Embed Size (px)
DESCRIPTION
http://vtoral.vernalpond.com/downloads/Bolin-article-JADA.pdf
Citation preview

2008;139;1530-1535 J Am Dent Assoc
Kenneth Anthony Bolin Study
Health Aide Therapists in Alaska: A Pilot Assessment of Treatment Provided by Dental
jada.ada.org ( this information is current as of November 1, 2008 ):The following resources related to this article are available online at
http://jada.ada.org/cgi/content/full/139/11/1530in the online version of this article at:
including high-resolution figures, can be foundUpdated information and services
http://www.ada.org/prof/resources/pubs/jada/permissions.aspthis article in whole or in part can be found at:
of this article or about permission to reproducereprintsInformation about obtaining
© 2008 American Dental Association. The sponsor and its products are not endorsed by the ADA.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
1530 JADA, Vol. 139 http://jada.ada.org November 2008
I nformation on the oral healthstatus of American Indian/Alaska Natives (AI/AN) hasbeen gathered by the U.S.Department of Health and
Human Services, U.S. IndianHealth Service (IHS).1 For compari-sons with the U.S. general popula-tion oral health national averages, Iused data from the Third NationalHealth and Nutrition Survey, 1988-1994, and the National Health andNutrition Examination Survey,1999-2002, conducted by theNational Center for Health Statis-tics.2 Oral health disparities arewidespread and significantly severein geographically isolated locationsin the United States in general3 andin the AN population in particular.Although the prevalence of dentalcaries in the general population ofthe United States decreased signifi-cantly during the 1980s and 1990s,4
there was only a small reduction ofdental caries in the AN populationin the 1980s. Existing disparities inoral health between ANs and theU.S. general population actuallyincreased during the 1990s.2,5
Comparing data from IHS sur-veys and National Health andNutrition Examination Surveyssheds some light on the magnitudeof the disparities in oral healthstatus between ANs and the gen-eral population. AN children andadolescents experience approxi-
Dr. Bolin is an associate professor, Department of Public Health Sciences, Texas A&M University HealthScience Center, Baylor College of Dentistry, 3302 Gaston Ave., Room 705, Dallas, Texas 75246, e-mail“[email protected]”. Address reprint requests to Dr. Bolin.
Assessment of treatment provided by dentalhealth aide therapists in AlaskaA pilot study
Kenneth Anthony Bolin, DDS, MPH
Background. Dental health aide therapists (DHATs) in Alaska areauthorized under federal law to provide certain dental services, includingirreversible dental procedures. The author conducted this pilot study todetermine if treatments provided by DHATs differ significantly from thoseprovided by dentists, to determine if DHATs in Alaska are deliveringdental care within their scope of training in an acceptable manner and toassess the quality of care and incidence of reportable events during or afterdental treatment.Methods. The author audited the dental records of patients treated bydentists and DHATs who perform similar procedures for selected variables.He reviewed the records of 640 dental procedures performed in 406patients in three health corporations.Results. The author found no significant differences among the providergroups in the consistency of diagnosis and treatment or postoperative com-plications as a result of primary treatment. The patients treated by DHATshad a mean age 7.1 years younger than that of patients treated by dentists,and the presence or adequacy of radiographs was higher among patientstreated by dentists than among those treated by DHATs, with the differ-ence being concentrated in the zero- to 6-year age group.Conclusions. No significant evidence was found to indicate that irre-versible dental treatment provided by DHATs differs from similar treat-ment provided by dentists. Further studies need to be conducted to deter-mine possible long-term effects of irreversible procedures performed bynondentists.Clinical Implications. A need to improve oral health care forAmerican Indian/Alaska Native populations has led to an approach for pro-viding care to these groups in Alaska. The use of adequately trainedDHATs as part of the dental team could be a viable long-term solution.Key Words. Health services accessibility; community health aides;Alaska Natives; dental therapist.JADA 2008;139(11):1530-1539.
