Embed Size (px)
DESCRIPTION
Mobile phone in oral cancer surveillance.
Citation preview

Mobile health application for remoteoral cancer surveillancePraveen N. Birur, MDS; Sumsum P. Sunny, MDS;Sidhant Jena, MS; Uma Kandasarma, MDS;Shubhasini Raghavan, MDS; Bhanushree Ramaswamy, MDS;Sunitha Perumal Shanmugam, BDS; Sanjana Patrick, BDS;Rohan Kuriakose; Janhavi Mallaiah, MBBS;Amritha Suresh, PhD; Radhika Chigurupati, DMD, MS;Rani Desai, MA; Moni Abraham Kuriakose, MD
E ighty percent of the worldwide burden of oralcancer occurs in low-resource settings withpoor access to oral cancer specialists.1,2 Thisis one of the primary reasons for delayed
diagnosis and poor outcome. The stage of disease atdiagnosis is the single most important factor that de-termines the treatment outcome of oral cancer patients.The estimated age-adjusted incidence rate of oral cancerin a low-resource setting such as India is 20 of 100,000,which is one of the highest in the world.3 Oral canceraccounts for 23% of all cancer-related deaths in theIndian subcontinent.4 A system that offers specialistconsultation for dentists and health workers in low-resource settings may help identify high-risk patientssusceptible to oral cancer or to diagnose the cancer atan early stage.
The use of wireless networking and telemedicinehas been investigated for improving disease surveillanceand to provide remote specialist consultation. Theaddition of Web-based evaluation has improved breastcancer screening by mammography and detection ofdisease relapse in lung cancer patients.5,6 The extensivenetwork of mobile phones prevalent across populationsof all socioeconomic strata makes it a logical mode todevelop a similar system for screening and early detec-tion of oral cancer. It has been previously demonstratedthat mouth self-examination7 or examination by trainedpersonnel8 can down-stage oral cancer and significantlyimprove survival rates in a high-risk population. An
Copyright ª 2015 American Dental Association. All rights reserved.
ABSTRACT
Background. To determine the effectiveness of a mobilephone–based remote oral cancer surveillance program(Oncogrid) connecting primary care dental practitionersand frontline health care workers (FHW) with oral cancerspecialists.Methods. The study population (N ¼ 3,440) included atargeted cohort (n ¼ 2,000) and an opportunistic cohort(n ¼ 1,440) screened by FHW and dental professionals,respectively. The authors compared the screening efficacyin both groups, with specialist diagnosis considered thereference standard. The outcomes measured were lesiondetection and capture of interpretable images of the oralcavity.Results. In the targeted cohort, among 51 of 81 (61%)interpretable images, 23 of 51 (45%) of the lesions wereconfirmed by specialists, while the opportunistic cohortshowed 100% concordance with the specialists (106 of 106).Sixty-two of 129 (48%) of the recommended patients un-derwent biopsy; 1 of 23 (4%) were in the targeted cohort,and 61 of 106 (57%) were in the opportunistic cohort.Ninety percent of the lesions were confirmed to be malig-nant or potentially malignant.Conclusions. The mobile health–based approach adop-ted in this study aided remote early detection of oral cancerby primary care dental practitioners in a resource-constrained setting. Further optimization of this programis required to adopt the system for FHW. Evaluation of itsefficacy in a larger population is also warranted.Practical Implications. The increased efficiency ofearly detection by dentists, when assisted by a remotemobile health–based approach, is a step toward a moreeffective oral cancer screening program.Key Words. Oral cancer; early detection; screening;mobile health; health workers; remote assistance; primarycare dentist.JADA 2015:-(-):---
http://dx.doi.org/10.1016/j.adaj.2015.05.020
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
ORIGINAL CONTRIBUTIONS
JADA -(-) http://jada.ada.org - 2015 1

improvisation of this program by providing remotespecialist consultation is likely to improve scalabilityof this concept. In this project, we attempted to develop amobile phone–based platform for risk stratification andevaluation of the mouth, which is remotely monitoredby oral cancer specialists. We hope that adapting thistechnology in a low-resource, high-risk population willbe a step toward down-staging oral cancer.
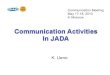
METHODSStudy design. Oncogrid is a mobile phone–based cancersurveillance program developed as a hub-and-node–based model (Figures 1 and 2). The hub is located at atertiary care cancer center (Mazumdar-Shaw CancerCenter, Bangalore, India), and the nodes are located in 2different settings: dentists in a dental clinic and frontlinehealth care workers (FHW) associated with a primaryhealth center. The project was approved by the relevantinstitutional research and ethics committees. Informedconsent was obtained from all participating patients. Thework flow involved the use of an Android mobile phone(HTCWildfire S, 5MP camera) and oral cancer screeningsoftware equipped with a clinical decision algorithm for
risk assessment and diagnosis (Figure 1). This study wasconducted over 12 months (January to December 2010).
