angiopathy Gatto et al.132

venous drainage does not have ectasia, in most cases.2,3 In thehistopathological analysis, the lesions are described as anintraparenchymal vascular proliferation, with irregular anddilated arterioles but normal aspect and veinswith thickeningdue to collagen fibers.2 The treatment must be consideredaccording to the characteristics of histological findings. Sincethoselesionsare intermingledwithhealthybrainparenchyma,surgery, radiotherapy and endovascular treatment have notbeen routinely recommended due to the risk of permanentneurologic deficits already described in the literature. Invasivetechniques are reserved for cases of epilepsy and headacherefractory to clinical treatment.2,5,8
According to the literature, after an incorrect diagnosisand an unrecommended embolization, there was worseningof the focal deficits.
Conclusion
The identification of cerebral PA as a distinct entity amongother vascular malformations is extremely important, sinceits natural history, treatment and prognosis are very differ-ent from the usual and more frequent AVM.
Conflict of InterestThe authors declare that there are no conflicts of interest.
References1 Osborn AG. Angiografia Cerebral Diagnóstica; in Revinter 2. ed.
Rio de Janeiro, RJ; 2002:4472 Lasjaunias PL, Landrieu P, Rodesch G, et al. Cerebral proliferative
angiopathy: clinical and angiographic description of an entitydifferent from cerebral AVMs. Stroke 2008;39(03):878–885. Doi:10.1161/STROKEAHA.107.493080
3 Rohit, Goh PS. Diffuse Proliferative Cerebral Angiopathy: A casereport and review of the literature. J Radiol Case Rep 2015;9(09):1–10. Doi: 10.3941/jrcr.v9i9.2402
4 EesaM, Sharma P, Goyal M. Cerebral Proliferative Angiopathy. CanJ Neurol Sci 2009;36(02):242–243
5 Biasi PR, Almeida TAL, Espanhol RA, et al. Cerebral ProliferativeAngiopathy -Description of a Rare Clinical Entity. Arq Bras Neu-rocir 2015;34(01):82–85. Doi: 10.1055/s-0035-1547393
6 Dória-Netto HL, Souza-Filho AM, Dória-Netto RH, et al. Cerebralproliferative angiopathy. Arq Neuropsiquiatr 2010;68(02):300–302. Doi: 10.1590/S0004-282 � 2010000200027
7 Gold JJ, Crawford JR. Acute hemiparesis in a child as a presentingsymptom of hemispheric cerebral proliferative angiopathy. CaseRep Neurol Med 2013;2013:920859. Doi: 10.1155/2013/920859
8 Liu P, Lv X, Lv M, Li Y. Cerebral proliferative angiopathy: Clinical,angiographic features and literature review. Interv Neuroradiol2016;22(01):101–107. Doi: 10.1177/1591019915609784
Fig. 2 Resonance with extensive ectasias and “flow void” throughout theleft hemisphere. (a) axial T1 with contrast; (b) sagittal T1; (c) coronal T2.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Cerebral Proliferative Angiopathy Gatto et al. 133

Neuroparacoccidioidomycosis: Case Report andLiterature Review
Neuroparacoccidioidomicose: relato de caso e revisão daliteratura
Marcus Vinicius de Morais1 Sérgio Murilo Georgeto2 Marcelo Lourenço Haddad2
José Guilherme da Silva Amorim2 Luis Guilherme Scaliante2 Anderson Luiz de Paula2
Igor Vasconcelos de Andrade2 Paulo Henrique Pires de Aguiar3
1Division of Neurosurgery, Hospital Militar de Área de São Paulo, SãoPaulo, SP, Brazil
2Division of Neurosurgery, Santa Casa de Londrina Hospital, Londrina,PR, Brazil
3Division of Neurology, Pontifícia Universidade Católica de São Paulo,Sorocaba, SP, Brazil
Arq Bras Neurocir 2018;37:134–139.
Address for correspondence Marcus Vinicius de Morais, HospitalMilitar de Área de São Paulo, R. Ouvidor Portugal, 230 - VilaMonumento, São Paulo, SP, 01551-010, Brazil(e-mail: [email protected]).
Keywords
► paracoccidio-idomycosis
► central nervoussystem
Abstract Introduction Paracoccidioidomycosis (PCM) is a systemic mycosis caused by thefungus Paracoccidioides brasiliensis, and it can compromise the central nervous system(CNS) in 10–27% of all cases.Case Report A 31-year-old man presented to the Emergency Department withheadache, left-sided weakness, clonus at the ankle and a positive Babinski sign.Head computed tomography (CT) and magnetic resonance imaging (MRI) scansshowed a 5.1 � 3.8 cm lobulated lesion with areas of liquefaction in the right centrumsemiovale.Discussion Central nervous system PCM canmimic a brain tumor, and most cases arediagnosed by biopsy of the lesion. The treatment includes antibiotics, but some casesrequire surgery.Conclusion Due to high morbimortality rates, the diagnosis must be considered, andearly treatment started in patients who live in rural regions endemic for PCM when aring-enhancing mass associated with perilesional edema is observed on MRI scans.
Resumo Introdução Paracoccidioidomicose (PCM) é uma micose sistêmica causada pelofungo Paracoccidioides brasiliensis e que pode comprometer o sistema nervoso central(SNC) em 10–27% dos casos.Relato de caso Um homem de 31 anos é admitido no pronto socorro com cefaleia,hemiparesia esquerda com clonus e presença de sinal de Babinski. As imagens datomografia computadorizada (TC) de crânio e da ressonância nuclear magnética (RNM)demonstraram uma lesão de 5,1 � 3,8 cm no centro semioval direito de aspectolobulado com áreas de liquefação no centro semioval direito.
receivedJanuary 29, 2018acceptedFebruary 27, 2018published onlineApril 4, 2018
DOI https://doi.org/10.1055/s-0038-1641578.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de CasoTHIEME
134

Introduction
Paracoccidioidomycosis (PCM) is a systemic mycosis andchronic granulomatous disease caused by Paracoccidioidesbrasiliensis, an aerobic and thermally dimorphic fungus. It isacquired by inhalation and can virtually affect any organ. Thecentral nervous system is compromised in 10–27% of allcases.1–7 Neurological symptoms can take place before,simultaneously or after systemic symptoms, and they rangefrom headaches, cranial nerve and motor deficits to seizuresand intracranial hypertension, depending on the location ofthe lesion.1,2,4,5 Paracoccidioidomycosis is themost frequentendemic systemic mycosis in Latin America, especially inBrazil, accounting for � 80% of all registered cases.4,7–9
Case Report
A 31-year-old man presented to the emergency departmentwith headache and left-sided weakness with clonus at theankle and a positive Babinski signal. The patient referred13 days of symptoms and no previous surgery, nor hospitali-zation. He lived in a rural area, and he was a bricklayer. Theemergency noncontrast computed tomography (CT) was sug-gestive of right centrum semiovale lesion and importantperilesional edema. The magnetic resonance imaging (MRI)scans showed a 5.1 � 3.8 cm lobulated lesion with areas ofliquefaction and low intensity on gradient echo T2 sequence.The white matter and basal ganglia adjacent to the lesionpresented a high intensity extending to the right-sided mes-encephalon and brainstem. The patient underwent microsur-gical resectionof thelesionwithout intercurrences.Onthefirstpostoperative day, he presented dilated pupils, no brainstemreflexes and died on the second day after surgery. The biopsywas positive for central nervous system (CNS) PCM.
Discussion
Paracoccidioidomycosis is a systemic mycosis and an en-demic disease in Latin America, with an estimated number of10 million affected individuals. Brazil represents� 80% of allcases reported. In one study, anti-P. brasiliensiswas detectedin 27% of Brazilian blood donors.10 The mycosis affectsprimarily white and middle-aged people ranging from 20to 40 years. It is more prevalent in men than women, andmore common in rural areas and in rural workers.1–4,7–11
Some authors suggest that the gender difference could beexplained by an estrogenic inhibitory action on the fungustransformation process.2
Paracoccidioidomycosis is also known as South Americanblastomycosis, but the terminology is not correct because thedisease is not restricted to South America. This termmay alsocause confusion in the international literature with blastomy-cosis, which is another disease.9 Paracoccidioidomycosis iscaused by P. brasiliensis, a thermally dimorphic and aerobicfungus. At environmental temperature, it is a mold, a saprobicmycelial form that produces slow-growing colonies withchlamydospores visible under the microscope. These micro-scopic structures are the infectious form of the fungus. Thepathogenic agent has been apparent as an oval-to-round yeastcell in mammalian tissues hosts and cultures under thetemperature of 37°C. Themicroscopic aspect of thepathogenicform is the classic “pilot wheel.” The mycosis is acquired byinhalation of the chlamydospores, which transform into theyeast formin thepatient’s body. Since thehosthouses theyeastform, PCM is not contagious from person to person.1–3,7,10
There are two main clinical forms of PCM. The acute/subacute form, also called juvenile type, is more common inchildren and young adults. It is an extra-pulmonary diseasewith lymphohematogenous dissemination and affects themononuclear phagocytic system.1,7,8,11,12Due to progressivefungal dissemination and reticuloendothelial system organhypertrophy, the disease ismore aggressive andmay presenthigh mortality rates.1,3 The symptoms generally appear in 4to 12 weeks, and the most common ones are lymphadenop-athy, digestive manifestations, hepatosplenomegaly and,mainly, skin and bone lesions. The juvenile type represents3–5% of PCM cases.7,8 The chronic form, also known as adulttype, accounts for more than 90% of all cases. It occurs asreactivation of quiescent foci or as an exogenous reinfectionin a male to female ratio of 10–15:1.1,7,11,12 In the chronicform, the fungus can virtually compromise any organ and themost affected ones are lymph nodes, adrenal gland, liver,bones, but primarily the lungs, mucousmembranes and skin.Chronic PCM generally involves more than one organ simul-taneously and presents insidious symptoms. In some cases, itmay only be diagnosed years after the infection.1–5,7,9,11,12
Diagnosis is confirmed by mycological exams (culture, his-topathologic and cytopathology exams) and serological tests(the most relevant is gp43 serum marker).2,4,7,9,10 It isimportant to note that the symptoms pattern is differentin patients with coinfection of PCM and HIV, making diag-nosis more challenging.7,11
Neuroparacoccidioidomycosis (NPCM) accounts for 10–36%of all PCMcases and it is even rarer in females. Considering justtheneurologic involvementof thePCM, themaleto female ratio
Discussão Paracoccidioidomicose do SNC pode simular um tumor cerebral, sendo amaioria dos casos diagnosticada por biopsia da lesão. O tratamento inclui antibióticos,mas alguns casos necessitam de abordagem cirúrgica.Conclusão Devido à alta morbimortalidade, o diagnóstico deve ser considerado e otratamento precoce iniciado em pacientes que vivem em áreas rurais endêmicas paraPCM e que apresentam lesão com captação anelar de contraste associada a edemaperilesional nas imagens de RNM.
Palavras-chave
► paracoccidio-idomycosis
► sistema nervosocentral
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Neuroparacoccidioidomycosis Morais et al. 135

is 23:1.2,4,5,9,13 In� 21% of the cases, the onset of neurologicalsymptomatology takesplacebefore systemic symptoms, in33%it appears simultaneously, and in 46% it starts after systemicmanifestations.13 Exclusive meningeal involvement is consid-ered rare inNPCM, althoughmeningeal extension is not so rarein somecase series.6 Somecase series reportmortality rates forNPCM up to 53%.9 Considering the affected areas, two mainclinical presentations are described by some authors:1,3 men-ingitis and pseudotumoral forms. The latter represents 90% ofcases andmaybecausedbysingle ormultiplegranulomaswiththepresenceofP. brasiliensis. These lesions are surroundedbyathick capsule and generally exhibit a central necrotic areawhere the fungus can be found. Reactive gliosis is observedin the neighboring parenchyma, causing the thick capsuleobserved in NPCM. These capsules do not allow free bloodaccess, which reduces natural defenses.3,14Granulomas can befound in the spinal cord, brainstem, cerebellum, ventricles, andcerebral hemispheres. Some authors cite the cerebral hemi-spheres as the most common place of PCM granulomas due tohematogenous dissemination in the CNS.1,5,6,9,13 The percen-tages vary extremely according to authors, with supratentoriallesionsbeingreportedfrom47–100%ofcasesand infratentoriallesions from 21–42.4% of cases. Simultaneously supra- andinfratentorial involvement varied from 23–37.5% of all cases.Multiple parenchymal lesions accounts for23–75%ofcases andthe number of lesions ranges from 1 to 10.1–3,5,6,8,9,13,15,16
Leptomeningeal and/or pachymeningeal involvement repre-sent themeningealpresentation,and itmanifestsbymeningealsigns. Spinal cord involvement is rare and accounts for 0.6% ofall cases of PCM and 4% ofNPCM. Themost frequently involvedspinal cord levels are thoracic, in 58%, cervical, in 25%, and bothin 8% of cases.1,6,8,13
The symptoms vary depending on the location of thelesion. Different authors suggest different main symptom-atology. The most common manifestation cited in the litera-ture are motor symptoms and signs (� 50% of cases),intracranial hypertension (near 50% of cases), seizures (ina quarter of all cases), cerebellar symptoms and signs (in20–25% of cases) and paresthesia and cognitive symptoms(in� 20% of cases). Medullary symptoms and signs representless than 10% of cases, and their clinical features suggesttransverse myelitis, spinal cord compression, and signsof spinal root compression or conus medullaris involve-ment. Some authors also cite weight loss in 46.1% ofcases.1–6,8,9,13,16,17 One case series study reported a highmorbidity among patients with NPCM, with � 63% of thepatients developing sequelae in the follow-up: 60% of themremained with sensitive deficits, 40% with motor deficits orseizures and 20% with gait disturbances.16
The radiologic evaluation of NPCM is based on contrast-enhanced head CT andMRI scans. There is no pattern for CT inNPCM. One study suggests that granulomatous or pseudotu-moral presentations have a biphasic CT aspect based on thelength of the disease. Images obtained before 5 months ofsymptoms have single or multiple round lesions presentinghypodense signal, ring-enhancement after contrast, andfainted perilesional edema with or without hydrocephalus.After 5 months, lesions may present a hyperdense signal and
ring-like contrast enhancement. The granulomas mean size is23 mm(range12–45mm).3Other authors alsodepictdifferentCT scan patterns. Some less frequent are multiloculated orcalcified lesions, in which ring enhancement and intralesionalseptation may also be present. No bone lesions were found inNPCM.1–3,5,15,18 A study with 1 and 2-year CT scan follow-updemonstrated that nearly a third of the lesions were calcifiedafter 23 months. This work also described that the size andedema intensity were the first signs to improve under treat-ment.8 Due to the lack of typical and characteristic features, afungalgranuloma inCTscancanmimicor bemisdiagnosed asaglioma, tuberculoma, lymphoma,meningioma, cholesteatoma,metastasis, pyogenic and non-pyogenic abscesses, infarct in asubacute phase, or resolving hematoma.3,5,18 Magnetic reso-nance imaging is also important forNPCMevaluation, since it isthe bestmethod to analyzemeningeal or parenchymal lesions.The granulomas in MRI are lesions with peripheral hyperin-tense signal on T1WI and hypointense signal in T2WI in mostcases. Some lesions may present hypo-to-isointense on T1WI.Necrosis and ring enhancement is found in most cases, butheterogeneous enhancement is also possible. Magnetic reso-nance spectroscopy may demonstrate lipid peaks. Restricteddiffusion isnotexpected. Enhancing lesions inpost-gadoliniumin T1WI may persist in the first few months.1,5,6,14,18–20
Very few authors analyzed the cerebrospinal fluid (CSF)alterations in NPCM. In one study, liquor analysis and culturewere performed in 17 patients, but there were no conclusivefindings.3 In another study, five patients underwent lumbarpuncture for CSF analysis. A double-immunodiffusion testpresented positive titers of 1:64 in only one of them.8 In asystemic review, liquor analysis contributed in diagnosis byimmunological tests in 16.3% of cases, direct microscopicexamination in 1.9% and CSF culture in 1.2%.5 Other authorsalso suggest that looking for the fungus is time consuming,not efficient, and rarely positive.2,13 The CSF is usually limpidand presents normal pressure during lumbar puncture. Totalprotein (TP) may be normal or elevated up to 200 mg/dL.2,5
Increased CSF TP was found in 61% of patients in one study.Gammaglobulin was also at higher levels in 63% of cases.2
Authors report low or normal levels of glucose.2,5 Enzymelinked immunosorbent assay (ELISA) anti-gp43 was positivein 89% of the CSF samples in one study, but other authorsnoted that gp43 cross-reacts with serum from patients withaspergillosis and histoplasmosis.21,22
In sum, when systemic PCM is not already diagnosed,NPCM is not part of the differential diagnosis and is con-firmed after CNS biopsy. It confirmed the diagnosis in 35%–92.3% of cases. Patients underwent stereotaxic or opensurgery biopsy.3,5,9
For moderate or severe cases of PCM, in which NPCM isincluded, the recommended treatment consists in two parts:the first one is an induction phase until the acute phaselaboratory parameters return to normal and the clinicalsymptoms are controlled. The second step is the mainte-nance phase. Usually, the induction phase is based onintravenous drugs and once the treatment achieves themaintenance phase, it can be changed to oral drugs.12 Theduration of the treatment depends on the clinical response,
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Neuroparacoccidioidomycosis Morais et al.136