A B S T R A C T
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
JADA, Vol. 139 http://jada.ada.org November 2008 1531
mately 2.5 times the amount of dental cariesthat children and adolescents in the general U.S.population do.5 For example, 20.7 percent of ANchildren 2 to 5 years of age are caries-free com-pared with 72.1 percent of children 2 to 5 yearsof age in the U.S. general population.2,6 Statedanother way, AN children aged 2 to 5 years havea caries history 3.5 times that of the same agegroup in the general U.S. population, and themean number of decayed and filled teeth foundin the IHS study group was almost five timesthat of the U.S. general population.1,2 Sixty per-cent of AI/AN children have severe early child-hood caries, which is defined as any child 5years or younger with dental decay in the maxil-lary anterior teeth or six or moreteeth with decay.1
This prevalence of caries existsdespite the implementation of sig-nificant dental decay preventionprograms by the IHS and tribalorganizations.6 Approximately one-half of AI/AN adults aged 35 to 44years have destructive periodontaldisease, compared with 22 percentin adults aged 35 to 44 years in thegeneral U.S. population.7 There aresignificant disparities in all aspectsof oral health for AI/ANpopulation.8
Barriers to dental care. Obtaining access toroutine and emergency dental care can be chal-lenging for ANs. Approximately 87,000 of the125,000 ANs live in rural communities, whichare remote and not accessible by road. Theextreme temperatures that occur in AN villagesmake travel, work and the operation of machin-ery difficult for those not accustomed to coldtemperatures. Throughout most of the state,transportation is accomplished by airplane, boat,all-terrain vehicle or snowmobile. In general,there are significant distances between villages,and the presence of mountain ranges and glac-iers compound the already difficult and dan-gerous task of travel.5 Alaska has a populationdensity of about 1.1 people per square mile, com-pared with the U.S. national average of 79.6people per square mile.9
While travel and geographic barriers arephysical difficulties in providing dental care toANs living in remote villages, other economicand cultural realities exist in that the villagesusually are small and cannot support a full-time
general dentist or physician, let alone special-ists.5 Dentists must travel to the villages periodi-cally to provide dental care, or patients must betransported to a dentist for treatment, often bymeans of high-cost air taxi.6 Many villages haveno lodging or dining facilities, and visiting den-tists and staff members may have to sleep in themedical facility or the dental clinic. Many vil-lages have no supermarkets at which to buyfood, and perishable goods are hard to come by,even in the relatively mild summer months. Vis-iting dentists and staff members often must flytheir own food into the village along with theirbaggage and dental supplies or risk having littleto eat (M. Kelso, DDS, oral communication, July
2006). Cultural barriers to care should
be fairly predictable but often arenot considered thoroughly whendiscussing access to care. ManyAlaska dentists who may reside inregional hub towns but travel toremote villages for temporary dutycan be viewed as itinerant peoplewho do not speak the native lan-guage and who do not live in thebush country of Alaska.8 Dentistswho may be seen as outsiders andwho provide oral health advice,
including oral hygiene instruction and dietarycounseling, may seem paternalistic or aloof atbest. For example, drinking soda pop rather thanwater is viewed by some in the Native Alaskanculture as a status symbol, and they continue todo so even though their dentists have told themthat it can be bad for their teeth.8,10
To address these and other issues, includingthe recruitment and retention of dentists by theIHS and native tribal health authorities, dentalhealth aide therapists (DHATs) were deployed inAlaska as part of the Community Health AideProgram (CHAP). The rationale and history ofthe development of the idea to introduce mid-level dental providers who are analogous to
ABBREVIATION KEY. ADA: American Dental Associa-tion. AI/AN: American Indian/Alaska Native. CDHC:Community Dental Health Coordinator. CDT: CurrentDental Terminology. CHAP: Community Health AideProgram. CODA: Commission on Dental Accreditation.DANB: Dental Assisting National Board. DHAT:Dental health aide therapist. IHS: U.S. Indian HealthService. OPA: Oral Preventive Assistant. SOAP: Sub-jective, Objective, Assessment, Plan.
Alaska has a population density of about 1.1 peopleper square mile,
compared with theU.S. national average
of 79.6 people persquare mile.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
1532 JADA, Vol. 139 http://jada.ada.org November 2008
physician assistants and nurse practitioners inmedicine have been published.6,11
I conducted a pilot study to determine via asystematic dental chart review if DHATs prac-ticing in rural Alaskan communities were deliv-ering dental care within their scope of trainingin an acceptable manner.
