Embed Size (px)
Citation preview

IMAGING
Brain Infection from Mycobacterium chimaera: A Case Report
Mariam Mansour1 & Valerio Vitale1 & Oriela Rustemi2 & Andrea Lupi3 & Daniela Danieli4 & Mariangela Novello4&
Vinicio Manfrin5& Mariano Zanusso2
Accepted: 15 November 2019 /Published online: 8 December 2019# Springer Nature Switzerland AG 2019
AbstractWe describe the first case report of pathology-proven brain infection by Mycobacterium chimaera (MC). A 35-year-old male,previously operated in 2010 of aortic valve and ascending aortic replacement, was addressed to our hospital for the acute onset ofaphasia preceded by absence. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed multiple left frontaland temporal cortical-subcortical lesions. During hospitalization the patient never presented fever and cerebrospinal fluid (CSF),PCR, FilmArray and blood tests were within normal ranges. Transesophageal echocardiography showed no cardiac abnormal-ities. A thorax-abdomenCTscanwas performed, revealing no extracranial abnormalities, and a whole body PET-CTscan showeda high uptake of brain lesions. Considering clinical results and the suspect of a tumoural lesion, the patient underwent surgery,where a left frontal enhanced nodular lesion was removed. Pathology finally revealed it was an abscess caused byMycobacteriumchimaera. This case confirms thatMycobacterium chimaera infection spread can be very subtle and diagnosis a real challenge,particularly years after surgery. We would like to underline the importance of suspecting an atypical infection source related to ahistory of cardiothoracic surgery, given a non-specific MR pattern and subtle clinical and laboratory findings.
Keywords Mycobacterium chimaera . MRI . Abscess . Brain infection
Introduction
Mycobacterium chimaera is a nontuberculous mycobacteri-um, causing invasive infections following cardiothoracic sur-gery [1]. In particular, it was found that heater-cooler units(HCU) of extracorporeal circulation are responsible of infec-tion’s spread [2]. Probably HCU contamination happens dur-
ing its production process; at that point,M. chimaera-contain-ing bioaerosols, which are released in the operating room bythe contaminated water tank (and HCU system), contaminateimplantation devices [3].
These infections are very subtle and have a high mortalityrate despite therapy [4]. We report a case of proven exclusivebrain infection from Mycobacterium chimaera, the first de-scribed to our knowledge.
Case Description
A 35-year-old immunocompetent male, who in 2010underwent aortic valve and ascending aortic replacement sur-gery, was addressed to our hospital in January 2018 for theacute onset of aphasia preceded by absence. An unenhancedCT scan revealed multiple left frontal and temporal cortical-subcortical hypoattenuated areas, suspicious of subacute isch-aemic lesions of middle cerebral artery territory. MR investi-gation performed immediately after, using a 1.5 Tesla scanner(Siemens, Erlangen, Germany), confirmed a high T2-weighted (w) signal in the left fronto-temporal cortical-sub-cortical region, with high ADC values, and an additional
This article is part of the Topical Collection on Imaging
* Mariam [email protected]
1 Neuroradiology Unit, San Bortolo Hospital, AULSS 8 Berica,Vicenza, Italy
2 Neurosurgery Unit, San Bortolo Hospital, AULSS 8 Berica,Vicenza, Italy
3 Nuclear Medicine Unit, San Bortolo Hospital, AULSS 8 Berica,Vicenza, Italy
4 Pathology Unit, San Bortolo Hospital, AULSS 8 Berica,Vicenza, Italy
5 Infectious Disease Unit, San Bortolo Hospital, AULSS 8 Berica,Vicenza, Italy
SN Comprehensive Clinical Medicine (2020) 2:82–86https://doi.org/10.1007/s42399-019-00193-z

similar but smaller abnormality in the left thalamus, with onlya slight DWI hypersignal and no restriction. All lesions re-vealed some T2* magnetic susceptibility content. MR angi-ography showed normal flow signal within intracranialarteries.
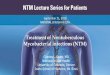
Gadolinium injection revealed some left fronto-temporalnodular-like lesions of contrast enhancement, surrounded byvasogenic oedema with nearby dural and leptomeningeal en-hancement (Fig. 1).
Based onMRI findings, clinical status and patient’s history(episodes of subtle fever during the last year, previous heartsurgery), infective brain localization was first suspected.
