Embed Size (px)
Citation preview

HEMOSTASIS AND BLOOD COAGULATION
HemostasisThe ability of the body to control the flow of blood following vascular injury is paramount to continued survival. The process of blood clotting (coagulation) and then the subsequent dissolution of the clot, following repair of the injured tissue, is termed hemostasis. It actually has 3 separate stages:
1. The vascular phase2. The platelet phase3. The coagulation phase
1) Vascular phase Cutting or damaging blood vessels leads to vascular spasm of the smooth muscle in the vessel wall. This produces a vasoconstriction which will slow or even stop blood flow. This response will last up to 30 minutes and is localized to the damaged area.
2) Platelet phaseDamaged endothelial cells lining the blood vessel release von Willebrand's Factor. This substance makes the surfaces of the endothelial cells "sticky". This condition may, by itself, be enough to close small blood vessels. In larger blood vessels, platelets begin to stick to the surfaces of endothelial cells. This effect is called Platelet Adhesion.
The platelets that adhere to the vessel walls now begin to secrete Adenosine diphosphate (ADP) which is released from "stuck" platelets. This material causes the aggregation of nearby free platelets which attach to the fixed platelets and each other. This aggregation of platelets leads to the formation of a platelet plug. This clumping of platelets serves a number of functions:a. It can plug the break in a small blood vessel.b. Aggregated platelets release Platelet Thromboplastin (Factor III) which activates the clotting
process.c. Clumped platelets provide a surface essential for the clotting process. Along with ADP, the
clumped platelets secrete thromboxane, a powerful vasoconstrictor.
3) Coagulation Phase Begins 30 seconds to several minutes after phases I and II have commenced. The overall process involves the formation of the insoluble protein Fibrin from the plasma protein Fibrinogen through the action of the enzyme Thrombin. Fibrin forms a network of fibers which traps blood cells and platelets forming a thrombus or clot. This process depends on the presence in the blood of 11 different clotting factors (proteins) and calcium (Factor IV).
Factor Number
Common Name Function
I Fibrinogen Forms clot (fibrin)

II Prothrombin Its active form activates I, V, VII, VIII, XI, XIII, protein C, platelets
III Tissue Factor Co-factor of VIIa (formerly known as factor III)
IV Ca2+ Required for coagulation factors to bind to phospholipid
V Proaccelerin Co-factor of X with which it forms the prothrombinase complex
VII Proconvertin Activates IX, XVIII Antihemophilic Factor A Co-factor of IX with which it forms
the tenase complexIX Antihemophilic Factor B or
Christmas FactorActivates X: forms tenase complex with factor VIII
X Stuart Factor Activates II: forms prothrombinase complex with factor V
XI Plasma thromboplastin antecedent
Activates IX
XII Hageman factor Activates factor XI, VII and prekallikrein
XIII Fibrin Stabilizing Factor Crosslinks fibrinTable: Showing all the 12 different clotting factors with respective functions
Ultimately, these factors will generate the production of Prothrombin Activator (Factor X). Depending on the initial trigger for the clotting reactions, there are two pathways leading to the formation of the thrombus; the Extrinsic Pathway and the Intrinsic Pathway.
i. Extrinsic Pathway –It is initiated with material outside of or "extrinsic" to the blood. This material, Tissue Thromboplastin (Factor III), is released by damaged tissue cells. Factor III permits the clotting process to take a chemical shortcut. As a result, the extrinsic pathway is a very rapid process, i.e., within 12 to 15 seconds. However, the production of Thrombin is low and the resulting clot is small. This pathway is most effective as a "quick patch" process. Tissue Thromboplastin (Factor III) activates Factor VII (Calcium dependent step). Factor VII then activates Factor X - Prothrombin Activator (Calcium dependent step).
ii. Intrinsic Pathway - It is initiated by the blood coming in contact with exposed collagen in the blood vessel wall, i.e., material within the blood or blood vessel wall. This process is considerably slower (5 to 10 minutes) but results in the formation of larger amounts of thrombin. This allows the formation of larger clots. Factor XII is activated by making contact with exposed collagen underlying the endothelium in the blood vessel wall. Factor XII activates Factor XI. Factors XII and XI (contact activation product) jointly activate Factor IX. Factor IX activates Factor VIII. Factor VIII together with Calcium ions and Factor III from platelets (Platelet Thromboplastin) activate Factor X - Prothrombin