METHODS
To assess quality of care and the incidence ofreportable events during or after treatment, Iaudited the charts of patients treated by DHATswho were under direct supervision and generalsupervision (DHAT groups) at five Alaskandental clinics that were components of threehealth corporations. (Alaskan health corpora-tions are designed in a similar structure to Fed-erally Qualified Health Centers and typicallyare nonprofit entities that deliver medical,dental, pharmacy and other health-related serv-ices under one corporate identity.) I comparedthese data with those of patients treated by thesupervising dentists (dentist group) in twoAlaskan regional hub clinics (in Bethel andNome) during the same period and from thesame sampling frame. I randomly selectedpatient charts at both the regional hub andremote satellite clinics in the villages of Aniak,Shungnak and Toksook Bay from either com-puter printouts or from paper records accordingto availability at the respective sites.
The procedure codes (Current Dental Termi-nology [CDT]) codes) I audited were those fortreatments that DHATs are trained to provideand authorized to perform under the rules ofCHAP. I audited the same procedure codes fromthe dentists’ charts to control for bias owing tovariation in treatment complexity between thetwo groups. I selected only irreversible pro-cedure codes, except for radiographs, for investi-gation. Hence, I did not include in my assess-ment any procedures that a dental hygienist orother expanded function dental auxiliary couldperform such as prophylaxis, placing sealants,and providing fluoride treatments and oralhygiene instruction.
I used selected indicators from the IndirectReview of Clinical Quality and Risk Manage-ment (Chart Review) section of the qualityassessment tool used by the IHS12 to examinethe dental treatment provided by DHATs. Thischart review tool consists of 12 categories con-taining 83 criteria that could be chosen in a full
chart review. For this pilot study, I selected onlythose criteria that I deemed to be of concernregarding the implementation of a dentaltherapy program. I pilot-tested these selectedcriteria with the clinical program directors oftwo of the three health corporations. I did notinclude criteria that did not apply to DHATs(that is, criteria for endodontics, prosthodontics,orthodontics, laboratory procedures, methods ofmeasuring periodontal case types or any otherprocedures that DHATs are not trained to per-form nor expected to perform). I also examinedchart entries for any recorded reportable out-comes or complications resulting from the treat-ments provided by practitioners in the DHATand dentist groups.
I minimized interexaminer bias by being theonly one to review the charts. All treatmentswere performed between Jan. 10, 2005, and July25, 2006, and my on-site chart audits took placein July and August of 2006. The study protocolwas approved by the Texas A&M Health ScienceCenter, Baylor College of Dentistry InstitutionalReview Board.
RESULTS
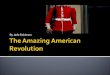
I audited 640 irreversible dental treatment pro-cedures performed on 406 different patients forselected quality of treatment indicators: thepresence of Subjective, Objective, Assessment,Plan (SOAP) notes; treatment code recorded con-sistent with diagnosis; presence or adequacy ofradiographs; and report of intra- or postopera-tive complications. The distribution of pro-cedures performed by provider type was as fol-lows: dentist, 171 (26.7 percent); DHAT underdirect supervision, 218 (34.1 percent); andDHAT under general supervision, 251 (39.2 per-cent). I recorded the procedure codes and tabu-lated them. The top three procedures groupedaccording to code families (for example, CDTseries D2100s, D2300s and D7000s) that wereperformed by all provider groups were as fol-lows: alloy restorations, 152 (23.8 percent); pos-terior composite restorations, 144 (22.5 percent);and extractions, 123 (19.2 percent). A cross-tabulation calculation that compared the distrib-ution of CDT procedure code families performedby the dentist group and the DHAT groupsshowed no significant difference among thegroups for any CDT code family except crowns,specifically stainless steel crowns (Fisher exacttest, P = .003). Figure 1 shows the total distribu-
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
JADA, Vol. 139 http://jada.ada.org November 2008 1533
tion of procedures grouped according to CDTcode families by provider type.
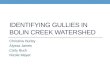
SOAP notes were available in 638 (99.7 per-cent) of all cases reviewed. The CDT procedurecode recorded was consistent with the diagnosisfor 630 (98.4 percent) of procedures performed.The differences among the DHAT groups and thedentist group were not significant in this area(Fisher exact test, P = .73). Overall, radiographswere present or adequate in 551 cases (86.1 per-cent). Further analysis showed the DHATgroups had significantly lower percentages ofpresent or adequate radiographs than did thedentist group (!2; P = .012); however, the defi-ciency was notable in that it was limited topatients 6 years or younger (!2; P < .001). Inaddition, analysis showed that practitioners inthe DHAT groups saw younger patients than didpractitioners in the dentist group. The mean ageof patients treated by DHATs was 16.9 years,and the mean age of patient treated by dentistswas 24.0 years. An independent samples t testshowed this was a significant difference (P = .002). The mean age of all patients treatedby all groups was 18.78 (standard deviation ±15.26) years. Figure 2 shows the age distributionof patients seen by DHATs compared with thatseen by dentists. This comparison shows thatDHATs treated a larger number of younger chil-dren, and dentists treated more of the popula-tion older than 35 years.