Nevertheless, during hospitalization the patient neverpresented fever, inflammatory markers were within nor-mal range and blood culture was negative. Cerebrospinalfluid (CSF) analysis showed only very mild increase ofproteins, cells and glucose, with negative PCR andFilmArray. A transesophageal echocardiography showedno cardiac abnormalities. Consequently, the alternative
diagnosis of a brain tumoural lesion was taken intostrong account. Therefore, thorax-abdomen CT scan wascarried out, reporting no extracranial abnormalities. Anadditional whole body PET-CT scan showed only a highuptake of the brain lesions, but no other systemiclocalization.
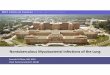
During the time of clinical investigation (14 days), thepatient’s neurological condition was progressively deteri-orating; therefore, a second MRI was performed; thistime using a 3 Tesla scanner (Siemens, Erlangen,Germany), which revealed the extension of two lesionsin the left frontal and temporal region. Further MR anal-ysis of the lesions, using dynamic susceptibility contrastperfusion (DSC-PWI) and MR spectroscopy (single andmultivoxel; TE 135 ms), demonstrated no significant per-fusion abnormalities and an increase of choline/creatine(Cho/Cr) and choline/N-acetil-aspartate (Cho/NAA) ratioswith a small abnormal peak in the lipid-lactate region(Fig. 2).
Fig. 1 MR images obtained witha 1.5 Tesla scanner showmultifocal oedematous lesionswithin the left hemisphere, in theleft thalamus, the opercular aspectof frontal-temporal region and thefrontal mesial region. Axial non-enhanced T1w image (A) showshypersignal within the thalamicand fronto-temporal opercular re-gion, surrounded by a largevasogenic oedema, better detect-ed in T2w images (B); lesionsshow a markedly low signal con-tent in both T2w and T2* images(B, C) and have a very high up-take of contrast medium,highlighting consistent involve-ment of adjacent leptomeninges(D)
SN Compr. Clin. Med. (2020) 2:82–86 83

Considering clinical progression and the consistentsuspect of a tumoural lesion, the patient underwent sur-gery, where a left fronto-temporal enhanced nodularitywas removed.
Histological analysis demonstrated a diffuse epithelioidgranulomatous inflammatory tissue containing few giant cells,and no caseous necrosis or neutrophilic abscesses (Fig. 3).Investigation was implemented with immunohistochemicalstaining, using rabbit polyclonal antibody (Cat.M7259;Abcam) against Mycobacterium bovis, known to cross reactwith both tuberculous and nontuberculous Mycobacteria ofthe avium complex, including M. chimaera (Fig. 4).
Just few Mycobacteria were identified within the granulo-mas by the immunostainings on paraffin-embedded tissues,and subsequent microbiological investigations confirmed thepresence ofMycobacterium chimaera on a fresh sample of thelesion.
Fig. 3 Brain parenchima showing a non-necrotizing granulomatous in-flammation with epithelioid histiocytes and lymphocyte (H.E. 10x OM)
Fig. 2 MRI images performedwith a 3T scanner showed nosignificant restriction values oflesions (left thalamus andipsilateral fronto-temporal oper-cular region) in ADC map (A), aswell as perfusion rCBV values(B) remained within symmetricalranges compared to normal cere-bral tissue. Single-voxel MRspectroscopy, using a TE of135 ms (C), showed an increasedratio of Cho/Cr and Cho/NAA adand an abnormal peak in the lipid-lactate region of the spectra. PET-CT (D) secondarily fused withrecent MR T2w images on thesame planes revealed an unspe-cific high uptake of the target le-sions and a large photopenic sur-rounding area; also, a reduceduptake in the left thalamus ispresent
84 SN Compr. Clin. Med. (2020) 2:82–86

Discussion
Mycobacterium chimaera has been classified withinMycobacterium avium complex (MAC) species [5]. In recentyears, it has been highlighted for subtle infections followingcardiac surgery, with an interval of up to some years fromsurgery to clinical onset [3]. Infections have been reportedin different European countries (Table 1) [6–12]. Recently,seven cases of infections from M. chimaera after cardiac sur-gery have been reported in Italy, with an average latency be-tween surgery and infection of 2 years [13]. This is the firstreported case with exclusive intracranial infection fromMycobacterium chimaera.
