Embed Size (px)
Citation preview

32 Inflammation & Allergy - Drug Targets, 2010, 9, 32-44
1871-5281/10 $55.00+.00 © 2010 Bentham Science Publishers Ltd.
Blood Coagulation as an Intrinsic Pathway for Proinflammation: A Mini Review
Arthur J. Chu*
Biological & Physical Sciences, Delta State University, Cleveland, MS 38733, USA
Abstract: Blood coagulation could be recognized as intrinsic inflammation. The coagulant mediators (FVIIa, FXa,
thrombin (FIIa), FXIIa) and fibrin(ogen) activate cellular signaling, eliciting the production of cytokines, chemokines,
growth factors, and other proinflammatory mediators. Hypercoagulability with elevated coagulant mediators would
certainly trigger hyper-inflammatory state not to mention about the direct hypercoagulable actions on thrombosis, and
platelet and complement activations, all of which contribute to inflammatory events. Furthermore, anticoagulant’s anti-
inflammatory effects readily reinforce the proposal that blood coagulation results in inflammation. The observations on
protease activated receptor (PAR) activation and PAR antagonists modulating inflammation are also in line with the
concept of coagulation-dependent inflammation.
Keywords: Blood coagulation, hypercoagulability, tissue factor, coagulant mediator, anticoagulant, inflammation, cytokines, protease-activated receptors, complement, thrombosis, cardioprotection.
1. INTRODUCTION
Inflammation plays a “diverging-converging” role in widely involving a broad spectrum of disease statuses and complications regardless of their pathogeneses. For instance, depression has even been recognized an inflammatory state [1]. Heterogeneous chronic obstructive pulmonary disease readily manifests as respiratory inflammation [2] somewhat similar to asthma outcome.
Inflammation could be generally associated with elevated proinflammatory network involving cytokines (e.g., TNF , IL-1 , IL-6, etc.), chemokines (CXCs, CCLs, etc.), adhesion molecules (MCP-1, ICAM, VCAM, selectins, etc.), growth factors (e.g., VEGF, PDGF, GM-CSF, etc.), and other inflammatory mediators (e.g., CRP, PGE2, LTs, PAF, histamine, matrix metalloproteinases (MMP), bradykinin (BK), calpain, complements, ET-1, ATII, etc.). The pleiotropic effects of these inflammatory mediators include activating T/B cell maturation/differentiation, non-immune cells, cellular signaling, and gene expressions. Inflammation damages surrounding tissues, contributes to angiogenesis/tumorigenesis, and manifests as many symptoms. Accordingly, combating inflammation becomes strategic approaches for relieving many disease complications. Anticytokine approaches, including reception suppression by soluble cytokine receptors and/or receptor analogous, offer broad clinical benefits to human inflammatory diseases [3] such as asthma [4], autoimmune disorders [5] (e.g., rheumatoid arthritis (RA), Crohn's disease, and psoriasis), and many others. Anti-VEGF Ab shows antagonism against RA by blocking VEGF reception and cytokine (TNF- and IL-6) production [6]. Anti-P-selectin antibody attenuates inflammation [7].
*Address correspondence to this author at the Biological & Physical
Sciences, Delta State University, Cleveland, MS 38733, USA;
E-mail: [email protected]
The source of inflammation is heterogeneous. Clinical studies readily demonstrate the close relationship of infection with inflammation. In most cases, inflammation in response to infection is essentially part of innate and adaptive immune systems. There is a perception that inflammation is most likely mediated by Toll-like receptors (TLR) [for reviews, see ref. 8, 9] receiving signals from either exogenous pathogen or endogenous danger -associated molecular patterns as a consequence of diverse infection or tissue injury/damage, respectively. Through MyD88- dependent or independent cellular activation of transcription factors (e.g, AP-1, NF B, and IRF3), proinflammatory genes are upregulated thereby resulting in local and/or systemic inflammation. Accordingly, TLR7/9 antagonists for immune-mediated inflammatory diseases have been reported [10].
Non-infectious conditions such as oxidative stress, arachidonate/eicosanoid metabolism, and many others could also lead to inflammatory responses. This mini-review addresses that blood coagulation triggers inflammation. Hypercoagulability accompanied by elevated clotting factors (e.g., FVIIa, FXa, FIIa, and FXIIa) and fibrin clot over-production [11-13] is responsible for cellular activation, which results in the elevated productions of cytokines, adhesion molecules, and many other inflammatory mediators. The evidence revealing the antiinflammatory property of anticoagulation further supports such coagulation-dependent inflammation. In addition, direct hypercoagulable consequences (e.g., thrombosis and platelet and complement activations) readily contribute to inflammation. Thus, blood coagulation could be considered as endogenous/intrinsic local or systemic inflammation.
2. OVERVIEW OF BLOOD COAGULATION PATHWAYS
Blood coagulation is a primary biological phenomenon, as a self defense system stopping bleeding during injury, in

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 33
mammals and other animals. However, often excessive or uncontrolled clot production leads to thrombosis shutting off blood flow that supplies oxygen and nutrients to cells. The resulting cell death manifests as stroke or heart attack. Coagulation has also been recognized an independent risk factor for atherosclerosis; fibrin stimulates plaque growth. Hypercoagulability shares similar risk factors with thrombosis involving congenital/acquired genetic deficiencies, diverse pathological conditions, lifestyle transitions, medical procedures, and aging [for review, see ref. 12]. Hypercoagulable state could also result from the defect in fibrinolytic system involving plasminogen activator (PA)-plasmin activation [for review, see ref. 14], which is beyond the focus of this review.
There are two coagulation pathways essentially proceeding as extracellular signaling cascades. The inducible extrinsic pathway plays an integral role [15], while the intrinsic pathway is constitutive facilitating blood coagulation merging with the extrinsic pathway at the point of tenase. The extrinsic but not intrinsic pathway is responsible for the initiation of thrombin generation and fibrin production [16].
2.1. Extrinsic Pathway
Integral membrane glycoprotein: tissue factor (TF; CD142) initiates the extrinsic pathways, which is susceptible to in vivo upregulation by inflammation [for review, see ref. 17], vascular injury (i.e., protein disulfide isomerase) [16, 18, 19], or advanced glycated end products under hyperglycemia. TF expression is mediated by the activations of signaling kinases (e.g., PTK, PKC, MAPK) and transcription factors (e.g., AP-1, Egr-1, NF B) while negatively correlating to intracelluar cAMP level [for review, see ref. 17]. Nitric oxide (NO) synthases and cyclo-oxgyenase (COX)1/2, however, seem to have nothing to do with TF expression [17]. In some clinical or pathological conditions, TF shed from vascular cells known as circulating plasma TF associated with microparticles also results in hypercoagulability and increased thrombotic risk [20, 21]. The microparticles involving selectin glycoprotein ligand 1 (PSGL-1) are captured by P-selectin to the sites of activated endothelium.
A series of zymogen activations take place on phospholipid-rich cell surfaces in a vitamin K and Ca+2 -dependent fashion [12, 16]. Upon FVII binding, TF-dependent FVII activation leads to FVIIa formation; this active serine protease triggers sequential proteolyses of FX and prothrombin to generate active serine proteases: FXa and thrombin (FIIa), respectively. FIIa is responsible for cleaving fibrinogen (FBG); the resulting fibrin is further polymerized and consequently cross-linked by FXIIIa, thereby producing insoluble blood clots (Fig. 1A). There are accessory loops for promoting the propagation of clotting. The initial FIIa formation activates FV and FVIII to form FVa and FVIIIa respectively, which activates tenase for fueling blood coagulation in the absence of TF [for review, see ref. 16].
2.2. Intrinsic Pathway
In the complementary intrinsic pathway (contact system) [for review, see refs. 22-24], the coagulation cascade involves high molecular weight kininogen (HK)-dependent
prekallikrein (PKK)/kallikrein (KK) regenerating cycle for FVIIa-dependent FXII activation (Fig. 1B). The resulting FXIIa subsequently activates FXI following with the activation of FIX so that the intrinsic tenase shunts into the major extrinsic pathway in contribution to FXa generation [16]. The role of FXII (Hageman factor) in thrombogenesis, however, remains largely unclear.
Its upregulation is associated with many infectious and inflammatory conditions including severe falciparum malaria [25], meningococcal septic shock [26], sepsis [27], Rhinovirus infection [28], Staphylococcus aureus infection [29], LPS [30, 31], and complement activation [32]. Others such as pregnancy [33], estrogen [34], and artifact thawing/freezing [35] also activate contact coagulation.
3. BLOOD COAGULATION- INTRINSIC INFLAMMATION
The contribution of blood coagulation to inflammation could result from coagulant mediators, thrombosis, complement activation, and platelet activation. The close clinical links of coagulation with inflammation have been reported in sepsis [36], DIC [37], inflammatory bowel diseases [38], lung diseases [39] including acute lung injury, acute respiratory distress syndrome and pneumonia [40]. Clinical studies implying the relationship of coagulation with inflammation showed that natural anticoagulant (e.g., activated protein C (APC), antithrombin (ATIII)) deficiencies are often associated with sepsis [41], DIC consequences [42], and inflammation [43]. C-1 inhibitor deficiency is also susceptible to inflammation and septic shock [44], and the deficiency is often associated with increased vascular permeability [45], a biomarker for inflammation.
Furthermore, anti-TF Ab shows anti-septic action [46], which lays the foundation for coagulation-dependent inflammation. TF and FVIIa receptor/ligand interactions induce proinflammatory effects in macrophages [47]. Convincingly, the role of TF in proinflammation comes from the demonstration that recombinant soluble TF (sTF1-219) readily induces inflammation in vivo arthritis model with elevated plasma IL-6 and paw swelling, which is accompanied by fibrin production and platelet activation [48]. In addition, FVII deficiency protects against acute inflammation [49], while elevated plasma level of FVIIa shows significant correlations to CRP and IL-6 [50]. Administration with recombinant FVIIa enhances IL-6 and -8 productions in healthy human subjects [51].
3.1. Proinflammatory Mediator Production by Coagulant Mediators
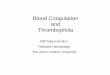
Fig. (1) depicts that both the extrinsic (A) and intrinsic (B) coagulation elicit inflammatory events. Unlike TLRs engaging in the majority of infection-triggered inflammation [for review, see ref. 8, 9], protease activated receptors (PAR) are in the interface between the extrinsic coagulant signals and intracellular activations. Active serine proteases such as coagulant mediators (FVIIa, FXa, and FIIa) readily cleave and activate PARs, G-protein coupled receptors. As the result of PAR activation, intracellular signaling components and transcription factors are upregulated, all of which are responsible for enhanced cytokine production. PARs

34 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
transmit the coagulant signals for the production of proinflammatory mediators, while TLR-4 transduces fibrin(ogen) signals (Fig. 1A). PAR-1 conveys FIIa and FXa signals, PAR-2 delivers FVIIa and FXa signals, PAR-3
mediates FIIa and FXa signals, and PAR-4 transduces FIIa signal.
(A)
(B)
Fig. (1). Coagulation-dependent inflammation. (A) TF-initiated extrinsic coagulation (left panel) proceeds as extracellular signaling and
results in the generation of active serine protease (coagulant mediators: FVIIa, FXa, FIIa) derived from their corresponding zymogens. FBG
is cleaved by FIIa to produce fibrin that is polymerized and crosslinked to yield insoluble blood clots. Through cell receptors (PARs and
TLR) on plasma membrane, the signals from the coagulant mediators as well as fibrin mediate diverse intracellular activation and the
production of proinflammatory mediators (right panel) including cytokines, adhesion molecules, growth factors, etc. (B) The contact system
(intrinsic coagulation) consists of a HK/PKK/KK regenerating cycle for FVIIa-dependent FXII activation. gC1qR/p33 protein receptor is
involved in KK production and subsequent BK release from PKK and HK, respectively. KK triggers complement component activation,
while BK activates cytokine production and intracellular signaling for proinflammation.

