Embed Size (px)
Citation preview

Br Heart J 1993;69:332-337
/B Adrenoreceptor subtype cross regulation in thehuman heart
J A Hall, A Ferro, J E C Dickerson, M J Brown
AbstractObjectives-To find out in a prospec-
tive study whether p1, blocker treatmentcauses selective P12 adrenoreceptor sensi-tisation, and to find whether such sensi-tisation is confined to the heart.Design-A placebo controlled cross
over study of two weeks of selective /1,blocker treatment with 10 mg of bisopro-lol daily.Subjects-Six healthy volunteers.Outcome measures-Three days after
stopping the 10 mg of bisoprolol or place-bo, subjects underwent treadmill exer-cise (to measure cardiac /1, receptorresponsiveness) and were given salbuta-mol injections (to measure cardiac 1P2receptor responsiveness). Secondary endpoints were the responses of serumpotassium, glucose, and insulin to P2stimulation.Results-There was no difference in
exercise induced increases in heart rate,but after treatment with bisoprolol thedose of salbutamol required to increaseheart rate by 40 beats/min was 19 ,ug/kgcompared with 2-9 ug/kg after placebo (p< 0.005). The fall in diastolic blood pres-sure was not significantly different on thetwo occasions. Hypokalaemia induced bysalbutamol, but not hyperglycaemia orhyperinsulinaemia, was enhanced afterbisoprolol.
Conclusion-This study shows thattreatment with a /1, blocker in vivo leadsto sensitisation of cardiac /12 adrenore-ceptors but not cardiac p1 adrenorecep-tors or vascular /12 receptors. Thispreviously unrecognised form of receptorcross sensitisation in the heart maynoticeably diminish the efficacy of selec-tive 01' blockade in preventing arrhyth-mias in patients with ischaemic heartdisease. These findings reopen the ques-tion of which type of /1 blocker is moreappropriate for such patients.
(Br Heart J 1993;69:332-337)
The /B blockers are among the most widelyused drugs in clinical practice. Both ,I selec-tive and non-selective blockers seem to beequally effective as antihypertensive andantianginal agents, but this has masked ourignorance about which type of fl blocker is tobe preferred for achieving the long-termobjective in both groups of patients, namely a
reduction in the incidence of myocardialinfarction and its complications. The possibil-ity that so called cardioselective fi blockersoffer less cardioprotection than non-selectivefi blockers has existed since the human heartwas found to differ from other species in not,after all, being itself f, selective.' About 30%of the # receptors are of the fl2 subtype2 andselective f2 receptor stimulation causes tachy-cardia.3
Chronic ,B blockade may paradoxicallyincrease the sensitivity of patients to sympa-thetic stimulation, although in the past thishas been considered important only duringthe immediate withdrawal period.4 Recent invitro studies, however, on strips of atrialmyocardium from patients still receiving fi,blockers have shown a previously unrecog-nised cross regulatory effect of chronic fi,blockade on other receptors coupled toadenyl cyclase, including a selective 10 foldincrease in sensitivity to /2 stimulation byadrenaline, with no change in sensitivity to P,stimulation.5-7 Therefore, such patients maybe at enhanced risk of tachycardia induced byadrenaline, and have indeed been found to befour times more sensitive to fl2 receptor stim-ulation by intracoronary salbutamol thanpatients who are not ,B blocked.8 These previ-ous studies were performed on patients, or ontissue from patients, whose drug treatmenthad been chosen by referring physicians longbefore the time of study. Therefore to estab-lish that the /2 hypersensitivity seen in thesestudies is being induced by fl blocker treat-ment, rather than being a consequence ofpatient selection criteria, we undertook thepresent prospective investigation. This was across over study of,B, blocker treatment innormal volunteers to find whether selective /2receptor sensitisation can be induced by 3,Bblockade. To find whether any sensitisationoccurs in the heart only, we gave salbutamoland measured the dose related changes indiastolic blood pressure and the metabolicresponses to salbutamol as indicators ofextracardiac /2 receptor stimulation.
Patients and methodsSUBJECTSSix healthy men aged 24-35 took part in thestudy. The subjects were non-smokers withno contraindications to ,B blockade on history,examination, or electrocardiogram.
PROCEDUREBefore starting drug treatment the subjects
ClinicalPharmacology Unit,University ofCambridge,CambridgeJ A HallA FerroJ E C DickersonM J BrownCorrespondence to:Dr J A Hall, SouthCleveland Hospital, MartonRoad, MiddlesbroughTS4 3BW.Accepted for publication29 September 1992.