MAC infections are typical in immunosuppressed patientsand extremely rare in immunocompetent subjects [14–16].IntracranialMycobacterium infections manifest with granuloma-tous lesions and leptomeningeal involvement. Granulomatouslesions may have caseous or non-caseous content, determiningdifferent MR signal changes. Non-caseous granulomas mayhave a low signal on T1-weighted and a high signal on T2-
weighted images, with a homogenous contrast enhancement.Low T1 and T2 signal are more typical of caseous lesions,depending on the presence of both gliosis and solid caseation,and diffusion restriction is influenced by caseous content withinthe lesion [14–17].
In our case, lesions presented with high T2 signal, showing apseudo-nodular pattern visible only in contrast-enhanced T1wimages. There was no substantial diffusion restriction. All le-sions presented T2* magnetic susceptibility content. The pres-ence of nearby leptomeningeal involvement could suggest aninfectious disease. SimilarMRI patterns can indicate alternativediagnosis (e.g. tumoural lesions, noninfective granulomatousdisease) [17]. Therefore, clinical history and CSF/blood testsare very important to give consistency to the diagnostic suspect,as well as PET-CTscan, which may identify a second site of theinfection (e.g. cardiac surgical site). Unfortunately patients withMC infections may show non-specific clinical signs and symp-toms, and blood cultures may result negative [1]. So, in case ofa previous cardiac surgery, atypical infections as MC must def-initely be taken into account.
MC infection therapy is similar to that used for MAC in-fections and administered for at least 6 months [5].
After surgical and prolonged medical therapy, our patientimproved, with reduction of brain lesions, but is now stillunder follow-up.
Conclusion
We report the first case of pathology-proven and exclusivebrain infection from Mycobacterium chimaera. It confirmsthat infection spread can be very subtle and diagnosis a realchallenge, particularly years after surgery.
With this case, we would like to underline the importanceof suspecting an atypical infection source related to a historyof cardiothoracic surgery, given a non-specific MR patternand subtle clinical and laboratory findings.
Table 1 Reported disseminated Mycobacterium chimaera infections related to cardiothoracic surgery in European countries
Country Year Number of cases Brain localization(N°)
Haller et al. [10] Germany 2016 5 Yes (1)
Sax et al. [6] Switzerland 2015 6 No
Kholer et al. [8] SwitzerlandThe NetherlandsGermany
2015 6 (already in Sax et al.)31 (already in Haller et al.)
Yes (2)
Boni et al. [2] Switzerland 2017 9 (5 already in Sax et al.) No
Scriven et al. [12] The United Kingdom 2018 30 Yes (4 post-mortem examinations)
Acosta et al. [11] Spain 2018 1 No
HPSC [9] Ireland 2016 4 Not specified
ECDPC [7] France 2016 2 Not specified
Cappabianca [13] Italy 2018 7 Yes (1)
Fig. 4 Filamentous organisms are highlighted by a polyclonalantimycobacteria antibody
SN Compr. Clin. Med. (2020) 2:82–86 85

Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
Ethical Approval All procedures performed in studies involving humanparticipants were in accordance with the ethical standards of the institu-tional and/or national research committee and with the 1964 HelsinkiDeclaration and its later amendments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individualparticipants included in the study.
References
1. O’Neil CR, Taylor G, Smith S, Joffe AM, Antonation K, Shafran S,et al. Mycobacterium chimaera infection after aortic valve replace-ment presenting with aortic dissection and pseudoaneurysm. OpenForum Infect Dis. 2018;5(2):ofy018. https://doi.org/10.1093/ofid/ofy018.
2. Böni C, Al-Sheikh M, Hasse B, Eberhard R, Kohler P, Hasler P,et al. Multimodal imaging of choroidal lesions in disseminatedMycobacterium chimaera infection after cardiothoracic surgery.Retina. 2019;39(3):452–64. https://doi.org/10.1097/IAE.0000000000001991.
3. Marra AR, Diekema DJ, Edmond MB. Mycobacterium chimaerainfections associated with contaminated heater-cooler devices forcardiac surgery: outbreakmanagement. Clin Infect Dis. 2017;65(4):669–74. https://doi.org/10.1093/cid/cix368.