Study population and screening. Cohort 1, the tar-geted group, consisted of participants from 2 rural vil-lages, Anakanur (n ¼ 2,055) and Poshetahalli (n ¼ 3,184),of the Chikkabalapur district in the suburbs of BangaloreCity. These participants, who had a high prevalence oforal cancer risk habits, were selected on the basis of aprior health survey carried out by a voluntary nongov-ernmental organization (Biocon Foundation, Bangalore,India). The targeted cohort, consisting of all eligibleparticipants in this defined population, was screened bythe FHW (n ¼ 4) (associated with the primary healthcenter) in a door-to-door manner. Cohort 2 includedparticipants screened by dental surgeons in a primarydental clinic. Because the screening was conducted inpatients attending the clinic (KLES Institute of DentalSciences, Bangalore) for other treatment, the cohort wastermed the opportunistic group. In both cohorts, the
Targeted Cohort(Frontline Health Care Workers)
Tertiary cancer centerRemote consultation with an oral
cancer specialist
Tertiary cancer centerHistologic evaluation of
confirmed patients
Opportunistic Cohort(Dental Surgeons)
Co-coordinatingcancer center
Frontlinehealth care
workers
Frontlinehealth care
workersFrontline
health careworkers
Nodal center
Primaryhealth center
Nodal center
Dental collegeor clinic
Dentist
Frontlinehealth care
workers
Frontlinehealth care
workers
A B
Nodal center
Primaryhealth center
Frontlinehealth care
workers
print&
web4C=F
PO
Figure 1. Node-and-hub model and overall study design. A. Study was carried out with a central coordinating center and multiple nodal centers.B. Study design included 2 patient cohorts, targeted and opportunistic; images from both cohorts were sent to the tertiary care center for remoteconsultation and histologic evaluation.
ABBREVIATION KEY. FHW: Frontline health care worker.GPRS: General packet radio service. mHealth: Mobile health.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
2 JADA -(-) http://jada.ada.org - 2015

triaging of the partici-pants as members of ahigh-risk group wasbased on the presence ofany of the following 3factors: history of riskhabits (smoking tobacco,chewing betel leaf orgutka [combination ofareca nut with or withouttobacco], or regular useof alcohol), older than 40years, and clinical signs(nonhealing ulcers, redor white patches of themouth that last morethan 3 weeks, restrictionof mouth opening, andswelling of the neck).
The dentists andFHW involved in thisproject underwent astructured training pro-gram by oral cancerspecialists on risk factorsand screening methodsto identify suspicious le-sions using interactiveeducation materials. The health care providers weretrained to examine different subsites of the oral cavity ina systematic fashion. These included right gingivobuccalmucosa and retromolar trigone, lower labial mucosa, leftgingivobuccal mucosa and retromolar trigone, upperlabial mucosa, palate, floor of the mouth, and oraltongue. The tongue was further divided into dorsal,ventral, right, left, and lateral borders. The FHWs werealso trained to specifically examine the region in the oralcavity where the gutka or tobacco was placed for chew-ing. The specialists providing remote consultation wereasked to report the lesions as nonneoplastic, potentiallymalignant, or malignant.
The patients who were diagnosed with oral lesions inthe targeted cohort were monitored by the FHW onceevery 3 months for 2 years by clinical examination andfor habit cessation counseling. Patients with oral lesionsrecommended for biopsy by remote experts review werereferred to oral cancer specialists in the dental college orto the tertiary care cancer center.
Technology platform. The mobile health (mHealth)system used for the Oncogrid project was developed usingthe Sana platform (Computer and Artificial IntelligenceLaboratory, Massachusetts Institute of Technology, http://sana.mit.edu) and OpenMRS (http://openmrs.org), anopen-source medical record system. Sana is designed as awork flow interface and is integrated with OpenMRS, aJava-based Web application that can be used to input and
store data for individual patients. The latter includes aconcept dictionary, which can be used to define andgather multiple observations from a single encounterand also has built-in support modules, which is key inimplementing Sana in rural areas.
At the front end, Sana, downloaded onto the phone, isused for media and data (audio, image, location-baseddata, and text) capture, and at the back end provides anintuitive user interface for management of the media.Sana also allows modularity and interoperation, allowingmultiple front-end data to be accessed by the coordina-tion center. The software also includes built-in trainingand work flow solutions at the mobile phone level. Datatransfer is carried out using a number of interfaces,including general packet radio service (GPRS), wi-fi, textmessages, and USB tethering, and was controlled algo-rithmically to ensure reliable upload in regions with poormobile network coverage. To avoid midupload failure ofdata containing large image files, Sana uses “packetiza-tion,” which allows upload of files in chunks so that largefiles can be sent to the server even with smaller bandwidth.