The definition I used for complication—intra-operative or postoperative—was two-tiered. Iconsidered a complication to be within normallimits if it was an event that could happen toany dental provider at any time and be reme-died easily (for example, a patient wishing tostop a procedure, an uncooperative child pre-venting completion of a procedure, debonding ofa composite restoration or breakage of anamalgam restoration before dismissal of thepatient). I defined a complication requiring fur-ther treatment as a reportable event thatrequires a return visit to the clinic, postopera-tive medications or intervention by a generaldentist or specialist. Examples of this type ofcomplication are debonding of a composite resto-ration or breakage of an amalgam restorationafter dismissal of patient, postoperative infec-tion, breakage of a root tip, as well as otherproblems (Box). When I used these definitions, Ifound that there were no complications reportedin association with 625 (97.7 percent) pro-cedures performed by providers in all groups.There was no significant difference in thenumber of any kind of complication between theDHAT group and the dentist group (Fisherexact test, P = .770).
DISCUSSION
Decades of poor oral health and failing efforts torecruit dentists and specialists to the remote
35
30
25
20
15
10
5
0Alloy
RestorationsAnterior
CompositeRestorations
PosteriorComposite
Restorations
Crowns SedativeFilling
PulpTherapy
Extraction
CODE FAMILY
PER
CEN
TA
GE
Dentist
DHAT
Figure 1. Bar graph showing Current Dental Terminology code families by provider type. DHAT: Dental health aide therapist.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
1534 JADA, Vol. 139 http://jada.ada.org November 2008
bush country of Alaska require new approachesto address the problem of oral health disparitiesin the AN population. One of the main objectionsto the solution of expansion of duties to nonden-tists was the issue of quality of care. Some whoare opposed to treatment provided by DHATshave suggested that it is “second-class care” or,since DHATs do not have dental licenses, thatthey are practicing dentistry without a licenseand, therefore, could be “unsafe.”13,14 Settingaside the political and philosophical nature of
these arguments, the scientific and objectiveevaluation of this new method of delivering careshould be studied in the United States as it hasbeen in other countries. Although the use ofDHATs or dental therapists is allowed in morethan 40 countries worldwide, including somedeveloped Western nations,10,15 the dental profes-sion in the United States has been opposed fordecades to providers other than dentists per-forming irreversible dental procedures, regard-less of the procedures’ complexity. This opposi-tion has occurred despite study results showingthat DHATs can perform primary care pro-cedures comparably to dentists, and that DHATtrainees perform equally well compared withdental students.15-18 However, the legality ofthese midlevel dental practitioners’ performingduties they are trained to perform no longer is inquestion after a court ruling upheld the exemp-tion of DHATs from the Alaska Dental PracticeAct.19
Limitations of the study. At the time I per-formed the chart audits, the deployment ofDHATs in Alaska was in its infancy; DHATs hadbeen seeing patients for only six months. Conse-quently, there were not as many DHAT chartsfor me to select from to obtain the numbers thatI needed to conduct a higher-powered analysis ofthe data. In addition, there were not sufficientnumbers of procedures available to control for
Examples of reportable complications.dAllergic reactiondAspiration or swallowed substancedCardiac arrest or dysrhythmiadExcessive pain, bleeding or swelling during or after
treatmentdFractured mandibledFractured or damaged nontreated toothdLaceration requiring suturesdLack of informed consent, patient-perceiveddMedical complications resulting from dental treatmentdOral-antral fistula, iatrogenicdParesthesiadSevered blood vesseldSevered nervedSyncope and vertigodWrong prescription: drug, dose, instructions, etc.dWrong tooth treated or extracted
BOX
40
35
30
25
20
15
10
5
00-6 > 6 to 12 > 12 to 18 > 18 to 35 > 35
AGE (YEARS)
PER
CEN
TA
GE
Dentist
DHAT
Figure 2. Bar graph showing age distribution of patients, by provider type. DHAT: Dental health aide therapist.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
JADA, Vol. 139 http://jada.ada.org November 2008 1535
age and sex matching by CDT procedure code incomparing DHATs and dentists. In some remotesatellite clinics, the audit essentially was acensus survey, rather than a random selection,of patients seen for treatment that involved irre-versible dental procedures. Chart availabilityvaried somewhat from health corporation tohealth corporation and from clinic to clinic. Thisvariation in retrievability may have injectedselection bias favorable to the dentist group intothe sample.