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 35
A receptor protein, gC1qR/p33 [52], initiates PKK activation to KK for complement activation, and B-1/B-2 receptors [53] are responsible for the transduction of bradykinin (BK) proinflammation (Fig. 1B).
3.1.1. PAR Activation Leading to Inflammation
PAR activating peptides elicit a broad spectrum of inflammation, which is consistent with the notion of coagulation-dependent inflammation.
3.1.1.1. PAR-1 Activation
An activating peptide (TRAP) enhances IL-6 [54], PGE2 [55], PGDF or P-selectin expression [56]. Another activating peptide (SFLLRN) induces the production of IL- 6 [57], -8 [58], iNOS [59], PGE2 [57], MCP-1 [58], NO [60], or P-selectin [61]. SFLLKNPNDKYEPF elicits the expression of ICAM [62] and VEGF [63]. A recent study has reported that activated protein C (APC) activates PAR-1 to induce MCP-1 expression in EC [64].
3.1.1.2. PAR-2 Activation
Tryptase or trypsin elicits the production of TNF- [65], IL-1 [65], IL-6 [65-67] or IL-8 [67, 68] and increases
[Ca+2]i [68]. Its signaling also activates Erk [67], AP-1 [67], c-Jun [67], p38 MAPK [67], or NF B [68]. Apart from enhanced PI hydrolysis [69], a PAR-2 activating peptide (SLIGKV) not only elicits [57] IL-6, -8 and PGE2, but also activates p38 MAPK [70] and MEK/Erk [71] to upregulate TNF- secretion [72], PGE2 production [55], and Erk activation [73]. Enhanced NO production [60] or P-selectin expression [74] by SLIGRL (activating peptide) accounts for muscle relaxation or leukocyte rolling, respectively. Agonist proteinase-3 (PR3) enhances IL-8, MCP-1 and ICAM-1 expression [75]. An in vivo comparison of null mutant (PAR-2 -/-) with wide-type (PAR-2 +/+) mice consistently indicates that PAR-2 is responsible for the induction of IL-6, ICAM-1 and E-selectin expression [76]. Diverse PAR-2 actions also go beyond this review’s inflammation focus, involving pigmentation, vasodilation, pain/itch, IBS transmission, etc.
3.1.1.3. PAR-3 Activation
A peptide (TFRGAP) [77] induces Erk1/2 activation and [Ca+2]i, while SFNGGP [55] slightly elicits PGE2 release.
3.1.1.4. PAR-4 Activation
A peptide (GYPGQV) [57, 78] elicits TNF- , IL-6, -8 or PGE2 production. GYPGKF enhances PGE2 production [55], [Ca+2]i, and platelet aggregation [79]. AYPGKF [80] activates p38 MAPK, PLC, and SrC.
3.1.2. FVIIa
In TF-expressing cells, FVIIa elicits VEGF [81] and activates PAR-2 to enhance SMC migration [82], MAPK phosphorylation, and [Ca+2]i mobilization [83]. Enhanced IL-8 expression in response to FVIIa is mediated by PAR-2, facilitating cell migration [84]. In addition, PAR-2-mediated FVIIa signaling stimulates ET-1 synthesis [85].
3.1.3. FXa
FXa signaling elicits IL-6 [86, 87], IL-8 [86] or MCP-1 [55, 86] expression, which is PAR-1/3-dependent. PAR-2-dependent FXa signaling induces the expression of IL-6
[87]/-8 [86], PDGF or MCP-1 [86] as well as Erk1/2 activation [73].
3.1.4. FIIa
FIIa upregulates the production of IL-6 [52, 86, 88-90], IL-8 [86], TGF- [91], MCP-1 [86, 87, 89], PDGF [90], bFGF [90], ICAM-1 [62], P-selectin [91], or VEGF [63, 92]. PAR-1-dependent FIIa signaling enhances proinflammatory actions including NF B activation [62], intracellular Ca+2 ([Ca+2]i) mobilization, Erk1/2 phosphorylation [92], iNOS [57], COX-2 [94], MMP-9 [95], and PI hydrolysis [69]. FIIa-induced PAR-1 signaling of IL-6, IL-8, MCP-1, PGE2 production and NF B activation is apparently sphingosine kinase 1-dependent [96].
3.1.5. Fibrin
TLR 4 is proposed to mediate FBG pro-inflammation [97] including IL-6 and MCP-1 production [88]. Fibrin and its fragments elicit IL-1 [98], IL-6 [99], IL-8 [100] and ICAM [100] expression through undefined mechanism(s).
3.1.6. FXIIa
Proinflammatory effects of FXII activation are largely mediated by KK and BK generation [101]. In the PKK/KK/ HK regenerating loop, FXII undergoes autoactivation to FXIIa that further activates PKK to KK [102] (Fig. 1B), subsequently releasing BK. gC1qR/p33, a membrane-bound receptor protein binding to HK, initiates PKK activation to KK in the presence of Zn+2 and FXII [52, 103], thereby serving as a molecular bridge between contact activation and complement systems.
3.1.6.1. KK-Dependent Complement Activation
Proinflammatory KK directly activates not only complement components C3 and C5 [104], but also C1 esterase (Fig. 1B) leading to inflammation via the classical complement activation [104, 105]. As the result of complement activation, it leads to NF B activation, the transcription and expression of adhesion molecules (VCAM-1, ICAM-1 and E- and P-selectins), production of IL-8 and MCP-1, platelet activation, and platelet-leukocyte aggre-gation, all of which represent inflammation [for review, see ref. 106]. KK also cleaves HK to liberate BK [105], another proinflammatory mediator (see below section 3.1.6.2.). It, however, remains largely unknown whether PARs mediate KK proinflammatory action.
3.1.6.2. BK Release
Proinflammatory mediator BK (Arg-Pro-Pro-Gly-Phe-Ser-Pro-Phe-Arg) is known as a major contributor to the innate inflammatory response. Derived from HK through the direct catalysis by KK (Fig. 1B), BK is responsible for vasodilatation, increased vascular permeability, and inflammatory pain [104, 107-109].
The involvement of BK in inflammatory process has been demonstrated in disease status [for review, see ref. 109]. BK proinflammation is largely mediated by its inducible B1 receptor or constitutive B2 receptor [53]. More specifically, B2-receptor is responsible for swelling and pain, while B1 receptor is specific in hyperalgesia. These G protein coupled receptors initiate complex intracellular signaling cascade involving adenylate cyclase, PLC, Ca+2

36 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
signal, MAPKs, etc., leading to NO and prostaglandin production. BK through B1 receptor promotes ICAM/VCAM expression [110]; B1 receptor activation also induces TNF- and IL-1 release [111]. Through B2 receptor, BK induces COX-2 expression in aortic vascular smooth muscle cells [112] involving the activation of MAPK p42/p44, PKC, and NOS. COX-2 products (e.g., TXA2,
PGE2) have inflammatory properties. BK via B2 receptor
induces MMP-2 production [113].
Concerning intracellular activation, BK generally upregulates MAPK [114-116], NOS [117], and JAK/STAT signaling [118]. BK induces IL-6 [119] and IL-8 [120] expression, which is mediated by ERK1/2 and p38 MAPK activation in AP-1-dependent fashion [119].
3.2. Complement Activation and Inflammation
KK in the intrinsic pathway activates complement components (Fig. 1B; also see section 3.1.6.1). In addition, FIIa could directly activate C5 and C3 [121]. Platelet activation resulting from coagulation also engages in complement activation (see section 3.3.).
Complement activation readily engages in virtually all phases of an acute inflammatory reaction including the increase in vascular permeability, extravasation of leukocytes, and chemotaxis. Complement activation presents inflammation [106], eliciting an array of proinflammatory mediators including upregulated mRNA levels of CRP, TF, COX-2, TNF, E-selectin, ICAM, VCAM, I B , IL-1 , IL-1 , IL-8, and PAI-1. C1q is able to induce the production
of
IL-8, while C5a elicits IL-3 and MCP-1 production. C5b-9 induces IL-6/IL-8 production and the expression of AP-1 and NF B.
3.3. Platelet Activation and Inflammation
As a direct consequence of blood coagulation, platelet activation is primarily mediated by FIIa [122]. Platelet activation [122, 123] per se releases a broad spectrum of cytokines, adhesion molecules, growth factors, chemokines, and other inflammatory mediators. For cell neighboring effects, activated platelets result in activations of vascular cells such as endothelial cells, smooth muscle cells, lymphocytes, etc., which leads to local/systemic inflam-mation.
Apart from FIIa reception, other platelet receptors such as GPIb/IX/V, P-selectin, PSGL-1, CD40, gC1qR, and
IIb 3 integrin participate in the progression of inflammatory conditions [124]. Interestingly, platelet activates C5 [125], while C3 activation is mediated by C1q-dependent classical pathway [125]; all represent inflammatory events [106, 121]. In addition, platelet activation results in aggregation and fibrin recruitment for thrombosis [16] that also contributes to inflammation (see below section 3.4.).
3.4. Thrombosis and Inflammation
The close association of thrombosis with inflammation has previously been reviewed by Esmon [126], which is in line with hypercoaguability presenting the high tendency of thrombogenesis [13] and thrombotic contributions to inflammation [for review, see ref. 127]. In these regards, platelet activation and aggregation play roles in inflammation as described in the above section 3.2. & 3.3. The notion of profibrinolysis via plasminogen activation showing antiinflammation could be in further agreement with thrombosis-dependent inflammation [128].
4. ANTAGONISM AGAINST INFLAMMATION DERIVED FROM BLOOD COAGULATION
Blood coagulation could become a target for anti-inflammation (Table 1). Convincing evidence demonstrates natural anticoagulants and their analogs resulting in antiinflammation. Mounting observations also reveal anti-inflammatory benefits resulting from anticoagulation (Fig. 2). The direct PAR blockade of the transmissions of blood coagulant mediators [for review, see ref. 17] and BK receptor antagonists show antiinflammation. Collectively, all of which further support such a coagulation-dependent inflammation phenomena.
4.1. Inhibition of Cytokine Production by Anticoagu-lation Approaches
4.1.1. Natural Anticoagulants
4.1.1.1. APC
Natural anticoagulant APC inactivates FVa and FVIIIa. In addition, APC exerts a profibrinolytic effect by inactivation of PAI-1 and inhibition of thrombin activated fibrinolytic inhibitor (TAFI) activation, which makes APC strong anti-thrombotic. As the result of the respective inhibitions on intrinsic tenase and prothrombinase for downregulating FXa and FIIa generation, APC thereby
Table 1. Possible Antagonisms Against Blood Coagulation-Dependent Inflammation
Strategy Selected Target
Anticoagulation Extrinsic coagulation TF expression; TF/FVII activation; FVIIa; FXa; FIIa
Intrinsic coagulation FV; FVIII; FXIIa; KK
PAR blockade PAR-1/2/3/4
Contact system interface with complement gC1qR/p33
Complement inactivation C1; C3; C5; C3/C5 convertase
Prevention of complement activation DAF/MCP/CD59/crry
BK antagonism B1 receptor; B2 receptor