The synchronization between the server that hostsSana and the OpenMRS was through GPRS. The projectalso involved customization of OpenMRS through thedevelopment of an Oncogrid-specific dashboard tomonitor the work flow, individual patient evaluation, andfeedback. The individual images were visualized in detailvia zooming and contrast adjustment. As the OpenMRS
Oral cancer specialist at thecancer center
OpenMRSOpen-source medical
record program
SanaOpen-source mobile
health platform
Server
Frontline health care workers
print&
web4C=F
PO
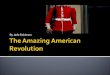
Figure 2. Oncogrid technology architecture. Overall pipeline of Oncogrid program is depicted; patient details andimages are captured through Sana. Data are then uploaded to the OpenMRS system and subsequently accessedby specialists at the tertiary care center. Feedback from the specialists is sent back to frontline health care workers.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
JADA -(-) http://jada.ada.org - 2015 3

is health level 7 standard messaging systemcompatible, the data could be exported tothe hospital medical record system in casesin which the patients required a visit to thespecialist center. The data could also beexported standard statistical softwarepackages for detailed analysis and report-ing. The overall technology platformdeployed for Oncogrid is depicted inFigure 2.
Work flow. The Sana software on mo-bile phone generates patient registrationnumber, date of registration, and de-mographic details. Each participant wasinterrogated using a risk evaluation ques-tionnaire incorporated in the application.The details obtained consisted of demo-graphics, risk factors, and symptoms (Box).It included the following questions: Is yourage greater than 40? Do you have a familyhistory of cancer? Do you drink alcohol? Doyou smoke cigarettes or beedi (local ciga-rette)? Do you chew paan (betel leaf) withtobacco (gutka or areca nut)? Do you haveany white or red patches in your mouth? Doyou have any ulcers in your mouth? Doyou have any swelling of neck or difficultyin opening the mouth? If the answer to anyof these questions is yes, then the patientwas considered to be at high risk and wasenrolled onto the study after providinginformed consent. Intraoral lesions, if pre-sent, were photographed. The data obtainedthrough the mobile phones, along withphotographs of the suspicious lesions, wereuploaded to the OpenMRS system througha secure server.
The system then created a queue thatwas reviewed at the coordinating centerby the oral cancer specialist. The specialistreviewed the image and judged it as inter-pretable or not interpretable. The inter-pretable images were clinically stratified asnonneoplastic, potentially malignant, ormalignant. For oral potentially malignantand malignant lesions, it was recommendedthat the patients undergo biopsy. Textmessages (also known as short messagingservices, or SMS) with follow-up in-structions were sent to the respective FHWand dentists. On receiving the message, theFHW and dentists referred patients withsuspected lesions to the nodal centers (pri-mary health clinic or dental college) forbiopsy. Reporting errors at all levels weremanaged effectively with digital storage and
BOX
Questionnaire to assess clinical details ofpatients.
TARGETED SCREENING COHORT1. Enter patient medical record identification number2. Enter patient first name3. Enter patient last name4. Enter patient birthdate5. Select patient sex6. Enter patient mobile number7. Health center8. Age (40þ): yes or no9. Family history of cancer: yes or no10. Education level: none, high school, or college11. Employed: yes or no12. Drinker: no, social, or heavy13. Smoker: no, social, or heavy14. Paan or chewing tobacco: no, social, or heavy15. Visit dentist: yes or no16. Does the patient have or had any symptoms of oral lesion, lump in neck, or difficultyopening mouth: yes or no17. Add picture.18. Save and upload to server.
OPPORTUNISTIC SCREENING COHORT1. Enter patient medical record identification number2. Enter patient first name3. Enter patient last name4. Enter patient birthdate5. Select patient sex6. Enter patient mobile number7. Health center8. Age (40þ): yes or no9. Family history of cancer: yes or no10. Education level: none, high school, or college11. Employed: yes or no12. Drinker: no, social, or heavy13. Smoker: no, social, or heavy14. Paan or chewing tobacco: no, social, or heavy15. Visit dentist: yes or no16. Does the patient have or had any symptoms of difficulty opening mouth, mouth ulcer,white or red patch in mouth. swelling in neck, or growth in mouth: yes or no.- If yes for mouth ulcer or sore: less than 3 weeks or more than 3 weeks; one or multiple;painful, loss of sensation, or no pain; how is surrounding tissue: everted or not everted.- If yes for white patch: duration of patch: less than 3 weeks or more than 3 weeks;cannot be wiped off or can be wiped off; how many patches: single or multiple; how isthe surface of the patch: irregular or uniform; what is the color of the patch: white orwhitish red; how does the patch feel: painful or no pain.- If yes for swelling in neck; less than 3 weeks or more than 3 weeks; consistency ofswelling in neck: firm or soft; fixation of swelling in neck: mobile or fixed; skin overswelling in neck: smooth, normal, or irregular; location of swelling in neck: lateral ormidline; size of swelling in neck: less than 2 centimeters, 2 to 4 cm, 4 to 6 cm, or morethan 6 cm.- If yes for growth: less than 3 weeks or more than 3 weeks; any changes in size ofgrowth: increased, no change, or decreased; how does the growth feel: painful, lossof sensation, or no pain; how is the consistency of the growth: firm or soft; how is thesurface of growth: irregular overlying mucosa or regular overlying mucosa; conditionof teeth around growth: loose or normal.17. Add picture18. Save and upload to server
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
4 JADA -(-) http://jada.ada.org - 2015

transfer of data to improve FHW and dentists’ efficiencyin screening. A continuous feedback of the results wasprovided to the FHW and dentists through mobilephones. A Web-based dashboard also facilitated the pro-gram coordinators to detect bottlenecks and rectify them.