Activator. Since Factor III is released from activated platelets, the completion of the Intrinsic Pathway depends on there being an adequate number of platelets in circulation.
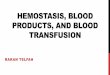
It should be noted that both pathways lead to the same reaction, namely, the activation of Factor X - Prothrombin Activator. From this point on, both pathways follow the same course to Fibrin formation. For this reason the steps from Factor X activation to Fibrin formation are referred to as the Common Pathway.
Common Pathway- Factor X (active) engages in a series of reactions with Factor V, Calcium ions and phospholipids derived from platelets. This composite of clotting factors and their reactions is referred to as the Factor V Complex or Prothrombin Activator. Factor V Complex initiates the conversion of Prothrombin to active form of the enzyme Thrombin. Thrombin accelerates the formation of Fibrin threads from Fibrinogen (Factor I).
Figure: Intrinsic and extrinsic pathway

Clot Retraction After 2 or 3 days, the clot begins to contract. Platelets in the clot contain contractile proteins. These proteins pull the edges of the wound together and reduce the chance of further hemorrhage. This activity also assists the repair processes.
Fibrinolysis When the clotting cascade is activated, so is the process of fibrinolysis. This is basically a mechanism that prevents clotting from getting out of control, and prevents the excessive deposition of fibrin. It is also the process of degrading or dissolution the fibrin clot when it is no longer needed. The breakdown of the clot is due to the production of a powerful proteolytic enzyme Plasmin. The main mechanism involved is the release of tissue plasminogen activator (tPA) by damaged endothelial cells. These circulating activators will then convert plasminogen to plasmin, which then breaks down fibrin clot.
ANTICOAGULANT
An anticoagulant is a substance that prevents coagulation (clotting) of blood. Anticoagulants reduce blood clotting. This prevents deep vein thrombosis (when a blood clot forms in one of the large veins in leg or arm), pulmonary embolism (a blood clot that forms in, or travels to, lungs), myocardial infarction and stroke. Anticoagulants is required if one has been diagnosed with or treated for one or more of the following:1. Atrial fibrillation (AF)2. Artificial heart valve3. Deep vein thrombosis (DVT)4. Pulmonary embolism (PE)5. Prevention of blood clots e.g. genetic clotting disorders6. Stroke7. Heart Attack
Table: Showing some of the common anticoagulant drugs
DIRECT THROMBIN INHIBITORS (DTIs)

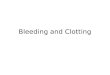
Current members of this class include the bivalent drugs hirudin, lepirudin, and bivalirudin; and the monovalent drugs argatroban and dabigatran. DTIs inhibit thrombin by two ways; bivalent DTIs block simultaneously the active site and exosite 1 and act as competitive inhibitors of fibrin,[12] while univalent DTIs block only the active site and can therefore both inhibit unbound and fibrin-bound thrombin as shown in the figure below. Thus, DTIs are able to inactivate both fibrin-bound and unbound thrombin, unlike UFH and LMWH.
Figure: Showing the three domains (one active site and two exosites); exosite 1 acts as a dock for substrates such as fibrin in order to promote orientation for active site binding, and exosite 2 is
the heparin-binding domain.
Argatroban: Argatroban is a selective thrombin inhibitor that binds reversibly to the active site of the thrombin molecule. Thrombin, a serine protease, is responsible for the conversion of fibrinogen to fibrin in the coagulation cascade. It does not require the cofactor antithrombin. It exerts its anticoagulant effects by inhibiting thrombin-catalyzed or -induced reactions, including fibrin formation; activation of coagulation factors V, VIII, and XIII; protein C formation; and platelet aggregation.
Dabigatran: Dabigatran etexilate is an inactive pro-drug that is converted to dabigatran, the active form, by esterase-catalyzed hydrolysis in the plasma and liver. Dabigatran, the main active principle in plasma, is a rapid-acting competitive and reversible direct inhibitor of thrombin. Inhibition of thrombin consequently prevents thrombus development. Dabigatran inhibits free thrombin, fibrin-bound thrombin and thrombin-induced platelet aggregation.
Lepirudin: Lepirudin binds to thrombin and prevents thrombus or clot formation. It is a highly potent, selective, and essentially irreversible inhibitor of thrombin and clot-bond thrombin. Lepirudin forms a stable non-covalent complex with alpha-thrombin, thereby abolishing its ability to cleave fibrinogen and initiate the clotting cascade. The inhibition of thrombin prevents the blood clotting cascade.
Drug name
Bivalent/ Univalent
Route ofadministration
Metabolism Binding toactive site
Indications