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 37
inactivates the production of IL-1, -6, -8 or TNF- [129]. APC is recognized one of the effective anti-inflammatory agents in clinical application. APC consistently reduces septic mortality and blocks DIC upon E. coli infection in either animal or human models [130-133]. In animal models, recombinant human soluble thrombomodulin (TM) prevents LPS-induced pulmonary vascular injury, inhibiting leukocyte activation [134, 135] and accumulation [136, 137]. In view of TM being a cofactor of FIIa, its facilitation of PC activation could further support anti-inflammatory significance in relation to APC anticoagulation.
4.1.1.2. Tissue Factor Pathway Inhibitor (TFPI)
With respect to its ability to directly inhibit FXa followed by a feedback inhibition on TF/FVIIa complex, natural anticoagulant TFPI suppresses coagulation-dependent IL-8 production [138] or VCAM-1 expression [139]. In VSMC, TFPI reduces the autocrine release of PDGF-BB, MCP-1 and MMP-2 in response to FVIIa and FXa [140]. Its coagulation-independent action includes the direct suppression in TNF- , IL-6, and IL-8 production [141], reducing mortality from E. coli septic shock in baboons. TFPI also directly interferes with LPS reception [142]. The failure in human studies [143-145], however, warrants further research to clarify any clinical anti-inflammatory potential.
4.1.1.3. Antithrombin III (ATIII)
ATIII mediates pentasaccharide and heparin actions to inhibit FXa and FIIa, respectively. ATIII blocks FXa-induced IL-6, IL-8, MCP-1, ICAM/VCAM, and E-selectin expressions [146] in addition to arresting FIIa-induced (PAR-1-dependent) VEGF release [92] and MCP-1 expression [147]. Apart from inactivating NF B [148], AT III direct antiinflammatory action includes the suppression in INF- and ILs (e.g., 1, 2, 4, 6 & 8) production, which is
mediated by enhanced PGI production and diminished inducible nitric oxide synthase (iNOS) [149]. However, the discrepancy exists concerning the survival rate beings improved in baboons [150] but not in severe human sepsis treated with the high dose of ATIII [151]. Further research warrants verifying its anti-inflammatory potential.
4.1.2. Warfarin
Also known as Coumadin or Acenocumarol, 4-hydroxy-3-(3-oxo-1-phenylbutyl)-2H-1-benzopyran-2-one is an inhibitor of the synthesis for vitamin K-dependent clotting factors [12]. It suppresses the reductases for vitamin K regeneration that is a cofactor for the posttranslational carboxylation of glutamates to form gamma-carboxyglutamates (Gla). The Gla domain is essential for phospholipid membrane anchoring and Ca
+2 binding, which
is present in the N-terminal of coagulation zymogens such as FII, FVII, FIX, FX, PC and PS [152]. Namely, warfarin generally depresses the functions of the clotting factors, thereby blocking global coagulation. Its antiiflammatory effect has been demonstrated in 1979 [153]. Oral warfarin significantly reduces IL-6 at day 15 [154]; further investigation warrants exploring broad anti-inflammatory benefits, if any.
4.1.3. FVIIa Inhibition
Recombinant nematode anticoagulant protein c2 diminishes coagulation-dependent IL-6 and IL-8 productions [51]. Active site-inhibited FVIIa depresses LPS-inducible plasma levels of TNF- [144], IL-6 [155-157], and IL-8 [156, 157]. FVIIai abolishes VIIa signaling of Erk1/2 phosphorylation [83] in TF-expressing cells, while it suppresses sTF-induced inflammation in vivo model [48]. A small molecule BCX-3607 (TF/FVIIa inhibitor) also decreases IL-6 level in an endotoxemia mouse model [158].
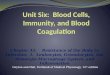
Fig. (2). Anticoagulation blocks coagulation-inflammation cycle. Coagulation-dependent inflammation derived from the extrinsic pathway in
turn upregulates TF expression. Coagulation and inflammation are causes and consequences mutually, essentially refueling each other.
Similar coagulation-inflammation cycle also occurs in the intrinsic pathway (not shown). Natural anticoagulants (APC, TFPI, ATIII),
inactivated FVIIa, FVIIa inhibitors, FXa inhibitiors, FIIa inhibitors, heparins, etc. block the extrinsic coagulation by suppressing/inhibiting
serine protease activities as indicated . Alternatively, PAR antagonists also block such cycle by directly arresting the signal transduction from coagulant mediators.

38 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
4.1.4. FXa Inhibition
LMWH, enoxaparin, or DX9065a suppresses P-selectin, TNF- , IL-6 [159], or MCP-1 [160] expression, resulting in depressed platelet activation [161] and leukocyte adhesion to EC [162]. A direct inhibitor (ZK-807834) blocks FXa signaling of eliciting IL-6 [87]. The anti-inflammatory effects of a newer anticoagulant rivaroxaban, however, remain largely unknown.
4.1.5. FIIa Inhibition
Heparin shows a variety of inflammatory potentials [for review, see ref. 163]. Heparin-bonded circuit prevents the increases in IL-6 and IL-8 in CPB patients without any effect on P-selectin [164], while heparin bolus reduces neutrophil activation without affecting platelet aggregation [165]. Heparin and delteparin downregulate PAR-1 cleavage [166], blocking PAR-1-mediated VEGF release in response to FIIa [92].
Direct FIIa inhibitor (hirudin) binds to FIIa active site and prevents PAR-1 from cleavage [166], thereby diminishing FIIa signaling in ICAM/VCAM expression [167] and elicitation of VEGF [63, 92], IL–6 [168], IL-8 [58], or MCP-1 [58]. Hirudin suppresses sTF1-219-induced inflammation [46]. A hirudin analog (lepirudin) alleviates LPS-induced platelet activation [169], and an active site inhibitor (melagatran) diminishes P-selectin expression [166]. Whether dabigatran could show any inflammatory effect warrants further study.
4.2. Antiinflammation by Blockade of Contact System
Consistent with the fact of FXIIa and KK being proinflammatory (section 3.1.6.), PA (urokinase) readily downregulates contact system with the consequence of lowering BK production and complement inactivation, accounting for its prevention of inflammation [128].
4.2.1. FXIIa Inhibition
C-1 inhibitor, a protease inhibitor of the serpin family, downregulates contact coagulation by inactivating FXIIa, showing antiinflammation [102, 170]. ATIII-bound heparin and heparin sulfate inhibit FXII activation [171]. Ecotin is a potent inhibitor for FXIIa [172].
4.2.2. KK Inhibition
Antiinflammatory contribution of KK inhibition is essentially mediated by blocking complement activation. C-1 inhibitor inactivates KK [102, 170] together with its ability to directly suppress complement C-1 [173], showing diverse anti-inflammatory effects.
A recombinant small protein Eecallantide (DX88) [174], based on the first Kunitz domain of human TFPI, is a potent and specific inhibitor of plasma KK; DX88 reverses the increased vascular permeability in C-1 inhibitor deficient mice. Ecotin [172] and Aprotinin [175] also directly inhibit KK and suppress BK release. However, anti-inflammatory effects by such inhibitors have not been reported thus far.
4.2.3. BK Inhibition
BK antagonists have already shown antiinflammatory action by improving survival of septic animals several decades ago. A wide variety of BK and B-1/B-2 receptor
antagonists are currently available for clinical applications for antiinflammation [for review, see ref. 176]. It, however, remains to be determined if these antagonisms specifically block coagulation-dependent inflammation.
5. REMARKS
Coagulation-dependent inflammation is revealed by which coagulant mediators are proinflammatory (Fig. 1) and anticoagulation is of anti-inflammation (Fig. 2). Furthermore, coagulation-mediated platelet and complement activations readily present an array of inflammation (Fig. 3). Hypercoagulation per se elicits elevated generation of FVIIa, FXa, FIIa, FXIIa, KK, and BK as well as fibrin over-production, all of which in turn initiate cellular activation and signaling for inflammation (Fig. 1). Both extrinsic and intrinsic pathways in fact play diverging as well as converging roles in proinflammation. Such vicious cycle linking blood coagulation to inflammation mutually refuels each other, ensuring hypercoagulability as well as hyper-inflammatory (Fig. 2). In these regards, blood coagulation could become a target for antiinflammation.
With respect to its thrombogenic as well as proinflammatory natures, it is not surprising that hypercoagulability triggers diverse cardiovascular complications. Namely, hypercoagulation extends one arm for thrombotic consequence and the other for inflammatory events. A paradigm: circuit (Fig. 3) integrates the coagulation-inflammation cycle to thrombosis [for review, see ref. 127] that is closely related to inflammation [for review, see ref. 126]. Accordingly, any interruption of the circuit could be of cardioprotection. Table 1 summarizes possible approaches to antiinflammation in relation to its blood coagulation-dependence. Apart from anticoagulants described in the above section 4, antagonism against complement components, PARs, cytokine reception, or gC1qR/p3 could be expecting to achieve anticoagulation, antiinflammation, antithrombosis, and cardioprotection. Even nutrient such as antioxidant curcumin suppressing TF expression could attenuate such coagulation-dependent inflammation.
Anticoagulation not only blocks thrombogenesis, but also arrests the coagulation-inflammation cycle (Figs. 2, 3). The biopharmaceutical applications of anticoagulant development could be several-fold. (1) Anticoagulation certainly confers intervention remedy by offsetting the induced extrinsic hypercoagulability resulting from inflammation, vascular injury, or circulating TF microparticles. (2) Anticoagulation could provide broad spectrum of anti-inflammatory relevance regarding the operational coagulation-inflammation vicious cycle. (3) In view of hypercoagulability driving the circuit linking thrombosis and inflammation (Fig. 3), anticoagulants block the coagulation-inflammation cycle to interrupt the coagulation-inflammation-thrombosis circuit, showing cardioprotection. The ability of PAR1 and 2 to induce TF [177] reveals not only coagulation-dependent inflammation but also diverging and converging roles of TF in refueling the cycle [17]. It remains challenging that selective upstream antagonism (i.e., inhibition on TF-dependent FVII activation) arrests only the extrinsic hypercoagulability to prevent thrombotic complication instead of blocking the