Variation in the availability of digital radiog-raphy and reliability of the information tech-nology systems of the respective organizationsalso may have influenced the absence or pres-ence of radiographs in either the traditionalchart or the electronic health record, whichcould be determined only by conducting alarger and more exhaustive examination ofrecords.
Finally, this pilot study cannot be interpretedas a true outcomes study, which would requiremuch more abstraction of data, patient question-naires, patient satisfaction surveys and possiblelive examination of patients’ treatment in aprospective cohort study. A much larger, long-term study needs to be performed to continue toexamine the immediate and long-range effects ofhaving culturally competent, local native peopleprovide the oral health advice, dietary coun-seling, preventive care and necessary thera-peutic procedures within the intended scope ofpractice in a consistent manner over time.
CONCLUSIONS
I found no significant evidence to indicate thatirreversible dental treatment provided byDHATs differed from similar treatment providedby dentists. Analysis of the dental charts Iaudited showed that DHATs were beingdeployed to treat younger patients than theirdentist supervisors. They obtained significantlyfewer radiographs for patients 6 years oryounger, and they placed significantly morestainless steel crowns than did the dentists. Nosignificant difference in reportable eventsoccurred between the DHAT groups and the den-tist group in the dental charts I audited. Furtherstudies need to be conducted to determine pos-sible long-term effects of irreversible proceduresperformed by nondentists. !
Disclosure. Dr. Bolin did not report any disclosures.
This study was funded by the Texas A&M University SystemHealth Science Center Research Development Grant Program, College Station, Texas.
The author thanks the Yukon-Kuskokwim, Norton Sound andManiilaq health corporations for their cooperation in the chart reviewand advice in navigating in the bush country of rural Alaska.
1. U.S. Department of Health and Human Services, Indian HealthService. An Oral Health Survey of American Indian and AlaskaNative Dental Patients: Findings, Regional Differences and NationalComparisons. Rockville, Md.: U.S. Department of Health and HumanServices, Indian Health Service; 2002.
2. Beltran-Aguilar ED, Barker LK, Canto MT, et al.; Centers forDisease Control and Prevention. Surveillance for dental caries, dentalsealants, tooth retention, edentulism, and enamel fluorosis: UnitedStates, 1988-1994 and 1999-2002. MMWR Surveill Summ 2005;54(3):1-43.
3. U.S. Department of Health and Human Services. A National Callto Action to Promote Oral Health. Rockville, Md.: U.S. Department ofHealth and Human Services, Public Health Service, National Insti-tutes of Health, National Institute of Dental and CraniofacialResearch; 2003. NIH publication 03-5303.
4. U.S. Department of Health and Human Services. Oral Health inAmerica: A Report of the Surgeon General. Rockville, Md.: U.S.Department of Health and Human Services, National Institute ofDental and Craniofacial Research, National Institutes of Health;2000.
5. Sekiguchi E, Guay AH, Brown LJ, Spangler TJ Jr. Improving theoral health of Alaska Natives. Am J Public Health 2005;95(5):769-773.
6. Nash DA, Nagel RJ. Confronting oral health disparities amongAmerican Indian/Alaska Native children: the pediatric oral healththerapist. Am J Public Health 2005;95(8):1325-1329.
7. U.S. Department of Health and Human Services. Healthy People2010. 2nd ed. Washington: U.S. Department of Health and HumanServices; 2000.
8. Smith EB. Dental therapists in Alaska: addressing unmet needsand reviving competition in dental care. Alaska Law Rev 2007;24(1):105.
9. U.S. Census Bureau. State and County Quick Facts: Alaska—Persons per square mile, 2000. “http://quickfacts.census.gov/qfd/states/02000.html”. Accessed Sept. 16, 2008.
10. Garvin J. Controversy in Alaska: are dental therapists theanswer to Alaska natives’ caries crisis. AGD Impact 2005;33:18-23.
11. Nash DA, Nagel RJ. A brief history and current status of a dentaltherapy initiative in the United States. J Dent Educ 2005;69(8):857-859.