and/or exositeArgatroban Univalent Parenteral (iv) Hepatical,
mostly biliaryReversible Prevention and
treatment ofthrombosis inpatients withHIT
Dabigatran etexilate
Univalent Oral Primarily renal, remainder isconjugated with glucuronic acid in liver
Reversible Prevention ofstroke andembolism inpatients withAF
Lepirudin Bivalent Parenteral (iv/sc)
Renal Irreversible Prevention offurtherthrombosis inpatients withHIT
Table: Overview of some DTIs
Common Side Effects: Heart failure; bleeding in injection site, wounds and allergic skin reactions; nosebleed; gastrointestinal and rectal bleeding; abnormal kidney function, blood in urine and vaginal bleeding; anemia and sepsis; abnormal liver function; pneumonia; miscellaneous effects like- fever and nausea.
INDIRECT THROMBIN INHIBITORS
Heparin: Heparin and its low molecular weight derivatives (e.g. enoxaparin, dalteparin, tinzaparin) are effective at preventing deep vein thromboses and pulmonary emboli in patients at risk. Heparin binds to the enzyme inhibitor antithrombin III (AT) causing a conformational change that results in its activation through an increase in the flexibility of its reactive site loop. The rate of inactivation thrombin and other proteases involved in blood clotting by AT can increase by up to 1000-fold due to the binding of heparin.
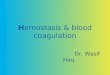
1. Unfractionated heparin (UFH): AT binds to a specific pentasaccharide sulfation sequence contained within the unfractionated heparin polymer. The conformational change in AT on heparin-binding mediates its inhibition of factor Xa. For thrombin inhibition, however, thrombin must also bind to the heparin polymer at a site proximal to the pentasaccharide. The highly negative charge density of heparin contributes to its very strong electrostatic interaction with thrombin. The formation of a ternary complex between AT, thrombin, and heparin results in the inactivation of thrombin. For this reason, heparin's activity against thrombin is size-dependent, the ternary complex requiring at least 18 saccharide units for efficient formation. In contrast, anti-factor Xa activity requires only the pentasaccharide binding site. It can be given either subcutaneously or intravenously.

2. Low-molecular-weight heparins (LMWH): LMWH (e.g. enoxaparin) target anti-factor Xa activity rather than anti-thrombin activity, with the aim of facilitating a more subtle regulation of coagulation and an improved therapeutic index. With LMWH there is a reduced risk of osteoporosis and heparin-induced thrombocytopenia (HIT).
Figure: A- To inactivate thrombin, unfractionated heparin forms a ternary complex with antithrombin and thrombin. B- Because of their lower molecular weight, LMWH species are unable to form the ternary complexes with antithrombin and thrombin. Thus, LMWHs produce their anticoagulant effect mainly by inhibiting factor Xa.
Side effects of heparin:1. Haemorrhage – the risk is greatest in the elderly, and may be exacerbated by alcohol intake.
This is by far the most common side effect.2. Osteoporosis – can occur if the drug is used for more than a few weeks. This does not occur
with LMWH’s.3. Thrombocytopaenia – can occur after 7-10 days of therapy. It is a result of heparin induced
antiplatelet antibodies.4. Hyperkalaemia – due to inhibition of aldosterone secretion5. Hypersensitivity
Fondaparinux: Fondaparinux is indicated for the prophylaxis of deep vein thrombosis, which may lead to pulmonary embolism in patients undergoing hip fracture surgery, hip replacement surgery or knee replacement surgery. The antithrombotic activity of fondaparinux is the result of

antithrombin III [ATIII]-mediated selective inhibition of Factor Xa. Fondaparinux binds specifically to ATIII and activates it. Bound to fondaparinux, antithrombin selectively and rapidly inhibits factor Xa. By inhibiting factor Xa, thrombin generation and fibrin formation are blocked. Fondaparinux is further released to act on other molecules of antithrombin. Thus fondaparinux potentiates the innate neutralization of Factor Xa by ATIII. Neutralization of Factor Xa interrupts the blood coagulation cascade and thus inhibits thrombin formation and thrombus development.
Drug name Route ofadministration
Metabolism Excretion
Indications
Fondaparinux SC Eliminated unchanged in urine
Renal Prophylaxis & treatment ofacute deep vein thrombosis
Table: Overview of fondaparinux
Figure: Mechanism of action of fondaparinux.
Side-effects of fondaparinux: Anemia; Hematoma; Hypokalemia; Hypotension; Thrombocytopenia; Urinary tract infection; edema; fever; insomnia; local irritation (injection site bleeding; pruritus; rash;); nausea
VITAMIN K ANTAGONISTS
Warfarin: Warfarin (also known under the brand names Coumadin) is an anticoagulant normally used in the prevention of thrombosis and thromboembolism, the formation of blood clots in the blood vessels and their migration elsewhere in the body respectively.