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 39
constitutive intrinsic coagulation for hemostasis, which would effectively suppress inflammation while avoiding bleeding episode.
ABBREVIATIONS
AP-1 = Activator protein-1
APC = Activated protein C
AT II = Angiotensin-II
AT III = Antithrombin III
BK = Bradykinin
COX-2 = Cycloxygenase-2
CRP = C-reactive protein
Egr-1 = Early growth reponse-1
ET-1 = Endothelin-1
FBG = Fibrinogen
FIIa = Thrombin
FVIIa = Activated factor VII
FVIIai = Active-site inhibited FVIIa
FXa = Activated factor X
HK = High molecular weight kininogen
ICAM = Intracellular adhesion molecule
IL = Interleukin
IRF3 = Interferon response factor 3
JAK = Janus-activated kinase
KK = Kallikrein
LDL = Low density lipoprotein
LMWH = Low-molecular-weight-heparin
Lp(a) = Lipoprotein (a)
LPS = Lipopolysaccharide; bacterial endotoxin
MAPK = Mitogenic activating protein kinase
MCP = Monocyte chemotractic protein
MMP = Matrix metalloproteinase
NF- B = Nuclear factor –kappa B
NOS = Nitric oxide synthase
OxLDL = Oxidizaed LDL
PA = Plasminogen activator
PAF = Platelet activating factor
PAI-1 = Plasminogen activator inhibitor-1
PAR = Protease activated receptor
PC = Protein C
PDGF = Platelet derived growth factor
PF 1+2 = Prothrombin fragments 1+2
PGE2 = Prostagrandin E2
Fig. (3). The paradigm: coagulation-inflammation-thrombosis circuit, implication on cardiovascular events. Hypercoagulability with elevated
coagulant mediators, fibrin overproduction, complement activation, and platelet activation results in inflammation (elevated production of
cytokines, adhesion molecules, growth factors, and other mediators) as well as thrombosis (thrombus, platelet aggregation, fibrin deposit). A
circuit links the coagulation-inflammation cycle and inflammation-thrombosis association. Inflammation and thrombosis are two risk factors
for cardiovascular events. Accordingly, any interruption of the cycle and/or any part of the circuit could exhibit cardioprotection benefits.

40 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
PKC = Protein kinase C
PKK = Prekallikrein
PN-2/A PP = Protease nexin-2 amyloid beta protein precursor
PTK = Protein tyrosine kinase
RA = Rheumatoid arthritis
ROS = Reactive oxygen species
SMC = Smooth muscle cell
TAP = Tick anticoagulant peptide
TAT = Thrombin-antithrombin complex
TF = Tissue factor
TFPI = TF pathway inhibitor
TGF = Transforming growth factor
TLR = Toll-like receptors
TM = Thrombomodulin
TNF- = Tissue necrosis factor-alpha
TT = Thrombin time
REFERENCES
[1] Adler, U.C.; Marques, A.H.; Calil, H.M. Inflammatory aspects of depression. Inflamm. Allergy Drug Targets, 2008, 7, 19-23.
[2] Sethi, S.; Murphy, T.F. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N. Engl. J. Med., 2008,
359, 2355-65. [3] Dinarello, C.A. Inflammation in human disease: anticytokine
therapy. Biol. Blood Marrow Transplant, 2008, 15, 134-6. [4] Brightling, C.; Berry, M.; Amrani, Y. Targeting TNF-alpha: a
novel therapeutic approach for asthma. J. Allergy Clin. Immunol., 2008, 121, 5-10.
[5] Tincani, A.; Andreoli, L.; Bazzani, C.; Bosiso, D.; Sozzani, S. Inflammatory molecules: a target for treatment of systemic
autoimmune diseases. Autoimmun. Rev., 2007, 7, 1-7. [6] Yoo, S-A.; Bae, D-G.; Ryoo, J-W.; Kim, H.R.; Park, G.S.; Cho,
C.S.; Chae, C.B.; Kim, W.U. Arginine-rich anti-vascular endothelial growth factor (anti-VEGF) hexapeptide inhibits
collagen-induced arthritis and VEGF-stimulated productions of TNF- and IL-6 by human monocytes. J. Immunol., 2008, 174,
5846–55. [7] Downing, L.J.; Wakefield, T.W.; Strieter, R.M.; Prince, M.R.;
Londy, F.J.; Fowlkes, J.B.; Hulin, M.S.; Kadell, A.M.; Wilke, C.A.; Brown, S.L.; Wrobleski, S.K.; Burdick, M.D.; Anderson,
D.C.; Greenfield, L.J. Anti-P-selectin antibody decreases inflammation and thrombus formation in venous thrombosis. J.
Vasc. Surg., 1997, 25, 816-27. [8] Beg, A.A. Endogenous ligands of Toll-like receptors: implications
for regulating inflammatory and immune responses. Trends Immunol., 2002, 23, 509-12.
[9] Atkinson, T.J. Toll-like receptors, transduction-effector pathways, and disease diversity: evidence of an immunobiological paradigm
explaining all human illness? Int. Rev. Immunol., 2008, 27, 255-81. [10] Sun, S.; Rao, N.L.; Venable, J.; Thurmond, R.; Karlsson, L.
TLR7/9 antagonists as therapeutics for immune-mediated inflammatory disorders. Inflamm. Allergy Drug Targets, 2007, 6,
223-35. [11] Chandler, W.L.; Rodgers, G.M.; Sprouse, J.T.; Thompson, A.R.
Elevated hemostatic factor levels as potential risk factors for thrombosis. Arch. Pathol. Lab. Med., 2002, 126, 1405-14.
[12] Chu, A.J. Biochemical strategies to anticoagulation: a comparative overview. Curr. Vasc. Pharmacol., 2004, 4, 199-228.
[13] Thomas, R.H. Hypercoagulability syndromes. Arch. Intern. Med., 2001, 161, 2433-9.
[14] Weisel, J.W.; Litvinov, R.I. The biochemical and physical process of fibrinolysis and effects of clot structure and stability on the lysis
rate. Cardiovasc. Hematol. Agents Med. Chem., 2008, 6, 161-80.
[15] Broze, G.J, Jr. Tissue factor pathway inhibitor and the revised
theory of coagulation. Annu. Rev. Med., 1995, 46, 103-12. [16] Furie, B.; Furie, B.C. Mechanisms of thrombus formation. N. Engl.
J. Med., 2008, 359, 938-48. [17] Chu, A.J. Tissue factor mediates inflammation. Arch. Biochem.
Biophys., 2005, 440, 122-31. [18] Cho, J.; Furie, B.C.; Coughlin, S.R.; Furie, B. A critical role for
extracellular protein disulfide isomerase during thrombus formation in mice. J. Clin. Invest., 2008, 118, 1123-31.
[19] Reinhardt, C.; von Bruhl, M.L.; Manukyan, D.; Grahl, L.; Lorenz, M.; Altmann, B.; Dlugai, S.; Hess, S.; Konrad, I.; Orschiedt, L.;
Mackman. N.; Ruddock, L.; Massberg, S.; Engelmann, B. Protein disulfide isomerase acts as an injury response signal that enhances
fibrin generation via tissue factor activation. J. Clin. Invest., 2008, 118, 1110-22.
[20] Giesen, P.L.; Rauch, U.; Bohrmann, B. Grahl, L.; Lorenz, M.; Altmann, B.; Dlugai, S.; Hess, S.; Konrad, I.; Orschiedt, L.;
Mackman, N.; Ruddock, L.; Massberg, S.; Engelmann, B. Blood-borne tissue factor: another view of thrombosis. Proc. Natl. Acad.
Sci. USA, 1999, 96, 2311-5. [21] Morel, O.; Toti, F.; Hugel, B.; Bakouboula, B.; Camoin-Jau, L.;
Dignat-George, F.; Freyssinet, J.M. Procoagulant microparticles: disrupting the vascular homeostatsis equation? Artherioscler.
Thromb. Vasc. Biol., 2006, 26, 2594-604. [22] Gailani, D.; Renne, T. Intrinsic pathway of coagulation and arterial
thrombosis. Artherioscler Thromb Vasc. Biol., 2007, 27, 2507-13. [23] Schmaier, A.H. Assembly, activation, and physiologic influence of
the plasma kallikrein/kinin system. Int. Immunopharmacol., 2008, 8, 161-5.
[24] Schousboe, I. Pharmacological regulation of factor XII activation may be a new target to control pathological coagulation. Biochem.
Pharmacol., 2008, 75, 1007-13. [25] Clemens, R.; Pramoolsinsap, C.; Lorenz, R.; Pukrittayakamee, S.;
Bock, H.L.; White, N.J. Activation of the coagulation cascade in severe falciparum malaria through the intrinsic pathway. Br. J.
Haematol., 1994, 87, 100-5. [26] Wuillemin, W.A.; Fijnvandraat, K.; Derkx, B.H.; Peters, M.;
Vreede, W.; ten Cate, H.; Hack, C.E. Activation of the intrinsic pathway of coagulation in children with meningococcal septic
shock. Thromb Haemost., 1995, 74, 1436-41. [27] Coppola, R.; Cristilli, P.; Cugno, M.; Ariëns, R.A.; Mari, D.;
Mannucci, P.M. Measurement of activated factor XII in health and disease. Blood Coagul. Fibrinolysis., 1996, 7, 530-5.
[28] Christiansen, S.C.; Eddleston, J.; Bengtson, S.H.; Jenkins, G.R.; Sarnoff, R.B.; Turner, R.B.; Gwaltney, J.M. Jr,; Zuraw, B.L.
Experimental Rhinovirus Infection Increases Human Tissue Kallikrein Activation in Allergic Subjects. Int. Arch Allergy
Immunol., 2008, 147, 299-304. [29] Mattsson, E.; Herwald, H.; Cramer, H.; Persson, K.; Sjobring, U.;
Bjorck, L. Staphylococcus aureus induces release of bradykinin in human plasma. Infect. Immun., 2001, 69, 3877-82.
[30] Roeise, O.; Bouma, B.N.; Stadaas, J.O.; Aasen, A.O. Dose dependence of endotoxin-induced activation of the plasma contact
system: an in vitro study. Circ. Shock, 1988, 26, 419-30. [31] Perkins, R.; Ngo, M.D.; Mahdi, F.; Shariat-Madar, Z. Identification
of lipopolysaccharide binding site on high molecular weight kininogen. Biochem. Biophys. Res. Commun., 2008, 366, 938-43.
[32] Jurd, K.M.; Stephens, C.J.; Black, M.M.; Hunt, B.J. Endothelial cell activation in cutaneous vasculitis. Clin. Exp. Dermatol., 1996,
21, 28-32. [33] Briseid, K.; Hoem, N.O.; Johannesen, S.; Fossum, S. Contact
activation factors in plasma from pregnant women--increased level of an association between factor XII and kallikrein. Thromb Res.,
1991, 61, 123-33. [34] Citarella, F.; Misiti, S.; Felici, A.; Farsetti, A.; Pontecorvi, A.;
Fantoni, A. Estrogen induction and contact phase activation of human factor XII. Steroids, 1996, 61, 270-6.
[35] Stief, T.W.; Otto, S.; Renz, H. Intrinsic hemostasis activation by freezing and thawing of plasma. Clin. Appl. Thromb Hemost.,
2009, 15, 59-64. [36] Thijs, L.G.; de Boer, J.P.; de Groot, M.C.; Hack, C.E. Coagulation
disorders in septic shock. Intensive Care Med., 1993, 19, S8-15. [37] Gando, S.; Kameue, T.; Nanzaki, S.; Nakanisi, Y. Disseminated
intravascular coagulation is a frequent complication of systemic inflammatory response syndrome. Thromb. Haemost., 1996, 75,
224-8.