Histologic evaluation and follow-up. The histo-pathologic reporting of the oral lesion was done asper the World Health Organization classification; oralepithelial precursor lesions were classified into 6 cate-gories (squamous cell hyperplasia; mild, moderate,and severe dysplasia; carcinoma-in-situ; invasive carci-noma).9 For treatment decisions, we adopted the binarysystem developed by Kujan and colleagues.10 Accord-ingly, nondysplastic lesions were combined with milddysplasia as low-risk lesions, while moderate and severedysplasia along with carcinoma-in-situ were grouped ashigh-risk lesions. The biopsy results were also uploadedvia mobile phone by the nodal center to the OpenMRS.
Patients with nonneoplastic lesions were dischargedafter antitobacco counseling while those with low-risklesions were counseled for habit cessation and prescribedtopical application of water-soluble vitamin A palmitrate(Aquasol-A, USV Limited [Mumbai]; 50,000 UnitedStates Pharmacopeia units per milliliters) twice daily for3 months.11,12 Patients with high-risk lesions and invasivecancer were referred to the tertiary care cancer center forsurgical excision and adjuvant treatment as per estab-lished cancer treatment guidelines.
Compliance with biopsy and treatment at nodal andcancer centers were monitored through OpenMRS.Long-term surveillance after completion of treatmentwas carried out in the community in partnership withthe nodal center. All patients were educated about theharmful effects of tobacco and areca nut. Patients withhigh-risk habits were kept under surveillance by theFHW to monitor compliance to counseling and the
Patients involvedin mobile phone
screening(n = 83)
Patients notinvolved in mobilephone screening
(n = 47)
Cohort ITargeted screening by
frontline health care workers(n = 2,000)
Patients in thehigh-risk group
with lesion(n = 130)
Noninterpretableimages(n = 32)
Interpretableimages(n = 51)
Lesions negative onremove diagnosis
(n = 28)
Lesions positive onremove diagnosis
(n = 23)
Patients involvedin mobile phone
screening(n = 106)
Patients notinvolved in mobilephone screening
(n = 0)
Cohort IIOpportunistic screeningby dental professionals
(n = 1,440)
Patients in thehigh-risk group
with lesion(n = 106)
Noninterpretableimages(n = 0)
Interpretableimages
(n = 106)
Lesions negative onremove diagnosis
(n = 0)
Lesions positive onremove diagnosis
(n = 106)
Studypopulation
print&web4C=F
PO
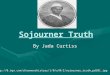
Figure 3. Patient distribution across 2 cohorts—cohort 1 (targeted; n ¼ 2,000) and cohort 2 (opportunistic; n ¼ 1,440)—and number of high-risklesions identified. All patients screened in cohort 2 consented to mobile screening; in cohort 1, 47 patients were not involved in screening. All 106images were interpretable and diagnosed positively in cohort 2, while in cohort 1, 38% (n ¼ 32) of the images were noninterpretable, and 45% (n ¼ 23)of identified lesions were confirmed positive.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
JADA -(-) http://jada.ada.org - 2015 5

progression of the lesions, if any, using the Oncogridplatform.
Statistical analysis. Statistical analysis was carriedout to determine the concordance of the diagnosisby FHW and dentists with remote diagnosis by the
specialist. All statisticalcalculations were carriedout by GraphPad software(GraphPad Software).
RESULTSPatient cohort. Thetotal study population con-sisted of 3,440 patients,with 2,000 patients assignedto cohort 1 (screened byFHW) and 1,440 to cohort2 (screened by dental pro-fessionals). Patient distri-bution is provided inFigure 3.