332
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from
,B Adrenoreceptor subtype cross regulation in the human heart
exercised on a treadmill to familiarise them-selves with the equipment and protocol. Alevel of exercise was found for each subjectthat produced a stable heart rate of about 150beats/min. The subjects then took a 14 daycourse of treatment with bisoprolol (10 mg)or matched placebo once daily. The order oftreatment was double blinded and ran-
domised according to a latin square design.Bisoprolol was used because its fl, selectivity(about 75-fold) is higher than that of atenololor metoprolol.9
Three days after stopping each course oftreatment the subjects underwent treadmillexercise followed by an intravenous salbuta-mol dose response study. A similar lightbreakfast was permitted before the two visits,excluding all caffeine containing drinks. Twointravenous cannulae were inserted in fore-arm veins. The subjects rested for 30 minutesand the resting heart rate was noted. Theythen walked on the treadmill at the previouslydetermined level of exercise for two minutesand the heart rate was measured. Blood sam-
ples were taken to measure plasma potassiumbefore exercise, at peak exercise, and at fiveminutes after exercise.
After exercise the subjects rested for 15minutes and were then given salbutamol byintravenous injections. The bolus injectionswere given over two minutes, and after a fur-ther three minutes the next dose was given.Injections started at 0 5 pg/kg and were
increased by doubling increments up to a
final dose of 4 pg/kg. Heart rate and bloodpressure were recorded at one minute andthree minutes after the end of each injection.Baseline measurements were taken in dupli-cate. During the dose response curve heartrate and blood pressure were determined bysingle measurements. Peak responses to eachinjection were seen at the one minute record-ing and these readings were used for furtheranalysis. Blood samples were taken for mea-
surement of potassium, glucose, and insulinconcentrations before the start of the salbuta-mol injections and at five minute intervals for40 minutes.
METHODS OF ASSESSMENT
Heart rate was calculated from the RR inter-vals averaged over 15 seconds from a contin-uously monitored electrocardiogram. Bloodpressure was measured with an automatedsphygmomanometer (Datascope, USA).Potassium was measured with an ion sensitiveelectrode, glucose by the glucose oxidasemethod, and insulin by a double antibodyradioimmunoassay.'°The study was approved by the district
medical ethics committee and was in accordwith the Helsinki Convention (Tokyo andVenice ammendments). Subjects gave writteninformed consent.
STATISTICSChanges in heart rate induced by exerciseand plasma potassium concentration afterbisoprolol treatment were compared withthose after placebo by a paired Student's ttest. Changes in systolic blood pressureinduced by salbutamol after bisoprolol treat-ment were compared with those after placeboby repeated measures analysis of variance.The dose of salbutamol needed to decreasediastolic blood pressure by 10 mm Hg (vaso-dilator dose 10 (VD10)) was found for eachdose response curve from a fitted linear equa-
tion. VD1Os (log doses) were compared afterbisoprolol treatment and after placebo by a
paired Student's t test. The dose of salbuta-mol to increase heart rate by 40 beats/min(chronotropic dose 40 (CD40)) was foundfor each individual dose response curve froma fitted quadratic equation, and CD40s (logdoses) were compared by a paired Student's ttest." For changes in the metabolic variables,serum potassium, insulin, and glucose con-
centrations, responses after bisoprolol treat-ment were compared with those after placeboby repeated measures analysis of variance. Ap value of < 0 05 was considered significant.All results are expressed as mean (SEM).