but some authors suggest schemes lasting from 12 to84 months, ceasing medication in the absence of diseaseactivity and upon improvement of clinical, laboratory andradiological conditions.1,2,4,5,8,9,12 The treatment is based onanti-P. brasiliensis drugs, andmost studies report sulfameth-oxazole-trimethoprim (SMZ-TMP) association as first thera-peutic option, combined or not with fluconazole.Amphotericin B (AmB) was used by some authors in theinitial treatment of severe cases.2,4,8,12,16
Sulfamethoxazole-trimethoprim has adequate CSF levels,but itsmaindisadvantage is the need for long-term treatmentsin moderate to severe cases, surpassing 12 months. Some ofthe recommended posology is 480–960 mg every 8–12 hours,andseverecasesmaydemandhigher intravenousdosesduringthe induction phase. Due to a theoretical possibility of resis-tance to SMZ-TMP and the good CNS penetration of flucona-zole, a study suggests the use of this drug in association withSMZ-TMP. Fluconazole is also recommended when hepaticenzymes are elevated or there is any intolerance to sulfas orAmB. The recommended dose for fluconazole is 200 mg/dayuntil the end of treatment.8,12
The starting dose of AmB ranges from 5–10 mg/day, but itcan be increased to 1 mg/kg/day, if necessary, in severe casesof NPCM. Although it is a highly active fungistatic andfungicidal compound, some authors describe low drug levelsin CNS, and therefore suggest administering it intrathecallywhen there is no response to the intravenous therapy. Ifprescribed intrathecally, it is necessary to also administerhydrocortisone (25–30 mg or the equivalent dose of dexa-methasone) to avoid arachnoiditis.8,12 Other antifungaldrugs considered by various authors are voriconazole anditraconazole.2,4,5,8,9,12,16,23
Table 1 Patients data from literature review of Neuropara-coccidioidomycosis
Data Quantity (%)
Total cases reported 44 (100)
Sex
Male 39 (88.6)
Female 5 (11.4)
Symptoms
Headache 24 (54.5)
Cerebellar symptoms 15 (34.1)
Hemiplegia or hemiparesis 13 (29.5)
Ocular motility or visual deficits 10 (22.7)
Intracranial hypertension 9 (20.4)
Generalized seizure 9 (20.4)
Consciousness alterations 9 (20.4)
Speech deficits 5 (11.4)
Sensitivity deficits 4 (9.1)
Meningism 3 (6.9)
Spinal cord compression symptoms 3 (6.9)
Focal seizure 1 (2.3)
Cervical pain 1 (2.3)
Fever 1 (2.3)
Time of symptoms onset (months)
One or less 13 (29.5)
Two or more 8 (18.2)
Not informed 21 (47.7)
Primary site of PCM
Oral 6 (10.2)
Skin 9 (15.3)
Lungs 25 (42.4)
Others 4 (6.8)
Not informed or not identified 15 (25.4)
Associated comorbidity
HIV 2 (4.5)
Lesion location
Supratentorial 29 (48.3)
Infratentorial 28 (46.7)
Spinal cord 3 (5)
Lumbar puncture
Patients submitted tothe procedure
9 (20.5)
Diagnosis confirmed by CSF 4 (9.1)
Antibiotic treatment
Sulfamethoxazole/Trimethoprim 27 (41.5)
Amphotericin B 13 (20)
Sulfadiazine 12 (18.5)
(Continued)
Table 1 (Continued)
Data Quantity (%)
Itraconazole 5 (7.7)
Ketoconazole 3 (4.6)
Ampicillin 1 (1.5)
Chloramphenicol 1 (1.5)
Intrathecal Amphotericin B 1 (1.5)
Fluconazole 1 (1.5)
Antituberculosis drugs 1 (1.5)
Morbimortality
Death 7 (15.9)
Hemiplegia or hemiparesis 6 (12.8)
Sensitivity alterations 3 (6.4)
Visual deficits 2 (4.3)
Seizure 2 (4.3)
Spinal cord injury 2 (4.3)
Cerebellar complications 1 (2.1)
Abbreviations: CSF, cerebrospinal fluid; HIV, human immunodeficiencyvirus; PCM, paracoccidioidomycosis.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Neuroparacoccidioidomycosis Morais et al. 137

There are some discussions over the usage of corticoste-roids forPCMandNPCM.Therationale for their use is to reducethe inflammatory response, which may be harmful if notchecked. Although previously not recommended, a recentstudy24 described the use of corticosteroids adjunct therapy(aCST) for some NPCM cases. The drugs usedwere prednisoneand dexamethasone. The dose for the former was 1mg/kg/dayfor 10 days and then tapered off until removal, within 30 days.The dose for dexamethasone was 16 mg/day for 6 days andthen tapered off in 7 days. Dexamethasone can be prescribedfor oral intake or intravenous administration. Hydrocortisoneis also cited as a good alternative. It is important to note thenecessity to rule out subclinical associated infections, such astuberculosis and strongyloidiasis, which may become severeand disseminated with corticotherapy. The authors of thisstudy also depicted that microbiological response to the anti-fungals remain unaffected during aCST. Another study notedthat PCMis a commoncauseof adrenal insufficiency, thereforerequiring corticosteroid administration due to stress or infec-tion episodes that can induce life-threatening conditions.12,24
Surgical intervention may be necessary if the patientpresents elevated intracranial pressure caused or not byhydrocephalus,presenceofmasseffect causedbyagranuloma,unresponsive clinical treatment, or progressive spinal cordcompression.1,2,24
Case reports about NPCM are growing over the years, andmost data are recent, showing the importance of the diseasein the differential diagnosis when the patient meets riskfactors and epidemiology. As a literature review, for thispaper we also searched the keywords “neuroparacoccidioi-domycosis” and “central nervous system paracoccidioido-mycosis” in PubMed and selected the case series reportspublished since 1998 that included these terms. There were24 reports, but 6 were excluded due the lack of specific andindividualized information about the cases. The 18 reportsleft provided 44 cases.1,4,16,17,23,25–37 The information avail-able were categorized and the results are in ►Table 1.
Inconclusion,NPCMisararediseasewithabroaddifferentialdiagnosis in imaging.Due itshighmorbidityandmortality rates,NPCMshouldbe considered inpatientswho live in rural regionsendemic for PCMwhen a ring-enhancing mass associated withperilesional edema is observed on MRI scans. Early diagnosisand treatmentare important to reduce thedevastatingeffectsofthe disease. Sulfamethoxazole-trimethoprim associated withfluconazole appears to be a feasible treatment option. Ampho-tericin B should be considered in severe cases, and aCST canpotentially help in themanagement of these situations. Surgerymust be considered depending on lesion location and patient’sclinical and neurological conditions.1,3–6,8,9,16,24
Conflicts of InterestThe authors declare that there are no conflicts of interest
References1 Elias J Jr, dos Santos AC, Carlotti CG Jr, et al. Central nervous
system paracoccidioidomycosis: diagnosis and treatment. SurgNeurol 2005;63(01, Suppl 1):S13–S21, discussion S21
2 de Almeida SM. Central nervous system paracoccidioidomycosis:an overview. Braz J Infect Dis 2005;9(02):126–133
3 Gasparetto EL, Liu CB, de Carvalho Neto A, Rogacheski E. Centralnervous system paracoccidioidomycosis: imaging findings in 17cases. J Comput Assist Tomogr 2003;27(01):12–17
4 Isolan GR, Vieira DM,Hehn F, Antunes AC. Paracoccidioidomycosissimulating brain tumor. Surg Neurol Int 2014;5(05):134
5 Pedroso VSP, Vilela MdeC, Pedroso ERP, Teixeira AL. [Paracocci-dioidomycosis compromising the central nervous system: asystematic review of the literature]. Rev Soc Bras Med Trop2009;42(06):691–697
6 Reis F, Collier PP, Souza TF, et al. Neuroparacoccidioidomycosis(NPCM): magnetic resonance imaging (MRI) findings. Myco-pathologia 2013;175(1-2):181–186
7 Shikanai-Yasuda MA, Telles Filho FdeQ, Mendes RP, Colombo AL,Moretti ML. Guidelines in paracoccidioidomycosis. Rev Soc BrasMed Trop 2006;39(03):297–310
8 Francesconi F, da Silva MT, Costa RL, et al. Long-term outcome ofneuroparacoccidioidomycosis treatment. Rev Soc Bras Med Trop2011;44(01):22–25
9 Fagundes-PereyraWJ,CarvalhoGT,GóesAM,dasChagasLimaeSilvaF, de Sousa AA. Central nervous system paracoccidioidomycosis:analysis of 13 cases. Arq Neuropsiquiatr 2006;64(2A):269–276
10 Maluf MLF, Pereira SRC, Takahachi G, Svidzinski TIE. Prevalence ofparacoccidioidomycosis infection determined by sorologic test indonors’ blood in theNorthwest of Paraná, Brazil. Rev Soc BrasMedTrop 2003;36(01):11–16
11 Almeida FA, Neves FF, Mora DJ, et al. Paracoccidioidomycosis inBrazilian Patients With and Without Human ImmunodeficiencyVirus Infection. Am J Trop Med Hyg 2017;96(02):368–372
12 Shikanai-YasudaMA. Paracoccidioidomycosis Treatment. Rev InstMed Trop São Paulo 2015;57(19, Suppl 19):31–37
13 de Almeida SM, Queiroz-Telles F, Teive HAG, Ribeiro CEL,WerneckLC. Central nervous system paracoccidioidomycosis: clinical fea-tures and laboratorial findings. J Infect 2004;48(02):193–198
14 da Rocha AJ, Maia ACM Jr, Ferreira NPDF, do Amaral LLF. Granu-lomatous diseases of the central nervous system. TopMagn ResonImaging 2005;16(02):155–187
15 Rodacki MA, De Toni G, Borba LA, Oliveira GG. Paracoccidioido-mycosis of the central nervous system: CT findings. Neuroradiol-ogy 1995;37(08):636–641
16 Pedroso VSP, Lyon AC, Araújo SA, Veloso JMR, Pedroso ERP,Teixeira AL. Paracoccidioidomycosis case series with andwithoutcentral nervous system involvement. Rev Soc Bras Med Trop2012;45(05):586–590
17 França MC Jr, de Castro R, Balthazar MLF, Faria AV, Cendes F. Focalstatus epilepticus as the first manifestation of paracoccidioido-mycosis. Eur J Neurol 2005;12(01):73–74
18 NaikV, AhmedFU,GuptaA, et al. Intracranial Fungal Granulomas:ASingle Institutional Clinicopathologic Study of 66 Patients andReviewof theLiterature.WorldNeurosurg2015;83(06):1166–1172
19 Magalhaes AC, Caramelli P, Silva ED, et al. Magnetic resonanceimaging in intracranial paracoccidioidomycosis. J Neuroimaging1993;3(04):216–219
20 Jorge LA Jr, Yamashita S, Trindade AP, et al. Pseudotumoralneuroparacoccidioidomycosis of the posterior fossa: A case reportand review of the literature. Surg Neurol Int 2017;8(08):76
21 Sandhu GS, Aleff RA, Kline BC, da Silva Lacaz C. Molecular detectionand identification of Paracoccidioides brasiliensis. J Clin Microbiol1997;35(07):1894–1896
22 de Almeida SM, Queiroz-Telles F, Doi EM, Ono M, Werneck LC.Anti-gp43 antibodies in the cerebrospinal fluid of patients withcentral nervous system involvement by paracoccidioidomycosis.Am J Clin Pathol 2002;118(06):864–868
23 Villa LA, Tobón A, Restrepo A, et al. Central nervous system para-coccidioidomycosis. Report of a case successfully treated withitraconazol. Rev Inst Med Trop São Paulo 2000;42(04):231–234
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Neuroparacoccidioidomycosis Morais et al.138