Targeted screening byFHW. Among the 2,000patients screened by FHW(n ¼ 4), the female-to-maleratio was high (3:1); patientswere within the age rangeof 20 to 85 years. Targetedscreening identified 130 pa-tients (6.5%) with suspi-cious lesions. Thirty-sixpercent of these patients(n ¼ 47) did not provideconsent for being photo-graphed and were excludedfrom the study. The imagesfor 83 accrued patients werecaptured and transmittedto the coordinating centerfor consultation (Figure 4).Images for 32 patients (38%)were judged to be non-interpretable by the oralcancer specialist at thecenter. Among the 51 in-terpretable images, theremote specialist confirmedthe diagnosis of 23 patientswith either potentially ma-lignant (n ¼ 22) or malig-nant lesions (n ¼ 1). TheFHW were hence able todetect the patients withpositive lesions with a pos-itive predictive value of45%, with the specialist
consultation being the reference standard. These patientswere referred to the nodal center for biopsy.
Opportunistic screening by dental professionals.Among the 1,440 patients screened by the dental pro-fessionals in cohort 2, the male-to-female ratio was 3:1;
print&web4C=F
PO
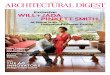
Figure 4. Representative images taken from opportunistic and targeted cohorts and from OpenMRS. Imagestaken by dentists of patients in the opportunistic cohort (A, B) and by frontline health care workers in thetargeted cohort (C, D). D. Uninterpretable image taken by a frontline health care worker. E. Snapshot of theOpenMRS system. Patient details are masked to protect patient confidentiality.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
6 JADA -(-) http://jada.ada.org - 2015

patients were within the agerange of 18 to 73 years. Onehundred six patients were iden-tified to have oral potentiallymalignant or malignant lesions.All patients consented to andwere accrued for the study. Theimages of all patients uploaded bythe dental professionals werefound to be of diagnostic quality(Figure 4, Table). The oral cancerspecialists at the coordinatingcenter confirmed all the lesionsto be potentially malignant(n ¼ 101) or malignant (n ¼ 5).The concordance and positivepredictive value of dental pro-fessionals’ interpretation was100%.
Histologic evaluation. Thepatients from both cohort 1(n ¼ 23) and cohort 2 (n ¼ 106)with high-risk lesions were referred for histologic eval-uation. Out of these 129 patients, 62 (cohort 1, n ¼ 1;cohort 2, n ¼ 61) underwent biopsy; compliance incohort 1 was 4% (1 of 23) compared with 57% (61 of 106)in cohort 2. Seventy-nine percent of the biopsy resultswere reported as lesions with dysplasia (49 of 62), while9.6% were malignant lesions (n ¼ 6). Nine percent (6 of62) of the biopsy findings were reported as nonmalig-nant (no evidence of malignant or potentially malignantchanges) and 2% (n ¼ 1) were nondysplastic leukoplakia(epithelial hyperplasia without dysplasia). Amongthe dysplastic lesions, 49% were with mild dysplasia(n ¼ 24), while others were moderate (31%, n ¼ 15) andsevere (20%, n ¼ 10). The patient referred from cohort 1was diagnosed with malignancy (Table). All the malig-nant lesions (n ¼ 6) in both the cohorts were stage I(T1, N0, M0) lesions.
Among the dysplastic patients in cohort 2, 38%(n ¼ 19) of patients showed compliance for follow-upin the dental clinic. None of these patients developedclinical evidence of disease progression during the2 years of follow-up. All 23 patients in cohort 1 duringthe 2 years of follow-up also did not develop malignanttransformation.
DISCUSSIONThe low survival rates of oral cancer patients in low-resource settings are primarily dependent on the stageat diagnosis. The late presentation of patients is attrib-uted to the limited access to specialized clinical services.Population-based oral cancer screening programs by vi-sual inspection in low-resource settings have shown toreduce mortality by 34%.8 Similar benefits have been
reported in cervical and breast cancer screeningprograms.8,13,14
The use of mobile phone technology has the poten-tial to bridge disparity in terms of access to healthcare by combining visual screening with remote con-sultation. Mobile diagnostic systems in combinationwith e-communication and off-site expert diagnosishave been attempted at remote locations for early de-tection of lung and cervical cancers as an effort towardproviding specialist expertise to inaccessible, low-resource settings.6,15 Accessibility for clinical examina-tion, presence of well-defined risk factors, and clinicalfeatures make oral cancers well suited for mobile phone–based screening. In this study, we report potentialeffectiveness of mHealth-aided oral cancer screeningin targeted (by FHW) and opportunistic (by dentalprofessionals) cohorts.
A comparative analysis of screening in both the co-horts, aided by remote diagnosis of oral cancer specialists,indicated that opportunistic screening (dentists) workedbetter in terms of lesion detection, image quality, anddiagnostic accuracy. The FHW were able to detect lesionsin 5% of the patients and transmit images with 61% ac-curacy, compared with the 100% accuracy achieved by thedental surgeons. In mHealth-based studies, the depen-dence of diagnosis on the quality of the photographs isan issue. However, the high efficacy of image captureby dental professionals indicated that the technology isrobust. In contrast, 38% of the images in the targetedcohort were not interpretable, suggesting that furthertraining of the FHW or newer technology that overcomeshuman error needs to be developed. We are in the processof developing an automated oral photography capturedevice to overcome this limitation.