ResultsThere was no significant difference in thebasal heart rate or blood pressure three daysafter treatment with bisoprolol or placebo.The increases in heart rate in response to
exercise (peak exercise rate-resting rate)after treatment with bisoprolol (86-5 (3 0)beats/min) were not significantly differentfrom those after placebo (87-3 (4 0)beats/min) (table 1). The study had a 90%power to detect a > 15% difference in exer-
cise tachycardia at the 5% level.By contrast, the increases in heart rate in
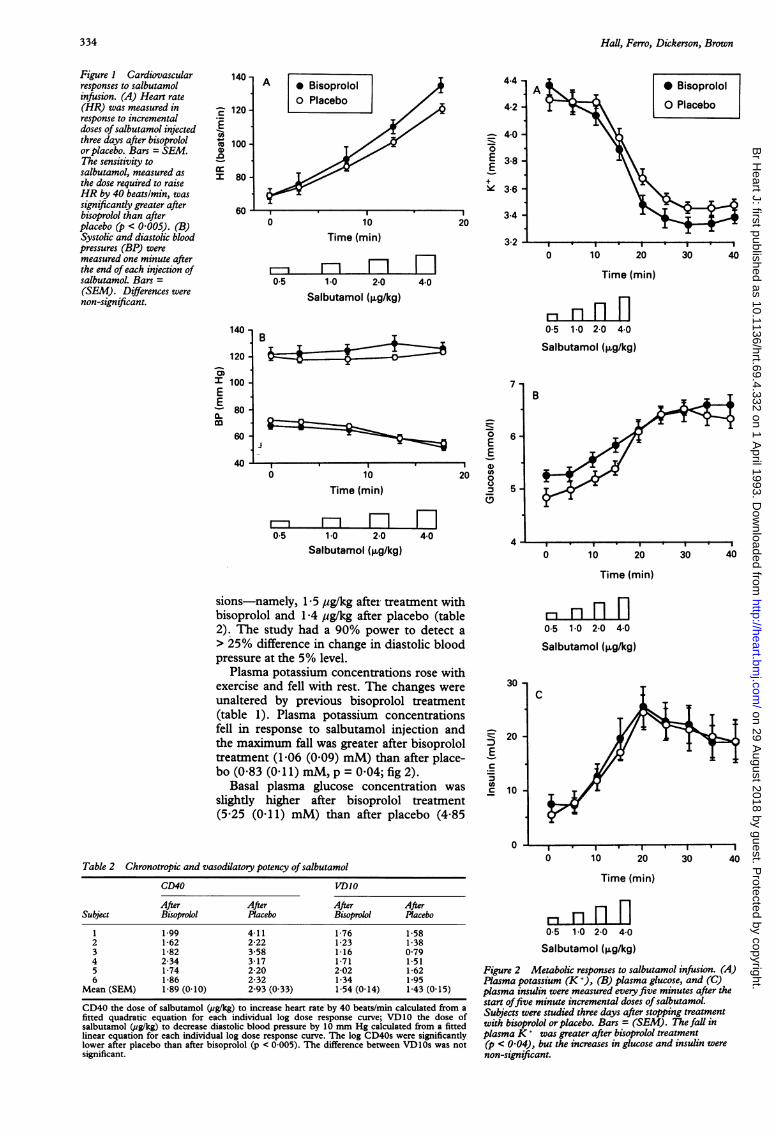
response to salbutamol injection were signifi-cantly greater after bisoprolol treatment thanplacebo. The maximum increases (peak rateafter 4 pg/kg-preinjection heart rate) were
66-3 (6 1) beats/min after bisoprolol and 51-3(5 9) beats/min after placebo, with CD40s of1-9 pg/kg and 29 ,ug/kg, (p < 0-002; fig 1 andtable 2). Salbutamol caused a fall in diastolicand no change in systolic blood pressure (fig1): the dose of salbutamol required todecrease diastolic blood pressure by 10 mmHg (VD 10) was similar on the two occa-
Table 1 Cardiovascular and metabolic responses to two minutes sub-maximal exercise
Placebo Bisoprolol
Before Peak After Before Peak After
Heart rate (beats/min) 61 5 (2 6) 148-8 (4-3) - 64-0 (2 9) 150-5 (25) -
Plasma potassium (mmol/1) 4 17 (0 08) 4-64 (0-11) 4.20 (0 10) 4-25 (0 06) 4-68 (0 05) 4-33 (0 07)
Values are mean (SEM); differences were non-significant.
333
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from
Hall, Ferro, Dickerson, Brown
Figure 1 Cardiovascularresponses to salbutamolinfusion. (A) Heart rate(HR) was measured inresponse to incrementaldoses of salbutamol injectedthree days after bisoprololor placebo. Bars = SEM.The sensitivity tosalbutamol, measured asthe dose required to raiseHR by 40 beatslmin, wassignificandy greater afterbisoprolol than afterplacebo (p < 0005). (B)Systolic and diastolic bloodpressures (BP) weremeasured one minute afterthe end ofeach injection ofsalbutamol. Bars =(SEM). Differences werenon-significant.