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 41
[38] Yoshida, H.; Granger, D. N. Inflammatory bowel disease: A
paradigm for the link between coagulation and inflammation. Inflamm. Bowel Dis., 2009,15, 1245-55.
[39] van der Poll, T. Tissue factor as an initiator of coagulation and inflammation in the lung. Crit. Care, 2008, 12, S3.
[40] Nieuwenhuizen, L.; de Groot, P.G.; Grutters, J.C.; Biesma, D.H. A review of pulmonary coagulopathy in acute lung injury, acute
respiratory distress syndrome and pneumonia. Eur. J. Haematol., 2009, 82, 413-25.
[41] White, B.; Perry, D. Acquired antithrombin III deficiency in sepsis. Br. J. Haematol., 2001, 112, 26-31.
[42] Tollefsen, D.M. Antithrombin deficiency. In: Scriver CR, Beaudet AL, Sly WS, Valle D, eds. The metabolic and molecular bases of
inherited disease. 8th ed. 2001, New York, NY: McGraw-Hill, pp. 4455-71.
[43] Asakura, H.; Ontachi, Y.; Mizutani, T.; Kato, M.; Ito, T.; Saito, M. Morishita, E.; Yamazaki, M.; Aoshima, K.; Takami, A.; Yoshida,
T.; Suga, Y.; Miyamoto, K.; Nakao, S. Decreased plasma activity of antithrombin or protein C is not due to consumption
coagulopathy in septic patients with disseminated intravascular coagulation. Eur. J. Haematol., 2001, 67, 170-5.
[44] Liu, D.; Lu, F.; Qin, G.; Fernandes, S.M.; Li, J.; Davis, A.E. III. C1 Inhibitor-Mediated Protection from Sepsis. J. Immunol., 2007, 179,
3966-72. [45] Han Lee, E.D.; Pappalardo, E.; Scafidi, J.; Davis, A.E. III.
Approaches toward reversal of increased vascular permeability in C-1 inhibitor deficient mice. Immunol. Lett., 2003, 89, 155-60.
[46] Taylor, F.B. Jr.; Chang, A.; Ruf, W.; Morrissey, J.H.; Hinshaw, L.; Catlett, R.; Blick, K.; Edgington, T.S. Lethal E. coli septic shock is
prevented by blocking tissue factor with monoclonal antibody. Circ. Shock, 1991, 33, 127-34.
[47] Cunningham, M.A.; Romas, P.; Hutchinson, P.; Holdsworth, S.R.; Tipping, P.G. Tissue factor and factor VIIa receptor/ligand
interactions induce proinflammatory effects in macrophages. Blood, 1999, 94, 3413-20
[48] Busso, N.; Chobaz-Péclat, V.; Hamilton, J.; Spee, P.; Wagtmann, N.; So, A. Essential role of platelet activation via protease activated
receptor 4 in tissue factor-initiated inflammation. Arthritis Res. Ther., 2008, 10, R42 (online open access)
[49] Xu, H.; Ploplis, V.A.; Castellino, F.J. A coagulation factor VII deficiency protects against acute inflammatory responses in mice.
J. Pathol., 2006, 210, 488-96. [50] Porreca, E.; Di Febbo, C.; di Castelnuovo, A.; Baccante, G.;
Amore, C.; Angelini, A.; Di Nisio, M.; Donati, M.; Cuccurullo, F.; Iacoviello, L. Association of factor VII levels with inflammatory
parameters in hypercholesterolemic patients. Atherosclerosis, 2002, 165, 159-66.
[51] de Jonge, E.; Friederich, P.W.; Vlasuk, G.P.; Rote, W.E.; Vroom, M.B.; Levi, M.; van der Poll, T. Activation of coagulation by
administration of recombinant factor VIIa elicits interleukin 6 (IL-6) and IL-8 release in healthy human subjects. Clin. Diagn. Lab.
Immunol., 2003, 10, 495-7. [52] Peerschke, E.I.; Ghebrehiwet, B. The contribution of gC1qR/p33 in
infection and inflammation. Immunobiology, 2007, 212, 333-42. [53] Eric, J.; Gabra, B.H.; Sirois, P. Implication of the bradykinin
receptors in antigen-induced pulmonary inflammation in mice. Br. J. Pharmacol., 2003, 138, 1589-97.
[54] Gordon, J.R.; Zhang, X.; Stevenson, K.; Cosford, K. Thrombin induces IL-6 but not TNFalpha secretion by mouse mast cells:
threshold-level thrombin receptor and very low level FcepsilonRI signaling synergistically enhance IL-6 secretion. Cell Immunol.,
2000, 205, 128-35. [55] Lan, R.S.; Knight, D.A.; Stewart, G.A.; Henry, P.J. Role of PGE(2)
in protease-activated receptor-1, -2 and -4 mediated relaxation in the mouse isolated trachea. Br. J. Pharmacol., 2000, 131, 689-94.
[56] Graff, J.; Klinkhardt, U.; Schini-Kerth, V.B.; Harder, S.; Franz, N.; Bassus, S.; Kirchmaier, C.M. Close relationship between the
platelet activation marker CD62 and the granular release of platelet-derived growth factor. J. Pharmacol. Exp. Ther., 2002,
300, 952-7. [57] Asokananthan, N.; Graham, P.T.; Fink, J.; Knight, D.A.; Bakker,
A.J.; McWilliam, A.S. Thompson, P.J.; Stewart, G.A. Activation of protease-activated receptor (PAR)-1, PAR-2, and PAR-4 stimulates
IL-6, IL-8, and prostaglandin E2 release from human respiratory epithelial cells. J. Immunol., 2002, 168, 3577-85.
[58] Hirota, Y.; Osuga, Y.; Yoshino, O.; Koga, K.; Yano, T.; Hirata, T.
Nose, E.; Ayabe, T.; Namba, A.; Tsutsumi, O.; Taketani, Y. Possible roles of thrombin-induced activation of protease-activated
receptor 1 in human luteinized granulosa cells. J. Clin. Endocrinol. Metab., 2003, 88, 3952-7.
[59] Meli, R.; Raso, G.M.; Cicala, C.; Esposito, E.; Fiorino, F.; Cirino, G. Thrombin and PAR-1 activating peptide increase iNOS
expression in cytokine-stimulated C6 glioma cells. J. Neurochem., 2001, 79, 556-63.
[60] Mule, F.; Baffi, M.C.; Capparelli, A.; Pizzuti, R. Involvement of nitric oxide and tachykinins in the effects induced by protease-
activated receptors in rat colon longitudinal muscle. Br. J. Pharmacol., 2003, 139, 598-604.
[61] Bernatowicz, M.S.; Klimas, C.E.; Hartl, K.S.; Peluso, M.; Allegretto, N.J.; Seiler, S.M. Development of potent thrombin
receptor antagonist peptides. J. Med. Chem., 1996, 39, 4879-87. [62] Rahman, A.; True, A.L.; Anwar, K.N.; Ye, R.; Voyno-
Yasenetskaya, T.A.; Malik, A.B. Galpha(q) and Gbetagamma regulate PAR-1 signaling of thrombin-induced NF-kappaB
activation and ICAM-1 transcription in endothelial cells. Circ. Res., 2002, 91, 398-405.
[63] Caunt, M.; Huang, Y.Q.; Brooks, P.C.; Karpatkin, S. Thrombin induces neoangiogenesis in the chick chorioallantoic membrane. J.
Thromb. Haemost., 2003, 1, 2097-102. [64] Riewald, M.; Petrovan, R.J.; Donner, A.; Ruf, W. Activated protein
C signals through the thrombin receptor PAR1 in endothelial cells. J. Endotoxin Res., 2003, 9, 317-21.
[65] Malamud, V.; Vaaknin, A.; Abramsky, O.; Mor, M.; Burgess, L.E.; Ben-Yehudah, A. Lorberboum-Galski, H. Tryptase activates
peripheral blood mononuclear cells causing the synthesis and release of TNF-alpha, IL-6 and IL-1 beta: possible relevance to
multiple sclerosis. J. Neuroimmunol., 2003, 138, 115-22. [66] Wu, C.C.; Hwang, T.L.; Liao, C.H.; Kuo, S.C.; Lee, F.Y.; Lee,
C.Y.; Teng, C.M. Selective inhibition of protease-activated receptor 4-dependent platelet activation by YD-3. Thromb.
Haemost., 2000, 87, 1026-33. [67] Temkin, V.; Kantor, B.; Weg, V.; Hartman, M.L.; Levi-Schaffer, F.
Tryptase activates the mitogen-activated protein kinase/activator protein-1 pathway in human peripheral blood eosinophils, causing
cytokine production and release. J. Immunol., 2002, 169, 2662-9. [68] Shpacovitch, V.M.; Brzoska, T.; Buddenkotte, J.; Stroh, C.;
Sommerhoff, C.P.; Ansel, J.C.; Schulze-Osthoff, K.; Bunnett, N.W.; Luger, T.A.; Steinhoff, M. Agonists of proteinase-activated
receptor 2 induce cytokine release and activation of nuclear transcription factor kappaB in human dermal microvascular
endothelial cells. J. Invest. Dermatol., 2002, 118, 380-5. [69] O'Brien, P.J.; Koi, H.; Parry, S.; Brass, L.F.; Strauss, J.F. 3rd.;
Wang, L.P.; Tomaszewski, J.E.; Christenson, L.K. Thrombin receptors and protease-activated receptor-2 in human placentation:
receptor activation mediates extravillous trophoblast invasion in vitro. Am. J. Pathol., 2003, 163, 1245-54.
[70] Kanke, T.; Macfarlane, S.R.; Seatter, M.J.; Davenport, E.; Paul, A.; McKenzie, R.C.; Plevin, R. Proteinase-activated receptor-2-
mediated activation of stress-activated protein kinases and inhibitory kappa B kinases in NCTC 2544 keratinocytes. J. Biol.
Chem., 2001, 276, 31657-66. [71] Jikuhara, A.; Yoshii, M.; Iwagaki, H.; Mori, S.; Nishibori, M.;
Tanaka, N. MAP kinase-mediated proliferation of DLD-1 carcinoma by the stimulation of protease-activated receptor 2. Life
Sci., 2003, 73, 2817-29. [72] Kim, M.S.; Jo, H.; Um, J.Y.; Yi, J.M.; Kim, D.K.; Choi, S.C.; Kim,
T.H.; Nah, Y.H.; Kim, H.M.; Lee, Y.M. Agonists of proteinase-activated receptor 2 induce TNF-alpha secretion from astrocytoma
cells. Cell Biochem. Funct., 2002, 20, 339-45. [73] Koo, B.H.; Chung, K.H.; Hwang, K.C.; Kim, D.S. Factor Xa
induces mitogenesis of coronary artery smooth muscle cell via activation of PAR-2. FEBS Lett., 2002, 523, 85-9.
[74] Lindner, J.R.; Kahn, M.L.; Coughlin, S.R.; Sambrano, G.R.; Schauble, E.; Bernstein, D. Foy, D.; Hafezi-Moghadam, A.; Ley,
K. Delayed onset of inflammation in protease-activated receptor-2-deficient mice. J. Immunol., 2000, 165, 6504-10.
[75] Uehara, A.; Sugawara, S.; Muramoto, K.; Takada, H. Activation of human oral epithelial cells by neutrophil proteinase 3 through
protease-activated receptor-2. J. Immunol., 2002, 169, 4594-603. [76] Seeliger, S.; Derian, C.K.; Vergnolle, N.; Bunnett, N.W.; Nawroth,
R.; Schmelz, M.; Von Der Weid, P.Y.; Buddenkotte, J.;