4. Moutsoglou DM, Merritt F, Cumbler E. DisseminatedMycobacterium chimaera presenting as vertebral osteomyelitis.Case Rep Infect Dis. 2017;2017:9893743. https://doi.org/10.1155/2017/9893743.
5. Chiesi S, Piacentini D, Salerno ND, Luise D, PeracchiM, Concia E,et al. Disseminated Mycobacterium chimaera infection after openheart surgery in an Italian woman: a case report and a review of theliterature. Infez Med. 2017;25(3):267–9.
6. Sax H, Bloemberg G, Hasse B, Sommerstein R, Kohler P,Achermann Y, et al. Prolonged outbreak of Mycobacterium chi-maera infection after open chest heart surgery. Clin Infect Dis.2015;61:67–75.
7. European Centre for Disease Prevention and Control. Invasive car-diovascular infection by Mycobacterium chimaera associated with3T heater-cooler system used during open-heart surgery – 18November 2016. Stockholm: ECDC; 2016.
8. Kohler P, Kuster SP, Bloemberg G, Schulthess B, Frank M, TannerFC. Healthcare-associated prosthetic heart valve, aortic vascular
graft, and disseminated Mycobacterium chimaera infections subse-quent to open heart surgery. Eur Heart J. 2015;36(40):2745–53.https://doi.org/10.1093/eurheartj/ehv342.
9. Health protection surveillance centre (HPSC), Report oh case find-ing investigation to identify Mycobacteria chimaera infections po-tentially associated with heater-cooler units used during cardiotho-racic surgery in Ireland- November 2016.
10. Haller S, Holler C, Jacobshagen A, Hamouda O, Abu Sin M,Monnet DL, et al. Contamination during production of heater-cooler units by Mycobacterium chimaera potential cause for inva-sive cardiovascular infections: results of an outbreak investigationin Germany, April 2015 to February 2016. Euro Surveill.2016;21(17). https://doi.org/10.2807/1560-7917.ES.2016.21.17.30215.
11. Acosta F, Pérez-Lago L, Ruiz Serrano MJ, Marín M, Kohl TA,Lozano N, et al. Fast update of undetected Mycobacterium chimae-ra infections to reveal unsuspected cases. J Hosp Infect. 2018.https://doi.org/10.1016/j.jhin.2018.08.018.
12. Scriven JE, Scobie A, Verlander NQ, Houston A, Collyns T, CajicV, et al. Mycobacterium chimaera infection following cardiac sur-gery in the United Kingdom: clinical features and outcome of thefirst 30 cases. Clin Microbiol Infect. 2018;24(11):1164–70. https://doi.org/10.1016/j.cmi.2018.04.027.
13. Cappabianca G, Paparella D, D'Onofrio A, Caprili L, Minniti G,Lanzafame M, et al. Mycobacterium chimaera infections followingcardiac surgery in Italy: results from a national survey endorsed bythe Italian Society of Cardiac Surgery. J Cardiovasc Med(Hagerstown). 2018;19(12):748–55. https://doi.org/10.2459/JCM.0000000000000717.
14. Dubbioso R, Cerillo I, D'Arco F, D'AmicoA, Pettinato G, BoldoriniR, et al. Isolated intracranial Mycobacterium avium complex gran-ulomas in an immune-competent man. J Neurol Sci. 2015;349(1-2):264–5. https://doi.org/10.1016/j.jns.2015.01.020.
15. Cai R, Qi T, Lu H. Central nervous system infection with non-tuberculous mycobacteria: a report of that infection in two patientswith AIDS. Drug Discov Ther. 2014;8(6):276–9. https://doi.org/10.5582/ddt.2014.01047.
16. Phowthongkum P, Puengchitprapai A, Udomsantisook N,Tumwasorn S, Suankratay C. Spindle cell pseudotumor of the brainassociated with Mycobacterium haemophilum andMycobacteriumsimiae mixed infection in a patient with AIDS: the first case report.Int J Infect Dis. 2008;12(4):421–4. https://doi.org/10.1016/j.ijid.2007.11.010.
17. da Rocha AJ, Maia AC Jr, Ferreira NP, do Amaral LL.Granulomatous diseases of the central nervous system. Top MagnReson Imaging. 2005;16(2):155–87.
Publisher’s Note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
86 SN Compr. Clin. Med. (2020) 2:82–86