24 Benard G, Campos AF, Netto LC, et al. Treatment of severe forms ofparacoccidioidomycosis: is there a role for corticosteroids? MedMycol 2012;50(06):641–648
25 do Valle ACF, Skacel M, Costa RLB, Ribeiro CT, Montagna NA, daCruz LCH. A case report of intraspinal paracoccidioidomycosis.Rev Inst Med Trop São Paulo 1998;40(03):203–207
26 Silva-Vergara ML, Rocha IH, Vasconcelos RR, et al. Central nervoussystem paracoccidioidomycosis in an AIDS patient: case report.Mycopathologia 2014;177(1-2):137–141
27 Pereira GH, Lanzoni VPB, Beirão EM, Timerman A, Melhem MdeS.Disseminated Fungal InfectionWith Adrenal Involvement: Reportof Two Hiv Negative Brazilian Patients. Rev Inst Med Trop SãoPaulo 2015;57(06):527–530
28 Corti M, Trione N, Risso D, et al. Disseminated paracoccidioido-mycosis with a single brainstem lesion. A case report and litera-ture review. Neuroradiol J 2010;23(04):454–458
29 Teive HAG, Zanatta A, Germiniani FMB, Almeida SM, Werneck LC.Holmes’ tremor and neuroparacoccidioidomycosis: a case report.Mov Disord 2002;17(06):1392–1394
30 FinamorLP,Muccioli C,MartinsMC,RizzoLV,Belfort R Jr.Ocular andcentral nervous system paracoccidioidomycosis in a pregnantwomanwith acquired immunodeficiency syndrome. Am JOphthal-mol 2002;134(03):456–459
31 Teixeira MJ, Fonoff ET, Machado LdosR, Nóbrega JPS, Sterman-Neto H, Amorim RL. Paracoccidioidomycosis: intralesional ther-apy. Arq Neuropsiquiatr 2010;68(03):458–459
32 Lorenzoni PJ, Chang MR, Paniago AMM, Salgado PR. Paracocci-dioidomycosis meningitis: case report. Arq Neuropsiquiatr 2002;60(04):1015–1018
33 da Silva CE, Cordeiro AF, Gollner AM, Cupolilo SMN, Quesado-Filgueiras M, Curzio MF. Paracoccidioidomycosis of the centralnervous system: case report. Arq Neuropsiquiatr 2000;58(3A):741–747
34 Rojas-Jaimes J, Castillo Cordova R, Tárraga Gonzales D. Paracocci-diomicosis in the central nervous system: a case report. Rev PeruMed Exp Salud Publica 2015;32(01):183–186
35 dos Santos VM, Xavier RM, Cortes JA, Osterne EMC, de WorischFerreira Lopes M. Pseudotumoral neuroparacoccidioidomycosis:one case report. Mycopathologia 2008;166(03):155–158
36 Duarte ALWP, Baruffa G, Terra HBG, Renck DV, de Moura D,Petrucci C. [Systemic paracoccidioidomycosis with central ner-vous system involvement]. Rev Soc Bras Med Trop 1999;32(04):439–442
37 Lambertucci JR, Lana-Peixoto MA, Pitella JEH. [Paracoccidioido-mycosis of the central nervous system]. Rev Soc Bras Med Trop2001;34(04):395–396
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Neuroparacoccidioidomycosis Morais et al. 139

Intramedullary Dermoid Cyst of the CervicalSpinal Cord – C5–C7 Level
Cisto dermoide intermedular da medula espinhalcervical – nível C5–C7
Palanisamy Seerangan1 Aravinth Kumar Ashok1 Jolarpettai Venugopal Mahendran1
1 Institute of Neurosurgery, Madras Medical College, Chennai,Tamil Nadu, India
Arq Bras Neurocir 2018;37:140–144.
Address for correspondence Jolarpettai Venugopal Mahendran, PhD,Institute of Neurosurgery, Madras Medical College, Park Town,Chennai, Tamil Nadu 600003, India(e-mail: [email protected]).
Keywords
► intramedullarydermoid cyst
► cervical spinal cord► rare presentation► absence of spinal
dysraphism
Abstract Introduction Inclusion cysts of the spinal cord are rarely intramedullary. Such cystsare commonly located in the lumbar and thoracic regions and are usually associatedwith congenital spinal dysraphism and dermal sinus. Intramedullary dermoid cysts inthe cervical region without spinal dysraphism are extremely rare. To our knowledge,only seven such cases are reported in the literature to date.Materials and Methods An 18-year-old female patient presented with weakness in allfour limbs, more distal than proximal muscle weakness, that had been progressing for3 years. The magnetic resonance imaging (MRI) showed an intramedullary lesion fromC5– C7with peripheral ring enhancement. “Whorls”were observedwithin the lesion onT2 weighted image, with associated excavation of vertebral bodies C5– C7. Operativeprocedure and findings: partial laminectomy of C5– D1was performed. The dura wasopened. A small myelotomy wasmade in the root entry zone. About 1.5ml of yellowishcolored fluid was drained. White shiny debris with hair, whitish pultaceous content andteeth were removed. Complete excision of cyst and its wall was performed.Results The histopathological examination revealed that the cyst wall was lined bystratified squamous epithelium with underlying dermis showing hair follicles, sebaceousglands, adipose tissue and cyst filled with keratin debris suggestive of dermoid cyst.Conclusion The intramedullary location of the dermoid cyst in the cervical cord andthe absence of any congenital spinal dysraphism make this case a very unique and rareentity and warrants its inclusion in the reported cases of rare intramedullary spaceoccupying lesions.
Resumo Introdução Cistos de inclusão da medula espinhal raramente são intramedulares.Tais cistos são comumente localizados nas regiões lombares e torácicas e geralmenteestão associados com disrafismo espinhal congênito e sinus dérmico. Cistos dermoidesintramedulares na região cervical sem a presença de disrafismo espinhal são extrema-mente raros. Apenas sete casos foram relatados na literatura até a data do presenteestudo.
receivedNovember 23, 2017acceptedJanuary 5, 2018published onlineMarch 27, 2018
DOI https://doi.org/10.1055/s-0038-1639605.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de CasoTHIEME
140

Introduction
Inclusion cysts of the spinal cord are rarely intramedullary,with only a few cases having been reported in the literature.Intraspinal dermoid cysts are commonly located in thelumbar and thoracic regions and are usually associatedwith congenital spinal dysraphism and dermal sinus. Intra-medullary dermoid cyst in the cervical regionwithout spinaldysraphism (►Fig. 1) is extremely rare,with only seven casesbeing reported in the literature to date.We report a case of anintramedullary dermoid cyst in the cervical cord of an 18-year-old female patient.
Presentation
Our patient was an 18-year-old female, who presented withgradual progressiveweakness ofmuscles of both upper limbsand both lower limbs, weakness of the distal limb muscles,more than the proximal muscle group, ongoing for 3 years inthe form of difficulty in holding objects, mixing food, anddifficulty in walking, climbing, squatting on the floor, etc.
Upon examination, power in the upper limbs was⅗ on theright side and ⅘ on the left side with weakness of hand grip(right-20%, left-30%). In the upper limbs, the triceps andsupinator reflexeswere absent. The power in both lower limbswas ⅘ and with spasticity, and the patient was able to walkwith difficulty. The plantar reflex was extensor bilaterally,with exaggerated ankle and knee jerks and the patient alsosustained clonus of both ankles. There were no sensorychanges in theupper and lower limbs, or in the restof thebody.
The MRI of the cervical spine with contrast study showedwidening of the cervical spinal cord fromC5–C7 (►Fig. 2). Anintramedullary space occupying lesion was present, whichwas hypo intense onT1weighted images, hyper intense onT2weighted images, and with peripheral ring enhancement oncontrast study. Also, “whorls”were seenwithin the lesion on
T2 weighted images (►Fig. 3). There was associated excava-tion of the cervical vertebral bodies in the C5–C7 levels.
Operative Technique
The patient was operated under general anesthesia in proneposition. An intraoperative injection of methyl-prednisolonewas given and continued in the postoperative period for23 hours at a dose of 30 mg/kg bolus over 1 hour followed by5.4 mg/kg/hr for 23 hours. Amidline incision extending fromjust below C2– D1 was made. The paraspinal muscles wereretracted laterally by sub periosteal dissection. A partiallaminectomy of C5, C6, C7 and D1 was performed.
After laminectomy, the cervical dura was found to bebulging and enlarged. The dura was opened in the midlineand retracted by stay sutures. The cord was enlarged, and alow-grade torsionwas noted. A smallmyelotomywasmade inthe root entry zone, initially. About 1 to 1.5 ml of yellowishcolored fluid was drained. The myelotomy was subsequentlyextended rostrally and caudally. White shiny debris with hair(►Fig. 4) was removed. Whitish pultaceous contents mixedwithhair and teeth (►Fig. 5)were removed. Complete excisionofcyst alongwith the cystwallwasperformed.Themyelotomywas left open. The dura was closed with 6-0 Prolene. Themuscles and skin were subsequently closed with absorbablestitches. Recovery from anesthesia was uneventful.
Results
Immediately after the surgery, the patient’s power in thelower limbs was ⅖ and ⅘ in the upper limbs. There was norespiratory distress. Over a period of 3 days, the powerimproved to ⅘ in the lower limbs and ⅘ in the upper limbs.The catheter was removed on the 10th postoperative day, andthe patient was able to void urine naturally without anybladder dysfunction. Bowel movements were normal, and
Materiais e Métodos Uma paciente de 18 anos de idade apresentou fraqueza nosquatro membros, mais distal que proximal, com três anos progressivos de duração. Aressonância magnética apresentou uma lesão intramedular de C5 a C7 com realce doanel periférico. Espirais foram observadas dentro da lesão na imagem ponderada em T2, com escavação dos corpos vertebrais C5–C7. Procedimentos operatórios e achados:realização de laminectomia parcial de C5 a D1. A dura cervical foi aberta. Uma pequenamielotomia foi feita na zona de entrada da raiz. Cerca de 1,5 ml de fluído amarelado foiextraído. Detritos brancos brilhantes com cabelo, polpa esbranquiçada e dentes foramremovidos. Foi realizada a excisão completa do cisto com parede de cisto.Resultados O exame histopatológico revelou que a parede do cisto estava alinhadapor epitélio escamoso estratificado com derme subjacente apresentando folículoscapilares, glândulas sebáceas, tecido adiposo e cisto cheio de detritos de creatinina,sugerindo cisto dermoide.Conclusão A posição intramedular do cisto dermoide no cordão cervical e a ausênciade disrafismo espinhal congênito faz deste um caso único, uma entidade rara, eassegura sua inclusão junto aos casos relatados de lesões raras ocupando espaçointramedulares.
Palavras-chave
► cisto dermoideintramedular
► cordão cervicalmedular
► apresentação rara► ausência de disrafia
espinhal
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Intramedullary Dermoid Cyst- C5 to C7 Level Seerangan et al. 141

there was no incontinence of feces. The patient was able towalk with support on the 10th postoperative day. The woundhealed well, and the stitches were removed on the 14th
postoperative day, after which the patient was discharged.
Histopathology
The sections show that the cyst wall was lined by stratifiedsquamous epithelium with underlying dermis showing hairfollicles, sebaceous glands, adipose tissue and cyst filledwithkeratin debris (►Fig. 6).
Discussion
The common locations of dermoid cysts are:
1. Scalp (angle of eye and retro mastoid region)2. Skull bones (intradiploic)3. Intracranial, in the suprasellar region and posterior fossa4. Intraspinal, mainly intradural, and associated with other
spine defects.
The dermoid cysts are a developmental abnormality andarise from the nests of embryonic ectoderm that get buried
Fig. 1 Intramedullary dermoid cyst at C5–C7 level without spinal dysraphism.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Intramedullary Dermoid Cyst- C5 to C7 Level Seerangan et al.142

or trapped under the lines of fusion of the ectodermal folds inthe developing embryo.1,2
It is well known that the nervous system develops from theectoderm. The cells on the dorsal aspect of the developingembryo thicken to form the neural plate or placode along theaxis of the embryo. The neural platebends and closes to fromatube called the neural tube, from which the entire nervoussystem develops. The neural tube closes in the dorsal midlinefirst, and the closure then extends cranially and caudally sothat the anterior neuropore closes at 24 days and the posteriorneuropore at 28days. Thus, as theneural tube closes last in thecaudal part, that is the lumbo-sacral region, there is a biggerchance that this process may be disturbed, and nests ofcutaneous tissue may get trapped within the developingtube, giving rise to dermoid cysts. Hence, the propensity forthe dermoid cyst to occur in the lumbosacral region.
Also, dermoid cysts are commonly associated with spinaldysraphism. This is because the process that gives rise tospinal dysraphism is also responsible for the development ofthe dermoid cyst.3,4 The low incidence of dermoid cysts inthe cervical region is likely related to the embryologicalprocess of neural tube closure, which begins in the area ofthe neural tube destined to become the lower cervical cordand proceeds rostrally and caudally.
Spinal inclusion cysts are usually intradural, intramedul-lary in the cervical spinal cord region, with the othercommon lesions being neuroenteric cysts, arachnoid cysts,epidermoid and dermoid cysts.1,2
Dermoid cysts usually present themselves in childhood,as a consequence of associated anomalies or by symptoms ofcord tethering and mass effects. However, in this case, thepatient had no associated developmental anomaly of the
Fig. 2 T1-weighted magnetic resonance imaging focusing on intra-medullary dermoid cyst at C5–C7 level.
Fig. 3 Whorls seen on T2-weighted magnetic resonance imaging.
Fig. 4 Intraoperative picture of dermoid cyst.
Fig. 5 Macroscopic image of the excised specimen showing itsectodermal derivatives.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Intramedullary Dermoid Cyst- C5 to C7 Level Seerangan et al. 143

spine. Because of the absence of any other congenital anom-aly of the spine, the patient presented at a later age, after shehad developed significant symptoms, particularly in the leftside of the body. Total excision of the dermoid cyst wasperformed by standard micro neurosurgical techniqueemployed for other intramedullary tumors.
We could find three other cases 5–8 in which a dermoidcyst was in the cervical cord andwas not associatedwith anyother congenital anomalies of the spine. In other reportedcases,6,7,9 the location of the dermoid cyst and the presenceor absence of congenital anomaly of the spine were not clearas they were dated before the advent of MRI. Hence, it isdifficult to ascertain whether these cases represent the“true” intramedullary dermoid cyst or are part of a develop-mental defect.
Conclusion
The intramedullary location of the dermoid cyst in thecervical cord and the absence of any congenital spinaldysraphism make this case a very unique and rare entityand add to the reported cases of rare intramedullary spaceoccupying lesions.
Conflict of InterestAuthors declare no conflicts of interest.
References1 ShubhaAM,Mohanty S, Das K, Garg I. Congenital inclusion tumours
in spinal dysraphism. Indian J Pediatr 2010;77(02):167–1702 Ogden AT, Khandji AG, McCormick PC, Kaiser MG. Intramedullary
inclusion cysts of the cervicothoracic junction. Report of twocases in adults and review of the literature. J Neurosurg Spine2007;7(02):236–242
3 Bourhis LE. [Intramedullary dermoid cyst]. RevNeurol (Paris) 1952;86(04):339–340
4 Buur T, MørchMM. [Intramedullary dermoid cyst]. Ugeskr Laeger1981;143(52):3552–3553
5 Kumar S, Gupta S, Puri V, Gupta RK, Malik R. Intramedullarydermoids in children. Indian Pediatr 1990;27(06):626–629
6 NajjarMW, Kusske JA, Hasso AN. Dorsal intramedullary dermoids.Neurosurg Rev 2005;28(04):320–325
7 SharmaNC, Chandra T, SharmaA, BajajM, KunduR. Long-segmentintramedullary spinal dermoid. Indian J Radiol Imaging 2009;19(02):148–150[PMC free article] [PubMed]
8 Gagliardi FM, Ferrari G. Su un caso di dermoide intramidollare.].Acta Neurochir (Wien) 1969;21(02):197–204
9 Roth M, Hanák L, Schröder R. [Intramedulární dermoid]. CeskNeurol 1966;29(05):351–354
Fig. 6 Histopathology slide
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Intramedullary Dermoid Cyst- C5 to C7 Level Seerangan et al.144