42 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
Sunderkötter, C.; Metze, D.; Andrade-Gordon, P.; Harms, E.;
Vestweber, D.; Luger, T.A.; Steinhoff, M. Proinflammatory role of proteinase-activated receptor-2 in humans and mice during
cutaneous inflammation in vivo. FASEB J., 2003, 17, 1871-85. [77] Bretschneider, E.; Spanbroek, R.; Lotzer, K.; Habenicht, A.J.;
Schror, K. Evidence for functionally active protease-activated receptor-3 (PAR-3) in human vascular smooth muscle cells.
Thromb. Haemost., 2003, 90, 704-9. [78] Baek, O.S.; Kang, O.H.; Choi, Y.A.; Choi, S.C.; Kim, T.H.; Nah,
Y.H.; Kwon, D.Y.; Kim, Y.K.; Kim, Y.H.; Bae, K.H.; Lim, J.P.; Lee, Y.M. Curcumin inhibits protease-activated receptor-2 and -4-
mediated mast cell activation. Clin. Chim. Acta., 2003, 338, 135-41.
[79] Kim, S.; Foster, C.; Lecchi, A.; Quinton, T.M.; Prosser, D.M.; Jin, J.; Cattaneo, M.; Kunapuli, S.P. Protease-activated receptors 1 and
4 do not stimulate G(i) signaling pathways in the absence of secreted ADP and cause human platelet aggregation independently
of G(i) signaling. Blood, 2002, 99, 3629-36. [80] Sabri, A.; Guo, J.; Elouardighi, H.; Darrow, A.L.; Andrade-
Gordon, P.; Steinberg, S.F. Mechanisms of protease-activated receptor-4 actions in cardiomyocytes. Role of Src tyrosine kinase.
J. Biol. Chem., 2003, 278, 11714-20. [81] Ollivier, V.; Bentolila, S.; Chabbat, J.; Hakim, J.; de Prost, D.
Tissue factor-dependent vascular endothelial growth factor production by human fibroblasts in response to activated factor VII.
Blood, 1998, 91, 2698-703. [82] Marutsuka, K.; Hatakeyama, K.; Sato, Y.; Yamashita, A.;
Sumiyoshi, A.; Asada, Y. Protease-activated receptor 2 (PAR2) mediates vascular smooth muscle cell migration induced by tissue
factor/factor VIIa complex. Thromb. Res., 2002, 107, 271-6. [83] Riewald, M.; Ruf, W. Mechanistic coupling of protease signaling
and initiation of coagulation by tissue factor. Proc. Natl. Acad. Sci. USA, 2001, 98, 7742-7.
[84] Hjortoe, G.M.; Petersen, L.C.; Albrektsen, T.; Sorensen, B.B.; Norby, P.L.; Mandal, S.K.; Pendurthi, U.R.; Rao, L.V. Tissue
factor-factor VIIa-specific up-regulation of IL-8 expression in MDA-MB-231 cells is mediated by PAR-2 and results in increased
cell migration. Blood, 2004, 103, 3029-37. [85] Sethi, A.S.; Lees, D.M.; Douthwaite, J.A.; Corder, R. Factor VIIa
stimulates endothelin-1 synthesis in TNF-primed endothelial cells by activation of protease-activated receptor 2. Clin. Sci., (Lond)
2005, 108, 255-63. [86] Bachli, E.B.; Pech, C.M.; Johnson, K.M.; Johnson, D.J.;
Tuddenham, E.G.; McVey, J.H. Factor Xa and thrombin, but not factor VIIa, elicit specific cellular responses in dermal fibroblasts.
J. Thromb. Haemost., 2003, 9, 1935-44. [87] McLean, K.; Schirm, S.; Johns, A.; Morser, J.; Light, D.R. FXa-
induced responses in vascular wall cells are PAR-mediated and inhibited by ZK-807834. Thromb. Res., 2001, 103, 281-97.
[88] Szaba, F.M.; Smiley, S.T. Roles for thrombin and fibrin(ogen) in cytokine/chemokine production and macrophage adhesion in vivo.
Blood, 2002, 99, 1053-9. [89] Colognato, R.; Slupsky, J.R.; Jendrach, M.; Burysek, L.; Syrovets,
T.; Simmet, T. Differential expression and regulation of protease-activated receptors in human peripheral monocytes and monocyte-
derived antigen-presenting cells. Blood, 2003, 102, 2645-52. [90] Stouffer, G.A.; Runge, M.S. The role of secondary growth factor
production in thrombin-induced proliferation of vascular smooth muscle cells. Semin. Thromb. Hemost., 1998, 24, 145-150.
[91] Ahn, H.S.; Foster, C.; Boykow, G.; Stamford, A.; Manna, M.; Graziano, M. Inhibition of cellular action of thrombin by N3-
cyclopropyl-7-[[4-(1-methylethyl)phenyl]methyl]-7H-pyrrolo[3,2-f]quinazoline-1,3-diamine (SCH 79797), a nonpeptide thrombin
receptor antagonist. Biochem. Pharmacol., 2000, 60, 1425-34. [92] Arisato, T.; Sarker, K.P.; Kawahara, K.; Nakata, M.; Hashiguchi,
T.; Osame, M.; Kitajima, I.; Maruyama, I. The agonist of the protease-activated receptor-1 (PAR) but not PAR3 mimics
thrombin-induced vascular endothelial growth factor release in human smooth muscle cells. Cell Mol. Life Sci., 2003, 60, 1716-24.
[93] Wang, H.; Ubl, J.J.; Stricker, R.; Reiser, G. Thrombin (PAR-1)-induced proliferation in astrocytes via MAPK involves multiple
signaling pathways. Am. J. Physiol. Cell Physiol., 2002, 283, C1351-64.
[94] Houliston, R.;A.; Keogh, R.J.; Sugden, D.; Dudhia, J.; Carter, T.D.; Wheeler-Jones, C.P. Protease-activated receptors upregulate
cyclooxygenase-2 expression in human endothelial cells. Thromb.
Haemost., 2002, 88, 321-8. [95] Choi, M.S.; Kim, Y.E.; Lee, W.J.; Choi, J.W.; Park, G.H.; Kim,
S.D.; Jeon, S.J.; Go, H.S.; Shin, S.M.; Kim, W.K.; Shin, C.Y.; Ko, K.H. Activation of protease-activated receptor1 mediates induction
of matrix metalloproteinase-9 by thrombin in rat primary astrocytes. Brain Res. Bull., 2008, 76, 368-75.
[96] Billich, A.; Urtz, N.; Reuschel, R.; Baumruker, T. Sphingosine kinase 1 is essential for proteinase-activated receptor-1 signalling
in epithelial and endothelial cells. Int. J. Biochem. Cell Biol., 2009, 41,1547-55.
[97] Smiley, S.T.; King, J.A.; Hancock, W.W. Fibrinogen stimulates macrophage chemokine secretion through toll-like receptor 4. J.
Immunol., 2001, 167, 2887-94. [98] Lee, M.E.; Rhee, K.J.; Nham, S.U. Fragment E derived from both
fibrin and fibrinogen stimulates interleukin-6 production in rat peritoneal macrophages. Mol. Cell., 1999, 9, 7-13.
[99] Lee, M.E.; Kweon, S.M.; Nham, S.U. Fibrin stimulates microfilament reorganization and IL-1 beta production in human
monocytic THP-1 cells. Mol. Cell, 2001, 11, 13-20. [100] Liu, X.; Piela-Smith, T.H. Fibrin(ogen)-induced expression of
ICAM-1 and chemokines in human synovial fibroblasts. J. Immunol., 2000, 165, 5255-61.
[101] Sharma, J.N. The kallikrein-kinin system: from mediator of inflammation to modulator of cardioprotection.
Inflammopharmacology, 2005, 12, 591-6. [102] Schmaier, A.H. The elusive physiologic role of Factor XII. J. Clin.
Invest., 2008, 118, 3006-9. [103] Ghebrehiwet, B.; CebadaMora, C.; Tantral, L.; Jesty, J.; Peerschke,
E.I. gC1qR/p33 serves as a molecular bridge between the complement and contact activation systems and is an important
catalyst in inflammation. Adv. Exp. Med. Biol., 2006, 586, 95-105. [104] Erdös, E.; Skidgel, R. Metabolism of bradykinin by peptidases in
health and disease. In: Farmer, S.; Ed.; The kinin system. San Diego: Academic Press; 1997, p. 111–41.
[105] Kaplan, A.P.; Joseph, K.; Shibayama, Y.; Nakazawa, Y.; Ghebrehiwet, B.; Reddigari, S.; Silverberg, M. Bradykinin
formation. Plasma and tissue pathways and cellular interactions. Clin. Rev. Allergy Immunol., 1998, 16, 403-29.
[106] Markiewski, M.M.; Lambris, J.D. The role of complement in inflammatory diseases from behind the scenes into the spotlight.
Am. J. Pathol., 2007, 171, 715-27. [107] Joseph, K.; Kaplan, A.P. Formation of bradykinin: a major
contributor to the innate inflammatory response. Adv. Immunol., 2005, 86, 159-208.
[108] Zhao, Y.; Qiu, Q.; Mahdi, F.; Shariat-Madar, Z.; Rojkjaer, R.; Schmaier, A.H. Assembly and activation of HK-PK complex on
endothelial cells results in bradykinin liberation and NO formation. Am. J. Physiol. Heart Circ. Physiol., 2001, 280, H1821–9.
[109] Kaplan, A.P.; Joseph, K.; Silverberg, M. Pathways for bradykinin formation and inflammatory disease. J. Allergy Clin. Immunol.,
2002, 109, 195-209. [110] Sainz, I.M.; Uknis, A.B.; Isordia-Salas, I.; DeLa Cadena, R.A.;
Pixley, R.A.; Colman, R.W. Interactions between bradykinin (BK) and cell adhesion molecule (CAM) expression in peptidoglycan-
polysaccharide (PG-PS)-induced arthritis. FASEB J., 2004, 18, 887-9.
[111] Cunha, T.M.; Verri, W.A.Jr; Fukada, S.Y.; Guerrero, A.T.; Santodomingo-Garzón, T.; Poole, S.; Parada, C.A.; Ferreira, S.H.;
Cunha, F.Q. TNF-alpha and IL-1beta mediate inflammatory hypernociception in mice triggered by B1 but not B2 kinin
receptor. Eur. J. Pharmacol., 2007, 573, 221-9. [112] Rodriguez, J.A.; De la Cerda, P.; Collyer, E.; Decap, V.; Vio, C.P.;
Velarde, V. Cyclooxygenase-2 induction by bradykinin in aortic vascular smooth muscle cells. Am. J. Physiol. Heart. Circ. Physiol.,
2006, 290, H30-6. [113] Zaczynska, E.; Gabra, B.H.; Sirois, P. Bradykinin stimulates MMP-
2 production in guinea pig tracheal smooth muscle cells. Inflammation, 2003, 27, 307-15.
[114] Fleming, I.; Fisslthaler, B.; Busse, R. Calcium signaling in endothelial cells involves activation of tyrosine kinases and leads to
activation of mitogen-activated protein kinases. Circ. Res., 1995, 76, 522-9.
[115] Marrero, M.B.; Venema, V.J.; Ju, H.; He, H.; Liang, H.; Caldwell, R.B.; Venema, R.C. Endothelial nitric oxide synthase interactions
with G protein-coupled receptors. Biochem. J., 1999, 343, 335-40.