TABLE
Comparison of outcome between targeted andopportunistic screening groups.EVENT TARGETED
SCREENING(N [ 2,000)
OPPORTUNISTICSCREENING(N [ 1,440)
NO. % NO. %
No. of High-risk Patients With Lesion 130 6.5 106 7.36
No. of Patients Consented to Capture Images 83 63.85 106 100.00
No. of Interpretable Images 51 61.45 106 100.00
Remote Diagnosis Confirmation of PotentiallyMalignant or Malignant Lesion by Specialists
23 45.10 106 100.00
No. of Patients Who Underwent HistologicEvaluation
1 4.35 61 57.55
Normal 0 0.00 6 9.84Severe dysplasia 0 0.00 10 16.39Moderate dysplasia 0 0.00 15 24.59Mild dysplasia 0 0.00 24 39.34Nondysplastic lesions 0 0.00 1 1.63Squamous cell carcinoma 1 100.0 5 8.20
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
JADA -(-) http://jada.ada.org - 2015 7

One of the issues in the program was the difficulty inevaluating the specificity of diagnosis in both the cohorts.The confirmation of a negative diagnosis by on-sitespecialists was not feasible because the program wasconceived as an outreach screening program. Neverthe-less, the fact that 45% of the lesions detected by the FHWwere confirmed by the specialists indicated that they maybe an invaluable resource for door-to-door screening inlow-resource settings. The accuracy of detection increasedwith remote diagnosis; 54% of the patients avoided un-necessary referral and biopsy.
This study also provided evidence that advancedtraining in terms of oral cancer detection and mHealthsystems can aid FHW in carrying out oral cancerscreening and surveillance. In a lung cancer program,when patients themselves were trained appropriately,early detection of disease relapse was observed.6 On-sitediagnosis by trained nurses also showed high concor-dance with off-site experts in a cervical cancer screeningprogram.15 Remote connectivity to specialist centers hasalso been successfully implemented in rural populations,including India, with a definite clinical advantage innonmalignant disorders.16-21 Nevertheless, these projectslacked the ability to reach out to asymptomatic patientsat their workplace or home, which is desirable in cancerscreening programs. However, it is to be noted thatall the cancer patients diagnosed in this study were stageT1 (< 2 centimeters) disease, further attesting to thepotential of mHealth for detection of both early stagemalignant or potentially malignant lesions.
In a cervical cancer screening study, telemedicineenabled effective diagnosis, thereby reducing delaysin referrals and the need for travel from distant sites.15
In our study, aided by remote consultation, 54% of thepatients were diagnosed as negative for the lesions whenassessed by the specialist, ensuring that only patientswith confirmed clinical lesions were referred to the ter-tiary care center. mHealth consultation is thus also aneffective strategy to increase the efficacy of the FHWin terms of detecting high-risk lesions and avoidingunnecessary referrals.
Compliance was a primary issue in the study, espe-cially in the targeted screening group. Only 4% fromcohort 1 and 57% from cohort 2 underwent the recom-mended biopsy. Similar results were observed in otherstudies, in which the compliance to biopsy was only10%.7 Multiple factors such as denial of their medicalcondition, asymptomatic nature of high-risk oral lesions,invasiveness of the procedure, need to travel to the nodalcenters, and poor socioeconomic background contributeto this poor compliance. As observed in other oral cancerscreening trials, multiple rounds of screening may berequired to improve compliance.22 In addition, alterna-tive noninvasive approaches such as the use of molecularimaging techniques23 and salivary biomarkers mightserve to address this issue. Nevertheless, mHealth has
shown potential to improve compliance through auto-mated communication directly to patients (text mes-sages, Web-based methods, tailored education), as hasbeen observed in many other studies, including colo-rectal cancer24 and breast cancer.5 On the basis of thesuccess of this project, we have initiated a randomizedstudy comparing the cost-effectiveness of mHealthand conventional oral cancer screening in a largerpopulation.
One of the major challenges in the management oforal potentially malignant lesions is the histologic inter-pretation of oral dysplasia and developing a decision-making algorithm based on the grade of dysplasia.Although Holmstrup and colleagues25 reported variousrates of malignant transformation in nondysplastic (2% to11%) and mild dysplastic lesions (11% to 14%), no corre-lation was observed between the levels of dysplasia andmalignant transformation. However, several other studieshave demonstrated severity of dysplasia to be a significantpredictor for malignant transformation.10,26,27 To lowerinterobserver variability and to make therapeutic de-cisions, a binary system of dysplasia grading was pro-posed by Kujan and colleagues.10 In this study, we haveused this binary system for the management of oralpotentially malignant lesions. According to thisdecision-making algorithm, nondysplastic and milddysplastic lesions were managed conservatively by habitcessation and chemoprevention, while moderate andsevere dysplastic lesions were treated by chemopre-vention and surgical intervention in addition to habitcessation.