12. U.S. Public Health Service Dental Category. IHS Division ofOral Health Quality Assessment Guide: Section VII—Quality Assess-ment, Indirect Review of Clinical Quality and Risk Management(Chart Review). “www.phs-dental.org/depac/chap/qa.rtf”. AccessedSept. 16, 2008.
13. Patkotak E. Dental association offers no solution. AnchorageDaily News; Voice of the Times. Aug. 3, 2005.
14. U.S. Newswire. American dental association protests second-class dental care for American Indians, Alaska Natives. July 15,2005. “http://findarticles.com/p/articles/mi_hb5554/is_2005/ai_n21859990”. Accessed April 26, 2008.
15. American Public Health Association. Policy Statement Data-base: Support for the Alaska dental health aide therapist and otherinnovative programs for underserved populations. “www.apha.org/advocacy/policy/policysearch?id=1328”. Accessed April 26, 2008.
16. Alaska Native Tribal Health Consortium. Perspective: Politicsand the dental health aide initiative. “www.anthc.org/cs/chs/dhs/”.Accessed April 26, 2008.
17. Powell WO Jr, Sinkford JC, Henry JL, Chen MS. Comparison ofclinical performance of dental therapist trainees and dental students. J Dent Educ 1974;38(5):268-272.
18. Roder DM. The school dental therapist of South Australia. J Public Health Dent 1972;32(2):70-82.
19. Hoyle J. Association reaches settlement in Alaska litigation.“www.ada.org/prof/resources/pubs/adanews/adanewsarticle.asp?articleid=2582”. Accessed April 26, 2008.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
1536 JADA, Vol. 139 http://jada.ada.org November 2008
CommentaryASSESSMENT OF TREATMENT PROVIDED BY DENTAL HEALTH AIDE THERAPISTS IN ALASKA
Albert H. Guay, DMD
The introduction of dental health aidetherapists (DHATs) in the United Statesrepresents a major change in our oral
health care system. Nondentists are allowed todiagnose oral disease, develop a treatmentplan, and perform both routine and emergencynonreversible surgical procedures for patients.Supervision of DHATs by dentists varies fromdirect to general, and there is no requirementthat a dentist be present at the site of deliveryor even in the same town or village in whichcare is being provided.
It appears that concerns for the availabilityof oral health care, particularly in remote andfrontier areas, have overridden concerns forpatient safety and the efficacy of the treatmentprovided by DHATs. It is important, rather, itis critical that appropriate clinical research beconducted to examine the outcomes of this newmethod of delivering care to determine thesafest and most appropriate use of DHATs to increase access to appropriate and safe oral health care and the efficiency of dentalpractice.
In conducting such research, it is importantthat the investigations be well-designed (thatis, be appropriately controlled, be of adequateduration to draw valid conclusions, have suit-able and comparable samples and be able togenerate objective and relevant information).Since the evaluation of the safety and efficacyof treatments provided by DHATs is so impor-tant to the well-being of the public, conclusionsdrawn from this research should be derivedsolely from the study data.
The article “Assessment of Treatment byDental Health Aide Therapists in Alaska: APilot Study” by Dr. Kenneth Anthony Bolinreports on the results of a short-term study offour parameters used to compare the results ofdental care provided by dentists, DHATs underdirect supervision of a dentist and DHATsworking under general supervision. Using post-operative chart review only, the author selected
and audited four quality-of-care indicators:notation in the patient record, was treatmentprovided consistent with the diagnosis, theadequacy of radiographs and any report ofadverse events that occurred during or aftertreatment.
The study found that clinical notes were present for nearly all patients. There was nosignificant difference found between the groupsin the consistency between the treatment pro-vided and the diagnosis recorded. The DHATgroups had a significantly lower percentage ofadequate radiographs than the dentist groupdid. There was no significant difference in theincidence of adverse events between the studygroups.
An assessment of the quality and adequacyof clinical treatment requires much more thana chart review. Such reviews can shed somelight on the administrative aspects of care orthe processes used in delivering care, but theyprovide little insight into the outcomes of thatcare. Although administratively easy and rela-tively inexpensive to accomplish, chart reviewssimply cannot supply the information that isrequired to determine the quality and clinicaladequacy of care provided.
The age distribution of the patients in the sample was significantly skewed towardbeing younger. The sample matching betweengroups could have been better. The ages of the patients treated differed between thestudy groups, changing the baseline for comparisons.