Figure: Schematic diagram of the action of warfarin
Warfarin prevents the formation of blood clots by altering the metabolism of vitamin K. Warfarin effectively prohibits the synthesis of clotting factors, called II, VII, IX and X, which are dependent on vitamin K.
Factors II ( Prothrombin), VII, IX and X have, at their amino terminus, a series of glutamate residues (Glu)-typically 9 to 12. These factors are vitamin K dependent. In a post translational modification in the liver, the glutamate residues are carboxylated in presence of O2, CO2 and the enzyme carboxylase, to form γ- carboxyglutamate (Gla) residues. Vitamin K is essential for the process. The clotting factors need carboxylation of glutamic acid residues to bind phospholipids to the clotting factors.
The carboxylation process is associated with the vitamin K cycle and is related to the oxidation of vitamin K, which produces vitamin K epoxide. Vitamin K epoxide is then reduced to its hydroquinone form by an enzyme called vitamin K epoxide reductase (VKOR). Vitamin K hydroquinone then catalyses the carboxylation process and is converted to its epoxide. This is then converted back to vitamin K hydroquinone by VKOR.
Warfarin prohibits the actions of VKOR, by binding competitively with the enzyme and reducing the available stores of vitamin K and the production of clotting (coagulation) factors. These results in decreased prothrombin levels and a decrease in the amount of thrombin generated and bound to fibrin. This reduces the thrombogenicity of clots.
Side-effects: Haemorrhage – this is especially common to the bowel and brain; hematuria (blood in the urine); epistaxis (nose bleed); ecchymosis (bruising); teratogenicity (meaning it causes birth defects); necrosis of soft tissues -rare and occurs mainly to tissues in buttock and breast and due to thrombosis in venules; leukopenia (decrease in white blood cell count), and agranulocytosis (no white blood cell production).

DIRECT Xa INHIBITORS
Oral drugs such as rivaroxaban and apixaban work by inhibiting factor Xa directly. These are oral, reversible, specific inhibitors of factor Xa. They inhibit both free and fibrin bound Xa. They effectively block the amplification of the coagulation cascade, preventing the formation of thrombus. These are unqiue anticoagulant for two reasons. First of all, they do not involve antithrombin III (ATIII) to exert their anticoagulant effects. Secondly, these are oral agent whereas the widely used unfractionated heparin and low molecular weight heparins are for parenteral use only. By inhibiting FXa, these drugs decrease thrombin generation and thrombus development.
Figure: Mechanism of action of Xa inhibitors
Side-effects: Upper GI, lower GI, and rectal bleeding (0.1% to 1%); skin rash (less than 1%); anaphylactic reactions (such as allergic edema) (less than 1%); intracranial bleeding (0.33%); syncope (less than 1%); intraocular bleed (0.21%).
ANTI-INHIBITOR COAGULANT COMPLEX
Coagulant drugs, also called anti-inhibitor coagulant complexes, treat blood coagulation disorders associated with inhibitors of factors VIII, XI or XII. Such drugs are used to treat and prevent hemorrhage. It is also used to treat or prevent bleeding in people with hemophilia A or B and Factor VIII inhibitors and to control bleeding during surgery. They are made from proteins normally found in human blood plasma that allow the blood to clot. Anti-inhibitor coagulant complex contains substances called coagulation factors (e.g., non-activated Factors II, IX, and X, and activated Factor VII) that are normally produced in the body. The exact mechanisms of anti-inhibitor coagulant complex is unknown, although it may be related to one or more of the active clotting factors, in DIC (disseminated intravascular coagulation), in fibrinolysis, or if there are normal coagulation mechanisms present.

Commonly used brand name(s): Autoplex T, Feiba NF, Feiba VH Immuno
Autoplex T: Autoplex-T is a partially activated prothrombin complex concentrate used primarily for the treatment of patients expressing factor VIII inhibitors. This medication is a clotting factor, prescribed for bleeding episodes or bleeding during surgery in patients with Factor VIII inhibitors. Its mechanism of action is not clearly known. Route of administration is IV. The recommended dosage range is 25 to 100/kg. Side effects include headache; lethargy; nausea; chest discomfort; chills; fever; flushing; hypotension; myocardial infarction; tachycardia; thromboembolic events; hypersensitivity reactions.
FEIBA NF: FEIBA NF (Anti-Inhibitor Coagulant Complex), nanofiltered and vapor heated, is a freeze-dried sterile human plasma fraction with Factor VIII inhibitor bypassing activity. It is manufactured from large plasma pools of human plasma. FEIBA NF contains Factors II, IX, and X, mainly non-activated, and Factor VII mainly in the activated form. In vitro and animal model data suggest that FEIBA NF has a mechanism of action that targets several processes in both the extrinsic and intrinsic pathways of coagulation:1. Factors II and Xa can directly support clot formation, producing thrombin on the back of the
activated platelet downstream from the inhibitor blockade.2. The other activated and non-activated factors raise the enzyme and substrate level of
coagulation and are believed to contribute to the bypassing hemostatic effect of FEIBA NF.
FEIBA NF is identical in formulation to FEIBA VH.
Figure: In vitro and animal model data suggested mechanism of action





















![Hemostasis & Coagulation Disorders(Ringkas II) - Dicky [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/577cc4cd1a28aba7119a7e52/hemostasis-coagulation-disordersringkas-ii-dicky-compatibility-mode.jpg)