CONCLUSIONSThis pilot telemedicine program is novel in that itfound that mobile phone–based oral cancer screeningand surveillance were feasible in low-resource settings. Itfacilitated optimal utilization of professional resourcesand early detection of asymptomatic oral neoplasticlesions. In the long term, this strategy is expected todown-stage oral cancer and improve survival rates.With wide penetration of the mobile phone network,including in remote locations, this project will have amajor impact in the way oral cancer is managed in thecommunity. In the future, we foresee that medical anddental institutions equipped with knowledge in epide-miology, prevention, and screening, when remotelyintegrated to a local community cancer screening ser-vice and a regional tertiary cancer center, will bringabout a paradigm change in cancer care and outcomesin low-resource settings. As an initial step in this direc-tion, we are in the process of developing a networkof mHealth-based oral cancer outreach screeningprograms. n
Dr. Birur is a professor and head, Department of Oral Medicine andRadiology, KLES Institute of Dental Sciences, Bangalore, India.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:39 pm ! ce
8 JADA -(-) http://jada.ada.org - 2015

Dr. Sunny is a senior house officer, Head and Neck Oncology, MazumdarShaw Cancer Center, and a doctoral student, Integrated Head and NeckOncology Program, Mazumdar Shaw Center for Translational Research,Mazumdar Shaw Medical Foundation, Mazumdar Shaw Medical Center,Bangalore, India.Mr. Jena is the chief executive officer, Jena Care, Koramangala, Bangalore,
India.Dr. Kandasarma is a professor and head, Department of Oral and
Maxillofacial Pathology, KLES Institute of Dental Sciences, Bangalore, India.Dr. Raghavan is a reader, Department of Oral Medicine and Radiology,
KLES Institute of Dental Sciences, Bangalore, India.Dr. Ramaswamy is a lecturer, Department of Oral Medicine and Radi-
ology, KLES Institute of Dental Sciences, Bangalore, India.Dr. Shanmugam is a surgeon, Dental Section, Government Hospital,
Hosur, India.Dr. Patrick is a post graduate student, Department of Oral Medicine and
Radiology, KLES Institute of Dental Sciences, Bangalore, India.Mr. Rohan Kuriakose is an undergraduate student, School of Engineering,
University of Buffalo, Buffalo, NY.Dr. Mallaiah is a program officer, Biocon Foundation, Bangalore, India.Dr. Suresh is a principal investigator, Integrated Head and Neck Oncology
Program, Mazumdar Shaw Center for Translational Research, MazumdarShaw Medical Foundation, Mazumdar Shaw Medical Center, Bangalore,India, and a research technologist, Mazumdar Shaw Cancer Centre, RoswellPark Collaborative Head and Neck Oncology Research Program, RoswellPark Cancer Institute, Buffalo, NY.Dr. Chigurupati is an associate professor, Department of Oral and
Maxillofacial Surgery, Boston University, Boston, MA.Ms. Desai is the head, Biocon Foundation, Bangalore, India.Dr. Moni Abraham Kuriakose is a director, Department of Surgical
Oncology, Mazumdar Shaw Cancer Center, Narayana Health, and a pro-fessor and vice chairman, Department of Head and Nech, Plastic andReconstructive Surgery, Roswell Park Cancer Institute, Buffalo, NY. Addresscorrespondence to Dr. Kuriakose at Department of Surgical Oncology,Mazumdar Shaw Cancer Center, Narayana Health, 258/A, BommasandraIndl Area, Anekal Taluk, Bangalore 560099, India, e-mail [email protected].
Disclosure. None of the authors reported any disclosures.
This project was funded by Krishak Bharati Co-operative Limited,Gautham Budh Nagar, UP, India. The authors acknowledge the supportof Mazumdar Shaw Medical Foundation, Narayana Health City, and KLESInstitute of Dental Sciences, Bangalore, India.
1. Mignogna MD, Fedele S, Lo Russo L. The World Cancer Report andthe burden of oral cancer. Eur J Cancer Prev. 2004;13(2):139-142.2. Warnakulasuriya S. Global epidemiology of oral and oropharyngeal
cancer. Oral Oncol. 2009;45(4-5):309-316.3. Coelho KR. Challenges of the oral cancer burden in India. J Cancer
Epidemiol. 2012;2012:701932.4. Dikshit R, Gupta PC, Ramasundarahettige C, et al. Cancer mortality in
India: a nationally representative survey. Lancet. 2012;379(9828):1807-1816.5. Atlas SJ, Grant RW, Lester WT, et al. A cluster-randomized trial of a
primary care informatics-based system for breast cancer screening. J GenIntern Med. 2011;26(2):154-161.6. Denis F, Viger L, Charron A, et al. Detection of lung cancer relapse
using self-reported symptoms transmitted via an internet web-application:pilot study of the sentinel follow-up. Support Care Cancer. 2014;22(6):1467-1473.