The mere existence of clinical notes is not aprime factor in the assessment of the quality ofcare. The consistency of the treatment pro-vided with the diagnosis made fades in impor-tance compared with the accuracy of the diag-nosis in the first place, which was notevaluated. The limited scope of diagnostic andtreatment training DHATs acquire make amismatch of those factors unlikely.
The significant difference in the presence or
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
JADA, Vol. 139 http://jada.ada.org November 2008 1537
adequacy of radiographs appears to have beenexplained away by the differences in the agesof the patients treated by the DHATs and thedentists. If radiographs are required to estab-lish a proper diagnosis, they should be ofadequate quality to be useful, regardless of thedifficulty in taking them. The idea of over-looking this inadequacy in a “safe” procedurebecause of apparent clinical difficulty portendssignificant problems in the future if it is car-ried over to irreversible procedures with somesafety risk.
There was no significant difference betweenthe groups in the incidence of adverse eventsreported, although there was an almost four-fold increase in the percentage of adverseevents reported in the DHAT groups.
The far-reaching conclusion drawn by theauthor that “no significant evidence to indicatethat irreversible dental treatment provided byDHATs differed from similar treatment per-formed by dentists” cannot be drawn from the design of this study or from the data generated.
An extensive study of the outcomes of theexpanded role of DHATs in providing dentalcare for people needs to be conducted. It needsto be done well, as outlined above, so that itwill provide objective information that can beused to evaluate better the safety and efficacyof using DHATs in this new ancillary per-sonnel role.
Why has this commentary been written?Being responsible for overseeing the oralhealth of the public, the dental profession hasa responsibility to investigate and understandthe implications of such a landmark change inwho can deliver dental care. Public policy andthe policies of the dental profession should bebased as much as possible on adequate andobjective information and analysis. The price offailing in this analysis may be too high andwill be paid by those in the greatest degree ofjeopardy. !
Dr. Guay is the chief policy advisor, AmericanDental Association, 211 E. Chicago Ave.,Chicago, Ill. 60611, e-mail “[email protected]”.
The views expressed in this commentary are those of the authorand are not necessarily those of the American Dental Association or its subsidiaries.
RESPONSE TO COMMENTARY
Kenneth Anthony Bolin, DDS, MPH
No one will disagree with the commen-tator that “the introduction of dentalhealth aide therapists (DHATs) in the
United States represents a major change in ouroral health care system.” However, the allega-tion that “concerns for the availability of oralhealth care, particularly in remote and frontierareas, have overridden concerns for patientsafety and the efficacy of treatment” is anopinion that is not substantiated by evidence.
I can assure Dr. Guay that my work in thisarea also is founded on concerns for patientsafety and efficacy of treatment. As I referencedin the article, studies have been done in otherfirst-world countries in which dental therapistsare legally providing care to patients with noevidence of significant adverse effects. In thosecountries, as a result of the studies, concernsrelated to the safety and efficacy of dentaltherapy practitioners were shown to be ill-founded. Thus, I agree with Dr. Guay that conclusions “should be derived from solely fromthe study data,” not personal opinion.
I fully agree that “appropriate clinicalresearch be conducted to examine the out-comes.” I also agree that a definitive “assess-ment of the quality and adequacy of clinicaltreatment requires much more than a chartreview.” However, a retrospective analysis ofexisting clinical records, such as I conducted, isa reasonable and scientifically appropriate stepto take in the study of this important topic. Awell-controlled, prospective, longer-term studywill be needed to satisfactorily answer manyimportant questions. In such a design, the out-comes of care by DHATs will be compareddirectly with the outcomes of care by dentists.The most rigorous study design to addresssuch concerns is a randomized controlled trialin which patients are assigned randomly toeither a dentist or a DHAT for care, with thesame outcomes evaluation criteria and blindedevaluators used to assess the care given byeach type of provider.
The points that are raised in the commen-tary regarding the methodology of the data col-lection of this Alaska study are thoroughlydescribed in the methods and results sections
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
1538 JADA, Vol. 139 http://jada.ada.org November 2008
ADA on access to careJames Berry
A s a matter of policy, the American DentalAssociation (ADA) is committed toimproving access to dental care for all
those in need nationwide.The Association has labored proactively for
more than two years to enhance the existing dentalworkforce in ways that are expected to boost accessto care for the underserved—while also ensuringthat the care delivered is provided safely and effec-tively under the supervision of dentists.