Meningioma of the Pineal Region — DifferentialRadiologic Aspects of Pineal Region TumorsBased on a Clinical Case
Meningioma da região da pineal – aspectos radiológicosdiferenciais dos tumores da região pineal baseado emum caso clinico
Tiago Marques Avelar1 Aline Lariessy Campos Paiva1 Márcio Alexandre Teixeira da Costa1
Guilherme Brasileiro de Aguiar1 João Luiz Vitorino1 José Carlos Esteves Veiga1
1Faculdade de Ciências Médicas da Santa Casa de São Paulo, SãoPaulo, SP, Brazil
Arq Bras Neurocir 2018;37:145–147.
Address for correspondence Tiago Marques Avelar, MD, Faculdade deCiências Médicas da Santa Casa de São Paulo, Rua Doutor CesárioMotta Júnior, 61 - Vila Buarque, São Paulo, SP, 01221-020, Brazil(e-mail: [email protected]).
Keywords
► meningioma► pineal gland► brain neoplasms
Abstract Pineal region tumors are uncommon among neoplasm of the central nervous system,with this region being the most heterogeneous in terms of histological types.Meningiomas are rarer still, but can be found at this site, with origins in either thevelum interpositum or falcotentorial junction. Neuroimaging exams can distinguishmalignant from benign lesions besides helping to define the origin of the lesion as thepineal parenchymal or surrounding structures. We report the case of a woman with apineal region tumor in which differential diagnoses included meningioma and germi-noma, with confirmation of the former based on radiological characteristics andhistopathology. In addition, a brief review of differential diagnoses and approachesfor cases of lesions in this region is provided.
Palavras-chave
► meningioma► glândula pineal► neoplasias encefálicas
Resumo Os tumores da região da pineal apresentam uma baixa frequência entre as neoplasiasdo sistema nervoso central, sendo esta região a mais heterogênea em termos de tiposhistológicos possíveis. Meningiomas são lesões ainda mais raras, porém possíveis deadvirem desta localização, sejam originados do velum interpositum ou da junçãofalcotentorial. Os exames de neuroimagem permitem distinguir lesões malignas debenignas além de auxiliar na definição entre origem do parênquima pineal ou deestruturas adjacentes. Apresentamos o caso de umamulher adulta com uma neoplasiada região da pineal cujos diagnósticos diferenciais incluíram meningioma e germi-noma, evidenciando-se pelas características radiológicas e resultados histopatológicostratar-se do primeiro. Além disso, fazemos uma breve revisão a respeito dos diag-nósticos diferencias e condutas frente a uma lesão desta região.
receivedAugust 15, 2017acceptedApril 3, 2018published onlineJuly 18, 2018
DOI https://doi.org/10.1055/s-0038-1651527.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 145

Introduction
Tumors of the pineal gland are uncommon, accounting foronly 0.4 to 1% of all intracranial tumors in adults. Otherneoplasms with origin in the pineal region, whose incidencelies in the 0.4 to 8% range depending on the author, are oftenaddressed together in the literature.1 The most commonhistological types of pineal tumors are those derived fromgerminative cells and pineal parenchymal tumors, repre-senting 89% of the lesions in this region.1Meningiomas of thepineal region are rare entities and make up 2 to 8% of alltumors found in this area.2
The pineal region is themost heterogeneous in the centralnervous system in terms of histological types of tumor,3 andimaging exams can help to confirm the diagnosis besideshelping to define the approach and plan of operation.4
Germinomas can secretemarkers such as β human chorionicgonadotropin (β-HCG) andα-fetoprotein (α-FP), whose pres-ence can preclude the need for surgical biopsy. Cases inwhich these markers are absent require histological confir-mation via biopsy or lesion removal.5 Surgical removal is thetreatment of choice for meningiomas, and is regarded as thedefinitive treatment.6
The objective of this article was to report the case of ameningioma in the pineal region and provide a brief reviewof its differential diagnoses and therapeutic management.
Case Report
A 43-year-old female teacher presented with a 1-year historyof headache. Initial physical exam revealed no visual changes,gait problems, motor deficits or cerebellar signs. Brain mag-netic resonance imaging (MRI)was thenperformed, disclosingan expansive lesion in the pineal gland region, with initiallysuspected differential diagnoses of meningioma and germi-noma. The patient was submitted to initial conservative treat-ment. However, the repeat MRI after 6 months (►Fig. 1)revealed lesion growth concomitant with worsening head-ache. Given the strong suspicion of meningioma based on theMRI characteristics, surgical treatment of the lesion waselected.
Occipital craniotomy with transtentorial access wasemployed to resect the lesion, since this route permits an
excellent view both above and below the tentorial notch. Thefrozen section biopsy revealed meningioma, subsequentlyconfirmed by histopathologic analysis and immunohis-tochemistry, which revealed a World Health Organization(WHO) grade I meningothelial meningioma. The follow-upMRI exam showed complete resection of the lesion. Thepatient evolved without neurological deficits and was head-ache free at 1-year follow-up.
Discussion
Pineal meningiomas can be classified into two distinct enti-ties: falcotentorial meningiomas and thosewith origin in thevelum interpositum.Neoplasia arising from the falcotentorialjunction occur where the dural folds of the tentorium meetwith the cerebral falx, and can project antero-superiorly,inferiorly or posteriorly. Meningiomas (rarer) of the veluminterpositum occupy the pineal region and have no connec-tion with the dura mater. They originate in the posteriorportion of this structure, formed by two layers of pia mater,which constitute the floor of the third ventricle and containsthe internal cerebral veins and their tributaries and medialposterior choroidal arteries.2 In this case, the meningiomahad no dural attachment, which leads to the diagnosis ofvelum interpositum meningioma.
The main symptoms presented by patients with pinealregion meningiomas are related to intracranial hyperten-sion and hydrocephaly, such as headache, gait difficulties,visual disturbances, papilledema, dizziness and cognitiveimpairments, which stem from obstructed CSF (cerebrospi-nal fluid) drainage; in the event of aqueduct obstruction,symptoms can develop rapidly.7 Parinaud syndrome (paral-ysis of vertical gaze, convergence-retraction nystagmus,abnormal pupils with unreactive photomotor reflex) isdescribed in up to 10% of the cases of pineal regionmeningioma; changes in extrinsic ocular movement arerare in meningiomas of the pineal region, aiding theirdifferentiation from other tumors of this area for whichthese findings are more common.2 Other presentationsdescribed include hemifacial spasm, hypoacusis and earlypuberty.5,7,8 In the present case, the time elapsed betweensymptom onset and diagnosis was similar to the periodreported in the literature.2
Fig. 1 6-month follow up head magnetic resonance imaging scan, T1-weighted post-contrast, axial (A), coronal (B) and sagittal (C) views,disclosing extra-axial lesion with intense homogeneous paramagnetic agent uptake.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Meningioma of the Pineal Region Avelar et al.146

Despite advances in diagnostic imaging techniques, dif-ferentiating between meningioma and other tumors of thepineal region remains a challenge.7 However, neuroimagingcan help to distinguish malignant from benign lesions andalso primitive pineal lesions from tumors with origins in thesurrounding structures.4Germinomas can be seen on cranialcomputed tomography (CT) as circumscribed expansive,hyperattenuating lesions of the pineal region, due to thehigh lymphocyte content of the tumor, and typically envelopthe gland; on MRI, they can have cystic components withinthe tumor lesion and are iso- and hyperintense in relation togray matter on T1 and T2-weighted images, showing lessdiffusion owing to their hypercellular nature.4,9 On axialviews post-contrast, germinomas exhibit a characteristic“butterfly” shape.4
Pineocytomas are generally less than 3 cm in diameterand therefore have a low mass effect, “exploded” calcifica-tions toward the periphery, and a cystic center.4,9 Thesetumors are characterized by a homogenous, isointense signalon T1 and hyperintense signal on T2-weighted MRI.4
Meningiomas typically have avid contrast uptake andtend to be seen separate from the pineal gland, raising themesencephalic tectum; they tend to have homogeneouscontrast uptake on T1 and present as extra-axial lesions onMRI,9 as seen in the images of the present case.
The management of pineal region tumors is generallyaccording to a series of questions that need to be defined,5
including: whether the origin of the tumor is in the pinealgland or surrounding regions;whether the tumor is localizedor disseminated; the possibility of reaching diagnosis with-out histological confirmation; and finally, the need forsurgical intervention, and if so, the indication for biopsy orexcision.
Germinomas tend to secrete markers in the CSF or bloodand, in cases in which these are detected, histological confir-mation is not obligatory, and adjuvant therapy can beemployed immediately. Pure germinomas are tumors withan excellent prognosis, and the current approach entailschemotherapy followed by radiotherapy with field extendedto the ventricles.5 Pineocytomas are the most highly differ-entiated pineal parenchymal tumors and should becompletely removed whenever possible. Pineoblastomasare not highly differentiated and can be managed by surgeryand adjuvant chemo-radiotherapy, having a variable prog-nosis depending on the age of the patient.5Meningiomas aremanaged surgically and their resectability depends onthe degree of adherence to surrounding vascular structures,
notably the Galenic venous system and anterior part of thestraight sinus.7 The best approach to the pineal region(transtentorial or infratentorial supracerebellar) remains amatter of debate in the literature,2,7 but preservation of thevascular structures (internal and basal cerebral veins, Galenveins, for instance) ismore important than complete removalof the tumor.2 In the present case, the Galen system waspushed downwardly, thus, the transtentorial route waselected.
Conclusion
Pineal region meningiomas are rare lesions. Given the non-specific characteristics of these lesions on imaging exams,they should be considered as a differential diagnosis ofexpansive lesions in this region.
Conflicts of InterestThe authors declare that there are no conflicts of interest.
References1 Mottolese C, Szathmari A, Beuriat PA. Incidence of pineal
tumours. A review of the literature. Neurochirurgie 2015;61(2-3):65–69. Doi: 10.1016/j.neuchi.2014.01.005
2 Nowak A, Dziedzic T, Czernicki T, Kunert P, Marchel A. Falcoten-torial and velum interpositummeningiomas: two distinct entitiesof the pineal region. Neurol Neurochir Pol 2014;48(06):397–402.Doi: 10.1016/j.pjnns.2014.09.009
3 Ahmed AI, Zaben MJ, Mathad NV, Sparrow OCE. Endoscopicbiopsy and third ventriculostomy for the management of pinealregion tumors. World Neurosurg 2015;83(04):543–547. Doi:10.1016/j.wneu.2014.11.013
4 Deiana G, Mottolese C, Hermier M, Louis-Tisserand G, BerthezeneY. Imagery of pineal tumors. Neurochirurgie 2015;61(2-3):113–122. Doi: 10.1016/j.neuchi.2014.10.111
5 Frappaz D, Conter CF, Szathmari A, Valsijevic A, Mottolese C. Themanagement of pineal tumors as a model for a multidisciplinaryapproach in neuro-oncology. Neurochirurgie 2015;61(2-3):208–211. Doi: 10.1016/j.neuchi.2014.03.003
6 Blakeley JO, Grossman SA. Management of pineal region tumors.Curr Treat Options Oncol 2006;7(06):505–516. Doi: 10.1007/s11864-006-0025-6
7 Matushita H, Pinto FC, Plese JP. Meningiomas of pineal region inchildren. Arq Neuropsiquiatr 2007;65(4A):1000–1006. Doi:10.1590/S0004-282 � 2007000600017
8 Mallucci CL, Obukhov S. Successful removal of large pineal regionmeningiomas: two case reports. Surg Neurol 1995;44(06):562–566. Doi: 10.1016/0090-3019(95)00220-0
9 Hallinan JT, Hegde AN, Lim WE. Dilemmas and diagnostic diffi-culties in meningioma. Clin Radiol 2013;68(08):837–844. Doi:10.1016/j.crad.2013.03.007
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Meningioma of the Pineal Region Avelar et al. 147