Coagulation-Dependent Inflammation Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 43
[116] Venema, R.C. Post-translational mechanisms of endothelial nitric
oxide synthase regulation by bradykinin. Int. Immunopharmacol., 2002, 2, 1755-62.
[117] Velarde, V.; Ullian, M.E.; Morinelli, T.A.; Mayfield, R.K.; Jaffa, A.A. Mechanisms of MAPK activation by bradykinin in vascular
smooth muscle cells. Am. J. Physiol., 1999, 277, C253-61. [118] Ju, H.; Venema, V.J.; Liang, H.; Harris, M.B.; Zou, R.; Venema,
R.C. Bradykinin activates the Janus-activated kinase/signal transducers and activators of transcription (JAK/STAT) pathway in
vascular endothelial cells: localization of JAK /STAT signaling proteins in plasmalemmal caveolae. Biochem. J., 2000, 351, 257-
64. [119] Huang, C.D.; Tliba, O.; Panettieri, R.A. Jr; Amrani, Y. Bradykinin
induces interleukin-6 production in human airway smooth muscle cells: modulation by Th2 cytokines and dexamethasone. Am. J.
Respir. Cell Mol. Biol., 2003, 28, 330-8. [120] Brunius, G.; Domeij, H.; Gustavsson, A.; Yucel-Lindberg, T.
Bradykinin upregulates IL-8 production in human gingival fibroblasts stimulated by interleukin-1beta and tumor necrosis
factor alpha. Regul. Pept., 2005, 126, 183-8. [121] McNicol, A.; Israels, S.J. Beyond hemostasis: the role of platelets
in inflammation, malignancy and infection. Cardiovasc. Hematol. Disord. Drug Targets, 2008, 8, 99-117.
[122] Danese, S.; Fiocchi, C. Platelet activation and the CD40/CD40 ligand pathway: mechanisms and implications for human disease.
Crit. Rev. Immunol., 2005, 25, 103-21. [123] Peerschke, E.I.; Yin, W.; Ghebrehiwet, B. Platelet mediated
complement activation. Adv. Exp. Med. Biol., 2008, 632, 81-91. [124] Huber-Lang, M.; Sarma, J.V.; Zetoune, F.S.; Rittirsch, D.; Neff,
T.A.; McGuire, S.R.; Lambris, J.D.; Warner, R.L.; Flierl, M.A.; Hoesel, L.M.; Gebhard, F.; Younger, J.G.; Drouin, S.M.; Wetsel,
R.A.; Ward, P.A. Generation of C5a in the absence of C3: a new complement activation pathway. Nat. Med., 2006, 12, 682-687.
[125] Peerschke, E.I.B.; Yin, W.; Grigg, S.E.; Ghebrehiwet, B. Blood platelets activate the classical pathway of human complement. J.
Thromb. Haemost., 2006, 4, 2035-42. [126] Esmon, C.T. Crosstalk between inflammation and thrombosis.
Maturitas, 2004, 47, 305-14. [127] Chu, A.J. Role of Tissue Factor in Thrombosis: Coagulation-
Inflammation-Thrombosis circuit. Front. Biosci., 2006, 11, 256-71. [128] Del Rosso, M.; Fibbi, G.; Pucci, M.; Margheri, F.; Serrati, S. The
plasminogen activation system in inflammation. Front. Biosci., 2008, 13, 4667-86.
[129] White, B.; Schmidt, M.; Murrph, C.; Livingstone, W.; O’Toole, D.O.; Lawler, M. Activated protein C inhibits lipopolysaccharide-
induced nuclear translocation of nuclear factor B (NF- B) and tumor necrosis factor (TNF- ) production in the THP-1 moncytic
cell line. Br. J. Haematol., 2000, 110, 130-4. [130] Barnard, G.R.; Ely, E.W.; Wright, T.J.; Fraiz, J.; Stasek, J.E.;
Russell, J.A.; Mayers, I.; Rosenfeld, B.A.; Morris, P.E.; Yan, S.B.; Helterbrand, J.D. Safety and dose relationship of recombinant
human activated protein C for coagulopathy in severe sepsis. Crit. Care Med., 2001, 29, 2051-9.
[131] Bernard, G.R.; Vincent, J.L.; Laterre, P.F.; LaRosa, S.P.; Dhainaut, J.F.; Lopez-Rodriguez, A.; Steingrub, J.S.; Garber, G.E.;
Helterbrand, J.D.; Ely, E.W.; Fisher, C.J. Efficacy and safety of recombinant human activated protein C for severe sepsis. N. Engl.
J. Med., 2001, 344, 699-709. [132] Nimah, M.; Brilli, R.J. Coagulation dysfunction in sepsis and
multiple organ system failure. Crit. Care Clin., 2003, 19, 441-58. [133] Joyce, D.E.; Grinnell, B.W. Recombinant human activated protein
C attunates the inflammatory response in endothelium and monocytes by modulating nuclear factor-kappa B. Crit. Care Med.,
2002, 30, S288-93. [134] Uchiba, M.; Okajima, K.; Murakami, K.; Nawa, H.; Okabe, H.;
Takatsuki, K. Recombinant human soluble thrombomodolin reduces endotoxin-induced pulmonary vascular injury via protein C
activation in rats. Thromb. Haemost., 1995, 74, 1265-70. [135] Uchiba, M.; Okajima, K.; Murakami, K.; Johno, M.; Okabe, H.;
Takatsuki, K. Recombinant thrombomodulin prevents endotoxin-induced lung injury by inhbiting activation of leukocyts in rats. Am.
J. Physiol., 1996, 271, L470-5. [136] Taoka, Y.; Okajima, K.; Murakami, K.; Johno, M..
Neuroprotection by recombinant thrombomodulin. Thromb. Haemost., 2000, 83, 462-8.
[137] Uchiba, M.; Okajima, K.; Murakami, K.; Johno, M.; Okabe, H.;
Takatsuki, K. Effect of urinary thrombomodulin on endotoxin-induced intravascular coagulation and pulmonary vascular injury in
rats. Am. J. Hematol., 1997, 54, 118-23. [138] Johnson, K.; Aarden, L.; Choi, Y.; De Groot, E.; Creasey, A. The
proinflammatory cytokine response to coagulation and endotoxin in whole blood. Blood, 1996, 87, 5051-60.
[139] Chen, D.; Riesbeck, K.; McVey, J.H.; Kemball-Cook, G.; Tuddenham, E.G.; Lechler, R.I.; Dorling, A. Human thrombin and
FXa mediate porcine endothelial cell activation; modulation by expression of TFPI-CD4 and hirudin-CD4 fusion proteins.
Xenotransplantation, 2001, 8, 258-65. [140] Park, C.T.; Creasey, A.A.; Wright, S.D. Tissue factor pathway
inhibitor blocks cellular effects of endotoxin by binding to endotoxin and interfering with transfer to CD14. Blood, 1997, 89,
4268-74. [141] Kopp, C.W.; Hoelzenbein, T.; Steiner, S.; Marculescu, R.;
Bergmeister, H.; Seidinger, D. Mosberger, I.; Kaun, C.; Cejna, M.; Horvat, R.; Wojta, J.; Maurer, G.; Binder, B.R.; Breuss, J.M.;
Ecker, R.C.; de Martin, R.; Minar, E. Inhibition of restenosis by tissue factor pathway inhibitor: in vivo and in vitro evidence for
suppressed monocyte chemoattraction and reduced gelatinolytic activity. Blood, 2004, 103, 1653-61.
[142] Creasey, A.A.; Chang, A.C.; Fiegen, L.; Wun, T.C.; Taylor, F.B.; Hinshaw, L.B. Tissue factor pathway inhibitor reduces mortality
from E. Coli septic shock. J. Clin. Invest., 1993, 91, 2850-60. [143] Abraham, E.; Reinhart, K.; Opal, S.; Demeyer, I.; Doig, C.;
Rodriguez, A.L.; Beale, R.; Svoboda, P.; Laterre, P.F.; Simon, S.; Light, B.; Spapen, H.; Stone, J.; Seibert, A.; Peckelsen, C.; De
Deyne, C.; Postier, R.; Pettilä, V.; Artigas, A.; Percell, SR.; Shu, V.; Zwingelstein, C.; Tobias, J.; Poole, L.; Stolzenbach, J.C.;
Creasey, A.A.; OPTIMIST Trial Study Group. Efficacy and safety of tifacogin (recombinant tissue factor pathway inhibitor) in severe
sepsis: a randomized controlled trial. JAMA, 2003, 290, 238-47. [144] Freeman, B.D.; Zehnbauer, B.A.; Buchman, T.G. A meta-analysis
of controlled trials of anticoagulant therapies in patients with sepsis. Shock, 2003, 20, 5-9.
[145] de Jonge, E.; Dekkers, P.E.; Creasey, A.A.; Hack, C.E.; Paulson, S.K.; Karim, A.; Kesecioglu, J.; Levi, M.; van Deventer, S.J.; van
der Poll, T. Tissue factor pathway inhibitor does not influence inflammatory pathways during human endotoxemia. J. Infect. Dis.,
2001, 183, 1815-8. [146] Colotta, F.; Sciacca, F.L.; Sironi, M.; Luini, W.; Rabiet, M.J.;
Mantovani, A. Expression of monocyte chemotactic protein-1 by monocytes and endothelial cells exposed to thrombin. Am. J.
Pathol., 1994, 144, 975-85. [147] Senden, N.H.; Jeunhomme, T.M.; Heemskerk, J.W.; Wagenvoord,
R.; van't Veer, C.; Hemker, H.C.; Buurman, W.A. Factor Xa induces cytokine production and expression of adhesion molecules
by human umbilical vein endothelial cells. J. Immunol., 1998, 161, 4318-24.
[148] Mansell, A.; Reinicke, A.; Worrall, D.M.; O'Neill, L.A. The serine protease inhibitor antithrombin III inhibits LPS-mediated NF-
kappaB activation by TLR-4. FEBS Lett., 2001, 508, 313-7. [149] Isobe, H.; Okajima, K.; Uchiba, M.; Harada, N.; Okabe, H.
Antithrombin prevents endotoxin-induced hyptension by inhibiting the induction of nitric oxide synthesis in rats. Blood, 2002, 99,
1638-45. [150] Minnema, M.C.; Chang, A.C.K.; Jansen, P.M.; Lubbers, Y.T.P.;
Pratt, B.M.; Whittaker, B.G. et al. Recombinant human antithrombin III improves survival and attenuates inflammatory
responses in baboons lethally challenged with E. Coli. Blood, 2000, 95, 1117-23.
[151] Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A.; Knaub, S.;
Keinecke, H.O.; Heinrichs, H.; Schindel, F.; Juers, M.; Bone, R.C.; Opal, S.M.; KyberSept Trial Study Group. Caring for the critically
ill patients. High-dose antithrombin III in severe sepsis: a randomized controlled trial. JAMA, 2001, 286, 1869-78.
[152] Stenflo, J. Contributions of GIA and EGF-like domains to the functions of vitamin K-dependent coagulation factors. Crit. Rev.
Eukaryotic Gene Expr., 1999, 9, 59-88. [153] Eichbaum, F.W.; Slemer, O.; Zyngier, S.B. Anti-inflammatory
effect of warfarin and vitamin K1. Naunyn Schmiedebergs Arch. Pharmacol., 1979, 307, 185-90.