140 -
120 -
I 100 -
E- 80-m
60
40
4-4 -
4-2 -
= 4-0 -
0E 3-8-
ie 3-6-
3-4 -
20
3-2
c
co.C
I
0 10Time (min)
mF H0-5 1-0 2.0 4-0
Salbutamol (,ug/kg)
B
7
6ij
0
Time I
Ev I C
10 20 o
0
m mF H0-5 1-0 2.0 4-0
Salbutamol (,ug/kg)4
A * BisoprololO Placebo
0 10 20 30 40
Time (min)
a n n n0-5 1-0 2-0 4-0
Salbutamol (,g/kg)
0 10 20 30 40
Time (min)
sions-namely, 1-5 pg/kg after treatment withbisoprolol and 1-4 pg/kg after placebo (table2). The study had a 90% power to detect a> 25% difference in change in diastolic bloodpressure at the 5% level.
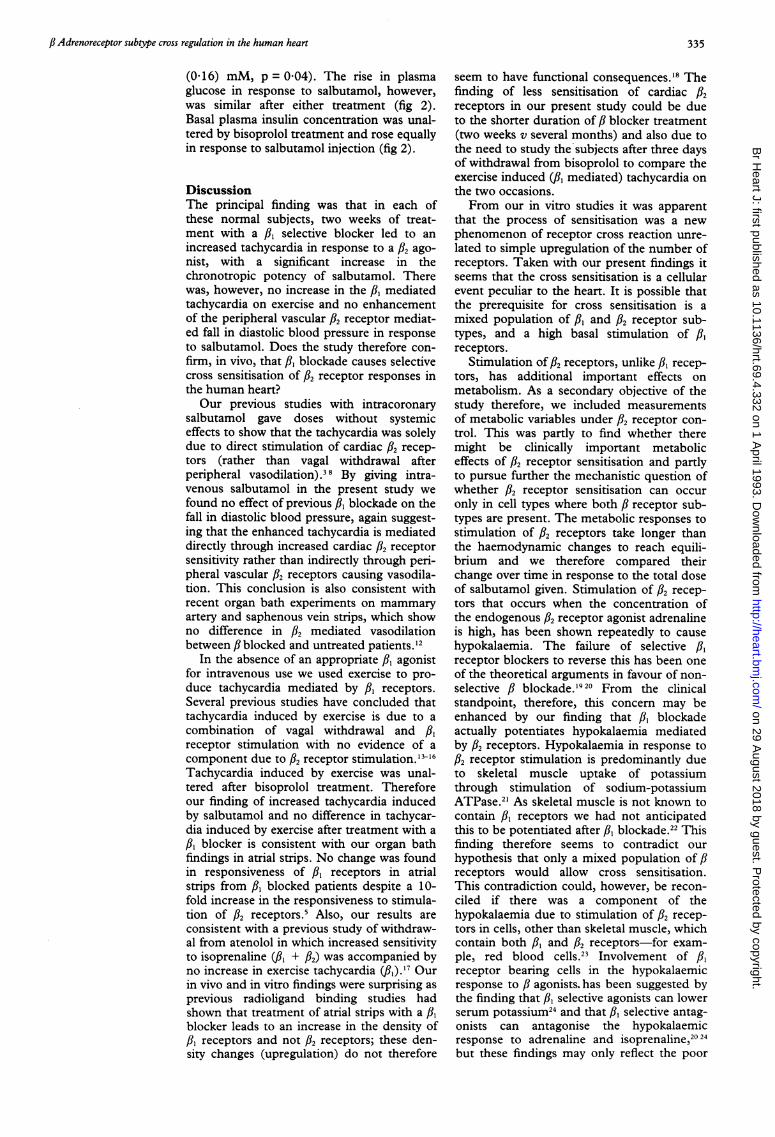
Plasma potassium concentrations rose withexercise and fell with rest. The changes wereunaltered by previous bisoprolol treatnent(table 1). Plasma potassium concentrationsfell in response to salbutamol injection andthe maximum fall was greater after bisoprololtreannent (1-06 (0-09) mM) than after place-bo (0-83 (0-11) mM, p = 0-04; fig 2).