Palsy of the Contralateral Abducens Nerve afterAneurysm Surgery and Temporal Meningioma in thePresence of Petroclival Meningioma: A Case Report
Paresia de nervo abducente contralateral pós-cirurgia deaneurisma e de meningioma temporal em presença demeningioma petroclival: relato de caso
Pedro Ferreira Paiva Moreira1 Anderson Rodrigo Souza1 Manoel Jacobsen Teixeira1
Eberval Gadelha Figueiredo1
1Division of Neurosurgery, Faculdade de Medicina, Universidade deSão Paulo, São Paulo, SP, Brazil
Arq Bras Neurocir 2018;37:148–150.
Address for correspondence Pedro Ferreira Paiva Moreira,Universidade de São Paulo, Av. Dr. Arnaldo, 455 - Cerqueira César,São Paulo, SP, 01246-903, Brazil (e-mail: [email protected]).
Introduction
After surgeries in places near the sixth abducens nerve,ipsilateral nerve palsy may occur due to injury by surgicalmanipulation. However, palsy of the sixth cranial nerve is alsoa rare complication following surgeries and procedures thatcan cause cerebrospinal fluid (CSF) hypotension in areasdistant from the nerve pathway. In the literature, there aredescriptions of this occurrence mainly in dural lesion spinal
surgeries1,2 and dura mater puncture procedures,3 such aslumbar punctures and spinal anesthesia.
The authors present a case of contralateral abducens nervepalsy after left middle cerebral artery aneurysm surgery andleft temporal meningioma, differing from most of the litera-ture reports describing lesions of the sixth cranial nervefollowing procedures and surgeries of the spine. Our objectiveis to discuss the mechanisms of the appearance of abducensnerve palsy when the site of manipulation is remote, along
Keywords
► abducens nerve palsy► petroclival
meningioma► intracranial aneurysm
Abstract The sixth abducens nerve is subject to injury after rare complications of intracranialhypotension caused by procedures such as dural punctures and spinal surgeries. Thepurpose of this case report is to discuss the mechanism of nerve palsy in thesesituations. Therefore, we describe a case of onset of contralateral sixth cranial nervepalsy after intracranial aneurysm and temporal meningioma surgery. Moreover, in thiscase there is a singularity due to the presence of the petroclival meningioma thatamplified the unfolding of the lesion.
Palavras-chave
► paresia de nervoabducente
► meningiomapetroclival
► aneurismaintracraniano
Resumo O sexto nervo abducente está sujeito a lesões após raros eventos de hipotensãointracraniana gerada por procedimentos como punções de dura-máter e cirurgias decoluna. O propósito deste relato de caso é discutir o mecanismo da paralisia destenervo nestas situações. Para isso, descrevemos um caso de aparecimento de paresia dosexto nervo craniano contralateral após cirurgia de aneurisma intracraniano e demeningioma temporal. Além do mais, neste caso há uma singularidade em razão dapresença do meningioma petroclival contralateral, que amplificou o desdobramentoda lesão.
receivedFebruary 8, 2018acceptedMarch 13, 2018published onlineMay 2, 2018
DOI https://doi.org/10.1055/s-0038-1648214.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de CasoTHIEME
148

with theparticularitiespresent in this case due to thepresenceof a petroclival meningioma ipsilateral to the injured nerve.
Case Report
Thepatient is a 49-year-oldwoman.Her initial symptomwas aheadache. As part of the diagnostic routine, a magnetic reso-nance imaging of the skullwas requested. In this examination,a left temporal meningioma, a left cerebral artery aneurysmanda rightpetroclivalmeningiomawere revealed (►Figs. 1,2).
After the identification of these lesions, the patient optedfor the surgery of only the left temporal meningioma and left
cerebral artery aneurysm. For this, a pterional craniotomywas performed on the left hemisphere of the brain.
In the postoperative period, the patient developed abdu-cens nerve palsy on the right side, contralateral to thesurgery. After 3 months, the function of this nerve wascompletely recovered spontaneously.
Discussion
Abducens nerve palsies in cases of procedures performed indistant sites were described in the literature after lumbarpuncture (diagnostic and therapeutic), inadvertent lumbarpuncture during epidural anesthesia, spinal anesthesia, CSFshunt, intrathecal drug delivery, myelography, and lumbardrainage.4 Cases of this occurrence have also been reporteddue to spinal surgery.5 These procedures may lead to intra-cranial hypotension due to CSF drainage,6 which would bethe explanation for nerve damage. This is due to the anatomyand the long course of the sixth cranial nerve and its relationto the base of the skull.
The abducens nerve innervates the lateral rectus muscle,whose function is the abduction of the eye. Its nucleus lies onthedorsal surfaceof theponsventrally to thefloorof thefourthventricle. Throughout its course, the nerve has three points ofpronounced curvature.7 When emerging from the lower partof the pons, the nerve performs its first sharp curve in theupper direction. It then goes through the subarachnoid spacesuperiorly along the clivus and through the Dorello channel.This channel lies between the petrosphenoidal ligament(Gruber ligament) and the apex of the petrous part of thetemporal bone and fixes the nerve.8 Farther, the nerve curvesfor thesecondtime, throughtheDorello canal, aroundtheapexof the petrous part of the temporal bone and penetrates intothe cavernous sinus. In this region, it runs laterally to theinternal carotid artery (around which it makes its thirdcurvature) and enters the orbit through the superior orbitalfissure. Soon after, it innervates the lateral rectus muscle.
In the course of its long intracranial path, the abducensnerve is subjected to mechanical forces of traction andcompression. In the aforementioned situations of intracra-nial hypotension by CSF drainage, the nerve loses its supportand remains stretched. This is due to its anatomical relation-ships with the base of the skull and its long and tortuoustrajectory. Thefirst sharp curve of the nerve in the petroclivalregionwhen piercing the dura and entering the Dorello canalis the region most susceptible to nerve stretching. In thisarea, the acute angle near the nerve fixation region in thecanal favors the risk of traction with the loss of brainstemsupport by intracranial hypotension.9 This stretching wouldinjure the nerve, generating its palsy.
However, reports in the literature point to the palsy of thesixth cranial nerve by this mechanism mostly through pro-cedures and surgeries in the spine with dural puncture, notintracranial surgeries. In this case, the drainage of the CSFand the opening of the cisterns during surgery was sufficientto cause nerve damage.
We believe that the particularity of the case lies in thepresence of the petroclival meningioma ipsilateral to the
Fig. 1 Gadolinium-enhanced T1-weighted axial magnetic resonanceimage showing the left temporal meningioma and the right petro-clival meningioma.
Fig. 2 Arteriography showing the left cerebral artery aneurysm.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Palsy of the Contralateral Abducens Nerve Moreira et al. 149

injured nerve. The presence of petroclival meningioma alonecan generate an abducens nerve palsy due to traction andcompression injury,10 but in this case, the palsy manifestedonly after the aneurysmand temporalmeningioma surgery. Asthe nerve region susceptible to stretching is just along itstortuous path through the petroclival region, the presence ofthe tumor in this area would amplify the nerve traction. Thus,both the relative CSF imbalance and the consequent loss ofnerve support in thebrainstemand the compression caused bythe petroclival meningioma were responsible, in this case, forthe palsy of the nerve contralateral to the surgery and ipsilat-eral to the unresected tumor.
Conclusion
Palsy of the abducens nerve, even when the site of manipu-lation is remote, is characterized as a rare complication aftersurgeries and procedures with dural puncture. With relativeintracranial hypotension due to CSF imbalance, the nerve issubject to stretching because of its long and tortuous course.Moreover, in this case, the petroclival meningioma contra-lateral to the surgery may have contributed to transientabducens nerve palsy.
Conflicts of InterestThe authors declare that there are no conflicts of interest.
References1 Sandon LH, Choi G, Park E, Lee HC. Abducens nerve palsy as a
postoperative complication of minimally invasive thoracic spinesurgery: a case report. BMC Surg 2016;16(01):47
2 Cho DC, Jung ES, Chi YC. Abducens nerve palsy after lumbar spinalfusion surgerywith inadvertent dural tearing. J Korean NeurosurgSoc 2009;46(06):581–583
3 Nishio I, Williams BA, Williams JP. Diplopia: a complication ofdural puncture. Anesthesiology 2004;100(01):158–164
4 Cain RB, Patel NP, Hoxworth JM, Lal D. Abducens palsy afterlumbar drain placement: a rare complication in endoscopic skullbase surgery. Laryngoscope 2013;123(11):2633–2638
5 Joo JD, Yoon SH, KimKJ, Jahng TA, KimHJ. Isolated abducens nervepalsy due to cerebrospinal fluid leakage following lumbar dis-cectomy: a rare clinical entity. Eur Spine J 2013;22(Suppl 3):S421–S423
6 Quintero I, Candamil Á, Mejía Mantilla J, Medina H, Ariza CadenaF. Síndrome de hipotensión endocraneana: ¿una cefalea pospun-ción dural? Rev Colomb Anestesiol 2013;41(01):57–60
7 Umansky F, Elidan J, Valarezo A. Dorello’s canal: a microanato-mical study. J Neurosurg 1991;75(02):294–298
8 Romero FR, Ramos JG, Chaddad-Neto F, Bethencourt JM, deOliveira E. Microsurgical anatomy and injuries of the abducensnerve. Arq Neuropsiquiatr 2009;67(01):96–101
9 Azarmina M, Azarmina H. The six syndromes of the sixth cranialnerve. J Ophthalmic Vis Res 2013;8(02):160–171
10 Shono T, Mizoguchi M, Yoshimoto K, Amano T, Natori Y, Sasaki T.Clinical course of abducens nerve palsy associatedwith skull basetumours. Acta Neurochir (Wien) 2009;151(07):733–738, discus-sion 738
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Palsy of the Contralateral Abducens Nerve Moreira et al.150

Schistosomal Cervical Myelopathy
Mielopatia esquistossomótica cervical
Ronald Farias1 Kléver Forte de Oliveira1 George de Albuquerque Cavalcanti Mendes1
Ussânio Mororó Meira1
1Center of Medical Science, Universidade Federal da Paraíba,João Pessoa, PB, Brazil
Arq Bras Neurocir 2018;37:151–153.
Address for correspondence Ronald Farias, MSc, Centro de CiênciasMédicas, Universidade Federal da Paraíba, João Pessoa, PB, Brazil(e-mail: [email protected]).
Keywords
► schistosoma mansoni► schistosomiasis► neuroschistosomiasis► cervical cord
Abstract Schistosomiasis is an infectious disease caused by trematode platyhelminths of the genusSchistosoma. The involvement of the cervical spinal cord is rare, with few cases reported inthe literature. The management of such patients is particularly challenging, since clinicaland radiological findings may be confounded with other inflammatory diseases and/ orspinal cord tumors. We describe a 20-year old male with a history of swimming outdoors.He first presented pain in the back of the neck extending to shoulders and upper limbsparesis associated with four limbs hyperreflexia. The magnetic resonance imaging (MRI)showed a hypointense T1-weighted lesion in the cervical spinal cord, which was hyperin-tense onT2 images. The serologic testing was negative for schistosomiasis. A cervical cordbiopsy at the C5-C6 level showed Schistosoma eggs in the histopathological examination.The treatment was performed using a single dose of praziquantel 50 mg/kg, withprednisone 40 mg/day for 3 weeks. On the follow-up, 1 year later, the patient presentedmild reductionof the vibratory sensitivity in thedistal thirdofboth legs.Our illustrative casestrengthens that, in endemic regions, Schistosoma mansoni infestation should be includedin the differential diagnosis of intramedullary expansive lesions.
Palavras-Chave
► schistosoma mansoni► esquistossomose► neuroesquis-
tossomose► medula cervical
Resumo A esquistossomose é uma doença infecciosa causada por platelmintos trematódeos dogênero Schistosoma. O acometimento damedula espinhal cervical é raro, com poucos casosapresentados na literatura.Omanejo dessespacientes é particularmente difícil, uma vez queos achados clínicos e radiológicos podem ser confundidos comoutras doenças inflamatóriase/ou tumores da medula espinhal. Descrevemos um homem de 20 anos de idade comhistória denatação aoar livre. Primeiramente, ele apresentou cervicalgia que se estendeuatéos ombros e paresia dosmembros superiores, associada à hiperreflexia de quatromembros.A ressonânciamagnética (RM)mostrou lesãohipointensa emT1namedula espinhal cervical,a qual foi hiperintensa nas imagens em T2. O teste sorológico foi negativo para esquistosso-mose. Uma biópsia da medula cervical ao nível C5-C6 evidenciou ovos de Schistosoma noexame histopatológico. O tratamento foi realizado com dose única de praziquantel 50 mg/kg, com prednisona 40 mg/dia por 3 semanas. No seguimento de 1 ano, o pacienteapresentou discreta redução da sensibilidade vibratória no terço distal de ambas as pernas.Nosso caso ilustrativo reforça que, em regiões endêmicas, a infestação pelo Schistosomamansoni deve ser incluída no diagnóstico diferencial de lesões expansivas intramedulares.
receivedApril 10, 2018acceptedMay 8, 2018
DOI https://doi.org/10.1055/s-0038-1661356.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 151

Introduction
Schistosomiasis is an infectious disease caused by trematodeplatyhelminths of the genus Schistosoma. Among the speciesof this genus, the most important for humans are Schisto-soma mansoni, Schistosoma haematobium e Schistosomajaponicum.1 It is estimated that at least 200 million peopleare affected by it worldwide, and 200 thousand deaths due tothis condition are registered annually, being endemic inAfrica, South America and most of Asia.1–3 S chistosomamansoni is the only species existing in Brazil. Around 26million Brazilians are at risk of contracting it.4
The typical manifestations of schistosomiasis include theurogenital, gastrointestinal and hepatolienal systems. Thecentral nervous system involvement by S. mansoni is an atypi-cal presentation, occurring by anomalous migration of theschistosome or unusual egg deposition from the portal venoussystem, through the venous plexus of Batson.3,4 This explainsthe higher prevalence of conus medullaris and thoracolumbarmedulla envelopment. The involvement of the cervical spinalcord is rare, with few cases being reported in literature. Themanagement of such patients is particularly challenging, sinceclinical and radiological findings may be confounded withother inflammatory diseases and/ or spinal cord tumors.3
Case Report
A male patient, 20 years old, white, with previous history ofswimming outdoors, presented pain in the back of the neckextending to the shoulders. The neurological examinationshowed upper limbs paresis 4/5 associated with 4 limbshyperreflexia. Sensory changes were not found. The magneticresonance imaging (MRI) showed a hypointense T1-weightedlesion in cervical spinal cord, which was hyperintense on T2images (►Fig. 1). The biochemical and cytological evaluationof the cerebrospinalfluid (CSF) showedno alterations. Indirectimmunofluorescence of CSF for schistosomiasis was negative.
The laboratory tests revealedmild leukocytosis (11,900/mm3)associated with moderate eosinophilia (1,035/mm3). Fecessamples (Kato-Katz method) showed no Schistosoma eggs.
A cervical cord biopsy at the C5-C6 level showed a chronicgranulomatous inflammatory process with multinucleatedgiant cells and birefringent material, suggestive of S. mansonieggs (►Fig. 2).
The treatment was performed using a single dose of pra-ziquantel 50 mg/kg, with prednisone 40 mg/day for 3 weeks,performing a gradual withdrawal.
At the one-year postoperative follow-up, the patientpresented mild reduction of the vibratory sensitivity in thedistal third of both legs. However, he preserved reflexes inthe four limbs, with normalization of muscular strength inthe upper limbs.
Discussion
Vascular obstruction occurs both through venousmigration ofthe eggs or direct deposition of these by the parasite in theperimedullary plexus, with formation of granulomas andintense local inflammatory reaction, followed by necrotizingmyelitis. There are two clinical forms of schistosomal involve-ment of the spinal cord: granuloma formation and transverse
Fig. 1 Preoperative magnetic resonance imaging (MRI). (A) T1-weighted sagittal view, showing hypointense signal in the C4-C6 spinalsegments; (B) in the T2-weighted sagittal view, hyperintense signal extending through almost the entire cervical spinal cord. (C) T2 axial viewshows hyperintense signal in the cervical spine at the C4-C5 transition level.
Fig. 2 Histopathological examinationof the cervical spinal cord evidencingfibroconjunctive stroma containing remains of Schistosoma mansoni eggs(birefringent material) in the middle of a granulomatous-like inflammatoryinfiltrate, compatible with the diagnosis of schistosomiasis.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Schistosomal Cervical Myelopathy Farias et al.152