At this writing (late September), the ADAHouse of Delegates was three weeks away fromdeliberating a resolution calling for continuedand expanded support for a new member of theoral health care team. The House also was dueto receive an informational report on a secondnew member of the team.
These new team members, briefly describedbelow, constitute only part of a much broaderADA response to the access problem. Other ele-ments of that response, to name a few, includeadvocating for improved funding and organiza-tion for Medicaid, expansion of the State Chil-
dren’s Health Insurance Program and such activ-ities as Give Kids A Smile.
COMMUNITY DENTAL HEALTH COORDINATOR
To be recruited from within their own distinctcommunities, Community Dental Health Coordi-nators (CDHCs) will help the underservedwithin the community to navigate the healthcare delivery system, breaking down barriers tocare and serving as patient advocates, facilita-tors and motivators.
CDHCs will work under a dentist’s supervi-sion in health and community settings such asschools and senior citizen centers, Head Startprograms and other public health settings.CDHCs will be trained to promote oral healthand to provide the most basic preventive servicesuntil the patient can receive comprehensive carefrom a dentist or dental hygienist. They will notdiagnose disease, nor will they perform any irre-versible procedures.
The CDHC is being developed in two phases.
of the article, and I addressed the items that areof concern to Dr. Guay in the discussion sectionof the article. My conclusion that no significantevidence was found “to indicate that irreversibledental treatment rendered by DHATs differedfrom similar treatment performed by dentists”is factually correct, and, thus, it is unclear whyDr. Guay believes that such a conclusion“cannot be drawn from the design of this studyor from the data generated.” As clinical scien-tists, we understand the limits of inference andrecognize that absence of evidence of an effect isnot the same thing as evidence for the absenceof an effect. Nevertheless, in my analysis, Ifound no statistically significant differences;that is, the null hypothesis was not rejected.Clearly, the rigorous scientific peer-reviewprocess followed by The Journal of the AmericanDental Association that preceded the acceptanceof my manuscript concluded that the analysis
and data were sound.In conclusion, I agree with Dr. Guay that fur-
ther “study of the outcomes of the expanded roleof DHATs in providing dental care for peopleneeds to be conducted.” Certainly, this articledescribes a pilot study as the subtitle states. Itgives us clues as to where we need to use ourscientific and critical thinking skills to help leadus in our design of further prospective outcomesstudies. In this way, the dental profession canbase conclusions on sound data, not on tradi-tion, opinion or political pressures. I look for-ward to seeing the results of those studies, oneof which is under way. !
Dr. Bolin is an assistant professor, Departmentof Public Health Sciences, Baylor College of Dentistry, Texas A & M University Health ScienceCenter, 3302 Gaston Ave., Room 705, Dallas,Texas 75246, e-mail “[email protected]”.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from

T R E N D S
JADA, Vol. 139 http://jada.ada.org November 2008 1539
Phase 1—development of an 18-month trainingprogram—has been completed. Phase 2involves pilot training programs at three sites:one Native American, one urban and one rural.Training is expected to begin in early 2009.
ORAL PREVENTIVE ASSISTANT
Also in development for two years, the OralPreventive Assistant (OPA) workforce model isdesigned to foster an expanded preventivecapability within the dental team by providingcertain basic preventive services and freeingdentists and dental hygienists to concentrate onpatients with more complex needs.
OPAs will provide patients with oral healtheducation and information, as well as performcertain limited procedures—coronal polishingfor all patients and scaling for patients withplaque-induced gingivitis—contingent on stateregulations.
OPAs will work mainly in private dentaloffices, though their knowledge of oral healtheducation also will enable them to work inschools, community health centers and othervenues to raise oral health literacy.
A modular OPA curriculum provides atraining program lasting about three monthsand assumes enrollees are dental assistantswho have qualified for the program through oneof four eligibility pathways:dgraduate of an accredited dental assistingprogram (accredited by the Commission onDental Accreditation [CODA]);dcertified dental assistant (certified by theDental Assisting National Board [DANB]);dgraduate of a dental assisting program notaccredited by CODA but still a DANB-certifieddental assistant;don-the-job–trained dental assistant who is aDANB-certified dental assistant.
Over the past several years, no single issuehas commanded more attention from theADA—and from ADA publications, both inprint and online—than access to care. Nodoubt, that will continue in the years ahead asthe Association’s response to the accessproblem gains ground. !
Mr. Berry is the associate publisher, ADA Publishing.
on Novem
ber 1, 2008 jada.ada.org
Dow
nloaded from