Basal plasma glucose concentration wasslightly higher after bisoprolol treatment(5-25 (0-11) mM) than after placebo (4-85
n nn110-5 1-0 2-0 4-0
Salbutamol (jig/kg)
30 -
c 20 -
Ec
C 10
0
Table 2 Chronotropic and vasodilatory potency of salbutamol
CD40 VDIO
After After After AfterSubject Bisoprolol Placebo Bisoprolol Placebo
1 1 99 4-11 1*76 1*582 1-62 2-22 1-23 1-383 1-82 3-58 1-16 0 794 2-34 3-17 1-71 1-515 1-74 2-20 2-02 1-626 1-86 2-32 1-34 1-95
Mean (SEM) 1-89 (0-10) 2 93 (0 33) 1-54 (0-14) 1-43 (0-15)
CD40 the dose of salbutamol (ug/kg) to increase heart rate by 40 beats/min calculated from afitted quadratic equation for each individual log dose response curve; VD10 the dose ofsalbutamol (ag/kg) to decrease diastolic blood pressure by 10 mm Hg calculated from a fittedlinear equation for each individual log dose response curve. The log CD40s were significantlylower after placebo than after bisoprolol (p < 0.005). The difference between VD1Os was notsignificant.
C
I . I I I I, . I
0 10 20 30 40
Time (min)
r' n n n0.5 1.0 20 4-0
Salbutamol (,ug/kg)
Figure 2 Metabolic responses to salbutamol infusion. (A)Plasma potassium (K+), (B) plasma glucose, and (C)plasma insulin were measured evety five minutes after thestart offive minute incremental doses ofsalbutamol.Subjects were studied three days after stopping treatmentwith bisoprolol or placebo. Bars = (SEM). The faUl inplasma K+ was greater after bisoprolol treatment(p < 0-04), but the increases in glucose and insulin werenon-significant.
334
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from
fi Adrenoreceptor subtype cross regulation in the human heart
(0d16) mM, p = 0O04). The rise in plasmaglucose in response to salbutamol, however,was similar after either treatment (fig 2).Basal plasma insulin concentration was unal-tered by bisoprolol treatment and rose equallyin response to salbutamol injection (fig 2).
DiscussionThe principal finding was that in each ofthese normal subjects, two weeks of treat-ment with a /3, selective blocker led to anincreased tachycardia in response to a /2 ago-nist, with a significant increase in thechronotropic potency of salbutamol. Therewas, however, no increase in the 3,B mediatedtachycardia on exercise and no enhancementof the peripheral vascular /32 receptor mediat-ed fall in diastolic blood pressure in responseto salbutamol. Does the study therefore con-firm, in vivo, that 3,' blockade causes selectivecross sensitisation of /32 receptor responses inthe human heart?Our previous studies with intracoronary
salbutamol gave doses without systemiceffects to show that the tachycardia was solelydue to direct stimulation of cardiac /32 recep-tors (rather than vagal withdrawal afterperipheral vasodilation).38 By giving intra-venous salbutamol in the present study wefound no effect of previous /3' blockade on thefall in diastolic blood pressure, again suggest-ing that the enhanced tachycardia is mediateddirectly through increased cardiac /2 receptorsensitivity rather than indirectly through peri-pheral vascular /2 receptors causing vasodila-tion. This conclusion is also consistent withrecent organ bath experiments on mammaryartery and saphenous vein strips, which showno difference in /2 mediated vasodilationbetween # blocked and untreated patients.'2
In the absence of an appropriate /3, agonistfor intravenous use we used exercise to pro-duce tachycardia mediated by 3,' receptors.Several previous studies have concluded thattachycardia induced by exercise is due to acombination of vagal withdrawal and 3,'receptor stimulation with no evidence of acomponent due to /32 receptor stimulation. 13-16Tachycardia induced by exercise was unal-tered after bisoprolol treatment. Thereforeour finding of increased tachycardia inducedby salbutamol and no difference in tachycar-dia induced by exercise after treatment with a3,B blocker is consistent with our organ bathfindings in atrial strips. No change was foundin responsiveness of /3, receptors in atrialstrips from /3 blocked patients despite a 10-fold increase in the responsiveness to stimula-tion of /32 receptors.5 Also, our results areconsistent with a previous study of withdraw-al from atenolol in which increased sensitivityto isoprenaline (R- + 3,B) was accompanied byno increase in exercise tachycardia (f,).'7 Ourin vivo and in vitro findings were surprising asprevious radioligand binding studies hadshown that treatment of atrial strips with a /,blocker leads to an increase in the density ofAl receptors and not /3, receptors; these den-sity changes (upregulation) do not therefore
seem to have functional consequences.'8 Thefinding of less sensitisation of cardiac /32receptors in our present study could be dueto the shorter duration of / blocker treatment(two weeks v several months) and also due tothe need to study the subjects after three daysof withdrawal from bisoprolol to compare theexercise induced (/3, mediated) tachycardia onthe two occasions.From our in vitro studies it was apparent
that the process of sensitisation was a newphenomenon of receptor cross reaction unre-lated to simple upregulation of the number ofreceptors. Taken with our present findings itseems that the cross sensitisation is a cellularevent peculiar to the heart. It is possible thatthe prerequisite for cross sensitisation is amixed population of /,3 and /32 receptor sub-types, and a high basal stimulation of /3receptors.