myelitis.3 The schistosomal myelopathy (SM) prevalence isunknown. However, strong evidences indicate it is an under-diagnosed condition.1,4 The typical patient of this disease isyoung, male, presenting low back or lower limbs pain, usuallyof radicular pattern, followed by weakness and progressivesensorial loss in the lower limbs, associated with autonomicdysfunction, mainly of the bladder.1
The diagnosis is primarily based on clinical examination.The MRI usually presents hyperintense T2-weighted lesions,which are isointense onT1 images.2 The laboratory tests of CSFreveal nonspecific findings.1,4 Our patient presented normalprotein and glucose levels; pleocytosis was not evidenced.
The SM treatment is based on the association of ananthelmintic (praziquantel or oxamniquine) and a cortico-steroid. In cases of granuloma formation, a surgical approachwith decompression is indicated.1,2
Reports of cervical spinal cord schistosomiasis have beenpreviously published. Junker et al3 and Laureys et al2 reportedcases of neuroschistosomiasis presenting as transverse myeli-tis in men in their fourth decade. A decompressive laminec-tomy was performed in the first case due to acute incompletetetraparesis and evidence of spinal stenosis at MRI. Silva et al5
described a case of granuloma formation case in a 34 years oldmale. In the three cases, the patients presented sensory andmotor impairment, in addition to pain. The proposed pharma-cological treatment was similar to our case (anthelmintic andcorticosteroid), as well as the clinical outcome (sensory andmotor improvement and pain resolution) (►Table 1).
Conclusion
Cervical myelopathy is an extremely rare presentation ofSchistosomiasis. Our illustrative case strengthens that, in
endemic regions, S. mansoni infestation should be includedin the differential diagnosis of intramedullary expansivelesions. The diagnosis is based on clinical and radiologicalfindings, and pharmacologic therapy is the primary treat-ment approach. Surgical decompression and biopsy arereserved to patients in whom no clinical improvement isobserved after institution of antischistosomal medicationsand/or in case of neurological deterioration. Only in suchcases, surgery should be indicated. The SM prognosis isexcellent when the diagnosis is early, and the treatment isappropriate.1,3
Conflicts of InterestThe authors declare that there are no conflicts of interest.
References1 Ferrari TCA, Moreira PRR, Cunha AS. Spinal cord schistosomiasis:
a prospective study of 63 cases emphasizing clinical and ther-apeutic aspects. J Clin Neurosci 2004;11(03):246–253. Doi:10.1016/j.jocn.2003.05.006
2 Laureys G, Chaskis C, Bourgain C, Stadnik T, Dielman C, Ebinger G.A case of ‘tropical’ myelopathy. Acta Neurol Belg 2007;107(04):131–133
3 Junker J, Eckardt L, Husstedt I. Cervical intramedullar schistoso-miasis as a rare cause of acute tetraparesis. Clin Neurol Neurosurg2001;103(01):39–42. Doi: 10.1016/S0303-8467(00)00124-4
4 Henriques-Souza AMDM, Valença MM. Schistosomal myelopathyin childhood: findings of magnetic resonance imaging in 26patients. Pediatr Neurol 2011;45(06):373–376. Doi: 10.1016/j.pediatrneurol.2011.09.006
5 Silva LCS, Kill CM, Lambertucci JR. Cervical spinal cord schisto-somiasis. Rev Soc Bras Med Trop 2002;35(05):543–544. Doi:10.1590/S0037-86822002000500023
Table 1 Cases of schistosomal myelopathy reported in the literature
Case Clinical Manifestations Treatment Outcome
Junker et al3
(2001)Pain in the four limbs; tetraparesisassociated with the occurrence ofclonus in the legs and hypoesthe-sia under the T4 level on the left,and the T8 level on the right
Decompressive laminectomy,followed by praziquantel, highdoses of corticoid andphysiotherapy
Distal spastic tetraparesis in thelegs and hypoesthesia from the C6level down
Silva et al5
(2002)Neck pain, tetraparesis, paresthesiain the four limbs andhypoesthesia atthe C5 level
Oxamniquine (15mg/kg in a singledose) and prednisone 60 mg/dayfor 2 months
Muscle strength improvement andhypoesthesia resolution;persistence of left hemi-bodyparesthesia
Laureys et al2
(2007)Pain, tactile hypoesthesia,hypoalgesia, hypopalesthesia anddecreased distal proprioception inthe legs, associated with flexionand extension paresis (strengthgrade 4); mild gait instability
Praziquantel (60 mg/kg/day for3 days) and methylprednisolone(64 mg/day)
Resolution of pain and sensorysymptoms, as well as markedmotor improvement
Our case Paresis of the upper limbs(strength grade 4) associated withhyperreflexia in the 4 limbs
Single dose of Praziquantel(50 mg/kg) associated with pre-dnisone (40 mg/day for 3 weeks,performing a gradual withdrawal)
Hypopalesthesia in the distal thirdof both legs; preserved reflexes inthe 4 limbs, with normalization ofmuscular strength (grade 5) in theupper limbs
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Schistosomal Cervical Myelopathy Farias et al. 153

Surgery of a Posterior Communicating ArteryAneurysm with Fetal-Type Circulation
Cirurgia de um aneurisma da artéria comunicanteposterior com circulação do tipo fetal
Nicolás González1 Manuel Morales1 Franco Ravera1 Arturo Ruiz-aburto1 Juan Vásquez1
José Muller1 Jhon Mosquera1 Rodrigo Zapata1
1Department of Neurosurgery, Hospital Regional Rancagua,Rancagua, Chile
Arq Bras Neurocir 2018;37:154–156.
Address for correspondence Nicolás González, MD, Hospital RegionalRancagua, Rancagua, Av. Libertador Bernardo O’Higgins 3065,Rancagua, Chile (e-mail: [email protected]).
Introduction
A fetal configuration of the circle of Willis is seen in up to17.5% of an adult patient population.1 Compromise of a fetal-type posterior communicating artery (PCOMM) or its perfo-rators by surgical clipping could result in posterior circula-tion infarction and neurological morbidity.2,3 The technicalconsiderations in the treatment of a patient with a PCOMManeurysm with lateral projection and a fetal-type PCOMMartery are presented.
Case
A 65-year-old female patient was admitted to our emergencyunit with a sudden onset of headache and diplopia. Physicalexamination revealed a left-sided complete third nervepalsy. The computed tomography (CT) scan was negativefor subarachnoid hemorrhage. The computed tomographyangiography (CTA) (►Fig. 1) revealed a left 4.9 mm � 9 mmunruptured left PCOMM aneurysm with a lateral projection.Ipsilateral fetal configuration of the circle of Willis was
Keyowords
► aneurysm► posterior
communicatingartery
► circle of Willis► microsurgery
Abstract Inadvertent occlusion of a fetal-type posterior communicating artery in aneurysmsurgery could result in posterior circulation infarction and neurological morbidity. Thecase of a patient with an unruptured posterior communicating artery aneurysm withlateral projection and a fetal-type posterior communicating artery is presented. Theutility of the carotid-oculomotor window as a surgical corridor to safely find the fetal-type posterior communicating artery is discussed.
Palavras-chave
► aneurisma► artéria comunicante
posterior► círculo de Willis► microcirurgia
Resumo A oclusão da artéria comunicante posterior do tipo fetal em cirurgia de aneurisma poderesultar em infarto da circulação posterior e morbidade neurológica. Apresentamos ocaso de um paciente com aneurisma não roto da artéria comunicante posterior comprojeção lateral e uma artéria comunicante posterior do tipo fetal. Discutimos autilidade da janela carótida-oculomotora como um corredor cirúrgico para encontrarcom segurança a artéria comunicante posterior do tipo fetal.
receivedMarch 23, 2018acceptedMay 8, 2018published onlineJuly 9, 2018
DOI https://doi.org/10.1055/s-0038-1661357.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Technical Note | Nota TécnicaTHIEME
154

observed, with a large hyperplastic PCOMMof 13 mm lengthand 2.5 mm width, and a hypoplastic P1 segment of theposterior cerebral artery.
Surgical Technique
A classic pterional craniotomy was performed on the leftside. Under the surgical microscope, initial arachnoid dissec-tion of the optic-carotid cistern allowed cerebrospinal fluid
aspiration and brain relaxation. Exposure of the PCOMMsegment of the internal carotid artery (ICA) revealed theaneurysm (►Fig. 2A), but visualization of the PCOMM originwas not possible. At this point, to allow visualization of thePCOMM it was necessary to do a proximal opening of theSylvian fissure, to reveal the carotid-oculomotor window(CoW). As previously reported,3 temporal lobe retractionshould be avoided to prevent aneurysm rupture. Pilot clip-ping with a 9 mm straight clip was performed (►Fig. 2B) toincrease the safety of Sylvian fissure dissection. In the CoW(►Fig. 2C, D) it was possible to find the PCOMM origin andthe perforators. Proximal control at the ophthalmic segmentand at the PCOMM segment (►Fig. 2E) allowed aneurysmsoftening and clip repositioning, under direct visualization ofthe PCOMM artery (►Fig. 2F) and anterior choroidal arteries.Doppler sonography confirmed vascular flow. The patienthad a good postoperative course without complications andwas discharged with ongoing improvement of her thirdnerve palsy.
Discussion
In a non-fetal configuration of the circle ofWillis, the PCOMMis found at the interpeduncular cistern in the opticocarotidwindow,4 and its origin is observed as a knuckle on theposterolateral carotid wall, just proximal to the neck of theaneurysm, with a lateral to medial path from the ICA to theposterior cerebral artery.5
Fig. 2 Surgical technique.
Fig. 1 Preoperative computed tomography angiography.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Surgery of a Posterior Communicating Aneurysm González et al. 155

Surgery of PCOMManeurysmswith a fetal configuration ofthe circle of Willis endangers inadvertent occlusion of thePCOMM, because of its medial to lateral projection.5 In thesecases, a laterally projecting aneurysm may hide the PCOMMorigin and perforators. In this scenario, we believe it is neces-sary to do a careful proximal dissection of the Sylvian fissure,avoiding temporal retraction, to fully expose the CoW: thespace between the ICAmedially, the oculomotor nerve lateral-ly, and the uncus posteriorly.6 The CoW has been traditionallymentionedasprovidingaccess to thebasilar apexaneurysm,6,7
but should also be considered as a surgical corridor in cases offetal type PCOMM. This surgical strategy achieves three goals:to gain proximal control at the PCOMM, to fully observe thePCOMMduringfinal clipapplication, andtoconfirmpatencyofPCOMM and perforators. Micro doppler ultrasound8 and/ornear infrared indocyanine greenvideoangiography9 are usefultools that may be utilized to confirm vascular flow. Addition-ally, in cases of third nerve palsy, nerve decompressionmay beperformed, although it has been reported that oculomotornerve palsy improves, inmost caseswith clipping andwithoutneed of nerve decompression.10,11
Anterior clinoidectomy12,13 and/or anterior petroclinoidfold14 release may be necessary in cases when the intra-operative view of the neck of the aneurysm is obstructed bytheanteriorclinoidprocess, as in casesof short lengthof the ICA.
Conclusion
A laterally projecting PCOMM aneurysm may hide thePCOMM origin in a fetal configuration of the circle of Willis.In these cases, careful proximal Sylvianfissure dissection andexposure of the carotid oculomotor window are needed toexpose the PCOMM artery, gain proximal control, and toconfirm patency after clipping.
Conflicts of InterestThe authors declare that they have no conflicts of interest.
References1 Beumer D, Delwel EJ, Kleinrensink GJ, Akouri S, Torres A, Krisht AF.
The perforator-free zone of the posterior communicating artery andits relevance in approaches to the interpeduncularcistern, especiallythe transcavernous approach: an anatomic study. Neurosurgery2007;61(05, Suppl 2):187–191, discussion 191–192
2 Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review ofthe management of posterior communicating artery aneurysmsin the modern era. Surg Neurol Int 2010;1:88
3 Thiarawat P, Jahromi BR, Kozyrev DA, et al. MicroneurosurgicalManagement of Posterior Communicating Artery Aneurysm:A Contemporary Series from Helsinki. World Neurosurg 2017;101:379–388
4 Martins C, Yasuda A, Campero A, Rhoton AL Jr. Microsurgicalanatomy of the oculomotor cistern. Neurosurgery 2006;58(04,Suppl 2):ONS-220–ONS-227, discussion ONS-227–ONS-228
5 González-Darder JM, Quilis-Quesada V, Talamantes-Escribá F,Botella-Maciá L, Verdú-López F. Microsurgical Relations betweenInternal Carotid Artery-Posterior Communicating Artery (ICA-PComA) Segment Aneurysms and Skull Base: An AnatomoclinicalStudy. J Neurol Surg B Skull Base 2012;73(05):337–341
6 Youssef AS, Abdel Aziz KM, Kim EY, Keller JT, Zuccarello M, vanLoveren HR. The carotid-oculomotor window in exposure ofupper basilar artery aneurysms: a cadavericmorphometric study.Neurosurgery 2004;54(05):1181–1187, discussion 1187–1189
7 Kim YD, Elhadi AM, Mendes GA, et al. Quantitative study of theopticocarotid and carotid-oculomotor windows for the interpe-duncular fossa, before and after internal carotid artery mobiliza-tion and posterior communicating division. Neurosurgery 2015;11(Suppl 2):162–179, discussion 179–180
8 Kapsalaki EZ, Lee GP, Robinson JS III, Grigorian AA, Fountas KN.The role of intraoperative micro-Doppler ultrasound in verifyingproper clip placement in intracranial aneurysm surgery. J ClinNeurosci 2008;15(02):153–157
9 Sharma M, Ambekar S, Ahmed O, et al. The utility and limitationsof intraoperative near-infrared indocyanine green videoangio-graphy in aneurysm surgery. World Neurosurg 2014;82(05):e607–e613
10 Güresir E, Schuss P, Seifert V, Vatter H. Oculomotor nerve palsy byposterior communicating artery aneurysms: influence of surgicalstrategy on recovery. J Neurosurg 2012;117(05):904–910
11 Anan M, Nagai Y, Fudaba H, et al. Third nerve palsy caused bycompression of the posterior communicating artery aneurysmdoes not depend on the size of the aneurysm, but on the distancebetween the ICA and the anterior-posterior clinoid process. ClinNeurol Neurosurg 2014;123:169–173
12 Park SK, Shin YS, Lim YC, Chung J. Preoperative predictive value ofthe necessity for anterior clinoidectomy in posterior communi-cating artery aneurysm clipping. Neurosurgery 2009;65(02):281–285, discussion 285–286
13 Sade B, Kweon CY, Evans JJ, Lee JH. Enhanced exposure of carotico-oculomotor triangle following extradural anterior clinoidectomy:a comparative anatomical study. Skull Base 2005;15(03):157-–161, discussion 161–162
14 Kim JH, Kim JM, Cheong JH, Bak KH, Kim CH. Simple anteriorpetroclinoid fold resection in the treatment of low-lying internalcarotid-posterior communicating artery aneurysms. Surg Neurol2009;72(02):142–145
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Surgery of a Posterior Communicating Aneurysm González et al.156