7. Elango KJ, Anandkrishnan N, Suresh A, et al. Mouth self-examinationto improve oral cancer awareness and early detection in a high-risk pop-ulation. Oral Oncol. 2011;47(7):620-624.8. Sankaranarayanan R, Ramadas K, Thomas G, et al. Effect of screening
on oral cancer mortality in Kerala, India: a cluster-randomised controlledtrial. Lancet. 2005;365(9475):1927-1933.9. Barnes L, Eveson JW, Reichart PA, Siransky D, eds. Pathology and
Genetics of Head and Neck Tumours. Lyon: IARC Press; 2005. Available at:http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb9/BB9.pdf.Accessed May 29, 2015.10. Kujan O, Oliver RJ, Khattab A, et al. Evaluation of a new binary
system of grading oral epithelial dysplasia for prediction of malignanttransformation. Oral Oncol. 2006;42(10):987-993.11. Epstein JB, Gorsky M. Topical application of vitamin A to oral leu-
koplakia: a clinical case series. Cancer. 1999;86(6):921-927.12. Piattelli A, Fioroni M, Santinelli A, Rubini C. bcl-2 expression and
apoptotic bodies in 13-cis-retinoic acid (isotretinoin)-topically treated oralleukoplakia: a pilot study. Oral Oncol. 1999;35(3):314-320.13. Feig SA. Screening mammography: a successful public health initia-
tive. Rev Panam Salud Publica. 2006;20(2-3):125-133.14. Heim K, Widschwendter A, Szedenik H, et al. Specific serologic
response to genital human papillomavirus types in patients with vulvarprecancerous and cancerous lesions. Am J Obstet Gynecol. 2005;192(4):1073-1083.15. Quinley KE, Gormley RH, Ratcliffe SJ, et al. Use of mobile telemed-
icine for cervical cancer screening. J Telemed Telecare. 2011;17(4):203-209.16. Bhaskaranarayana A, Satyamurthy LS, Remilla ML. Indian Space
Research Organization and telemedicine in India. Telemed J E Health.2009;15(6):586-591.17. Klein D, Davis P, Hickey L. Videoconferences for rural physicians’
continuing health education. J Telemed Telecare. 2005;11(suppl 1):97-99.18. Pak HS, Brown-Connolly NE, Bloch C, et al. Global forum on tele-
medicine: connecting the world through partnerships. Telemed J E Health.2008;14(4):389-395.19. Richter GM, Williams SL, Starren J, Flynn JT, Chiang MF. Tele-
medicine for retinopathy of prematurity diagnosis: evaluation and chal-lenges. Surv Ophthalmol. 2009;54(6):671-685.20. Hailey D, Roine R, Ohinmaa A. Systematic review of evidence for the
benefits of telemedicine. J Telemed Telecare. 2002;8(suppl 1):1-30.21. Mishra SK, Kapoor L, Singh IP. Telemedicine in India: current sce-
nario and the future. Telemed J E Health. 2009;15(6):568-575.22. Sankaranarayanan R, Ramadas K, Thara S, et al. Long term effect of
visual screening on oral cancer incidence and mortality in a randomizedtrial in Kerala, India. Oral Oncol. 2013;49(4):314-321.23. Baeten J, Suresh A, Johnson A, et al. Molecular imaging of oral
premalignant and malignant lesions using fluorescently labeled lectins.Transl Oncol. 2014;7(2):213-220.24. Menon U, Belue R, Wahab S, et al. A randomized trial comparing the
effect of two phone-based interventions on colorectal cancer screeningadherence. Ann Behav Med. 2011;42(3):294-303.25. Holmstrup P, Vedtofte P, Reibel J, Stoltze K. Long-term treatment
outcome of oral premalignant lesions. Oral Oncol. 2006;42(5):461-474.26. Sperandio M, Brown AL, Lock C, et al. Predictive value of dysplasia
grading and DNA ploidy in malignant transformation of oral potentiallymalignant disorders. Cancer Prev Res (Phila). 2013;6(8):822-831.27. Warnakulasuriya S, Kovacevic T, Madden P, et al. Factors predicting
malignant transformation in oral potentially malignant disorders amongpatients accrued over a 10-year period in South East England. J Oral PatholMed. 2011;40(9):677-683.
ORIGINAL CONTRIBUTIONS
FLA 5.2.0 DTD ! ADAJ173_proof ! 4 July 2015 ! 4:40 pm ! ce
JADA -(-) http://jada.ada.org - 2015 9