Stimulation of /32 receptors, unlike /3, recep-tors, has additional important effects onmetabolism. As a secondary objective of thestudy therefore, we included measurementsof metabolic variables under /32 receptor con-trol. This was partly to find whether theremight be clinically important metaboliceffects of /3, receptor sensitisation and partlyto pursue further the mechanistic question ofwhether /3, receptor sensitisation can occuronly in cell types where both /3 receptor sub-types are present. The metabolic responses tostimulation of /32 receptors take longer thanthe haemodynamic changes to reach equili-brium and we therefore compared theirchange over time in response to the total doseof salbutamol given. Stimulation of /32 recep-tors that occurs when the concentration ofthe endogenous /32 receptor agonist adrenalineis high, has been shown repeatedly to causehypokalaemia. The failure of selective /3'receptor blockers to reverse this has been oneof the theoretical arguments in favour of non-selective /3 blockade.'920 From the clinicalstandpoint, therefore, this concern may beenhanced by our finding that /3, blockadeactually potentiates hypokalaemia mediatedby /32 receptors. Hypokalaemia in response to/32 receptor stimulation is predominantly dueto skeletal muscle uptake of potassiumthrough stimulation of sodium-potassiumATPase.2' As skeletal muscle is not known tocontain 3,' receptors we had not anticipatedthis to be potentiated after 3,' blockade.22 Thisfinding therefore seems to contradict ourhypothesis that only a mixed population of /receptors would allow cross sensitisation.This contradiction could, however, be recon-ciled if there was a component of thehypokalaemia due to stimulation of /2 recep-tors in cells, other than skeletal muscle, whichcontain both 3,' and 32 receptors-for exam-ple, red blood cells.23 Involvement of /3,receptor bearing cells in the hypokalaemicresponse to 3 agonists.has been suggested bythe finding that /3' selective agonists can lowerserum potassium24 and that /3, selective antag-onists can antagonise the hypokalaemicresponse to adrenaline and isoprenaline,20 24but these findings may only reflect the poor
335
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from

Hall, Ferro, Dickerson, Brown
selectivity of the agents used. An alternativeexplanation of our increased hypokalaemia inresponse to salbutamol after treatment withbisoprolol may be that hypokalaemia isgreater because the greater increase in cardiacoutput augments the potassium load deliv-ered to the predominant site of potassiumuptake-namely, skeletal muscle.
By contrast there was no increase after ,blockade of salbutamol induced release ofglucose or insulin consistent with a lack ofknown fi, receptors on liver or pancreaticcells.25 We found, however, that basal plasmaglucose (before salbutamol infusion) wasincreased after bisoprolol treatment, with nodifference in basal plasma insulin. Theimplied insulin resistance has been previouslynoted with fi blockade.26 We would not attachtoo much importance to our own findingsuntil they are repeated with measurementsbefore and after a standard glucose load, butthey may shed indirect light on the mecha-nism of cross sensitisation.