Endoscopic Endonasal Odontoidectomy:Nuances of Neurosurgical Technique
Odontoidectomia endoscópica endonasal: nuances datécnica cirúrgica
Flavio Ramalho Romero1 Rodolfo Brum Vieira1 Bruno da Costa Ancheschi1
1Department of Neurosurgery, Universidade Estadual Paulista Júliode Mesquita Filho, Faculdade de Medicina Campus de Botucatu,Botucatu, SP, Brazil
Arq Bras Neurocir 2018;37:157–161.
Address for correspondence Flávio Ramalho Romero, MD, MSc, PhD,Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade deMedicina Campus de Botucatu, Botucatu, SP, Brazil(e-mail: [email protected]).
Introduction
Odontoidectomy is the treatment of choice for some diseasesthat cause irreducible ventral compression of the brainstem.1–3
Thetransoral routehasbeenusedformanyyearsas thestandardapproach to decompress the ventral craniovertebral junction(CVJ).1–4 However, this approach is associated with high com-plication rates involving swallowing and respiratory issues.1–5
Alfieri, in 2002,6 and Kassam, in 2005,7 were the pioneersto demonstrate that the endoscopic endonasal approach isfeasible to decompress the CVJ. The first performed ananatomical study, and the second used the endoscopicendonasal approach to treat a patient with ventral brainstemcompression due to rheumatoid pannus.6,7
Here, we present our series emphasizing the technicalnuances of endoscopic endonasal odontoidectomy.
Keywords
► craniocervicaljunction
► odontoidectomy► endoscopic
endonasal approach► transoral approach
Abstract Odontoidectomy is the treatment of choice for some diseases that cause irreducibleventral compression of the brainstem. In this study, we present our series emphasizingthe technical nuances of endoscopic endonasal odontoidectomy.
Palavras-chave
► transição crânio-cervical
► odontoidectomia► acesso endoscópico
endonasal► acesso transoral
Resumo Odontoidectomia é o tratamento de escolha para algumas doenças que cursam comcompressão irredutível do tronco encefálico. Neste trabalho, apresentamos nossa sérieenfatizando as nuances da técnica cirúrgica da odontoidectomia por via endonasalendoscópica.
receivedMay 20, 2018acceptedJune 5, 2018
DOI https://doi.org/10.1055/s-0038-1667181.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Technical Note | Nota Técnica 157

Casuistic
Weretrospectively reviewedaprospectivelycollecteddatabaseof all patients undergoing fully endoscopic endonasal surgerybetween 2009 and 2018. From this database, we identified 16patients (9 female and 7 male) treated by fully endoscopicendonasal odontoidectomy. The diagnoses were basilar im-pression in eight patients, rheumatoid pannus in six cases, andos odontoideum in two cases. The indication of surgery wasbased in the irreducible aspects of their conditions and theseverityofcompressionof thebrainstem.All basilar impressionpatients had irreducible subtype A according to the Goelclassification, while rheumatoid pannus and os odontoideumpatients had very severe brainstem compression with neuro-logical disabilities. All patients had signs ofmyelopathy, 13 hadneck pain (81.2%), and 6 had swallowing disturbances (37.5%).
Operative Technique
After general anesthesia, the patient is placed in proneposition with 3-point fixation and routinely receives 2 g ofcephazolin, intravenously. A binostril approach is performed.The middle and inferior turbinates are displaced laterally.Under endoscopic view (0-degree, 17 cm, 4 mm scope), theinferior, middle, and superior turbinates are identified, andthe mucosae of the inferior and middle turbinates are
injected with a solution of lidocaine 1% and epinephrine(1:100,000). The endoscope is gently advanced through thenasal floor to the choana (►Fig. 1).
When the nasopharyngeal mucosa is visualized, it is veryimportant to identify the landmarks. Eustachian tubes arethemain references to avoid an internal carotid artery injurythat runs posterolaterally, and the Rosenmuller fossae aredisplaced laterally. The mucosa incision is performed medi-ally to the Eustachian tubes, in a linear shape, over theanterior C1 tuberculus, advancing upward, until direct skel-etonization of the clivus and CVJ is obtained. Lateral andanterior fluoroscopy images or navigation devices should beused to confirm the position. Resection of the anteriorlongitudinal ligament is needed to access the atlantoaxialarticulation. The C1 anterior arch is removedwith a drill anda Kerrison punch in all our cases to have a good exposure ofodontoid process. After odontoid exposure, the removal isinitiated. The core of the odontoid is drilled out with adiamond drill and the residual shell of the odontoid isremoved before cutting the surrounding fibrous pathologictissue, if present, or sectioning of apical, alar, and cruciateligaments. The amount of removal depends on the abnor-mality to be treated. In patients with inflammatory condi-tions, such as rheumatoid pannus, thickening of thesurrounding tissue, including the ligaments, is mandatoryto have a good decompression (►Fig. 2).
Fig. 1 (A) Nasal cavity inspection showing inferior and middle turbinates and nasal septum. (B) View through the choana of nasopharyngealmucosa showing the Eustachian tube and the point of mucosal incision (�).
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Endoscopic Endonasal Odontoidectomy Romero et al.158

Closure is an important step. Cases of cerebrospinal fluid(CSF) leakmust be carefullymanaged. Abdominal fat and duralsealants are routinely used for this purpose, and a 48-hourlumbar drain is placed if CSF leak is present. Then, the naso-pharyngeal mucosa is closed, and nasal packing is performed.All patients were placed in ventral position and a occipito-cervical fusion was performed.
After the surgery, immediately removal of orotracheal tubeand restoring spontaneous ventilation is waited. Talking isallowed in thefirst postoperativeday if noCSF leak is observed.Otherwise, in cases of CSF leak, 3 days of bed rest are required.The nasal packing is removed after 2 days. Also, oral feedingcan be resumed in thefirst postoperative day, and a computedtomography (CT) scan is advised to confirmodontoid resectionand rule out early complications (►Figs. 3, 4 and 5).
Discussion
The CVJ ventral compression remains a challenge for neuro-surgeons. Congenital conditions, traumatic injuries, infec-tious diseases, inflammatory conditions, tumors, or otheracquired anatomic lesions may lead to basilar impression ofthe odontoid onto the brainstem and spinal cord. This
Fig. 2 Craniocervical junction (CVJ) after skeletonization. (A) Arrow indicates C1 anterior arch. (B) Drilling of C1 anterior arch. (C) Arrowindicates ventral C2 body. (D) Arrow shows odontoid process.
Fig. 3 (A) Preoperative sagittal computed tomography scan. (B) Preoper-ative T2 magnetic resonance imaging showing ventral compression ofbrainstem at craniovertebral junction.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Endoscopic Endonasal Odontoidectomy Romero et al. 159

compression results in neurologic impairment, most com-monly numbness and tingling in the limbs, early on, andlater, as the motor nerve weakens, sensitive disturbances,and sphincter control loss. Most of the times, surgicalintervention is needed to relieve compression and restorethe neurological function.3,5,7,8 Our casuistic was basicallycomposed of basilar impression (Goel A irreducible type),rheumatoid pannus and os odontoideum (congenital mal-formation) cases.
The transoral is the traditional approach used by most ofthe surgeons and remains as the gold standard for decom-
pression of this region.1–4 Many authors have reportedproblems in the postoperative management of thesepatients, mainly regarding swallowing and respiratory com-plications.9 Recently, the endoscopic endonasal approach forCVJ has beenproposed as an alternative to the transoral routein some selective cases with advantages over the traditionalroute, but also with limitations.8–14
The advantages include the fact that this is a well-tolerat-ed procedure by the patients, because it avoids soft or hardpalate cut, reducing the risks of food or liquid regurgitationto the nose due to palate incontinence. Also, tongue manip-ulation or glossotomy is not necessary, avoiding tongueedema, necrosis or ventilator impairment. Prompt and safeorotracheal extubation after the surgery is allowed, decreas-ing pulmonary infection rates.7–14 The risk of dysphagia isdecreased, when compared with the transoral approach,because the incision in the rhinopharynx muscle above thepalatal line is minimized, with lower rates of injury to theneural plexus in the oropharyngeal wall, allowing promptfeeding after the surgery.11 Regarding infection, the risk isreduced compared with the transoral approach due to lesscontamination of the surgical field with saliva and oralbacterial flora.11–14
Furthermore, one of the main advantages is the angle ofview of the odontoid in endoscopic approaches, allowing acaudal-cranial route and resection of anterior C1 arch ifnecessary. Some authors have advocated the preservationof the C1 anterior arch to keep the CVJ stable,15–17 but ourcases received a complementary occipito-cervical fusion,and, in our opinion, the exposure is very restricted withoutremoval of the C1 anterior arch. Also, opening the inferiorportion of the sphenoidal sinus wall through an endosinusalroute allows us to reach ventrally even in severe platybasiacases with high position of the dens.11,12
Fig. 4 (A) Preoperative sagittal computed tomography scan. (B) Postoperative sagittal computed tomography scan. (C) Preoperative coronalcomputed tomography scan. (D) Postoperative coronal computed tomography scan.
Fig. 5 Postoperative 3D computed tomography scan reconstruction.(A) Posterior view. (B) Anterior view. Yellow arrows indicate the part ofodontoid removed.
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Endoscopic Endonasal Odontoidectomy Romero et al.160

There are still limitations to this approach, which ischallenging for neurosurgeons due to the depth of the route,the narrowness of the corridor, and the risk of major neuro-logical disabilities related to the close relationship with thebrainstem and upper spinal cord. Specifically, the endoscopicapproach should be reserved for reference centers withwell-trained surgeons. Furthermore, the position of the dens inrelation to the palate is an important factor to take intoconsideration, as this approach is not considered a goodoption for dens located below the palate.18,19 Endoscopicendonasal odontoidectomy always lead to instability ofcranio-cervical junction by damaging regional ligaments,and occipito-cervical fusion is recommended to preventfuture problems.20
Conclusion
The endoscopic endonasal approach is a safe and effectiveoption for decompression of the CVJ. There are some advan-tages and some limitations to this technique. Decrease ofswallowing and respiratory issues are the main advantages.Position of dens in relation to the palate and learning curveare the major problems. Patient anatomy, disease character-istics and surgeon expertise must be considered whenchoosing the right approach. In our opinion, the transoraland the endoscopic endonasal approaches should be seen ascomplementary and not as alternatives.
Conflicts of InterestThe authors have no conflicts of interest to declare.
References1 Apuzzo ML, Weiss MH, Heiden JS. Transoral exposure of the
atlantoaxial region. Neurosurgery 1978;3(02):201–2072 Shaha AR, Johnson R, Miller J, Milhorat T. Transoral-transphar-
yngeal approach to the upper cervical vertebrae. Am J Surg 1993;166(04):336–340
3 Sakou T, Morizono Y, Morimoto N. Transoral atlantoaxial anteriordecompression and fusion. Clin Orthop Relat Res 1984;(187):134–138
4 Menezes AH, VanGilder JC. Transoral-transpharyngeal approachto the anterior craniocervical junction. Ten-year experience with72 patients. J Neurosurg 1988;69(06):895–903
5 Seker A, Inoue K, Osawa S, Akakin A, Kilic T, Rhoton AL Jr.Comparison of endoscopic transnasal and transoral approaches
to the craniovertebral junction. World Neurosurg 2010;74(06):583–602
6 Alfieri A, Jho HD, Tschabitscher M. Endoscopic endonasal approachto the ventral cranio-cervical junction: anatomical study. ActaNeurochir (Wien) 2002;144(03):219–225, discussion 225
7 Kassam AB, Snyderman C, Gardner P, Carrau R, Spiro R. Theexpanded endonasal approach: a fully endoscopic transnasalapproach and resection of the odontoid process: technical casereport. Neurosurgery 2005;57(1, Suppl)E213, discussion E213
8 Wu JC, Mummaneni PV, El-Sayed IH. Diseases of the odontoid andcraniovertebral junction with management by endoscopicapproaches. Otolaryngol Clin North Am 2011;44(05):1029–1042
9 Crockard HA. Transoral surgery: some lessons learned. Br J Neuro-surg 1995;9(03):283–293
10 Goldschlager T, Hartl R, Greenfield JP, et al. The endoscopicendonasal approach to the odontoid and its impact on earlyextubation and feeding. J Neurosurg 2014;31:1–8
11 Van Abel KM, Mallory GW, Kasperbauer JL, et al. Transnasalodontoid resection: is there an anatomic explanation for differingswallowing outcomes? Neurosurg Focus 2014;37(04):E16
12 WelchWC, Kassam A. Endoscopically assisted transoral-transphar-yngeal approach to the craniovertebral junction. Neurosurgery2003;52(06):1511–1512
13 Wolinsky JP, Sciubba DM, Suk I, Gokaslan ZL. Endoscopic image-guided odontoidectomy for decompression of basilar invaginationvia a standard anterior cervical approach. Technical note.J Neurosurg Spine 2007;6(02):184–191
14 Mummaneni PV, Haid RW. Transoral odontoidectomy. Neurosur-gery 2005;56(05):1045–1050, discussion 1045–1050
15 Shetty A, Kumar A, Chacko A, Guthe S, Kini AR. Reductiontechniques in themanagement of atlantoaxial subluxation. IndianJ Orthop 2013;47(04):333–339
16 Magrini S, Pasquini E, Mazzatenta D, Mascari C, Galassi E, Frank G.Endoscopic endonasal odontoidectomy in a patient affected byDown syndrome: technical case report. Neurosurgery 2008;63(02):E373–E374, discussion E374
17 El-Sayed IH, Wu JC, Dhillon N, Ames CP, Mummaneni P. Theimportance of platybasia and the palatine line in patient selectionfor endonasal surgery of the craniocervical junction: a radiographicstudy of 12 patients. World Neurosurg 2011;76(1-2):183–188,discussion 74–78
18 de Almeida JR, Zanation AM, Snyderman CH, et al. Defining thenasopalatine line: the limit for endonasal surgery of the spine.Laryngoscope 2009;119(02):239–244
19 El-Sayed IH, Wu J-C, Ames CP, Balamurali G, Mummaneni PV.Combined transnasal and transoral endoscopic approaches to thecraniovertebral junction. J Craniovertebr Junction Spine 2010;1(01):44–48
20 Duntze J, Eap C, Kleiber JC, et al. Advantages and limitations ofendoscopic endonasal odontoidectomy. A series of nine cases.Orthop Traumatol Surg Res 2014;100(07):775–778
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Endoscopic Endonasal Odontoidectomy Romero et al. 161