44 Inflammation & Allergy - Drug Targets, 2010, Vol. 9, No. 1 Arthur J. Chu
[154] Maclean, P.S.; Tait, R.C.; Rumley, A.; McMahon, A.D.; Lowe,
G.D. Anticoagulation with warfarin downregulates inflammation. J. Thromb. Haemost., 2003, 8, 1838-9.
[155] Miller, D.L.; Welty-Wolf, K.; Carraway, M.S.; Ezban, M.; Ghio, A.; Suliman, H.; Piantadosi, C.A. Extrinsic coagulation blockade
attenuates lung injury and proinflammatory cytokine release after intratracheal lipopolysaccharide. Am. J. Respir. Cell Mol. Biol.,
2002, 26, 650-8. [156] Carraway, M.S.; Welty-Wolf, K.E.; Miller, D.L.; Ortel, T.L.; Idell,
S.; Ghio, A.J.; Idell, S, Egan, J.; Zhu, X.; Jiao, J.A.; Wong, H.C.; Piantadosi, C.A. Blockade of tissue factor: treatment for organ
injury in established sepsis. Am. J. Respir. Crit. Care Med., 2003, 167, 1200-9.
[157] Taylor, F.B.; Chang, A.C.; Peer, G.; Li, A.; Ezban, M.; Hedner, U. Active site inhibited factor VIIa (DEGR VIIa) attenuates the
coagulant and interleukin-6 and -8, but not tumor necrosis factor, responses of the baboon to LD100 Escherichia coli. Blood, 1998,
91, 1609-15. [158] Arnold, C.S.; Parker, C.; Upshaw, R.; Prydz, H.; Chand, P.; Kotian,
P.; Bantia, S.; Babu, Y.S. The antithrombotic and anti-inflammatory effects of BCX-3607, a small molecule tissue
factor/factor VIIa inhibitor. Thromb. Res., 2006, 117, 343-9. [159] Lindmark, E.; Siegbahn, A. Tissue factor regulation and cytokine
expression in monocyte-endothelial cell co-cultures. Effects of a statin, an ACE-inhibitor and a low-molecular-weight heparin.
Thromb. Res., 2002, 108, 77-84. [160] Akahane, K.; Okamoto, K.; Kikuchi, M.; Todoroki, H.; Higure, A.;
Ohuchida, T.; Kitahara, K.; Takeda, S.; Itoh, H.; Ohsato, K. Inhibition of factor Xa suppresses the expression of tissue factor in
human monocytes and lipopolysaccharide-induced endotoxemia in rats. Surgery, 2001, 130, 809-18.
[161] Kaiser, B.; Jeske, W.; Walenga, J.M.; Fareed, J. Inactivation of factor Xa by the synthetic inhibitor DX-9065a causes strong
anticoagulant and antiplatelet actions in human blood. Blood Coagul. Fibrinolysis, 1999, 10, 495-501.
[162] Iba, T.; Kidokoro, A.; Fukunaga, M.; Fuse, S.; Suda, M.; Kunitada, S. et al. Factor Xa-inhibitor (DX-9065a) modulates the leukocyte-
endothelial cell interaction in endotoxemic rat. Shock, 2002, 17, 159-62.
[163] Tyrrell, D.J.; Horne, A.P.; Holme, K.R.; Preuss, J.M.H.; Page, C.P. Heparin in inflammation: potential therapectic applications beyond
anticoagulation. In: Advance in Pharmacology, 1999, Vol. 46, Academic Press, San Diego, p. 151-208.
[164] Aldea, G.S.; Scltow, L.O.; Chandler, W.L.; Triggs, C.M.; Vocelka, C.R.; Crockett, G.I. et al. Limitation of thrombin generation,
platelet activation, and inflammation by elimination of cardiotomy suction in patients undergoing coronary artery bypass grafting
treated with heparin-bonded circuit. J. Throac Cardiovasc. Surg., 2002, 123, 742-55.
[165] Koster, A.; Fischer, T.; Praus, M.; Haberzettl, H.; Kuebler, W.M.;
Hetzer, R.; Kuppe, H. Hemostatic activation and inflammatory response during cardiopulmonary bypass: impact of heparin
management. Anesthesiolgy, 2002, 97, 837-41. [166] Nylander, S.; Mattsson, C. Thrombin-induced platelet activation
and its inhibition by anticoagulants with different modes of action. Blood Coagul. Fibrinolysis, 2003, 14, 159-67.
[167] Kaplanski, G.; Marin, V.; Fabrigoule, M.; Boulay, V.; Benoliel, A.M.; Bongrand, P.; Kaplanski, S.; Farnarier, C. Thrombin-
activated human endothelial cells support monocyte adhesion in vitro following expression of intercellular adhesion molecule-1
(ICAM-1; CD54) and vascular cell adhesion molecule-1 (VCAM-1; CD106). Blood, 1998, 92, 1259-67.
[168] Johnson, K.; Choi, Y.; DeGroot, E.; Samuels, I.; Creasey, A.; Aarden, L. Potential mechanisms for a proinflammatory vascular
cytokine response to coagulation activation. J. Immunol., 1998, 160, 5130-5.
[169] Jilma-Stohlawetz, P.; Folman, C.C.; von dem Borne, A.E.; Pernerstorfer, T.; Hollenstein, U.; Knechtelsdorfer, M. et al. Effects
of anticoagulation on thrombopoietin release during endotoxemia. J. Lab Clin. Med., 2001, 137, 64-9.
[170] Cicardi, M.; Zingale, L.; Zanichelli, A.; Pappalardo, E.; Cicardi, B. C1 inhibitor: molecular and clinical aspects. Springer Semin.
Immunopathol., 2005, 27, 286-98. [171] Sánchez, J.; Olsson, P. On the control of the plasma contact
activation system on human endothelium: comparisons with heparin surface. Thromb. Res., 1999, 93, 27-34.
[172] Ulmer, J.S.; Lindquist, R.N.; Dennis, M.S.; Lazarus, R.A. Ecotin is a potent inhibitor of the contact system proteases factor XIIa and
plasma kallikrein. FEBS Lett., 1995, 365, 159-63. [173] Kirschfink, M.; Mollnes, T.E. C1-inhibitor: an anti-inflammatory
reagent with therapeutic potential. Expert Opin. Pharmacother, 2001, 2, 1073-83.
[174] Lehmann, A. Ecallantide (DX-88), a plasma kallikrein inhibitor for the treatment of hereditary angioedema and the prevention of blood
loss in on-pump cardiothoracic surgery. Expert Opin. Biol. Ther., 2008, 8, 1187-99.
[175] Fuhrer, G.; Gallimore, M.J.; Heller, W.; Hoffmeister, H.E. Aprotinin in cardiopulmonary bypass--effects on the Hageman
factor (FXII)--Kallikrein system and blood loss. Blood Coagul. Fibrinolysis, 1992, 3, 99-104.
[176] Kuduk, S.D.; Bock, M.G. Bradykinin B1 receptor antagonists as novel analgesics: a retrospective of selected medicinal chemistry
developments. Curr. Top. Med. Chem., 2008, 8, 1420-30. [177] Banfi, C.; Brioschi, M.; Barcella, S.; Pignieri, A.; Parolari, A.;
Biglioli, P.; Tremoli, E.; Mussoni, L. Tissue factor induction by protease-activated receptor 1 requires intact caveolin-enriched
membrane microdomains in human endothelial cells. J. Thromb. Haemost., 2007, 5, 2437-44.
Received: August 20, 2009 Revised: October 5, 2009 Accepted: November 2, 2009

Copyright of Inflammation & Allergy - Drug Targets is the property of Bentham Science Publishers Ltd. and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.

























![Abnormalities of Blood Coagulation[1]](https://img.pdfslide.us/doc/110x75/577cce2b1a28ab9e788d80ee/abnormalities-of-blood-coagulation1.jpg)