Previous experiments have pointed awayfrom changes in the fi receptor itself beingresponsible for sensitisation and have indicat-ed that the coupling of the receptor to itsadenyl cyclase through G proteins, is a morelikely site for regulation of sensitivity. In themitral valve prolapse syndrome # receptorsensitisation is found due to a change in thestimulatory G protein (Gs).2728 On the otherhand, altered fi receptor sensitivity could bedue to changes in the inhibitory G protein(Gi). Conditions in which there is a chronicincrease in fi receptor stimulation, such ascardiac failure, have been associated withincreased expression of Gi.2930 Consequentlyone of our hypotheses is that fi blockade leadsto the reverse of chronic fi receptor stimula-tion-namely, a reduced concentration of Gi.If this hypothesis proves to be correct thenthe hint that fi blockade induces insulin resis-tance is of mechanistic as well as clinicalinterest as some of the actions- of insulin areGi dependent and reduced expression of thisprotein has been found in some experimentalmodels of insulin resistance.3'The possible clinical implications are per-
haps of greater relevance to the present study.To find sensitisation of f2 receptors mightprovide the basis for explaining the clinicalsyndrome of fi blocker withdrawal.4 Also amajor clinical concern is whether sensitisationof, and failure to block, cardiac f2 receptorsin patients with ischaemic heart disease mightparadoxically increase the risk of arrhythmias.There have been no prospective comparisonsof f,, selective and non-selective antagonists insuch patients, but we have commented previ-ously on the generally better performance ofnon-selective antagonists in the secondaryprevention trials of fi blockade after myocar-dial infarction and the perhaps surprising fail-ure of the fi, selective atenolol to preventarrhythmia when given acutely to suchpatients.3233 These speculations on the clini-cal implications will now need to be tested ingroups of patients with ischaemic heart dis-ease or hypertension.
We thank Miss L DiSilvio for the metabolic assays andLederle for the supply of bisoprolol and placebo tablets. A F isa Medical Research Council Training Fellow, and furtherfunding was from the East Anglian Regional HealthAuthority.
1 Lands AM, Arnold A, McAuliff JP, et al. Differentiationof receptor subtypes by sympathetic amines. Nature1967;214:597-8.
2 Stiles GL, Taylor S, Lefkowitz RJ. Human cardiac beta-adrenergic receptors: subtype heterogeneity delineatedby direct radioligand binding. Life Sci 1983;33:467-73.
3 Hall JA, Petch MC, Brown MJ. Intracoronary injectionsof salbutamol demonstrate the presence of functional fi-2 adrenoreceptors in the human heart. Circ Res 1989;65:546-53.
4 Prichard BNC, Tomlinson B, Walden RJ, BhattacharjeeP. The ,B-adrenergic blockade withdrawal phenomenon.Jf Cardiovasc Pharmacol 1983;5(suppl 1):S56-62.
5 Hall JA, Kaumann AJ, Brown MJ. Selective fl-I adrenore-ceptor blockade enhances positive inotropic responsesto endogenous catecholamines mediated through,-2adrenoreceptors in human atrial myocardium. Circ Res1990;66:1610-23.
6 Kaumann AJ, Sanders L, Brown AM, Murray KJ, BrownMJ. A 5-HT receptor in the human atrium. Br JfPharmacol 1990;100:879-85.
7 Motomura S, Deighton NM, Zerkowski HR, et al.Chronic fl-I adrenoceptor antagonist treatment sensi-tizes fl-2 adrenoceptors but desensitizes M-2 muscarinicreceptors in the human right atrium. Br J Pharmacol1990;101 :362-9.
8 Hall JA, Petch MC, Brown MJ. In vivo evidence of car-diac fl-2 adrenoreceptor sensitisation due to atenololtreatment. CircRes 1991;69:959-64.
9 Wellstein A, Palm D, Belz GG, et al. Reduction in exer-cise tachycardia in man after propranolol, atenolol, andbisoprolol in comparison to ,B-adrenoreceptor occu-pancy. EurHeartJ 1987;8(suppl M):3-8.
10 Morgan CR, Lazarow A. Immunoassay of insulin with atwo antibody system: plasma concentration in normal,subdiabetic and diabetic rats. Diabetes 1963;12:115-26.
11 Sumner DJ, Elliot HL, Reid JL. Analysis of the pressordose response. Clin Pharmacol Ther 1982;52:450-8.
12 Ferro A, Kaumann AJ, Brown MJ.fl-adrenoreceptor sub-types and function in human internal mammary arteryand saphenous vein. BrJPharmacol 1992;105:229P.
13 Harry JD, Young J, Stribling D. Effects of ICI 118551 (a,6-2 adrenoreceptor blocker) on metabolic changesinduced by isoprenaline and on tachycardia induced byexercise. BrJ Clin Pharmacol 1982;14:584P.
14 Tattersfeild AE, Cragg DJ. Effect of ICI 118551 onbronchial f,-adrenoreceptor function and exercise heartrate in normal man. Br Jf Clin Pharmacol 1983;16:587-90.