Erratum - lnformation Sources and Decision-Making in Neurosurgery: Results of a Survey ofMembers of the Brazilian Neurosurgery Society
Errata - Fontes de informação e tomadas de decisão emneurocirurgia: resultados de uma pesquisa de membrosda Sociedade Brasileira de Neurocirurgia
Rodrigo Gorayeb1 Maria João Forjaz2 Antônio Gonçalves-Ferreira3 Joaquim Ferreira4
1Laboratory of Clinical Pharmacology, Faculty of Medicine,Universidade de Lisboa, Lisboa, Portugal
2National School of Public Health, Institute of Health Carlos III andREDISSEC, Biscay, Spain
3Clínica Universitária de Neurocirurgia e Instituto de Anatomia,Faculty of Medicine, Universidade de Lisboa, Lisbon, Portugal
4 Instituto de Medicina Molecular, Lisbon, Portugal; Laboratory ofClinical Pharmacology and Therapeutics, Faculty of Medicine,Universidade of Lisboa, Lisbon, Portugal; Campus NeurológicoSénior, Torres Vedras, Lisbon, Portugal
Arq Bras Neurocir 2018;37:162–163.
Address for correspondence Rodrigo Gorayeb, Faculdade deMedicina, Universidade de Lisboa, Avenida Professor Egas Moniz,1649-028, Lisboa, Portugal (e-mail: [email protected]).
ERRATUM Rio de Janeiro, May 28, 2018
Dear readers,In the article lnformation Sources andDecision-Making in Neurosurgery: Results of a Survey ofMembers of the Brazilian Neurosurgery Society (Arq Bras Neurocir 2018; doi 10.1055/s-0038-1656716), published online in Arq Bras Neurocir in May 2018, where it reads:
Rodrigo Gorayeb11Laboratory of Clinical Pharmacology, Faculty of Medicine, Universidade de Lisboa, Lisboa,Portugal
It should read:
Rodrigo Gorayeb1 Maria João Forjaz2 Antônio Gonçalves-Ferreira3 Joaquim Ferreira41Laboratory of Clinical Pharmacology, Faculty of Medicine, Universidade de Lisboa, Lisboa,Portugal2National School of Public Health, Institute of Health Carlos III and REDISSEC, Biscay, Spain3Clínica Universitária de Neurocirurgia e Instituto de Anatomia, Faculty of Medicine,Universidade de Lisboa, Lisbon, Portugal4Instituto de Medicina Molecular, Lisbon, Portugal; Laboratory of Clinical Pharmacologyand Therapeutics, Faculty of Medicine, Universidade of Lisboa, Lisbon, Portugal; CampusNeurológico Sénior, Torres Vedras, Lisbon, Portugal
DOI https://doi.org/10.1055/s-0038-1667058.ISSN 0103-5355.
Copyright © 2018 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
ErratumTHIEME
162

Rio de Janeiro, 28 de maio de 2018
Prezados leitores,No artigo Fontes de informação e tomadas de decisão em neurocirurgia: resultados de umapesquisa de membros da Sociedade Brasileira de Neurocirurgia (Arq Bras Neurocir 2018; doi10.1055/s-0038-1656716), publicado online em Arq Bras Neurocir emmaio de 2018, onde selê:
Rodrigo Gorayeb11Laboratory of Clinical Pharmacology, Faculty of Medicine, Universidade de Lisboa, Lisboa,Portugal
Lê-se:
Rodrigo Gorayeb1 Maria João Forjaz2 Antônio Gonçalves-Ferreira3 Joaquim Ferreira41Laboratory of Clinical Pharmacology, Faculty of Medicine, Universidade de Lisboa, Lisboa,Portugal2National School of Public Health, Institute of Health Carlos III and REDISSEC, Biscay, Spain3Clínica Universitária de Neurocirurgia e Instituto de Anatomia, Faculty of Medicine,Universidade de Lisboa, Lisbon, Portugal4Instituto de Medicina Molecular, Lisbon, Portugal; Laboratory of Clinical Pharmacologyand Therapeutics, Faculty of Medicine, Universidade of Lisboa, Lisbon, Portugal; CampusNeurológico Sénior, Torres Vedras, Lisbon, Portugal
ERRATA
Arquivos Brasileiros de Neurocirurgia Vol. 37 No. 2/2018
Erratum 163

Instructions to Authors
ISSN 0103-5355
Brazilian Neurosurgery (Arquivos Brasileiros de Neurocirurgia), an offi cial journal of the Brazilian Society of Neurosurgery (Sociedade Brasileira de Neurocirurgia) and Portuguese Language Neurosurgery Society (Sociedades de Neurocirurgia de Língua Portuguesa), aims to publish scientifi c works in Neurosurgery and related fi elds, unpublished and exclusive. As from January 2018, the journal publishes papers written in English with Portuguese abstracts.
Submitted articles shall be placed as one of the following categories:
• Original: result of clinical, epidemiological or experimental research. Abstracts of theses and dissertations.
• Review: review and update synthesis of spe-cifi c themes, with critical analysis and con-clusions. Databases and the period range must be specifi ed.
• Case Report: presentation, analysis and discus-sion of cases that present relevant interest.
• Technical Note: note on surgery techniques and/or surgical instruments.
• Miscellaneous: neurosurgery history, pro-fessional practice, medical ethics and other pertinent matters to the journal purpose.
• Letter to the Editor: critics and comments pre-sented in a brief ethical and instructive man-ner about published content in this journal. The copyright is safe to authors of the aimed subject. Letters, when accepted, will be pub-lished with authors reply.
General standards for publishing
• Article fi les for publishing must be submit-ted to the Editor, via http://www.editorial-manager.com/bns/.
• All articles will have a double blinded peer-review process, and no Article Publishing Charge (APC) – society funded. More about Open Access at http://open.thieme.com.
• Only new unpublished manuscripts will be ac-ceptable. Submitted articles must not be fullyor partially submitted to any other journal.
• The editorial board may reject or suggest changes in order to improve the clarity and structure of the text and maintain uniform-ity with the journal policy.
• Copyrights of articles published in the journal will belong exclusively to the Brazilian Neurosurgery and Thieme Publicações Ltda. The reproduction of articles or illustrations without prior consent is prohibited.
Standards for submission
Authors must send the following fi les:
1. Pub Letter (text fi le) stating the article has not yet been published partially or fully or submitted concomitantly to other journal.
2. Manuscript (text fi le).
3. Figures (Tiff , Jpeg, Pdf, Indd) sent in separate fi les with minimum resolution of 300 dpi.
4. Tables, charts and graphics (text fi le) sent separately.
Standards for articles structure
Articles must be structured with all the follow-ing items and paginated accordingly:
1. Title page: article title both in Portuguese and English; full name of all authors; academic or professional affi liation of each author; institutions names where the study took place; running title; corresponding author name, degree, full address, e-mail and phone number; followed by ICMJE CoI forms (http://www.icmje.org/confl icts-of-interest/).
2. Abstract: original articles need structured abstract with 250 words at the most: objec-tive, methods, results and conclusions; review articles, case reports, technical notes and miscellaneous need no structured abstract. Following the abstract comes keywords (six at the most), based on MeSH (Medical Subject Headings), published in Medline and available at: www.ncbi.nlm.nih.gov/mesh/.
3. Portuguese abstract: Portuguese version of title, abstract and keywords based on DeCS (Descritores em Ciências da Saúde, http://decs.bvs.br).
4. Main text: introduction; casuistry or mate-rial and methods; results; discussion; conclu-sion; acknowledgments.
5. References: number references as they are fi rst cited in the text with Arabic numerals. Use Vancouver style; list all authors until the sixth, using et al. after the third when more than six; when reference authors are cited in the text cite the fi rst and et al. for references with more that two authors; unpublished data or personal communication must be cited as such between parentheses and cannot be listed as reference; use journal abbreviation from Index Medicus; use the following examples:
Journal Article
Agner C, Misra M, Dujovny M, Kherli P, Alp MS, Ausman JI. Experiência clínica com oxime-tria cerebral transcraniana. Arq Bras Neurocir 1997;16(1):77–85
Book Chapter
Peerless SJ, Hernesniemi JA, Drake CG. Surgical management of terminal basilar and posterior cerebral artery aneurysms. In: Schmideck HH, Sweet WH, editors. Operative neurosurgical techniques. 3rd ed. Philadelphia: WB Saunders;1995:1071–86.
Book
Melzack R. The puzzle of pain. New York: Basic Books Inc Publishers; 1973.
Theses and dissertations
Pimenta CAM. Aspectos culturais, afetivos e terapêuticos relacionados à dor no câncer. [thesis]. São Paulo: Escola de Enfermagem da Universidade de São Paulo; 1995.
Annals and other congresso publications
Corrêa CF. Tratamento da dor oncológica. In: Corrêa CF, Pimenta CAM, Shibata MK, editores. Arquivos do 7º Congresso Brasileiro e Encontro Internacional sobre Dor; 2005 outubro 19–22; São Paulo, Brasil. São Paulo: Segmento Farma. pp. 110–20.
Available Article in ahead of print
International Committee of Medial Journal Editors. Uniform requirements for manuscripts submitted to biomedical journals. Writing and editing for biomedical publication. Updated October 2007. Available at: http://www.icmje.org. Access in: June 12, 2008.
6. Tables and charts: numbered by Arabic numerals according to its citation in the text; edited in double space, using separate sheets per table/chart; title right above; note, abbreviations, legends must follow right under;introduce only essential tables and charts; files must come separately.
8. Figures: digital formats (Tiff , Jpeg, Pdf, Indd) with minimum resolution of 300 dpi (trim 7.5 or 15 cm).
9. Legends and captions: numbered by Ara-bic numerals according to its citation in the text; edited in double space, using separate fi les; identify eventual labels present in the fi gure (arrows, characters, lines etc.); image previously published must have publisherauthorization and credits.
10. Ethics standards: No data or image identify-ing a patient can be used without formal consent; studies using human beings or animal trials must follow ethical standards from the International Committee of Medical Journals Editors – ICMJE, as well as approval of original institution’s Eth-ics Committee; confl icts of interest must have aICMJE form fi lled in by all authors (http://www.icmje.org/confl icts-of-interest/); commercial marks should be avoided; authors are the sole responsible for opinions and concepts in the published articles, as well as for the reference accuracy.
11. Other information: PDF proof will be sent to corresponding author for eventual queries and/or approval within 72 hours; except measure units, acronyms must be spelled out after its fi rst time mentioned.
Secretariat: R. Abílio Soares, 233/143, Paraíso. 04005-001, São Paulo, SP, Brazil. Phone:(+55 11) 3051-6075.Home page: www.sbn.com.br. e-mail: [email protected]


ADQUIRA JÁ EM http://www.thiemerevinter.com.br
Siga-nos: Facebook/ThiemeRevinter
A obra mais aguardada em Neurocirurgia!
MANUAL DE NEUROCIRURGIAOitava Edição
Mark S. Greenberg
Em sua Oitava Edição atualizada, o Manual de Neurocirurgia tem desfrutado de prestígio lendário nas prateleiras de todos os departamentos de neurocirurgia do mundo, por mais de um quarto de século. Reconhecido por sua abrangência e acessibilidade, este guia portátil, em um único volume, é o recurso indispensável para qualquer profissional envolvido no cuidado de pacientes com distúrbios do sistema nervoso central – tanto para residentes em neurocirurgia e enfermeiros quanto para especialistas e profissionais afins da área médica.
Este clássico da literatura abrange toda a extensão e profundidade da neurociência, incluindo distúrbios neurológicos hereditários e adquiridos, anomalias do desenvolvimento, além de tópicos mais obscuros, como toxinas que afetam os sistemas nervosos central e periférico. O texto também inclui condições tratadas primariamente por neurologistas, que podem vir a ser tratadas por um neurocirurgião, como Parkinsonismo, esclerose múltipla, doenças do neurônio motor e demência. As informações mais recentes sobre anatomia, fisiologia, diagnóstico diferencial e princípios atuais do tratamento não cirúrgico e cirúrgico são fornecidas, abrangendo todas as faixas etárias, desde as condições pediátricas até as geriátricas.
= Gráficos expandidos e ilustrações em quatro cores= Mais de 1600 páginas de informação prática, incluindo milhares de citações
bibliográficas, referências úteis e um índice detalhado= Princípios dos cuidados neurocríticos, com uma visão abrangente das
condições, desde SAH até traumatismo craniano e medular, incluindo complicações como perda de sal cerebral, ressangramento, vasospasmo e morte cerebral.
Abrangente e convenientemente compacto, esta é a referência diária indispensável, o parceiro de estudos perfeito para revisão e concursos, ideal para provas de título. É, com certeza, uma obra valiosa para legiões de residentes em neurocirurgia e uma ferramenta essencial para qualquer profissional que trabalhe com neurociência.
Medone Neurosurgery é a fonte online em neurocirurgia mais abrangente do mundo. Para uma avaliação gratuita, acesse a página: http://thieme.com/eneurotrial
1.662 Páginas – Papel CouchéFormato : 14 x 21 cmBrochuraRicamente Ilustrado em 4 CoresISBN: 978-85-67661-65-0Especialidades: Neurocirurgia, Neurologia
A obra mais aguardada em Neurocirurgia!