15 Wellstein A, Belz GG, Palm D. f,-adrenoreceptor subtypebinding activity in plasma and fl-blockade by propra-nolol and fl-I selective bisoprolol in humans. Evaluationwith Schild plots. J Pharmacol Exp Ther 1988;246:328-37.
16 Pringle TH, Riddell JG, Shanks RG. Characterisation ofthe fi-adrenoreceptors which mediate the isoprenalineinduced changes in finger tremor and cardiovascularfunction in man. EurJ Clin Pharmacol 1988;35:507-14.
17 Walden RJ, Bhatterjee P, Tomlinson B. The effect of ISAon fi-adrenoreceptor responsiveness after fi-adrenore-ceptor blockade withdrawal. Br Jf Clin Pharmacol1978;5:207.
18 Michel MC, Pingsmann A, Beckeringh JJ, et al. Selectiveregulation of l-I and /1-2 adrenoceptors in the humanheart by chronic f,-adrenoceptor antagonist treatment.BrJ Pharmacol 1988;94:685-92.
19 Brown MJ, Brown DC, Murphy MB. Hypokalaemia frombeta-2 receptor stimulation by circulating epinephrine.NEngJMed 1983;309:1414-19.
20 Struthers AD, Whiteside R, Reid JL, Rodgers JC. Effectsof cardioselective and non-cardioselective beta-blockadeon hypokalaemia and cardiovascular responses toadrenomedullary hormones in man. Clin Sci 1983;65:143-7.
21 Clausen T, Flatman JA. Beta-2 adrenoreceptors mediatethe stimulating effect of adrenaline on active electro-genic Na/K transport in rat soleus muscle. Br JPharmacol 1980;68:749-55.
22 Elfellah MS, Dalling R, Kantola RM, Reid JL. fi-adreno-ceptors and human skeletal muscle characterisation ofreceptor subtype and effect of age. Br Jf Clin Pharmacol1989;27:31-8.
23 Bree F, Gault I, d'Athis P, Tillement J-P. Beta adrenocep-tors of human red blood cells, determination of theirsubtypes. Biochem Pharmacol 1984;33:4045.
24 Vincent HH, Boomsma F, Man in't Veld AJ, et al. Effectsof selective and non-selective fi-agonists on plasmapotassium and norepinephrine. J Cardiovasc Pharmacol1984;6: 107.
25 John GW, Doxey J-C, Walter DS, Reid JL. The role of aand fi-adrenoceptor subtypes in mediating the effects ofcatecholamines on fasting glucose and insulin in the rat.BrJ Pharmacol 1990;100:699-704.
26 Pollare T, Lithell H, Selinus I, Berne C. Sensitivity toinsulin during treatment with atenolol and metoprolol: arandomised double blind study of effects on carbohy-
336
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from
,B Adrenoreceptor subtype cross regulation in the human heart
drate and lipoprotein metabolism in hypertensivepatients. BMJ 1989;298:1152-7.
27 Autonomic function in mitral valve prolapse [editorial].Lancet 1987;2:773-4.
28 Davies AO, Su CJ, Balasubramanyam A, Codina J,Birnbaumer L. Abnornal guanine nucleotide regulatoryprotein in MVP dysautonomia: evidence from reconsti-tution of Gs. Clin Endocrinol Metab 1991 ;72:867-75.
29 Reithmann C, Gierschik P, Sidiropoulos D, Werdan K,Jakobs KH. Mechanism of noradrenaline induced het-erologous desensitisation of adenylate cyclase stimula-tion in rat heart muscle cells: increase in the level ofinhibitory G-protein a subunits. Eur Pharmacol 1989;172:211-21.
30 Neumann J, Schmitz W, Scholz H, et al. Increase inmyocardial G-proteins in heart failure Lancet 1988;2:936-7.
31 Green A. Adenosine receptor downregulation and insulinresistance follows prolonged incubation of adipocyteswith an Al adenosine receptor agonist. Biol Chem1987;262: 15702-7.
32 First international study of infarct survival collaborativegroup. Randomised trial of intravenous atenolol among16,027 cases of suspected acute myocardial infarction:ISIS-1. Lancet 1986;1:57-66.
33 Norris RM, Brown MA, Clarke ED, et al. Prevention ofventricular fibrillation during acute myocardial infarc-tion by intravenous propranolol. Lancet 1984;2:883-6.
337
on 29 August 2018 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.69.4.332 on 1 April 1993. D
ownloaded from





























